Fitzgerald PMHNP Cert Exam Review 2026 Complete Questions and Answers Solved 100%
1/158
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
159 Terms
Chapter 2: Select Special Topics in Psychiatric-Mental Health Practice
Clinical Decision Making Process
• ADPIE
-Assessment: 1st step, subjective and objective data
• Diagnosis: analysis, formulation of nursing diagnosis
• Planning: prioritizing problems, determining goals, plan of care
• Implementation: nursing action (rather than medical action)
• Evaluating: comparing outcomes, communicate and document findings
Aspartate aminotransferase (AST)
Alanine aminotransferase (ALT)
Range?
Measures?
0-40 units/L
0-40 units/L
Hepatocellular damage
Potentially elevated in valproate therapy, hepatitis, cirrhosis
Glutamyltransferase (GGT)
Alkaline phospatase (ALP)
Range?
Measures?
Examples?
0-30 units/L
30-120 international units/L
Cholestasis: bike flow, either extrahepatic or intrahepatic
Elevated in alcohol abuse.
Elevated in gallbladder disease, liver disease. Elevated with bone injury
Creatine Kinase (CK)
Range?
Measures?
Examples?
0-139 units/L
Muscle Injury. muscle enzyme found in skeletal and cardiac muscle;
elevated blood levels associated with heart attack, muscular dystrophy, and other skeletal muscle pathologies
Urea Nitrogen (BUN)
Creatinine
8-20 mg/dL
0.6-1.2 mg/dl
Kidney Function
Increased in impaired kidney function
Measured with lithium therapy
Creatinine is more sensitive and specific indicator of kidney disease than BUN.
Measured with lithium therapy.
Glomerular Filtration Rate (GFR)
Range?
Measures?
Examples?
>90mL/min.
The best measurement of kidney function.
the amount of filtrate formed per minute by the two kidneys combined
Elderly pts have 30% reduced because of decreased muscle mass
Generally no dose adjustments or contraindications with psychotropics when GFR >60mL/min
Valproate and select epileptic drugs ex. Carbamazepine.
Lab testing?
Level?
Comment?
Discontinue when?
Liver pane (ALT, AST, ALP, bilirubin, albumin, total protein), CBC, WBC, platelet count, serum hCG, valproate level.
Level 50-120mcg/ml
Discontinue valproate with AST/ALT elevations >2-3x upper limit of normal.
Valpro ate a folate PLaTe
Lithium
Labs testing?
Comment?
What meds to avoid?
Creatine, bun, GFR, TSH, serum electrolytes, CBC, hCG, urinalysis.
Baseline EKG
Check serum lithium level 12 hour post dose (trough) after 4 days in medication. Then every 4-5 days.
Lithium level 0.6-1.2
LMNOP
Reduce lithium dose if GFR<60ml/min.
Lithium levels affected my renal function, sodium balance, water balance.
Toxicity occurs at levels >2mmol/L
Avoid medications that increase lithium levels
ACE inhibitors, ARB, NSAIDs
Tetracyclines
Potassium soaring diuretics
Thiazide diuretics
Clozapine (Clozaril)
Labs?
Comment?
Pt needs ANC > 1500/mm to initiate therapy.
Interrupt treatment if ANC < 1000/mm
Rems Program.
Chance of Agranulocytosis 1-2%.
Hemoglobin
PLT
Male 13.5-18
Female 12.5-14
If outside of these ranges anemia can resemble depression with fatigue.
140,000-340,000
Low is Thrombocytopenia can be seen in Valproate therapy.
inCarbamazpine (Tegretol) and Phenobarbital (Luminal) are very strong inducers of the 3A4 system. Remember Carb and Barb.
