Men's and Women's Health and Obstetrics
1/145
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
146 Terms
Estrogen and Progestin Combination Ethinyl estradiol and levonorgestrel Indications
Contraception
OL:
Abnormal uterine bleeding
Acne
Dysmenorrhea, endometriosis
Emergency contraception
Hirsutism
Hyper-lactation
Menstrual suppression
Polycystic ovary syndrome
Estrogen and Progestin Combination Ethinyl estradiol and levonorgestrel Adverse Reactions
Thrombosis
MI
CVA
Estrogen and Progestin Combination Ethinyl estradiol and levonorgestrel Safety/Monitoring
Pregnancy
Assess for contraindication
BP
Weight
Estrogen and Progestin Combination Ethinyl estradiol and levonorgestrel Pregnancy/Lactation
D/c in pregnancy
Avoid in breastfeeding
Estrogen and Progestin Combination Ethinyl estradiol and levonorgestrel MOA
Combination hormonal contraceptives inhibit ovulation via a negative feedback mechanism on the hypothalamus → alters the normal pattern of gonadotropin secretion of a follicle-stimulating hormone (FSH) and luteinizing hormone by the anterior pituitary
Changes in the cervical mucus and changes in the endometrium produce an unfavorable environment for nidation
Estrogen and Progestin Combination Ethinyl estradiol and levonorgestrel BLACK BOX
Cigarette smoke/CVD > 35 y/o
Obesity and DVT (patch)
Combined Oral Contraceptive Contraindications
