While you were sleeping (WYWS) Final study guide
1/154
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
155 Terms
Process S
"S" stands for Sleep Pressure or Sleep Debt
Homeostatic (constant, stable)
Sleep propensity increases the longer you stay awake
Sleep propensity decreases with sleep
You can think of Process S as intensity of sleepiness or a drive to put you to sleep
Process S is homeostatic
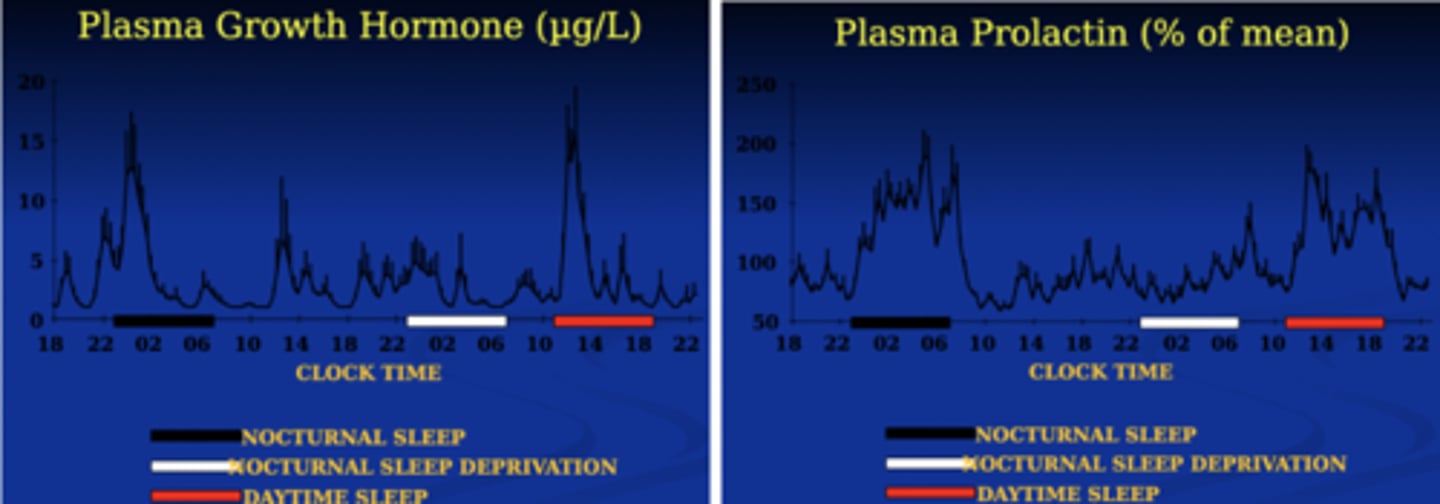
Growth hormone and Plasma Prolactin is under process S
Process S is sleep debt
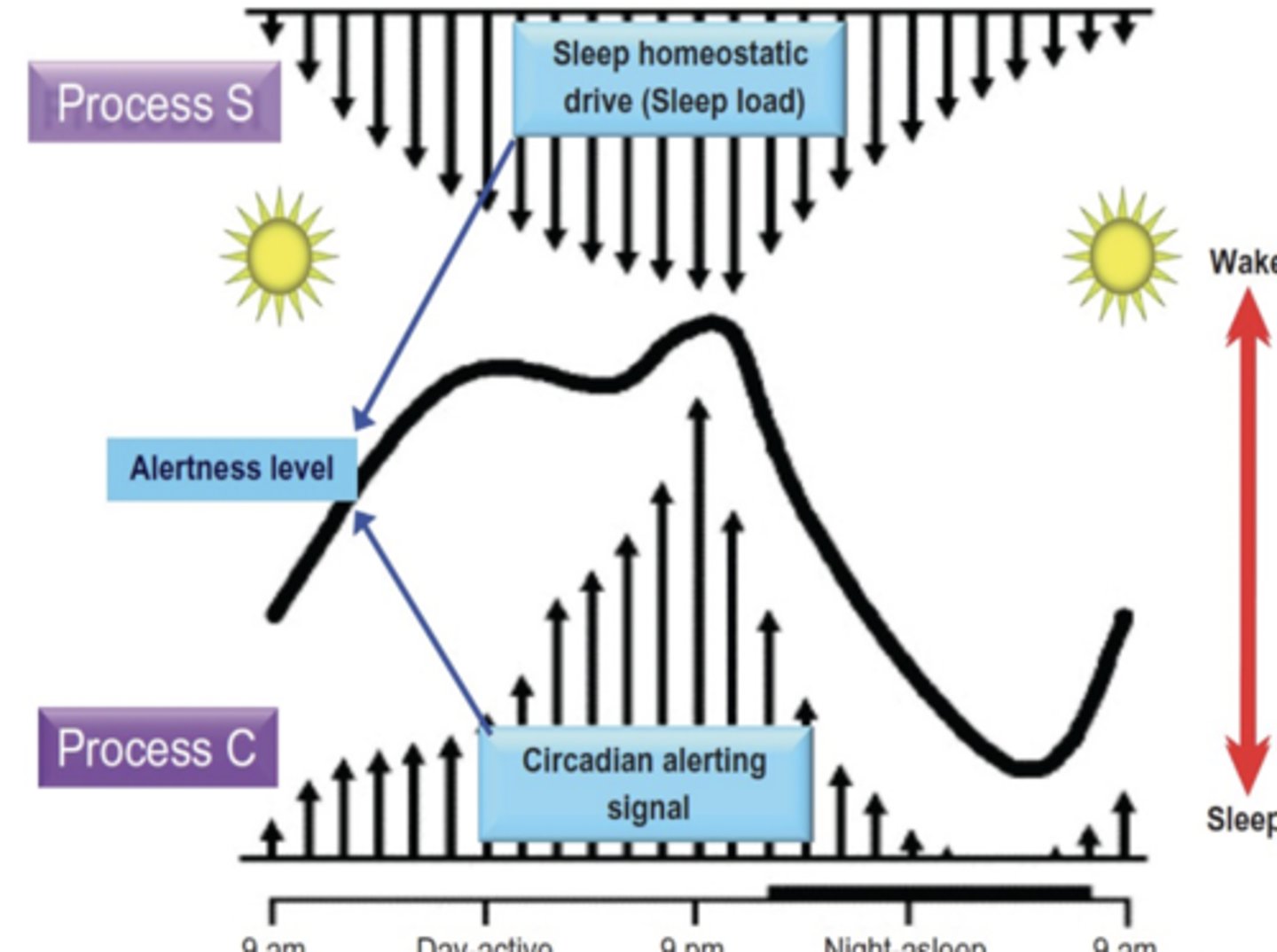
Process C
"C" stands for circadian
A self- sustained biological rhythm normally synchronized to roughly 24 hours
Circa means "approximately" or "near to"
Dia means "day"
the site of Process C is Suprachiasmatic nucleus (SCN)
Process C is: strongest at the end of the day, related to body temperature
Process C is circadian rhythm
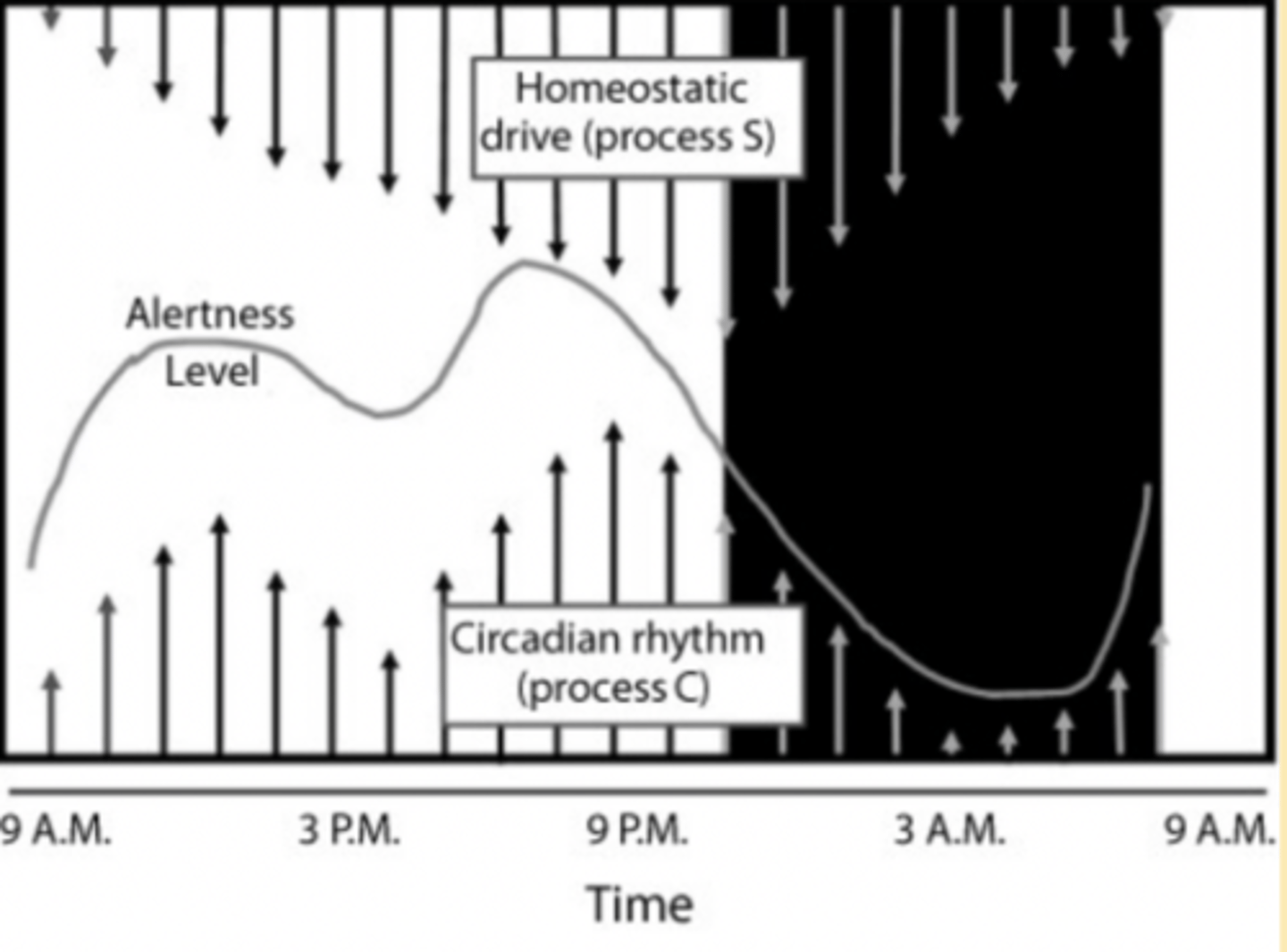
Opponent Process (Two Process) Model
Delta power or SWS during NREM can be used to estimate Process S
Delta power increases logarithmically as waking is prolonged
Core Body temperature is often used as a measure of Process C
Sleep propensity is greatest during the falling limb of the circadian body temp rhythm and decreases on the rising limb
Human and animal studies suggest that process C regulates arousal and REM but that NREM M is more strongly under the control of Process S
Suprachiasmatic nucleus and zeitgebers
where the clock is
Suprachiasmatic nucleus (SCN)
Located at the optic chiasm, where the optic chiasm, where the optic nerves cross, within the hypothalamus
Keeps the body on a roughly 24-hour clock but not perfectly and so still requires environmental cues (zeitgebers) to calibrate daily
Zeitgebers: Time Givers
Influences on timing of the circadian pacemaker
The period of the circadian pacemaker is not exactly 24 hours; organisms rely on external time cues to align their circadian system with the environment (entertainment).