Bupropion, Fluoxetine, and paroxetine are the most commonly encountered strond inhibitors of 2D6. Remember Big Freakin Problems
Valproate inhibits the metabolism of Lamotrigine. When prescribing VALproate with lamotrigine, use HALf the dose of LAmotrigine to avoid killing your patient and sending them to VALHALLA.
Use NAGging WORry to remind yourself of non-prescription interactions.
N is for Nicotine P450 (CYP) 1A2 and 2B6 inducers
A is for Alcohol
G is for Grape-fruit juice.
WOR is for St. John's wort 3A4 inducer
50% of all prescription medications are CYP450 3A4 substrates.
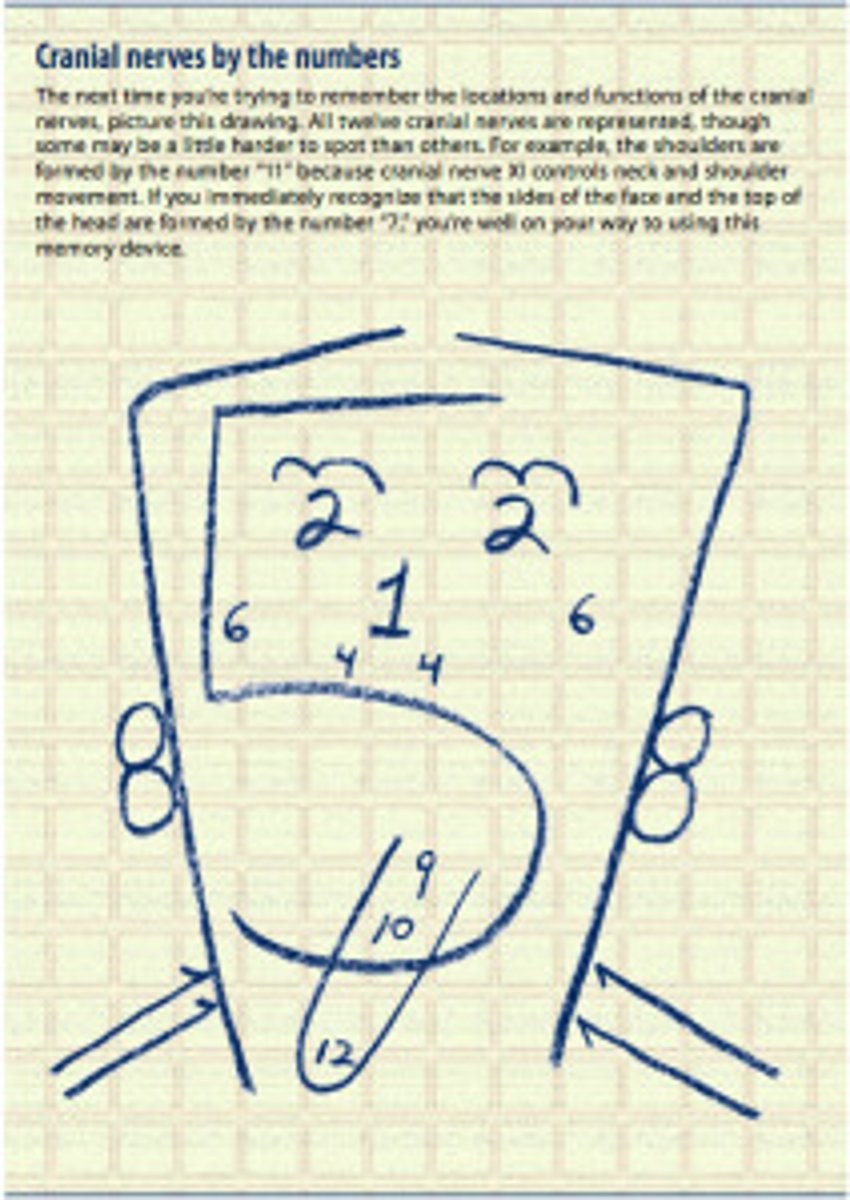
Cranial Nerves function
oh oh oh to touch and feel a great vein ah heaven!
1. olfactory = smell
2. optic = Vision
3. oculomotor = Eye lid and eye-ball movement
4. trochlear = moves eyeball downward and laterally
5. trigeminal = sensation of face, scalp, eyes, nose, mouth. innervates muscles of mastication
6. abducens = abducts eyes, turns them laterally
7. facial = innervates muscles of facial expression & digastric muscle (and lacrimal & salivary glands). sensation of tongue.
8. vestibulocochlear = sensation of hearing & equilibrium. adjusts sensitivity of sensory receptors.
9. glossopharyngeal = Taste Senses, innervates pharnygeal muscles and salivary glands. sensation of pharynx, tonsils, tongue, and receptor from cartoid artery.
10. vagus = innervates and sensation of pharynx & larynx. innervates cardiac muscle and smooth muscles of abdominal viscera. sensation of viscera. functions in parasympathetic nervous system
11. accessory = innervates sternocleidomastoid and trapezius.
12. hypoglossal = controls tongue movements
Thyroid stimulating hormone
NL?
Free T4
NL?
F
0.4-4
10-27
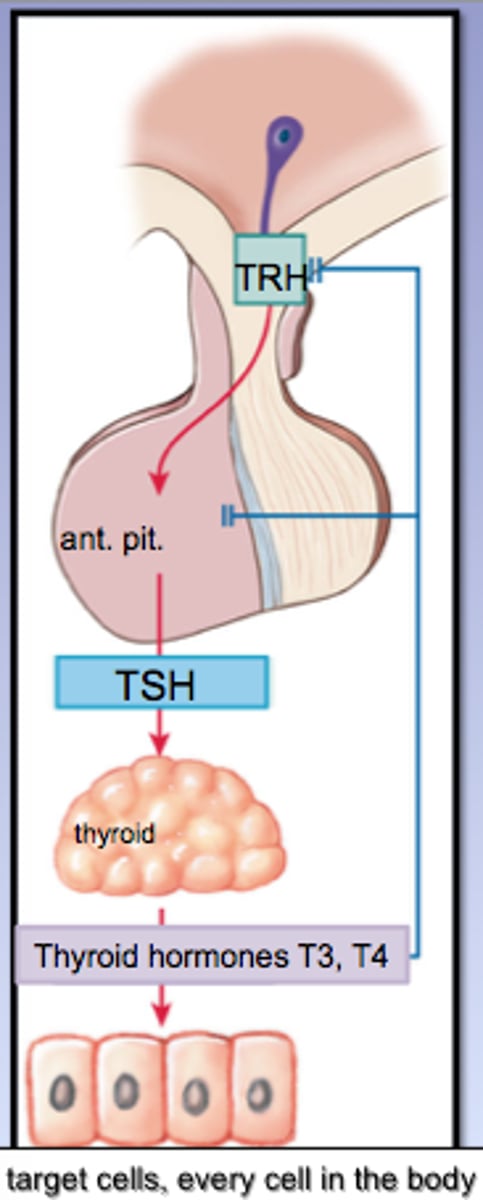
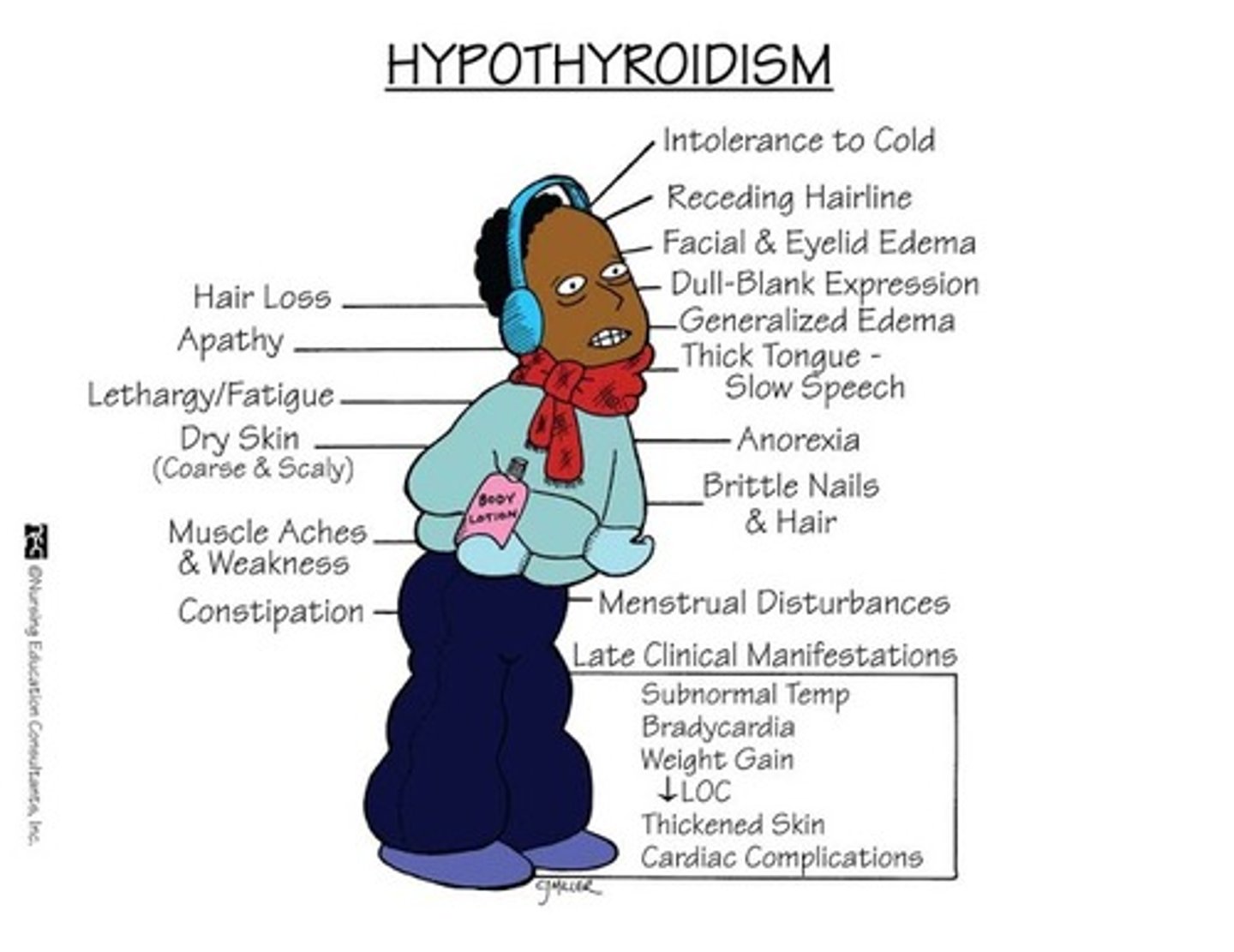
Hypothyroidism
High TSH, low T3 and T4
Hoshimotos thyroiditis
Post radioactive iodine treatment
Lithium use
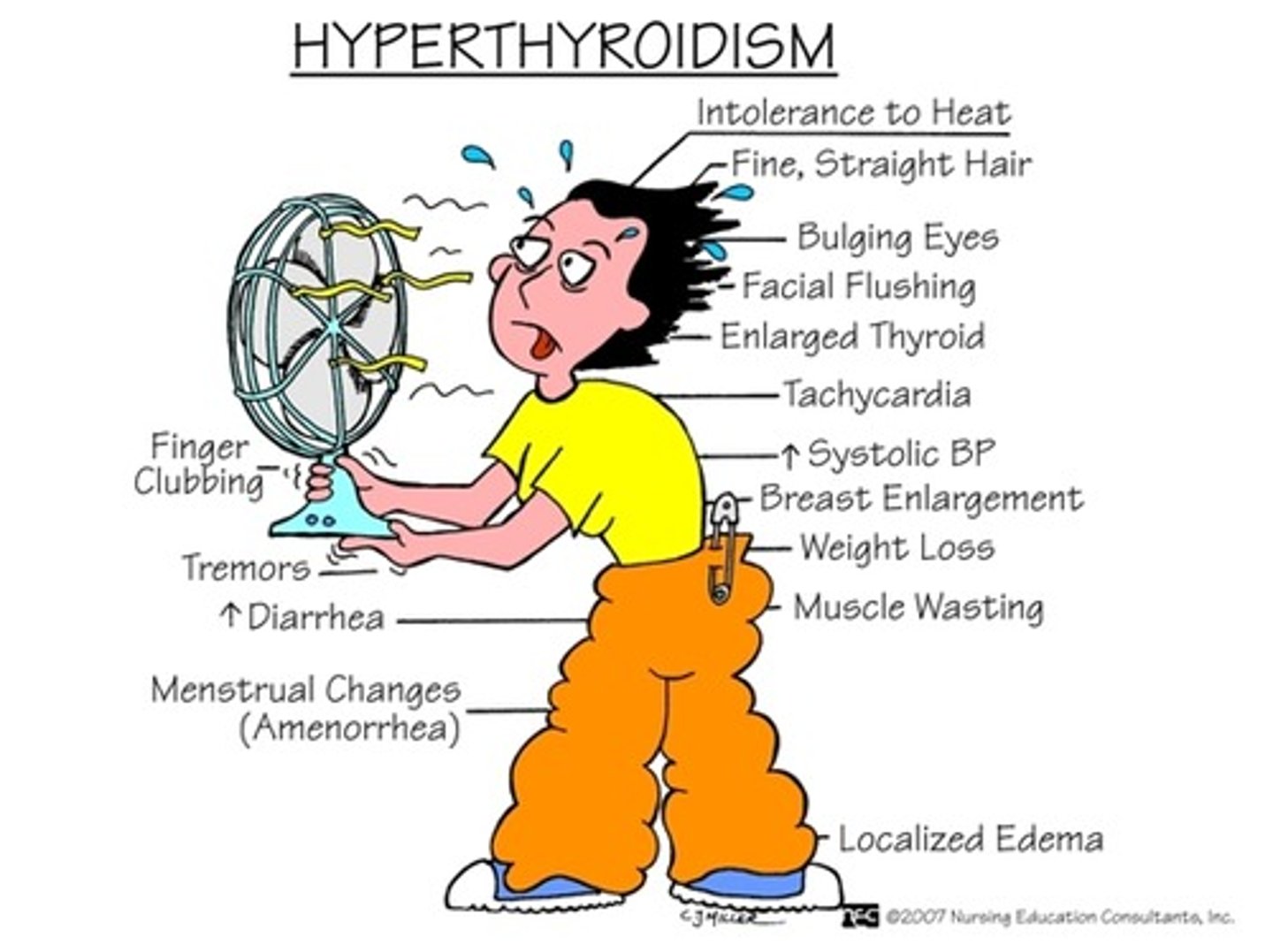
Hyperthyroidism
Low TSH, high T3 and T4
Graves disease
Toxic Adenoma
Thyroiditis
Chapter 3 Theoretical Models: Psychological, Nursing, and Developmental
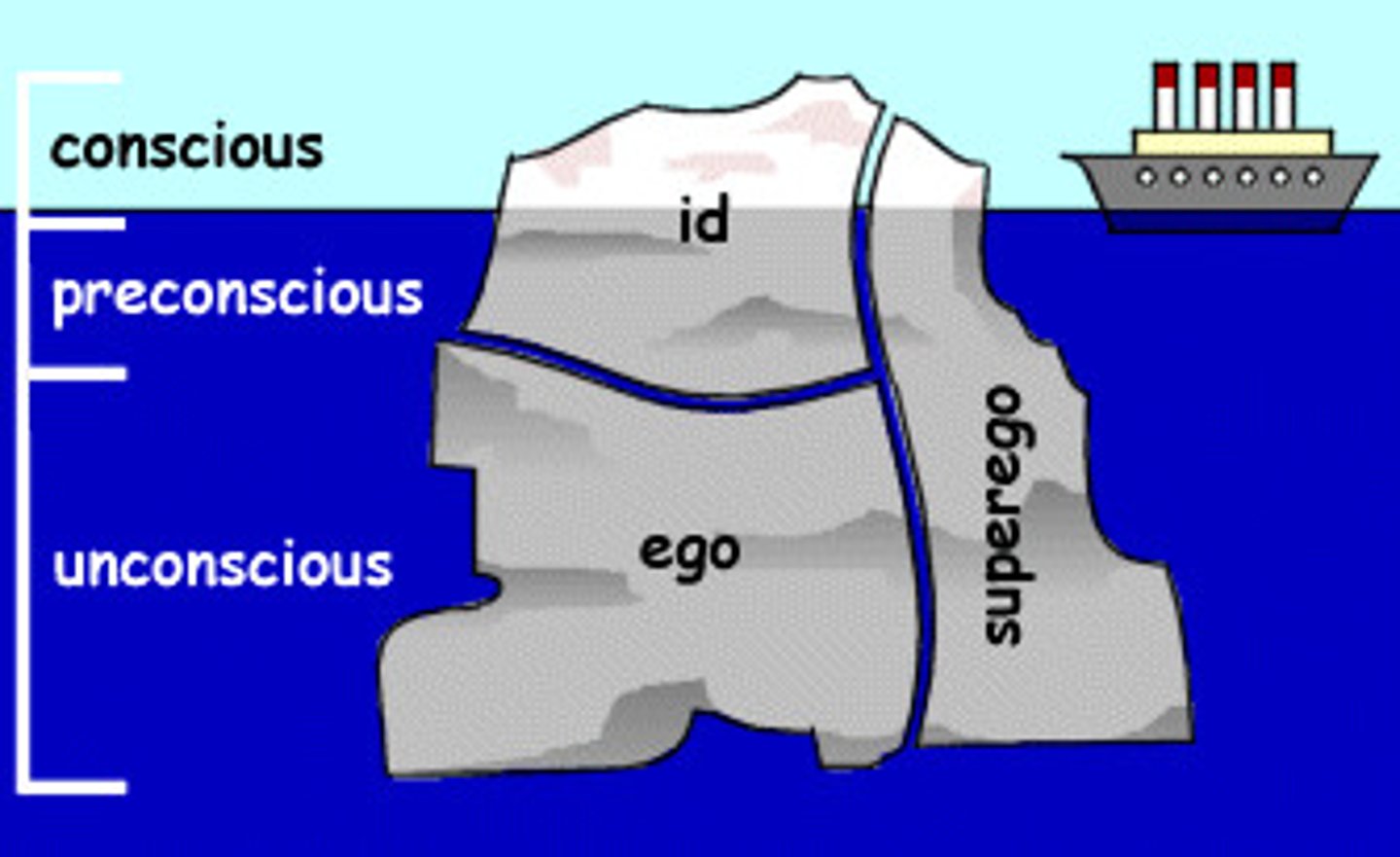
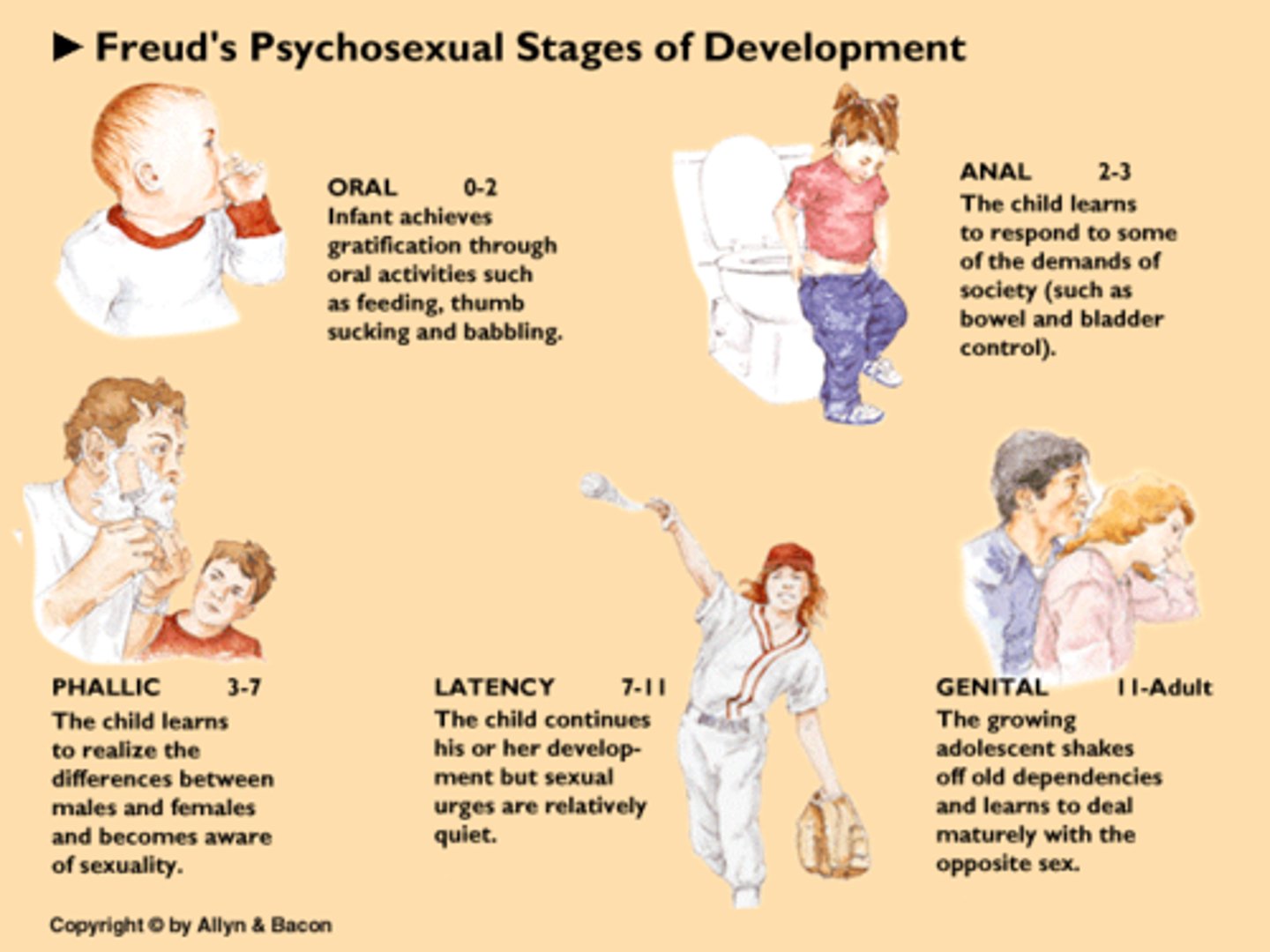
psychoanalytic theory
Stages?
A theory developed by Freud that attempts to explain personality, motivation, and mental disorders by focusing on unconscious determinants of behavior. Focuses on the Past
Freud
1. Oral Stage
2. Anal Stage
3. Phallic Stage
4. Latency Stage
5. Genital Stage
pychodynamic theory
Alfred Adler
holds that development is largely determined by how well people resolve conflicts they face at different ages
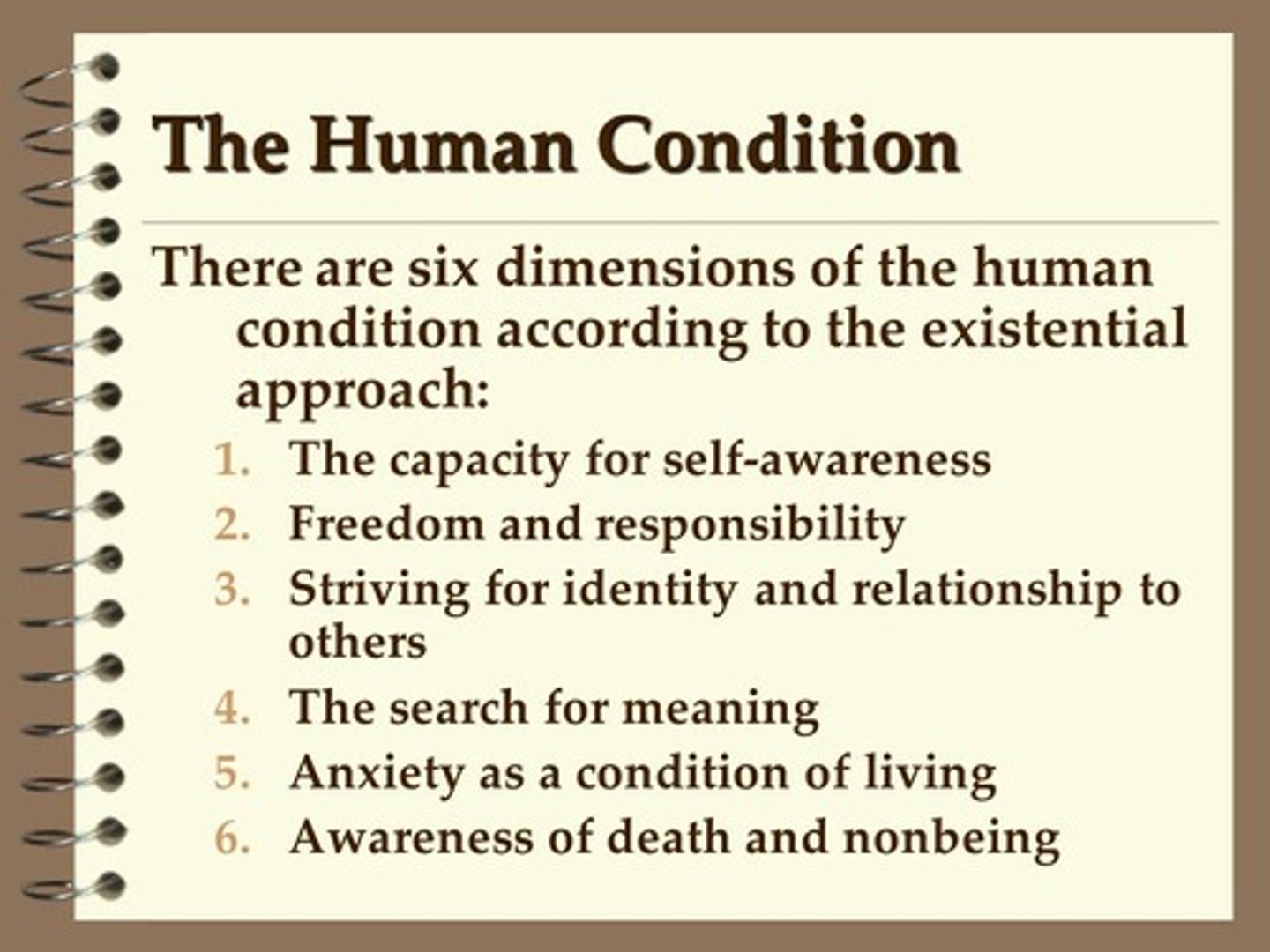
existential therapy
a therapy that encourages clients to accept responsibility for their lives and to live with greater meaning and value
Victor Frankl- Logotherapy therapy through meaning.
Rollo May
Irvin Yalom
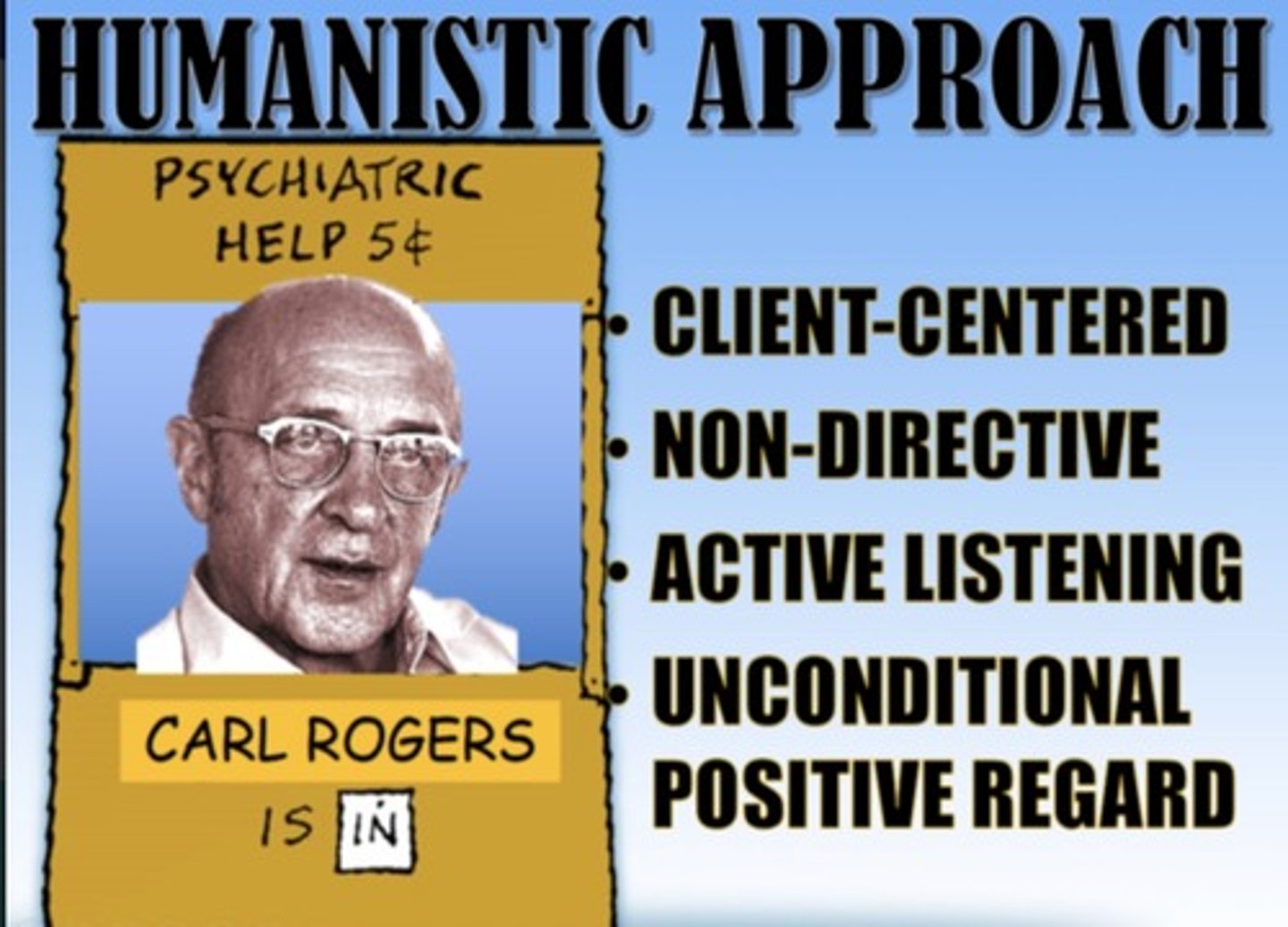
person-centered therapy
Carl Rogers
Relationship, Genuininess, Accurate Emapthy, Self-Actualization
Humanistic Motivational interviewing
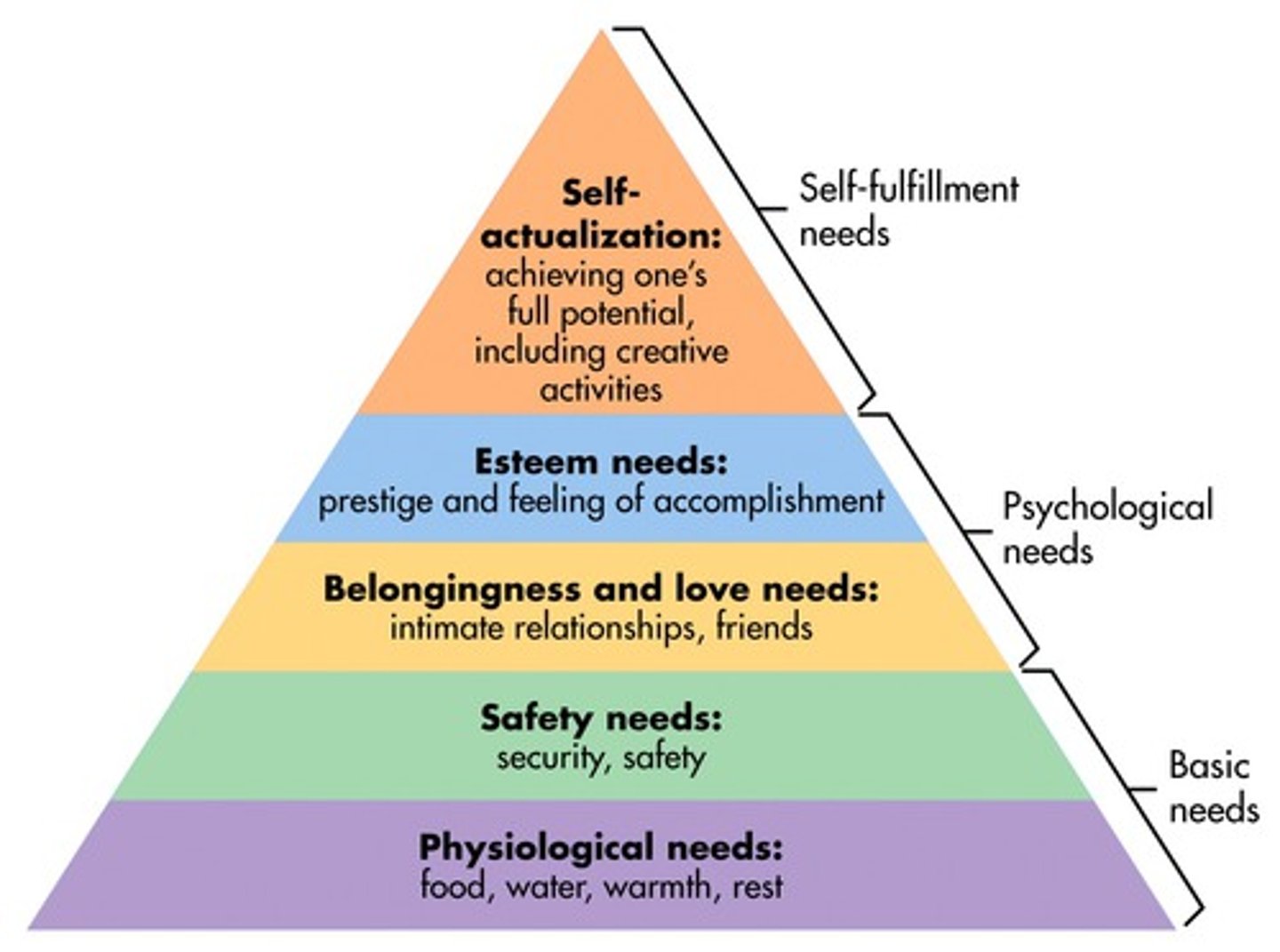
Humanistic Psychology
Abraham Maslow
Maslows heiarchy of needs
Gestalt/Experiential Therapy
Fritz Perls Process of forming wholeness
Focuses on the here and now versus the past with psychoanalytic theory.

