Case 4
1/312
Earn XP
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
313 Terms
What is the role of the cardiovascular system?
blood flow to tissues and organs, transport of nutrients, metabolic ditribution, hormones/signalling molecules, heat distrbution, immunological, regulation of pH and osmolarity
What is ascemic tissue
when the tissue isn’t getting sufficent oxygen
What is an infarction?
when cells in the tissue die due to lack of oxygen often caused by blocked blood vessles
What is hypotention normally talking about?
systemic circulation or ateriole pressure, but can also get pulmonary hypotention
Where is 65-70% of the blood found?
in veins
What is the word for blood vessles splitting into smaller blood vessles (by halving)?
biferate
How does blood move into the capillaries?
by moving down a pressure gradient, the pressure is generated by the heart
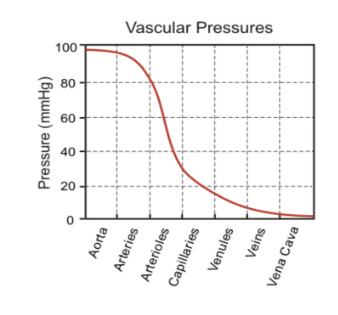
Why are arterioles so important?
can open and close (contract and dilate) them changing how much circulation goes to which part of the body, how blood pressure is controlled beat by beat, this is the point with the most segnificant drop in blood pressure
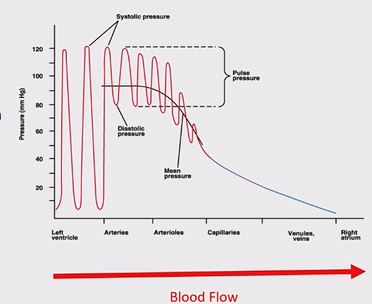
What is systolic pressure?
how much pressure the left ventricular wall is putting on the blood when contracted
What is diastolic pressure?
the pressure the left ventricular wall is putting on the blood when relaxed, needs to be a low number so the ventricle can refill
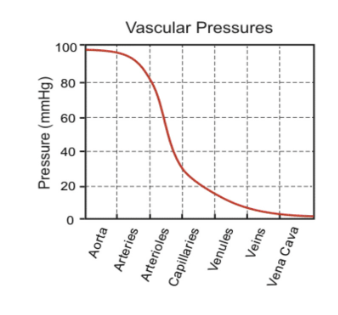
Why does blood pressure drop in the circulation?
the blood looses energy through friction as it rubs against blood vessel walls, this is resistance (R)
What is Q?
blood flow, how much blood is flowing down the blood vessle per unit
What is the ralationship between Q and pressure?
Q through each circulation is proportional to the pressure gradient (∆P)
At what point are you messuring blood pressure?
in the braicial artery, messuring arterial pressure
What is stroke volume (SV)?
volume of blood pumped by one ventricle, should be around 75mLs, should be the same every time and the same on both sides
What is cardiac output (CO)?
volume pumped per ventricle per minute, should be 5L/min
If there is an increase in the force of contration what does this incerease?
stroke volume and cardiac output
What is venous return (VR)?
the volume of blood returning to the heart, should be the same as cardiac output
Why would venous return not be the same as cardiac output?
heart failure, can’t pump out all the blood effectively, pressure backs up, in the lungs this can cause fluid in the lungs, in the capillaries causes fluid in the tissues
What is fluid in the tissues know as?
edema
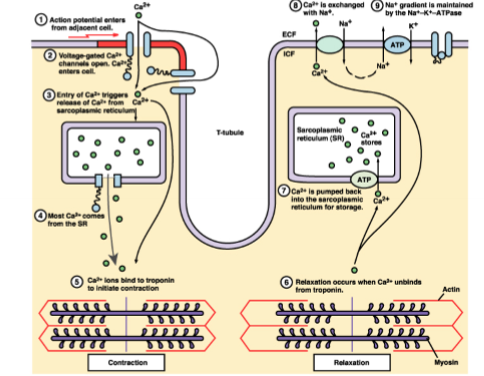
What is the difference between cardiac and smooth muscle contraction?
the Ca²⁺ sensor is troponin in cardiac cells not calmodulin
How does cardiac muscle contraction increase blood pressure?
actin and myosin filaments slide over each other increasing tention
How is atrial and ventricular contraction triggered?