"Zeitgebers" are "time-givers" and remind our bodies of what phase (awake/asleep) we should be at within a given environment.
In order of strength:
Light (most powerful)
Meals
Exercise
Caffeine
Larks and Owls
Humans probably evolved to sleep as groups and families, not couples
Larks- go to bed early and awaken early to guard the clan
Go to bed at 9pm, awaken at 5am
Owls- stay up late to guard the clan
Go to bed at 1am, awaken at 9am
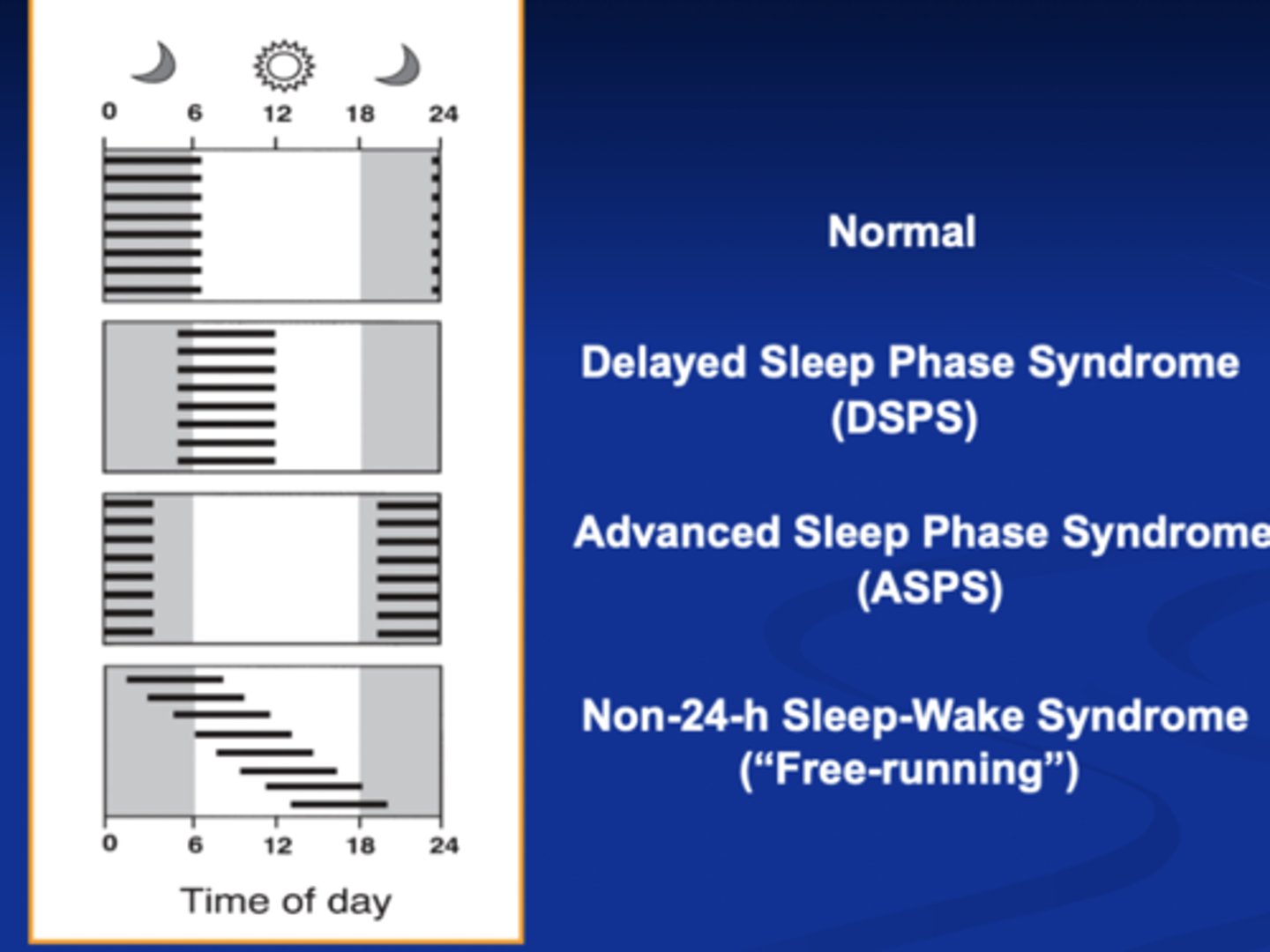
Sleep patterns (phase differences) in circadian rhythm disorders
Melatonin (function, site of origin)
A naturally occurring hormone found in animals, plants and microbes
Synthesized from tryptophan
Secreted into the blood by the pineal gland
Also found in high concentrations in bone marrow, lymphocytes, and epithelial cells (not regulated by the photoperiod in these cells)
Secreted in darkness
Inhibits secretion of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) from anterior pituitary gland
Kisspeptin
A protein that signals GnRH (gonadotropin releasing hormone) to start puberty
Kisspeptin is inhibited by melatonin
Children living on or near the equator see more sunlight, release less melatonin, and experience earlier puberty
Causes mild drowsiness and lowers core body temperature
Melatonin signals the start of sleep but isn't highly soporific
Production by the pineal gland is inhibited by light to the retina and permitted by darkness
Blue light (460-480 nm) suppresses melatonin
Wearing glasses that block blue light in the hours before bedtime may prevent melatonin loss (and help to adjust to an earlier bedtime, e.g., advance the clock)
Also has a role as an antioxidant,
Melatonin is high during the night and low during the day when under constant dim light conditions.
Melatonin with Age
Production of melatonin decreases with age
Adult melatonin production begins around 6-8 PM and peaks until 4 AM, stopping production around 5 AM
Adolescent melatonin production begins around 11 PM and peaks until 7 AM, stopping around 8 AM
Explains the adolescent delayed sleep phase, relative to adults
So waking an adolescent at 7 AM is like waking an adult at 4 AM
Jet lag
Hour a day, you want to keep to your home schedule +/- 1 hours each day
What we try to do: adjust your clock by about an hour a day
With light, caffeine, melatonin, and time givers
Trick your brain into thinking you are in between time (advance 2 hours ahead instead of 6)
Put your sunglasses/blue light glasses when you don't want light
Jet lag
Effects on the body
Generally transient and include:
Difficulty sleeping
Excessive daytime sleepiness
General malaise
Impaited performance
Gastrointestinal upset
Usually influence by direction of travel:
Slower adaptation when traveling east
Increases with the number of times zones crossed
Generally: people do better traveling west
Eastward Travel
The sleep cycle is shifted ahead (e.g., it's earlier where you arrive) or advanced
Usually, people sleep well the first night in the new locale (especially if they stay awake the day of arrival and sleep at the new locale's usual bedtime)
Probably due to Process S and a large sleep debt that accumulates, despite a misaligned Process C
Marked increase in stage 2 sleep on first night in new time zone; compensatory increase in REM several nights later
By the second night, however, Process S is less influential because much of the excess
Westward Travel
Changes in sleep quality after a phase delaying westward flight lasts fewer days for most people
Westward travelers show and increase in slow wave activity on the first night in the new time zone (showing an increase in sleep pressure, like eastward travelers)
This makes sense because most westward travelers stay awake during the flight and then stay awake until the usual new destination bedtime, so they've accumulated more sleep pressure Over the next few days, people often fall asleep easily but have late insomnia(early
East vs. west
In general, following phase changing travel, there is little trouble falling asleep the first night upon arrival because of an increase in sleep pressure (process S)
East
Usually people have more difficulty initiating sleep following eastward travel (a few days to a week) because they've been advanced
West
More difficulty maintaining sleep later
Core body temp
There is a small window related to the endogenous body temperature rhythm (as it approaches its daily minimum) during which time we may fall asleep and maintain sleep throughout the night
Misaligning CBT minimum with the light/dark cycle is a major target for jet lag desynchrony
Adjusting this, starts to drop an hour before habitual bedtime, we loose 1.8 degrees Fahrenheit on average
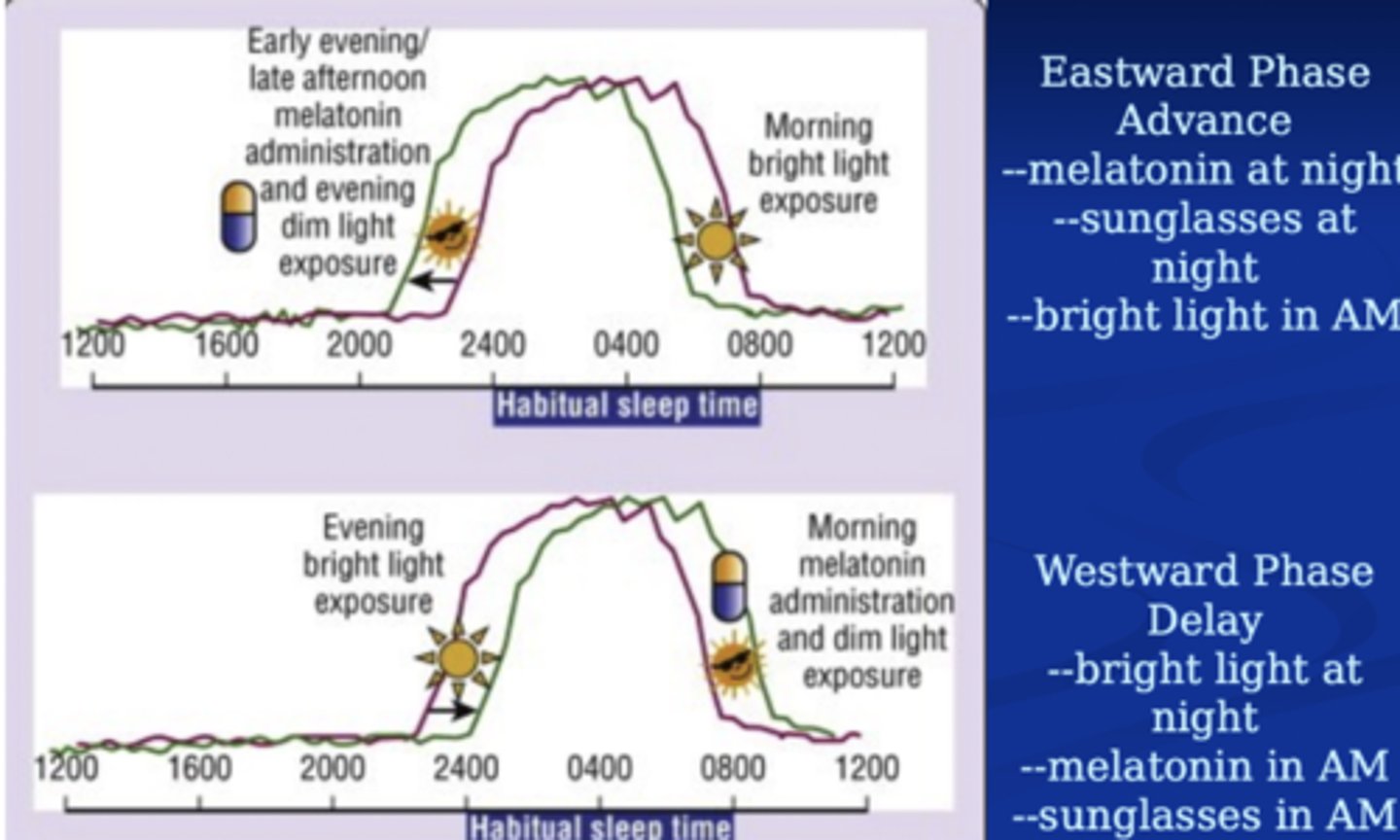
Role of bright light and melatonin
AM
Light advances the clock
Melatonin delays the clock
PM
Light delays the clock
Melatonin advances the clock
Light exposure during the Lag traveler's biological night (as would happen upon arrival in the new time zone) would cause a westward phase delay (opposite to what is needed for eastward travel). So, the eastward traveler should avoid bright light and/or wear sunglasses until after the habitual time of awakening in the home time zone; then the traveler should expose him/herself to bright light. Each day the time of exposure to bright light can be advanced by 1-2 hours.
