ABFM PREP
1/143
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
144 Terms
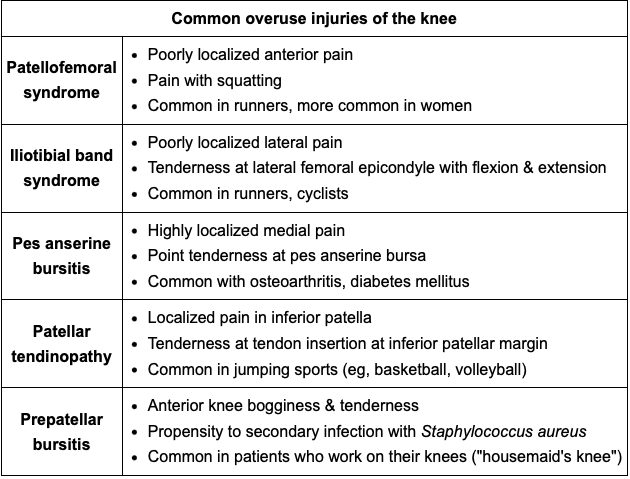
What do these common overuse knee injuries look like?
a) Patellofemoral syndrome
b) Illiotibial band syndrome
c) Pes anserine bursitis
d) Patellar tendinopathy
e) Prepatellar bursitis
a) Patellofemoral syndrome-pain reproduced w/squats
b) Illiotibial band syndrome-tenderness 2cm to lateral knee joint line
c) Pes anserine bursitis-high localized medial pain
d) Patellar tendinopathy-tender inferior patellar margin (jump sports)
e) Prepatellar bursitis-bogginess+tender anterior knee(housemaid knee)
How is ADHD medication management performed with Lisdexamfetamine?
A) How much to increase?
B) How often?
C) Max dose?
A) Increase 10mg-20mg
B) Increase weekly until 50% symptoms resolve or s/e unbearable.
C) 70mg
How does invasive cervical cancer present compared to early stage cervical cancer?
Patients with invasive cervical cancer often present with abnormal vaginal bleeding and pain after coitus. Tumor growth typically causes either an ulcerative or exophytic, friable lesion that bleeds on contact. Slough off the lesion causes watery, malodorous discharge
Lateral tumor extension=more advanced cancer stage.
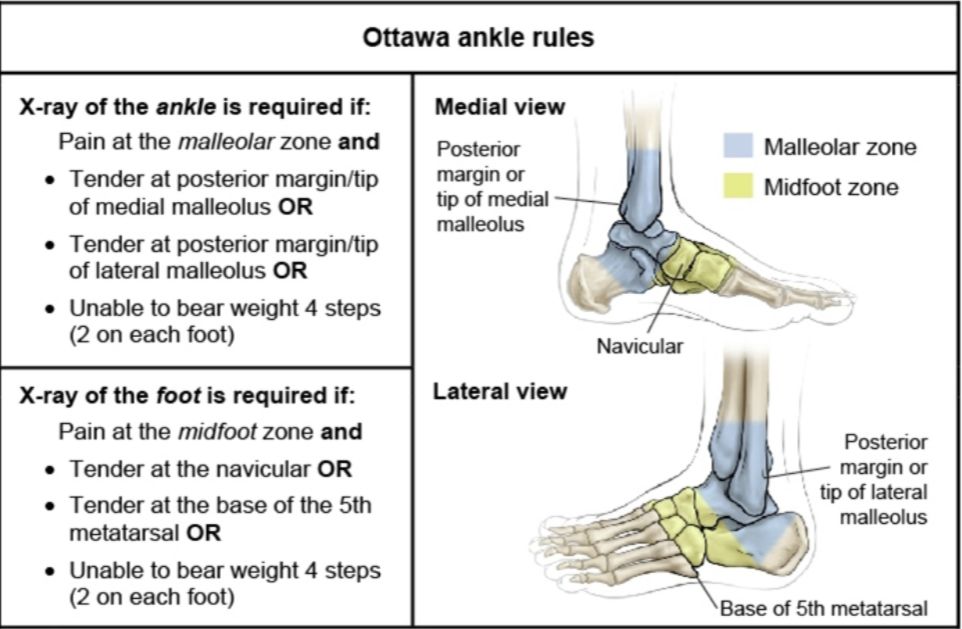
Ottawa Ankle Rules
A) Ankle
B) Foot
A: Malleolar pain + bone tenderness at posterior edge or tip of lateral malleolus or the medial malleolus or unable to walk 4 steps.
B: Midfoot pain + bone tenderness at the base of the fifth metatarsal or navicular bone or unable to walk 4 steps.
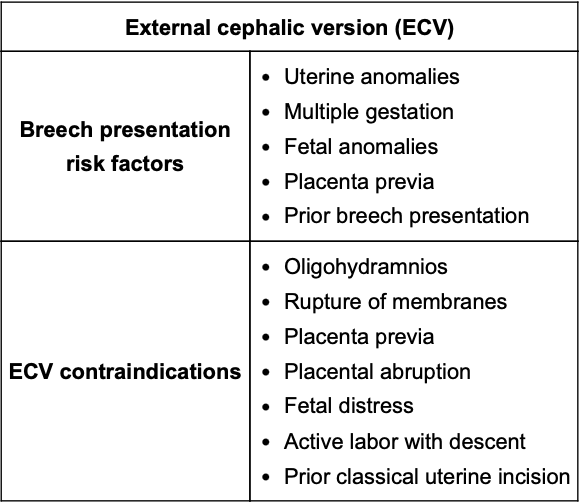
When is External Cephalic Presentation offered in pregnant women with breech positioning?
Offered between 36-37 weeks gestation, prior to onset of labor. Itdecreases the likelihood of cesarean delivery by 40%
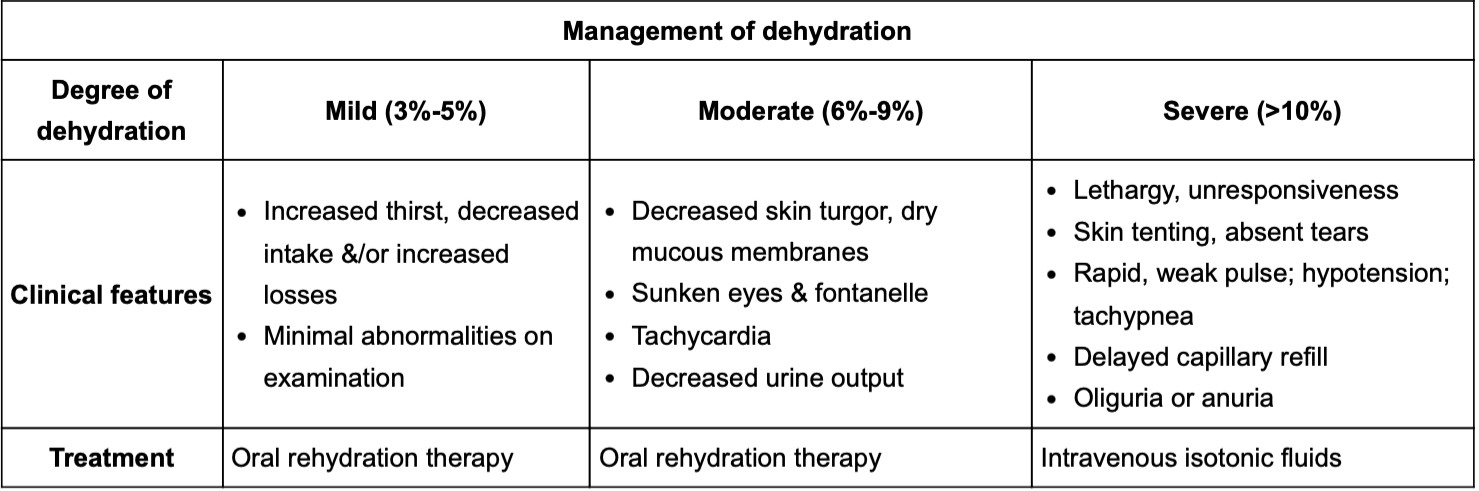
Management of dehydration?
Note: In IV replacement opt for NaCl bolus w/ 10-20ml over 10-30 minutes
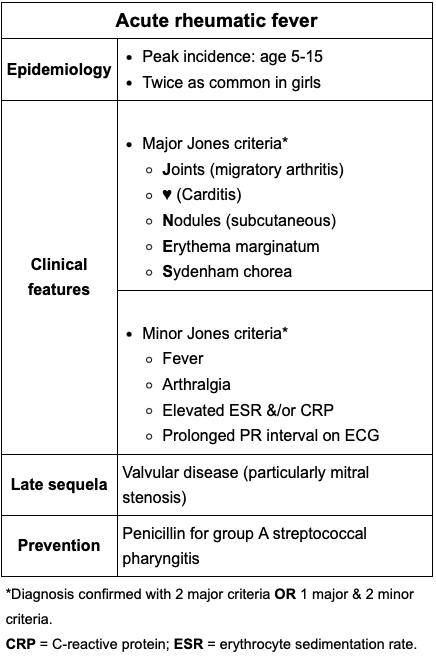
Mnemonic and diagnoses of Acute Rheumatic fever
>: "JONES" (Joint pain, Carditis, Nodules, Erythema marginatum, Sydenham's chorea).
<: Fever, migratory arthralgia, elevated ESR/ CRP, prolonged PR on EKG.
Dx: 2 > or 1 > + 2<
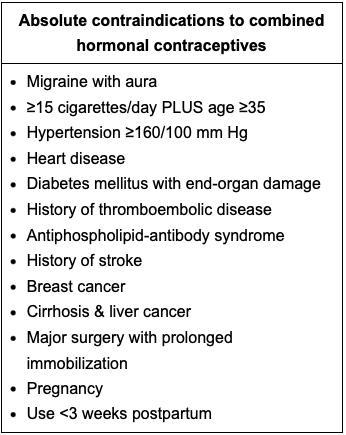
Contraindications to combined hormonal contraceptives
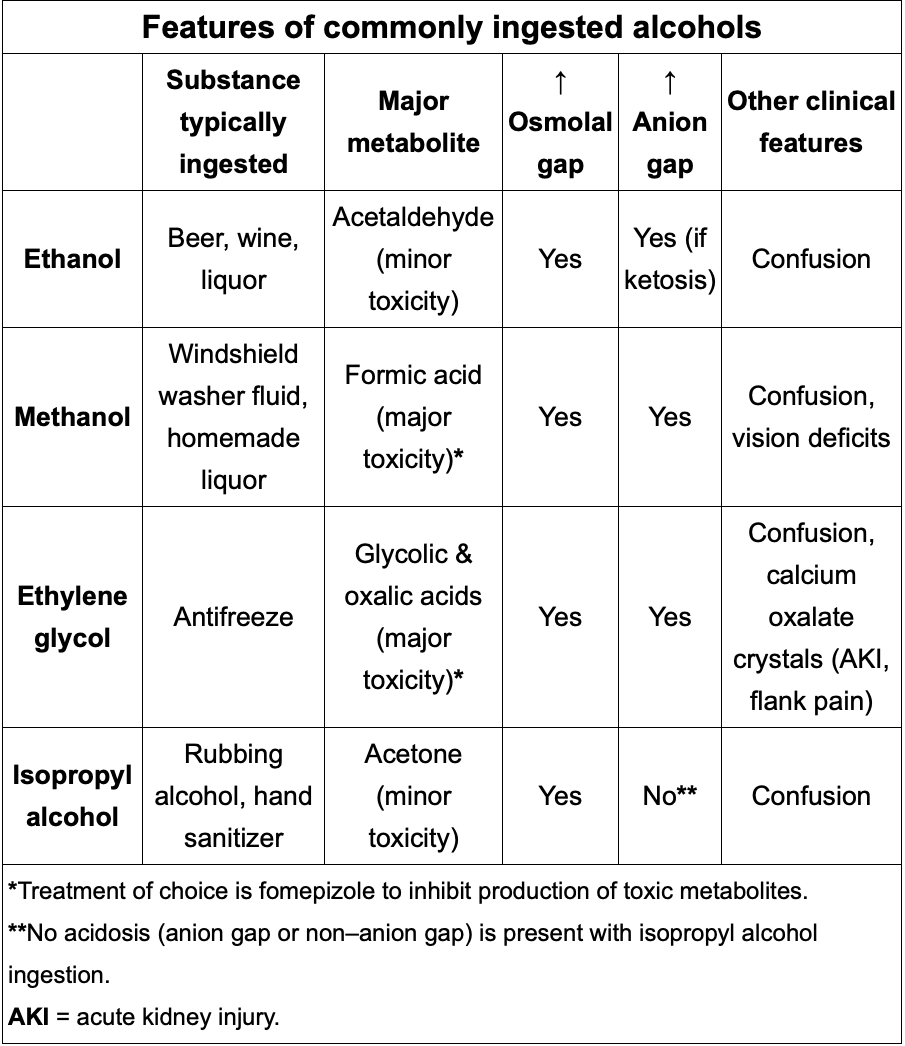
What can mimic ethanol intoxication and how does it present?
-Ethylene glycol poisoning.
-EG metabolism leads to formation of oxalic acid which can bind to Ca and lead to hypoCa + Calcium Oxalate crystals. Pt develops flank pain, hematuria, AKI and anion gap acidosis.
-Tto: Fomepizole
Patients are in pre-term labor when they have regular uterine contractions and 1 of the following:
>3cm cervical dilation (including change on repeat examination)
Shortened Cervix (<20mm) on transvaginal sonogram.
S/E of Zolendronic acid (1/year infusion for osteoporosis) and what Vit should be monitored?
Post infusion flu-like symptoms
Mild transient hypocalcemia which is worsened and prolonged in pts w/Vit D deficiency.
Signs of cerebellar dysfunction
Gait dysfunction
Truncal Ataxia
Nystagmus
Intention tremor
Impaired rapid alternating movements (Dysdiaochokinesia)
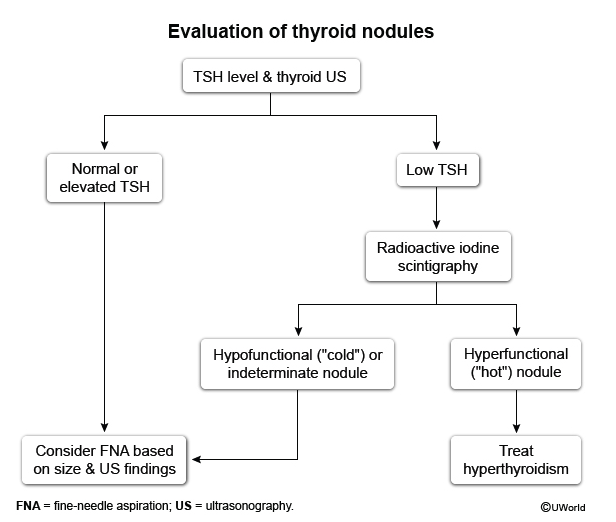
Evaluation of thyroid nodule per TSH:
a) Normal / elevated TSH
b) low TSH
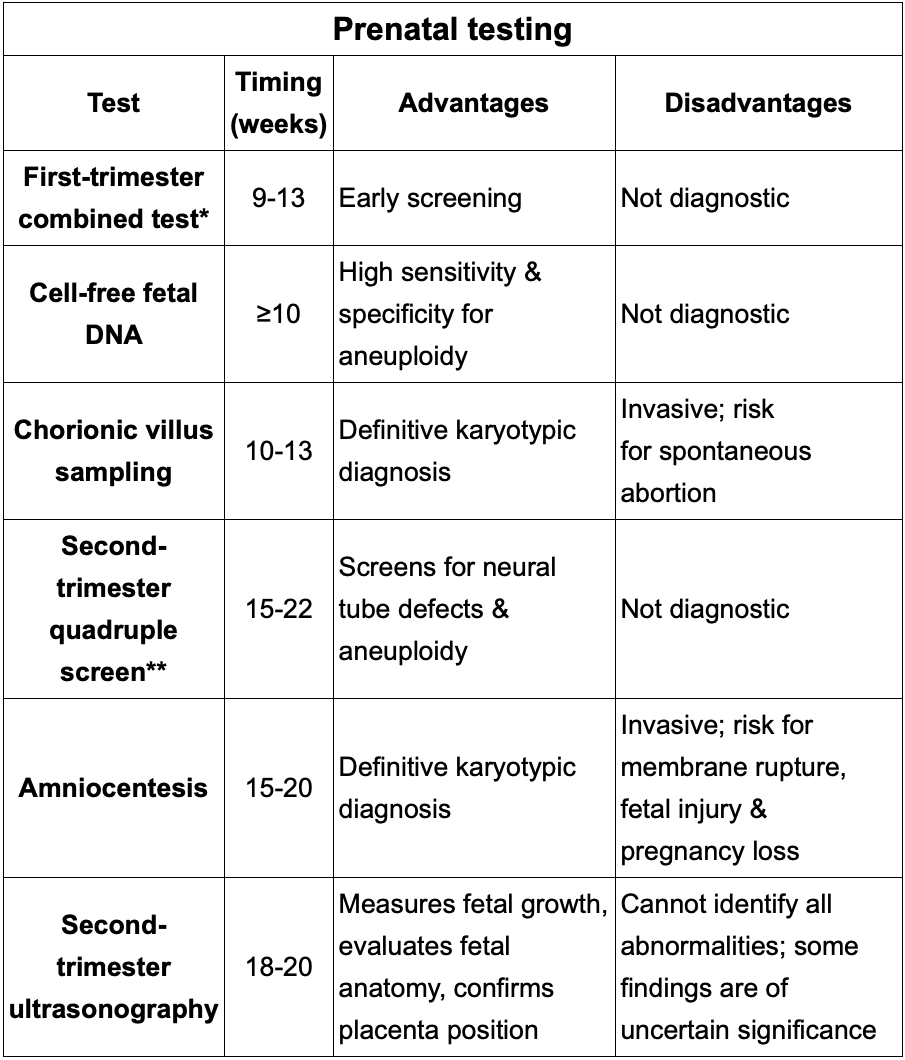
Review prenatal testing by week
-Maternal alpha fetoprotein-neuron tube defect + Abdominal wall defect.
S/E of metoclopramide I always forget?
Dopaminergic antagonist used for chemotherapy induced N/V.
Acts as a central and peripheral dopamine receptor blocker causing extrapyramidal symptoms (Akathisia, dystonia, and Parkinson like symptoms)
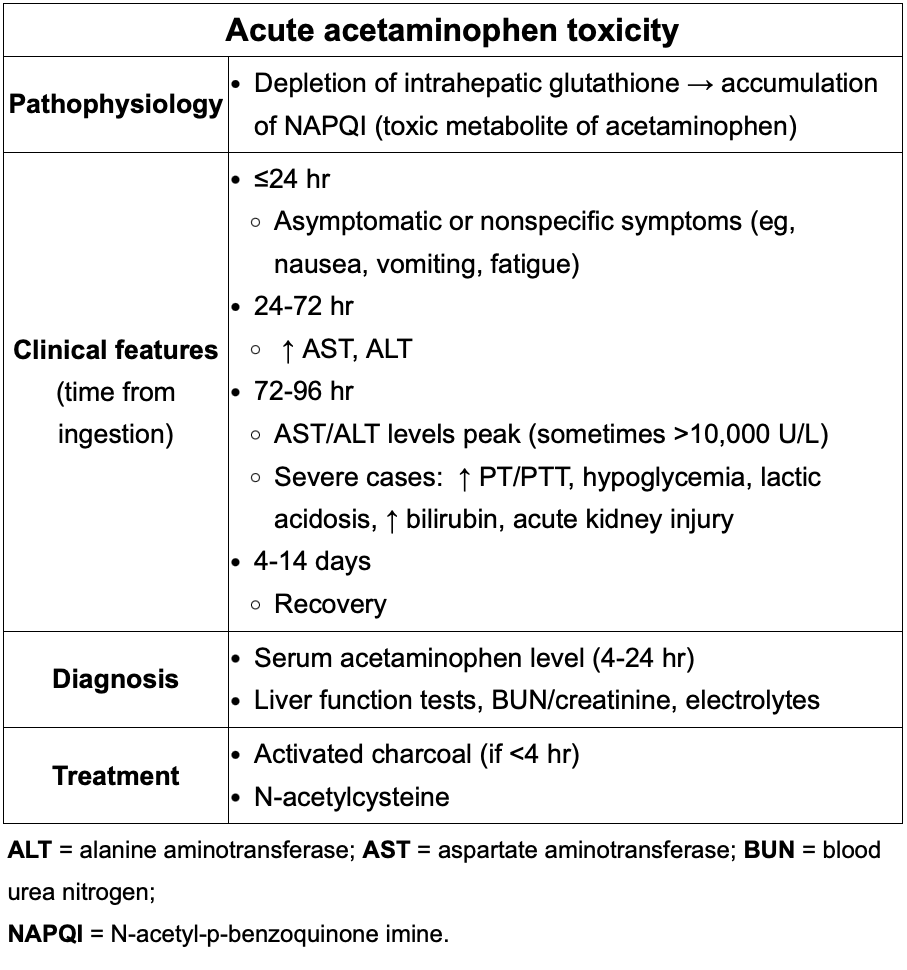
Clinical features, diagnosis and treatment of Acute acetaminophen toxicity?
Likely to occur with a single ingestion of >250mg/kg or multiple ingestions totaling > 12g in 24 hrs.
<24= asymptomatic
1-3d= AST/ALT increase into thousands+ RUQ pain+tenderness
3-d= AST/ALT peak, jaundice, encephalopathy, coagulopathy (high INR), spontangeous bleeding
Tx: N-acetylcysteine , activated charcoal if <4 hrs
Unilateral motor drift is a sign of what?
