Injuries
1/46
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
Head Injuries
Any injury to the skull, brain, or both that requires medical attention
A blow to the head may cause serious injury even when there are no external signs of injury
All head injuries are potentially serious because they may involve the brain, which is the seat of consciousness and controls every human action
Brain
Soft with a rich blood supply, and suspended in cerebrospinal fluid within the skull
Contrecoup Injury
When a severe blow to the head causes the brain to bounce from side to side, resulting in injury on the side opposite the blow
Open Head Injury
If skin overlying the broken bone is punctured
If an injury is open to the skull or meninges, the brain is vulnerable to damages and infection because its protective casing has been broken
Closed/Blunt Head Injury
Concussion, contusion, hemorrhage, or hematoma (Last 3 associated with bleeding)
The brain tissue may swell. The swelling is limited by the confines of the skull, and the resulting intracranial pressure (ICP) may cause extensive damage.
The brain has little healing power, so any injury to it must be considered potentially permanent and serious.
A rise in ICP may cause seizures, loss of consciousness, or respiratory arrest
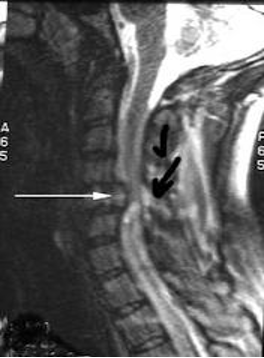
Basal Skull Fractures
May be open or closed depending on the skin overlying the broken bone
Often have accompanying fractures of the facial bones
This type of injury may result in a tear in the dura mater, the outer membrane surrounding the brain and spinal cord, and leakage of the cerebrospinal fluid may result
Open Head Injury Manifestations
Abrasions, contusions, or lacerations apparent on the skull
A break of penetration in the skull or meninges apparent by inspection or on radiographic images
Varying levels of consciousness
Basal fractures resulting in leakage of CSF may show as blood on sheet or dressing surrounded by a yellow halo sign
CSF may also leak from nose or ears or postnasal drip
Subconjuctival hemorrhage
Hearing loss
Facial nerve play
Periorbital eccymosis (Raccoon eyes)
Contusion
Bruising of the brain tissue
Occurs when an injury damages blood vessels under the skin and they leak below the skin surface
Hemorrhage
Active bleeding
A type of stroke
Caused by an artery in the brain bursting and causing localized bleeding in the surrounding tissues.
This bleeding kills brain cells
Hematoma
Collection of blood that has already clotted
A collection of blood outside of a blood vessel
It occurs because the wall of a blood vessel wall, artery, vein, or capillary, has been damaged and blood has leaked into tissues where it does not belong
May be tiny, with just a dot of blood or it can be large and cause significant swelling
4 types - Epidural, subdural, subarachnoid, and intracerebral
Epidural Hematoma
Bleeding between the dura mater and the skull
Subdural Hematoma
Bleeding between the arachnoid mater and the dura mater
Subarachnoid Hematoma
Bleeding in the subarachnoid space
Intracerebral Hematoma
Bleeding inside the brain
Concussion
Usually minimal amount of damage
Characterized by “seeing stars” or a very brief loss of consciousness
Most are mild and have a strong tendency toward spontaneous and complete recovery
Every one injures the brain to an extent
Does not contain significant bleeding like a contusion
Closed Head Injury Manifestations
Varying levels of consciousness, ranging from drowsiness, confusion, irritability, and stupor to coma
Lucid periods followed by periods of unconsciousness are possible
Loss of reflexes
Changes in vital signs
Headaches, visual disturbances, dizziness, and giddiness
Gait abnormalities
Unequal pupil dilation
Seizures, vomiting, and hemiparesis (weakness on one side of the body)
Basal Skull Fracture Manifestations
Raccoon Eyes
From bilateral subconjuctival hemmorrhage and occurs when damage at the time of the fracture tears the meninges and causes the venous sinuses to bleed into the arachnoid villi and the cranial sinuses. It develops 2-3 days after a closed head injury that results in a basilar skull fracture
Battle’s Sign
May accompany raccoon eyes
Bleeding behind the ear
Radiographer’s Response to Head Injuries
Keep head immobilized until spinal cord injury ruled out
If possible, elevate head 15-30 degrees
Do not remove immobilization devices
Do not flex or rotate patient’s head
Keep body temp as normal as possible
Check pulse and respirations frequently
Observe for airway obstruction
Apply a sterile pressure dressing if bleeding is profuse, and call for help
Watch for changes in loss of consciousness (LOC)
Be prepared to assist with oxygen administration
The Four Levels of Consciousness
Alert and conscious
Drowsy, but responsive
Unconscious, but reactive to painful stimuli
Comatose
Use the Glasgow Coma Scale to objectively assess changes in LOC over time
Score ranges from 3-15, immediately report changes in LOC to attending physician
Intoxicated Patients
Be aware of changes in consciousness with patients that are under the influence of alcohol
The alcohol effects may obscure important symptoms
Be especially alert to LOC changes
Spinal Injuries Clinical Manifestation - Complete Transection of Spinal Cord
Flaccid paralysis of the skeletal muscles below the level of the injury
Loss of all sensation below the level of the injury; pain at the site of injury possible
Respiratory distress
Bradycardia
Loss of body temperature control
Absence of somatic and visceral sensations below the site of injury
Unstable lowered blood pressure
Loss of ability to perspire below injury site
Bowel and bladder incontinence

