3- clinical forms of periodontal disease
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
19 Terms
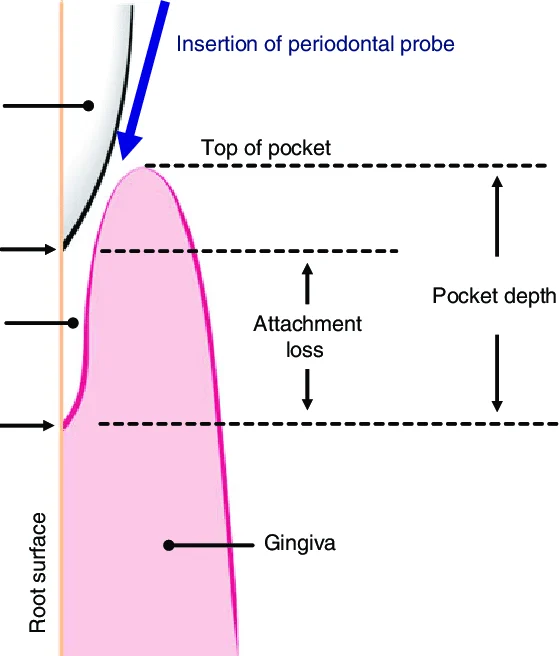
What is a periodontal pocket?
Gingival groove deepened by pathological process
Sulcus, when it deepens due to the apical migration of JE, with attachment loss
What can cause deepening of the gingival sulcus?(3)
Coronal movement of gingival margin
Apical displacement of gingival attachment
Combination of both
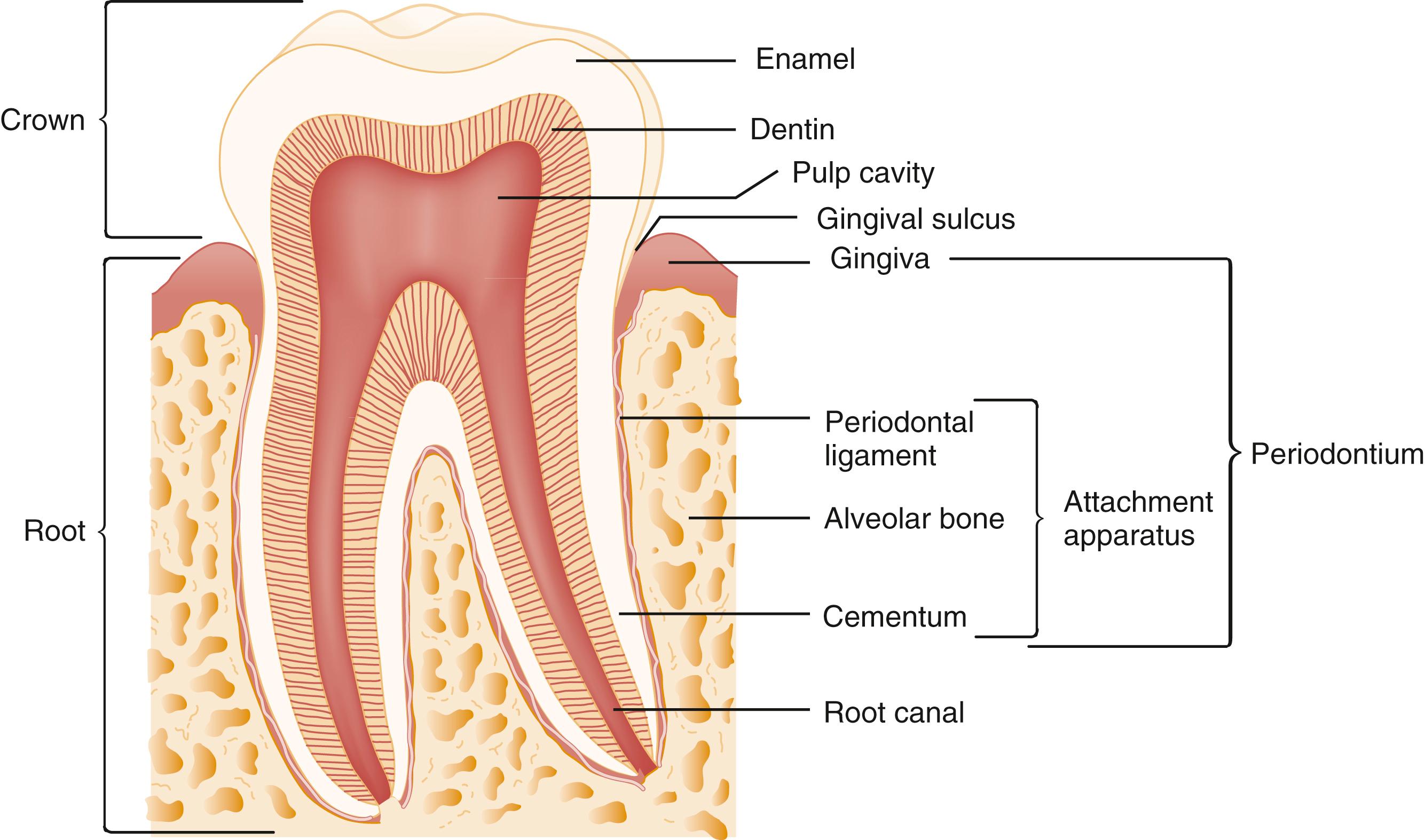
What is the gingival sulcus, healthy sulcus measurements?