“When her left leg is lifted above the examination table, it slowly falls back to the table over 5 seconds”
Sign of acute stroke
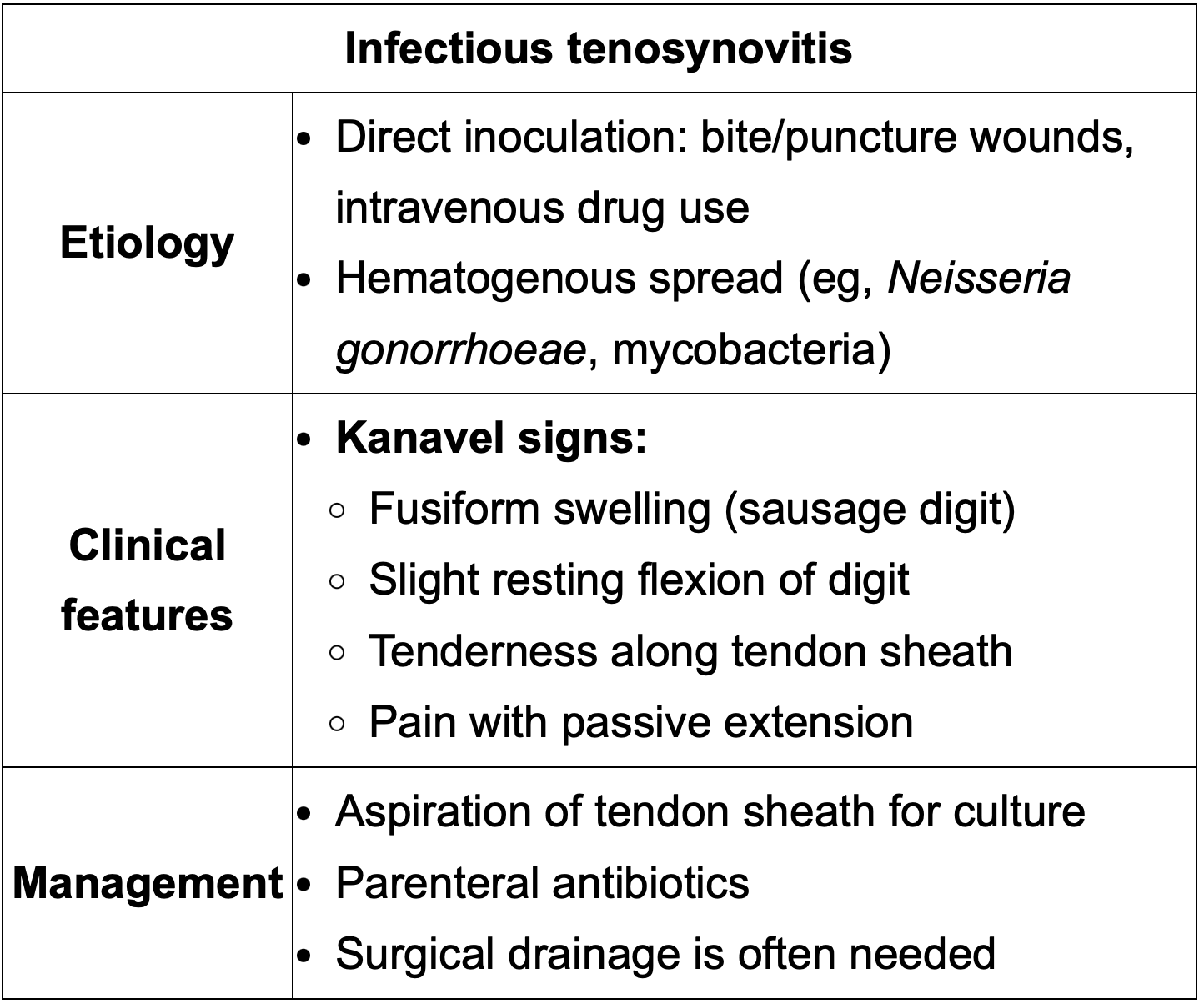
Name of the pathognomonic sign on infectious tenosynovitis
Kanvel sign→ Sausage digit with tenderness along the tendon sheath, pain with passive extension and slight resting flexion of digit.
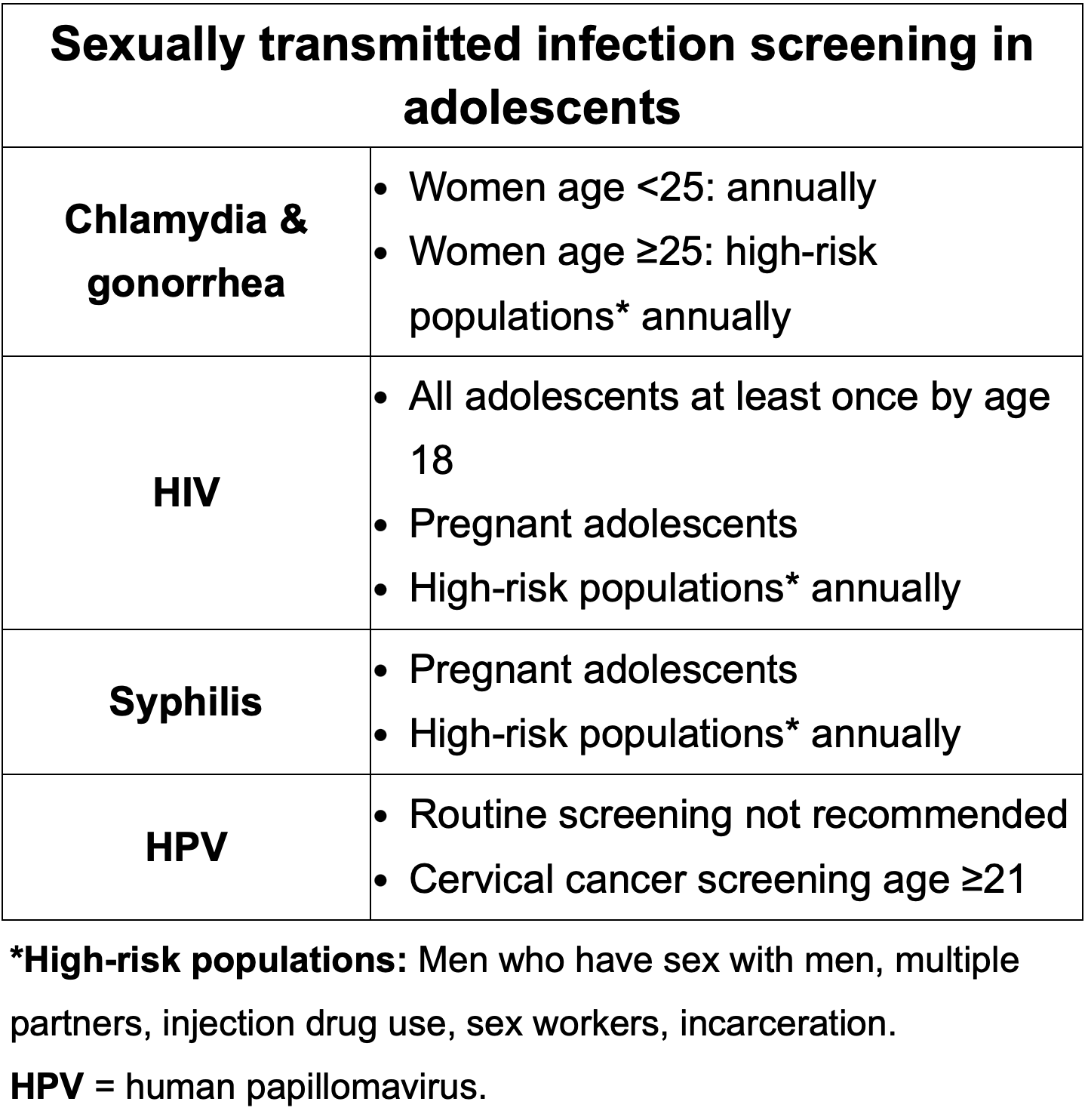
STI screening in women who have sex with women
How is scabies described for the boards? Dx? Tx?
Extremely pruritic, small, erythematous papules, interdigital distribution with web spaces, flexor or wrist extension. All can present in axillae, feet, umbilicus or genitalia. Burrows may not be visible but pathognomonic if present.
Dx: Clinical, skin scraping in microscopy is confirmatory.
Tx: 5% Permethrin or oral ivermectin. Treat family as well.
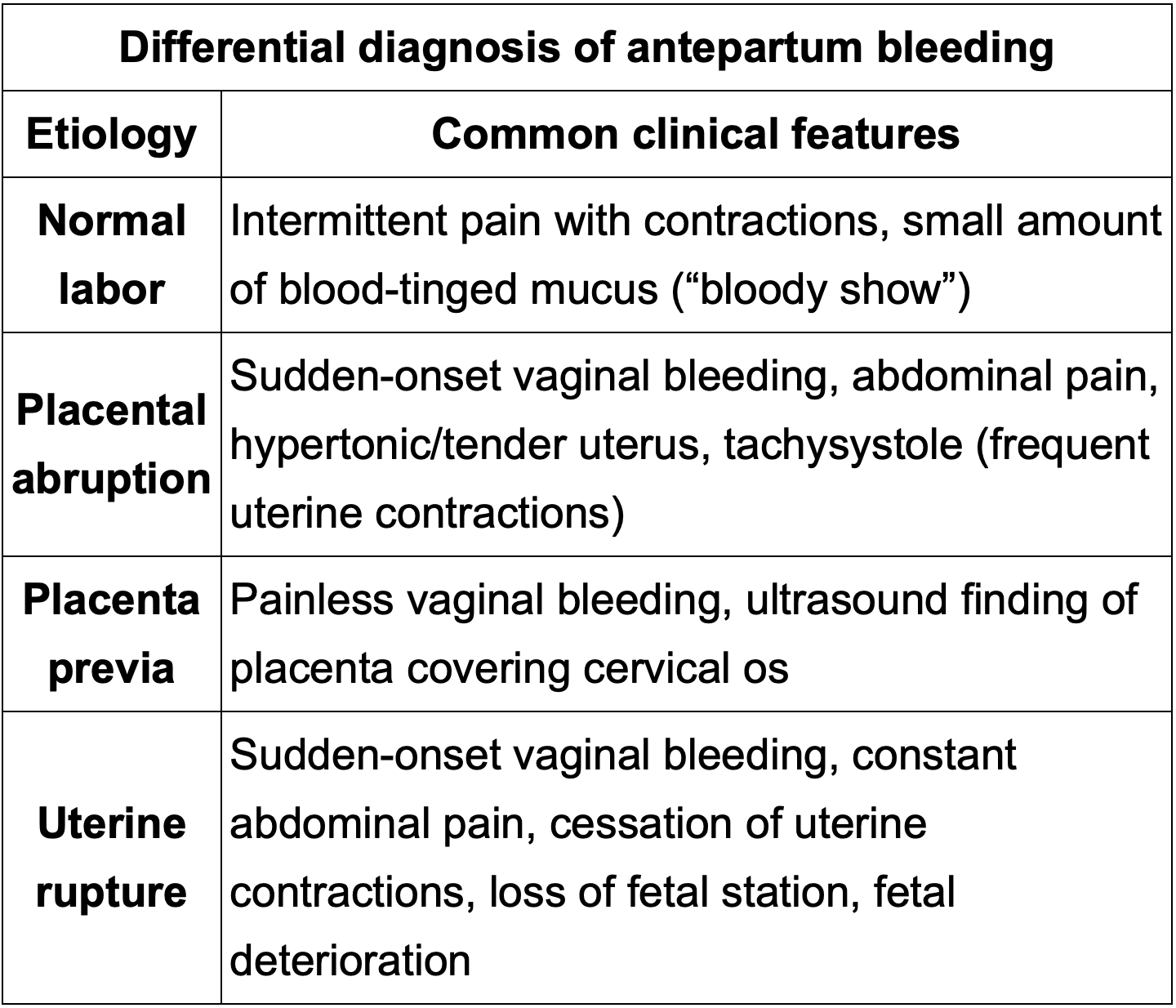
Differential Dx for antepartum Bleeding?
Remember to differentiate painless vs painful bleeding.
Only 1 painless vaginal bleed
Remember placental abruption has Tachysistole to differentiate from uterine rupture where there is cessation of contractions
Epididymitis different causing agent by age
Young: G/C
Old: E. Coli
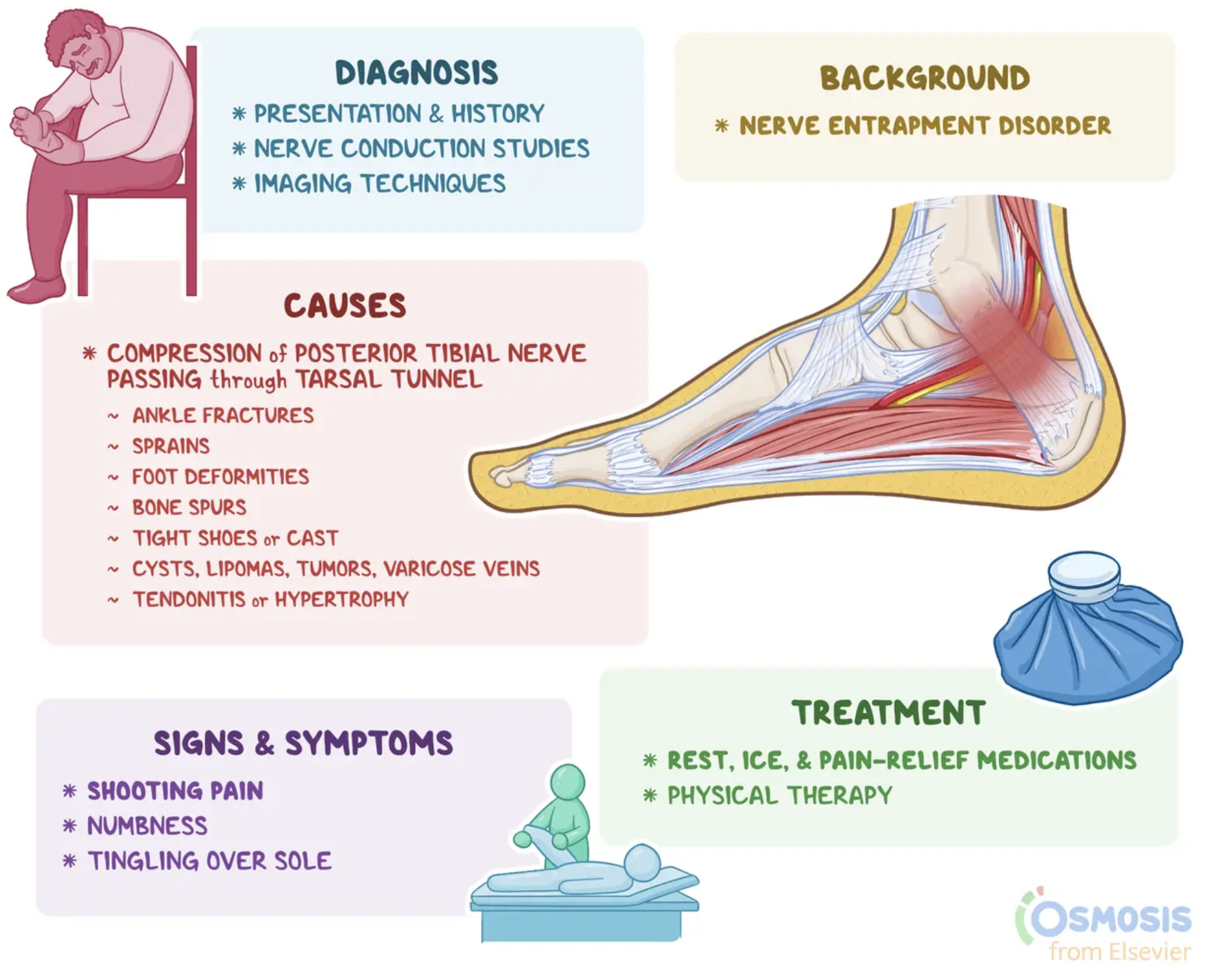
What should i know about Tarsal tunnel syndrome?
Cause:
Symptoms:
Tx:
Tarsal Tunnel Syndrome:
Cause: Compression of posterior tibial nerve, likely 2/2 to ankle fx or dislocation. Scar tissue, bone spur can develop and compress the nerve.
Symptoms: Numbness or paresthesias in the distribution of then nerve. Pain can radiate up the heel and calf, worse at night or w/standing.
Tinel sign: Tingling after percussion.
Tx: NSAIDS, shoe modification, steroid shot
Dx. of Tinea Versicolor and mgt?
Clinical , can be confirmed with Potassium Hydroxide (KOH),
The curved hyphae and round yeast cells appear as "spaghetti and meatballs" under the microscope. Topical therapy (ketoconazole, terbinafine, selenium sulfide) are the treatment of choice.

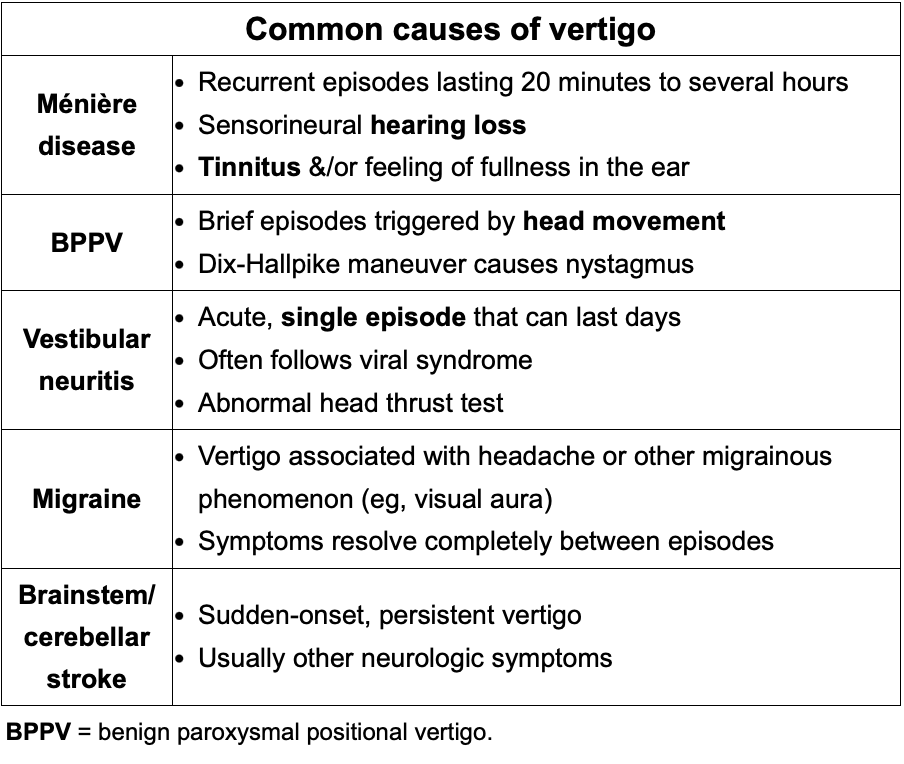
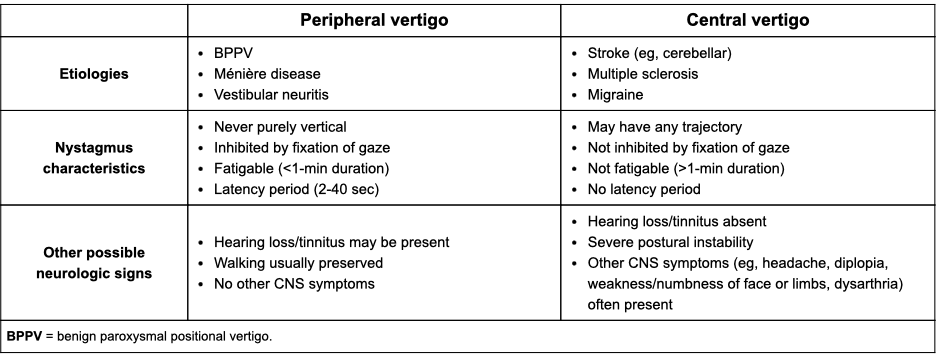
Review common causes for vertigo:
a) Meniere disease
b) BPPV
c) Vestibular Neuritis
d) Migraine
e) Brainstem/cerebellar stroke
Review peripheral vs central vertigo (low yield, just to be a smart ass)
Review emergency contraception:
a) What’s 2 have the highest pregnancy-prevention rate?
b) C/I of those two medications.
c) How long does it take Depo to become effective?
*REMEBER*
Ulipristal is great but less effective in overweight and obese women as it’s systemic. IUD are local and unaffected by BMI.
a) Copper IUD/ Progestin IUD
b) C-IUD= C/I Wilsons, active pelvic infection, uterine cavity distortion
P-IUD= Breast cancer, active pelvic infection, uterine cavity distortion
c) Depo takes 7 days to provide protection.
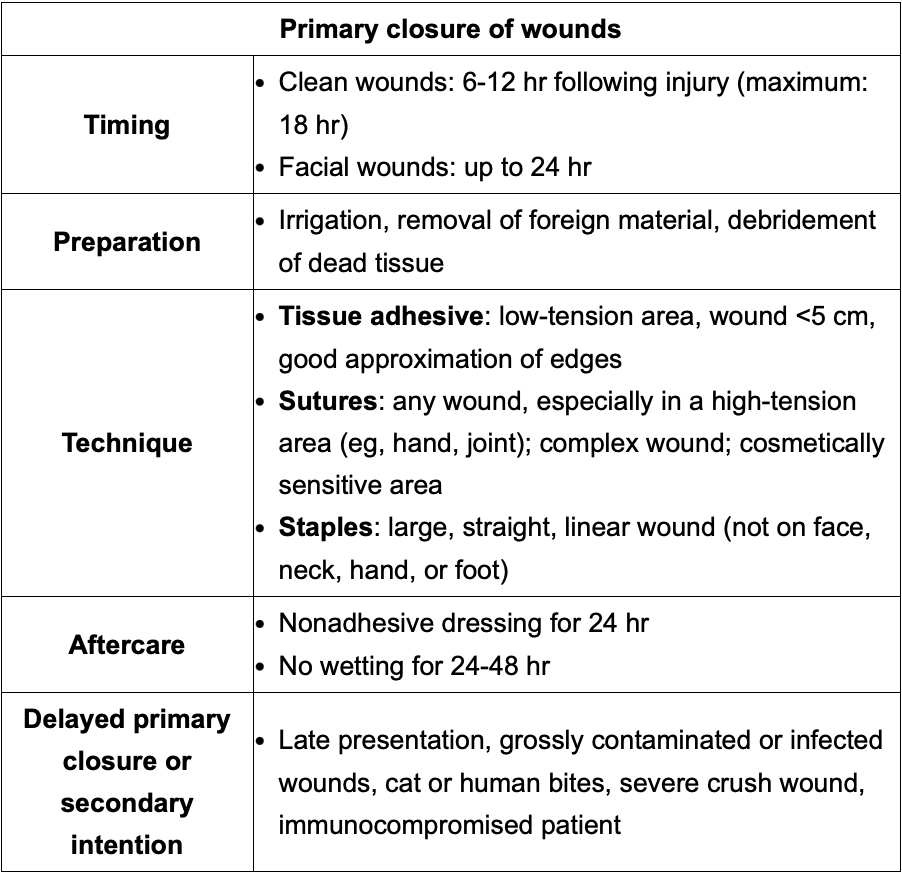
a) When to suture a wound and when to leave a wound open?
b) When is a wound to big to be taped?
c) What areas should be sutured 2/2 to tension?
a) Clean wound (6-12 hr) w/max 18 hr limit. Face: <24hrs
b) Sterile strip if wound <5cm
c) hand, joint, complex, irregular cut or cosmetic wounds.
