a&p - respiratory system
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
Primary role of respiratory system
Supply the blood with oxygen and remove carbon dioxide from the body
The five steps of respiration
Breathing
Alveolar gas exchange
Gas transport
Systemic gas exchange
Aerobic respiration
Breathing
Movement of air into and out of lungs
Gas transport of respiration
Transport of O2 and CO2 between the lungs and tissue with the help of cardiovascular system
Systemic gas exchange of respiration
Exchange of O2 and CO2 between blood in systemic capillaries and tissue cells
Aerobic respiration
The use of O2 and production of CO2 during ATP production
External respiration
breathing and alveolar gas exchange
Involves respiratory system structures
Internal respiration
Systemic gas exchange and aerobic respiration
Along with gas exchange the respiratory system is responsible for:
detecting odor
Producing sound
Regulating blood pH - should be between 7.35 to 7.45. Also called acid base balance
Trapping and defending the body from airborne pathogen
Assisting in movement of venous blood and lymph
Which structures compose the upper respiratory tract?
Nose and pharynx
Which structures compose the lower respiratory tract?
Larynx, trachea, bronchi, and lungs
Respiratory mucosa
mucous membranes containing pseudostratified ciliated columnar epithelium
Lines rest of nasal cavity, larynx, trachea, and bronchi
Goblet cells
Air is warmed by blood vessels in mucosae
Cilia move trapped particles to pharynx where they can be swapped
Digested by gastric juice
Goblet cells
In epithelium produce mucus - moisten incoming air and trap particles
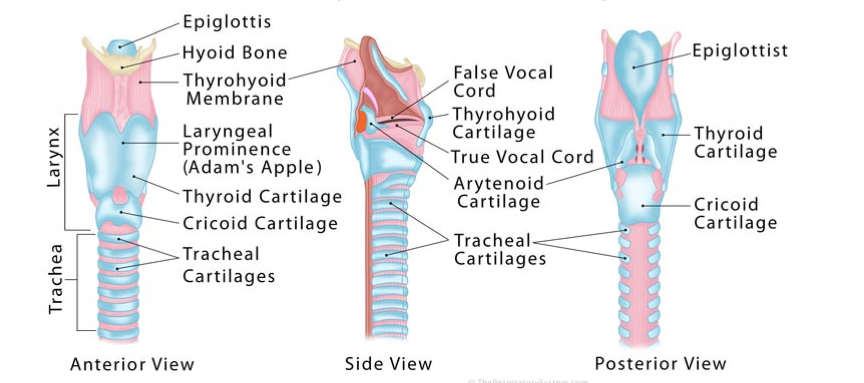
Larynx
cartilaginous and box life structure
Passageway for air between pharynx and trachea
Thyroid cartilage Adam’s Apple
Cricoid cartilage connects to trachea
Epiglottis - flap to keep solids and liquids out
Supported by ligaments that extend from hyoid bone
Vocal folds
Vestibular folds
Vocal folds - larynx
2 bands of elastic connective tissue covered by respiratory mucosa
Relaxed during resting breathing
Vibrate when contracted to produce sound
Pitch is determined by vibration frequency
Loudness is determined by vibration amplitude
Vestibular folds - larynx
lie above vocal folds
Keep solids and liquids from entering glottis
No role in sound production
Glottis
Vocal folds and space between them
Changes in larynx during swallowing
goal is to keep stuff out and direct to esophagus
Muscles lift this up
Epiglottis folds over to cover glottis
Food is directed into esophagus
Trachea
Airway that extends from larynx into thoracic cavity
branches form right and left main bronchi
tracheal cartilages support it
Inner wall lined by respiratory mucosa
Tracheal cartilage
Holds airway open during breathing. Open portion allows esophagus to expand slightly during swallowing
The exchange of oxygen and carbon dioxide between alveoli and blood is called:
alveolar gas exchange
The use of oxygen and production of carbon dioxide during ATP production is called:
aerobic respiration
Bronchi
2 main bronchi of trachea → three lobar bronchi in right lung and two in left → segmental bronchi
Walls have cartilaginous rings
Are pathogens and disease in upper or lower respiratory tract more dangerous?
Lower because they do not have mucous to get rid of particles
Bronchioles
very small tubes lacking cartilage that branch from bronchi
Smooth muscle for air flow - bronchoconstriction and dilation
Lined with mucous membrane containing simple cuboids epithelium. Can’t remove particles
what do the main bronchi branch branch into?
lobar bronchi
what do lobar bronchi branch into?
segmental bronchi - one for each segments within each lung
Alveolar ducts
Branches from smallest bronchioles that terminate in pulmonary alveoli
Pulmonary alveoli
Filled with watery fluid to aid in diffusion
need to fill with air for oxygen and carbon dioxide to exchange
Surrounded with capillary network both arterial and veinular
Site of alveolar gas exchange - bronchial tree and bronchioles have no role
Surfactant prevents collapse during exhalation - reduces attraction between water molecules
where does alveolar gas exchange occur?
across the respiratory membrane with pulmonary alveoli
lungs consist of:
pulmonary alveoli
air passageway
blood and lympathic vessels
nerves
connective tissue
how many lobes does the left lung have?
2
how many lobes does the right lung have?