Healthy- 0.5mm deep, 2mm on probing
Gingival sulcus- space between neck of tooth and gingival tissue
Gingival vs pseudo vs periodontal pockets
Due to inflammation- gingival enlargement, no insertion or periodontal loss, lateral proliferation of basal cells on JE
Due to edematous swelling- causes increase in groove depth- coronal migration
Due to pathological process- destruction of periodontal tissues- lose and exfoliates teeth
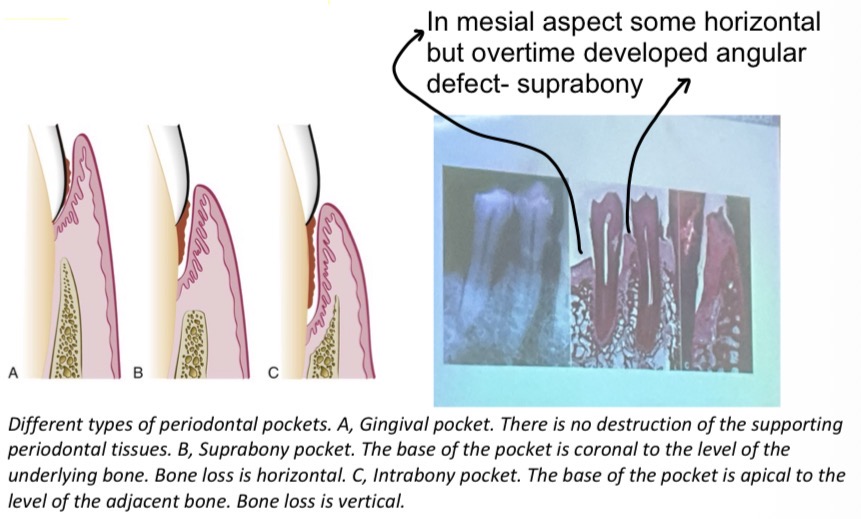
Suprabony vs infrabony
Bottom of pocket is coronal to underlying alveolar bone
Type 1- Bottom of pocket apical to level of adjacent alveolar bone, type 2- lateral pocket wall lies between tooth surface and alveolar bone
What is always a predecessor of periodontitis?
Gingivitis but not all gingivitis progresses to periodontitis
Describe the bone loss process (4)
Osteoclastic stimulation by the plaque
Bone destruction by the plaque
Gingival cells release products that induce osteoclast differentiation
Gingival cells release products that destroy bone by direct chemical action + constructive phase
What are the rates of progress of periodontitis (Loe et al)?
Rapid- 0.1-1mm attachment loss in 1 yr
Moderate- 0.05-0.5
Minimal/No- 0.05-0.09mm
Research shows periodontitis develops more in outbreaks- patient may be stable for a while, they’ll have an outbreak and spreads rapidly then stops
What anatomical features can effect the bone destructive pattern in periodontal disease? (7)
Interdental septa- thickness, width, crestal angulation
Thickness of facial and lingual alveolar plates
Presence of fenestrations and dehiscences
Alignment of the teeth
Root and root trunk anatomy
Root position within the alveolar process
Proximity with another tooth surface
Explain the radius of action/circular blow of destruction
Limited distance around a tooth within which plaque can cause bone resorption
The effective radius is about 1.5–2.5 mm
Beyond 2.5 mm plaque generally does not cause bone destruction.