In a F pt w/o her period but secondary sexual characters and blind vaginal pouch..what should I test her for? FSH/LH/Prolactin WNL
Consider mullein agenesis causing the blind ouch. Normal ovaries provide hormones. Women with uterine abnormalities often have renal defects, perform renal US
If thinking turner check ❤ echo for bicuspic aortic valve or aortic coarctation and bone density as low estrogen predisposes to Fx
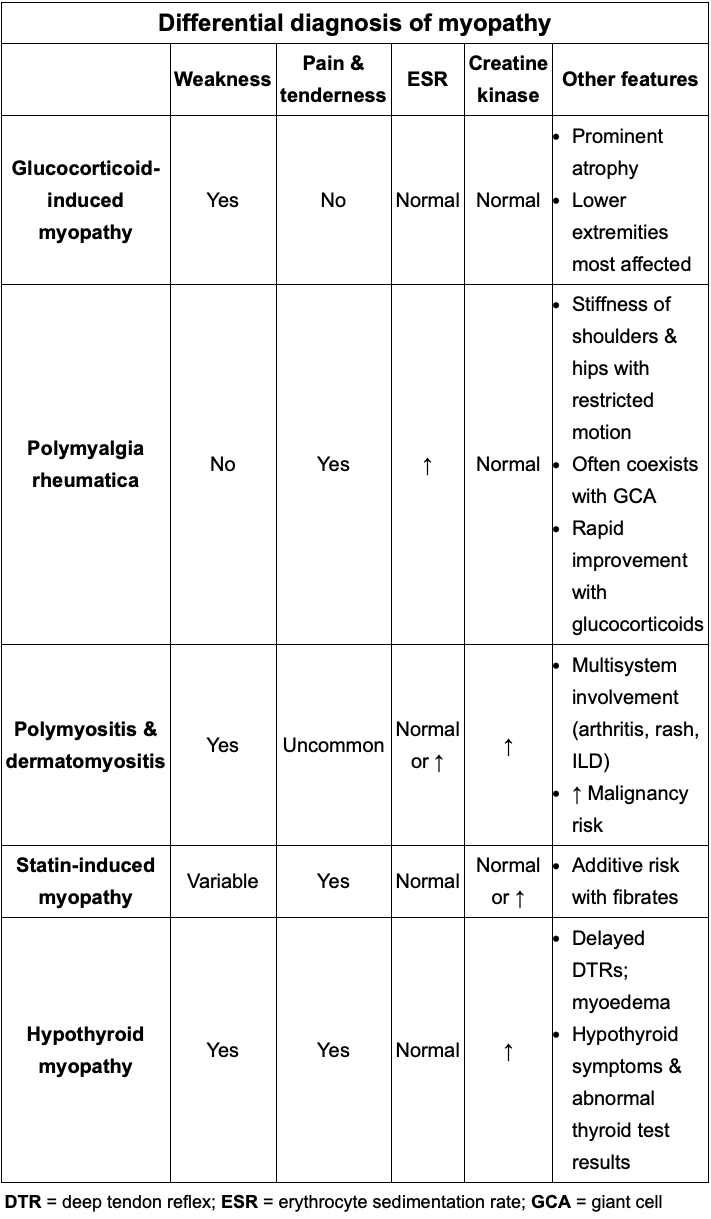
Review differential for myopathy
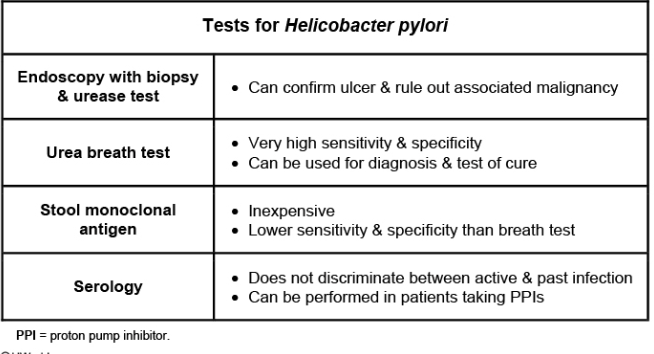
Review tests for H pylori
Remember tx fails 10%-30% of the time, perform test of cure.
Stool has lowest sensitivity and specificity.
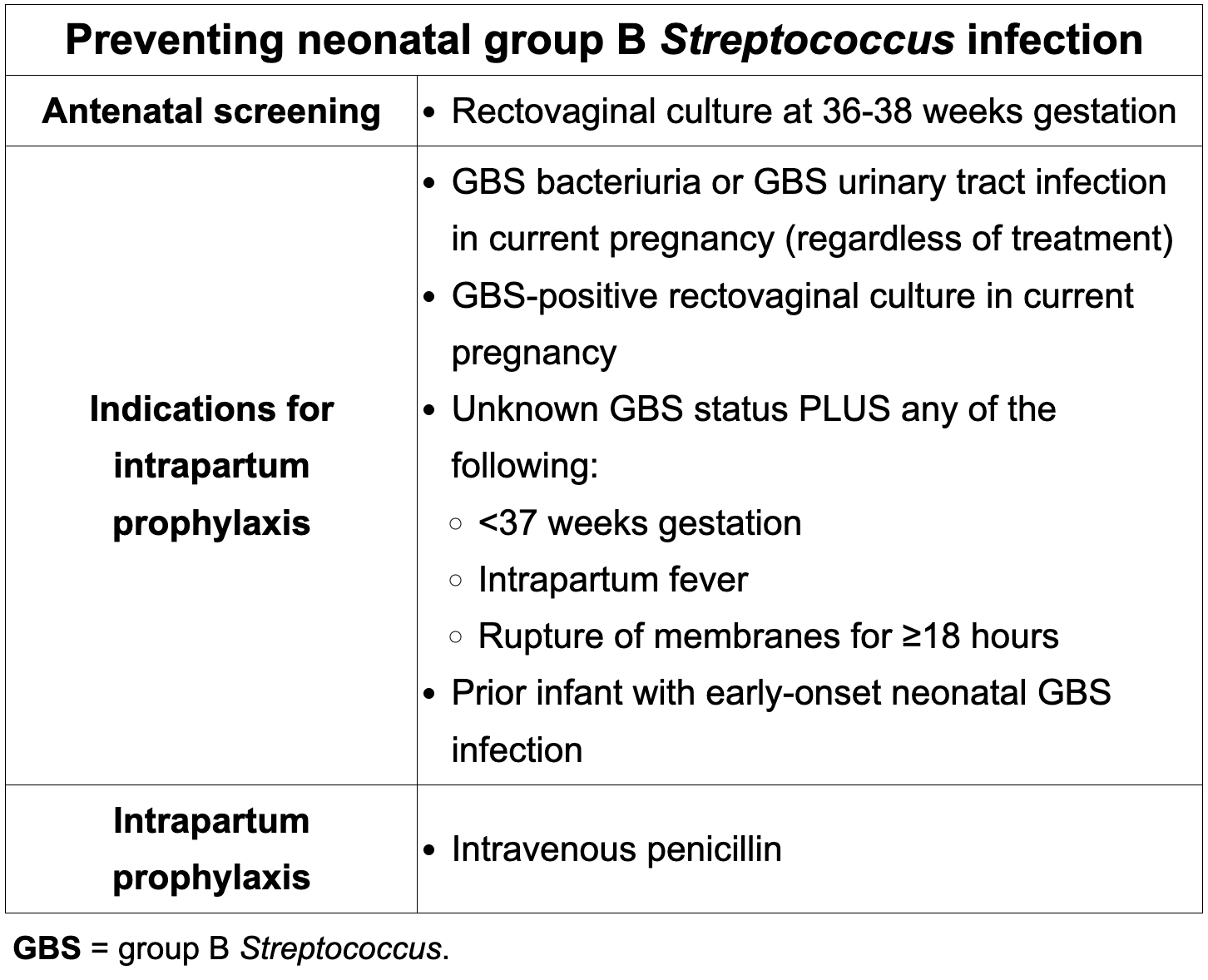
In which cases of GBS unknown status should prophylactic penicillin be given?
-Preterm delivery (<37 weeks)
-ROM >18 hours @any gestational age
-Intrapartum fever (III, Chorio)
-GBS Bacteriuria in current pregnancy
-Prior delivery of infant w/early onset neonatal GBS disease (sepsis, meningitis, pneumonia, etc)
Remember GBS status she be checked between weeks 36-38 and is only valid for 5 weeks
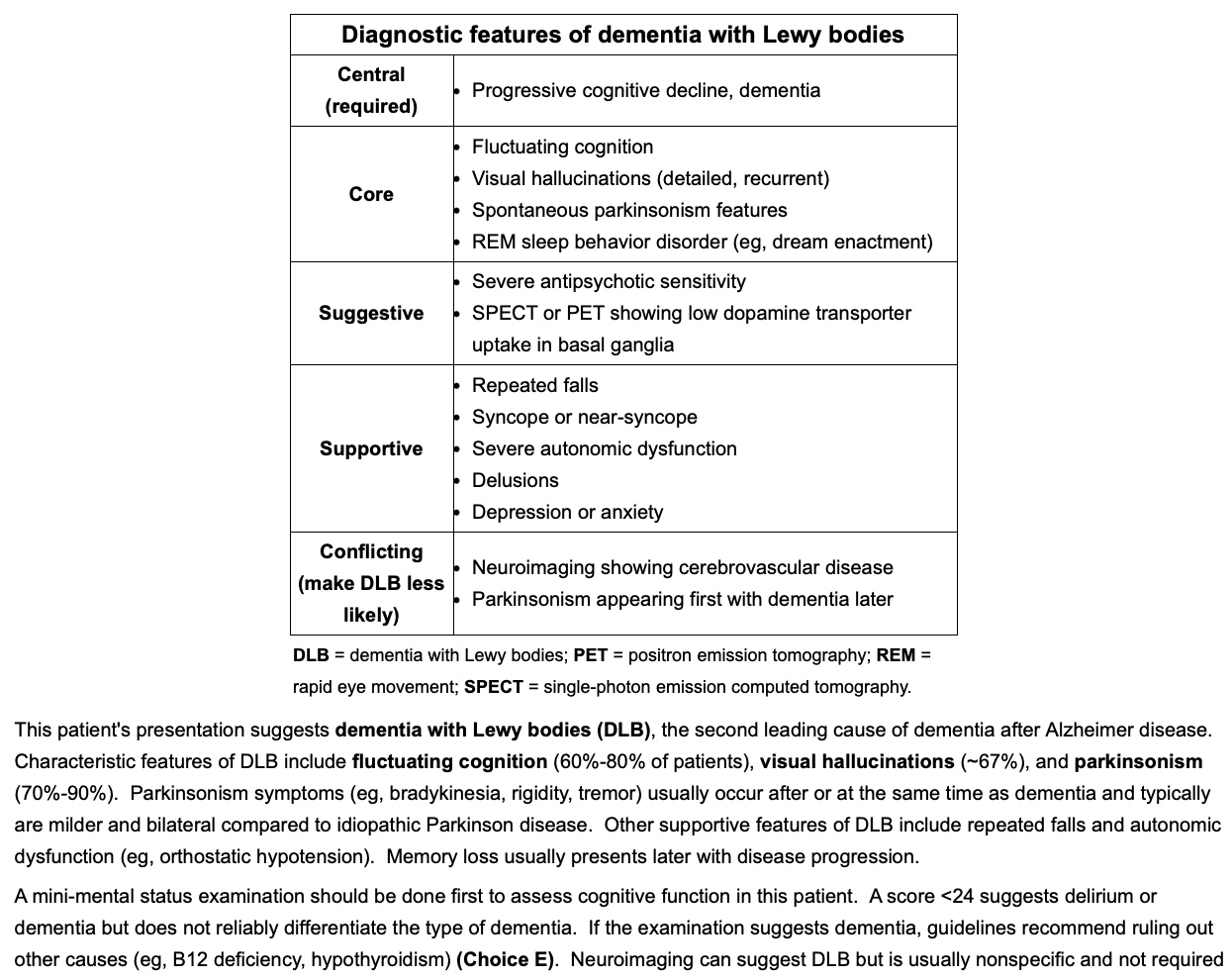
Dx. Features of dementia w/ Lewy bodies?
Which is first? Parkinson or dementia?
Dementia first then parkinson’s
What are the indications for TRUS prostate biopsy?
-Prostate nodule, induration or asymmetry on digital rectal exam (regardless of PSA)
-PSA >7 on initial test
-PSA >4 on a repeat
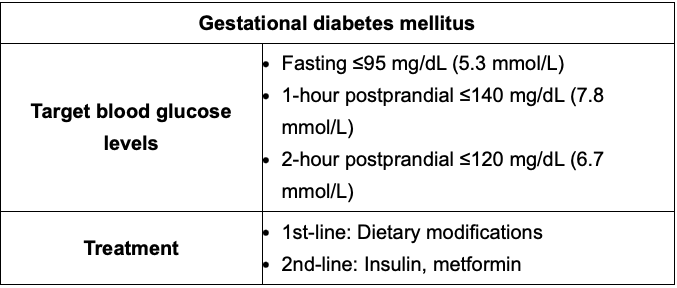
Gestational diabetes goals? What week to screen and when to begin treatment?
Screen: 24-28
Goal:
Fasting= <95
1 hr PP= <140
2 hr PP= <120
Tx: Hyperglycemia >50% above blood glucose target despite nutrition, should start insulin, metformin is alternative.
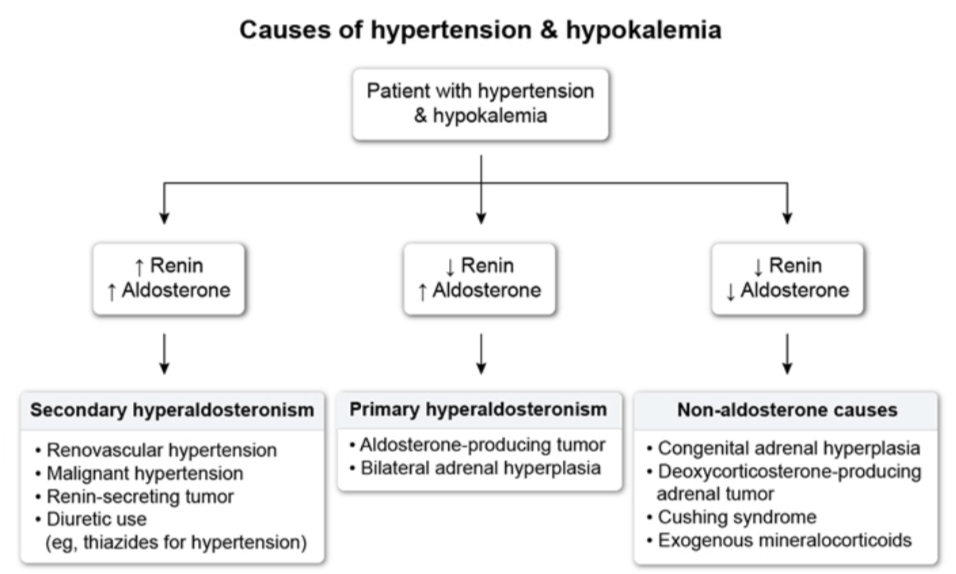
Interpretation of HTN + K levels
Always look for mild hypernatremia (143-147), met alkalosis, hypokalemia.
Dx: Plasma Aldosterone concentration / plasma renin activity= >20 + Aldosterone >15 suggests PHA.
B/I adrenalhyperplasia should be managed w/aldosterone antagonists.
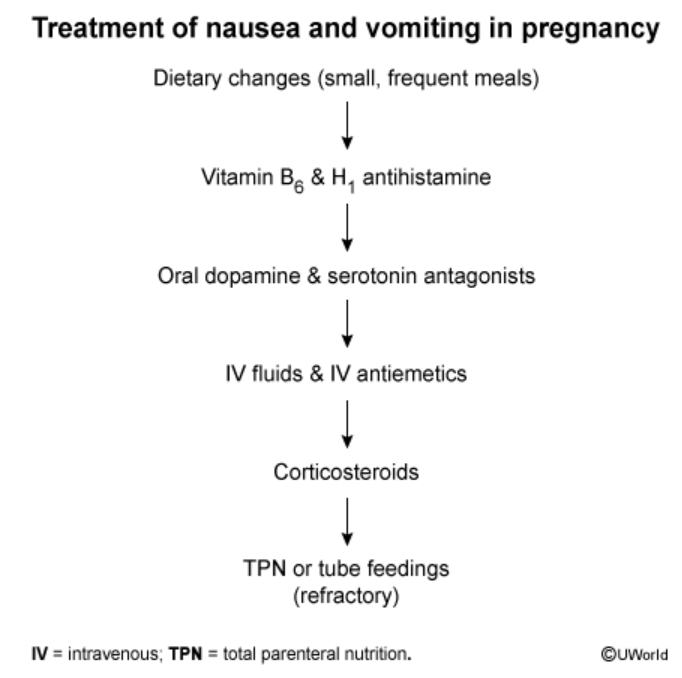
Mgt of Nausea and vomiting during pregnancy
1) Dietary changes (small portions, avoid certain foods)
2) B6 + antihistamine (Doxylamine)
3) Dopamine or serotonin —Ondanestron (can cause cardiac abnormalities so 3rd line) , Metoclopramide (can cause terdive dyskinesia)
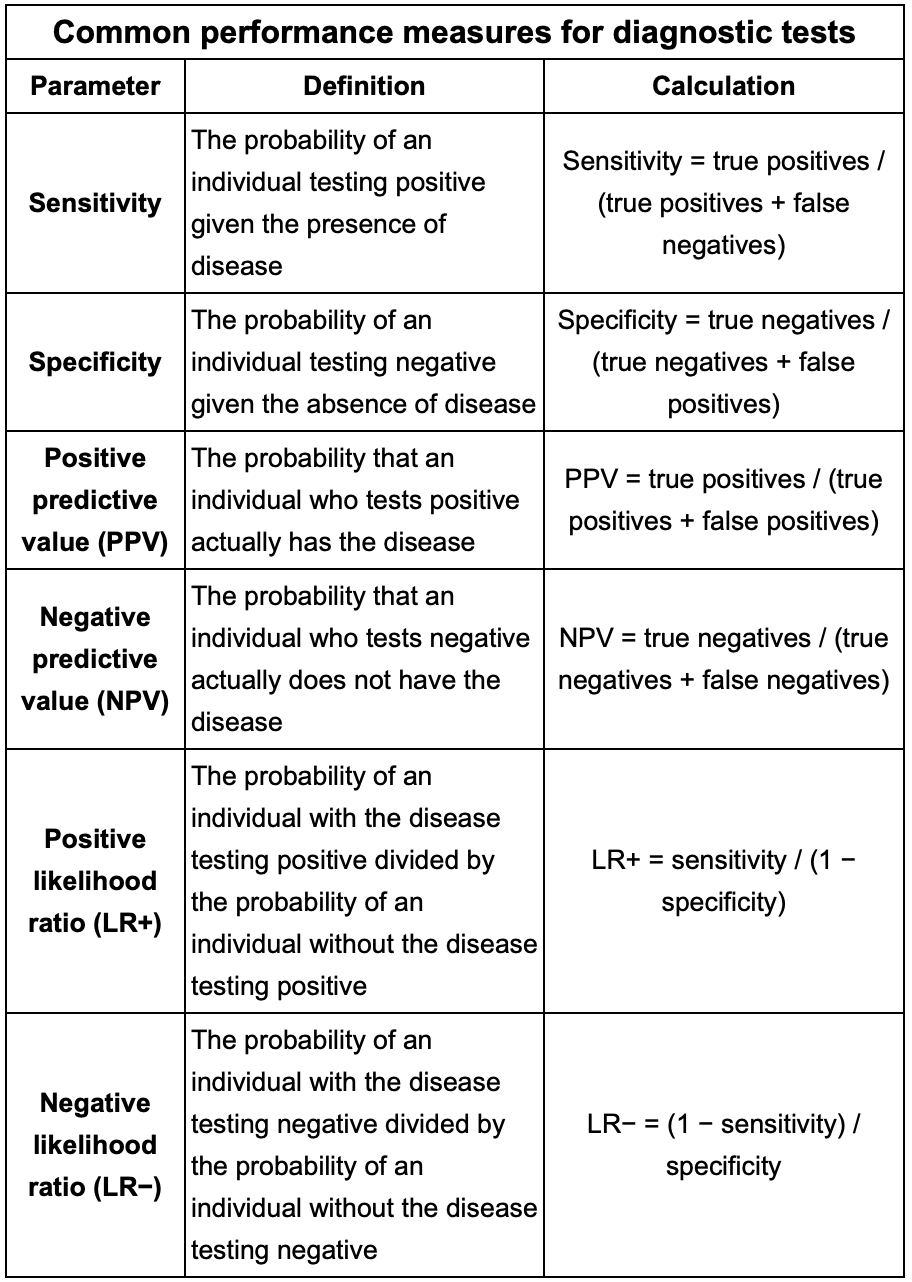
Formulas to know for the test:
Sensitivity
Specificity
PPV
NPV
+LR
-LR
When a patient has inadequate bowel preparation on Colonoscopy, when should it be repeated?