If cytosolic calcium (freely availible calcium) is high, the left ventricle contracts, recycling of calcium occurs to relax the muscle, some of the calcium comes from the extra cellular fluid, most is held in the scarcoplasmic reticulum, this release is triggered by the opening of voltage gated calcium channels on the cell membrane, a little bit of calcium enters the cell triggering the release of the calcium, voltage depolarisation then the calcium channels open
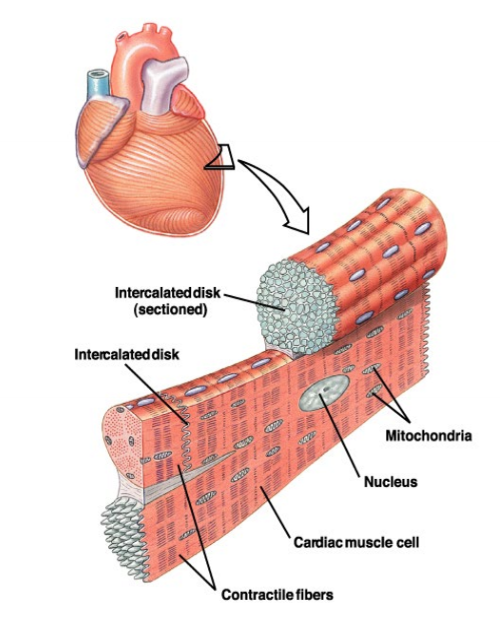
What are the features of cardiac tissue that allow for electrical conduction?
intercalated disks are full of protein and are located where two cardiac muscles touch, intercalated disks form gap junctions, allowing small molecules to move between adjectent cells
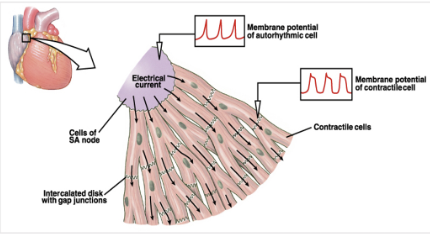
What is the synoatrial node?
located at the top of the heart, sponainously produce voltage, this triggers a contraction of the heart
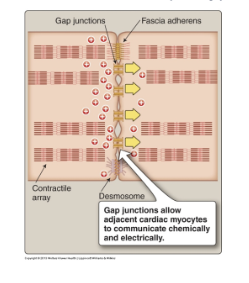
What is a gap junction?
a protein tube that physically connects one cell to the next, allows molecules to move to adjecent cells, allow electricity to jump from one cell to the next
How does the wave of contraction in heart occur?
waves of electricity spread via gap junctions, causes wave of electrical activity which in turn causes a wave of muscle contraction, this is useful as it helps fluids move in one direction
How do action potentials spread in the heart?
Start in the SA node, move through the atria, then to the atrioventricular node (only way charge can get to ventricles), AV node depolarises and holds the signal very breifly, then charge flows down the bundles of His, it then goes to the atrium of the heart, it then spreads upwards through the ventriculuar muscle, this then pushes the blood upwards into the arteries
What is the annulus fibrosis?
non-conducting layer between atria and ventricles, electrically insulates the chambers from each other, stops them touching each other
What is the bundle of His?
found in the ventricular septum, fast conducting tissues
What is fibrillation?
randomly twitching, not coordinated activity
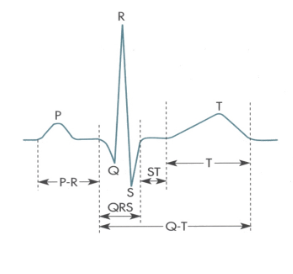
Describe the ECG wave
P wave - atrial depolarisation, P-R interval - between beginning of excitabillity of atria and ventricles, QRS complex - ventricular depolarisation, atrial repolarisation occurs but is obscured, Q-T interval - contraction occuring also includes ventricular repolarisation, S-T segment - all ventricular tissue depolarised contraction occuring, T wave - ventricular repolarisation
How are cardiac cells linked to the autonomic nervous system?
transmitters bind to adrenergic or cholengernic receptors on the cardiac cell membrane which then cause ion channels to open/close
How do sympathetic nerves affect heart rate?
releases noradrenaline when activated, binds to β₁ adrenoceptors on the cardiac pacemaker and myocyte cell membranes, increases opening of HCN channels in pacemaker cells, increases Na⁺ influx (increases positive charge in the cell slightly), opens Ca²⁺ channels (increased number), increases Ca⁺ influx, inside of cell becomes positive, get depolarisation, increase slope of prepotential, heart rate increases, cells hit threshold sooner
How do you reset the synoatrial node (after changing heart rate)?
potassium channels open, looses positive charge, repolarisation
How do parasympathetic cells affect heart rate?
