Surgical care
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
What is the pre assessment patients need to be considered for surgery?
Height, weight, BP, HR, bloods
MRSA swab (nose, back of throat, groin)
Medical and drug history
Explain options and procedure - pros and cons
Sign consent forms
Listing for surgery - can take weeks-years
What are the surgical considerations?
Medication management in the peri-operative period
Antibiotic prophylaxis
Thromboprophylaxis or VTE prophylaxis
Pain control
Post operative nausea and vomiting
What is the peri operative period?
The time between the pre op admission to hospital and the post operative discharge back home
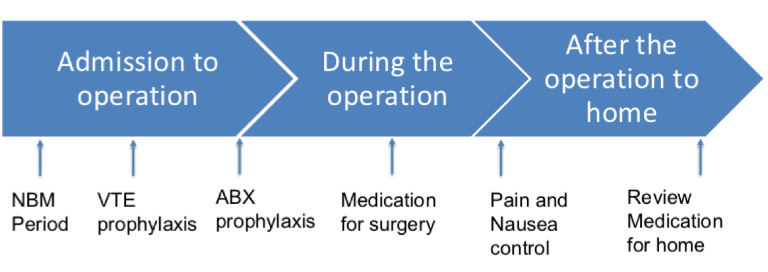
What is prophylaxis?
Any medical or health related procedure/medication/treatment designed to prevent diseases, infections or conditions before they happen
What is a NBM period and why is it necessary?
Nil by mouth - no eating or drinking before a surgery
Risk of aspiration - inhalation of stomach content during surgery as it’s acidic and microbial content can cause infections
Pneumonia and lung damage complications
Reduces post operative nausea
Clear fluids can be consumed 2 hours before
No food can be can be consumed up to 6 hours before
How is NBM weighed up against need for medications?
Medication can be given with small sips of water
Most meds can miss a dose or two
Prevents a relapse of chronic conditions and avoids effects of drug withdrawal
Other routes of administration should be considered
Would the drugs be risky for the surgery?
What drugs can cause an issue for surgical patients?
Anticoagulants (warfarin/apixaban) - bleeding risk, may need a short acting agent (heparin/enoxaparin)
Anti-platelets (aspirin/clopidogrel) - bleeding risk, stop a few days before surgery
NSAIDs - stop a day before, maybe earlier for longer acting drugs
Contraception/HRTs - VTE risk, stop 4-6 weeks before, risk to benefit is discussed
Monoamine-oxidase inhibitors - interacts with surgical drugs, management plan with psych and anaesthetist
Lithium - stop 24 hours before, monitor fluids and electrolytes
ACEI/ARB - causes severe hypotension with anaesthetics, stop 24 hours before
Why is clopidogrel stopped for longer than aspirin?
Stop to allow platelets to come back and clear the drugs
Clop is longer as it has a longer half life and more irreversible inhibition of platelet formation
What metabolic changes happen to diabetics during surgery?
Surgery = stress = metabolic changes
Increased risk of peri-op complications - unable to compensate for hyperglycaemic (affects delayed wound healing) response to stress
Risk of diabetic ketoacidosis T1 or non-keto hyperosmolar state T2
Maintain optimal blood glucose control to reduce this
Want to reduce risk of hypo and hyperglycaemia
Continuous variable rate intravenous insulin infusion and close monitoring of BMs and K+
How is cortisol affected from the stress of surgery?
Increased concentration (released by adrenal glands)
Adrenal insufficiency and long term steroid use will need supplements
Patients with this insufficiency can lead to hypo adrenal crisis with can cause shock and circulatory collapse
Double or triple dose of corticosteroids
High dose steroids can impair wound healing and increase infection risk
What changes to medication are necessary for different surgeries?
Total thyroidectomy - stop anti-thyroid meds, start levothyroxine replacement, Ca supplements as parathyroid glands can be damaged
Ileostomy - drug absorption is lost as a section of SI is gone, fluid and electrolyte loss, review immunosuppressant therapy (INR testing), short bowel syndrome can occur so give additional loperamide
Below knee amputation - diabetes control, phantom pain, drug kinetics (decrease VoD)
What is a surgical site infection and risk factors?