behavior therapy
B.F Skinner
Albert Bandura
Arnold A. Lazarus
ABC model
Operant Conditioning
Token economy
DBT
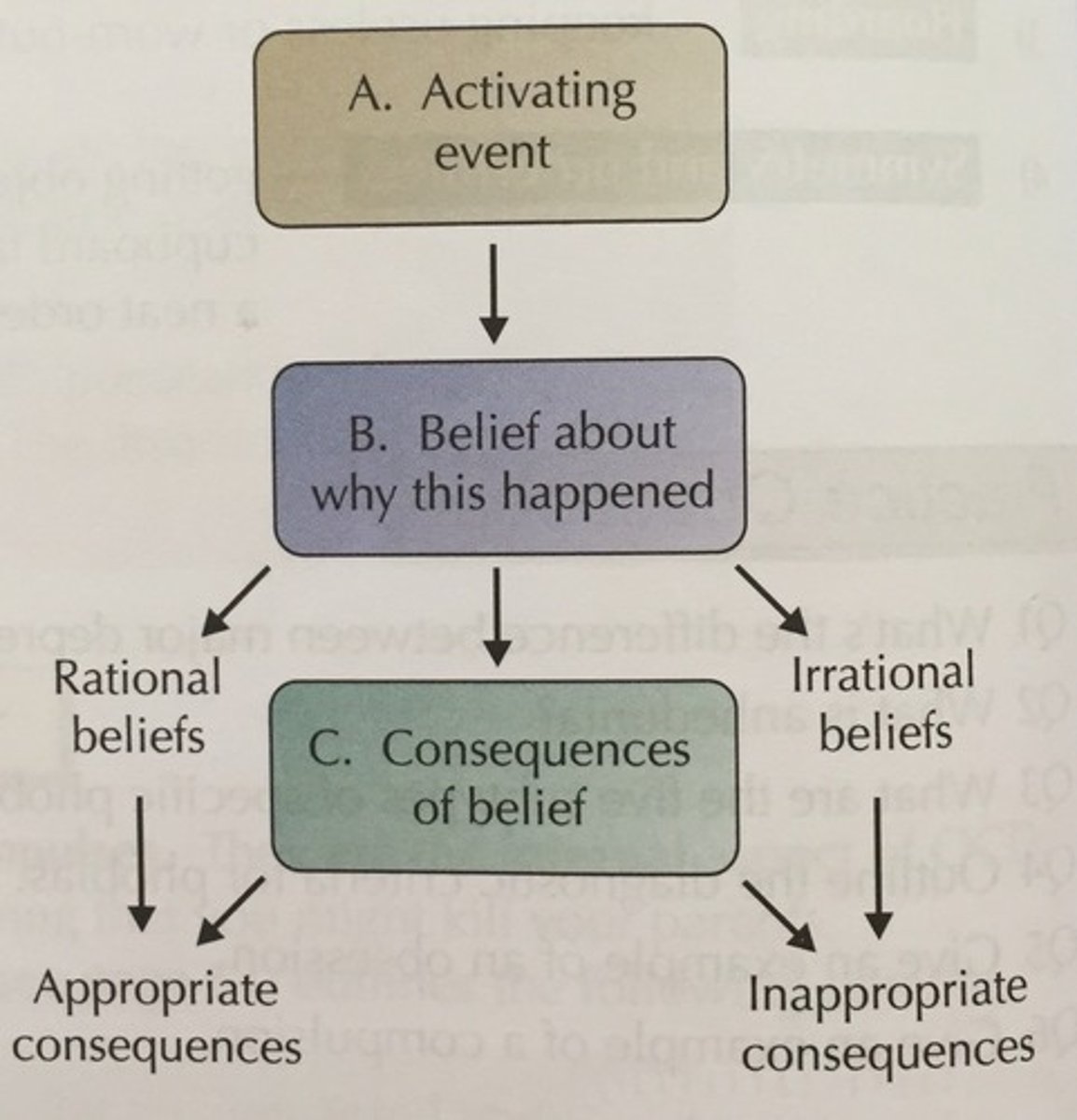
Cognitive Therapy
therapy that teaches people new, more adaptive ways of thinking and acting; based on the assumption that thoughts intervene between events and our emotional reactions
Cognitive restructuring
Albert Ellis
Aaron Beck
Interpersonal Therapy
treatment that strengthens social skills and targets interpersonal problems, conflicts, and life transitions.
Gerald Klerman
Myrna Weissman
Exposure and eye movement desensitization and reprocessing (EMDR)
Directly confronting fearful stimuli and the distressing anxiety or other emotions.
Edna Foa
Francine Shapiro
Systems Theory
Virginia Satir
Salvador Minuchin
Bowen Family Systems Therapy
Murray Bowen
Solution-focused brief therapy
Individuals can only be understood within their social context.
- People are healthy, competent, and capable of solutions.
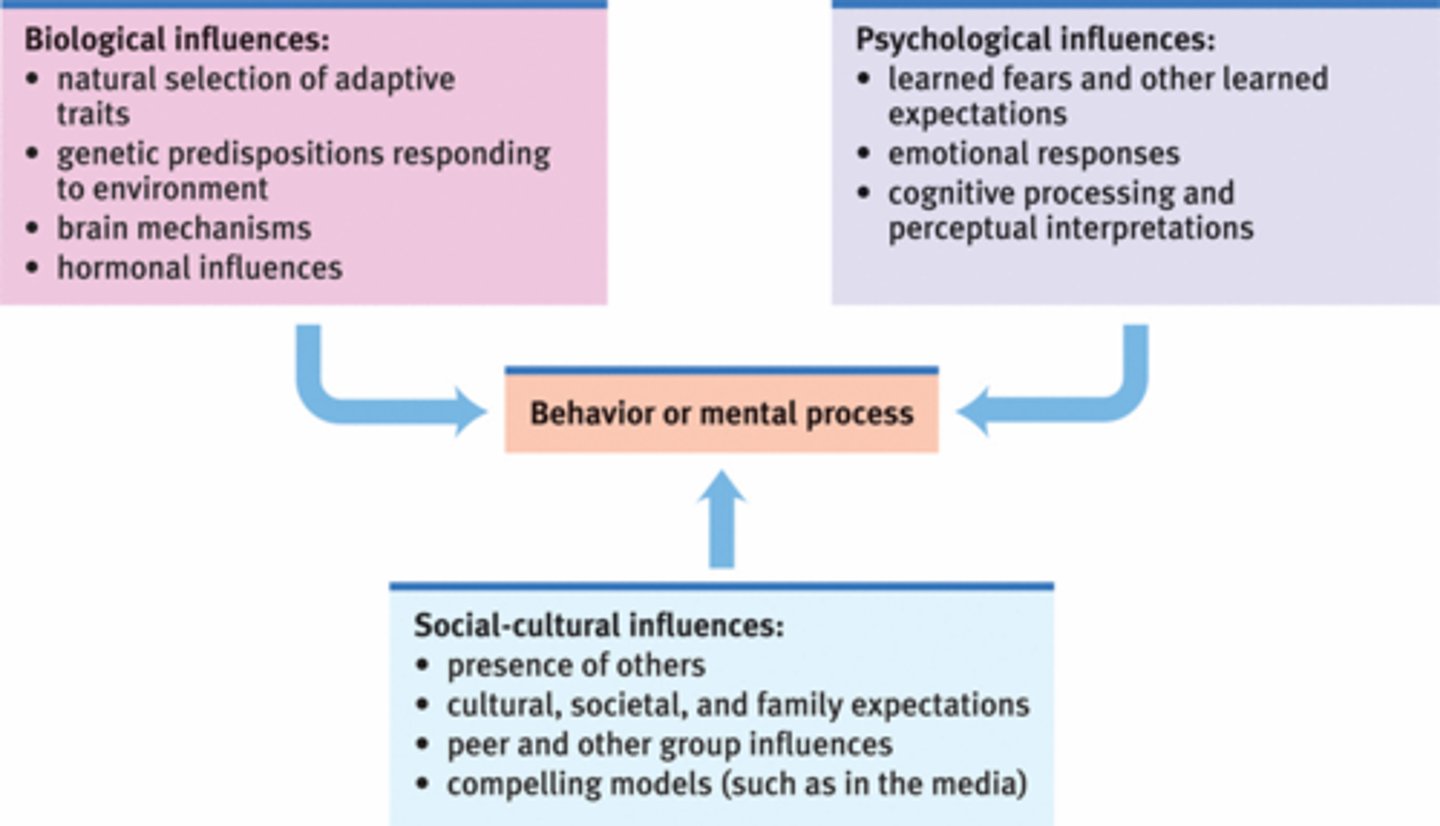
Biopsychosocial theory of mental ilness
a theory or perspective that relies on the interaction of biological, individual psychological, and social variables
Biologic: abnormalities of brain structure, function,, and alterations of brain chemistry.
Psychologic: past conflicts that affect thoughts and emotions.
Social: dysfunction among social and interpersonal relationships.
Erickson's stages of development
In
Early
Pre
School
Ad
Young
Middle
Late
Infancy (birth to 18 months) Trust vs. Mistrust
- Hope, Caregivers reliable?
Early Childhood (2 to 3 years) Autonomy vs. Shame and Doubt
- Will. Child needs to explore the world
Preschool (3 to 5 years) Initiative vs. Guilt
- Purpose. Can child do things on their own?
School Age (6 to 11 years) Industry vs. Inferiority
- Competence. comparing self-worth.
Adolescence (12 to 18 years) Identity vs. Role Confusion
- Fidelity. who am i?
Young Adulthood (19 to 40 years) Intimacy vs. Isolation
- Love. Dating, marriage, family
Middle Adulthood (40 to 65 years) Generativity vs. Stagnation
- Care. Accepts self, establish and guide next generation.
Late Adulthood (65 to death) Ego Integrity vs. Despair
- Wisdom. Last chapter in life.
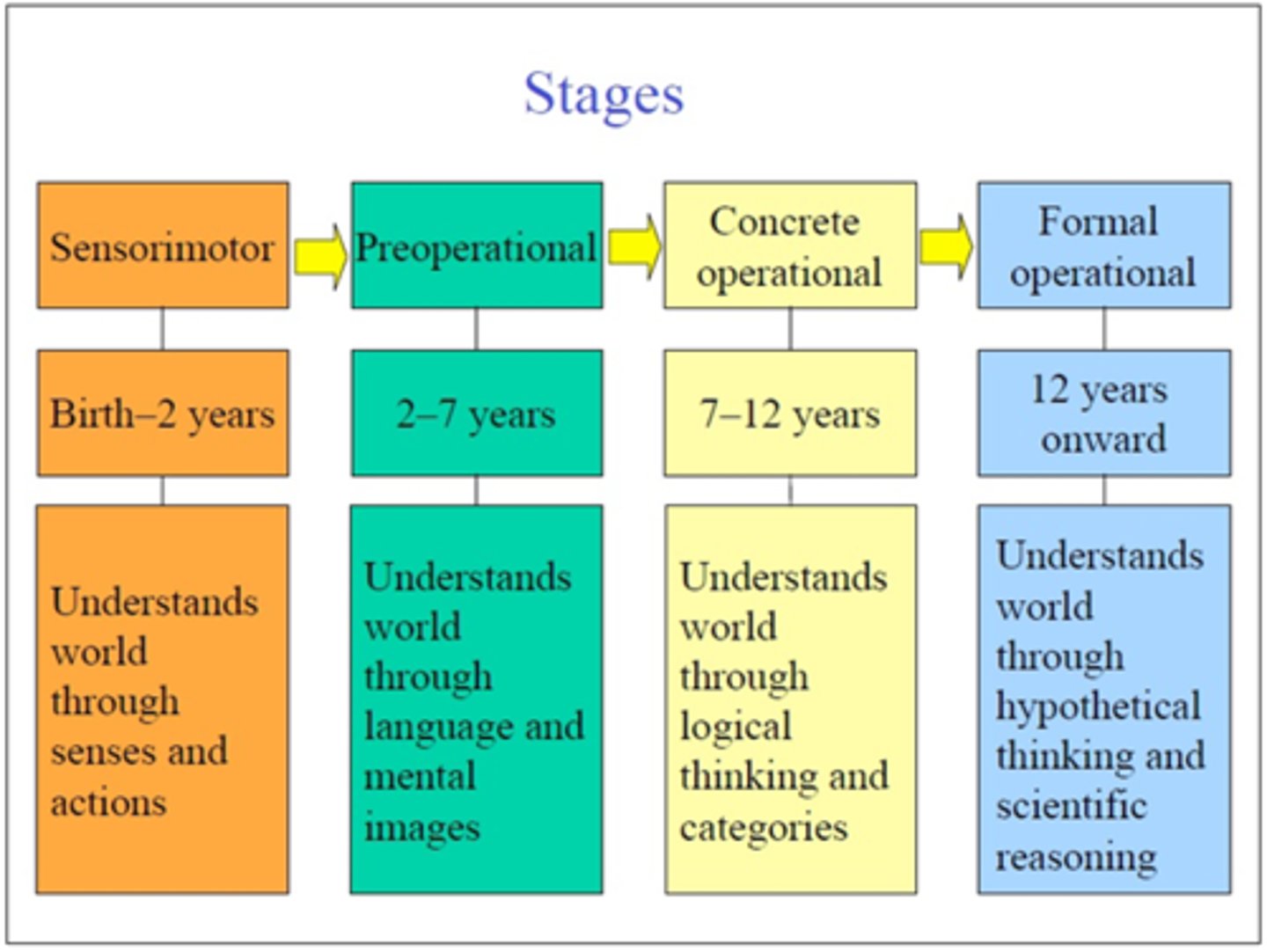
Piaget cognitive development theory
Kohlberg stages of moral reasoning
Children construct knowledge as they manipulate and explore their world. Information processing.
Kohlberg stages of moral reasoning
Birth-2 Preconventional infancy
2-7 Preschool period preconventional
7-11 Conventional morality
11-+ Principled morality
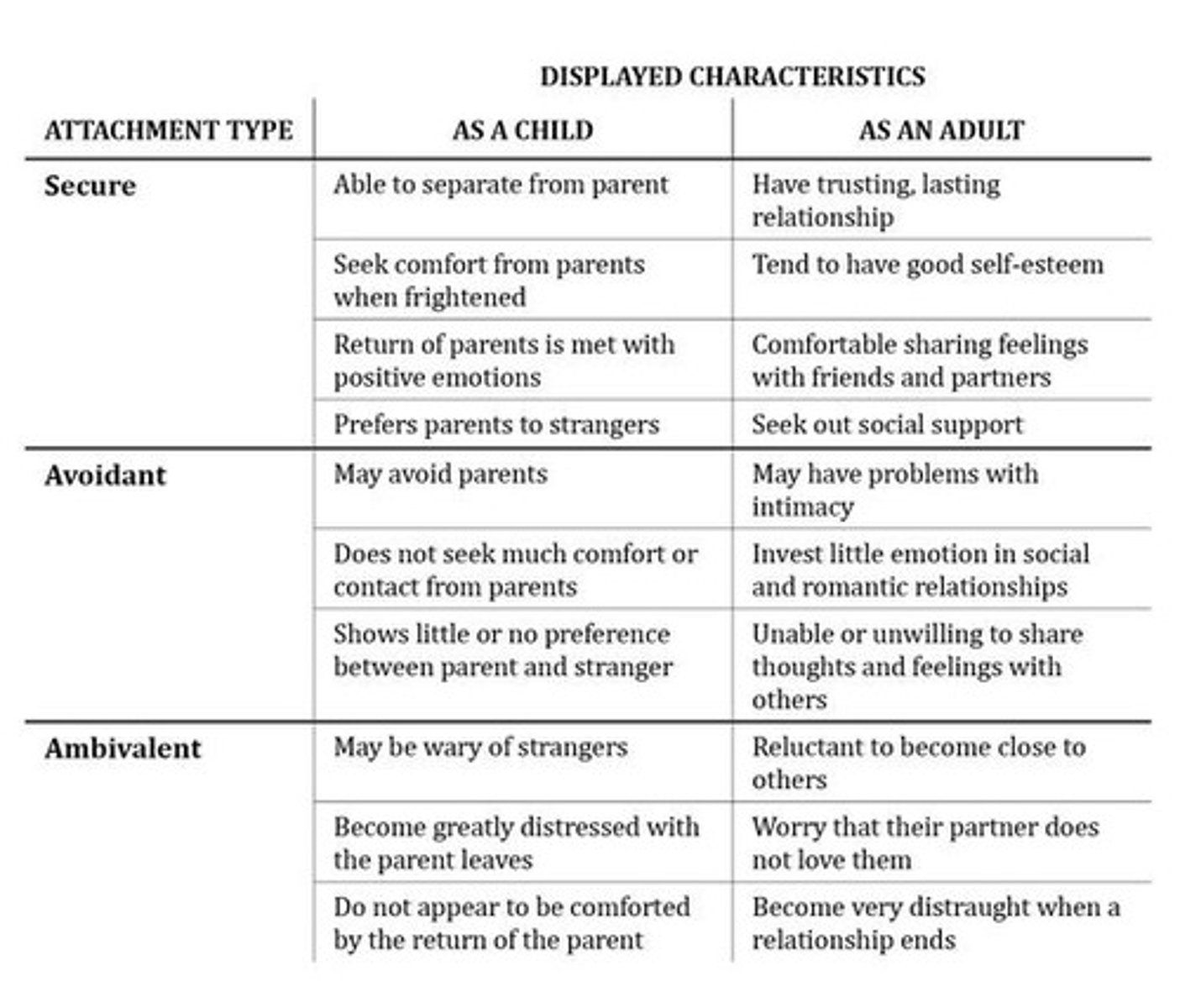
Attachment theory
Mary Ainsworth
Insecure-avoidant:
Insecure-ambivalent:
Insecure-disorganized:
John Bowlby
Mary Ainsworth
- Parents aggressive, child avoids
- Clings to inconsistent parents, has trouble exploring
- emotionally absent parents, the child behaves in bizarre way when threatened.
the idea that early attachments with parents and other caregivers can shape relationships for a person's whole life
Freud's Psychosexual Stages
1. Oral Stage
2. Anal Stage
3. Phallic Stage
4. Latency Stage
5. Genital Stage
Chapter 4 NeuroScience
Neural plasticity or neuroplasticity
Synaptic Pruning:
The brain's ability to reorganize itself by forming new neural connections throughout life.