1 year
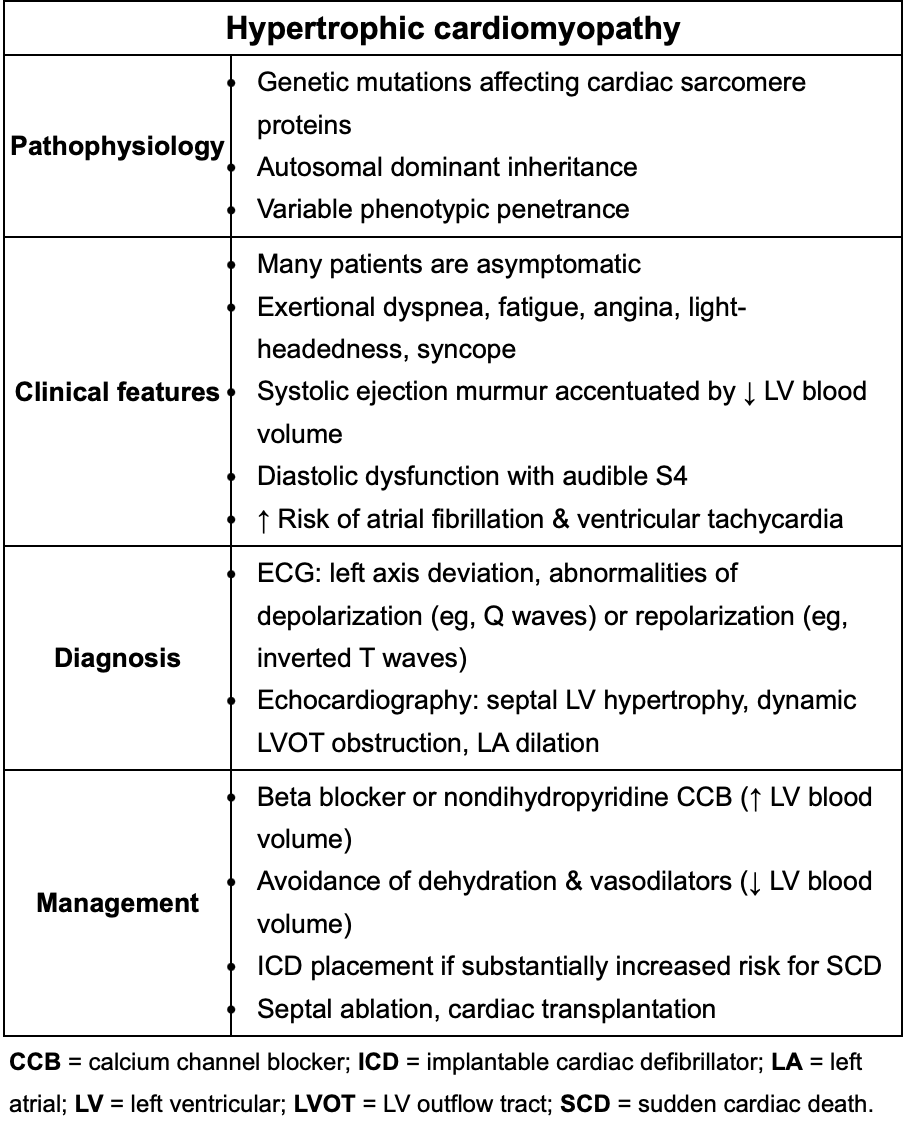
Quick review of HOCM
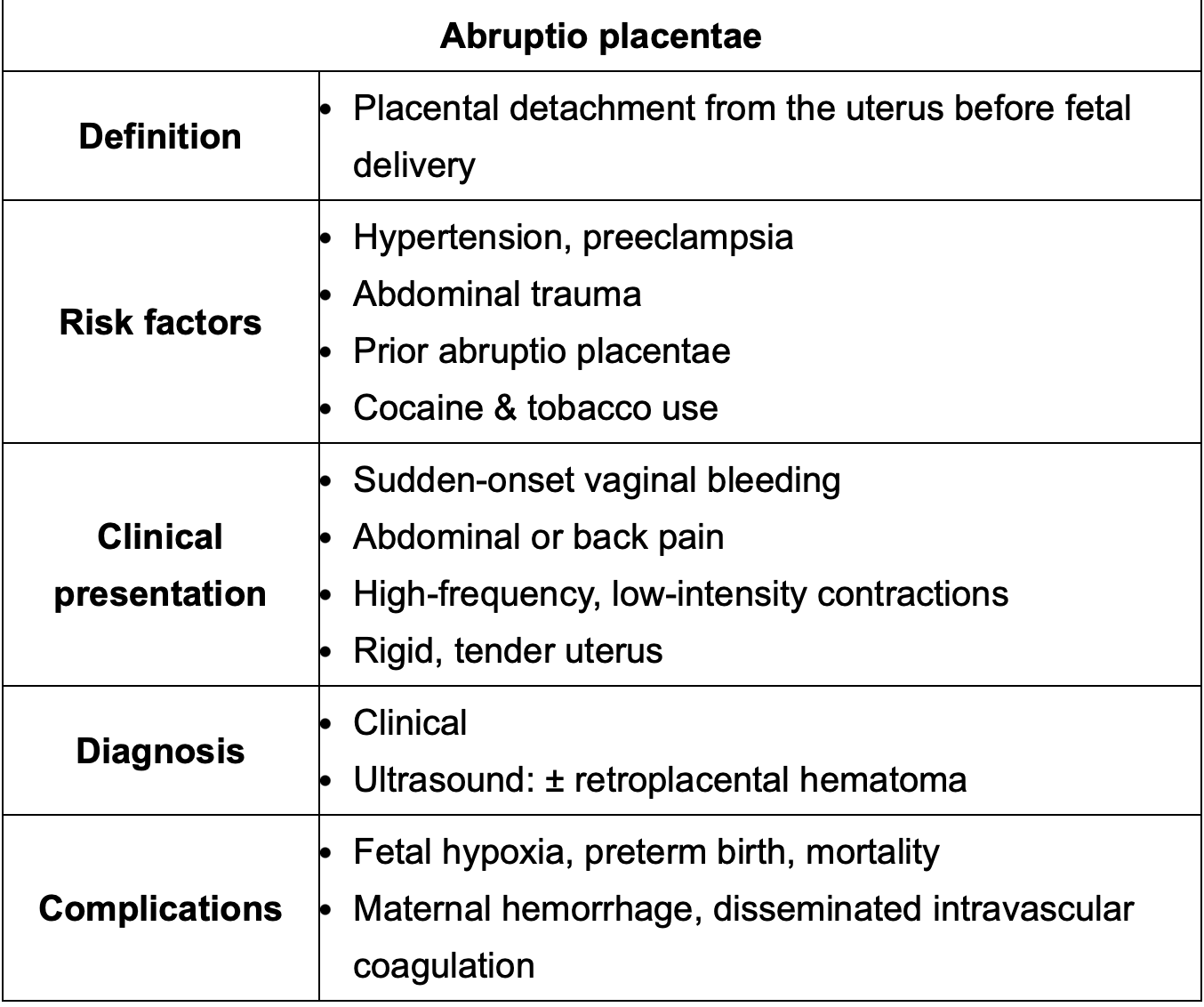
Main difference between uterine rupture and abruptio placentae?
In uterine rupture contractions STOP where in abrupt placenta they become more frequent but less intense.
It’s not just caused by trauma! Cocaine, pre-e and HTN cause it as well.
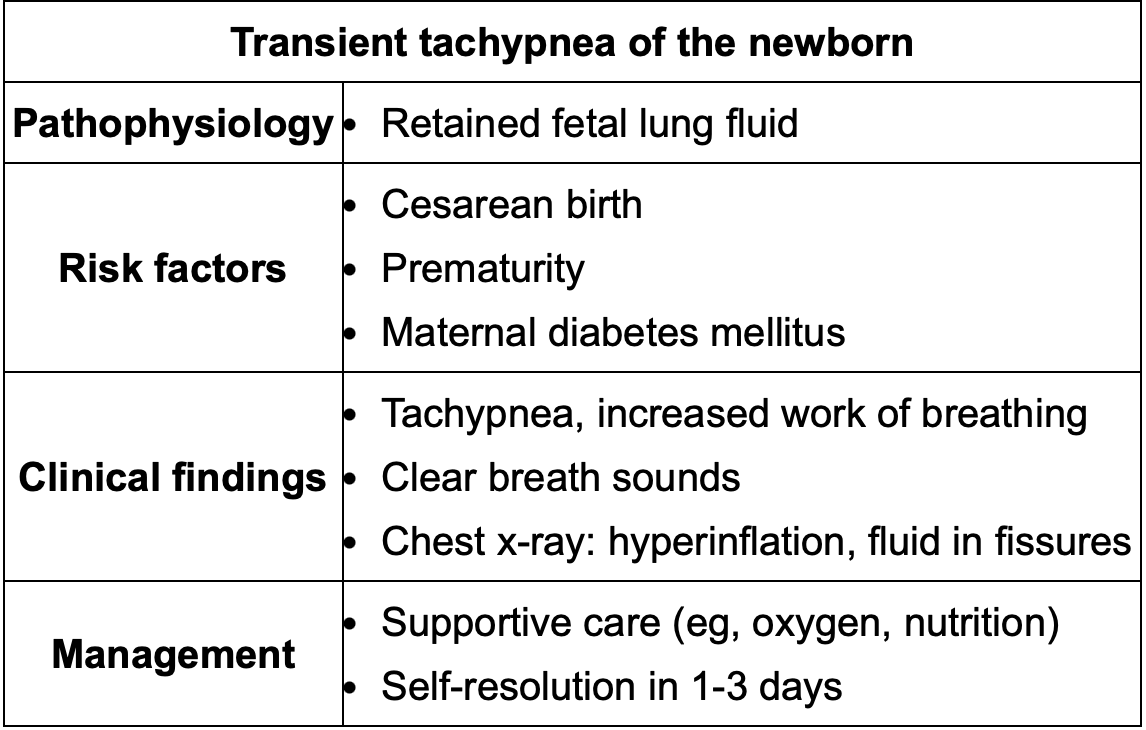
What is elevated RR for a newborn? Review TT
>60
Remember C-section baby’s have higher risk than vaginal delivery. Can last up to 3d.
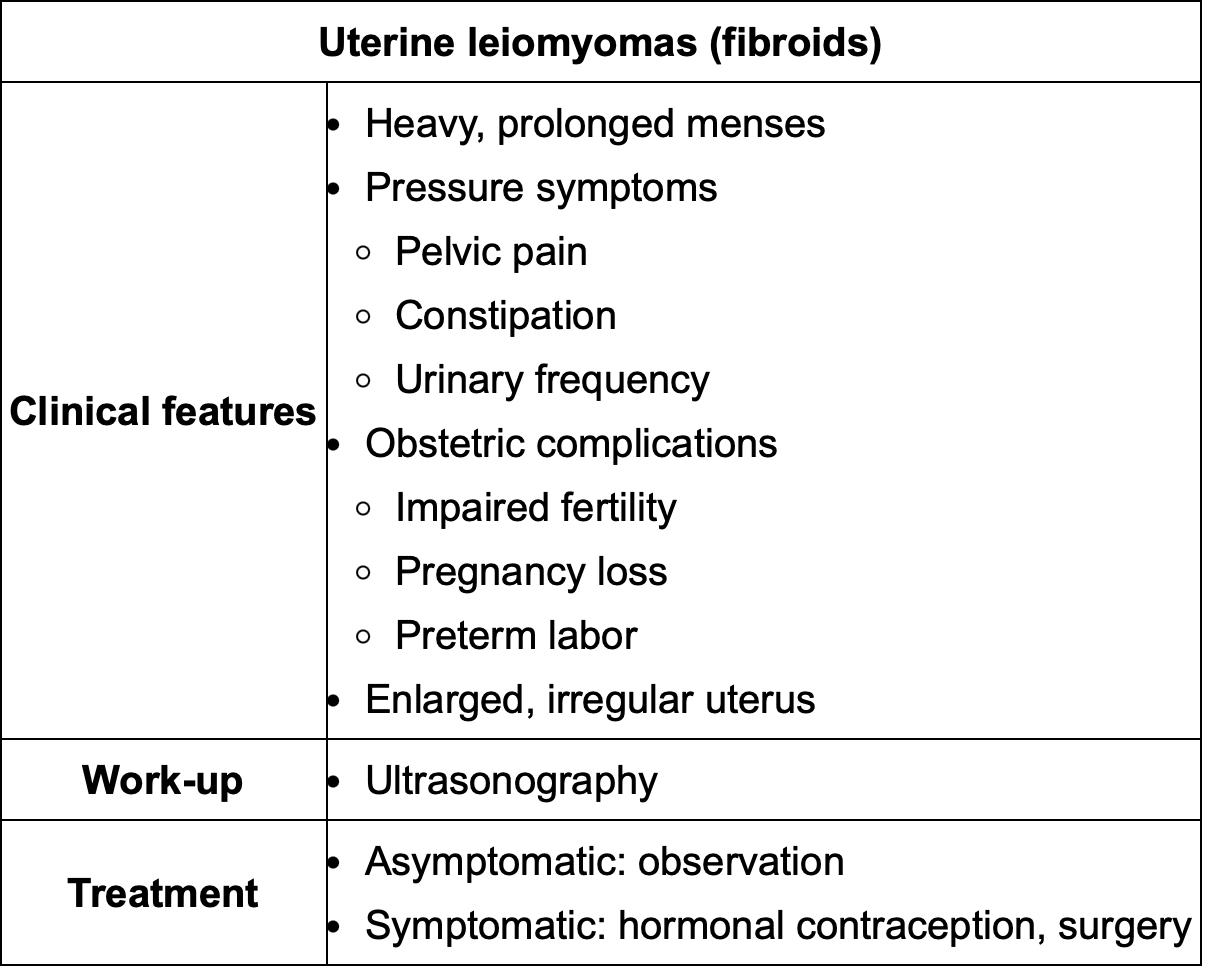
Easy way to differentiate endometriosis vs uterine fibroids?
Endometriosis doesnt necessarily need to be in the uterus, only uterine fibroids will have enlarged, irregular shaped uterus on PE.
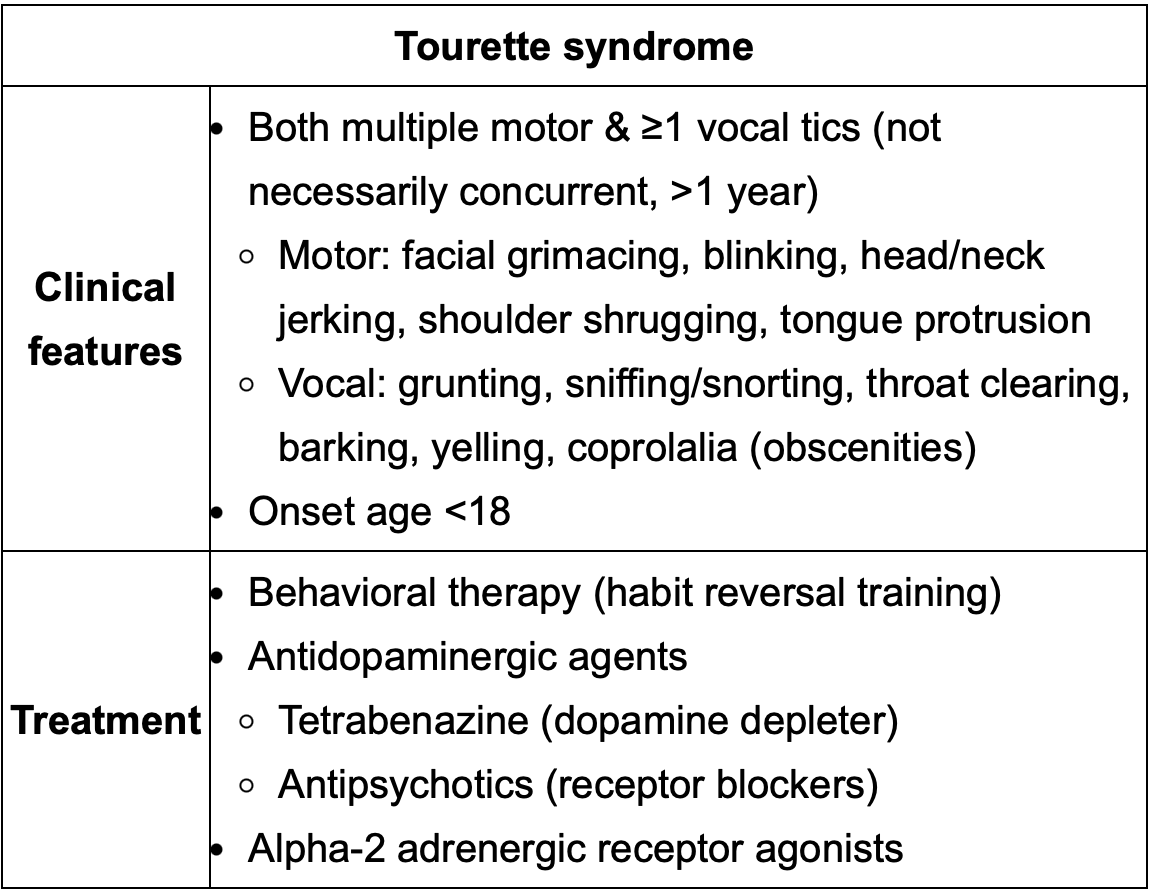
Medication to be used for Tourette’s
Tetrabenazine
Behavioral therapy
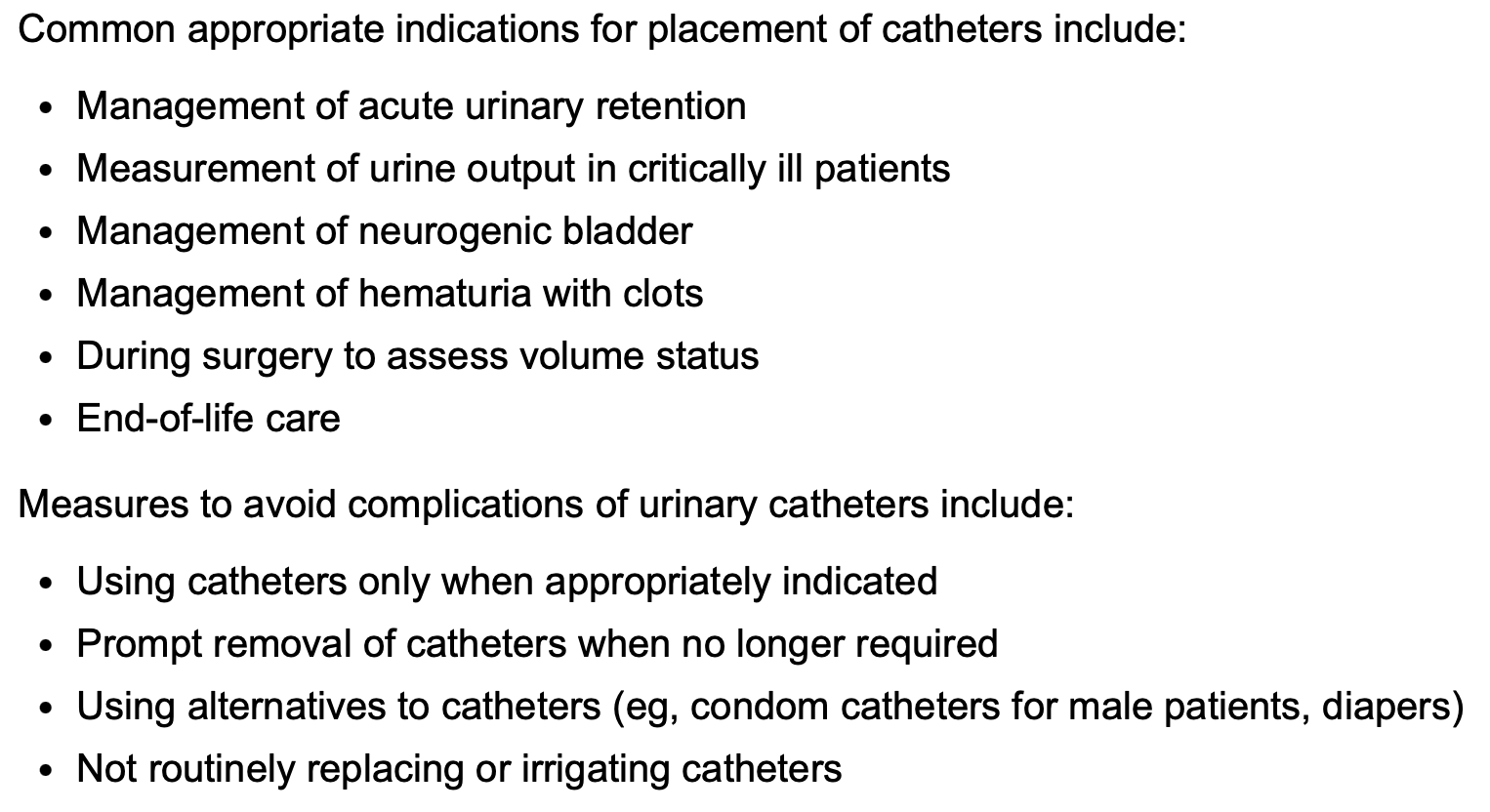
Indications for urinary catheter management
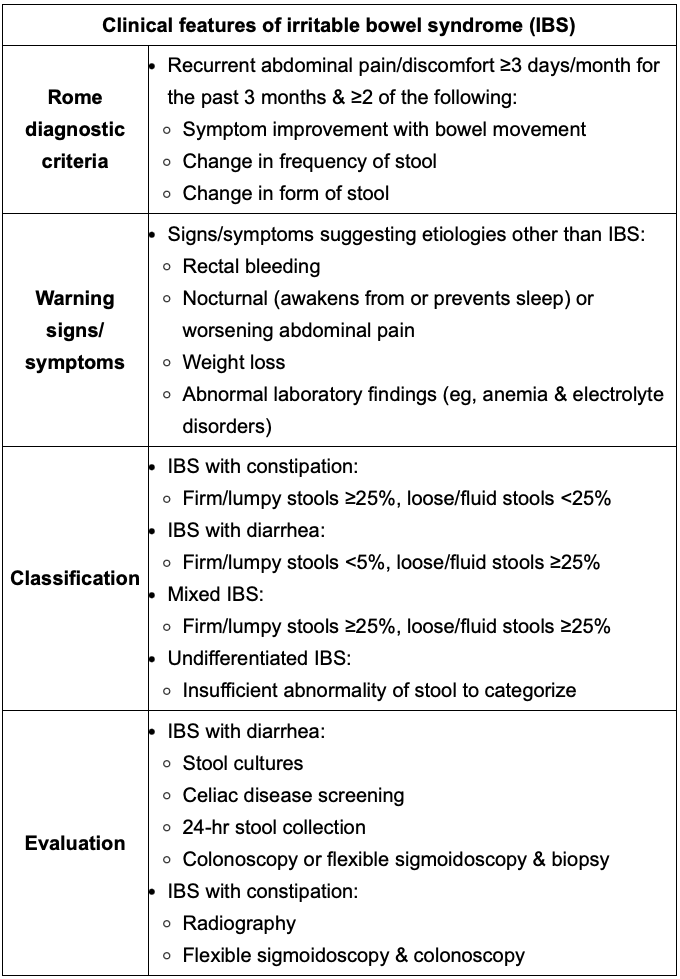
Definition of IBS w/ constipation vs w/ Diarrhea vs mixed vs undifferentiated IBS.