Common but avoidable complication of any surgery
Surgeon skill and environmental factors
Type of operation
Number of MOs
Patient risk factors
How can surgery antibiotic prophylaxis risks be managed?
MRSA screening
Antiseptic washes
Surgical site decontamination
Prophylactic antibiotics
Hospital policies
Theatre cleaning regimen
Sterilised equipment
Infection control training
What are the 4 classifications of operation?
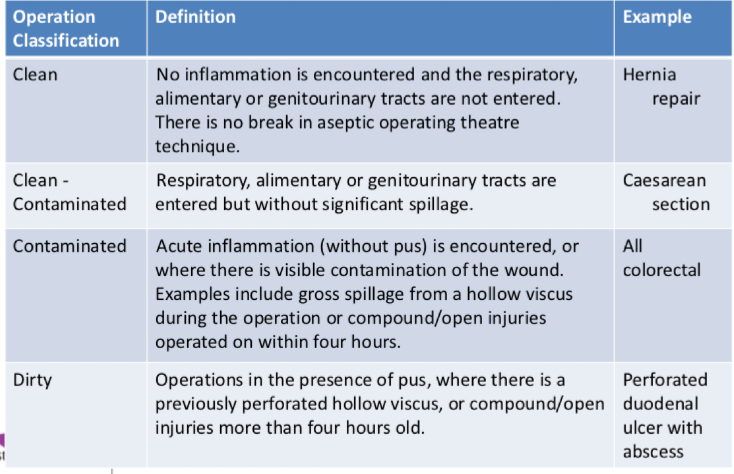
What considerations are taken when an antibiotic is indicated?
Effective against likely agents
Decreases antibiotic resistance
Decreases C.difficile infection
Decreases incidence of post op SSI
Decreases morbidity
Decreases mortality because of SSIs → sepsis
Decreases hospital stay
Adequate tissue levels
Cheaper and less side effects
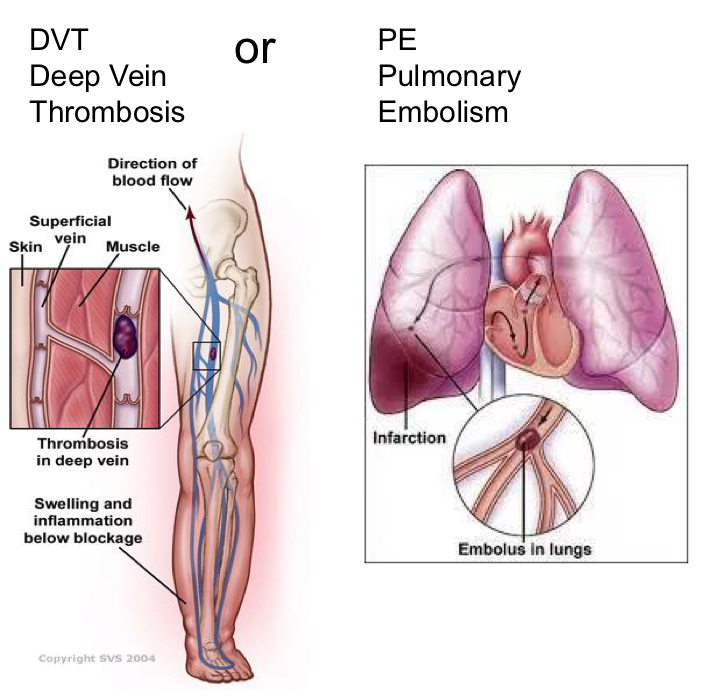
What is Venous thromboembolism (VTE)?
Prevention of deep vein thrombosis and pulmonary embolism
DVT - clot forms in deep vein of legs (can be in arms). Can be asymptomatic until too late (shortness of breath)
PE - artery in lung is blocked by a clot
What are the risk factors of Venous thromboembolism (VTE)?
