Supp Care, Pain/Agitation/Delirium, Shock
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
FASTHUG acronym →
feeding
analgesia
sedation
thromboembolism prophylaxis
head of bed elevation
stress (ulcer prophylaxis)
glucose control
STRESS-RELATED MUCOSAL DISEASE Clinical Presentation
Occult
Overt
Clinically significant
no visible blood loss, +fecal blood test, iron def anemia
frank hemorrhage
HD changes, transfusion required
STRESS ULCER PROPHYLAXIS
Independent risk factors
→
Coagulopathy →
mech vent >48h
plt count <50k, INR >1.5, PTT >2x normal
What acid suppressants are used for stress ulcer prophylaxis in the ICU?
H2RAs, PPIs
GOALS OF THERAPY
Target pH for prevention of SRMD (stress-related mucosal disease)
Target pH for prevention of peptic ulcers
4
6
H2RAs may be associated with _________ but _________ compared to PPIs
+risk GI bleeding, -incidence of infectious complications
H2RA WARNING/PRECAUTIONS
→
→
→
→
DDIs (CYP450)
tachyphylaxis
CNS ADEs
TC
PPI WARNING/PRECAUTIONS
→
→
→
→
+risk pneumonia and C diff
DDIs
osteo-related bone fractures
hypoMg
VIRCHOW’S TRIAD (contributors to thrombosis)
Hypercoagulability → 5
Vascular injury → 4
Venous stasis → 3
hx VTE, malignancy, obesity, preg, estrogen
trauma, recent surg, IV catheter, atherosclerosis
immobilization, AFib, obstruction
NONPHARM VTE PROPHYLAXIS → 2
compression stockings
intermittent pneumatic compression
UNFRACTIONATED HEPARIN
Potentiates the action of _________ to inactivate thrombin & prevent conversion of fibrinogen → fibrin
Dosing:
Monitoring: 3
antithrombin III
<50 kg = 5000U SQ q12h, >100kg = 7500U SQ q8h
Hgb/Hct, plt, aPTT
LOW MOLECULAR WEIGHT HEPARIN
Enoxaparin (Lovenox)
Potentiates the action of _________ to inactivate thrombin & prevent conversion of fibrinogen to fibrin; stronger inhibition of ______ than thrombin
Dosing:
NOT approved for use in _______
Monitoring → 4
antithrombin III, Factor Xa
40 mg SQ daily; CrCL <30 use 30 mg SQ
hemodialysis
Hgb/Hct, plt, peak anti-Xa, renal fx
FONDAPARINUX
_______
Dosing
Contraindications → 2
NOT recommended for critically ill patients → why? (3)
Monitoring → 3
Factor Xa inhib
2.5 mg SQ once daily, CrCL 30-50 reduce dose by 50%
<50 kg, CrCL<30
high renal CL, long t1/2, no reversal agent
Hgb/Hct, plt, renal fx
__________ may be as effective as pharmacologic stress ulcer prophylaxis with fewer infectious complications
enteral feeding
Gold standard of assessing pain =
Self report
________ are NOT valid indicators of pain
vital signs
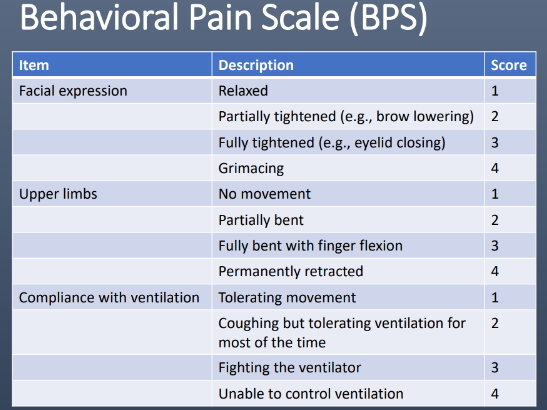
Behavioral Pain Scale (BPS)
A score _____ indicates significant pain
>5
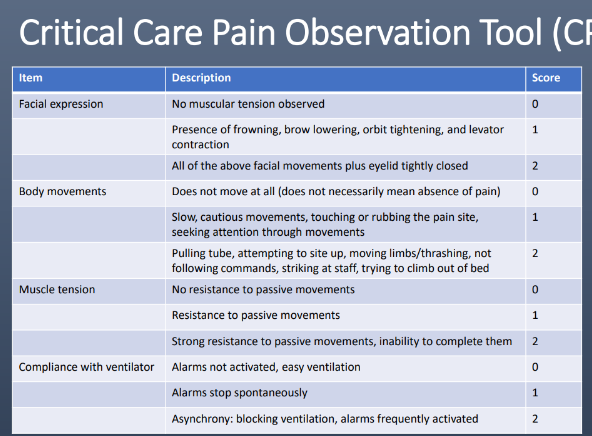
Critical Care Pain Observation Tool (CPOT)