-Review Rome and Dx testing
W/constipation: Firm/lumpy stool >25%, loose/fluid stools <25%
W/diarrhea: Firm/lumpy stool <5%, loose/fluid stools >25%
Mixed IBS: Firm/lumpy stools >25%, loose/fluid stools >25%
Undifferentiated IBS: Insufficient abnormality of stool to categorize
Main difference between Parkinson tremor and essential tremor?
Essential: B/I action tremor of the hands, improves w/OH
Parkinson: Restring tremor, asymmetric, pill rolling, OH does not change it.
In a patient with a boxers fx of the 5th metacarpal with no rotation and a 25 degree volar angulation, what is the best next step?
Up to 40° of volar angulation is acceptable for fifth metacarpal fractures. For second and third metacarpal fractures, less angulation is acceptable. Appropriate treatment is a gutter splint.
Risk factors for delirium in hospitalized patients?
Delirium occurs in 11%–42% of hospitalized patients. Risk factors for delirium in hospitalized patients
include vision impairment, hearing impairment, dehydration, immobility, cognitive impairment, and sleep
deprivation.
Main cardiac S/E of typical and atypical antipsychotics?
Prolongation of the QTc interval, resulting in torsades
de pointes, ventricular tachycardia, and sudden death. The best way of monitoring the QTc interval is
electrocardiography.
How does presbycusis (aging hearing loss) present?
It’s gradual in onset, bilateral, symmetric, and sensorineural.
Which is the most accurate way of estimating gestational age?
Estimation of gestational age by ultrasound is most accurate early in the first trimester and begins to decline by 22 weeks gestation. Crown-rump length is typically used to estimate gestational age before 13 weeks gestation.
Initial treatment for Dyspareunia (painful sexual intercourse occurring with both initial entry and deep penetration)?
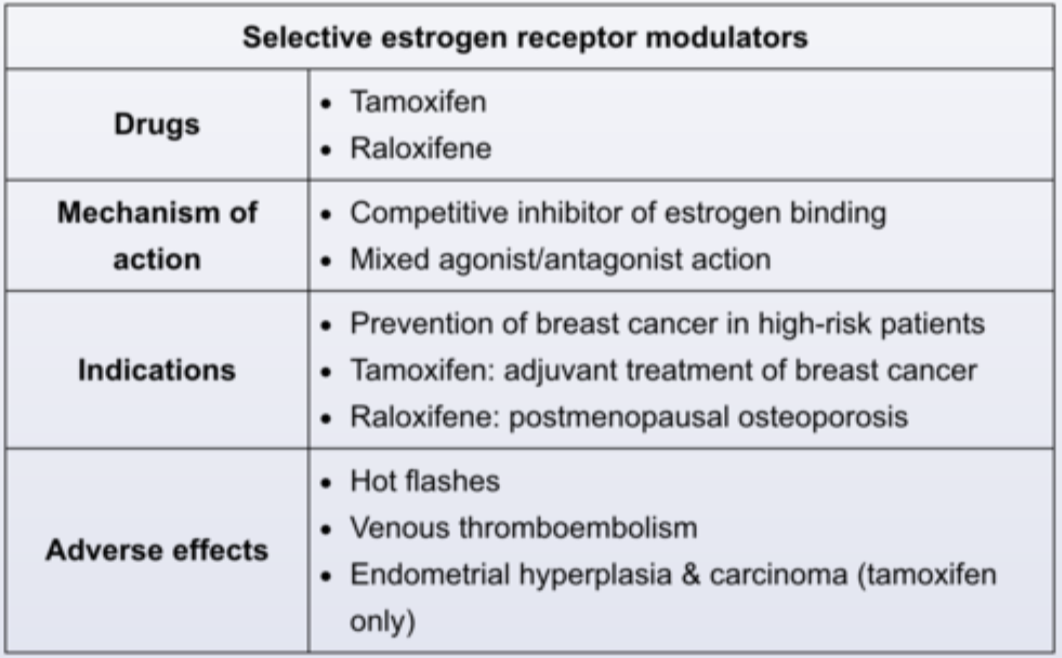
It may be treated with vaginal moisturizers or lubricants, but further treatment may be needed. Topical estrogen is the most effective initial therapy and is much more cost-effective than other alternatives. For patients with a preference for non-estrogen treatment, ospemifene is a selective estrogen receptor modulator. However, it costs more than $200 per month.
Timeline of symptoms for common food toxins:
-Staph
-Clostridium botulinum
-Clostridium perfringens
-Clostrium Difficile
Staphylococcal food poisoning symptoms usually begin 1–6 hours after ingestion and resolve within 24–48 hours. Foodborne botulism is most commonly found in homecanned foods, and symptoms begin 18–36 hours after ingestion. Clostridium perfringens is transmitted in feces and water, and symptoms begin 6–24 hours after ingestion. Clostridium difficile is associated with antibiotic use.
What’s the expected Cr increase when starting ACE-I and by when should it go back to normal? If BP is still high what should you always think of and how to R/O?
The renal protective effects of ACE inhibitors have been shown to be so efficacious in long-term trials as to warrant tolerating up to a 30% increase in baseline serum creatinine level within the first 6–8 weeks of therapy,
Think RAS vs FMD , R/O w/ US
Signs of alarm in patients with epigastric pain? (Name 5)
-age >n60
-persistent vomiting
-unintended weight loss
-dysphagia or odynophagia
-gastrointestinal bleeding
-palpable mass
-lymphadenopathy
-night waking,
-symptoms that have a sudden/recent onset or are progressive in character
-family history of gastrointestinal cancer
-poor response to empiric therapy.
In what patient population is routine cancer screening not recommended?
Per choosing wisely campaign, patients with end-stage renal disease with limited life expectancy who are not candidates for kidney transplantation.
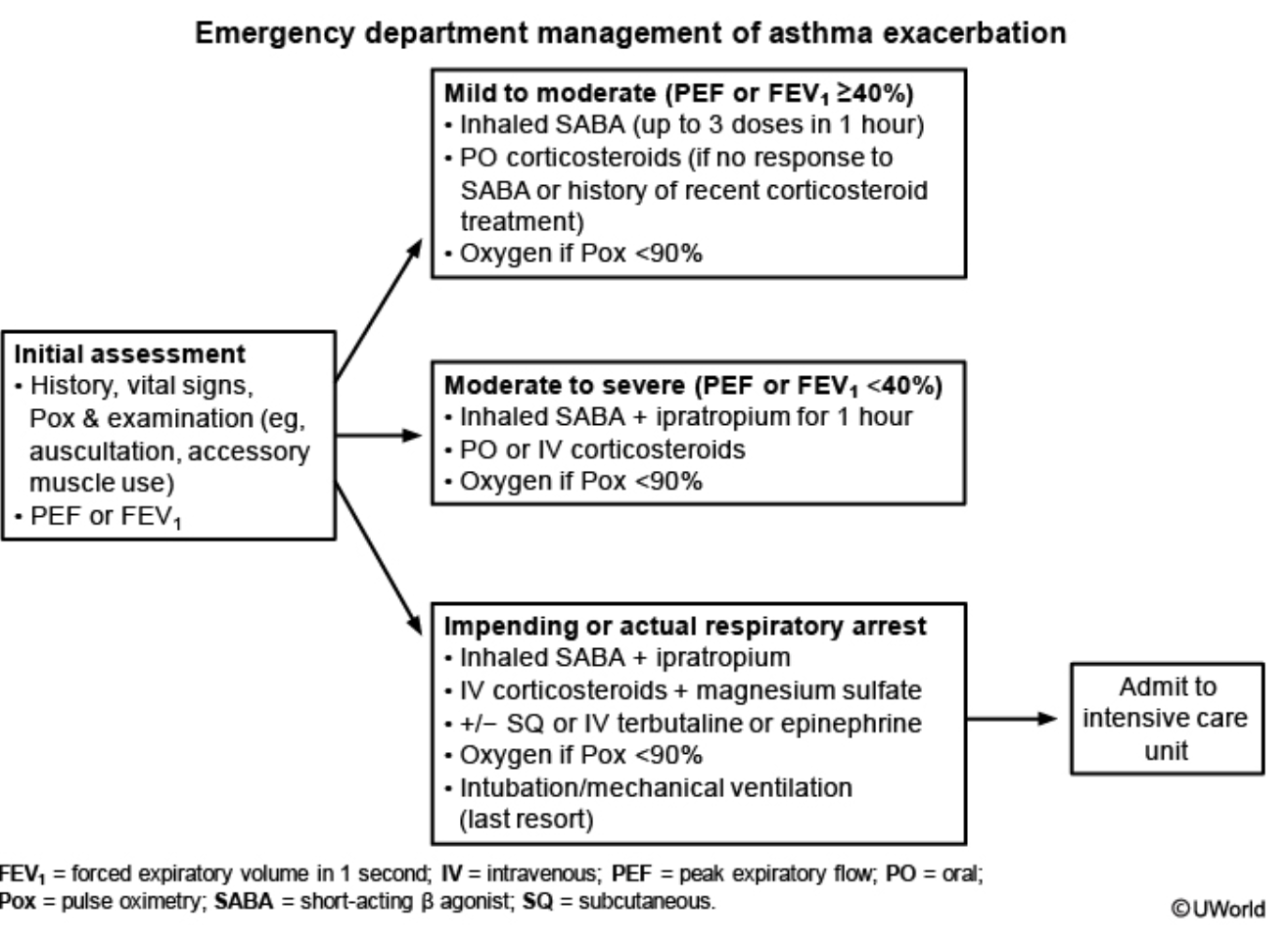
1) Management of moderate to severe asthma exacerbations?
2) Medication combo shown to decrease the risk of hospitalization when compared to use of B agonist alone?
1) View image
2) Albuterol + Ipratropium
1) IV atb Tx for GBS + mom.
2) What if Penicillin allergy exists?
1) Penicillin, Ampicillin
2) Cefazolin (if mild pen allergy such as rash)
3) Clindamycin (If severe pen allergy such as anaphylaxis, respiratory distress, urticaria)
4) Vancomycin (If severe pen allergy AND Clindamycin is resistant to GBS)
Clinical presentation of Acute bacterial sinusitis and treatment
Amoxicillin/clavulanate (Augmentin)
Indicated for acute bacterial sinusitis: symptoms ≥10 days without improvement, severe symptoms (fever ≥39 °C and purulent discharge ≥3–4 days), or “double-worsening.”
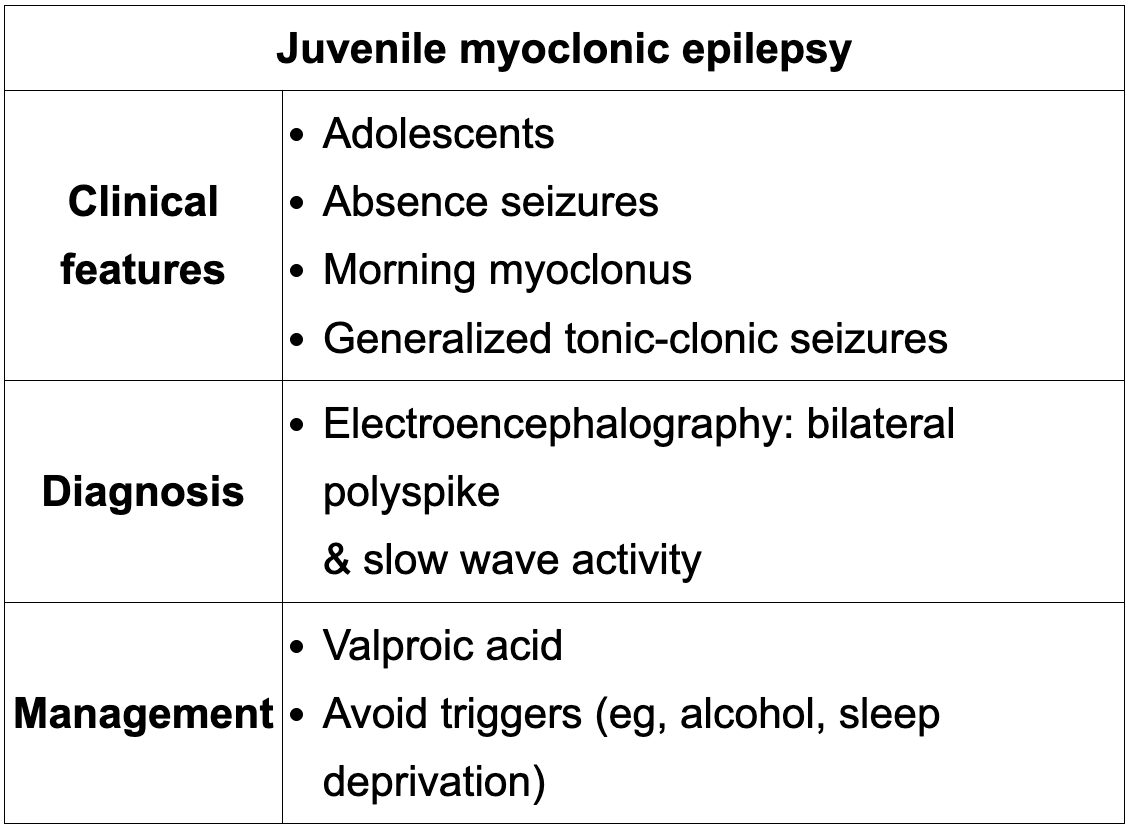
A 15-year-old boy has months of brief “spacing out” episodes, morning arm jerks, and now a generalized tonic-clonic seizure. EEG shows 4–6 Hz bilateral polyspike and slow wave discharges. What is the diagnosis and first-line treatment?
This presentation and EEG pattern are classic for juvenile myoclonic epilepsy (JME), a generalized idiopathic epilepsy of otherwise healthy adolescents characterized by absence seizures, morning myoclonic jerks, and generalized tonic-clonic seizures. The most appropriate first-line treatment is valproic acid, and narrow-spectrum agents such as carbamazepine, gabapentin, phenytoin, and pregabalin should be avoided because they may worsen JME
What are the true contraindications to breastfeeding, and why are chronic hepatitis B infection, maternal smoking, and stable buprenorphine therapy not among them?
Breastfeeding is contraindicated with maternal HIV infection, untreated active tuberculosis, herpetic or varicella lesions on the nipple, ongoing active substance use disorder, chemotherapy or radioactive isotope therapy, and in infants with galactosemia. Chronic hepatitis B infection is not a contraindication once the infant receives HBIG and starts the hepatitis B vaccine series, and maternal smoking and stable buprenorphine therapy are also not contraindications, so breastfeeding is still recommended because benefits outweigh risks.
Definition of infertility by age
Women under 35: infertility = no conception after 12 months of regular, unprotected intercourse.
Women Over 35: infertility = no conception after 6 months of regular, unprotected intercourse.
Front:
38-year-old woman with constipation, painless bright red blood coating the stool and dripping into the toilet at the end of defecation; no abdominal or rectal pain, no weight loss, no family history of colon cancer. Most likely cause and initial evaluation? What important differential also causes bleeding?
Back:
Diagnosis: Internal hemorrhoids.
Key features: Painless BRBPR, blood coating stool or dripping into toilet, associated with constipation, no systemic or alarm features.
Important differential: Anal fissures also cause minimal bright red rectal bleeding but are classically associated with severe tearing pain with defecation, which is absent here.
Why not others: Anal fissure causes painful defecation; villous adenoma and diverticulosis more common in older adults; rectal ulcer usually has mucus discharge, incomplete evacuation, pelvic fullness.
Initial evaluation: Anoscopy in patients <40 without red flag features; sigmoidoscopy for 40–49 without red flags; colonoscopy if age >45, red flags, or no source found.
Front:
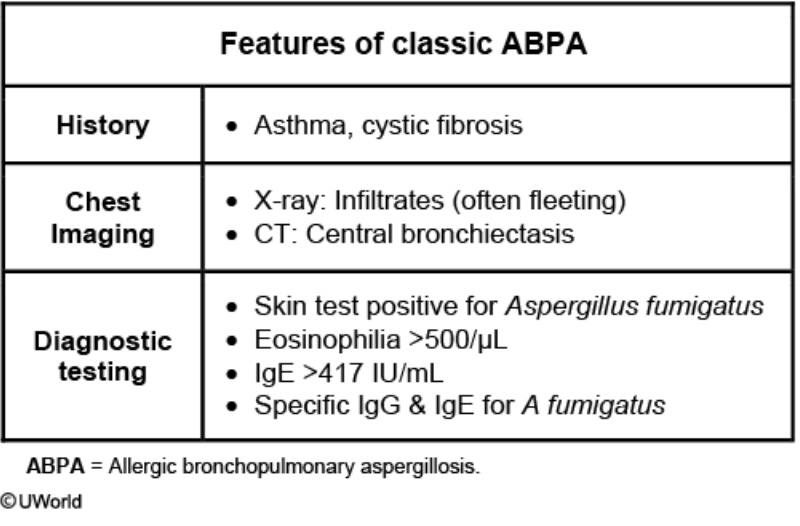
Allergic bronchopulmonary aspergillosis (ABPA) in a long-standing asthmatic: key features and first diagnostic test?
Hint: It improves with STEROIDS
Recurrent asthma exacerbations with fever, brown mucus plugs, peripheral eosinophilia, and bronchiectasis due to hypersensitivity to Aspergillus; initial diagnostic step is Aspergillus skin testing.
Summary:
Long standing asthma+ recurrent exacerbations with fever and thick brown sputum that improve with prednisone are classic for ABPA.
Idiopathic hypercalciuria with recurrent calcium oxalate stones: key dietary changes to reduce stone formation?
Increase fluids, maintain normal dietary calcium, increase fruits/vegetables (citrate), and restrict sodium and animal protein to lower urinary calcium and stone risk; low-calcium diets are harmful.
What Percentage of the body involved in Steven Johnson syndrome vs. TEN?