Hydration
Anaesthetic choice
Positioning during surgery
Length of surgery
Immobility post op
Drugs - OCP/HRT
Obesity
Previous history of DVT/PE
Other medical conditions
How much of a risk is not having any prophylaxis?
VTE would happen in these percentages of surgery
20% of major general surgery
40% of major orthopedic surgery
44% of elective hip surgery
10-20% of medical patients
Need to consider patient risk factors and surgical risk to decide appropriate thromboprophylaxis. Has to balance against risk of bleeding
How is VTE risk managed?
Mechanical prophylaxis - graduated elastic compression socks, reduce venous stasis
Pharmacological prophylaxis - injections of heparin/fondaparinux, oral anticoagulants, aspirin, side effects and contraindications
Mobilisations/leg exercises
Hydration
What surgical factors influence pain?
Intraoperative pain management
Nature and duration of surgery
Site and size of infusion
Extent of surgical trauma
Patient factors
How is it known which analgesic to pick?
Mild to moderate pain - strong opioid ± nonopioid ± adjuvant
Moderate to severe pain - weak opioid and/or nonopioid codeine/tramadol ± adjuvant
Severe pain - non opioid codeine/tramadol/NSAID ± adjuvant
What are the opioids, adjuvants and others to choose from?
Opioids - morphine, oxycodone or dihydrocodeine
Adjuvants - paracetamol regularly ± NSAID
Other - PCA, epidural, nerve blockers, ketamine, gabapenguin
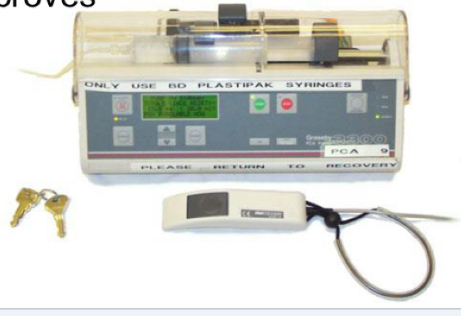
What is patient controlled analgesia (PCA) and how does it work?
Intravenous opiate - morphine in infusion pump
Patient titrates analgesia for breakthrough pain
Limits set for dose and lockout to prevent overdose
Can set continuous background if necessary
Records 24 hour opiate use
As pain decreases can switch to oral, stop oral opioids if still on PCA
Monitor opiate toxicity (sedation, respiratory depression, pinpoint pupils) and pain score
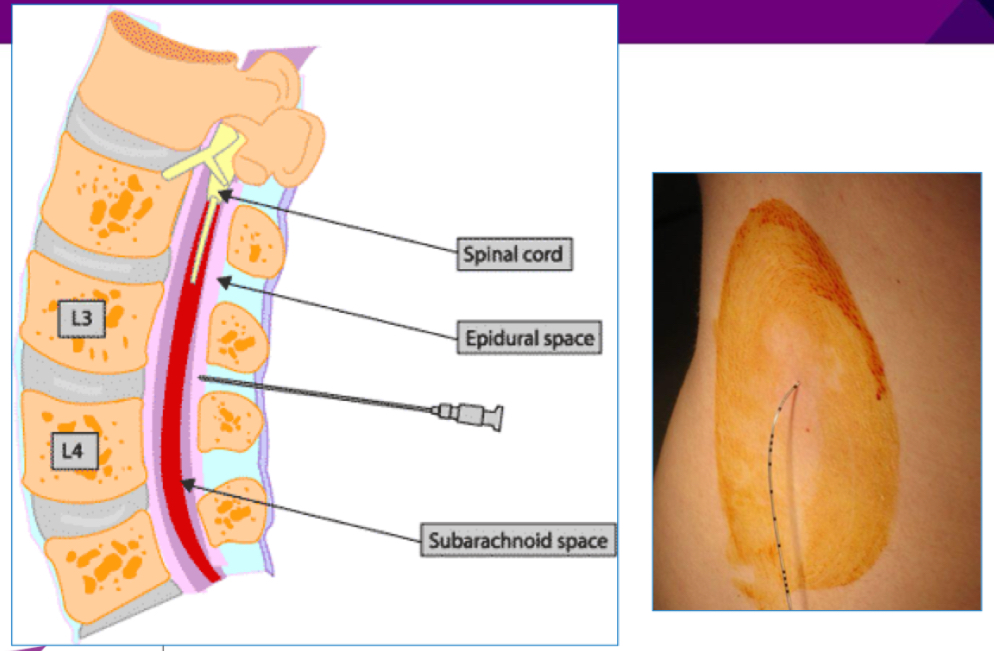
How does the epidural work?