Spinal Injuries Clinical Manifestation - Partial Transection of the Spinal Cord
Asymmetrical flaccid paralysis below injury level
Asymmetrical loss of reflexes
Some sensory retention; feeling of pain, temperature, pressure, and touch
Some somatic and visceral sensation
More stable blood pressure
Ability to perspire intact unilaterally
Radiographer’s Response to Spinal Injury
Monitor vital signs
Maintain an open airway, if respirations changes notify team
Do not allow or request the patient to move for xrays, may log roll patients with physician supervision
Do not move head or neck
Do not removed immobilization devices
Observe for signs and symptoms of shock
Keep the patient warm
If unconscious, assume there is a spinal cord injury
Log Roll
A - Pull table pad toward you and lift edge, keeping spine in one plane
B - As patient approaches lateral position, stabilize with hand on hip. Flexing knees helps to maintain position
C - The sheet alone may serve as support for returning patient to supine position
Closed Fracture
May not be obvious to the untrained eye
Often there is swelling around the injured areas, pain, and deformity of the limb
All or some of these symptoms may be absent and this fracture still present

Open Fracture/Compound Fracture
Indicates a visible wound that extends between the fracture and skin surface
The broken bone itself often breaks through the soft tissue making the fracture visible

Greenstick Fracture
A fracture in a young soft bone in which the bone bends and partially breaks


Spiral/Torsion Fracture
Occurring when torque is applied along the axis of a bone
While torsional forces are being applied along the parallel axis of a bone, planes perpendicular to this axis are not affected
Tension is exerted upon on part of the bone, while compressive forces are exerted upon the other
When these forces have exceeded the limit tolerable by the bone, fracture occurs


Overriding Fracture
A fracture in which the broken ends of the bone slip past each other and are held in the overlap position by contracted muscles

Comminuted Fracture
One in which the bone is splintered or crushed


Transverse Fracture
One at right angles to the axis of the bone


Compression Fracture
A collapse of a vertebra


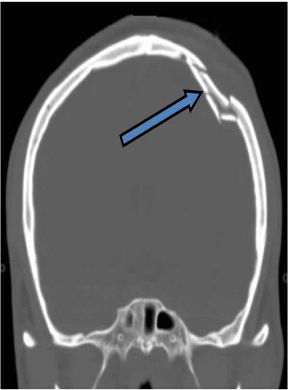
Depressed Fracture
A fracture especially of the skull in which the fragment is depressed below the normal surface

Avulsion Fracture
Occurs when a fragment of bone tears away from the main mass of bone as a result of physical trauma

Fracture Clinical Manifestations
Pain and swelling
Functional loss
Deformity of the limb
Grating sound or feel or crepitus if moved
Discoloration of surrounding tissue caused by hemorrhage with tissue (closed fracture)
Overt bleeding (open fracture)
Possible signs and symptoms of shock
Radiographer’s Response Fractures
Keep affected limb or body part immobilized
Any movement must be directed by the physician
Do not remove splints or supportive devices
In moving a splinted limb support both joints and the injury, move in a single motion
With an open fracture wear sterile gloves if in contact with the wound and use standard precautions
Observe patient for signs and symptoms of shock
Care with a Plastic Cast
Be careful not to put undue pressure on a wet cast
May cause it to change shape. Lift the cast by placing your open hands underneath it; never grasp it from above. Observe patient’s fingers or toes for evidence of impaired circulation
Pay attention to the condition of fingers and toes
Should be warm pink and sensitive to touch and pressure. Coldness, numbness, or lack of normal coloration should be reported
Swelling and pressure can cause permanent damage
Can compromise circulation and cause nerve and tissue damage
Open Wounds
Maintain dressings and report any fresh bleeding sufficient to soak through a fresh dressing
If a laceration or incision opens, causing severe hemorrhaging, apply direct pressure to the site of bleeding while summoning immediate assistance
Post Surgical Wound Dehiscene
When a surgical suture line parts
Partial or superficial
Involves only the outer layers of the wound
Complete
Involves all layers of the wound. It may lead to protrusion of underlying tissues through the wound, or to evisceration (loss or organs from the body cavity). Patient may state that something has given way and complain of pain, or a rush of liquid may saturate the dressings. If this occurs, ease the patient to a recumbent or semi-recumbent position to take the strain off of the area
Postsurgical Care
If patient is ambulatory, stand nearby to steady them. An abdominal binder may be applied to help support the abdominal tissues. Unless stated, do not remove the binder. If you must, wait until the patient is comfortable on the table. Replace the binder before the patient is transferred back to stretcher
Burns
Frequently associated with respiratory complaints
Inhalation of hot gases may result in edema (swelling) of the respiratory tract, pleural effusion, or pneumonia
Burn Categories
Categorized by the cause of injury, percentage of body surface involved, and depth of tissue destruction
The depth of burns is classified as first, second, third, or fourth degree
First Degree Burn
Epidermis Only
Skin is red, warm, tender, and painful. May be swelling without blistering
Second Degree Burn
Dermal layer, but not enough to prevent the growth of new epidermis during healing
Pain swelling and blisters may be extensive and require medical attention
Third Degree/Full Thickness
Deep into the subcutaneous tissues and destroy nerve endings
The skin appears charred or white and lifeless, such as burns caused by scalds or steam. Subcutaneous tissue, dermis and epidermis are involved and skin transplants may be needed
Fourth Degree/Full Thickness
Involves skin, fat, muscle, and sometimes bone
The charred skin may be completely burned away. Extensive surgical debridement and grafting are commonly needed, and sometimes amputation is necessary
Radiography of Burn Victims
Coordinate with nurse to ensure pain medications have been given around 30 minutes prior to exam
May have protective precautions to avoid infection
Beware of grafts or healing skin that is tender. It is easily damaged during transfer and positioning
Allow them to move themselves as much as possible
Use a transfer sheet to avoid abrasion