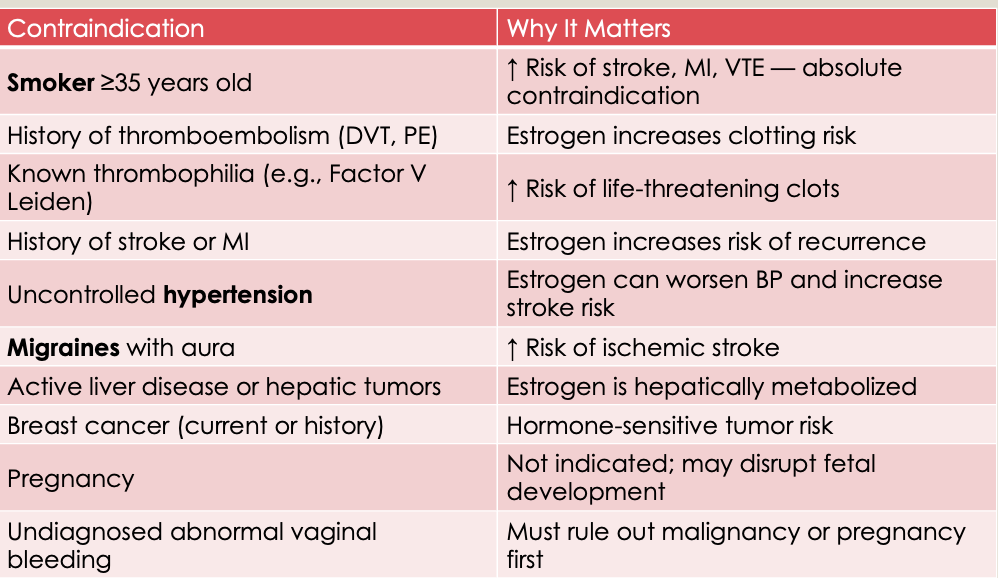
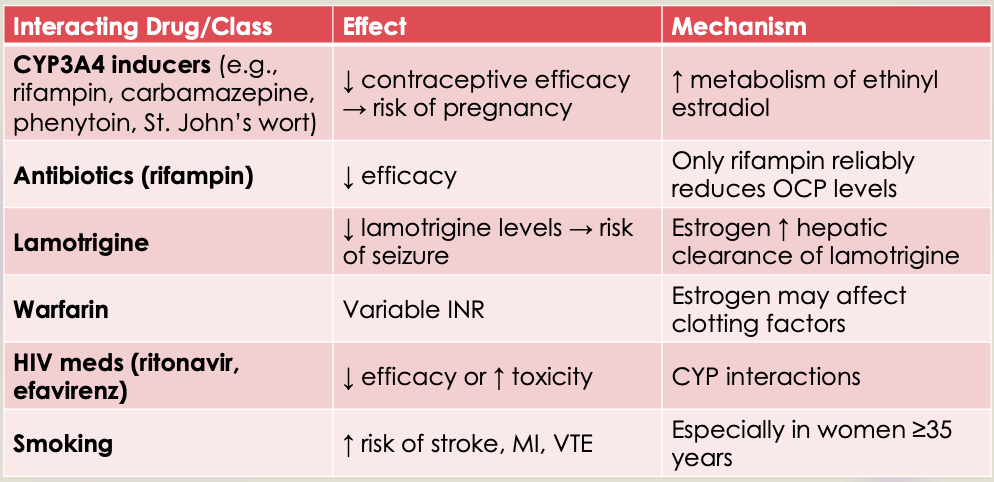
Combined Oral Contraceptive Drug Interactions
Progestin Only Norethindrone (Camila), Drosperinone (Slynd) Indications
Contraception
Abnormal uterine bleeding
Endometriosis
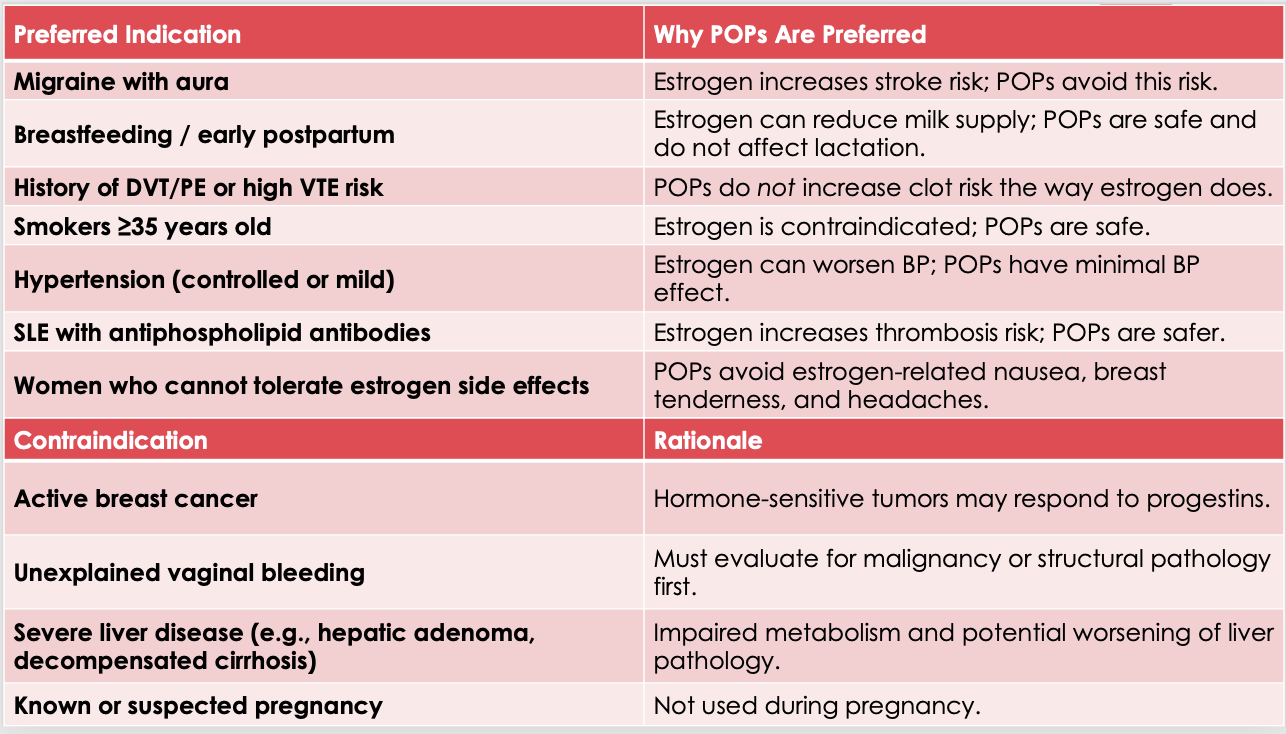
Progestin Only Norethindrone (Camila), Drosperinone (Slynd) Contraindications
Progestin dependent malignant tumor
Benign or malignant liver tumors
Acute liver disease
Progestin Only Norethindrone (Camila), Drosperinone (Slynd) Drug Interactions
Rifampin
Anti-convulsants
Progestin Only Norethindrone (Camila), Drosperinone (Slynd) Adverse Reactions
Menstrual bleeding irregularities
Progestin Only Norethindrone (Camila), Drosperinone (Slynd) Safety/Monitoring
Pregnancy
Assess for abnormal bleeding
Monitor glucose and lipids
Progestin Only Norethindrone (Camila), Drosperinone (Slynd) Pregnancy/Lactation
D/c in pregnancy
Preferred in breastfeeding
Progestin Only Norethindrone (Camila), Drosperinone (Slynd) MOA
Suppresses ovulation
Thickens cervical mucus (which inhibits sperm penetration)
Alters follicle-stimulating hormone (FSH) and luteinizing hormone (LH) concentrations
Slows the movement of ovum through the fallopian tubes
Alters the endometrium
Progestin Only
Progestin Only Depot Injection Medroxyprogesterone acetate Indications