A score _____ indicates significant pain
>2
TREATMENT OF PAIN IN THE ICU
*Mainstay:
_________ as adjunct to -pain and opioid use
_________ as adjunct to -opioid use in postsurgical patients
_________ for neuropathic pain
Preemptive analgesia prior to painful procedures → 2
opioids
APAP
low dose ketamine
gabapentin, carbamazepine, pregabalin
opioids (lowest effective dose), NSAIDs
TREATMENT OF PAIN IN THE ICU → ______ ARE NOT ROUTINELY RECOMMENDED
NSAIDs
IV OPIOIDS
Onset → metabolism
Fentanyl
Morphine
Hydromorphone
Remifentanil
1-2min → hepatic
5-10min → glucuron; accumulates in renal fail
5-15min → glucuron
1-3min → hydrolysis by esterases
OTHER OPIOIDS
_________ → not routinely recommended, neurologic toxicity
_________ → LONG half life, DDIs, +QTc
meperidine
methadone
OPIOIDS ADES
_______
GI intolerance →
_______ → most common w morphine
_______
_______
resp depress
constipation → prophylactic stimulant + stool softener
HD instability
altered mental status
withdrawal
BB is a 75-year-old male admitted to the ICU after a motor vehicle crash in which he sustained multiple rib fractures. His PMH is significant for HTN and CKD. After intubation, he is agitated and grimacing. Which initial treatment is most appropriate?
a. Fentanyl
b. Midazolam
c. Morphine
d. Propofol
A
SEDATION CHOICE OF AGENT → 2 recommended over benzos
propofol, dexmedetomidine
TARGETING “LIGHT” SEDATION
Patients should receive sedation only if required
Assess sedation status and goals ________
______ to allow responsiveness and awareness
Spontaneous awakening trial ________
atleast daily
titrate
daily
BENZODIAZEPINES
Indications → 3
Lorazepam →
Midazolam →
status epilepticus, alc/benzo withdrawal, DEEP sedation and/or neuromusc blockade
intermed acting, hepatic glucuron, DC if osmolar gap 10+ (propylene glycol diluent toxicity)
short acting, CYP3A4, caution renal/hepatic dysfx
PROPOFOL 1% (10 mg/mL)
MOA
Effects
PK/PD
Dosing
ADEs → 5
GABA-A agonist, NMDA antag
sedative, anesthetic, anti convuls at higher doses
lipophilic, large Vd
5-50 mcg/kg/min
hypotension, bradycardia, resp depress, hyperTG, pancreatitis
PROPOFOL RELATED INFUSION SYNDROME (PRIS)
Over ____ mortality
Mechanism of injury: disruption of __________ production
Clinical effects → 5
Monitoring → 6
INCREASED risk with doses ____ mcg/kg/min and duration _____
50%
mitochondrial energy
bradycardia, lactic acidosis, renal/liver fail, rhabdo, hyperTG
CK, lactate, TG, LFTs, SCr, lipase
>50, >48h
DEXMEDETOMIDINE
MOA
Effects
Dosing
ADEs → 2
central alpha agonist
sedative, analgesic, anxiolytic
0.2-0.7 (max 1.5) mcg/kg/h
hypotension, bradycardia
Which does NOT affect respiratory drive?