(vagus nerve) activation causes release of acetylcholine, binds to muscarinic cholinergic receptor, decreases opening of HCN channels, decreased Na influx, slows opening of Ca²⁺ channels, decreased Ca²⁺ influx, opens additional K⁺ channels (ligand gated), increased K⁺ efflux, hyperpolarises membrane and reduces slope of prepotential, heart rate decreases
How is heart rate balanced?
natural rate of firing of SA is about 110 action potentials per min (= heart rate), vagus nerve is constantly firing, so contantly decreasing heart rate, sympathetic nerve is occational firing
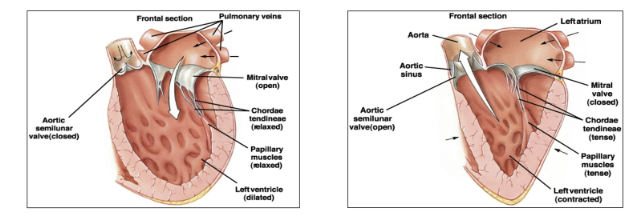
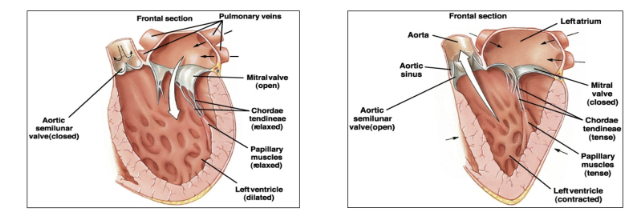
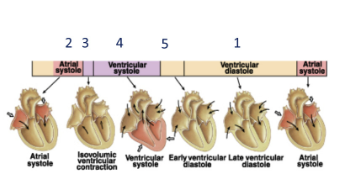
What is the sequence of mechanical events in the cardiac cycle?
ventricular filling (refilling with blood low pressure), atrial contraction (atriole systole), isovolumetric ventricular contraction, ventricular ejection, isovolumetric ventricular relaxation (both semi-luna and atrioventricular valves are closed until pressure drops)
Why does atrial systole occur?
to push the last bits of blood into the ventricle
When do the heart valves closed?
atrioventricular valves close when ventricular contraction takes place
semi-luna valves open when the ventricular pressure
Why is diastolic blood pressure higher than the minimum pressure in the left ventricle during distole?
blood can’t go anywhere until it has overcome the aortic blood pressure
What is isovolumetric ventricular filling?
pressure is increasing in the left ventricle, atrialventricular valves and semi-luna valves are closed
What is contractillity?
mechanism extrinsic to the heart, changes in stroke volume without changes in resting ventricular muscle fibre length, more cyostolic calcium increases this, anthing that increases calcium increases this including drugs, also affected by noradrenaline and adrenaline
What is preload (venous return)?
degree of stretch in the ventricules due to end diastolic pressure dependent of end diastolic volume, changes in stroke volume dependent in resting ventricular muscle fibre length, mechanism intrisic to the heart, if you stretch the muscle beforehand then the actin lines up with the myosin better so they have more tention so more forceful contraction
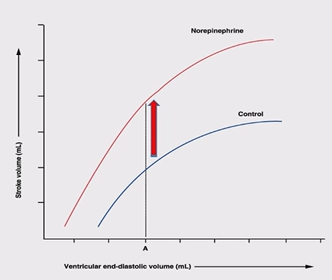
What is starling’s law of the heart?
force of contraction is proportional to the initial fibre length in diastole, an increase in blood returning to heart (increase in ‘filling’ pressure) increases EDV, this stretches the cardiac muscle and produces a more forceful contraction
(Heterometric intrinsic)
What happens if there is low preload?
actin and myosin overlap is not opitial, reduces ability to contract
What happens if there is a high preload?