SJS= <10%
TEN= 10-30%
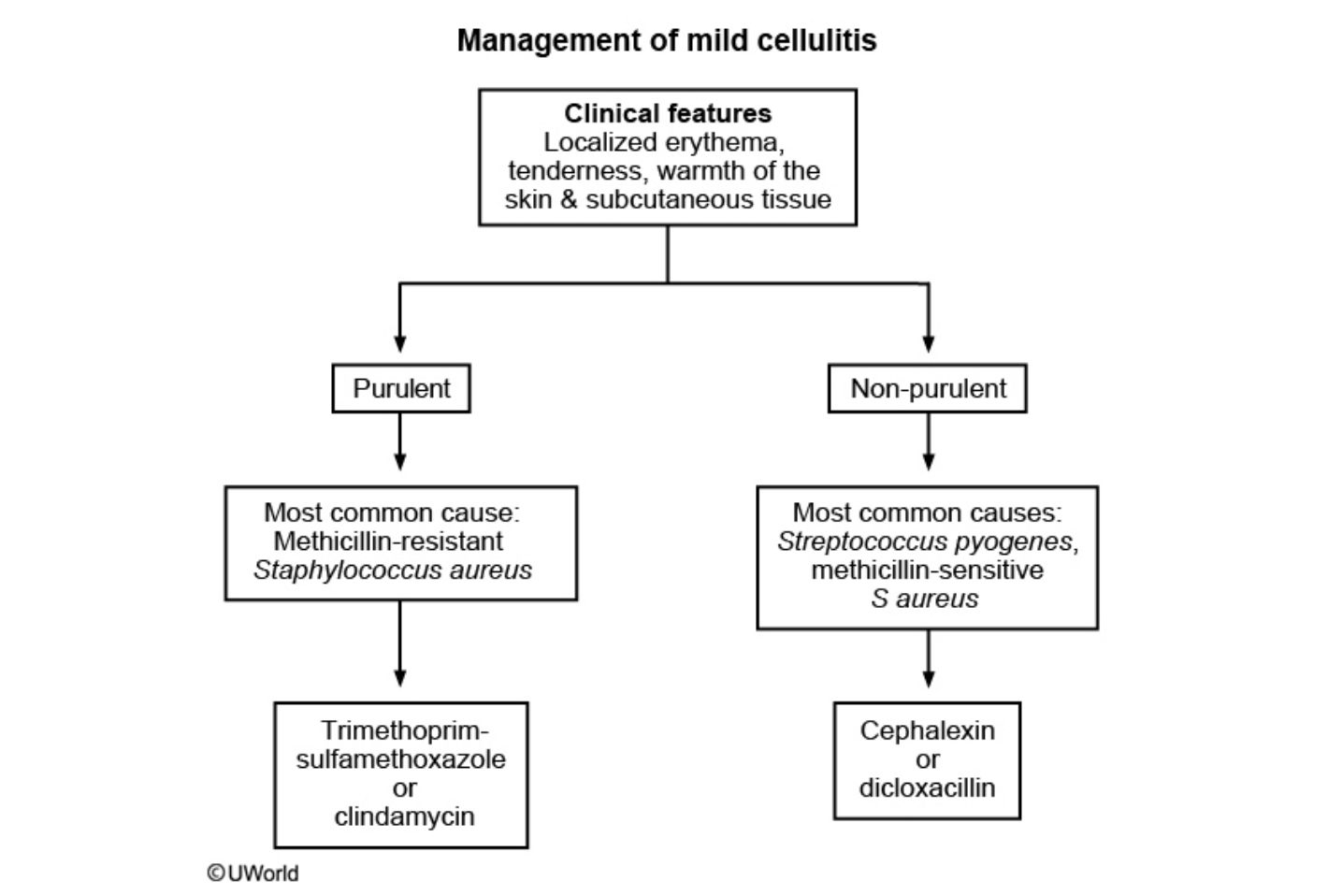
Management of Cellulitis when purulent vs non purulent
Purulent often associated to MRSA= Bactrim
Non-purulent associated to S. Pyogenes= Dicloxacillin or Keflex
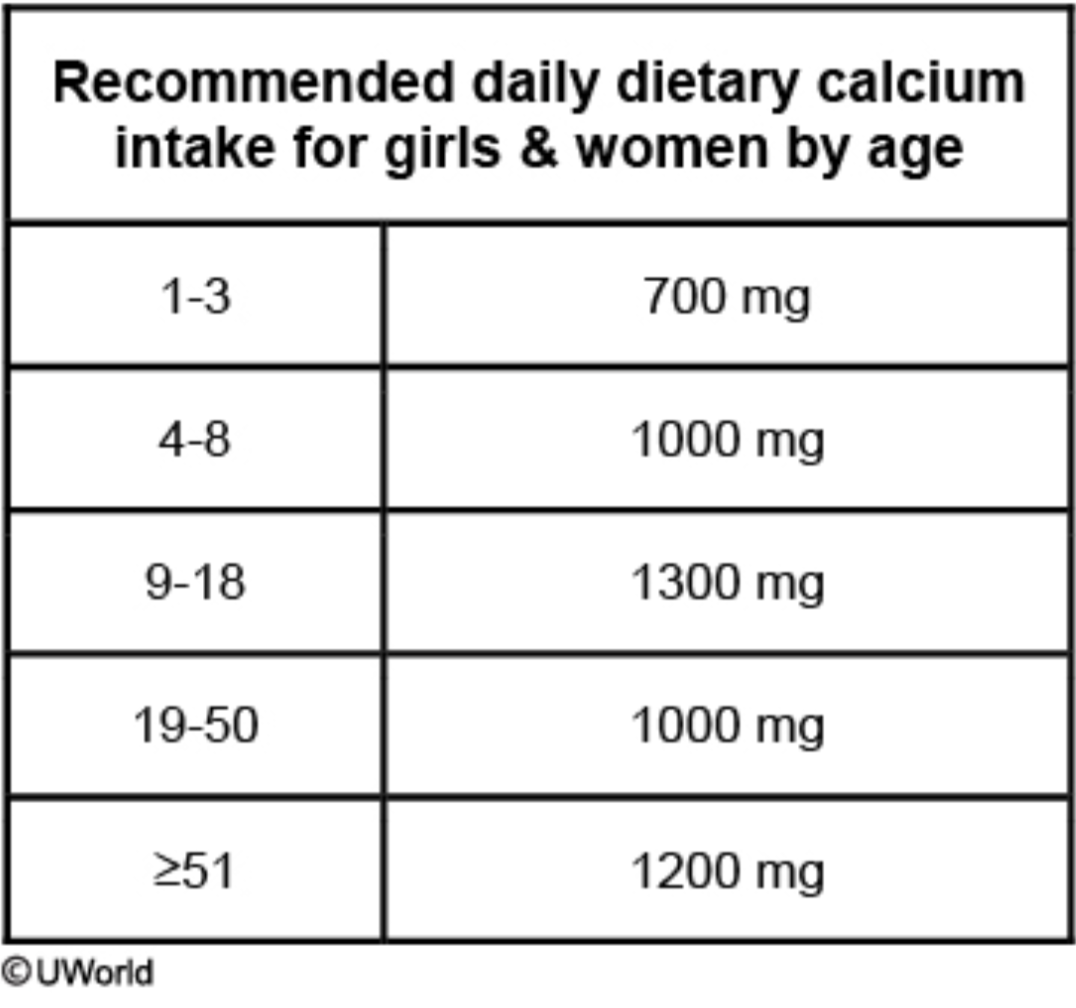
Age recommendations for Calcium supplementation:
1-3=
4-8=
9-18=
19-50=
View chart
Indications for GBS intrapartum prophylaxis and when should I start screening?
Exceptions when dont screen just treat?
Start screening between weeks 36-38.
Indications to treat on the image.
Exception: GBS Bacteriuria or prior delivery complicated by neonatal GBS infection.
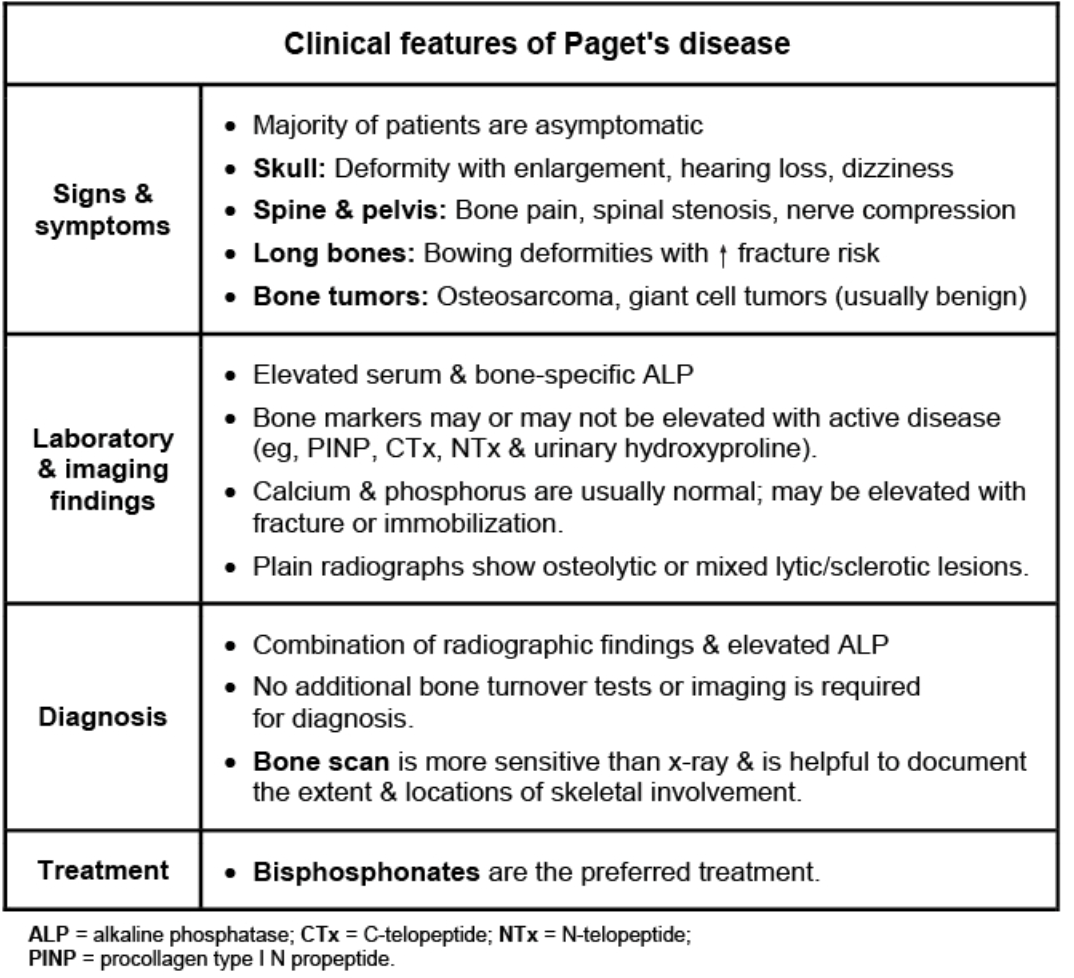
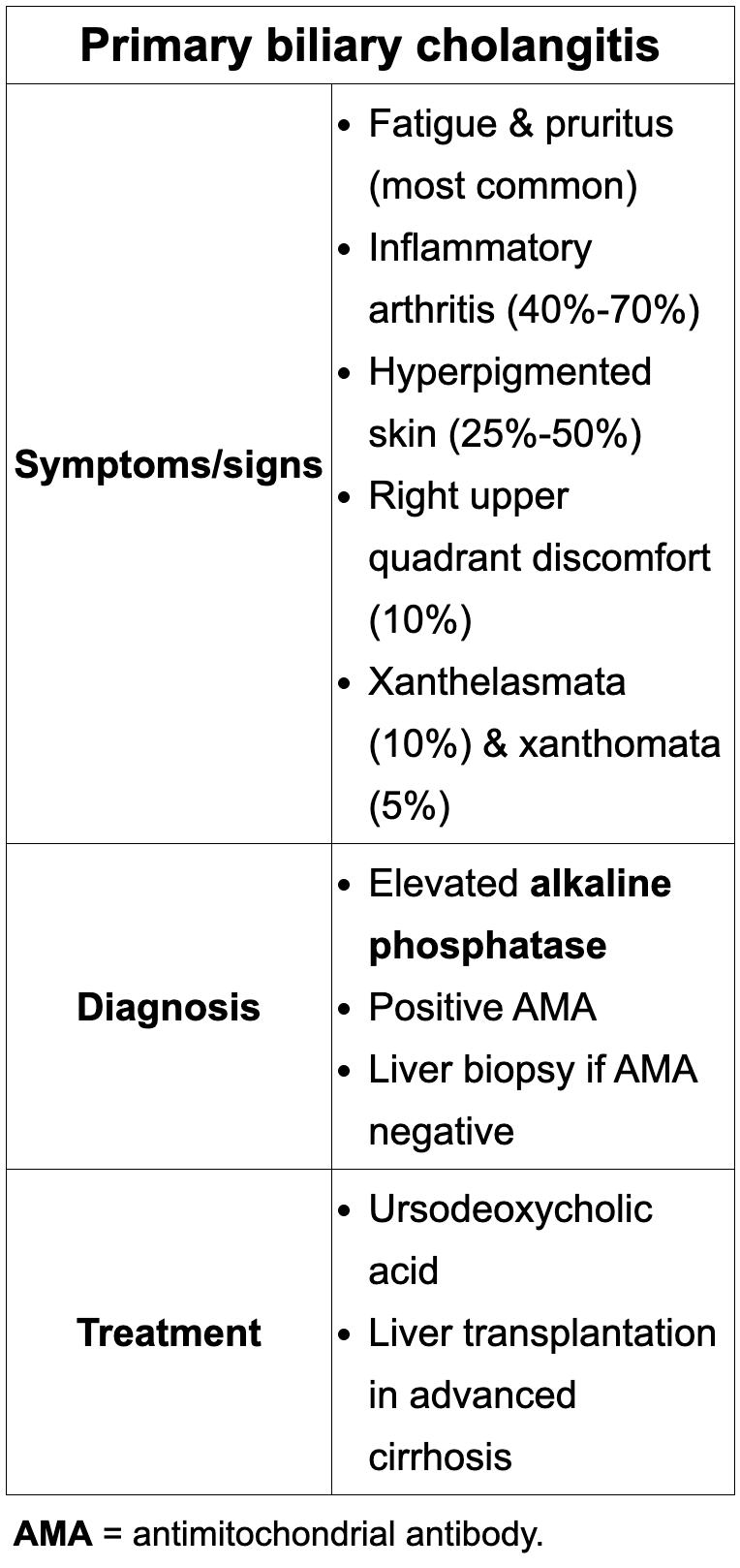
Educational objective: Cause of isolated elevated alkaline phosphatase in an asymptomatic elderly man with normal liver tests
Back (Definition):
Paget's disease of bone—characterized by high bone turnover leading to isolated elevation of alkaline phosphatase with normal AST/ALT, bilirubin, calcium, and often subtle bony enlargement in older adults.
What is the most common inherited thrombophilia?
Factor V Leiden (activated protein C resistance) is the most common inherited cause of venous thromboembolism in Caucasians and a classic cause of DVT/PE in otherwise healthy young adults.
Key pattern: first-time, unprovoked DVT/PE in a young adult with no clear risk factors → most likely underlying cause is Factor V Leiden (APC resistance).
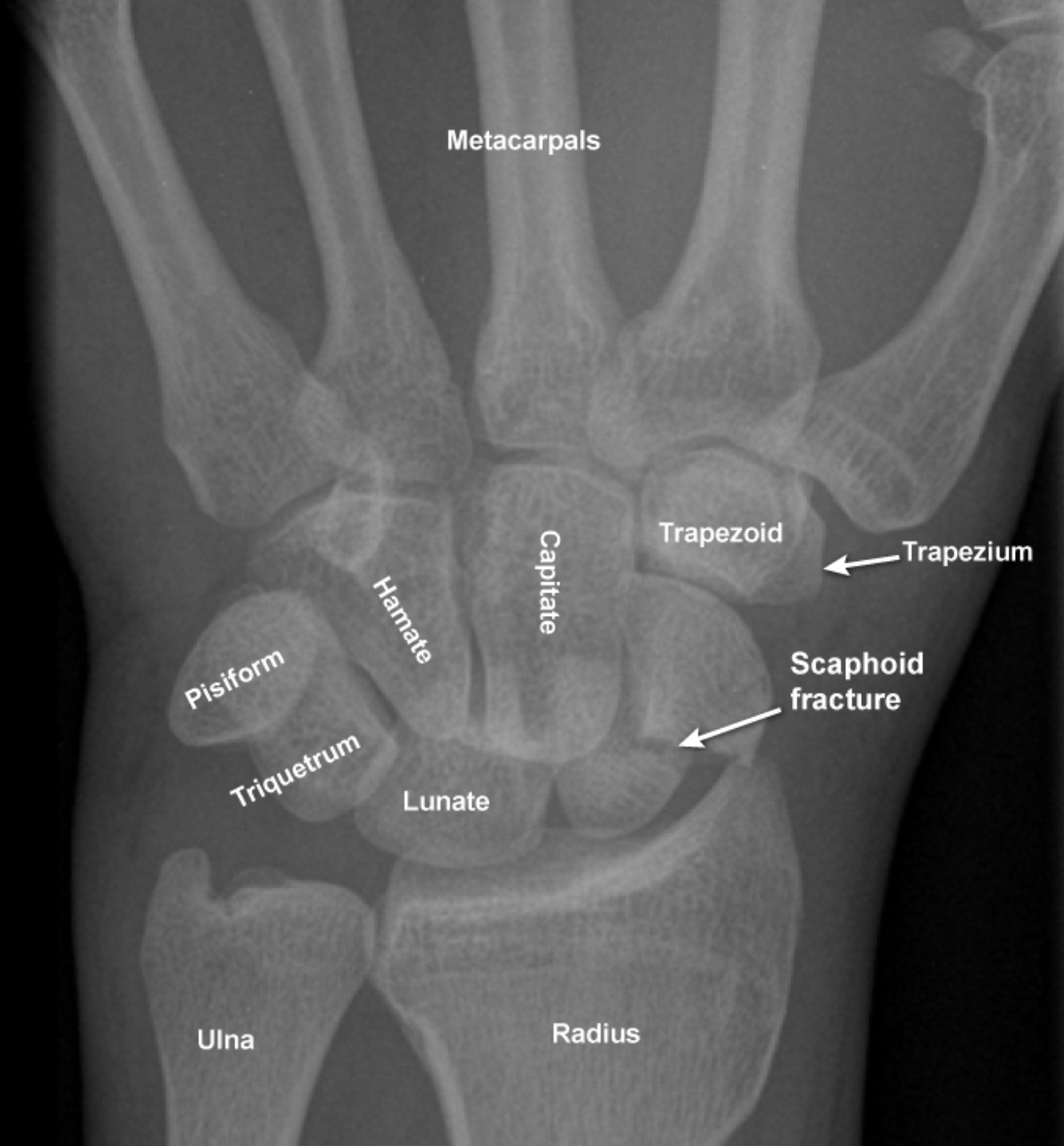
How does a scaphoid fracture look on x-ray?
View image
9-year-old boy with repetitive eye blinking, hemifacial spasms, shoulder shrugging, and repetitive throat clearing; normal exam otherwise. Parents worry about bullying. What is the most appropriate pharmacotherapy, and how are the other options used?
Key treatment options to remember for Tourette:
Behavioral therapy (habit reversal training).
Antipsychotics: haloperidol, pimozide, risperidone.
Alpha-2 agonists: clonidine, guanfacine.
Dopamine depleter: Tetrabenazine
![<p>Key treatment options to remember for Tourette:</p><ul><li><p class="my-2 [&+p]:mt-4 [&_strong:has(+br)]:inline-block [&_strong:has(+br)]:pb-2">Behavioral therapy (habit reversal training).</p></li><li><p class="my-2 [&+p]:mt-4 [&_strong:has(+br)]:inline-block [&_strong:has(+br)]:pb-2">Antipsychotics: haloperidol, pimozide, <strong>risperidone</strong>.</p></li><li><p class="my-2 [&+p]:mt-4 [&_strong:has(+br)]:inline-block [&_strong:has(+br)]:pb-2">Alpha-2 agonists: clonidine, guanfacine.</p></li><li><p class="my-2 [&+p]:mt-4 [&_strong:has(+br)]:inline-block [&_strong:has(+br)]:pb-2">Dopamine depleter: Tetrabenazine</p></li></ul><p></p>](https://knowt-user-attachments.s3.amazonaws.com/85016a41-7bce-4c7a-bb95-6d78fd66f355.png)
4-month-old full-term infant with progressive drop in weight percentiles (10th → 5th → 3rd) despite increased formula calories; small spit-ups, normal vitals and exam. Most appropriate next step in management?
Failure to thrive (FTT) – weight crossing >2 major percentile lines downward due to inadequate usable nutrition.
Best next step: Obtain detailed medical and psychosocial history and observe formula preparation to assess feed volume, caloric density, and social factors.
Not first step:
Hospitalization (A) – reserved after outpatient history/assessment or if safety/medical concerns arise.
CPS (B) – only when abuse/neglect suspected; no clear red flags yet.
Screening labs (C) – chosen based on history/exam, not before them.
Antireflux meds (E) – small spit-ups without large-volume emesis; GERD does not explain FTT and patient has already failed outpatient management.
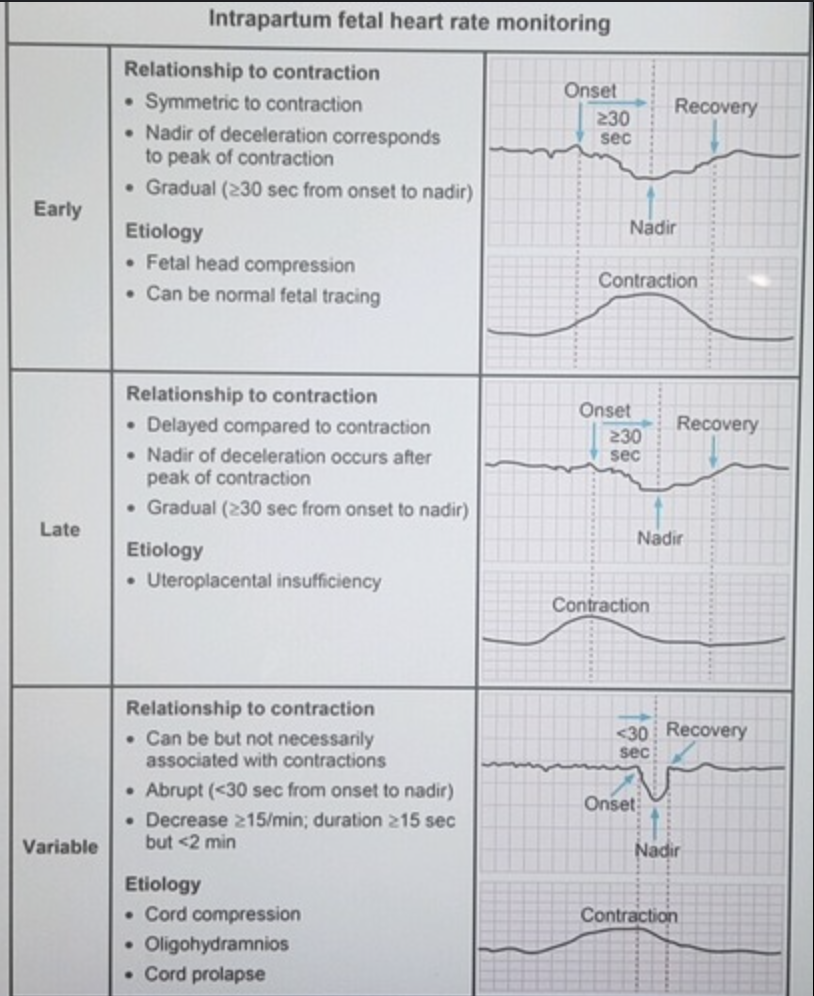
Review intrapartum heart tracings and cause:
a. Early
b. Late
c. Variable
Describe the timeline of events for:
a) Acute Stress disorder
b) Adjustment disorder
c) Depression
d) Dysthymia
a) Acute Stress disorder- < 3 days and resolves < 1m, if not think→PTSD
b) PTSD- >1m
c) Adjustment disorder- >3 and resolves <6m
d) Depression - > 2 weeks
e) Dysthymia - > 2 years
First-line pharmacotherapy choice for a patient with alcohol use disorder who has relapsed despite psychosocial treatment, is currently drinking, has chronic kidney disease, and no liver disease or opioid use.
Use naltrexone, a mu-opioid receptor antagonist that reduces alcohol cravings and heavy drinking days and can be started while the patient is still drinking; acamprosate is for abstinent patients and should be avoided or used cautiously in renal impairment.