When traveling west, the traveler should remain awake during the trip (using caffeine and naps strategically). Exposure to bright light should occur during the entire trip and until just before bedtime in the new time zone.
Treatment of jetlag
Short trips
One possibility is to keep to your usual schedule, in your home time zone
Or you can take sleeping pills for a few nights to put you on the new schedule
And/or you can use wake promoting agents, like modafinil and stimulants, to promote awakening in the new environment
Long Trips
Begin a few days prior to travel by timing bright light exposure progressively later in the day (for a westbound trip to delay cycle) or earlier in the morning (for an eastbound trip to advance cycle)
Light boxes can be used (containing light with wavelengths in the blue range)
Give melatonin in the early evening to phase advance the clock (going east) or in the morning to delay the clock (going west)
Doses of melatonin should be "circadian," not pharmacologic (e.g., 100 mcg every hour for 34 hours not 310 mg in a bolus dose for
Move towards the new time zone by 1-2 hours per day (whatever you can tolerate)
Use melatonin and dark glasses to manage light and circadian timing
Give a low dose of melatonin (300 - 500 mcg, or 0.5 mg) about 4 hours before desired bedtime
Give a bolus/large dose of melatonin (3-5 mg) an hour before bed if needed
School start times & their effects on kids
Damn Those Kentucky Drivers
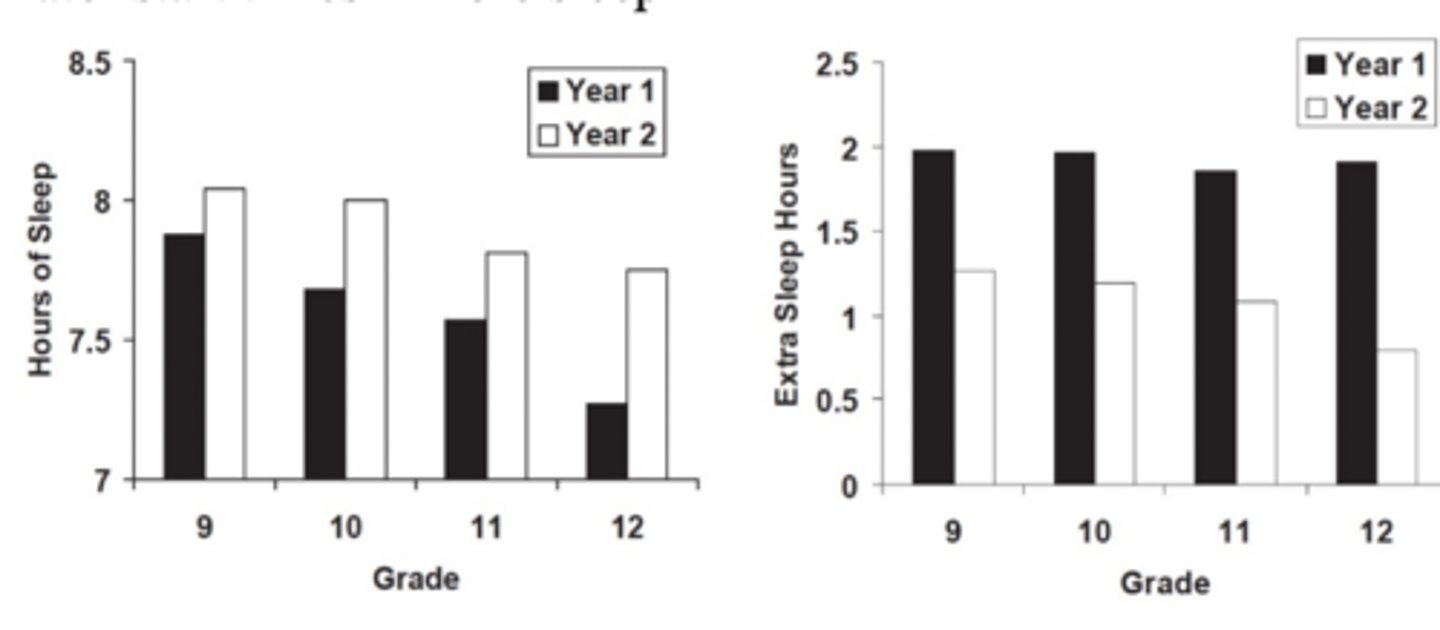
Nearly 10,000 students in one Kentucky County, grades 6 - 12, provided self-report on sleep habits (bed and awake times), naps, daytime functioning, and difficulty staying awake in 1998 & 1999.
During Year I, schools started at the usual time (7:30 AM for high school & 8 AM for middle school)
During Year II, schools started one hour later (8:30 AM for high school & 9 AM for middle school)
Auto accidents dropped by 16.5% in Year II Teen auto-accidents increased by 8% in Year II
Land of 10,000 Lakes
Edina and Minneapolis changed their school start times from:
7:15 AM to 8:40 AM (Minneapolis) 7:25 AM to 8:30 AM (Edina) Students tend to keep the same bedtime when start time is delayed, so kids do, in fact, get more sleep (by 1 hour in this study) when school start time is delayed
Findings included: Less EDS, less sleepy during homework, less tardiness, & better attendance
Top 10% of students increased SAT scores from 1288/1600 to 1500/1600
Later start times = more sleep
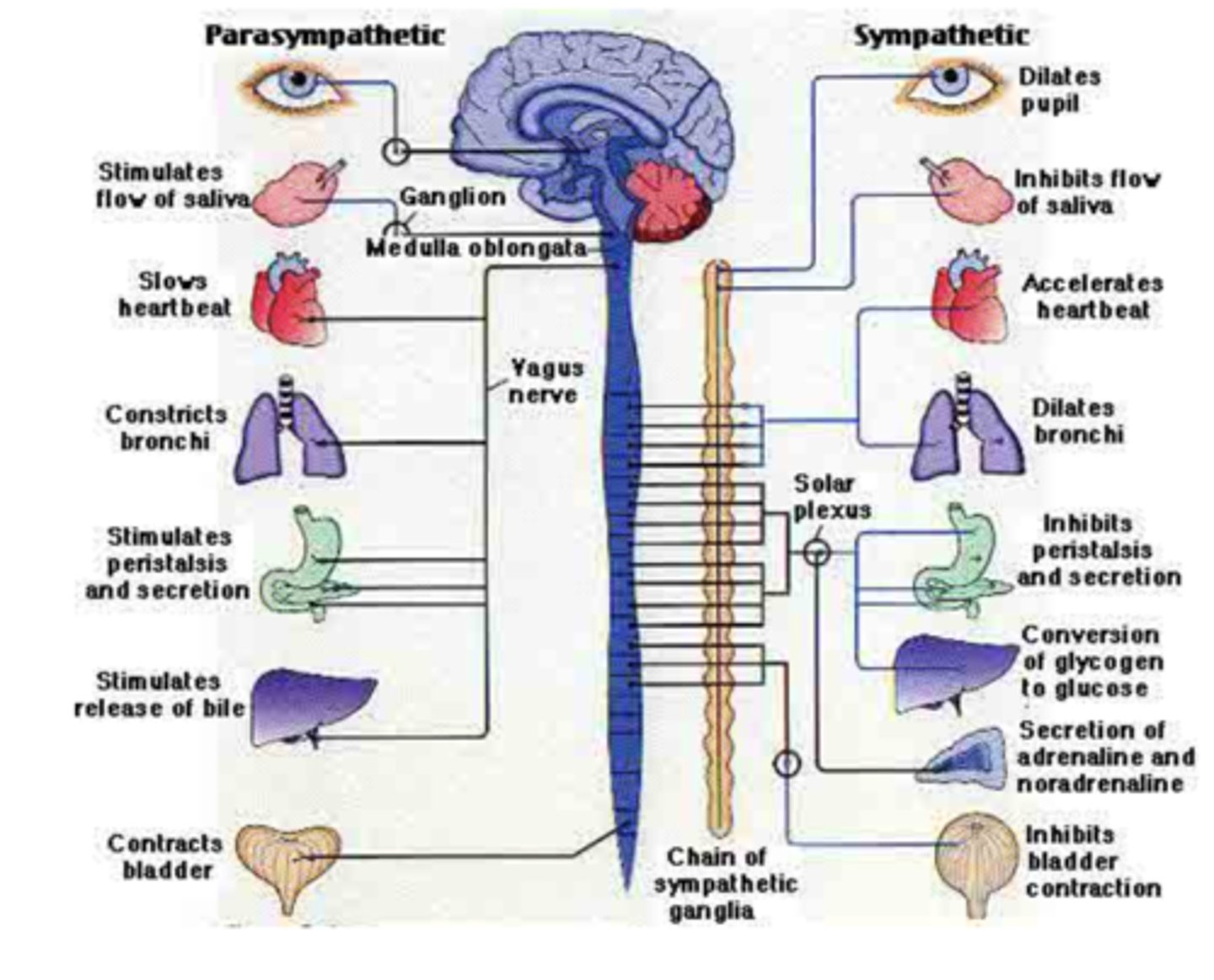
Autonomic Nervous System in sleep (cardiovascular, gastrointestinal, respiratory)
Largely involuntary system
Preserves homeostasis
Regulates multiple organ systems
Highly integrated system
Centers located throughout CNS
Two branches
Sympathetic Nervous System (SNS)
Parasympathetic Nervous System (PNS)
Sympathetic (fight-flight or freeze)and parasympathetic (rest and digest)
Pulling an all-nighter, being exhausted at 2am but energy comes back at 10am
ANS is physiologically important during:
Transition from wake to sleep
Normal architecture changes associated with the sleep cycle (non-REM, SWS, REM)
Maintenance of
Blood pressure (CV events)
Gastric acid secretion (GERD)
Renal function
Breathing (OSA & asthma)
Endocrinology of sleep
Hormone release
Process C vs. S
Hormone release is influenced by:
Circadian Rhythm (Process C)
Sleep-Wake Homeostasis (Process S)
Environmental factors, such as postural changes, stress, food intake and exercise also modulate hormone release
You need to sleep to grow healthy
Growth hormone and Plasma Prolactin is under process S
Process S is sleep debt
ProcessC is circadian rhythm
Cortisol is under process C
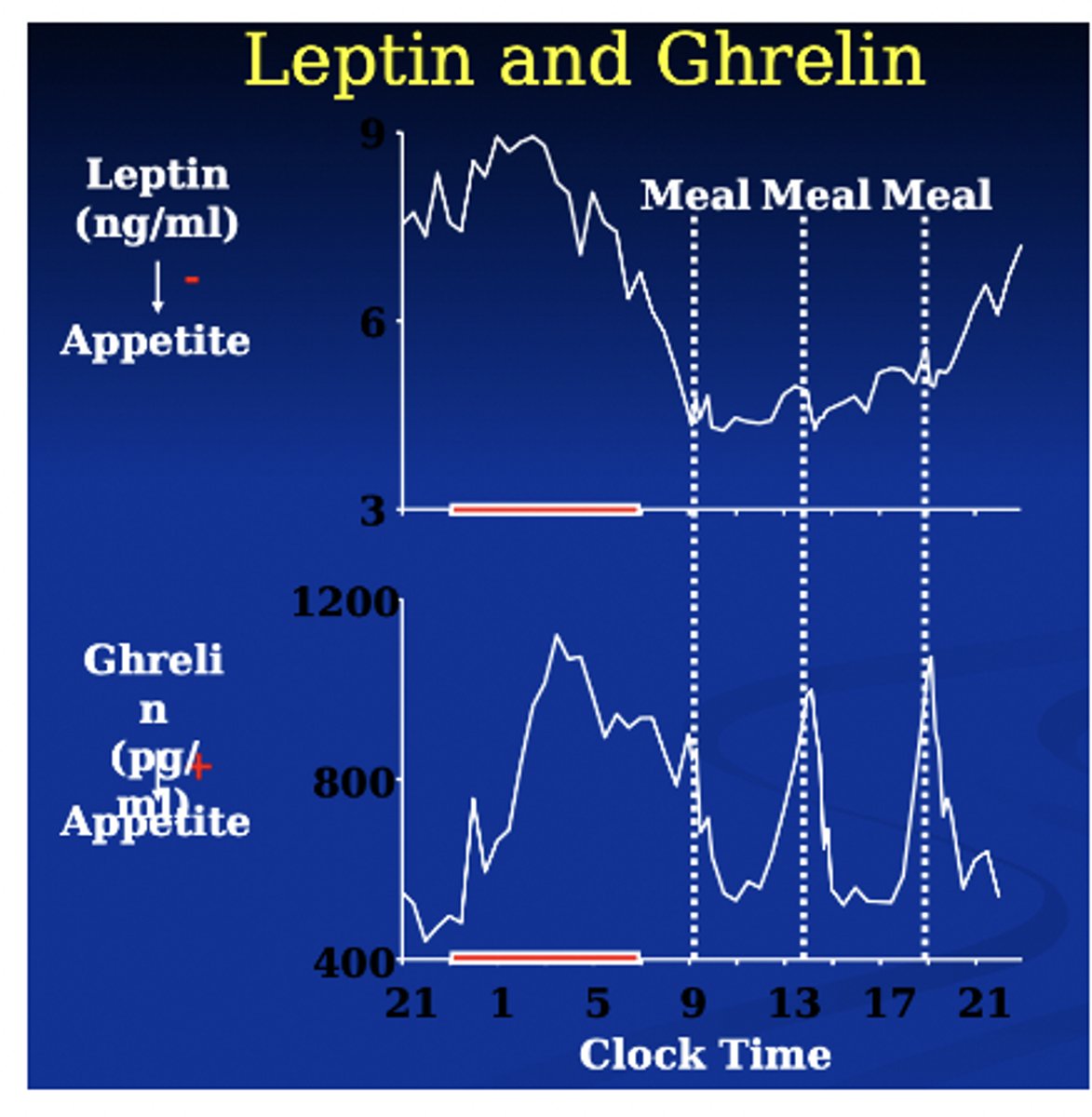
Grehlin & leptin
Leptin is high throughout the night
Leptin → decrease in appetite
Ghrelin → increase in appetite
Immunology
Chronic sleep loss is associated with obesity, diabetes, CV disease, HTN
All are associated with inflammatory processes
Sleep deprivation in some lab animals leads to septicemia and death
Sleep is dramatically altered during infection
Human infection with influenza or rhinovirus leads to increase SWS
Bacteria, virus, yeast, and protozoan infections alter sleep
Sleep and thermoregulation/temperature effects
When we sleep our body temperature decreases
Sleep onset is associated with a dramatic reorganization of thermoregulatory control
Core Body Temperature (CBT) falls at sleep onset, accompanied by heat loss mechanisms (vasodilation & sweating)
Fall in CBT and slowed metabolism presumably contribute to an energy conservation function of sleep
Thermoregulation is less responsive during sleep (more responsive in NREM than REM)