A. propofol
B. dexmedetomidine
B
MEDICATION-ASSOCIATED DELIRIUM → 6
benzos
opioids
antichol (diphenhydramine, metoclopramide, tricyclics)
anticonvuls
steroids
DA agonists (ropinirole, pramipexole)
NON-PHARM THERAPY FOR DELIRIUM
Reduce modifiable _____
Optimize ______
Increase ______
Optimize _______ and ________
Frequent ________
risk factors
sleep
mobility
hearing, vision
reorientation
DELIRIUM ICU TX
Prevention:
Consider _______ or ________ in patients with significant distress or agitation leading to physical harm
_______ suggested in mechanically ventilated adults where agitation is precluding weaning/extubation
not rec
haloperidol, atypical antipsychotics (SGAs)
dexmedetomidine
ANTIPSYCHOTICS
1st generation: haloperidol dosing → ADEs
2nd generation: agents → ADEs
1-2 mg q 4-6h PRN → sedation, EPS, +QTc
quetiapine, olanzapine, risperidone, ziprasidone → low and slow → sedation, +QTc, NMS
ANTIPSYCHOTIC PLAN
Consider low starting dose, especially in the _____
Normalize ______ and monitor _____
Monitor daily for ADEs (especially _______)
Ideally, ____________; otherwise clearly communicate plan to floor team or outpatient provider
elderly
ELs, QTc
sedation
taper off before ICU discharge
MARKERS OF ORGAN DYSFUNCTION
Brain
altered mental status
MARKERS OF ORGAN DYSFUNCTION
Lungs
mech vent
hypoxemia (PaO2/FiO2<200-250)
MARKERS OF ORGAN DYSFUNCTION
Heart
SBP<90
MAP<65
MARKERS OF ORGAN DYSFUNCTION
Liver
Tbili <2
Plt <100k
INR >1.5, aPTT >60s
MARKERS OF ORGAN DYSFUNCTION
Kidneys
acute oliguria
+Cr
MARKERS OF ORGAN DYSFUNCTION
Gut
ileus (absent bowel sounds)
abd pain
MARKERS OF ORGAN DYSFUNCTION
Skin
mottled
dusky
MARKERS OF ORGAN DYSFUNCTION
Lactate _____ mmol/L
>2
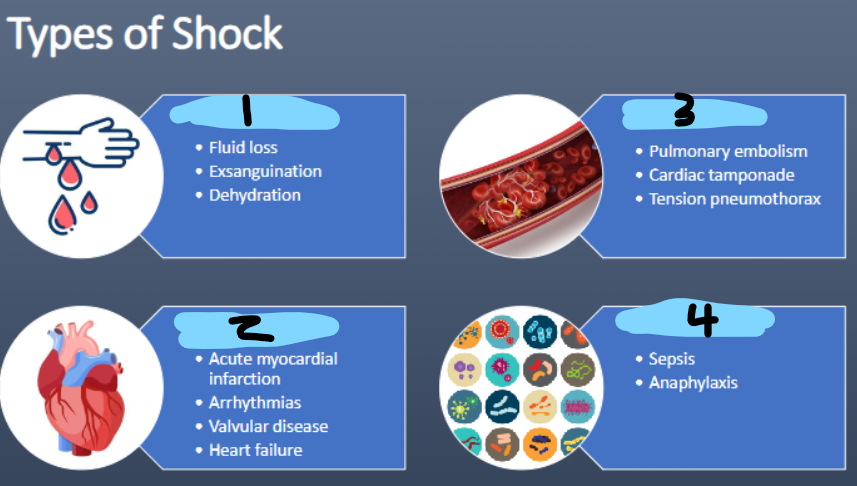
TYPES OF SHOCK → 4
hypovolemic
cardiogenic
obstructive
distributive
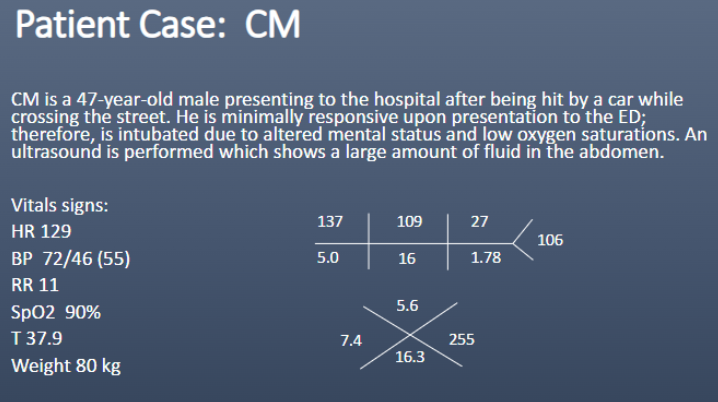
What type of shock does CM most likely have?