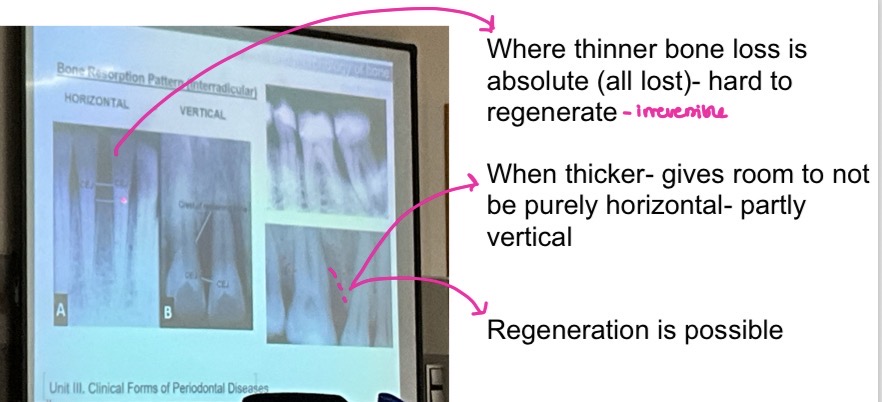
Horizontal and vertical resorption pattern?(interadicular)
Interdental septum determines type of bone loss
Horizontal- Bone height is reduced evenly, bone margin stays straight (perpendicular) to the tooth surface- perio pocket will be suprabony
Vertical- Bone loss is uneven, creating an angular defect usually when interdental septum more than 1.5-2.5mm thick- infrabony
What 4 bone resorption patterns can occur?
Angular defects
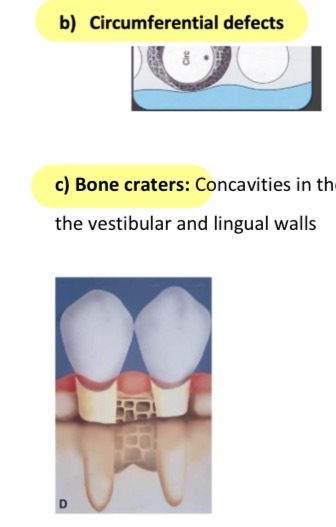
Circumferential defects- cicrcular wall of destruction
Bone craters- if 2 circular defects connect next to each other
Hemiseptal defect- bone crater loses one of its outer walls
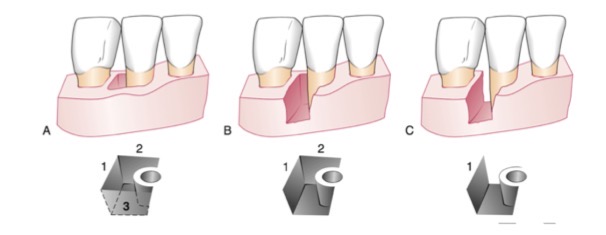
Describe the angular defects that can occur?
Bone profile is oblique to the root profile, leaves an undercut pocket
Depends on the number of bone walls-
- Defect of 3 walls- worst prognosis
- Defect of 2 walls
- Defect of 1 wall- can clean and put in bone graft
3 furcation grades?
1- probe penetrates up to 3mm deep
2- beyond 3mm but not permeable
3- permeable furca

What are the 3 distinguished subgroups of periodontitis and peri-implant diseases?
1. Necrotizing Periodontal Diseases
2. Periodontitis
3. Periodontitis as manifestations of Systemic Diseases
What are risk factors of periodontitis (5)?
Prior history
Local factors- anything that facilitates accumulation/prevents removal of plaque- hygiene, overcrowded teeth, uncleanable resto
Systemic factors- influences effectiveness of host response like diabetes
Environmental and behavioural factors- smoking, stress
Genetic- polymorphism in genes encoding interleukin 1a, 1b
Localised vs generalised periodontitis
When less than 30% of sites show attachment and bone loss
30% or more show attachment and bone loss
Clinical features of necrotising periodontitis?
Necrosis + ulceration of coronal part of interdental papilla and gingival margin
Painful, bright red, suppurative margin- bleeds easy
Recession, severe mobility
Conventional pockets missing due to destruction of marginal epithelium and ct
Related to an AIDS or HIV+ diagnosis
4 etiological factors of necrotising periodontitis?
Microbial flora- hiv patients, spirochete aggregate fusiforms, Candida albicans, herpes virus
Immunosuppressed
Stress
Malnutrition