some stretching of ventricular muscle, optimum cross bridges availible, increased affinity of troponin C to Ca²⁺, maximal force produced
What happens if there is an overfull heart?
heart failure, actin and myosin are physically seporated, preventing interaction, reduced force generated
What is the effect of the sympatheric nerve stimulation on the heart?
increase in stroke volume without a change in initial fibre length, increase in contractility, positive inotropic effect
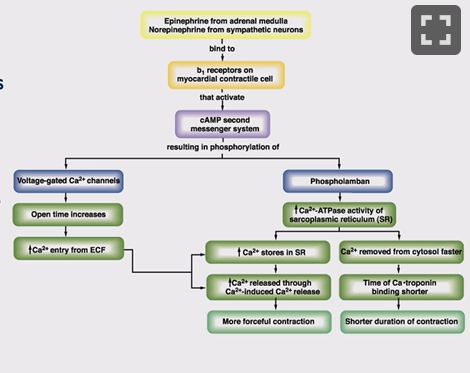
What is the mechanism for the release of calcium in cardiac cells?
Noradrenaline (or drug) binds to β₁ adrenic receptor, if on SA node heart rate increases, if in ventricular muscle cAMP second messenger system activated, opens voltage-gated calcium channels, so more calcium enters the cell from ECF, this in turn triggers more release of calcium from the SR (also more calcium in the SR), triggers more forcefull contraction, this is a positive ionotrophic effect, cAMP also increases Phospholamban, increases the mechanism pulling calcium into the SR, the next time they release the calcium they have more to release, more forcefull and shorter contractions (as calcium put back fast)
What are catecholamines?
nuroreceptors including noradrenaline and adrenaline
How is blood pressure controlled?
systolic pressure is maintained in the aorta and arteries due to their thick walls, diastolic pressure (2/3 of the process) stays higher in the aorta than the left ventricle as the elastic recoil returns energy/pressure to the blood and the aortic valve is closed, as blood goes through the system energy/pressure is lost to the vessel wall due to friction
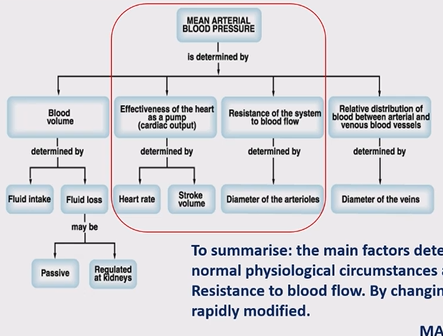
What controls you mean arterial blood pressure?
blood volume - determind by fluid intact and loss (passive or kidneys) (not very relevent)
effectivness of the heart as the pump - heart rate and stroke volume
resistance of the system to blood flow - diameter of the aterioles
relative distribution of blood between aterial and venous blood vessels - diameter of the veins (most blood in veins)
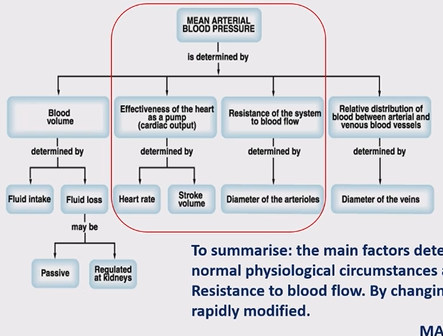
How would you calculate mean arteriole blood pressure?
(under normal physiological circumstances, MAP = cardiac output (CO) x Total peripheral resistance (TPR)
What is total peripheral resistance?
how difficult it is for the blood to flow throught the peropheries (vasoconstriction so blood pressure increases) (when standing up pressure goes up as has to go to the brain and has all gone to your feet, brain not getting enough blood)
What is the barrow receptor reflex?
borrow receptors located in the carotid and aortic bodies above heart, detect changes in blood pressure, shunt blood where it is needed to, shut down if not needed, uses flattening of arterioles

What happens when your barrow receptor detects low blood pressure?
sensory nerve takes signal to cardiovascular control centre in the brain, sympathetic neurones synapse on SA node increasing heart rate, synapse on ventricular muscle increasing force of contraction, synapse on arterioles causing peripheral vasoconstriction (α₁ receptor), also cause vasoconstriction shunting blood into the arteries (barrow receptor reflex)

What are β-blockers?