Contraception
OL
Abnormal uterine bleeding
Endometrial hyperplasia
Menstrual suppression
Progestin Only Depot Injection Medroxyprogesterone acetate Contraindications
Thromboembolic disorders (current or history of)
Cerebral vascular disease
Undiagnosed vaginal bleeding
Breast cancer (known, suspected, or history of)
Significant hepatic disease
Progestin Only Depot Injection Medroxyprogesterone acetate Drug Interactions
Rifampin
Anti-convulsants
HIV antivirals
St. John’s Wart
Progestin Only Depot Injection Medroxyprogesterone acetate Adverse Reactions
Bone loss
Menstrual irregularities
Weight gain
Progestin Only Depot Injection Medroxyprogesterone acetate Safety/Monitoring
Pregnancy
Glucose
Progestin Only Depot Injection Medroxyprogesterone acetate Pregnancy/Lactation
D/c during pregnancy but low risk
Consider breastfeeding after 6 weeks
Progestin Only Depot Injection Medroxyprogesterone acetate MOA
When used as an injection for contraception (doses of 150 mg IM or 104 mg SUBQ), medroxyprogesterone inhibits the secretion of pituitary gonadotropins, which prevents follicular maturation and ovulation and causes endometrial thinning.
Progestogens, such as medroxyprogesterone when used for endometriosis, lead to atrophy of the endometrial tissue
They may also suppress new growth and implantation
Pain associated with endometriosis is decreased