In general sleep is best in humans at night when the CBT is low and melatonin is high
Sleep onset latency is minimized if sleep is initiated about 5 hours before minimum CBT
Electric blankets that increase CBT slightly cause increased nocturnal awakenings
Spicy meal increase in CBT by 0.2 C led to a decrease in SWS
There is some evidence that soporifics induce sleep in part by increasing peripheral body temp and decreasing core (BZDs & melatonin)
Caffeine has the opposite effect by increasing CBT
Sleep hygiene Definition and Typical sleep hygiene measures
A series of recommendations and practices designed to improve sleep quality, quantity, and daytime alertness, including the typical measures:
Environmental (e.g., temp, noise, light)
Scheduling (e.g., sleep/wake schedule)
Practices (e.g., bedtime routine)
Physiological (e.g., exercise, meal timing, caffeine)
Often advised by healthcare practitioners, although the evidence-base is not significant for most of the recommendations
Validity of sleep hygiene data
It's difficult to find any two studies with an identical set of recommendations
Most of the data supporting specific behaviors comes from studies of normal adult sleepers (not insomniacs)
American Academy of Sleep Medicine has found insufficient evidence to use sleep hygiene as a stand-alone treatment for insomnia (1999)
Research studies often use sleep hygiene as an "active placebo" making it difficult to determine its potential as a stand alone treatment
Almost all of our sleep hygiene data comes from studies of adults
The vast majority of the data appears relevant to older adolescents, college age, and emerging adults
You can extrapolate to children...or not
Caffeine Effects
Caffeine also causes increased neuron firing indirectly via the hypothalamus and pituitary gland
The hypothalamus senses that adenosine is blocked and (probably) thinks that some sort of emergency is happening (b/c the brain isn't relaxing as usual); it sends a message to the pituitary gland
The pituitary tells the adrenal glands to release adrenaline (epinephrine) and cortisol (a stress hormone), resulting in "fight or flight"
90% of americans consume caffeine in one form or another every day
More than half of americans consume more than 300 mg/day
The FDA and AMA consider 400 mg/day the upper limit of a moderate daily dose
20 - 30% of Americans consume more than 600 mg/day
Stimulates us, blocks adenosine receptors
FDA recommended limit of 400mg
If it sits in the water and brews longer then it will be stronger and have more caffeine
Caffeine Physiology
To a nerve cell, caffeine looks like adenosine
Caffeine competitively binds to the adenosine receptor, but unlike adenosine, caffeine doesn't slow down the brainl it just blocks the receptor
So instead of slowing down, the nerve cells keep going strong
Caffeine also causes the brain's blood vessels to constrict b/c they block adenosine's ability to open them up
Caffeine also inhibits acetylcholinesterase, so the duration of acetylcholine, another NT, is increased in nicotinic and muscarinic receptors in the CNS
How does caffeine contribute to wakefulness?
- Blocks. adenosine
- Fight or flight
- Brain isn't relaxed as usual
Alcohol (effects on sleep)
Alcohol/drugs → Alters sleep architecture, causes a block of stage 1 and rem
Alcohol increases NREM and reduces REM and Stage 1 in the first sleep cycles
Tobacco (effects on sleep)
Nicotine → Alters sleep architecture, decrease in restful sleep
Tobacco increases sleep latency and stage one sleep decreasing SWS, restful sleep and sleep time
Cigarette smokers have many sleep related complaints
PSG study of 6400 subjects found increased sleep latency (5.4 min), less total sleep time (14 min), more Stage 1 sleep, and less Slow Wave Sleep
No differences in sleep architecture between former and non-smokers
Analysis of sleep EEGs found less delta power (SWS) and higher alpha power
Nicotine is thought to exert its strongest effects on sleep architecture at the beginning of sleep but then exert effects of nicotine withdrawal later in sleep epoch
Nicotine
Dose dependent- - lower doses tend to stimulate REM and higher doses suppress REM
Rebound upon discontinuation increases wake time and decreases Stage 3
Withdrawal begins 6 - 12 hours after last use and can last 3 weeks
MJ (effects on sleep)
Delta-9-tetrahydrocannabinol (THC), the main active ingredient in MJ that gets you "high", has effects on sleep that has been known about since the '70s
THC is known to decrease both SWS and REM
Regular users generally report fewer dreams than occasional or non users
When regular users stop using MJ, they often report a REM rebound effect and a period of vivid dreaming
Implications?