a. Cardiogenic
b. Distributive
c. Hypovolemic
d. Obstructive
C
PHASES OF SHOCK TREATMENT → 4
Salvage → min acceptable BP, MAP >65
Optimization → O2, cardiac output, tissue perfusion
Stabilization → organ supp, minimize complications
De-escalation → wean vasoactive agents, achieve -fluid balance
SEPSIS
Sepsis criteria
SIRS criteria → 4
infxn (suspected or documented) + >/=2 SIRS criteria
temp >38C or <36C, HR>90, RR>20 or PaCO2<32, WBC>12×10^9
Yes
(T 39.9C, HR 121, RR 30 = ¾ SIRS
suspected infxn = green sputum)
SEVERE SEPSIS = sepsis + _______
organ dysfx
yes
(+SCr, lactate>2, MAP 64)
SEPTIC SHOCK =
sev sepsis + hypotension
SEPSIS ANTIMICROBIAL THERAPY INITIATION
Stat =
Initiate antimicrobial therapy within ______
_____________ as rapidly as possible
obtain cultures
1h
obtain source control
EMPIRIC ANTIMICROBIAL THERAPY 4 important factors →
right agent
right dose
right site
right time
SEPSIS IV FLUID RESUSCITATION
________ IVF to be given within the first _____
Type =
Goals =
30 mL/kg, 3h
balanced crystalloids (LR, plasmalyte)
MAP 65+, lactate <1 (in elevated lactate)
Which is the most appropriate fluid to administer to DS? (weight = 70 kg)
a. 1000 mL Albumin
b. 1000 mL Lactated Ringer’s
c. 2000 mL Normal saline
d. 2000 mL Plasmalyte
D
When to initiate vasopressors?
When to initiate inotropes?
fluid resus fails
myocardial dysfx, ongoing signs of hypoperfusion
Adrenergic receptors
alpha 1
beta 1
beta 2
+SVR
+SV and CO
opposes a1
VASOPRESSOR MOA
Epinephrine
Norepinephrine
Phenylephrine
Dopamine
Vasopressin (2nd line)
Dobutamine
ALL
a1 + a2 > b1
a1**
a1 + b1 + b2
peripheral V1
b1 + b2 > alpha
DOPAMINE DOSING EFFECTS
_____ mcg/kg/min = renal artery vasodilation
_____ mcg/kg/min = cardiac + vasoconstriction =
_____ mcg/kg/min = cardiac + marked vasoconstriction =
<2.5
2.5-10 = b1 + b2
>10 = a1
ADRENERGIC RECEPTORS ADES
a1, V1 →
b1 →
b2 →
tissue ischemia, AKI
tachycardia/arrhythmias, +myocardial O2 demand, impairs insulin sens (hyperglycemia)
impairs insulin sens, +serum lactate
WHICH VASOPRESSOR FOR SEPSIS?
Vasopressor therapy should initially target a MAP of ____ mmHg
1st line vasopressor =
______ or _____ may be added if additional agent is needed
May use ________________ with persistent hypoperfusion despite adequate fluids & MAP
65
NE
EP, vasopressin
dobutamine + NE or EP alone
THERAPEUTIC GOALS & MONITORING
BP/MAP
Urine output
Lactate
MAP >65
0.5 mL/kg/h
-20% in 2h period
After receiving 2L of Plasmalyte, DS’s blood pressure is 94/48 (MAP: 56 mm Hg). What vasoactive agent is most appropriate to start to increase her blood pressure?
a. Dobutamine
b. Dopamine
c. Epinephrine
d. Norepinephrine
D
CORTICOSTEROIDS
Who should receive steroids? patients with shock in which ______ and ______ do not restore HD stability
How should it be given?
Taper when …
fluid resus, vasopressors
IV 200 mg/day
vasopressors no longer req