In Adolescence synapses that are relevant persist, refining the efficiency of the brain.
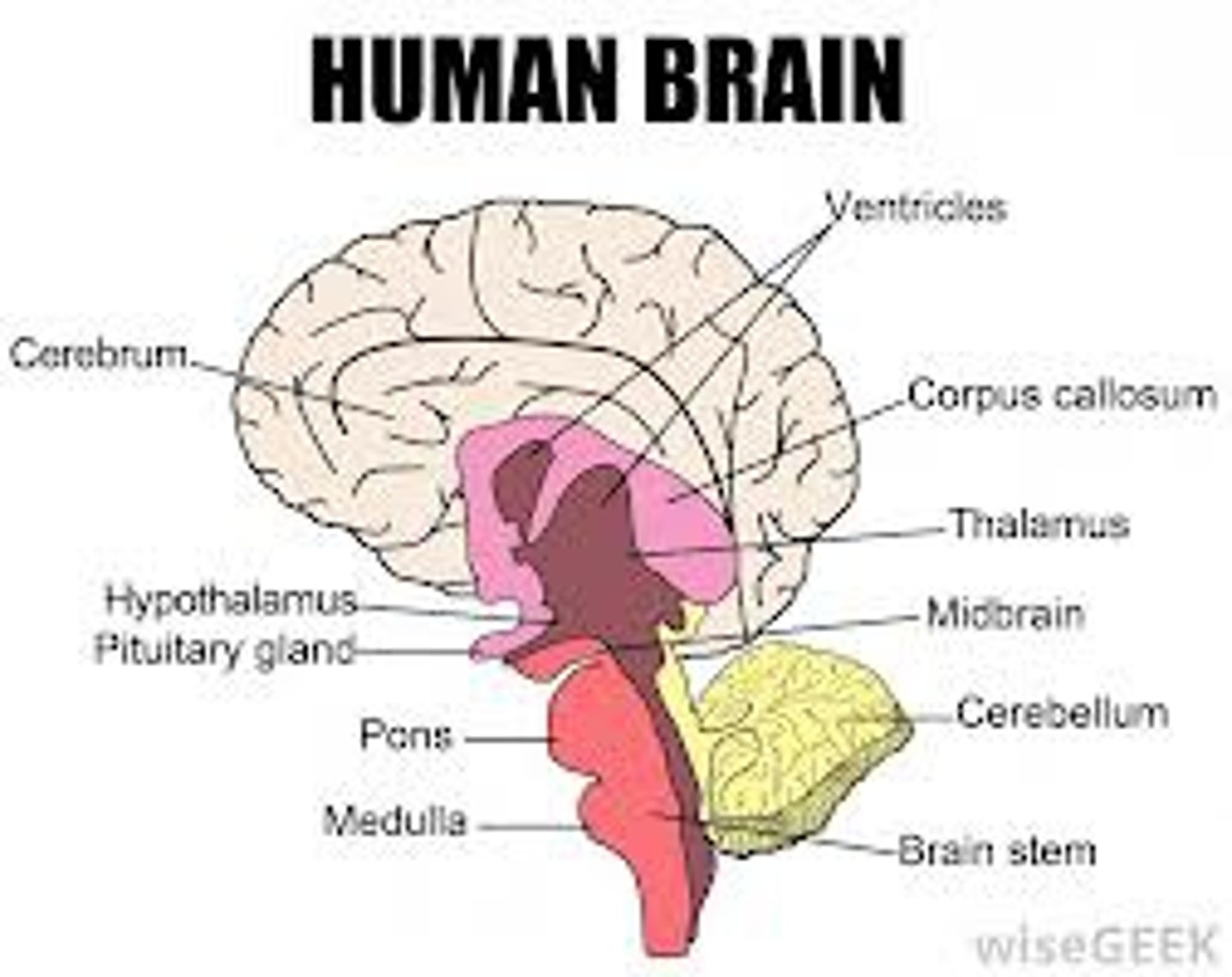
brainstem function
Cerebellum function
consists of medulla, pons, and midbrain
origin of most cranial nerves, contains reticular formation (important for arousal, sleep-wake cycles), location of respiratory, cardiovascular, and digestive control centers
process and store information, coordinates voluntary movements (posture, balance, speech)
Amygdala
Regulates basic powerful emotions,: Fear, rage, sexual desire.
two lima bean-sized neural clusters in the limbic system; linked to emotion.
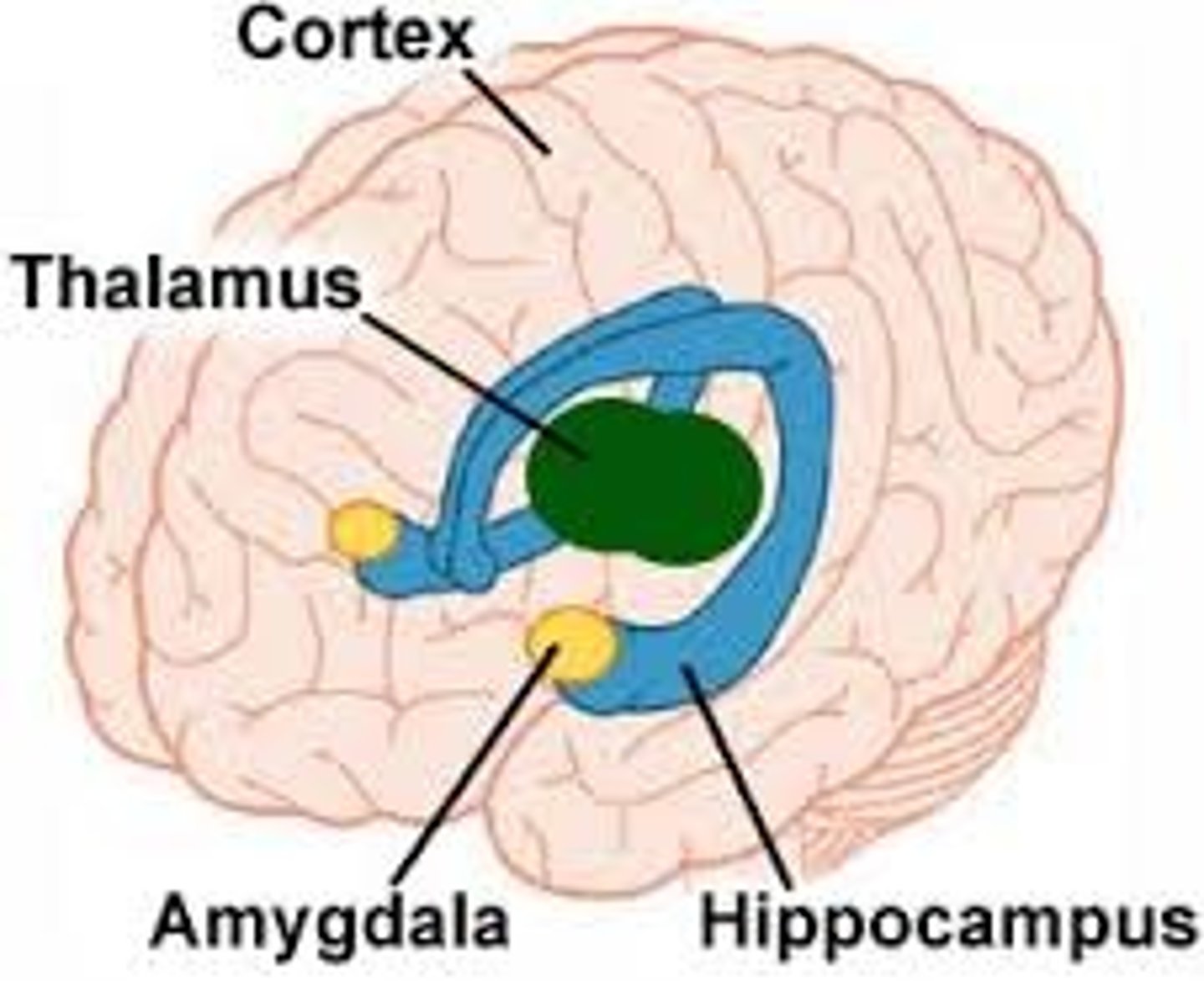
Hippocampus
short-term memory into long-term memory, learning
Seeing a hippo on campus whould be in short tierm and then go to long term memory.
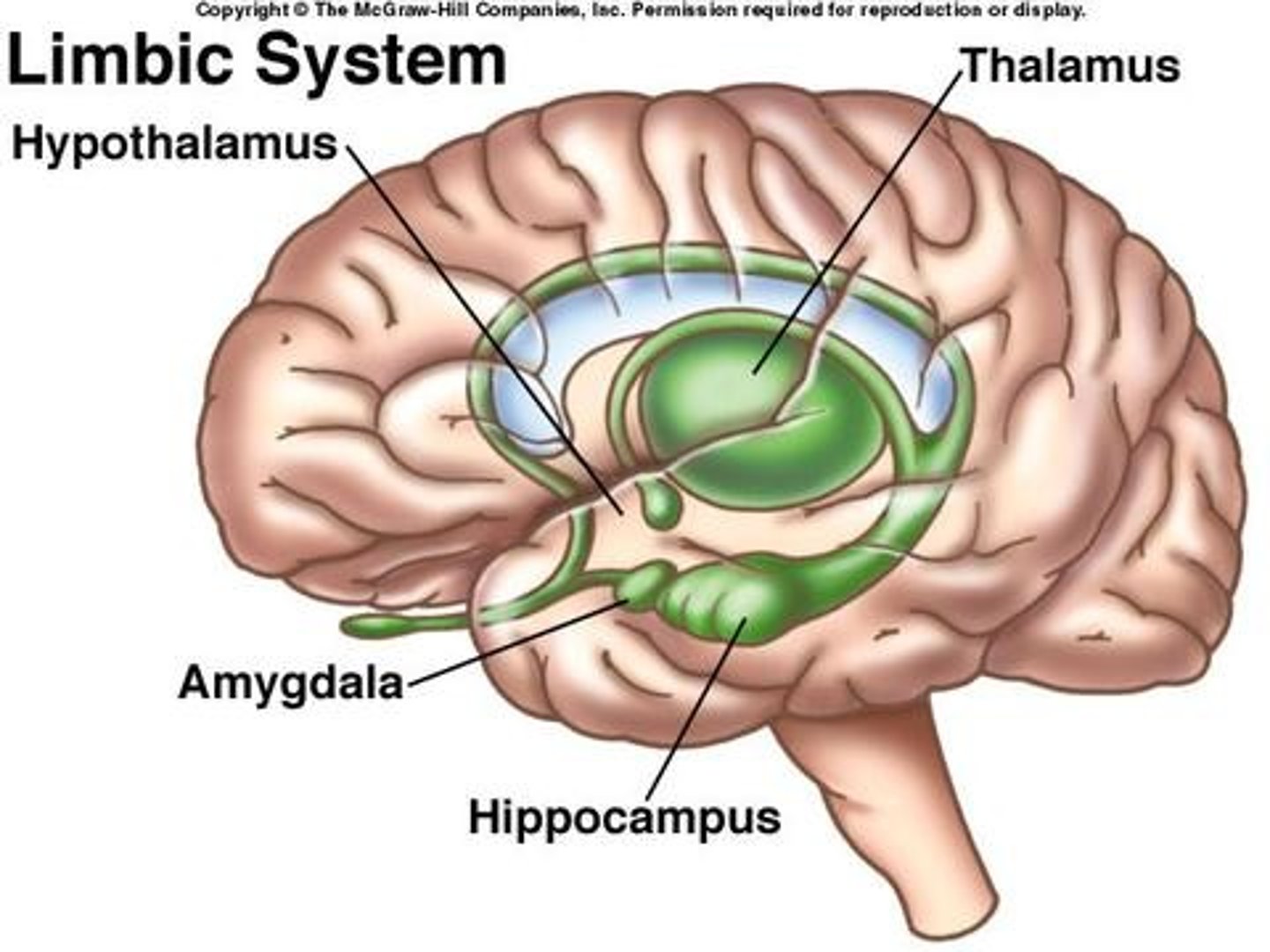
Thalamus
the brain's sensory switchboard, located on top of the brainstem; it directs messages to the sensory receiving areas in the cortex and transmits replies to the cerebellum and medulla
Hypothalamus
a neural structure lying below the thalamus; directs eating, drinking, body temperature; helps govern the endocrine system via the pituitary gland, and is linked to emotion
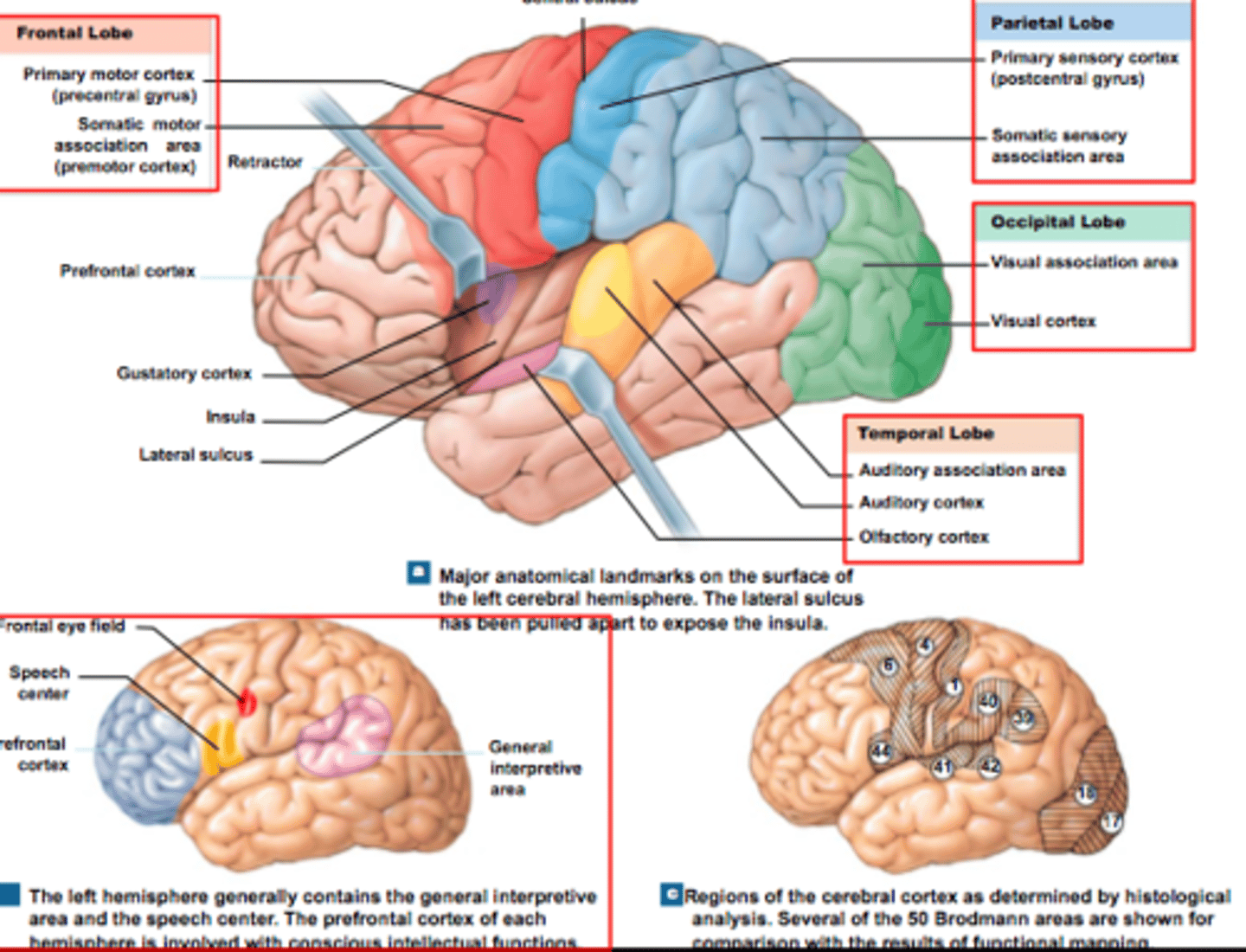
Cerebral Cortex functions
Frontal Lobe:
Parietal Lobe:
Occipital Lobe:
Temporal Lobe:
Executive Functioning has Motor strip, Supplemental motor area, Broca's area, Prefrontal cortex
- Recieves and evaluates sensory information.