Disulfiram is second-line, aversive therapy that is only appropriate for patients who are already abstinent and highly motivated or in a supervised setting
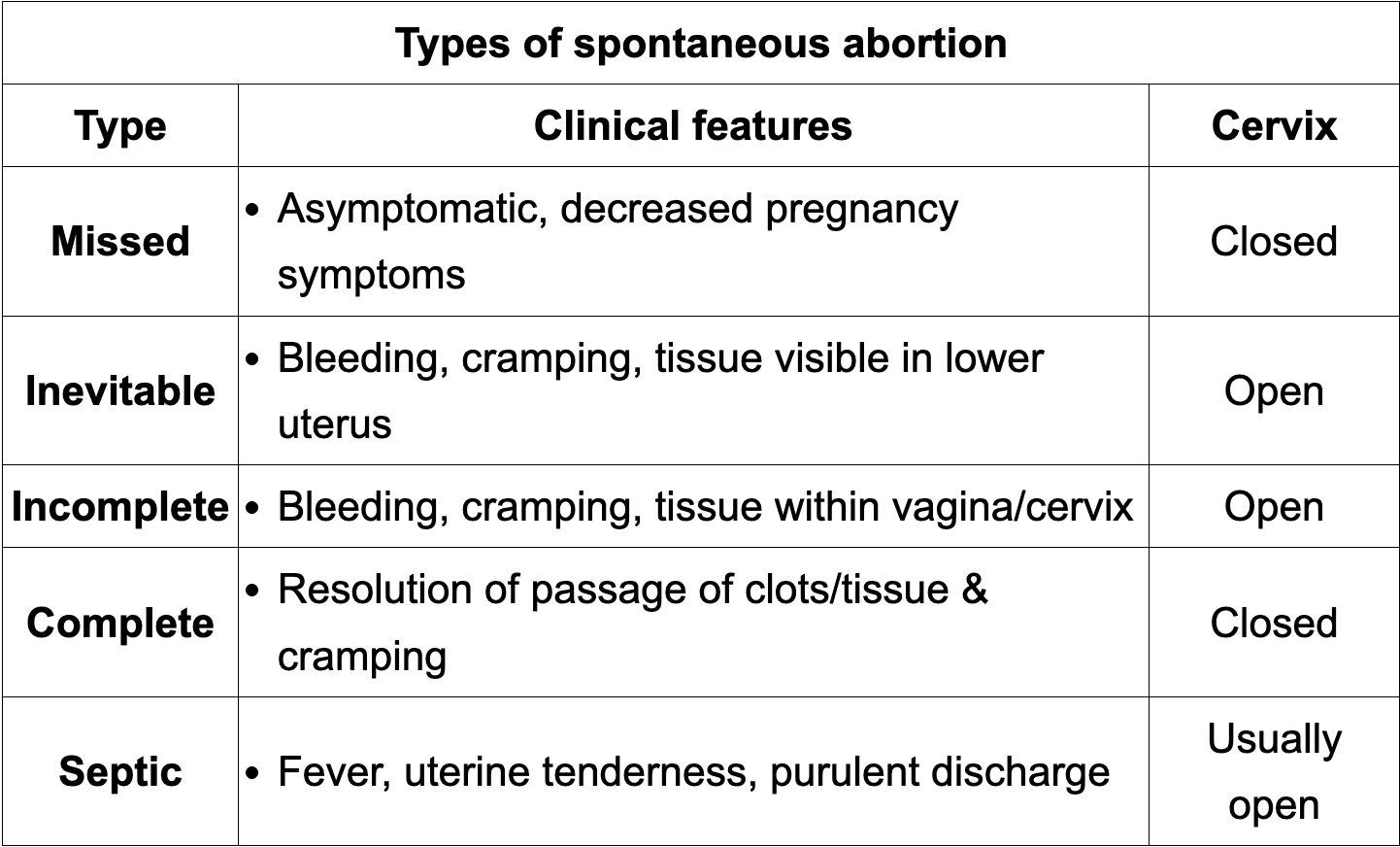
Types of abortions:
view image
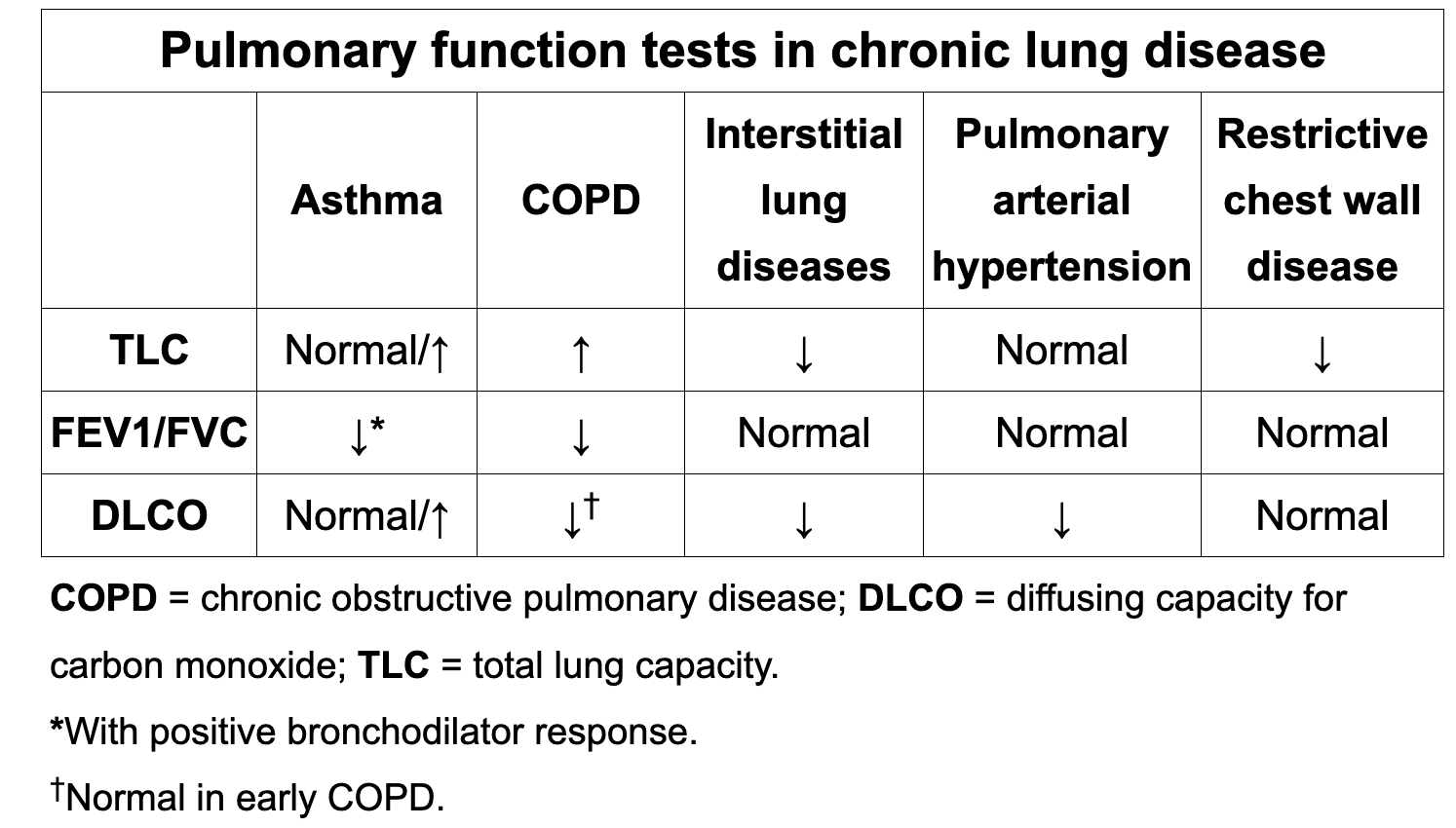
Review spirometry for:
asthma
COPD
ILD
PAH
Restrictive wall
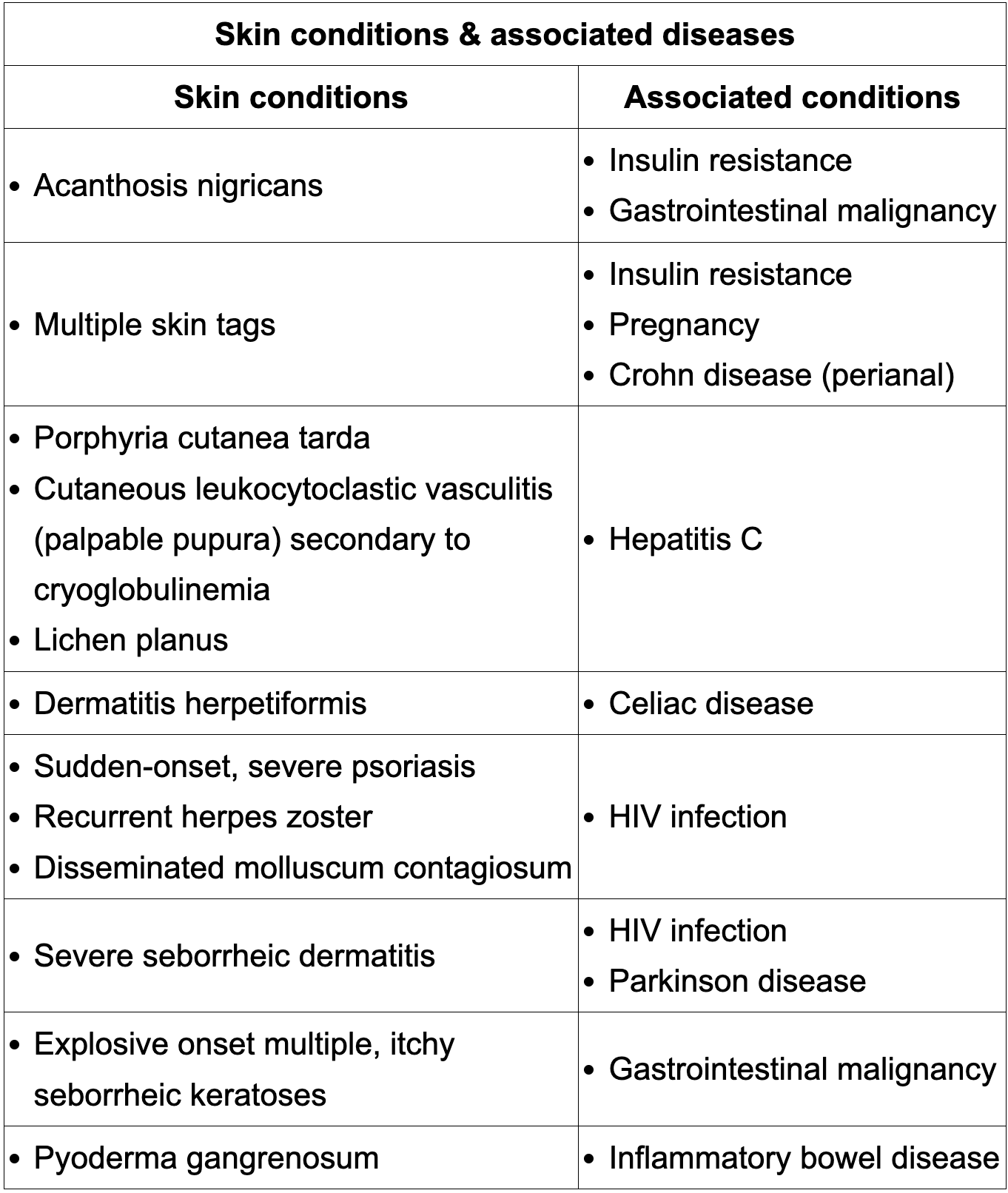
Review skin manifestation of common pathologies:
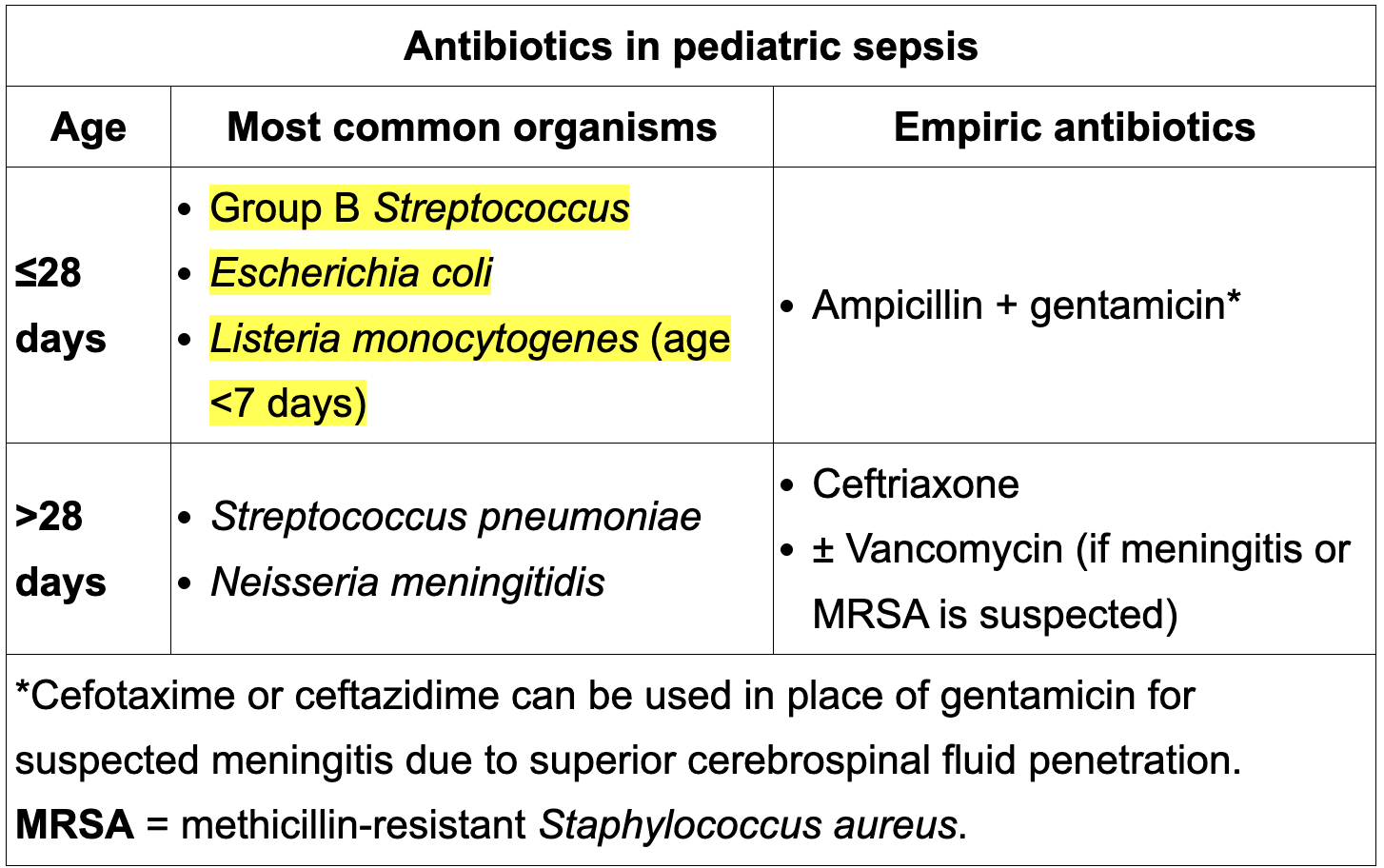
Pediatric antibiotic treatment in sepsis by age?
< 28 d
>28 d
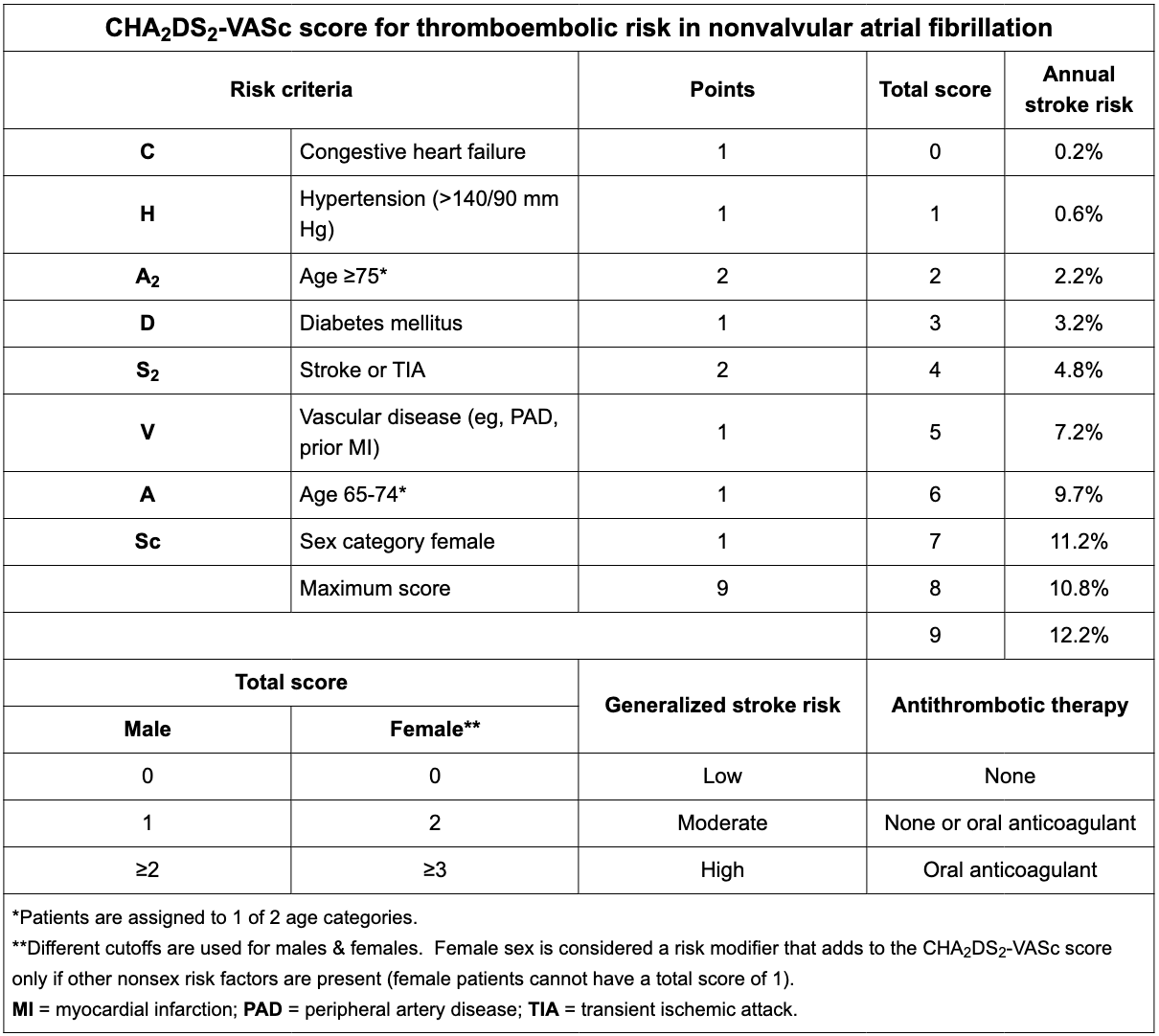
Review Cha2DS2-VASc?
View image
In rotator cuff tear , does passive or active ROM cause pain?
Only active causes pain, passive does not.
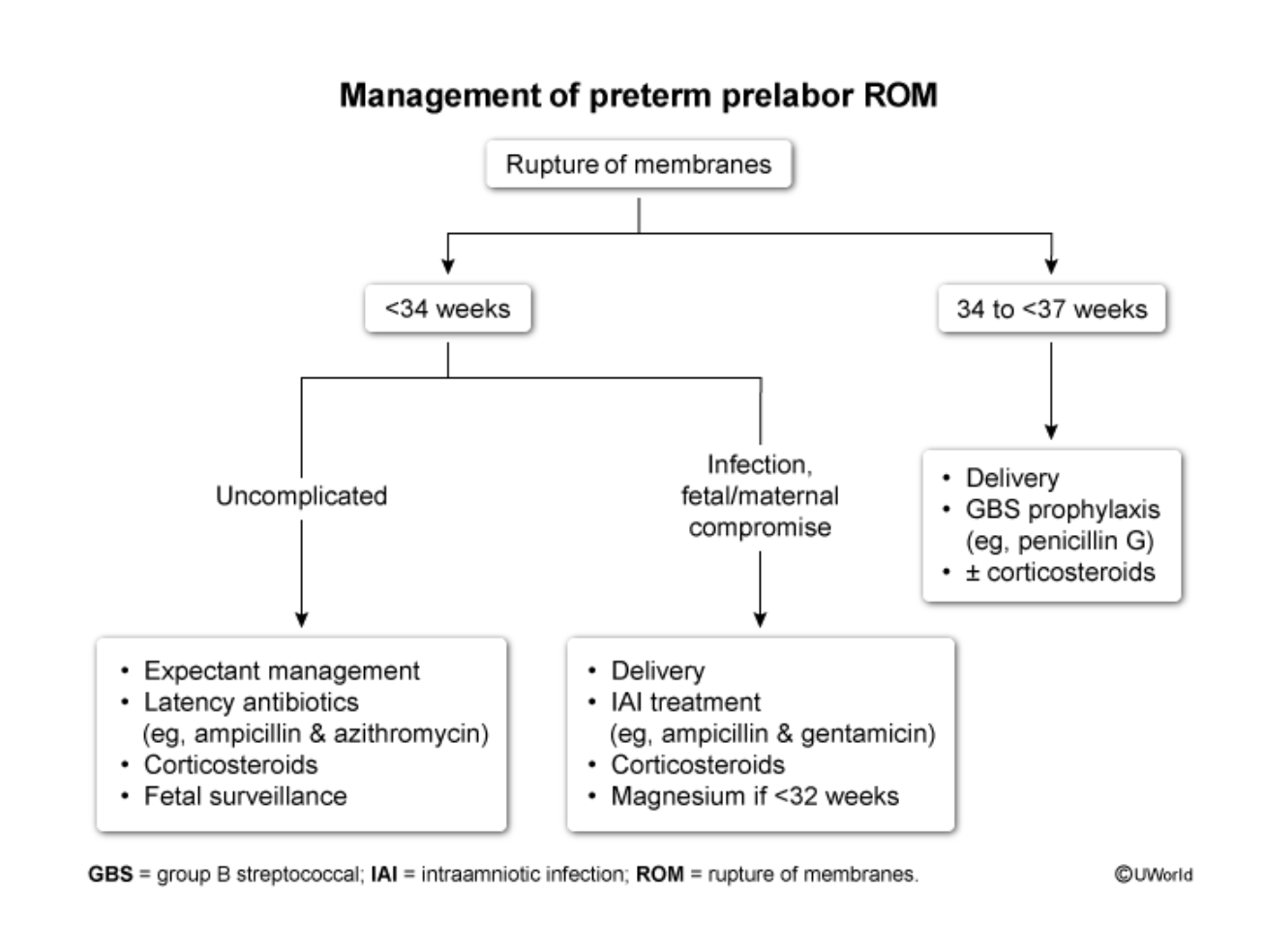
Management of PPROM:
<34 weeks?
34-<37 weeks?
View iamge
On OB US:
When should a gestational sac be visible?
When should a yolk sac be visible?
When should cardiac motion be visible?