THC decreases SWS and REM, less dreaming
Melatonin & ways to use it (sleep onset vs. chronotype adjustment)
Adjust the CBT set-point, allowing more blood flow to distal areas of the body and cooling of the core
sleep-promoting
Napping, Timing
When to Nap
Take advantage of circadian "windows of opportunity"- e.g., when clock dependent alerting is low and melatonin is high
2 AM - 5 AM (corresponds to lowest daily CBT)
2 PM - 5 PM (corresponds to midday melatonin surge)
But if you cannot, nap when you can
Great, adds up, encouraged,
No nap vs 5,10, 20 and 30 min naps, 24 young adults, good sleepers, not regular nappers held to 5 hours sleep for one night then given a nap opportunity at 3pm with 3-hours of post nap testing
Strategic napping
Preventative (before an activity that will make you tired - e.g., a long evening drive, shift work, physicians on night float, etc.)
Operational (on the job)
Short naps (20 - 30 minutes) avoid sleep inertia (e.g., the grogginess that you feel upon awakening from deep sleep)
Power naps (20 min Stage 2 nap)
Caffeine nap
Long naps (30 - 180 minutes) are more rejuvenating but also are more likely to interfere with the sleep cycle
Napping Benefits
Numerous studies confirm that daytime naps are sufficient to induce performance improvements in declarative and procedural memory
45 minute early afternoon nap, dominated by Stage 2 (slight SWS/REM), resulted in improvements in procedural (not declarative) memory (Backhaus & Junghanns, 2006)
Napping may benefit cardiovascular health
A 6 year study of greek men found that those who napped at least 3x/ week had a 37% reduction in CV related deaths (Naska et al, 2007)
Naps may reduce stress and BP (Zaregarizi, 2007)
These studies are possibly confounded
Bedtime snacks
A small snack before bed has been shown to promote sleep by keeping hunger at bay
The most sleep promoting foods are rich in tryptophan, a precursor of serotonin & melatonin, which induce sedation
Warm milk, turkey, and chamomile tea are all high in tryptophan
Good but not too close to bedtime
Exercise with sleep
Data are mixed
Little evidence that morning exercise affects sleep
Physical activity can increase sleep latency on the MSLT
Exercise later in the day may increase the depth of sleep, demonstrated by increase in SWS and total sleep time
But exercise just before bed may increase sleep latency
And research suggests that core body temp may be what matters, not exercise
Not within 4 hours of bedtime
Teaching infants/children to sleep through the night (techniques)
Extinctions
Positive Bedtime routines
Faded bedtime
Bedtime pass
Reinforcement
Sleep fairy
Alternative treatments
Extinction (unmodified, graduated, with parental presence)
Eliminate the associations
modifying environment of infant to help them put themselves to sleep
- establish regular sleep and wake time
- Create a relaxing bedtime ritual
Unmodified extinction
Child is placed in bed while any sleep interfering behaviors are ignored until morning
Ignoring is discontinued if child is ill, in danger, or becoming destructive
Graduated extinction
The extinction procedure is combined with checking procedure that is faded over time
Parents wait for progressively longer periods of time prior to responding to the child
Parents decrease the time they spend with the child over time
Extinction with parental presence
The parent is instructed to sleep in the same room with their child, but in a different bed, ignoring the child's crying or attempts to get out of bed
This sleep arrangement continues for 1 week, then the parent returns to sleeping in a separate room
This approach appears to reduce nighttime awakenings while limiting the post-extinction response burst
Positive Bedtime routines
Same every night
Last portion in sleeping environment
Short and sweet, heading in one direction
Consistent bedtime environment
Faded bedtime
The child's bedtime is temporarily delayed approximately 30 min later than the typical sleep onset time (or the time he usually falls asleep)
Remove child from bed and keep him awake for 30-60 min if he does not fall asleep quickly
Once child begins to fall asleep more quickly, the bedtime is systematically faded 30 min earlier over successive night until the bedtime goal is reached
Reminds you of?
Sleep restriction
Bedtime pass
Bedtime pass is a modified extinction for children who exhibit bedtime resistance, including calling our leaving the room after bedtime
Provide child a card or "free pass" exchangeable for one permitted trip out of their room.
After the child uses the pass parents are instructed to ignore additional requests or crying
Reinforcement
Caregivers first identify a specific target behavior
Achieving the target allows a child to get a reward
Sleep fairy
Combines the use of a social story with tangible rewards
Social story consists of reading the tale of the "Sleep Fairy" who leaves rewards under the child's pillow contingent upon appropriate compatible behaviors
Alternative treatments for helping a child sleep on their own
Massage helps to relax and reduce stress. There is some evidence that massage was more effective than rocking
Chiropractic manipulations are less studied.
Hypnosis and self-hypnosis
Definition of a dream
No universally accepted definition
Almost all definitions include 3 features:
A dream is "conscious"
A dream is accessible to recall
A dream occurs during sleep
"A train of thought & images passing through the mind in sleep" (Funk & Wagnall)
"A vivid, complex, hallucinatory experience generally accepted as real by the dreamer, and having mostly logical progression in time" (Dement)
Methods to improve dream recall
Whatever has citicoline is good to remember dreams, not weed
To improve dream recall:
Make an effort
Keep a dream log or recorder by the bed
Keep an object in the room to remind you to log
Give the dream a "tag" or title
Write down or record as much as you can first, analyze after
Use the present tense in recording your dream
(helps with recall; & reverting to past tense suggests discomfort)
Highlight the feelings, action, and symbols
Avoid saying you do not remember
Medications to Improve Dream Recall (& Lucidity?):
Vitamin B6 (250mg?); for recall
Galantamine (4-8mg); for recall
Choline(250-500 mg+?); for recall
Silene Capensis/ African Dream Root (brewed into a tea); for lucid dreaming
Mugwort (1 punch dried herb to 1 pint boiling water, 5-10 minutes); for dream recall
Calea Zacatechichi (tea or capsules); for bth
Dream recall
Why is it so difficult?
Areas of the brain involved in forming memories (like the frontal lobe) are quiet and chemicals important for encoding memories (like certain neurotransmitters) are reduced
Plus, maybe we don't "want" to remember our dreams
Not super trustworthy - state change, time delay, visual dreams hard to describe, self censorship
Could be improved thru using dream logs, highlighting feelings/actions
Dream meds - vitamin b6, galantamine, choline, silene capensis, mugwort, calea zacatechichi
Dream Recall Problems
What might dream reports be less than 100% trustworthy?
State change (reporting a sleep experience when awake)
Time delay (dream reports are obtained after the experience, which can lead to forgetting and interference)
Visual imagery may be difficult to verbally describe
Censorship (we may not report embarrassing, violent, sexual and aggressive material)
Lucid dreaming
Lucid Dreaming: a dream in which the dreamer is aware he/she is dreaming
Seems real, aware you are dreaming
This phenomena was the subject of many books in the 20th century, which contained not only personal accounts of lucid dreaming, but also tools for lucid dream work.
Despite the cultural fascination with lucid dreaming, the phenomena remained largely unstudied by scientists
Despite the seeming prevalence of this phenomena, scientists are still unsure what structure within the brain induces lucid dreaming
Lucid dreaming has a tendency to occur later at night, when most REM occurs
Unlike regular dreams, in which the dreamer is largely led by the dream, in lucid dreams, the dreamer is able to take control of the dream content
Many lucid dreamers report that the dream possesses qualities which seem to be enhanced beyond the usual dream experience
False Awakening: when the dreamer thinks he/she is awake but is, in fact, still dreaming
Physiologic effects during dream sleep
NREM vs. REM
Sexual content
Awakening is often disorienting - sleep inertia is a factor
Mental activity occurs during sleep
Dreams do occur in NREM but harder to recall, can be affected by sounds
Sleep talking / sleep terrors associated with NREM parasomnias
Many of the physiological events in REM replicate what the body would do with an identical experience in the real world
Evidence suggests that dreams can occur in NREM and do not simply reflect recall of earlier REM sleep dreams:
It is possible to influence dream content by sounds delivered in NREM (e.g., phone calls, discussions, etc.)
Some NREM parasomnias (sleep talking & sleep terrors) correspond to reported dream experiences
Full dreams are sometimes reported upon awakening from NREM only (before the first REM period or after NREM naps)
Reports obtained upon awakening from NREM (especially deep sleep) are hard to evaluate because of the disorientation associated with sleep inertia
It is now believed that mental activity occurs throughout sleep
Much of NREM "dreaming" is considered sleep mentation
Abstract thoughts, fragmentary images, and isolated feelings
Dreams Senses
Unless blind, all dreams are visual
2/3 of dreams contain sounds
8% of dreams contain touch
All other senses occur in only 4% of dreams
Pain is extremely rare in dreams
One's own death almost never occurs in dreams
Depression/negative emotion/amygdala and dreaming
Negative dream content is typical of depression
More frequent nightmares
Increased hostility
More mundane, trivial, masochistic, vivid and disturbing content
Depression also induces reduced dream recall frequency and reduced length of dream reports
Negative emotion in depression and amygdala is more activated and more rem as well as negative dreams
Negative emotion in REM
The amygdala (aka "threat hub") is highly activated in REM
The amygdala is an area of the brain that is engaged when unpleasant emotions like fear or aggression are felt
This may help to explain the preponderance of negative emotion in dreams
Note: People with MDD experience a greater amount of REM and sooner in the sleep cycle, which may increase the proportion of negative emotion in sleep and contribute to their depression
REM Sleep Decreases Amygdala Activity
Two groups of individuals (n = 34) are shown 150 emotionally charged photos, which they rate for emotional intensity
The group that slept showed lower amygdala reactivity in fMRI when shown the images at Time 2
Those who slept also showed an increase in "top down" control (interconnectivity) of the amygdala from the vmPFC
Those who slept also demonstrated lower emotional intensity ratings when viewing the images at Time 2
Those who didn't sleep also showed hyperactive striatal activity (e.g., nucleus accumbens) or a greater interest in rewards (also with less prefrontal control)
PTSD/prazosin
Prazosin
Higher than normal levels of Noradrenaline (NA) are found in the CSF of people with PTSD and correlates to greater symptoms of PTSD
These high levels of NA may block people with PTSD from entering and maintaining REM
Prazosin treats HTN by reducing NA in the brain
Prazosin is often helpful for reducing nightmares in PTSD
Reduction in nightmares can reduce PTSD
When traumatized, norepinephrine is increased, prazosin decreases this
Nightmares
Some suggest that nightmares and bad dreams are necessary rehearsals left over from evolution to help us prepare for threats that may come our way
Wild animals, fire, etc.