Progestin Only Depot Injection Medroxyprogesterone acetate BLACK BOX
Long term use > 2 years → bone mineral density
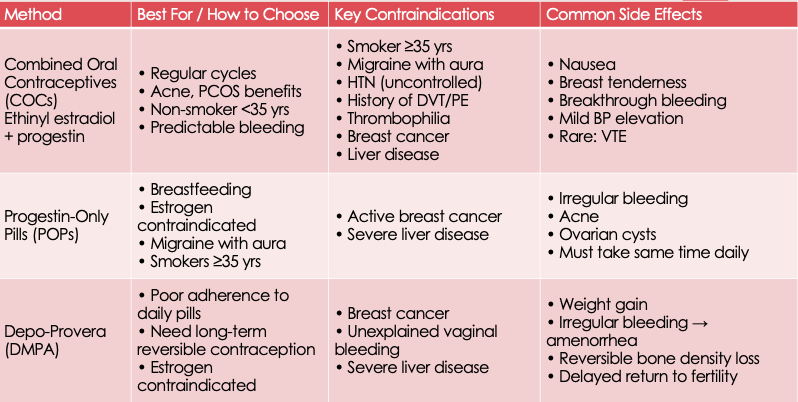
Contraceptive Choice: Pharmacology Comparison
Emergency Contraception High dose Progestin Levonorgestrel Indications
Emergency contraception
Emergency Contraception High dose Progestin Levonorgestrel Contraindications
OTC labeling
Do not use if already pregnant
Do not use for regular birth control
Emergency Contraception High dose Progestin Levonorgestrel Adverse Reactions
Irregular menses
Abdominal pain
Nausea
HA
Emergency Contraception High dose Progestin Levonorgestrel Safety/Monitoring
Evaluate for pregnancy
Emergency Contraception High dose Progestin Levonorgestrel Pregnancy/Lactation
Avoid in pregnancy
Safe in lactation
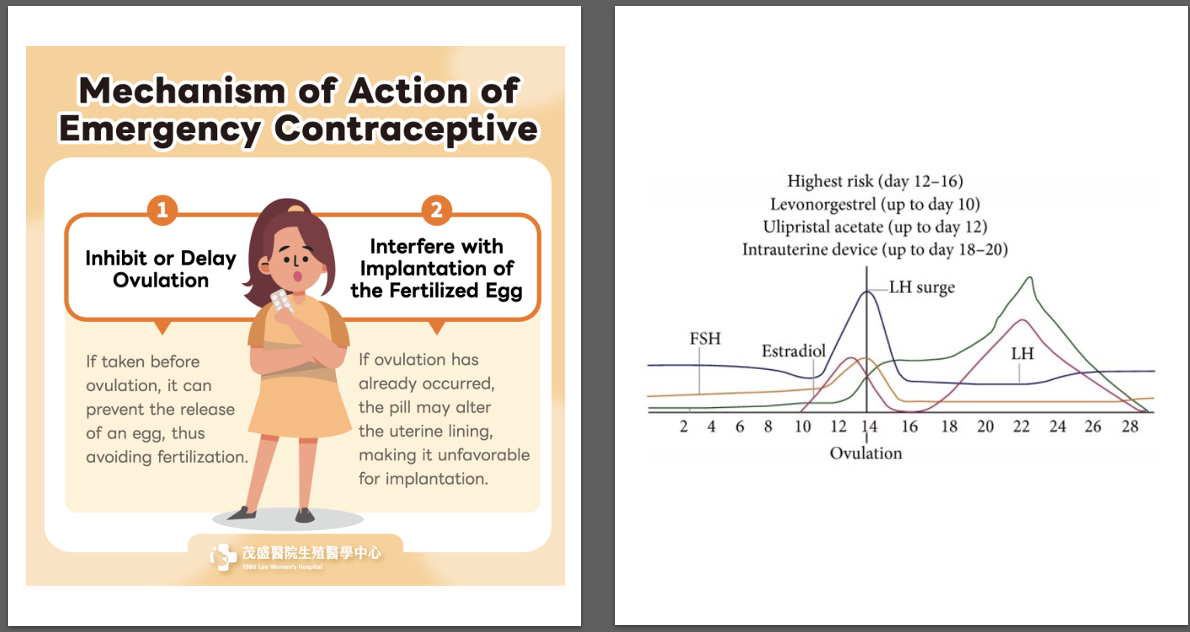
Emergency Contraception High dose Progestin Levonorgestrel MOA
Pregnancy may be prevented through several mechanisms:
Thickening of cervical mucus, which inhibits sperm passage through the uterus and sperm survival
Inhibition of ovulation, from a negative feedback mechanism on the hypothalamus, leading to reduced secretion of follicle stimulating hormone (FSH) and luteinizing hormone (LH)
Altering the endometrium, which may affect implantation
Levonorgestrel is not effective once the implantation process has begun.