When should a gestational sac be visible? 4-5 weeks
When should a yolk sac be visible? 5-6 weeks
When should cardiac motion be visible? 6-7 weeks
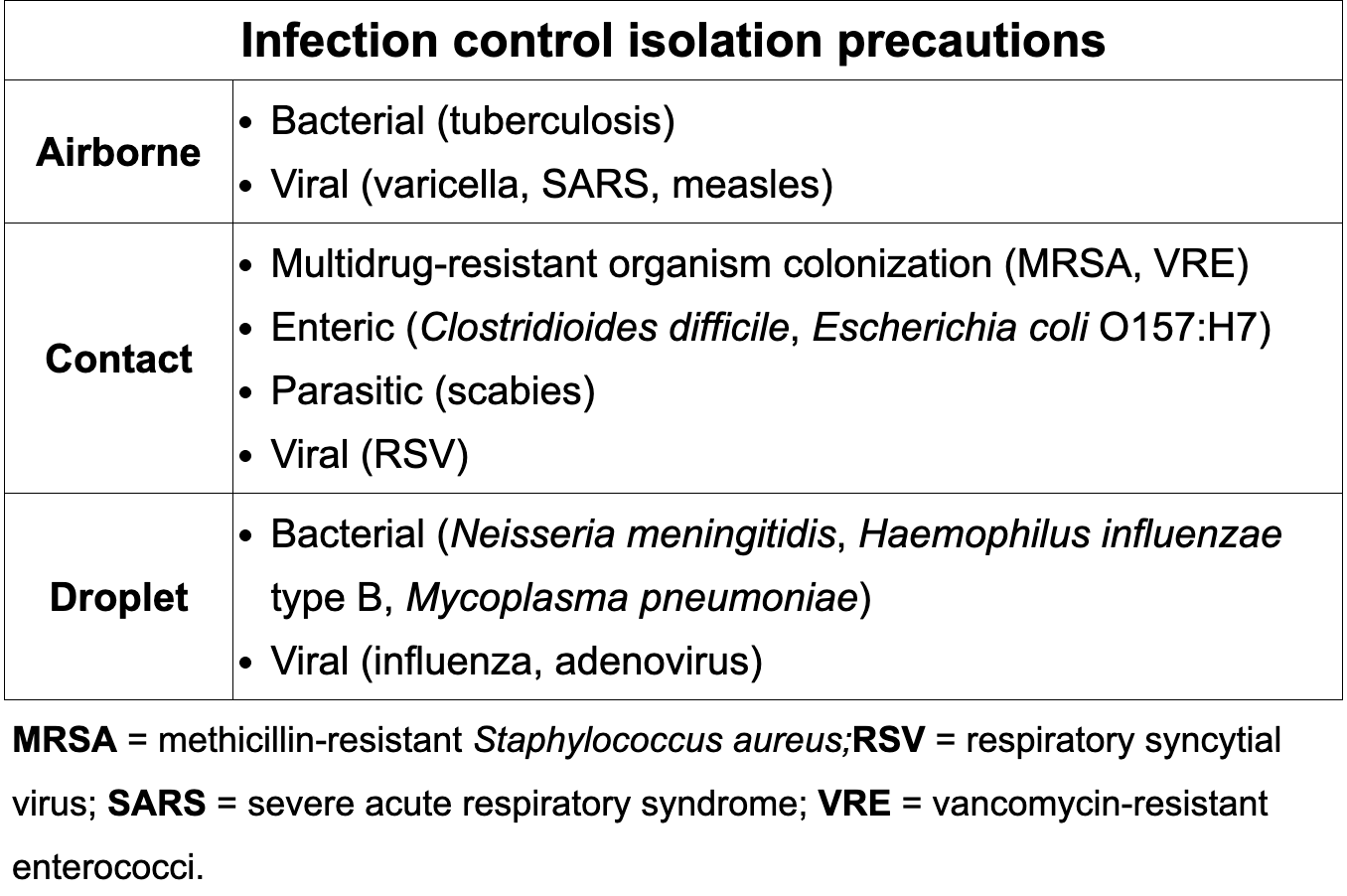
Review infection control precautions
+ Antinuclear antibody is suggestive of what disease?
PBC= Primary Biliary Cholangitis
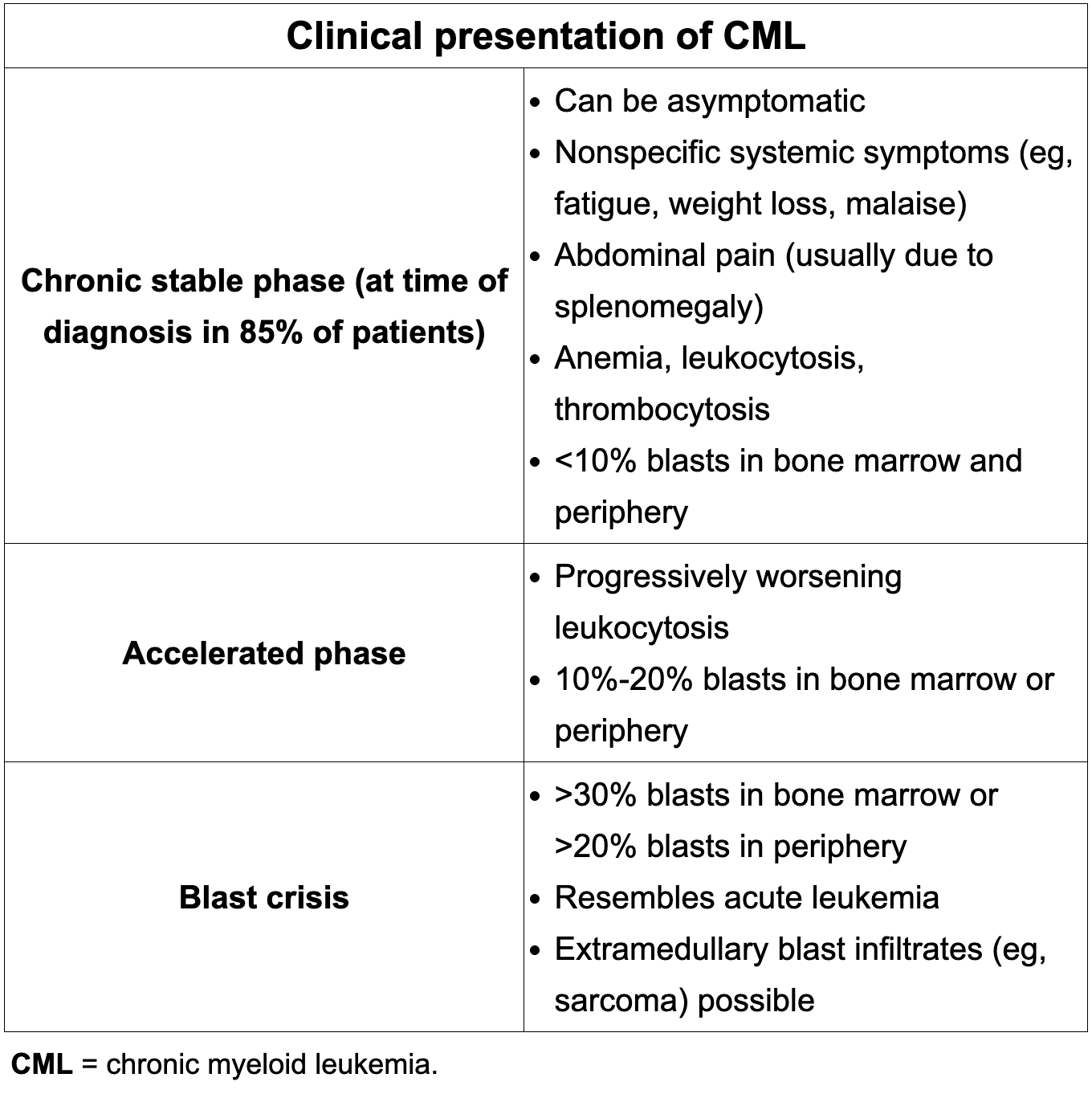
1) What disease is characterized by a BCR/ABL translocation? Or a chromosome 9 and 22 leading to the formation of the philadelphia chromosome?
2) What is the treatment?
1) CML
2) Tyrosine Kinase Inhibitor
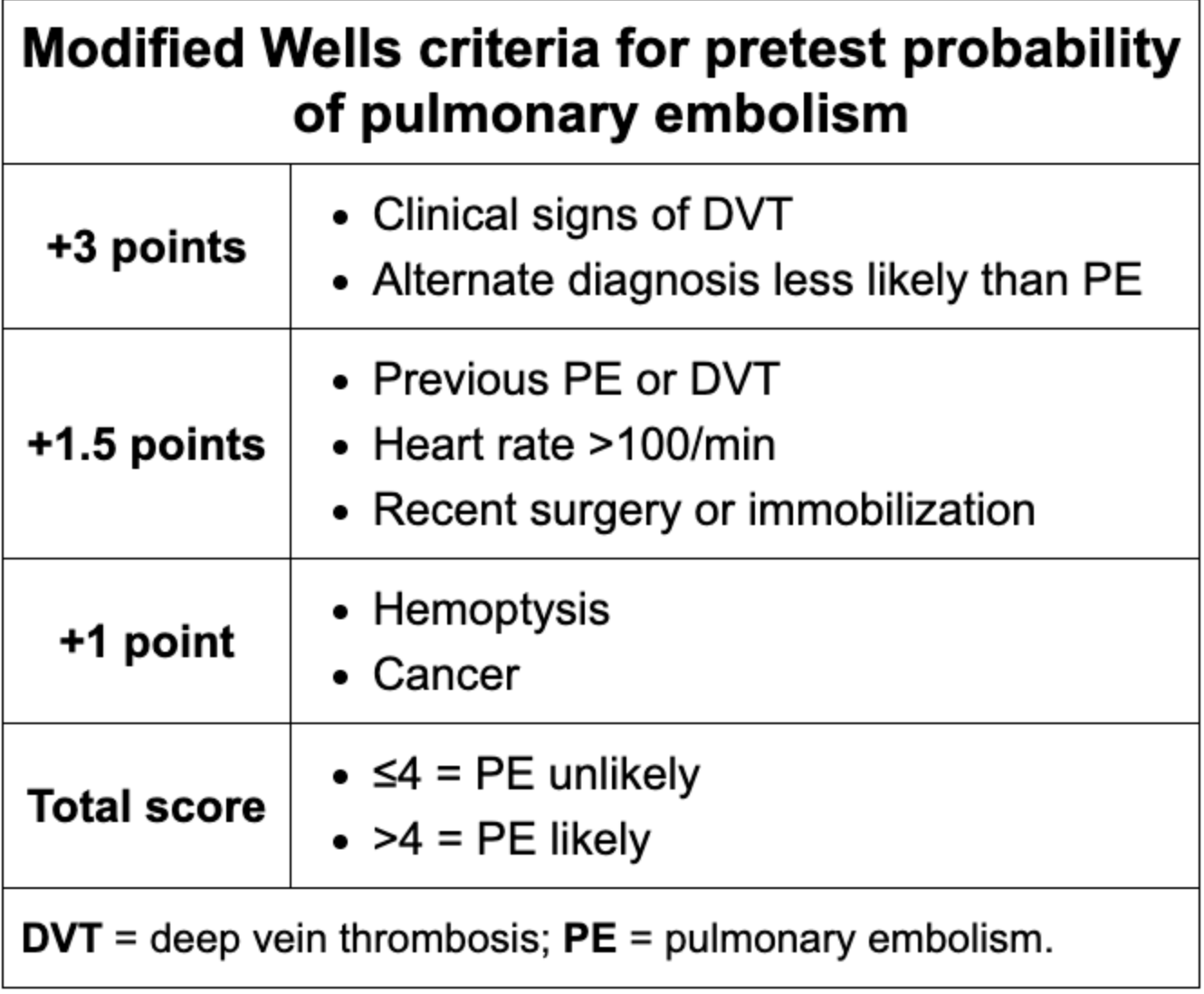
When to screen vs when to treat Pulmonary Embolism
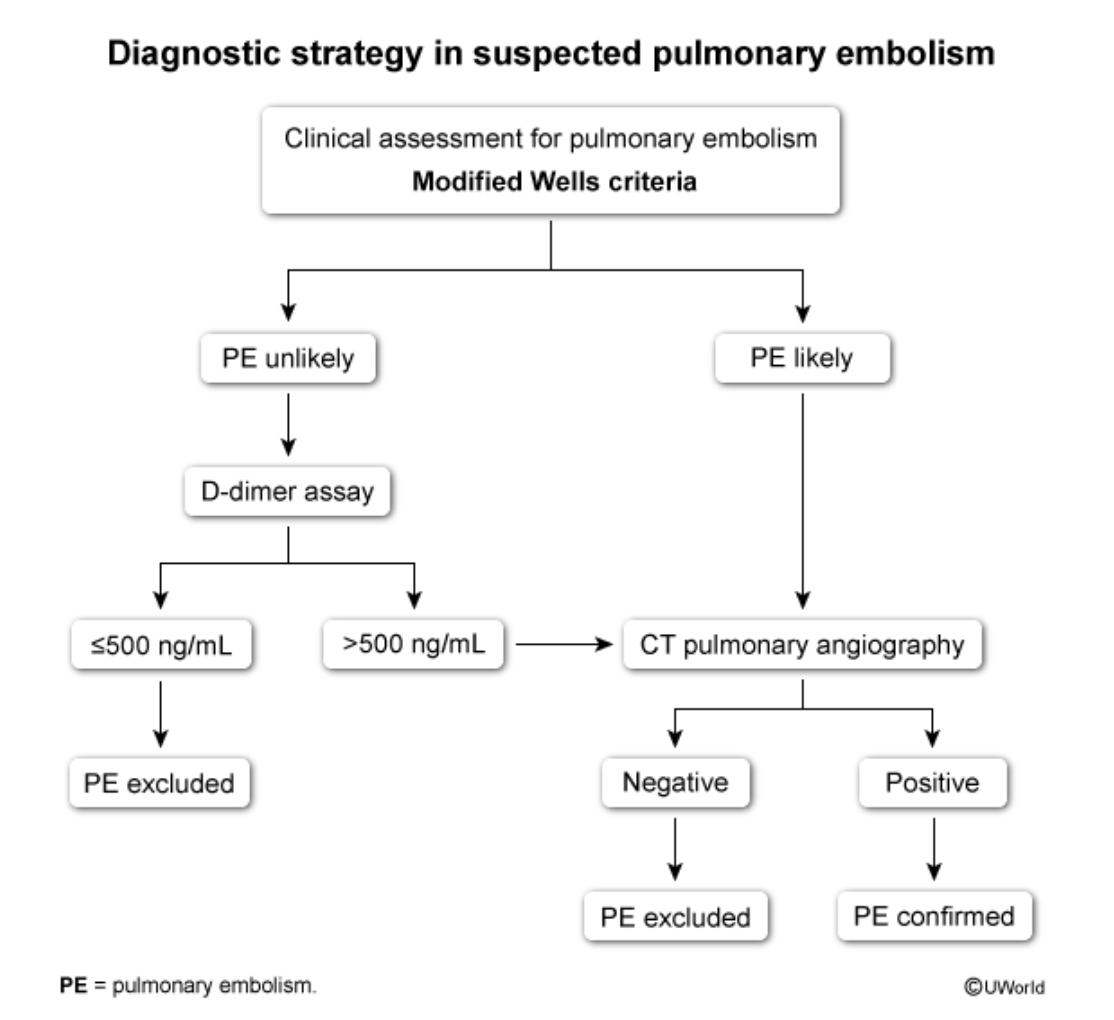
Review modified Wells Criteria
Management for IBS:
A) Diarrhea predominant
B) Constipation predominant
A) Citalopram (SSRI or TCA)
B) Neomycin
Asthma classifications:
Intermittent: Symptoms less than or equal to twice weekly, nighttime awakenings ≤2 times/month, short-acting β-agonist usage ≤2 days/week, no interference with daily activities, and normal FEV1 and FEV1/FVC ratio at baseline
Mild Persistent: Symptoms >2 days/week but not daily, nighttime awakenings 3–4 times/month, short-acting β-agonist usage >2 days/week but not more than once daily, minor limitation to daily activities, FEV1 ≥80% predicted, and normal FEV1/FVC ratio
Moderate Persistent: Daily symptoms, nighttime awakenings greater than once weekly but not nightly, daily use of a short-acting β-agonist, some limitation to daily activity, FEV1 >60% but <80% of predicted, and FEV1/FVC ratio reduced by 5%
Severe Persistent: Symptoms throughout the day, nighttime awakenings nightly, short-acting β-agonist usage several times daily, extremely limited daily activities, FEV1 <60% of predicted, and FEV1/FVC ratio reduced by >5%
Status asthmaticus is a medical emergency and requires emergent treatment in a hospital setting.
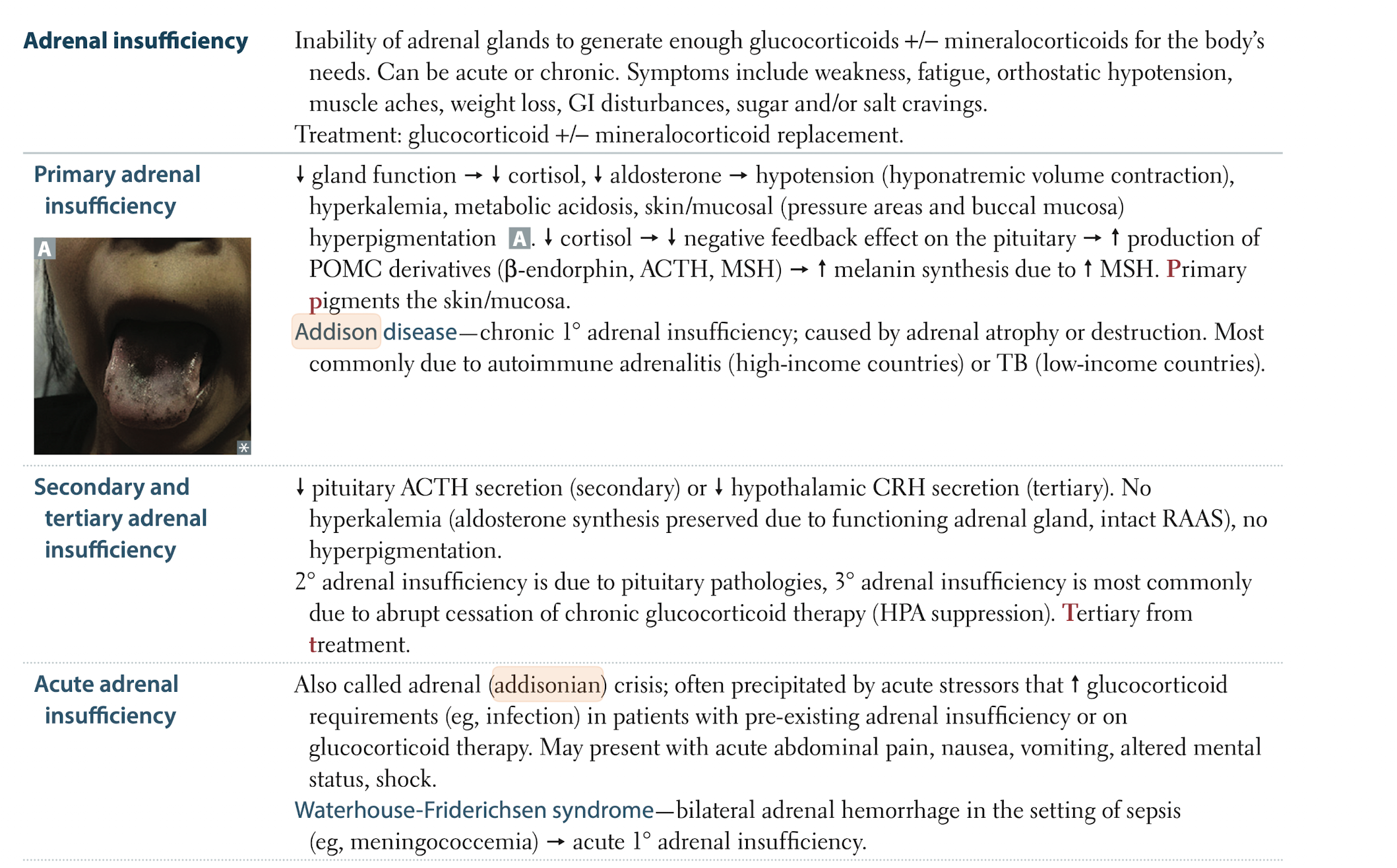
Addison disease (primary adrenal insufficiency): clinical cues, diagnosis, and treatment
Addison disease (primary adrenal insufficiency) presents with chronic fatigue, weakness, weight loss, GI symptoms, orthostatic hypotension, and often hyperpigmentation plus salt craving with hyponatremia and hyperkalemia; diagnosis is suggested by this clinical picture with low morning cortisol and high ACTH, confirmed by an ACTH (cosyntropin) stimulation test (poor cortisol rise) and supported by low aldosterone/high renin and adrenal autoantibodies when autoimmune; chronic treatment is lifelong glucocorticoid replacement (e.g., divided‑dose hydrocortisone) plus mineralocorticoid replacement with fludrocortisone, along with education on stress‑dose steroids, emergency injectable hydrocortisone, and rapid IV hydrocortisone with fluids for adrenal crisis.
Anticoagulation tips:
a) Lovenox
b) Warfarin
a) CKD, very obese or if pregnant
b) Mitral valve replacement or for DVT 2/2 antiphospholipid syndrome
Management of initial episode of C-diff by severity?
Mild: Metronidazole 500mg PO TID x 10-14d
Severe: Vancomycin, 125 mg PO QID x 10-14 d
How does adhesive capsulitis present?
Adhesive capsulitis, manifested as the typical cardinal symptoms of pain, stiffness, and dysfunction of the affected shoulder (impaired active and passive range of motion in all planes).
Diagnostic criteria for chronic fatigue syndrome and treatment:
Fatigue for 6 months and a minimum of four of the following physical symptoms:
-Impaired memory
-Postexertional malaise
-Muscle pain
-Polyarthralgia
-Tender lymph nodes
-Sore throat
-New headaches
-Unrefreshing sleep
Treatment: CBT
Explain key difference between Tamoxifen and Raloxifen as far as usage and what to watch out for?