These "primitive" dreams still occur in children
In adults, the modern version of these events is losing your wallet or having an auto accident
Dementia dreams are often "primitive" (loss of cortical functions)
AIM model (Hobson)
Consciousness is determined by:
Activation- total and regional brain activity levels
Input- activation generated internally and externally
Modulation-ratio of aminergic to cholinergic neuromodulation
With cholinergic activity on in REM, the limbic system is activated without the prefrontal cortex turned on to work out logical associations
Dreams originate "bottom up" from activation of the sensory cortex by the brainstem PGO waves, which are "interpreted" by higher order brain structures
Dreaming is the brain's best attempt at interpreting activating signals in a coherent manner, and contents of individual dreams
AIM Theory
Activated brain areas in REM include Theory) awareness, eye movements, instincts, vestibular sensation (body in space), memory consolidation, and emotions
Areas involved in the production of motor movements and processing of sensory information are also activated
Areas involved in primary reception of sensory info are not active; nor are dorsolateral prefrontal cortex areas
Thus, the difference between dreaming and wakefulness is where the "activation" comes from
External when awake internal when in REM
Consciousness, helps us understand dream sleep, the difference between wake and sleep consciousness
PGO waves
Ponto-geniculo-occipital waves
Originate in the pons, lateral geniculate nucleus (thalamus), and occipital cortex
Start in the pons and spread to the lateral geniculate nucleus (which resides in the thalamus) and then end up in the primary visual cortex of the occipital lobe
These are prominent just before REM
Waves that start right before rem, start in the pons and go up, gatekeeper
Neurochemical activity
- Dreams have no function but do have coherence and meaning
- Dreams are based upon stored memory representation
-Dreaming is due to complex neurochemical mixture of acetylcholine and dopamine (and serotonin, norepinephrine, and histamine are absent)
Dreams are "top down"
Freud versus Jung
difference between dreams
Freud- symbolic, unconscious, they are real, have meaning, what is going on with us which is hidden, latent and manifest content, dream condenses in many forms
The dream is a symbolic representation of some other meaning
Free association is used to uncover hidden meaning
Repression
"What is the dream repressing? What is it covering up?"
Sex was the primaty dtive underlying dream content
Dreams are a representation of unconscious conflict that psychoanalysis can resolve
Jung- dreams are real, were explored by amplifying, tell the dream and get deeper and deeper into the dream
The dream itself is factual
Amplification is used to identify the facts within the frame
Creative approach to interpretation
"What is this dream telling me? What is it for?"
Saw many possible explainations
Dreams reveal key aspects of our defended selves that must be integrated to make us whole
Insomnia Definition
Typical symptoms
Insomnia is characterized by subjective complaints about dissatisfaction with sleep quality or duration, difficulty falling asleep at bedtime, waking up in the middle of the night or too early in the morning, or non-restorative sleep
Most common single symptom of insomnia are having multiple awakenings or unrefreshing sleep
Insomnia (DSM-5)
Difficulties initiating sleep (in children without caregiver intervention)
Difficulties maintaining sleep characterized by frequent awakening or problems returning to sleep (in children difficulties to return to sleep without caregiver intervention)
At least 3 nights per week, for at least 3 months
Coexisting mental disorders and medical conditions do not adequately explain the complaint of insomnia
Typical Symptoms
-EDS, fatigue, low energy, bad move, cognitive impairment- difficulty functioning- Difficulties initiating sleep
flip flop switch
Insomnia Comorbidities
Adults with insomnia
> 5x comorbid anxiety or depression
>2x comorbid congestive heart failure
Compared those without insomnia (US National Health Interview Survey, 2002)
>3x comorbid anxiety, mood, impulse-control or substance use
(US National Comorbidity Survey, 2006)
Strong correlation between chronic pain and insomnia
Tang et al (2007) found that 53% of chronic pain patients suffered insomnia
Insomnia accompanies medical disorders in approx. 35% of cases
Insomnia is also causally associated with
Hypertension (high blood pressure)
Sensitivity to pain
Altered metabolic function
Insulin resistance, a condition associated with diabetes mellitus
Obesity
Cardiovascular morbidity
Higher level of physiological arousal
Elevated heart rate
Insomnia
Predisposing factors
before insomnia
personality/genetic
Sleep-wake cycle
Circadian rhythm
Coping mechanisms
Age
gender
Insomnia
Precipitating factors
life rating
illness
a loss
Situational
Environmental
Medical
Psychiatric
Medications
Insomnia
Perpetuating factors
maintaining factors, adressed in the CBT-I
Conditioning (negative)
Substance abuse
Performance anxiety
Poor sleep hygiene
excessive napping
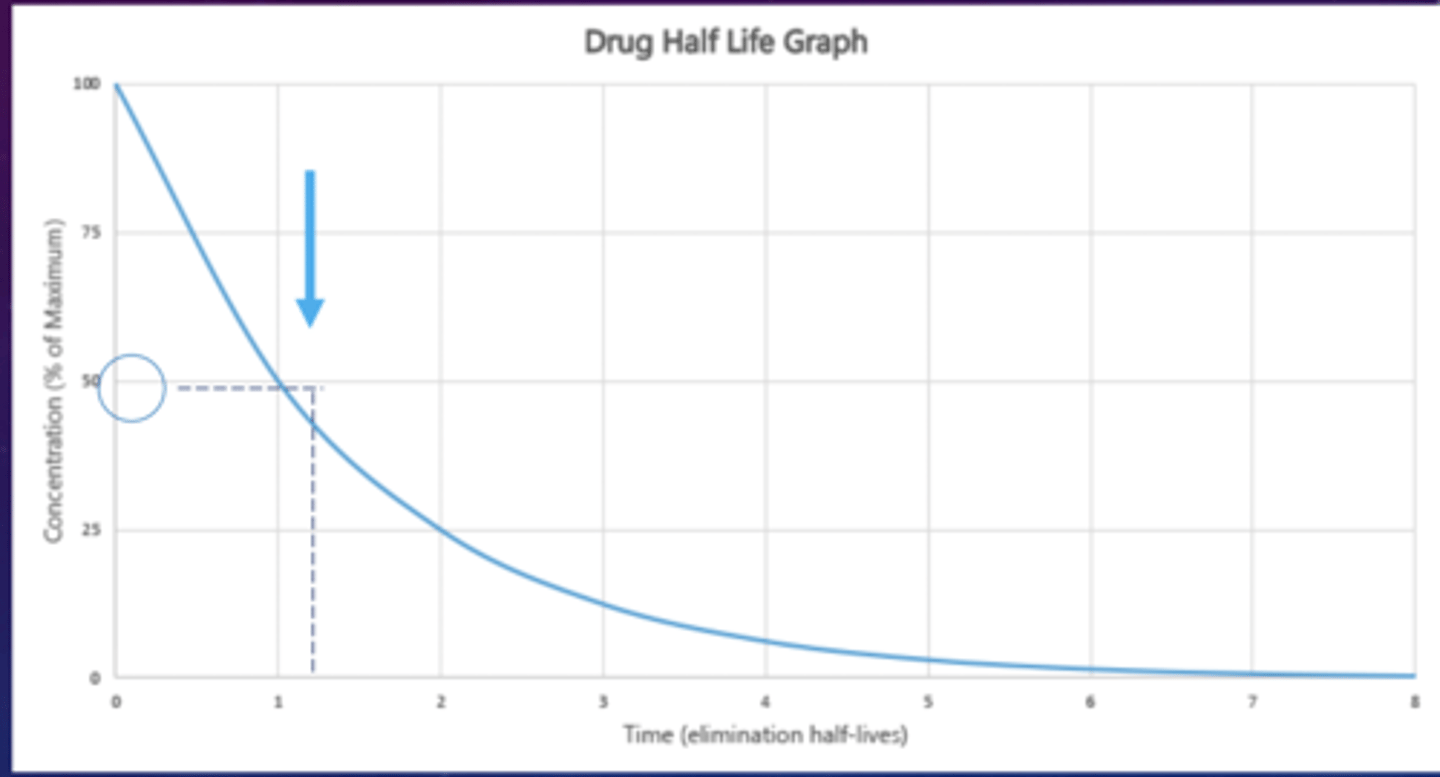
half life
the process in which our body eliminates any medicine or drug
how long does it take until your body contains half of the dose in your body
Treatment of insomnia
Use of medication (no names required)
How medications work
Benzodiazepine receptor agonists (= increase GABA activity)
"non-benzodiazepine sleeping pills" or "Z drugs":
They bind to GABA receptor in the same area benzodiazepines act even if they are structurally different
Controlled substance but with less potential for abuse
They do not suppress SWS as much as Benzodiazepine
Sleeping pills induce a little more sleep, decrease sleep latency, people feel more rested because the medicines makes it difficult for memory to be encoded, so people forget they ever awoke in the night even though they did
Typical medication side effects
Potential adverse effects:
Residual effects
Confusion
Dry mouth
Constipation
Blurred vision
Difficulties urinating
- abuse
- lethal in overdose if in combination with other medication
- respiratory depressant
- suppress SWS
- sleep paralysis
- hallucinations
- decrease sleep latency
- anterograde amnesia
Treatment of insomnia
CBT-I
Cognitive Behavioral Therapy for Insomnia CBT-I:
Education about sleep
Sleep Hygiene
Sleep Cycles
Sleep Duration
Stimulus Control
Sleep Restriction
Cognitive Therapy
Relaxation techniques
Biofeedback
Visualization
Start with their sleep goals
E.g., reducing the amount of time awake in bed (as opposed to the number of hours asleep)
Validate that the behavioral changes they're about to start aren't easy and will be difficult
E.g., they must be very resilient to have come this far in life sleeping this poorly
Roll with resistance (e.g., people don't understand how much you're suffering)
Provide sleep education and start sleep logs
Photograph the sleep environment. Identify pros and cons
CBT-I stimulus control therapy
Assumes that there is a learned association between wakefulness and the bedroom
To break the cycle, the patient must not spend time wide awake in the bedroom
Go to bed only when sleepy
Do not use the bedroom for sleep-incompatible activities
Leave the bedroom if awake for more than 20 minutes
Return to bed only when sleepy
Do not nap during the day
Arise at the same time every morning
Not only use the bed only for sleep but also sleep only in bed in order to associate the bed only with sleep
Relaxing bedtime routine
No clock watching overnight
CBT-I sleep restriction
The basis of sleep restriction therapy is that, regardless of initial reasons for insomnia, one of the perpetuating factors for insomnia is staying in bed for a much longer time than one sleeps each night.