- Vision and visual memory, language formation
- Recieves and processes auditory information.
Dopamine:
Norepinephrine:
Serotonin:
Histamine:
Glutamate
GABA:
Acetylcholine:
DOPAMINE
Pathways: Nigro, Tub, Mesolimbic, mesocortical
Chapter 5 Psychiatric Assessment
CHAMPION FISH CALLER
C hief Complaint
H ow Can We Help?
A llergies
M edications
P ast History
I deation
O rientation
N arcotics and
Substances
F amily
I ncome
S ocial Support
H ousing
C ollateral
A buse
L egal
L eaving
E xamination
R eview of Systems
Clues to a medical disorder
-Later age onset
-Known underlying medical condition
-Atypical presentation of psychiatric condition
-Absence of personal or family history of a psychiatric condition
-Poor response to usual treatment
-Substance use or medication use
-Waxing and waning mental status
-Abnormal vital signs
ABS! MATT Please, Can I Judge?
A ppearance,
B ehavior,
S peech,
M ood,
A ffect,
T hought content,
T hought process,
P erception,
C ognition,
I nsight,
J udgment.
Apperance and Behavior
Speech
Mood
Affect
Level of consciousness
Posture and motor behavior
Dress, grooming, personal hygiene
Facial expressions
Manner, affect,
relationship to persons and things
-Not language abilities! Dysphasia, volume, amount, speed, tone
- Pts own words to describe mood. Subjective
- The expression of mood as it appears to the clinician.
Thought Content
Thought Process
-Thoughts that occur the the patient. Example Ruminative, obsestional, delusions.
-
Thought process
Normal?
Flight of ideas?
Circumstatial?
Tangential?
Loose thoughts or associations?
Perseveration?
Thought-blocking?
Neologisms?
Word Salad?
How thoughts are formulated, organized, and expressed
- Normal thought process is linear, organized, and goal-directed.
- Rapidly moving from one thought to another but logically connected
-Includes non-relevant details, but eventually returns to address the subject or question
- Begins OK but the patient never returns to the original question
- Difficult to see connections between content
- Unable to move to other topics despite attempts to change the subject
- Unable to complete a thought, stopping mid-sentence
- New Word or combination of several words
- Confused language with no apparent meaning
Perceptual Disturbances
Hallucinations
Illusions
Depersonalization
Derealization
Cognition
Alertness, orientation
Concentration (seriel sevens)
Memory (Short and long-term)
Calculations (What is 2x24?)
Fund of Knowledge (Past 5 presidents?)
Abstract reasoning (people in a glass house should not throw stones)
Insight
Judgment
Pts understanding of how they are feeling, presenting and functioning, as well as potential causes to their distress.
Pt capacity to make good decisions and act on them. Can they participate in their own care.
FMLA
Reasons for leave?
The Family and Medical Leave Act of 1933 to allow employees to take time off from work for family or medical reasons. The FMLA requires employers that have 50 or more employees to provide employees with up to 12 weeks of unpaid family or medical leave during any 12 month period.
FMLA: Reasons for Leave
1. Birth of a child and caring for an infant. Fathers and mothers, if both parents work together the combined total leave may not exceed the 12-week total. Leave must be within 12 months of the child's birth.
2. Placement of an adopted/foster child. Same as (1)
3. To provide care for spouse, son, daughter or parent with a serious health condition. Spouse defined by the state one lives. Parent can be biological or in loco parentis (care giver). Child must be under 18 and unable to care for themselves because of physical or mental disability. EE'rs may require documentation to support relationship.
4. EE unable to perform functions of a job because of "Serious Health Condition"
5. Provide care for a covered service member, family members can take 26 weeks of leave in a 12-month period.
6. To Provide leave for "qualifying exigencies" for families of national guard or reserves.
Chapter 6 Culture, Racism, and Discrimination
Mental disorders are defined and recognized in the conxtex of?
cultural context, societal norms, and values.
Cultural Syndrome
a cluster of symptoms specific to the culture in which they occur and are not seen as an ilness, but outsiders mya recognize it as such
cultural idioms of distress
terms or phrases used to describe suffering or distress within a given cultural context
Cultural Explanation or perceived cause
a label, attribution, or feature of an explanatory model that provides a culturally conceived etiology or cause for symptoms, illness, or distress
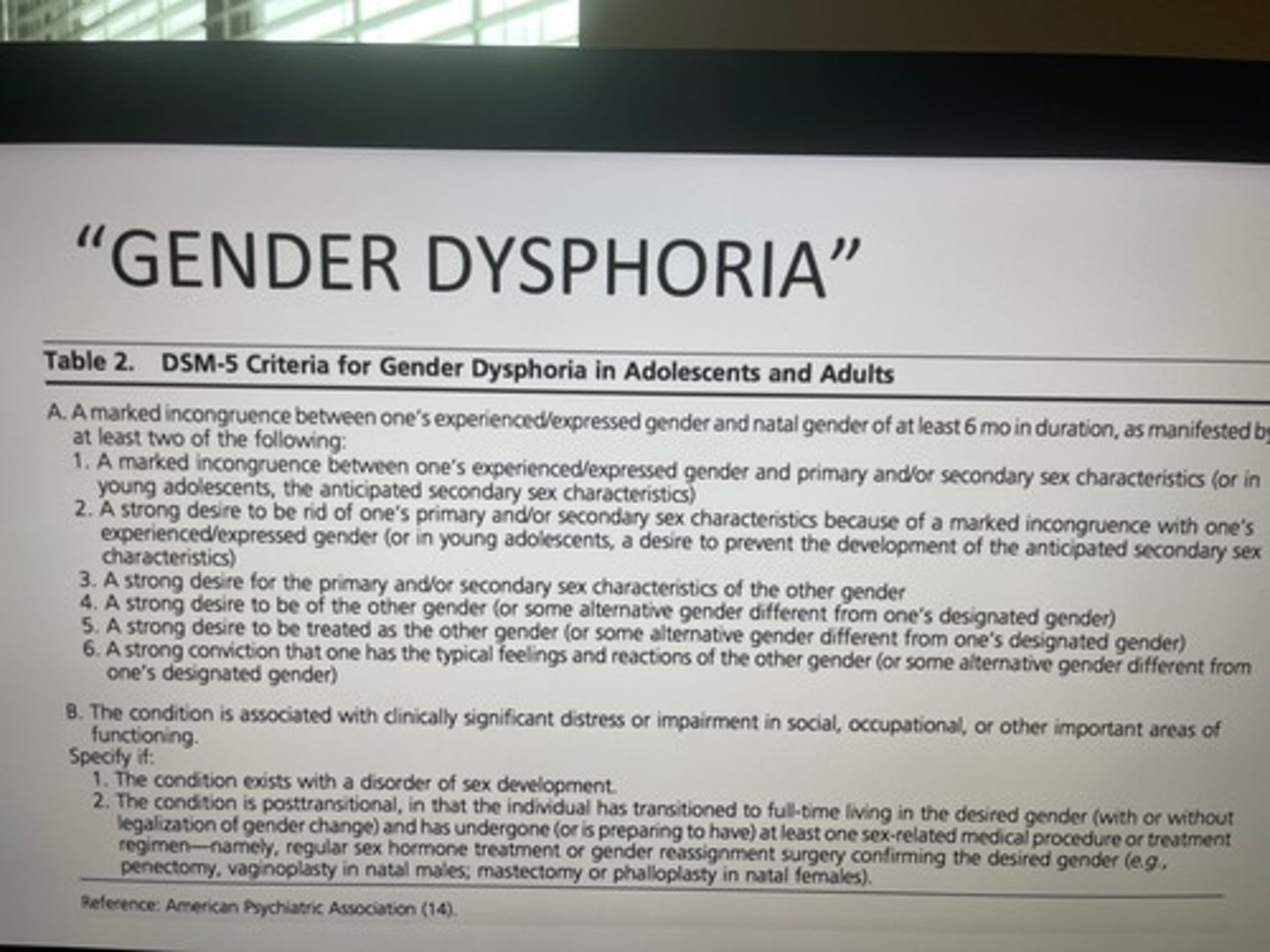
DSM-5 criteria Gender Dysphoria
incongruence of expressed gender and gender assigned at birth. present for at least 6 months
Chapter 7 Communication and Psychotherapy
interpersonal psychotherapy (IPT)
Weissman and Klerman
a form of psychotherapy that focuses on helping clients improve current relationships
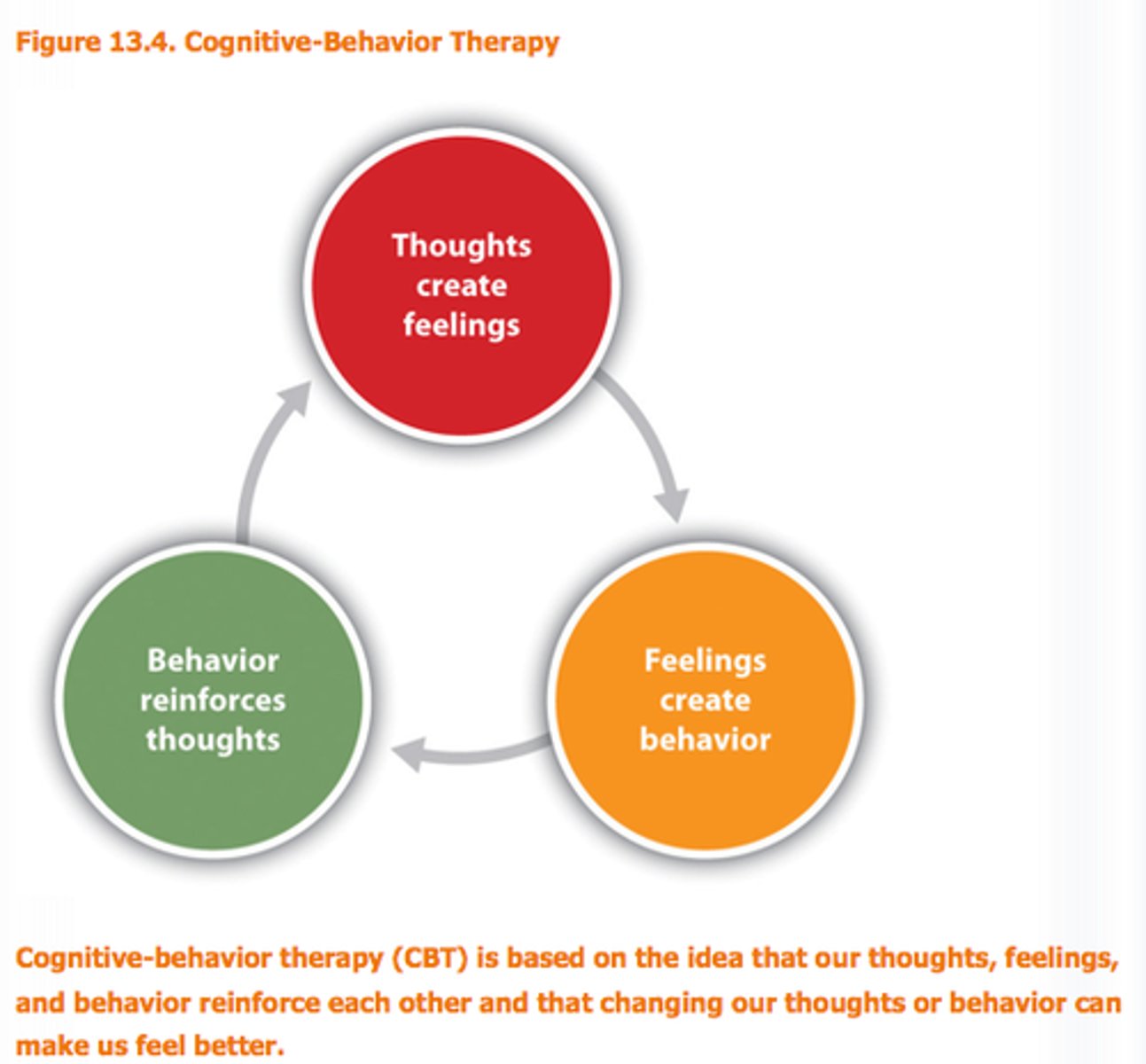
Cognitive Behavioral Therapy (Beck)
a popular integrative therapy that combines cognitive therapy (changing self-defeating thinking) with behavior therapy (changing behavior)
Psychoeducation on cognitive distortions
- Downward arrow " If that were true, what would happen then?"
- Automatic thought records
-Cognitive distortions
- Cognitive restructuring
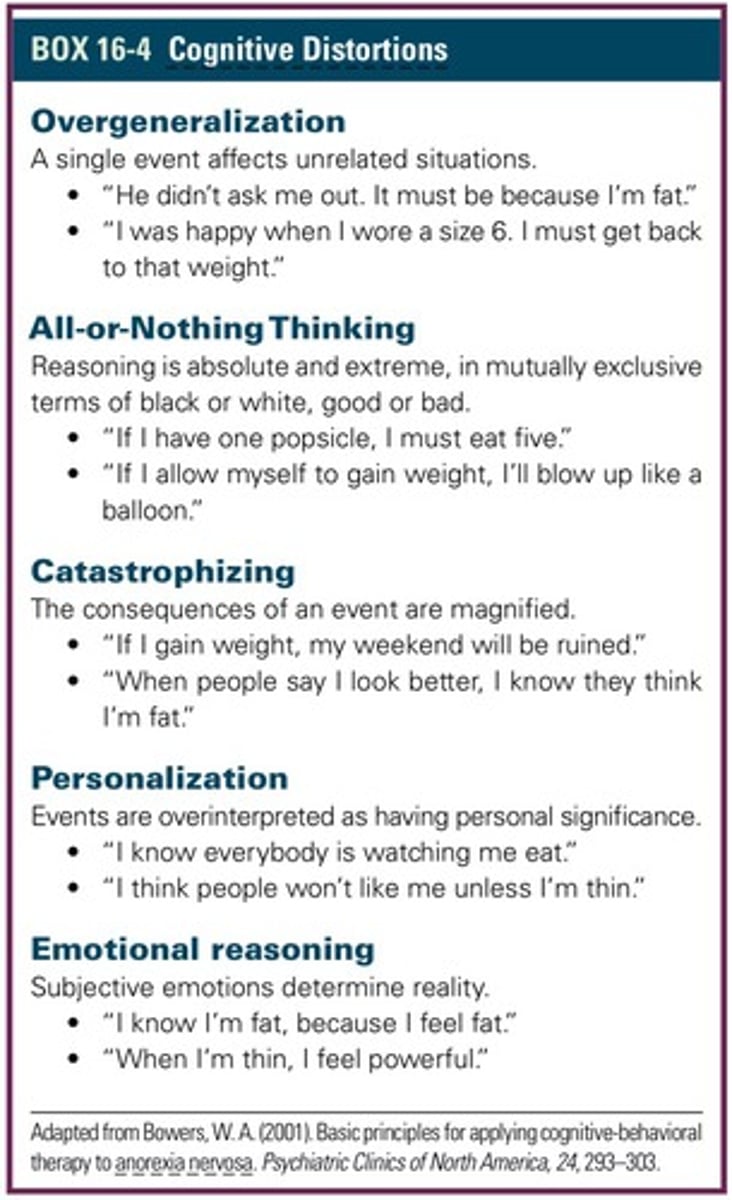
Cognitive Distortions
Inaccurate and irrational automatic thoughts or ideas that lead to false assumptions and misinterpretations.
psychodynamic psychotherapy (Alder)
Understand patterns and relationships of the past in order to change behavior.