Emergency Contraception Progestin Receptor Modulator Ulipristal Indications
Emergency contraception
Emergency Contraception Progestin Receptor Modulator Ulipristal Contraindications
OTC labeling
Do not use if already pregnant
Do not use for regular birth control
Emergency Contraception Progestin Receptor Modulator Ulipristal Adverse Reactions
Irregular menses
Abdominal pain
Nausea
HA
Emergency Contraception Progestin Receptor Modulator Ulipristal Safety/Monitoring
Evaluate for pregnancy
Emergency Contraception Progestin Receptor Modulator Ulipristal Pregnancy/Lactation
Avoid for pregnancy
Safe in lactation
Emergency Contraception Progestin Receptor Modulator Ulipristal MOA
Prevents progestin from binding to the progesterone receptor
Postpones follicular rupture when administered prior to ovulation, thereby inhibiting or delaying ovulation
May also alter the normal endometrium, impairing implantation
MOA Emergency Contraception
Cervical Ripening Prostaglandins Misoprostol and Dinoprostone Indications
Cytotec: NSAID-induced gastric ulcers, pregnancy Termination
(OL):
Cervical ripening
Postpartum hemorrhage
Pregnancy loss
Cervidil: Cervical ripening
Cervical Ripening Prostaglandins Misoprostol and Dinoprostone Contraindications
Abortifacient
Cervical Ripening Prostaglandins Misoprostol and Dinoprostone Adverse Reactions
Uterine rupture
Abdominal pain
Diarrhea
Cervical Ripening Prostaglandins Misoprostol and Dinoprostone Safety/Monitoring
Fetal HR
Uterine activity
Progression of cervical dilation and effacement
Signs of amniotic fluid embolism
Cervical Ripening Prostaglandins Misoprostol and Dinoprostone MOA
•Dinoprostone (prostaglandin E2) is an endogenous hormone found in low concentrations in most tissues of the body → when administered for labor induction, it relaxes the smooth muscle of the cervix, allowing dilation and passage of the fetus through the birth canal
Cervical Ripening Prostaglandins Misoprostol and Dinoprostone BLACK BOX
Abortifacient property
Uterine rupture
Oxytocin Indications
Refractory postpartum hemorrhage
OL
Prion or augmentation
Pregnancy termination
Oxytocin Contraindications
Significant cephalopelvic disproportion
Unfavorable fetal presentation
Cord presentation
Total placenta previa
Contraindicated vaginal delivery
Oxytocin Drug Interactions
Prostaglandins (misoprostol, dinoprostone)
Uterine hyperstimulation
QT-prolongation
Oxytocin Safety/Monitoring
Fluid intake and output during administration
Uterine activity (tonus, amplitude, and frequency of contractions), maternal blood pressure
Continuous electronic fetal heart rate monitoring in relation to uterine contractions
Oxytocin Pregnancy/Lactation
Safe
Oxytocin MOA
Oxytocin stimulates uterine contractions by acting on receptors that trigger the release of intracellular calcium and local prostaglandin production
Oxytocin specific receptors are not present in the uterus until ~13 weeks' gestation and increase as pregnancy progresses and reach maximum concentration at term → term pregnancies are more sensitive to lower oxytocin doses
Oxytocin BLACK BOX
Elective induction of labor
Tranexamic Acid Indications
Refractory postpartum hemorrhage
Pregnancy termination
Tranexamic Acid Adverse Reactions
HA
Thromboembolic event
Tranexamic Acid Safety/Monitoring
Hypersensitivity
Seizures
Tranexamic Acid Pregnancy/Lactation
Safe in pregnancy
Avoid in lactation
Tranexamic Acid MOA
Forms a reversible complex that displaces plasminogen from fibrin resulting in inhibition of fibrinolysis
It also inhibits the proteolytic activity of plasmin
Tranexamic Acid BLACK BOX
IV only
Carboprost Tromethamine Indications
Refractory postpartum hemorrhage
Pregnancy termination
Carboprost Tromethamine Adverse Reactions
Fever
N/V
HTN