β-adrenergic blocking agents, blocks the effects of epinephrine (all carecholamines), heart beats slower with less force lowering blood pressure, widen veins and arteries improving blood flow, competitive inhibition of receptor
What are β-blockers used to treat?
irregular heart rhythm, angina, hypertention
What are all the types of adrenoceptors?
α-1 - smooth muscle contraction, mydriasis
α-2 - mixed smooth muscle effects
β-1 - increased cardiac chronotropic and inotrophic effects
β-2 - bronchodilation
β-3 - increased lipolysis
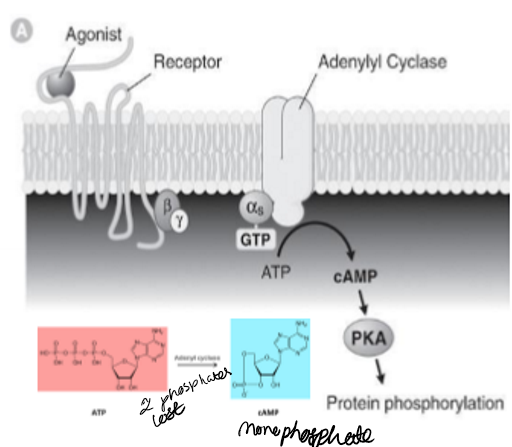
How is the amount of cAMP controlled?
cyclised, degraders phosphatases that break it down, sometimes this happens too much and causes problems
What does inotropic mean?
increases contractility
What does chronotrophic mean?
increases heart rate
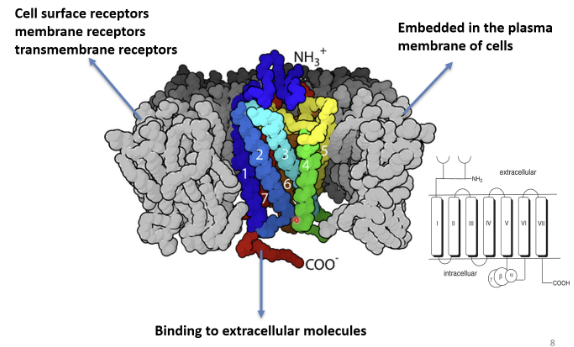
What are the good things about G coupled receptors?
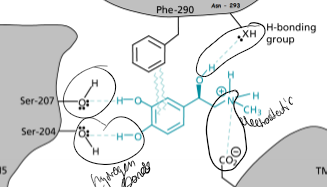
if the drug/ adrenaline/ noradrenaline isn’t able to fully penertrate into the cell, they can bind to the exposed part on the outside of the plasma membrane, NH₃⁺ is extracellular, COO⁻ is intracellular
Where are β receptors found?
most likely β₁ in cardiac and β₂ in bronchial smooth muscle and blood vessels, but a number of tissues contains mixed populations, can lead to offtargeting
What receptors can trigger vasodilaton?
α,β, and α/β potentcy
What do β₃ receptors do?
metabolic rate control in animals - adipose tissue, involved in fatty acid metabolism
What are the differences between β₁ and β₂ receptors?
differences in stucture (some different amino acids), different size, level of homology is high in membrane spanning region, this is where the molecules interact so can cause problems
What is the structure of a β₁ receptor?
7-Transmembrane receptors, G protein linked to adenyl cyclase, ATP to cAMP (two phosphates lost) , protein phosphorylation drives response
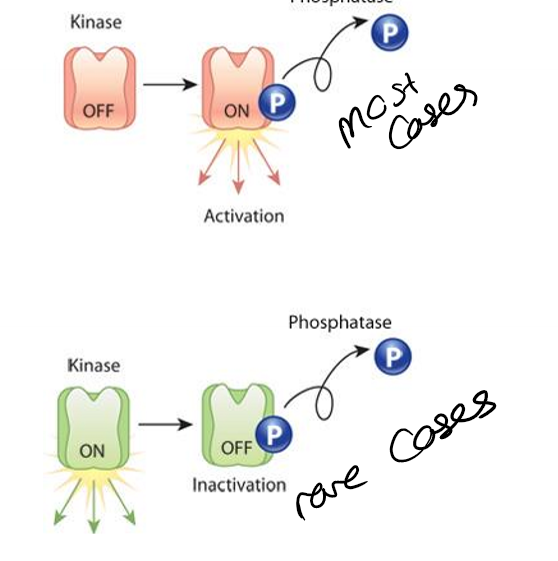
What are protein kinases?