Sleep restriction serves to
Re-educate the body to sleep in a consolidated fashion
Increase propensity to sleep by increasing homeostatic sleep drive with partial sleep deprivation
Systematic reduction of time in bed to the amount of total sleep time from sleep log data
Behavioral treatments for pediatric insomnia
- consistent bed time
- sleep associations
- self-soothing skills
- bedtime fading
Unmodified extinction - ignored until morning
Graduated extinction - checking procedure faded over time
Extinction with parental presence - parent sleeps in same room, but different bed
Scheduled awakenings - parent awakens child prior to expected awakening times and gradually delayed
Delayed Sleep Phase Syndrome
Definition
Sleep disruption due to a misalignment between the endogenous circadian rhythm and the sleep-wake schedule required
The sleep disruption leads to excessive sleepiness or insomnia, or both
Delayed sleep phase type: A pattern of delayed sleep onset and awakening times, with an inability to fall asleep and awaken at a desired or conventionally acceptable earlier time
advanced sleep phase syndrome
wake up early go to bed early
a 4-hour advance in rhythms of sleep and temperature cycles, apparently caused by a mutation of a gene (per2) involved in the rhythmicity of neurons of the SCN
Delayed Sleep Phase Syndrome
Causes, prevalence and risk factors
Often corresponds with natural wake up times
Conforming to external social requirements can lead to sleep restriction
High energy, and alertness in evening
Difficulties falling asleep earlier, fogginess / low mood
Unsupervised time for adolescents (video games / TV)
Different effect of light on circadian rhythms depending on core body temperature
Body temp fluctuations / effect of light changes are in sync
Melatonin secretion is regulated by circadian rhythm, and light during night suppresses melatonin
Circadian rhythms misalignment
Difficulties falling asleep when expected
Forbidden zone (evening peak of alertness)
No daytime symptoms when allowed to sleep according to preference
Worsened by incorrect use of light and/or use of evening electronics
Majority of adolescents suffer from delayed sleep phase rather than insomnia
treatments for delayed sleep phase syndrome
Light therapy
Melatonin
Sleep phase chronotherapy
Circadian rhythm disruption treatment - melatonin timings before expected sleep time
2-4 hours before desired bedtime of melatonin dose
Light therapy
Light exposure in AM after lowest point of CBT
Light after latest wakeup time
30 minutes of light maintenance dose at wakeup time
Sleep phase chronotherapy
Moving bedtime - rising time later each day, stopping when sleep is on normal schedule
Definition of parasomnia
disruption of sleep
loss of REM atonia, act out dreams while dreaming
Undesirable physical or cognitive experiences occurring during specific sleep stages or during the transitions between awake and asleep states
Undesirable physical / cognitive experiences that occur during sleep stages or during sleep wake transition
Abnormal behaviors during sleep such as sleep terrors, nightmares, sleepwalking, and enuresis.
Nightmares occur during REM sleep.
Sleep terrors occur during stages 3&4 (delta sleep).
Sleepwalking is associated with stage 3 or 4 delta sleep in the first third of the night and with REM later in the night.
Childhood enuresis typically takes place within 3 to 4 hours of bedtime but is not limited to particular stages of sleep.
NREM parasomnias (or Disorders of Arousal DOA)
Disorders of arousal during NREM sleep
Sleep Terrors
Sleepwalking or Somnambulism(not actually dreaming)
Confusional Arousals
Sleep Related Eating Disorder
Sexsomnia
Behavioral and medication treatments for NREM parasomnia
Psychosocial Interventions
Repeat of a violent episode is rare
Family/patient education
Treat any primary disorders (SDB, RLS)
Avoid possible precipitants
Avoid sleep disruptions
Loud noises, limit evening oral fluid intake
Safeguard the home
Movement sensors, locks on windows, remove potentially lethal objects, etc.
Enforce afternoon naps (with Sleep Terrors)
Plan for scheduled awakenings
Medication
Risk factors NREM parasomnias (or Disorders of Arousal DOA)
Inadequate sleep
Irregular sleep schedule Fever, illness Sleeping with a full bladder
Sleeping in a new/unfamiliar environment Sleeping in a noisy environment (e.g., TV on) Stress, anxiety Medications (e.g., chloral hydrate, LiCO3, clonidine, TCAs)
Primary sleep disorders (e.g., OSA, PLMD, RLS) S
leep disruption (e.g., asthma, GERD, ear infection, pain, caffeine, EtOH, congestion)
Enuresis (bedwetting) and its treatments
- caused by primary enuresis
- occurs in kids
- nocturnal enuresis is associated with poor self image, diminished achievement in school, significant time by families compensating for the symptoms
Enuresis treatment
education
discontinue all caffeine
restrict late-night fluid intake
- afternoon nap
- brief wakening for the bathroom at midnight
- pelvic and bladder training
Nighttime fears
Animals, fictitious characters (e.g., witches & monsters), being kidnapped, or burglars
Anxiety is believed to predispose children to parasomnias and nightmares
Occasional nightmares occur in 80% of children
15% report frequent nightmares (>1/month)
69% of children report that the content of their nightmares is influenced by frightening material viewed on TV or at the movies
Positive self talk and coping thoughts
Desensitization and reinforcement
Relaxation
Deep breathing
Progressive muscle relaxation
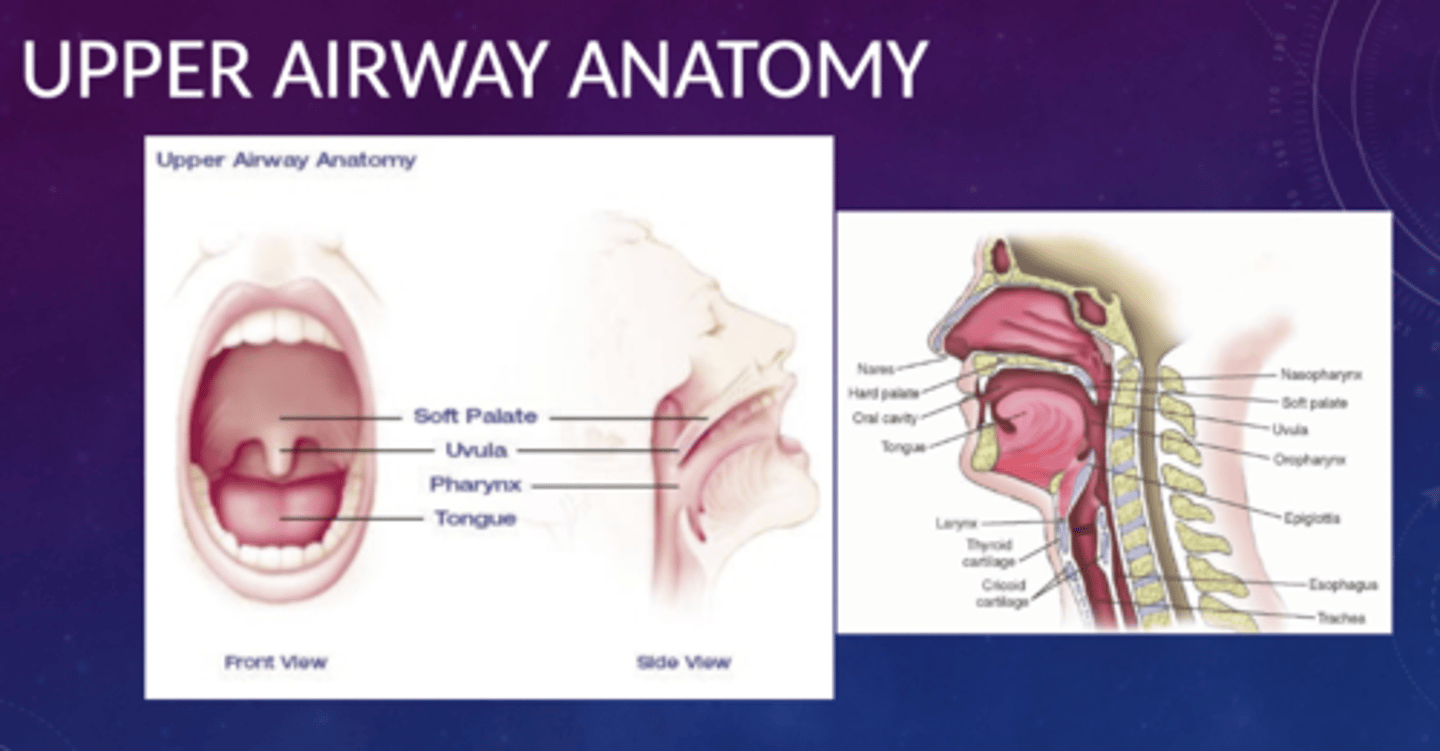
Obstructive Sleep Apnea Definition
Obstructive events refer to moments in which there is cessation of airflow due to obstruction in the upper airway.
During these episodes, the muscles that promote breathing (the diaphragm and chest wall musculature) continue to work.
The obstruction is caused by the throat muscles relaxing, eventually closing the throat for short periods
Apneas can lead to moments of asphyxia (O2 decreases and CO2 increases)
During apneas, we awaken to restart breathing
Episodes can happen multiple times per hour through the sleep period
People are generally unaware of these occurrences
2 - 8% of the population suffer from OSA
Anatomy of the throat and pharynx (OSA)
Risk factors of OSA
Obesity (BMI >30), neck circumference >17" male, 16" female
Airway conformation
Gender: M>F
Menopause • Older age
Nasal problems (deviated septum, nasal polyps)
Family history of OSA/snoring
Consumption of alcohol or sedatives prior to bedtime
Exposure to cigarette smoking
Craniofacial abnormalities
Sleeping supine
Comorbid conditions (e.g., neuromuscular disorders)
Symptoms of OSA
EDS (Excessive Daytime Sleepiness)
Fatigue (not necessarily sleepiness)
Unrefreshing sleep ("I wake up more tired than when I went to bed")
Insomnia
Morning headaches (brain starving for O2)
Dry mouth (because they try to open their mouth to improve breathing)
Awaken to urinate multiple times per night
Bed partner complaints about snoring, apneas, choking sounds and restlessness during sleep
OSA SYMPTOMS IN CHILDREN
Sleep apnea occurs in about 2% of children; symptoms include:
Longer total sleep time than normal More effort when breathing (flaring nostrils, heaving chests, sweating); the chest may have an inward motion during sleep
Behavioral difficulties (e.g., hyperactivity and inattention)-ADHD-like ?