Carboprost Tromethamine Safety/Monitoring
BP
Carboprost Tromethamine Pregnancy/Lactation
Not safe
Carboprost Tromethamine MOA
Carboprost is an analog of naturally occurring prostaglandin F2 alpha (dinoprost) → stimulates uterine contractility which usually results in expulsion of the products of conception and is used to induce abortion between 13-20 weeks of pregnancy
When used postpartum, hemostasis at the placentation site is achieved through the myometrial contractions produced by carboprost
Carboprost Tromethamine BLACK BOX
Appropriate use
Experienced physician
Methylergometrine/Methylergonovine Indications
Post-partum hemorrhage
Methylergometrine/Methylergonovine Contraindications
CAD
Methylergometrine/Methylergonovine Drug Interactions
Oxytocin
Prostaglandins
Methylergometrine/Methylergonovine Adverse Reactions
HTN
hTN
Methylergometrine/Methylergonovine Safety/Monitoring
BP
Methylergometrine/Methylergonovine MOA
Increases the tone, rate and amplitude of contractions on the smooth muscles of the uterus, producing sustained contractions which shortens the third stage of labor and reduces blood loss
Magnesium Sulfate Indications
Asthma
COPD
Constipation
Eclampsia/preeclampsia
Hypomagnesemia
Torsades de pointes
Magnesium Sulfate Contraindications
Heart block/myocardial damage within 2 hours of delivery
Caution in renal impairment and neuromuscular disease
Magnesium Sulfate Drug Interactions
Some antibiotics and antivirals
Magnesium Sulfate Adverse Reactions
hTN
Flushing
Vasodilation
Magnesium Sulfate Safety/Monitoring
ECG monitoring
Vital signs
Deep tendon reflexes
Magnesium
Magnesium Sulfate Pregnancy/Lactation
Safe
Magnesium Sulfate MOA
Magnesium sulfate prevents and controls seizures in preeclampsia and eclampsia through three primary mechanisms
Blocking neuromuscular transmission
Blocking central nervous system depression
Blocking peripheral vasodilation
Magnesium Sulfate Toxicity
Early & Late Clinical Signs
Early (most testable):
↓ or absent deep tendon reflexes
Somnolence
Nausea, flushing
Late (danger signs):
Respiratory depression
Hypoxia
Cardiac conduction abnormalities
Risk Factors
Renal insufficiency (most common)
High infusion rates
Iatrogenic dosing errors
Immediate Management
STOP magnesium infusion
Administer calcium gluconate (antidote)
10 mL of 10% solution IV over 2–3 minutes
Support airway/ventilation if needed
Monitor urine output, reflexes, respiratory status

Sildenafil, Tadalafil, Varenafil, Avanafil Indications
Erectile Dysfunction
BPH (Cialis only)
High Altitude pulmonary edema (HAPE)
Pulmonary artery HTN (PAH)
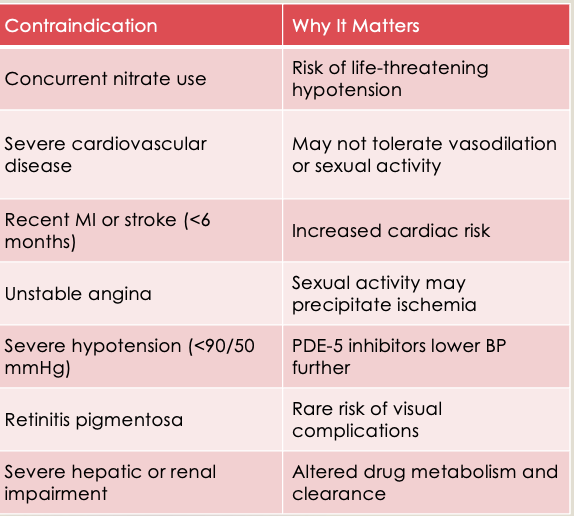
Sildenafil, Tadalafil, Varenafil, Avanafil Contraindications
CVD
CAD
Sildenafil, Tadalafil, Varenafil, Avanafil Drug Interactions
Nitrates
BP lowering agents
Protease inhibitors (HIV)
Sildenafil, Tadalafil, Varenafil, Avanafil Adverse Reactions
•Flushing
HA
Hearing loss,
hTN
Priapism
Visual disturbance
Sildenafil, Tadalafil, Varenafil, Avanafil Safety/Monitoring
HR
BP
Sildenafil, Tadalafil, Varenafil, Avanafil Pregnancy/Lactation
Avoid
Sildenafil, Tadalafil, Varenafil, Avanafil MOA
Sildenafil enhances the effect of NO by inhibiting phosphodiesterase type 5 (PDE-5), which is responsible for degradation of cGMP in the corpus cavernosum → when sexual stimulation causes local release of NO, inhibition of PDE-5 by sildenafil causes increased levels of cGMP in the corpus cavernosum, resulting in smooth muscle relaxation and inflow of blood to the corpus cavernosum
At recommended doses, it has no effect in the absence of sexual stimulation
PDE5 Inhibitors Contraindications and Patient Counseling
Patient Counseling Points
Review all medications, especially nitrates and alpha-blockers
Assess cardiovascular status — is sexual activity safe?