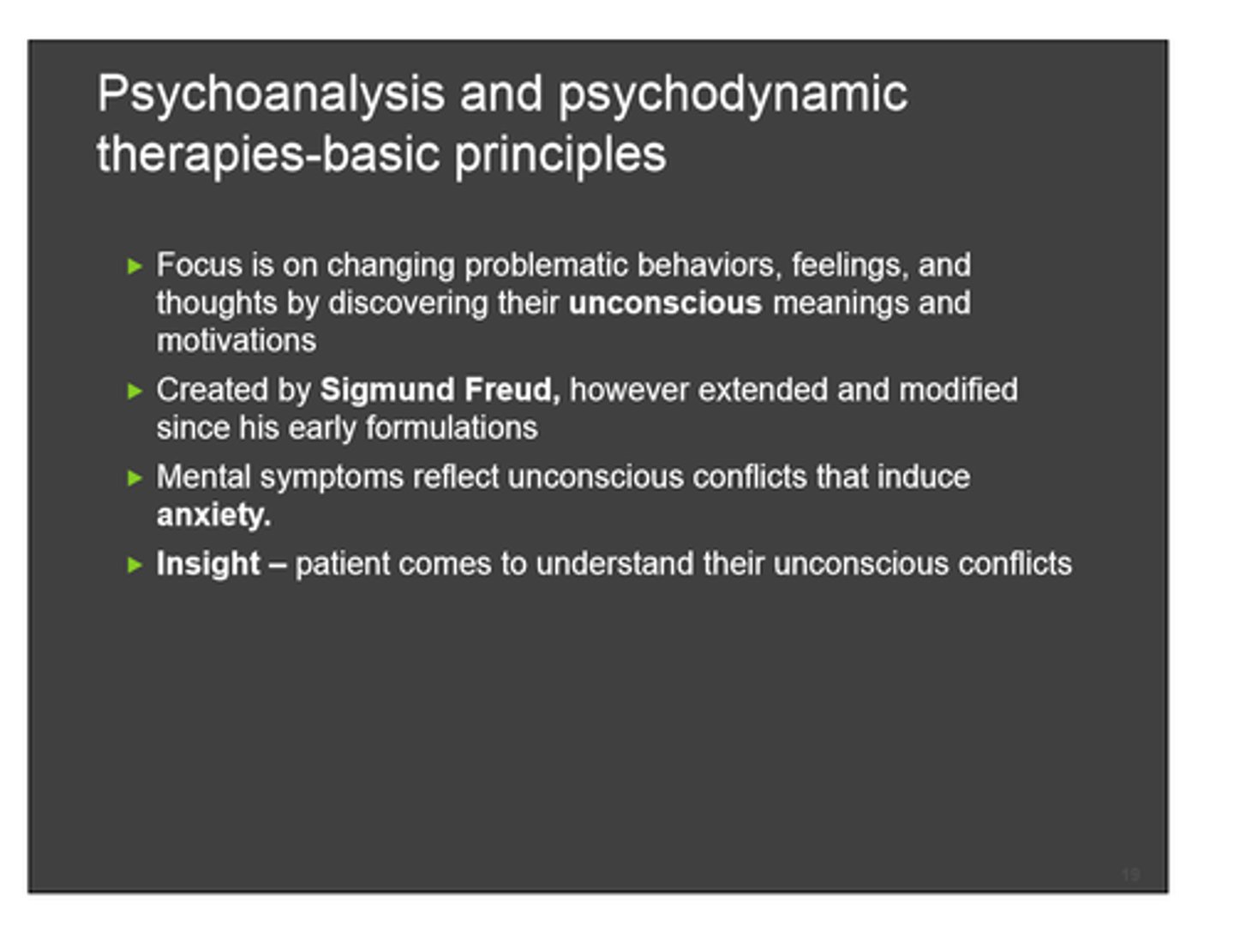
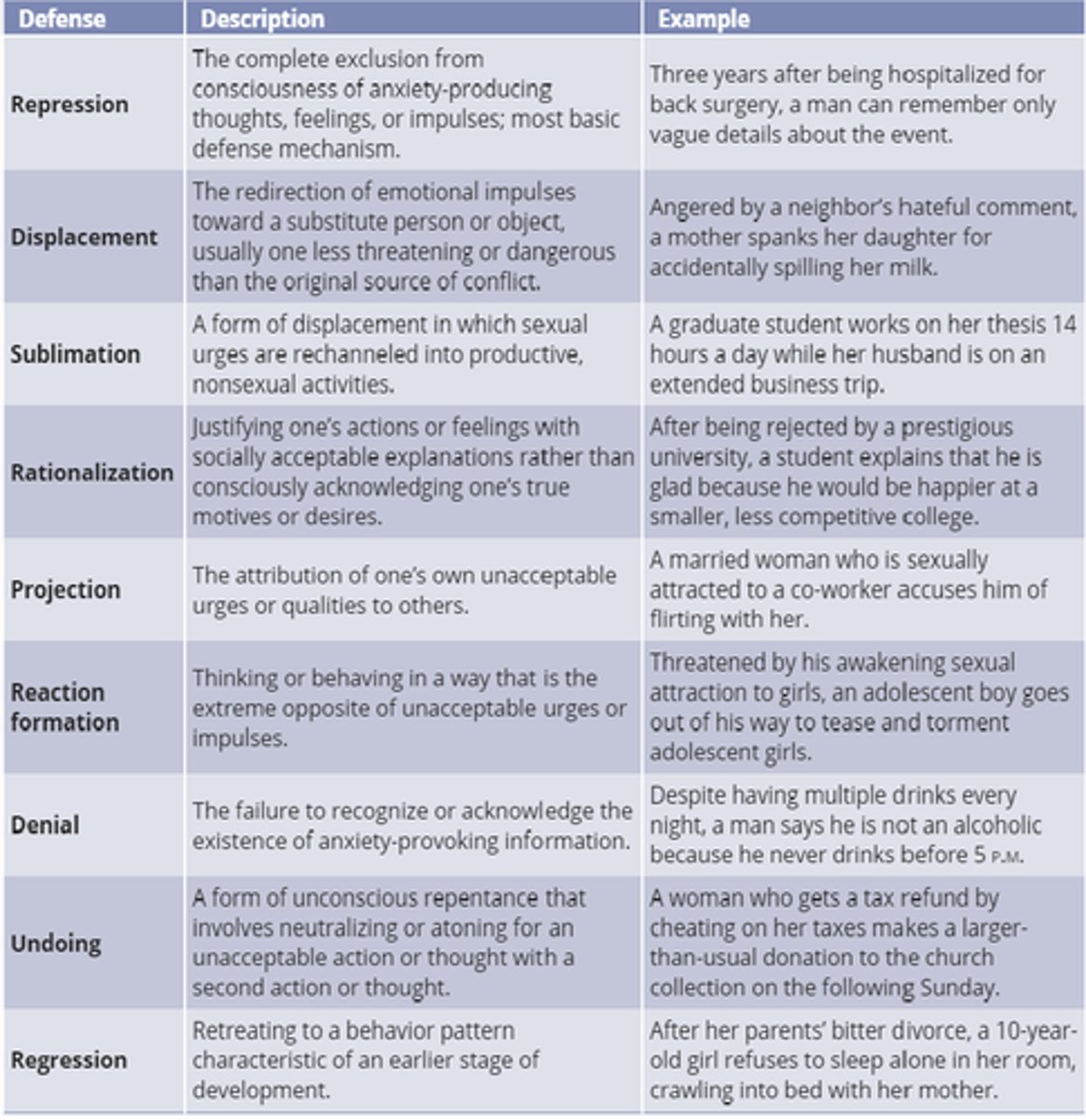
defense mechanisms
mental processes that protect individuals from strong or stressful emotions and situations
DBT (Linehan)
dialectical behavior therapy for personality disorders
Therapists follow a detailed procedural manual.

Solution Focused Therapy (de Shazer and Berg)
Miracle questions
• Change occurs through accessing client's
strengths and resources.
• This is a brief, goal-directed therapy focused on
client's strengths and resources
• Focuses on what the client wants to achieve
instead of focusing on the problems
• Focuses on the client's strengths and resources
in order to create a more effective future
humanistic therapy (Rogers, Maslow)
Focuses on removing obstacles that block personal growth and potential.
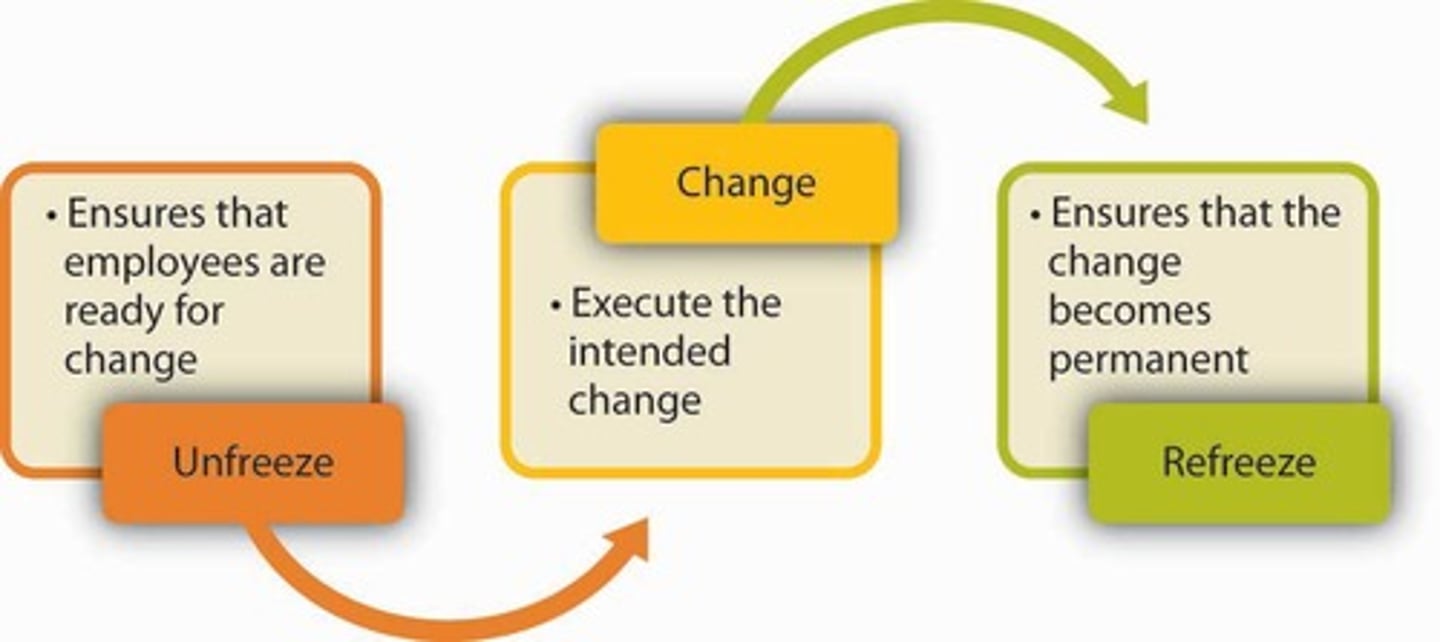
Lewins Change Theory
A three-step process: unfreezing; moving or change; refreezing
Motivational Interviewing (MI)
For use of SUD, CHronic medical ilnesses
- Provider doesn't have what the patient needs. The patient has what they need.
- OARS communication Skills
Open ended questions
Affirming statements
Reflecting statements
Summarizing
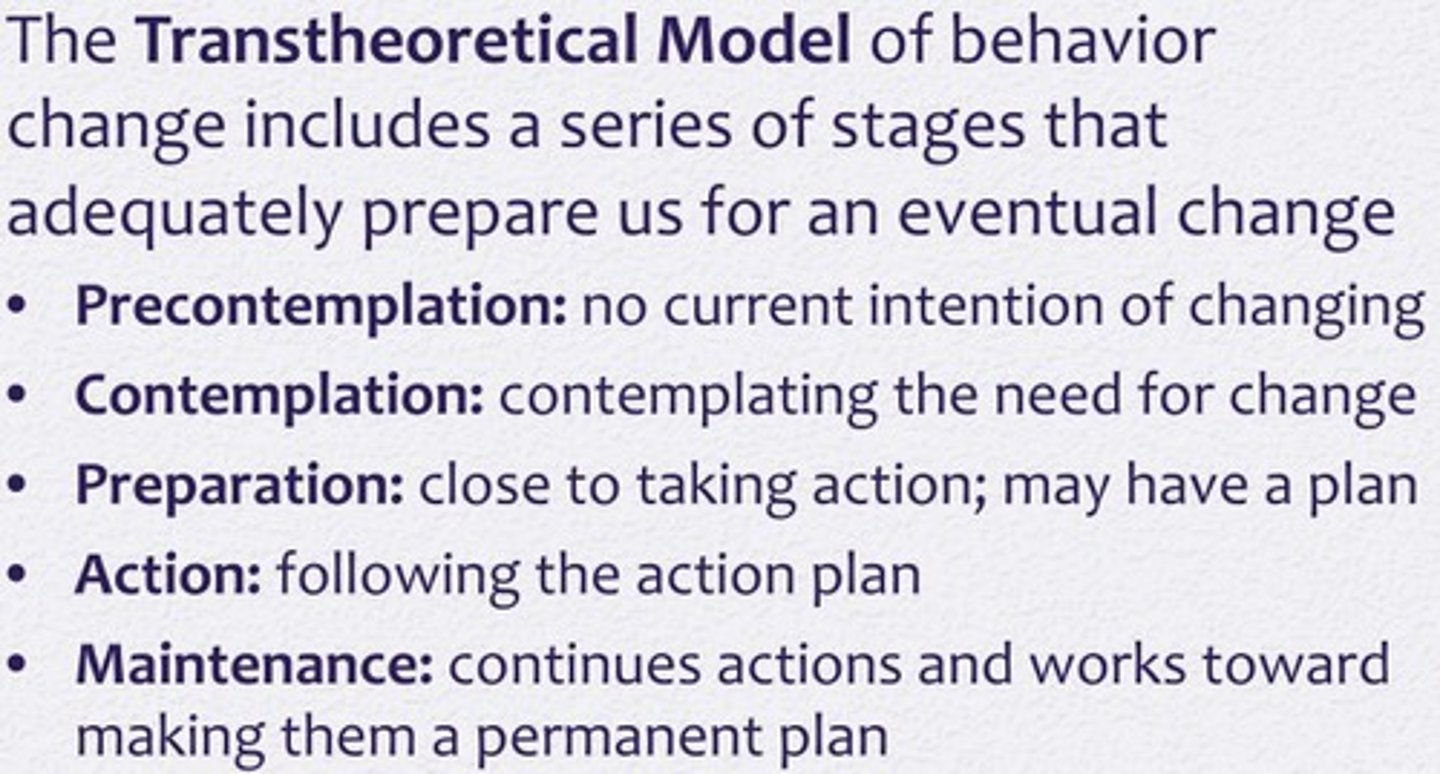
Transtheoretical Model of Change
Proshaska and DiClemente: Stages of change
1. Precontemplation
2. Contemplation
3. Preparation
4. Action
5. Maintenance
Yalom's Therapeutic Factors
- Universality
- Instillation of hope
- Imparting of information
- Altruism
- Corrective repeat of the family of origin
- Development of social skills
- Imitative behavior
- Interpersonal learning
- Group cohesiveness
- Catharsis
- Learning to accept painful aspects of life
Phases of group formation/development
Orientation: members adapt being in the group.
Storming: individuals find a place in the group and ideas exchanged
Norming: trust develops and work toward goals.
Perfroming: increased sharing, group ownership or experience in the group.
Adjourning: Termination, appreciation for group members expressed.
Chapter 8 Mood disorders
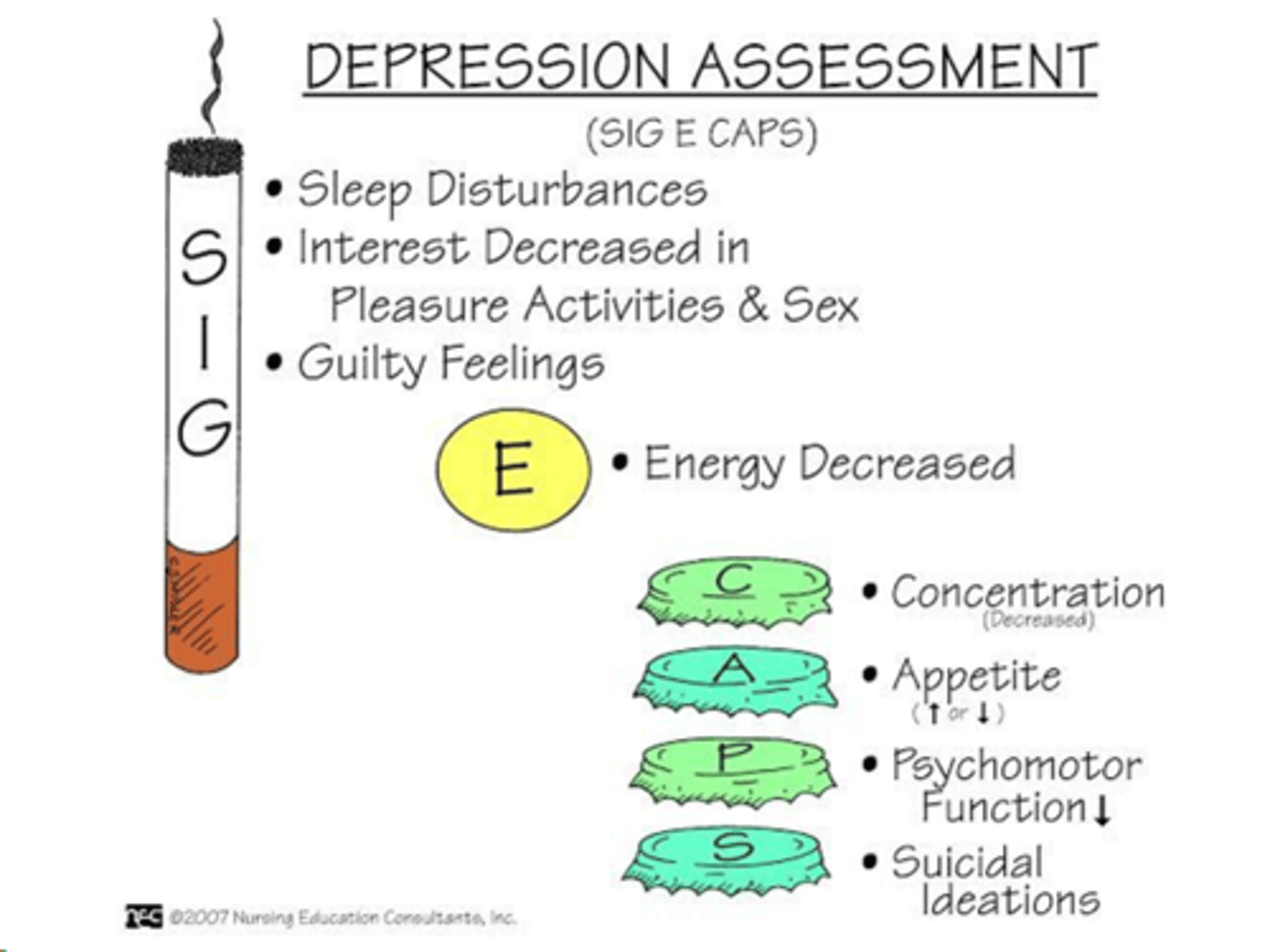
SIGECAPS
Interfere with social, occupational, or interpersonal functioning is present.