3
lung lobes
separated by the mediastinum. each lobe is supplied by a lobar bronchus, blood vessels, lymphatic vessels, and nerves
pleurae
two layers of serous membrane that surround each lung
viseral pleura
parietal pleura
pleural cavity
pleural cavity
space in lungs filled with pleural fluid which:
reduces friction between pleurae
helps hold the pleural together
when one pleura expands the other must also to expand the lungs
breathing
the process of exchanging air between atmosphere and pulmonary alveoli
air moves along an air pressure gradient (high to low)
the three pressures important to breathing
atmospheric, intra-alveolar, and intrapleura
intrapleural pressure
pressure within the pleural cavity
•Keeps lungs pressed against inner walls of thoracic cage
•Keeps lungs expanded even during exhale
→ If it equaled atmosphere pressure, lungs would collapse
for inspiration what must happen to intra-alveolar pressure?
it must be reduced to less than atmospheric air pressure
diaphragm in resting inspiration
Moves downward and flattens with contraction
external intercostals
Elevate and protract ribs and push sternum forward with contraction
process of resting inspiration
•Thoracic cavity size increases
•Lungs are pulled along when the thoracic cage expands
•Increases lung volume and decreases intra-alveolar pressure to -1 centimeter H_2 O
•Higher atmospheric pressure pushes air towards the lower intra-alveolar pressure in lungs
Air inflow continues until both pressures are equal
forceful inspiration requires what additional muscles?
sternocleidomastoid, serratus anterior, pectoralis minor
contraction further elevates and protracts ribs which requires more of an increase in thoracic cavity volume
what must happen to intra-alveolar pressure for expiration?
it must be elevated above atmospheric pressure
resting expiration
Diaphragm and external intercostals relax
Thoracic cavity and lungs to return to original size
Aided by abundant elastic tissue in lungs and thoracic wall
process of resting expiration
•The decrease in lung volume increases intra-alveolar pressure to +1 centimeter H_2 O
•High intra-alveolar pressure pushes air out of lungs
•Air outflow continues until both pressures are equal
forceful expiration requires what additional muscles?
internal intercostal muscles
depress and retract the ribs
contraction of abdominal muscles
force abdominal viscera and diaphragm up
muscle role in forceful expiration
Muscle contraction further decreases volume of lungs
Causes a greater increase in intra-alveolar pressure, causing more air to flow out
tidal volume - in spirogram
•Volume of air exchanged during a resting breathing cycle
•Approximately 500mililiters
inspiratory reserve volume
•Maximum volume of air that can be forcefully inhaled after a tidal inspiration
•Approximately 3,000mL
Expiratory reserve volume - spirogram
•Maximum volume of air forcefully exhaled after a tidal expiration
•Approximately 1,100mL
residual volume - spirogram
•Volume of air remaining in lungs after expelling ERV
•Approximately 1,200mL
•Exists because of intrapleural pressure and surfactant
Vital capacity - spirogram
•Maximum amount of air that an be forcefully exchanged
•TV + IRV + ERV
Approximately 4,600mL
total lung capacity - spirogram
VC + RV
Approximately 5,800 mL
what controls involuntary breathing?
centers in the medulla oblongata and pons
ventral respiratory group
dorsal respiratory group
pontine respiratory group
what controls voluntary breathing?
primary motor area of the cerebral cortex
ventral respiratory group
in medulla oblongata
Responsible for normal rhythmic cycle of breathing
Neurons rhythmically send action potentials to diaphragm and external intercostals
Action potentials cause muscles to contract
When action potentials stop, muscles relax
dorsal respiratory group
•Center for receiving and integrating input from sensory sources
•Sends action potentials to VRG to alter breathing as the needs of the body change
•Deeper or shallower, faster or slower
pontine respiratory group
Located in pons
Receives input from higher brain centers
Sends action potentials to DRG and VRG to modify breathing pattern
Has neurons that stimulate or inhibit the VRG and DRG
Alters the rate and depth of breathing
Adapts breathing to speaking, singing, exercise, sleep, and emotional responses (crying, gasping)
chemical factors affecting respiration
csf most important
co2
h+
by product of co2 transport therefore an increase in co2 will increase this concentration
o2
chemoreceptors
in medulla oblongata detect changes in H^+ and CO_2 in CSF
in carotid and aortic bodies detect changes in H^+, CO_2, and O_2 in blood
what happens if co2 and h+ increase in blood or csf?
DRG stimulates the VRG to increase rate and depth of breathing
→ Causes loss of CO_2 and H^+, which lowers levels to homeostasis
what happens if co2 and h+ decreases in blood or csf?
breathing will be shallow and slow
→ Provides time for concentrations to increase back to homeostasis
what parts are sensitive to decline in o2 concentration?
carotid and aortic bodies
•Increases the sensitivity of chemoreceptors in respiratory area to changes in CO_2 concentrations
it does not alter rate or depth of breathing unless very low
Action potentials voluntarily generated by cerebral cortex involved in breathing
Created when a person chooses to alter the pattern of resting breathing
Voluntary control is limited
Involuntary action potentials from cerebral cortex and hypothalamus involved in breathing
•Created during emotional experiences that activate the autonomic division
Fear, anxiety, and excitement can lead to an increase in breathing rate
Sudden emotional experience, sharp pain, or sudden cold stimulus can cause apnea
respiratory disorders are grouped as:
inflammatory and noninflammatory disorders
chronic obstructive pulmonary disease
inflammatory
long term obstruction that reduces airflow to and from the lungs
chronic bronchitis
emphysema
emphysema
inflammatory disorder caused from long term exposure to airborne irritants
exhaling requires voluntary effort
Uncommon except in long term smokers or people with long term exposure to second hand smoke
No cure but can be prevented and progressive deterioration can be stopped by removing the irritant
Effects:
Large spaces form when pulmonary alveoli rupture
Air trapped in pulmonary alveoli due to excess mucus production in bronchioles
Reduces respiratory surface area and impairs gas exchange
inflammatory disorders include:
asthma, influenza, and pneumonia
lung cancer
Second most common cancer, leading cause of cancer death in Americans
Develops due to long-term exposure to irritants, such as cigarette smoke
Metastasizes rapidly and spreads quickly to other body areas
Treatments include surgery and chemotherapy