add a phosphate group, mainly add to activate a molcule, rarely to inactivate a molecule
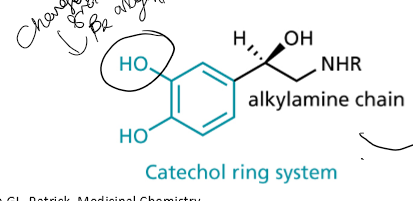
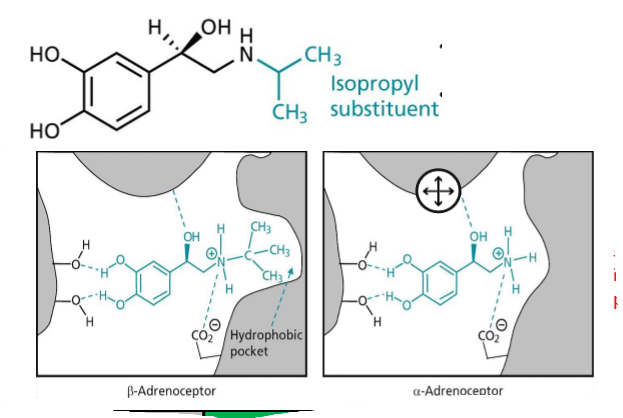
What is the name of the ring and chain contained in things that interact with the β receptor binding sites?
catechol ring system, with alkylamine chain
What interactions happen at the adrenergic binding site?
H-bonds, electrostatic interactions, interacted between two benzene rings
What is the stucture activity relationship with beta blockers (and other for the same receptors?
R is more active than S, the two hydroxyl groups on the catachol ring can be any hydrogen bond forming group, if the R group attached to the NH (R₂) is larger then it has increased β selectivity, the substituent increases α-receptor binding (on the C next to the NHR₂) so avoid
What is isoprenaline?
Isopropyl substituent added to the NH, due to hydrophobic pocket in β-receptor, has low half life (bad), good β₂ binding, evolutionary redundency
What is evolutionary redundancy?
the presence of more causal componants in a system than what is required for its proper function, more resistance, if the drug gets stuck, exploit to have effect, body uses it to make it resistant
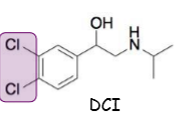
What is DCI?
dichloroisoprenaline or dichloroosoproterenol, 1st β-blocker, antagonist, partial agonist as well, no clinical value, chlorines instead of hydroxyl groups
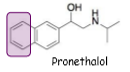
What is Pronethalol?
DCI with replaced 3,4-dichloro substituents for a carbon bridge, blocks β-receptors and only a marginal partial agonist, 1st clinically availible, treated high blood pressure, angina and certain cardiac arrhythmias, withdrawn due to toxicology concerns (thymic tumours in rats), only used in life threating situations
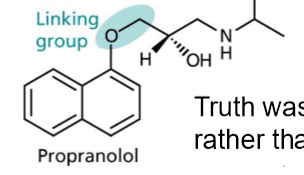
What is propanolol?
20x more active than pronethalol, original target no better, higher potency with fewer side effects, used α-naphthol instead of β-naphthol in the linking group
What are epoxides?
strained 3-membered rings containing an oxygen atom - therefore the carbons are electrophilic, ring strained (angle close to 60) helps drive reactions with neuclephiles as electrophilic and very reactive
Where do strong nucleophiles under basic conditions open?
at the least subsituted end
Where do strong nucleophiles with an acid catalyst open?
more of the subsituted end product is produced
What is epichlorohydrin?
a special epoxide for providing a 1,2,3-substituted compound
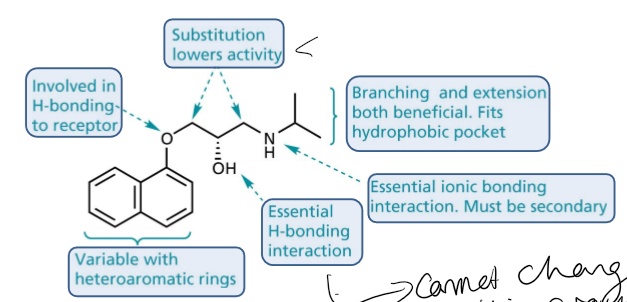
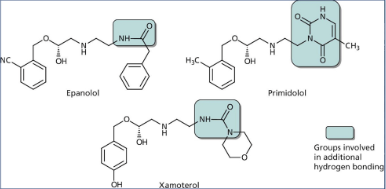
Explain the structure activity relationship of aryloxypropanolamines?