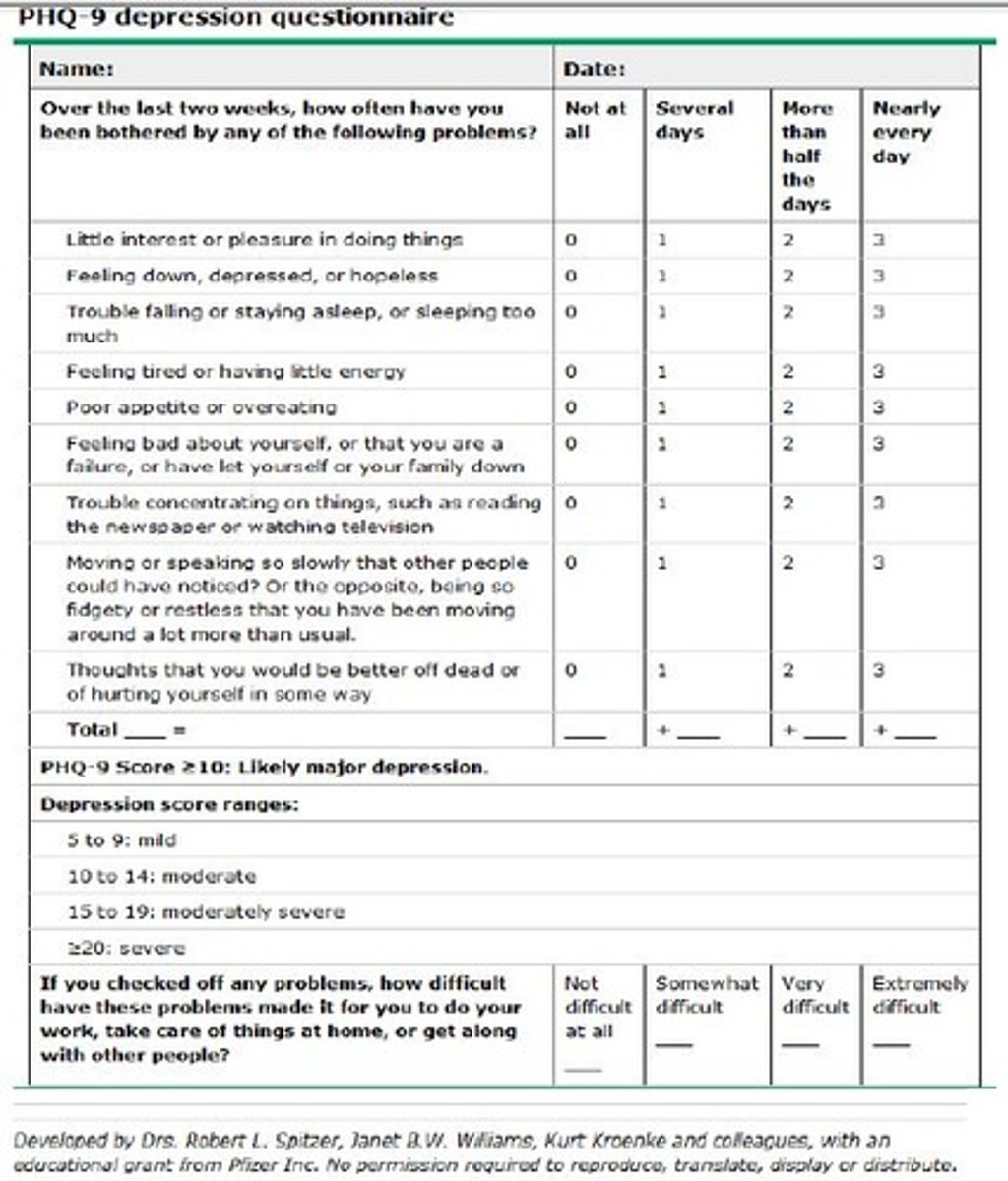
PHQ-9
Know the severity ratings
assessment that evaluates degree of depression
5-9 mild
10-14 moderate
15-19 mild depression
20 + severe
Hamilton Depression Rating Scale (HAM-D)
17-21 questions
Normal = 0-9
Mild = 10-13
Moderate = 14-17
Moderate-Severe = greater than 20
- MDD Single Episode
- MDD recurrent
- Persistent Depressive disorder (Dysthymia)
- Other Specified Depressive Disorder
- Singe episode
- 2 or more split by 2-month interval
- Depressed mood plus at least 2 MDD criteria present for 2 years not been symptom free for more than 2 months
- Depressive symptoms but do not meet the criteria for MDD
Unspecified Depressive Disorder
Adjustment Disorder with depressed mood
Premenstrual Dysphoric Disorder
Substance/Medication-induced Depressive Disorder
Depressive Disorder Caused by another medical condition
- Depressive symptoms are present but do not meed the full criteria.
- Psychological symptoms present within 3 months of the stressor and don't meet criteria for MDD.
- Affective lability and other depressive symptoms that are present repeatedly before menses and end at or around the start of menses. Remits within 1 month of substance cessation.
- Associated with use of substance and extend beyond the psyciological effects of the substance.
- Related to another medical condition.
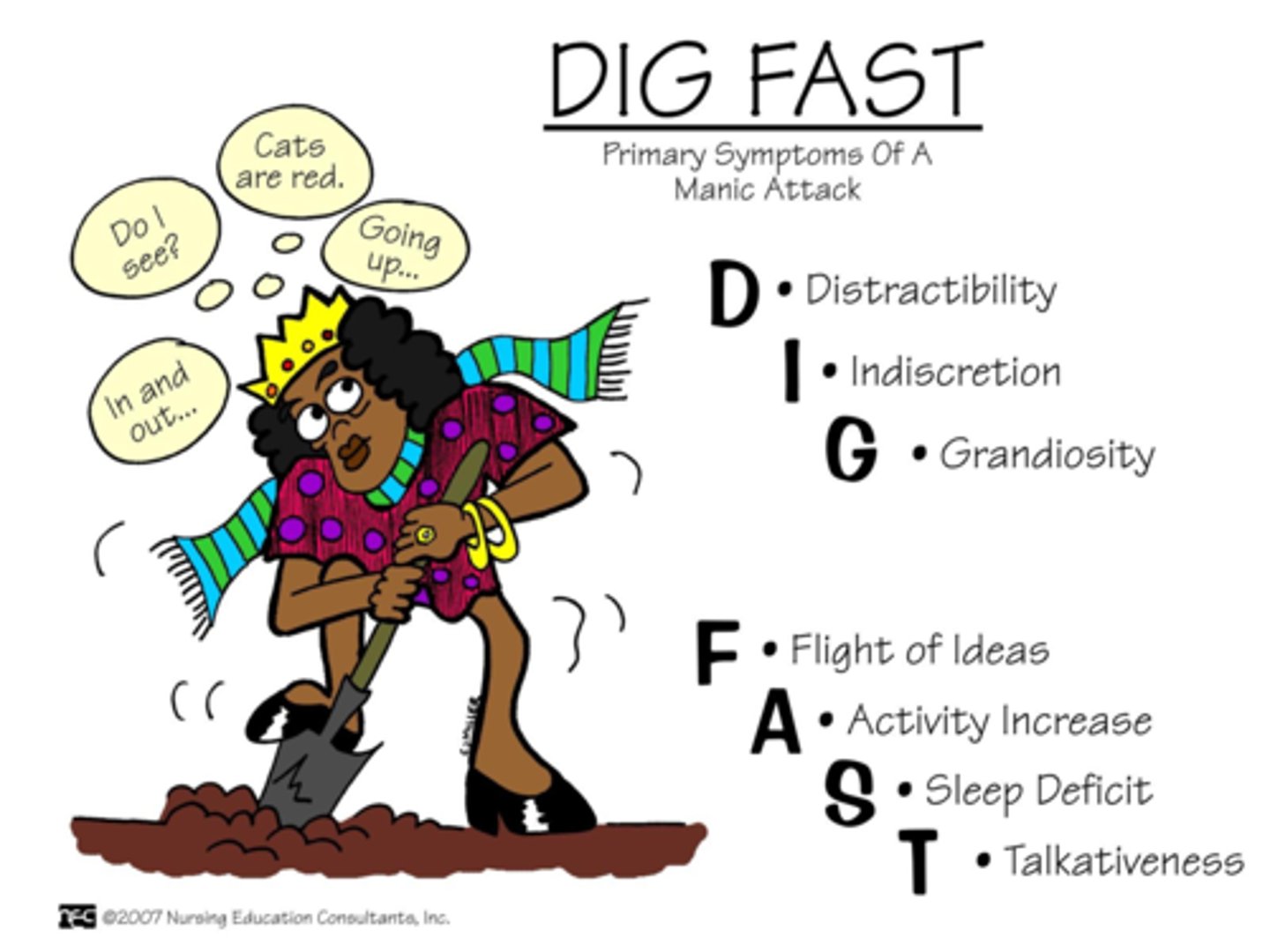
DIGFAST for mania
Difference for Hypomanic episode
- distractibility, impulsivity, grandiosity, flight of ideas, activity increase, sleep deficit, and talking increase
4 out of 7 for one fun week.
- persistently elevated for 4 days instead of 1 week.
Not severe enough to cause impairment in social or occupational functioning.
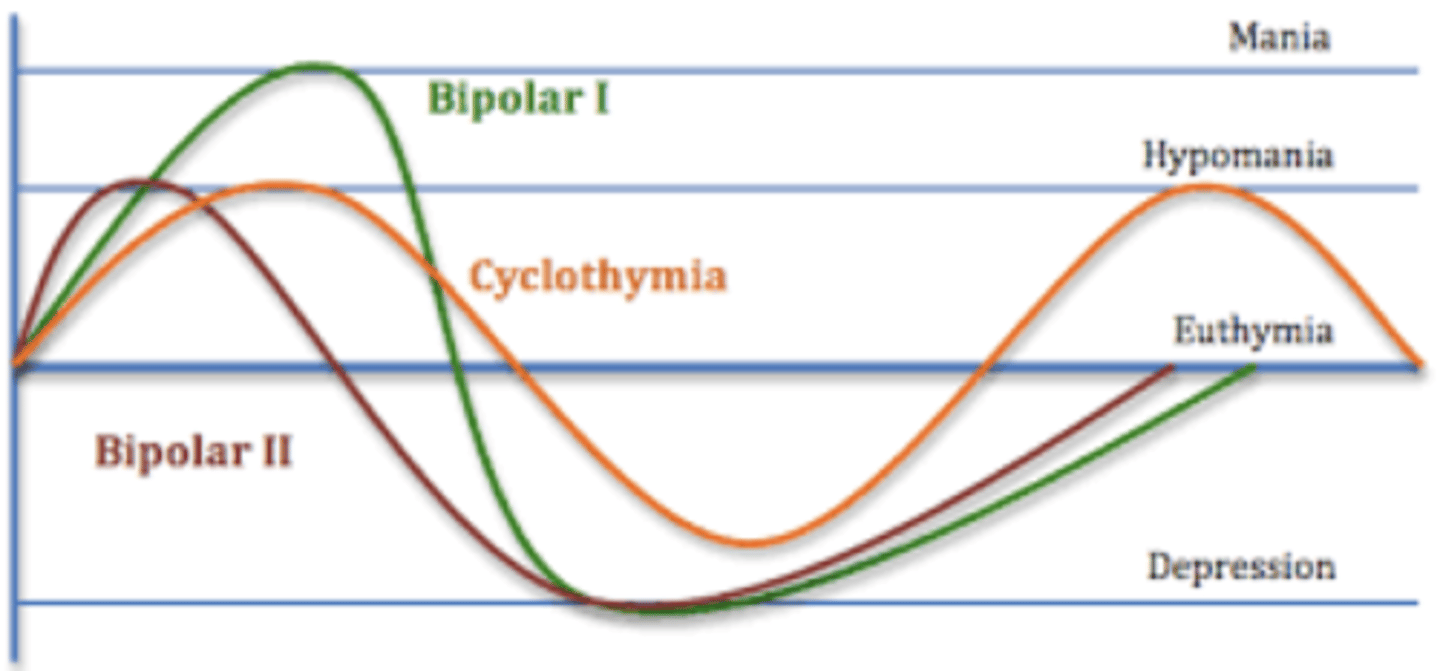
Bipolar 1
Bipolar 2
Cyclothymia
types of bipolar disorders
Cyclothymic is hypomania and dysthymia
Substance/Medication-induced bipolar disorder
Bipolar and related disorders caused by another medical condition
- Other specified Bipolar and related disorder.
- Disturbance of mood is a direct result of physiological effects of a substance
- Caused by another medical condition
- Mood disorders that do not meet criteria for specific bipolar disorder
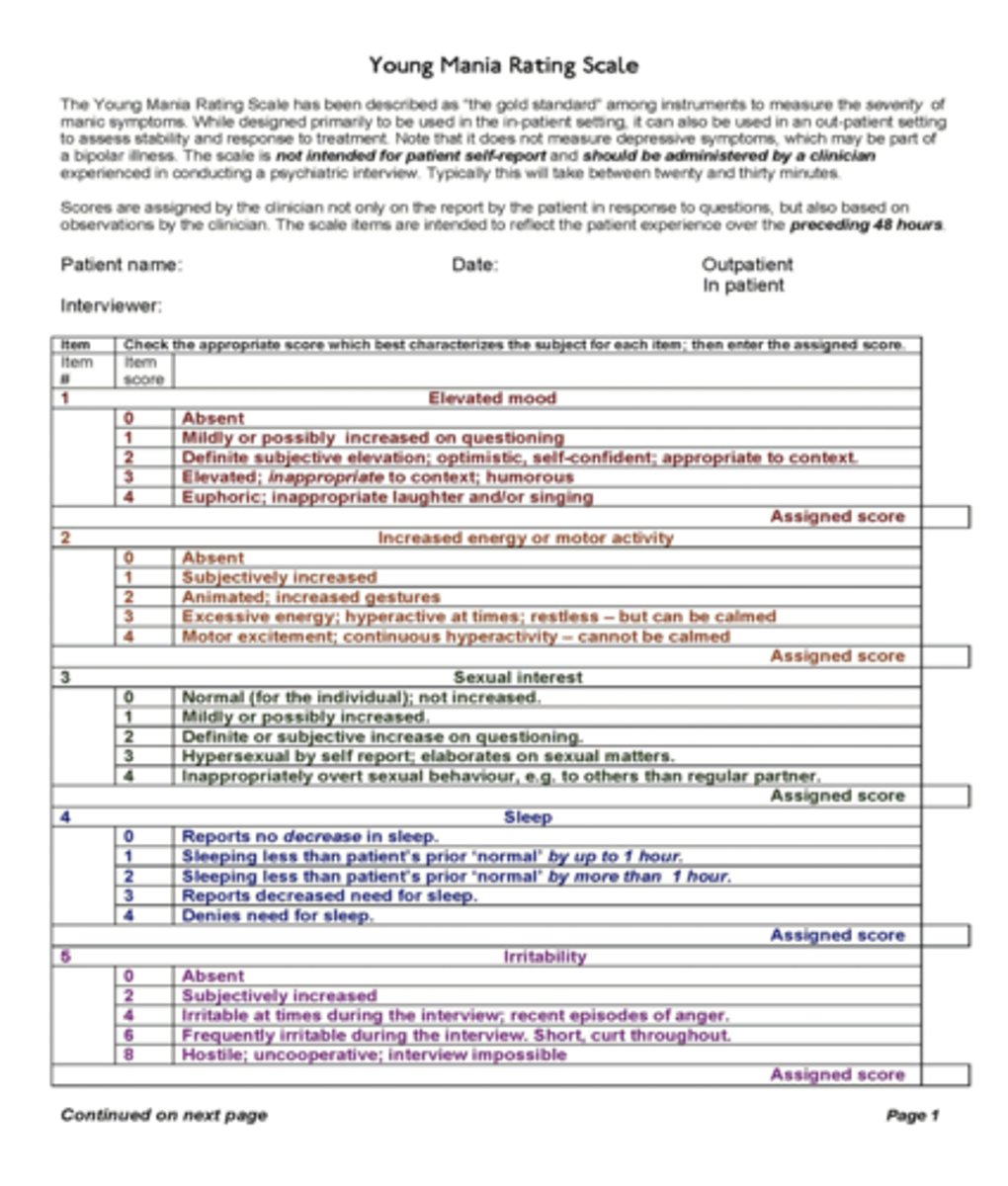
Mania Rating Scale
Mood Disorder Questionnaire (MDQ)
Young Mania Rating Scale (YMRS)
0-60 score
Bipolar Spectrum Disorder Scale (BSDS)
7-12 low risk
13-19 moderate
20-25 highly likely
MDD alternate therapies
Omega 3 fatty acids
St johns wort
S-adenosyl-L-methionine (SAMe)
Folate
Bright light
Acupuncture
Exercise
Vitamin D
Psychotropics with highest risk of birth defect.
Paroxetine
Lithium
Benzos
Valproic acid
Carbamazepine
Topiramate
MAOIs
TCA
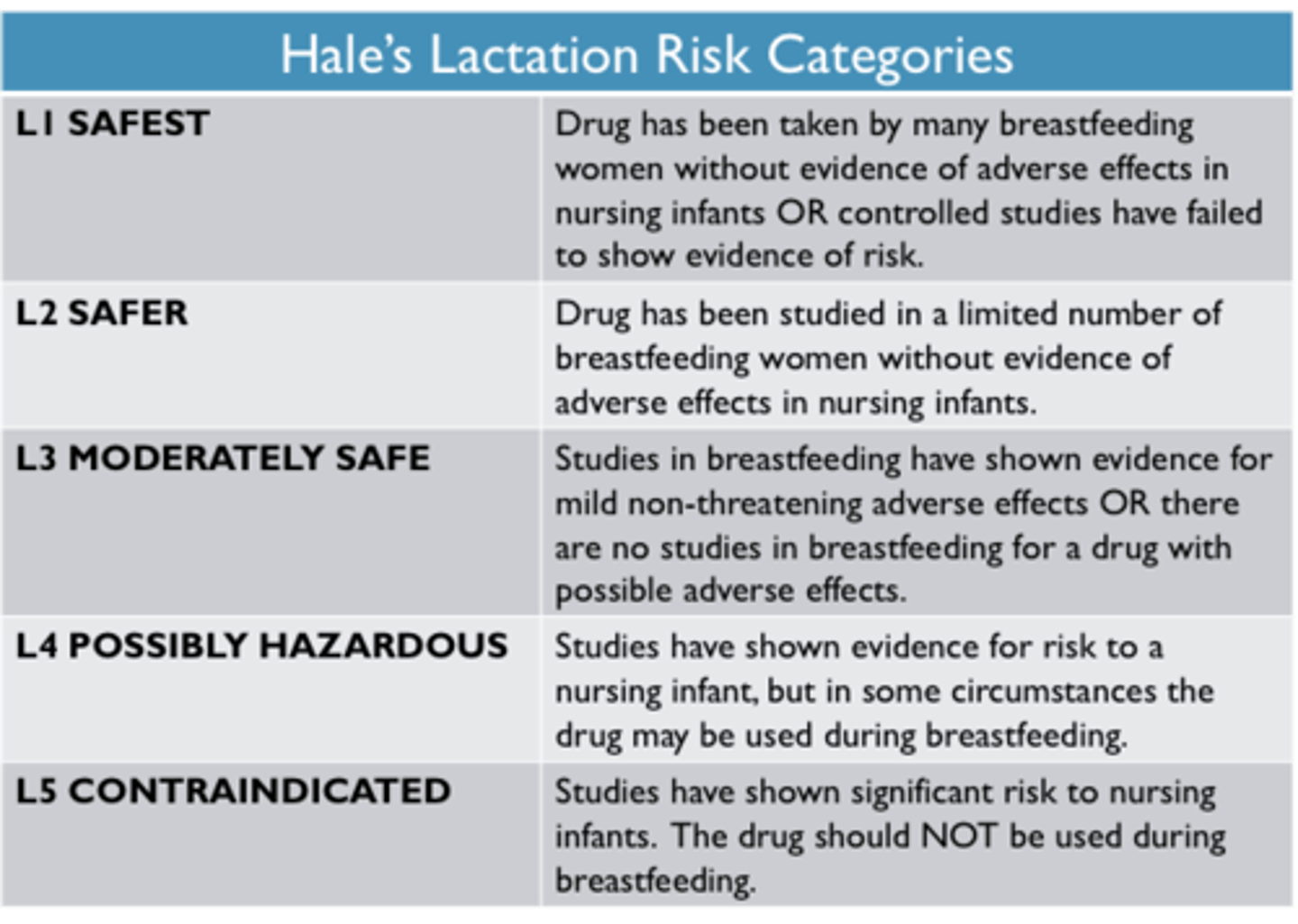
Lactation Risk Categories
L1-L5
L1 - safest
L4 - posing hazards
L5 - contraindicated
Activating Antidepressants: - good for patients who want to avoid medications that cause tiredness
Sedating:
Maintenance for MDD treatment?