Discuss timing — onset varies by agent:
Sildenafil/Vardenafil: ~30–60 min before
Avanafil: ~15 min before
Tadalafil: daily or as needed (longest duration)
During Use
Avoid nitrates for 24–48 hours after PDE-5 use
Limit alcohol — may worsen hypotension
Report priapism (>4 hours) — medical emergency
Report sudden vision or hearing loss — rare but serious
Lifestyle & Safety
Do not combine with recreational "poppers" (amyl nitrate)
Do not use with grapefruit juice (CYP3A4 interaction — mainly with sildenafil)
Tadalafil also treats BPH — dual benefit
Avanafil has the fastest onset, the lowest food interaction
Sildenafil may cause blue-tinged vision (PDE-6 inhibition)
Always ask about chest pain meds before prescribing
Hypogonadism Androgen Testosterone (AndroGel) Indications
Hypogonadism
Hormone replacement
Hypogonadism Androgen Testosterone (AndroGel) Contraindications
Breast cancer
Prostate cancer
Pregnancy
Hypogonadism Androgen Testosterone (AndroGel) Adverse Reactions
HTN
Hepatotoxicity
Polycythemia
Venous thromboembolism (VTE)
Hypogonadism Androgen Testosterone (AndroGel) Safety/Monitoring
Confirm hypogonadism by measuring serum total testosterone on at least 2 separate mornings following overnight fasting
LFTs
Lipid panel
Hemoglobin and hematocrit
BP
PSA
Testosterone
Hypogonadism Androgen Testosterone (AndroGel) Pregnancy/Lactation
Contraindicated
Hypogonadism Androgen Testosterone (AndroGel) MOA
Principal endogenous androgen responsible for promoting the growth and development of the male sex organs and maintaining secondary sex characteristics in androgen-deficient males
Hypogonadism Androgen Testosterone (AndroGel) BLACK BOX
HTN
Secondary exposure
Pulmonary oil embolism
Alpa 1 Blockers Tamsulosin, Terazosin, Doxazosin, Alfuzosin Indications
BPH
OL
Chronic prostatitis
LUTS
Lower urinary tract symptoms
Ureteral stent and stones
Alpa 1 Blockers Tamsulosin, Terazosin, Doxazosin, Alfuzosin Contraindications
Sulfa allergy
HF
Floppy iris
Alpa 1 Blockers Tamsulosin, Terazosin, Doxazosin, Alfuzosin Drug Interactions
Numerous
BP lowering agents
Alpa 1 Blockers Tamsulosin, Terazosin, Doxazosin, Alfuzosin Adverse Reactions
hTN
Flushing
Alpa 1 Blockers Tamsulosin, Terazosin, Doxazosin, Alfuzosin Safety/Monitoring
UA
BP,
Prostate symptom score
Prostate cancer screening
Alpa 1 Blockers Tamsulosin, Terazosin, Doxazosin, Alfuzosin Pregnancy/Lactation
Limited data
Alpa 1 Blockers Tamsulosin, Terazosin, Doxazosin, Alfuzosin MOA
Tamsulosin is an antagonist of alpha1A-adrenoreceptors in the prostate
Smooth muscle tone in the prostate is mediated by alpha1A-adrenoreceptors; blocking them leads to relaxation of smooth muscle in the bladder neck and prostate, causing an improvement of urine flow and decreased symptoms of BPH
5 alpha reductase inhibitors Finasteride, Dutasteride Indications
Alopecia
Alternative agent for BPH (indicated for high prostate volume)