double benzene rings are varible with heteroaromatic rings, the oxygen attached to the right ring is involved in H bonding with the receptor, the carbons in the chain if hydrogens are substited it lowers activity, the OH is essential in H bonding interactions, the NH has to be secondary and is involved in essential ionic bonding interaction, branching and extention are both benificial as fits in the hydrophobic pocket
What where the issues with 1st gen β-blockers?
crossed BBB causing dizzyness and sedation as highly hydrophobic, caused brochoconstriction in athsmatics, lowered cardiac output
How was propanolol modified to make it a better β-blocker?
reduce logP (want below 0), remove one aromatic ring, logP lowering group (acetamide and sulphonamide), add NHCOCH₃ to the bottom of the remaining ring to ncrease hydrophilicity
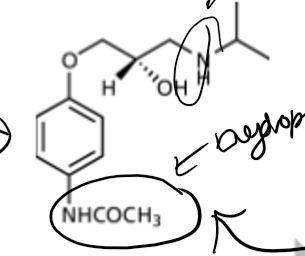
What is practolol?
β-blocker, not as potent as propanolol but more selective (less CNS side effects), β₁ selective over β₂, used for angina, hypertention ad immediate use post MI, rashes, eye problems and peritoitis have led to withdrawal
What are the 2nd gen β-blockers?
acebutolol, atenolol, metaprolol, and betaxolol
What are the features of 2nd gen β-blockers?
contain extended para subsituent, capable of H bonding, cardioselective, few side effects, some effect on smooth muscle and used when no alternative in asthmatics,
What are the advantage of acebutolol in particular (β-blocker)?
a partial agonist and causes less bradycardia and coldness of extremities
What are the disadvantages of 1st gen β-blockers?
broncoconstriction in athsmatics, fatigue and tiredness of the limbs, reduced cardiac output, CNS effects, dizziness, nightmares and sedation, coldness of extremities (reduced cardiac output), heart failure for patients on verge of heart attack - produce a fail in the resting heart rate and this may be enough to cause near MI patient over edge
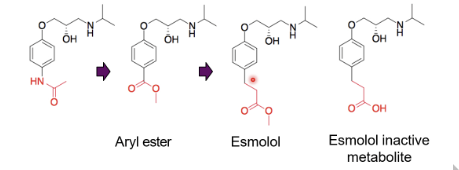
What are short acting β-blockers?
add ester - introduce of labile functionality, aryl ester wasn’t hydrolysed quickly, esmolol identified, a couple more carbons away from the ring
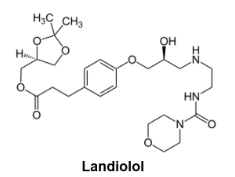
What is landiolol?
seven-fold higher cardioselectivity for landiolol over esmolol, 8 to 12 fold potentcy as well
What are the features of 3rd gen β-blockers?
incorperate extended amine substituent - idea that interact with another part of the β₁ receptor - fill hydrophobic pocket, have selectivity, logP issues
Name a 3rd gen β-blocker and what it is used for?
Carvedilol used in congestive heart failure
Why is hypertention important?
if pressure is increased in blood vessles then the blood vessels may burst, common condition, more common in older people
What are the problems with defining blood pressure?
it is a continous varible that varies throughout the day, thresholds for blood pressure can change
What are the risks of increasing blood pressure?
2mm/Hg increase in systolic blood pressure increases risk of stroke by 10%
What are the symptoms of hypertention?
genrally asymptomatic, person can feel worse on medication so adherance is a problem, with really high blood pressure can get subconguitival hemorage, red in sclera, retinal hemorage, might affect vision, headache
What is primary hypertention?
don’t really know the cause, most common, just due to aging
What is secondary hypertention?
there is a known cause, caused by certain conditions: tumour on top of kidney causing increased adrenaline, more commonly medication: NSAIDs, combined oral contraceptive increase fluid retention