Most lethal SSRI in overdose =•Associated with dose-dependent QTC prolongation in doses 40+mg•Max dose in Geriatrics= 20mg
All SSRIs
2 flu's
Pregnant
2 sits
Relax
Which SSRI has least drug-drug interactions?
Which one has the most sexual dysfunction and makes you tired?
- Fluoxetine, Sertraline, Escitalopram, Effexor ( symptoms restlessness, agitation, anxiety)-
Fluvoxamine(Luvox), Paroxetine
- at least 6 months (Up to 1 year)
-Citalopram (Celexa)
- Escitalopram
- Paroxetine
SNRI
Venlafaxine
Desvenlafaxine
Duloxetine
Monitor BP
Bupropion
TCA's
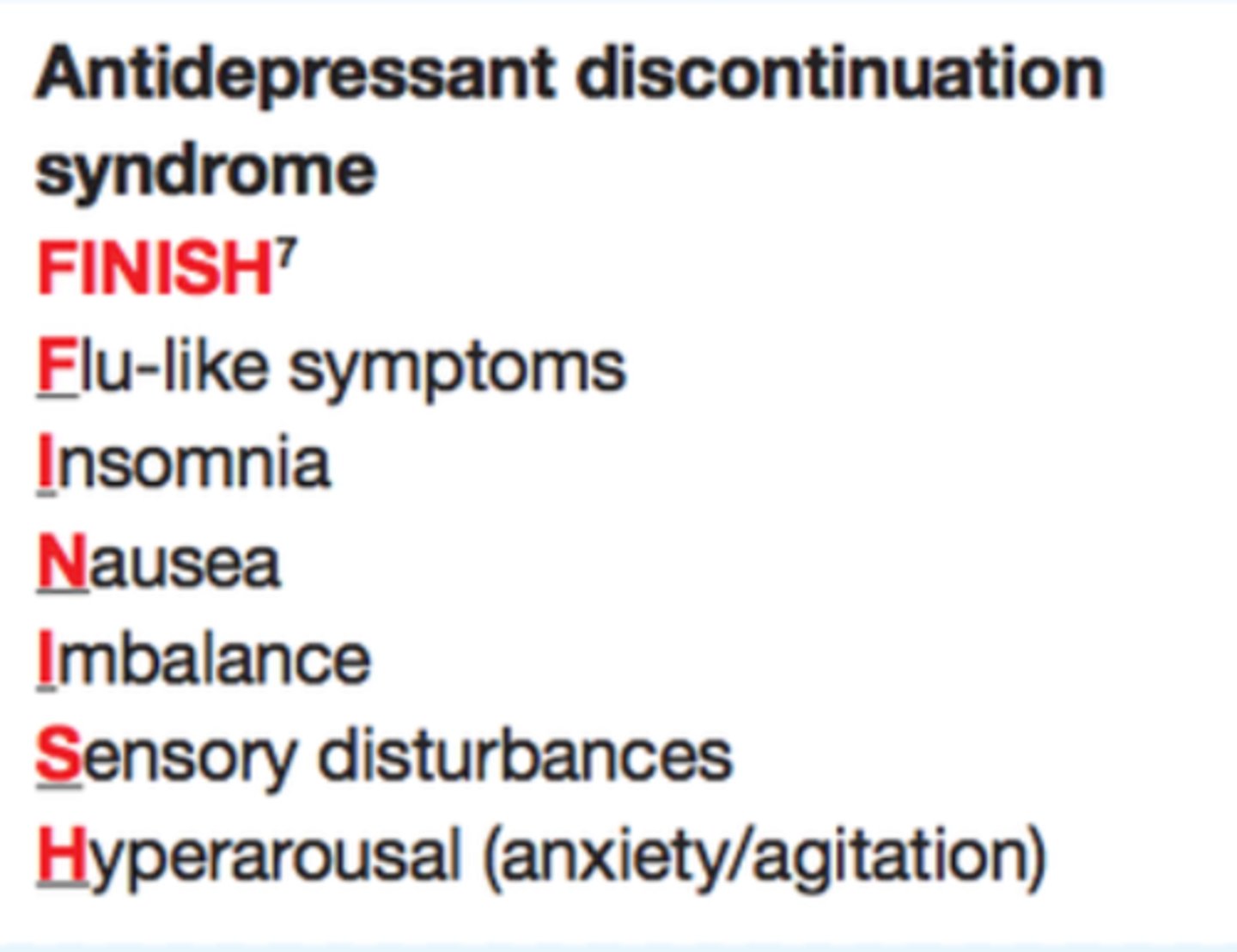
Serotonin discontinuation syndrome
FINISH
Sensory disturbance, sleeping disturbance, disequilibrium, flu like sx, dizzy, n/v
Chapter 9 Anxiety Disorders
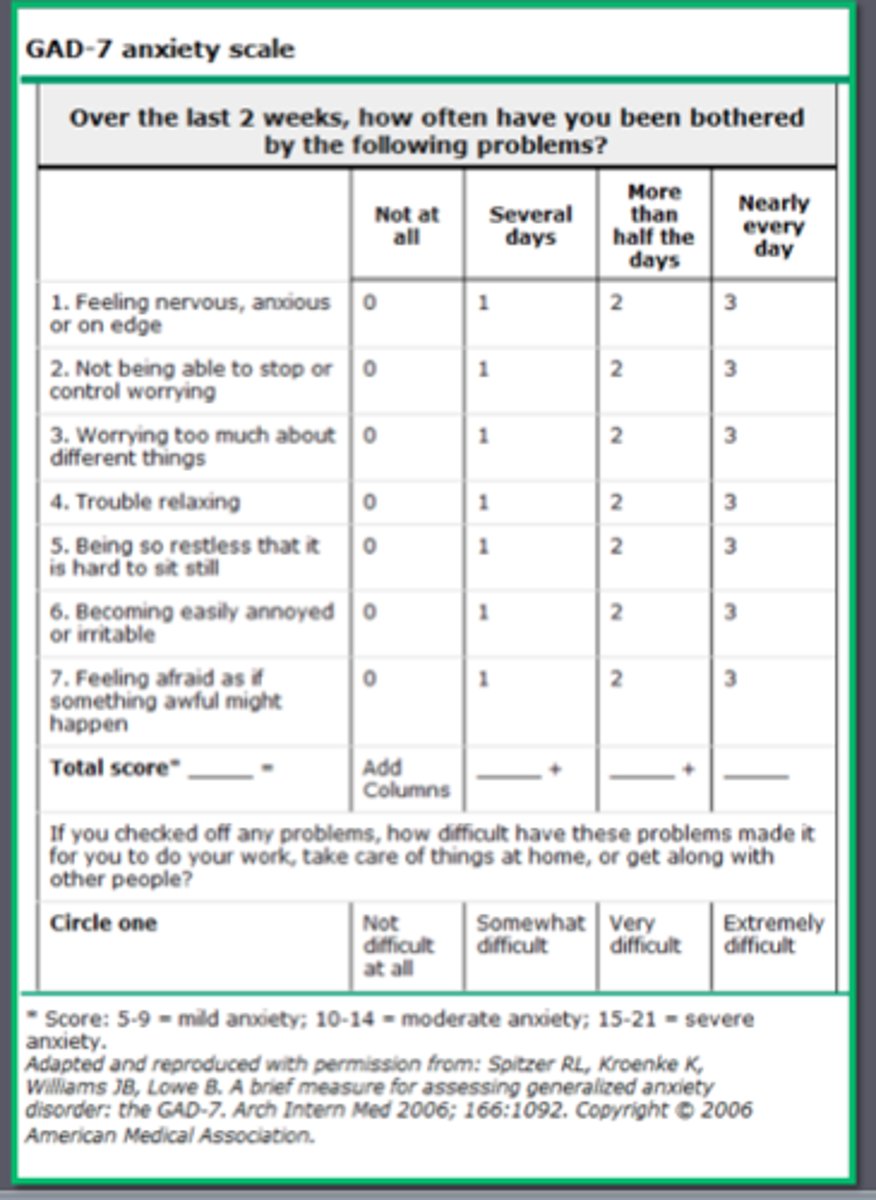
GAD 7
Generalized Anxiety Disorder /used to get objective data.. evidence based assessment.
- 5-9 mild
10-14 moderate
15-21 severe
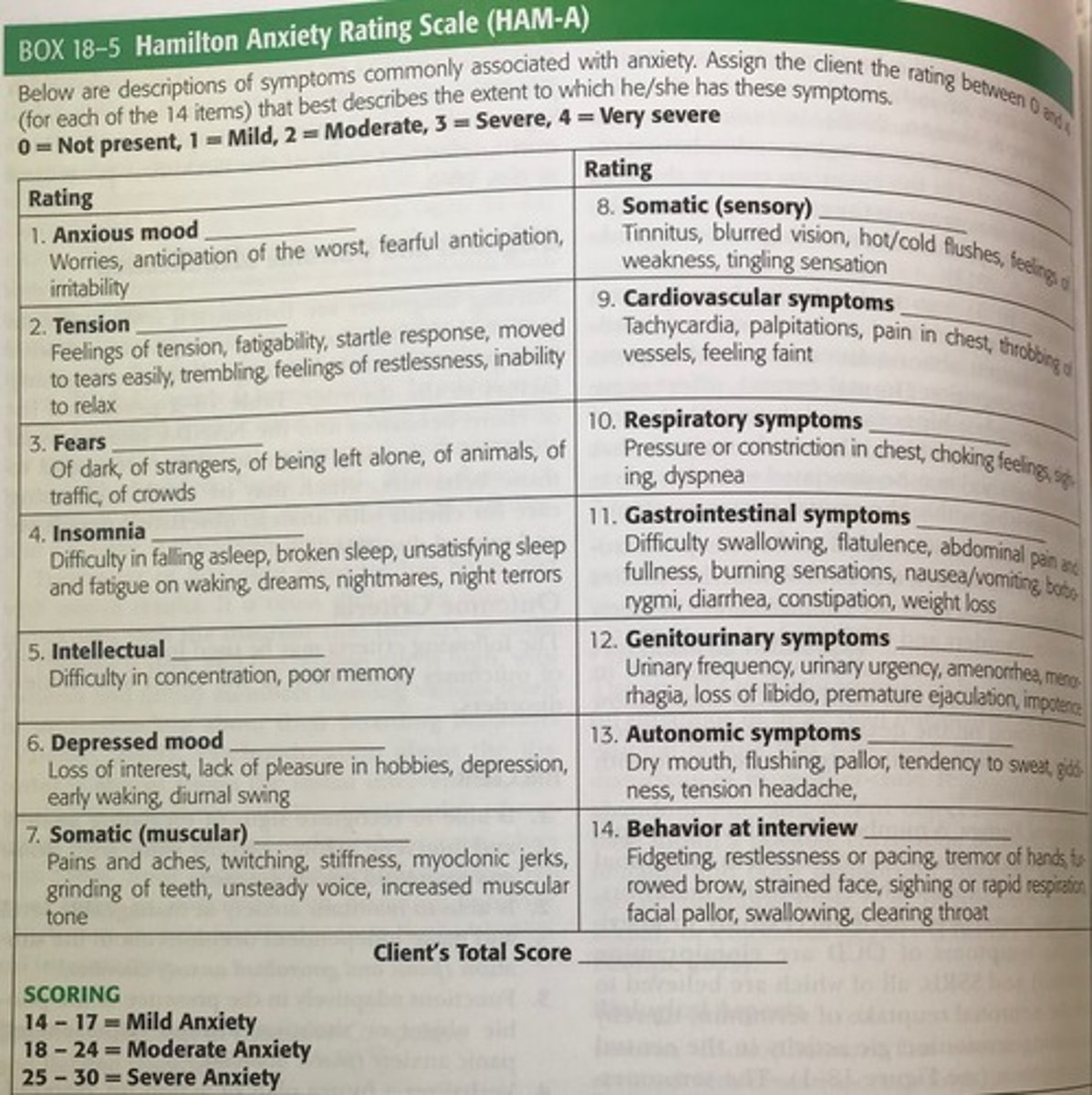
Hamilton Anxiety Rating Scale (HAM-A)
14-17 Mild Anxiety
18-24 Moderate Anxiety
25-30 Severe Anxiety
Zung Self-rating Anxiety Scale
20-44 normal range
45-59 mild to moderate
60-74 marked to severe
75-80 extreme anxiety
Yale-Brown Obsessive Compulsive Scale (Y-BOCS)
OCD
0-7 subclinical
8-15 Mild
16-23 Moderate
24-31 Severe
32-40 Extreme
Clinician Administered PTSD Scale for DSM-5 (CAPS-5)
For... diagnosis PTSD symptoms/severity
Clinician-rated
Higher the score = bad
Screen for Child Anxiety Related Emotional Disorders (SCARED)
41 item tool that screens for pediatric anxiety including GAD, social anxiety, seperation anxiety, and panic disorder
- >25 may indicate an anxiety disorder
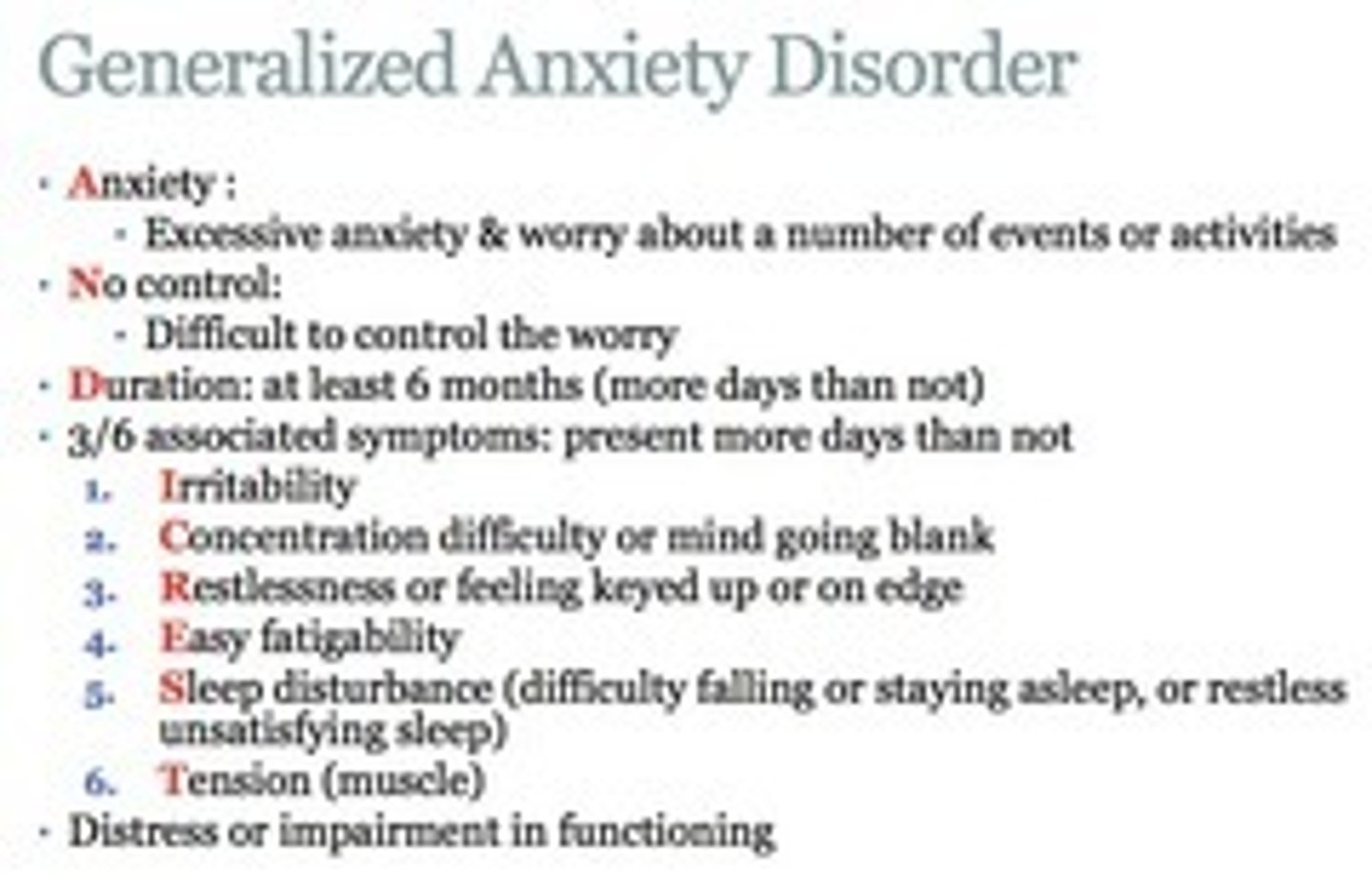
GAD
Amos mos 6
Cause significant distress or impairment.
50-90% have another psychiatric disorder.
Panic Attacks
Not a mental disorder and not a codable disorder.
This can be listed as a specifier like PTSD with panic attacks.
Panic Disorder
Women 2-3x more affected than men.
4 or more physical smptoms and one or more psychologic symptoms
peaks within 10 mins
-SUPRISE