Irritability
Bed-wetting
Morning headaches
Failure to achieve expected growth and weight gain
Health consequences of OSA
Cor Pulmonale (& subsequent CHF and MI)
Hypertension
Stroke
Headaches
Obesity
Seizures
Diabetes
Pulmonary hypertension
Worsening of asthma
Snoring vs. apnea
SNORING
Habitual snoring is reported in 24 % of women and 40% of men and increases with age
Snoring may be a sign or a precursor of OSA
Old studies showed that habitual snoring might increase the risk for cardiovascular disease, stroke, hypertension, and EDS
However, many of these studies did not differentiate between simple snoring (primary) and snoring associated with obstructive sleep apnea
Apnea
Temporarily cessation of breathing
Apneas can lead to moments of asphyxia (O2 decreases and CO2 increases)
During apneas, we awaken to restart breathing
Sleep Apnea is defined as a recurrent, temporary cessation of breathing during sleep due to:
Obstruction
Tongue and/or tonsils & adenoids
Central
The brain fails to transmit signals to the breathing muscles
Mallampati Classification
anatomical inspection of upper airway patency, used to classify degree of intubation difficulty on a scale of 1-4
*the larger the number, the MORE obstructed
**1-2 = normal airway
**3-4 = problematic airway (difficult to intubate)
Treatment of OSA
Lifestyle changes -losing weight and avoiding alcohol and smoking (SAME for snoring)
If lifestyle changes do not eliminate OSA:
Positional therapy
Oral appliances
Traditional surgery / uvulopalatopharyngoplasty (UPPP).
Alternative surgery procedures (laser and radiofrequency tissue ablation, somnoplasty)
Continuous positive airway pressure (CPAP)
TRACHEOSTOMY
The original treatment
The surgeon makes an opening through the neck into the airway & inserts a tube
Nearly 100% successful
Requires a quarter-size opening in the throat, producing potentially other medical and psychological problems associated with recovery.
Today, this operation is performed rarely, usually only if sleep apnea is life-threatening.
Narcolepsy & cataplexy Definition
The two primary symptoms in narcolepsy are related to its name (numbness attack):
Excessive daytime sleepiness, with frequent daily sleep attacks or a need to take several naps during the day
The naps or "attacks" are refreshing
Temporary and sudden muscle weakness (cataplexy), usually brought on by strong emotions, such as laugher or, less frequently, anger
The muscles most frequently involved are knees and jaw
Cataplexy is a unique and distinctive symptom for narcolepsy (pathognomonic)
Narcoleptics experience all stages of sleep but start by going directly in REM
Narcolepsy & cataplexy Symptoms
Micro-sleep episodes, in which the patient behaves automatically but without conscious awareness (automatic behaviors)
Sleep paralysis
REM Intrusions
Dreamlike states between waking and sleeping (called hypnagogic hallucinations )
Sleep Onset Rapid Eye Movements Periods (SOREMP)
Proposed etiology (Narcolepsy & cataplexy)
Autoimmune response
Hypocretin/orexin
Narcolepsy is a neurological sleep disorder
It is not caused by mental illness or psychological problems
It is most likely the end result of a number of genetic abnormalities that affect specific biologic factors in the brain, coupled with an environmental trigger such as a virus.
People who develop narcolepsy have a predisposition to developing an autoimmune disorder which leads to the destruction of hypocretin (orexin) cells
Some data suggests that the flu vaccination and flu infection are related to narcolepsy
Hypocretin (orexin) level in the CNS
People who develop narcolepsy have a predisposition to developing an autoimmune disorder which leads to the destruction of hypocretin (orexin) cells
damage to hypothalamus
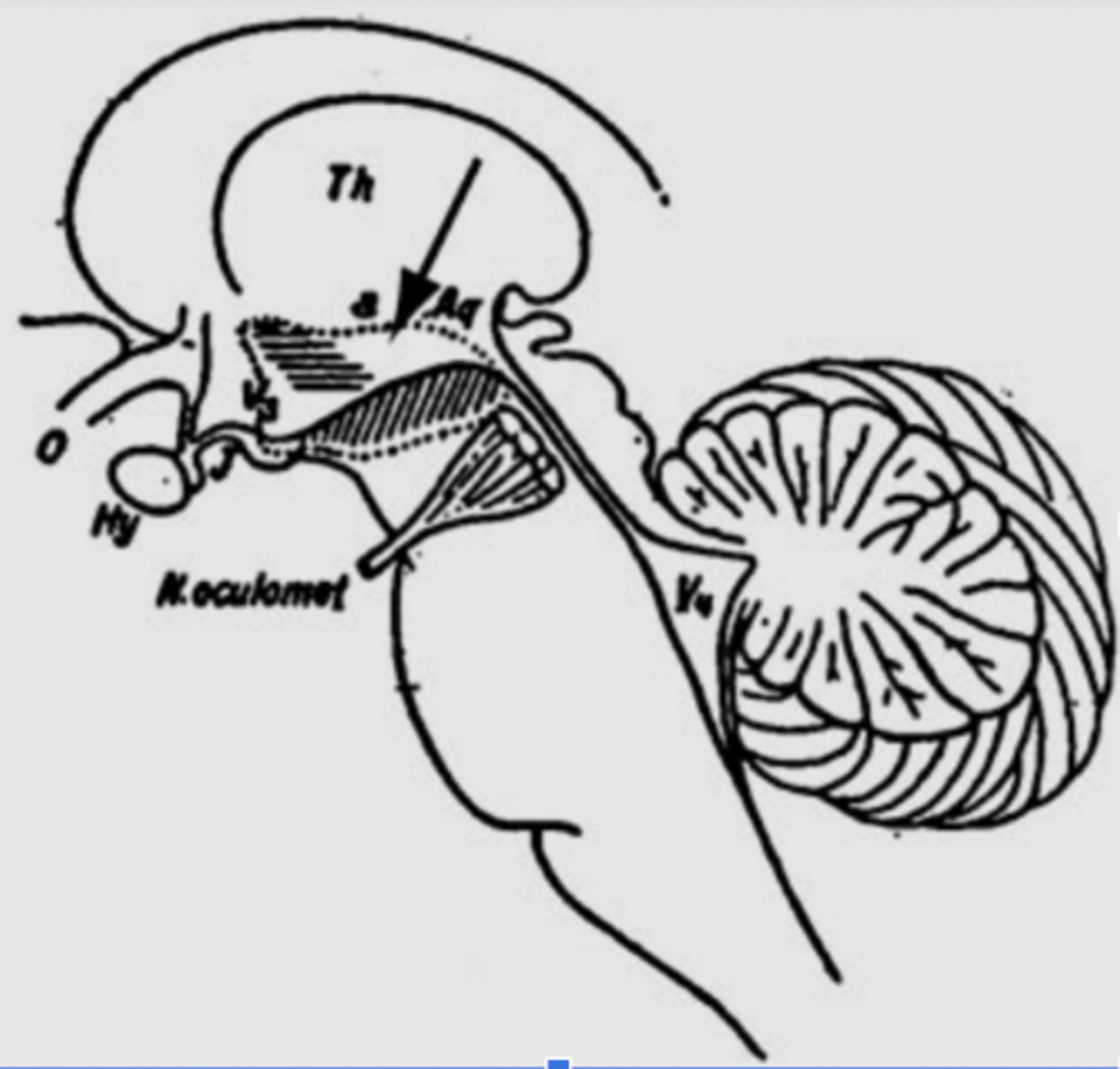
Von Economo's Inferences
(dotted lines)
*Diagonal hatching = hypersomnolence
*Horizontal hatching = insomnia
*Lesions at the arrow induce narcolepsy
These findings suggested to Von Economo that these two areas were the neural circuitry of sleep and wakefulness
Von Economo learned that there are two ares responsible for the neural circuitry of sleep and wakefulness. Lesion to one area lead to hypersomnolence and lesion to another area lead to insomnia. A lesion in between these sites leads to narcolepsy.- HLA (immune system maker), found in 100% of people with narcolepsy
Treatment (Narcolepsy & cataplexy)
Education
Patients, family, friends, & employers
Sleep hygiene
Safety regarding driving and occupational hazards
Doctors are under no obligation to report in NY state
Patients "must" be symptom free for one year if known to DMV and are driving (doctor attestation)
Strategic napping: Two 15 minutes naps per day usually after lunch and around 5 pm
Medications
Cataplexy
Gamma-Hydroxybutyric acid (GHB)
Xyrem
Antidepressants with an action on
Noradrenalin (norepinephrine) and serotonin
Venlafaxine
Atomoxetine
Clomipramine
Sleep Attacks
Gamma-Hydroxybutyric acid (GHB) Xyrem
Modafinil & Armodafinil
Concerta (methyphenidate)
Other stimulants
Restless Legs Syndrome (RLS) Symptoms
a neurological disorder characterized by uncomfortable feelings in the legs, producing a strong urge to move themAn urge to move legsHappens when you're sitting or lying downRelieved by movement (walking)Worse in evening or night
Nocturnal cramps:
Painful and palpable muscular contractions.
Relieved with stretching.
Painful peripheral neuropathy:
Sensory symptoms described as numbness, burning, and pain.
Typically not relieved while walking or during sustained movement.
Arthritis:
Discomfort is centered in the joints.
Volitional movements:
Occurs in fidgety patients, during times of anxiety or boredom.
Typically lack sensory symptoms, discomfort, or the urge to move.
Positional discomfort:
Associated with prolonged sitting or lying in the same position, relieved by changing position.
Periodic Limb Movement Disorder (PLMD) Symptoms
legs jerk 2-3 times per minute during sleep, differs from RLS which occurs during wakeful rest periods as well
Brief limb jerks during sleep (esp legs)
Begin near sleep onset and decrease in stage 3 and REM Movements are rhythmic, every 20-60 seconds, causing repeated and brief arousals People are usually unaware but c/o insomnia and EDS Although most people with RLS experience PLMS, the opposite is not true PLMS diagnosed by polysomnography, while RLS is a subjective diagnosis Association with ADHD, RLS, SDB, Tourette's and iron deficiency
URGE criteria
URGE diagnostic criteria: URGE
Urge to move limbs
Rest or inactivity precipitates or worsens symptoms
Getting up or moving improves the sensation
Evening or nighttime apparence or worsening symptoms
Supportive features: sleep disturbances, PLMS (80% of the cases), positive FH, positive response to tx
Diagnostic Criteria for RLS
1. An urge to move the legs usually but not always accompanied by or felt to be caused by uncomfortable and unpleasant sensations in the legs.
2. The urge to move the legs and any accompanying unpleasant sensations begin or worsen during periods of rest or inactivity such as lying down or sitting.
3. The urge to move the legs and any accompanying unpleasant sensations are partially or totally relieved by movement, such as walking or stretching, at least as long as the activity continues.
4. The urge to move the legs and any accompanying unpleasant sensations during rest or inactivity only occur or are worse in the evening or night.
5. The occurrence of the above features are not solely accounted for as symptoms primary to another medical or a behavioral condition (e.g., myalgia, venous stasis, leg edema, arthritis, leg cramps, positional discomfort, habitual foot tapping.)