Local anaesthetic ± opiate in the space outside the dura (eg bupivacaine + fentanyl)
Drugs can selectively block sensation without shutting off motor function entirely
Level of analgesia depends on where the catheter is inserted
Bonus with continuous background or as a PCA
What are the potential side effects of epidural analgesia?
Individual drug side effects
Hypotension
Bradycardia
Haematoma risk with heparins - note timings
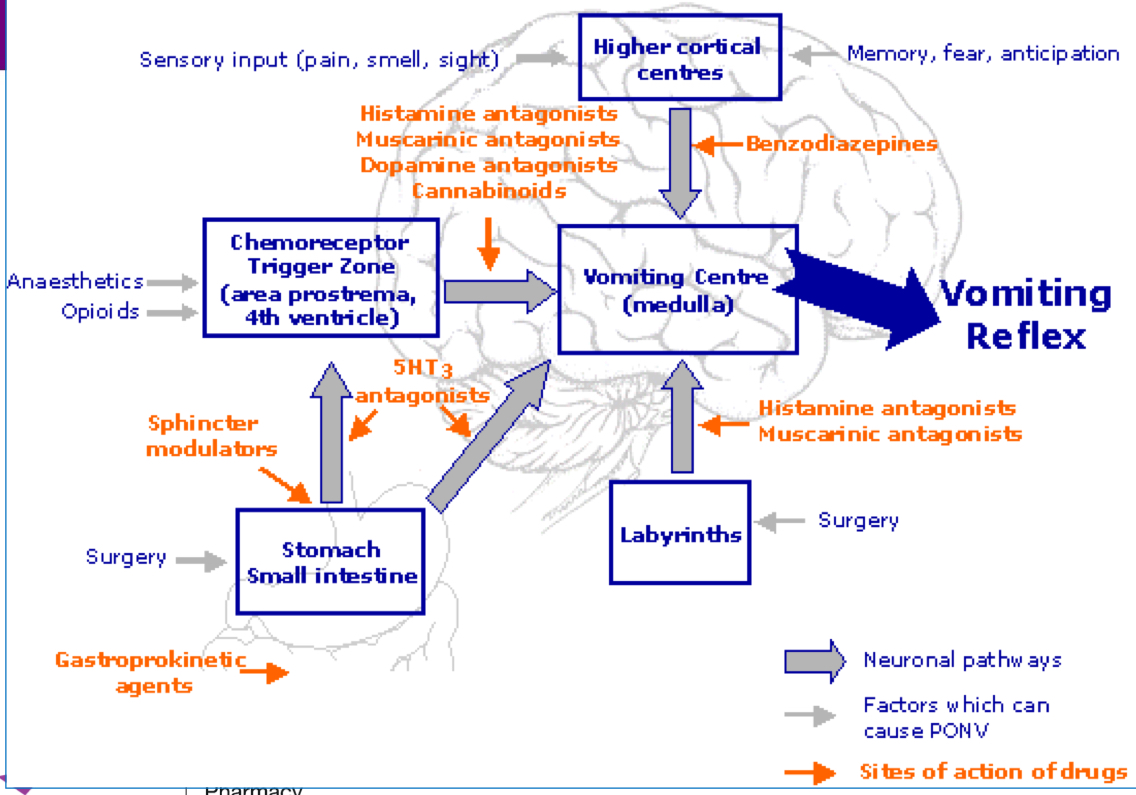
What are the consequences of post op nausea and vomiting?
Potential for aspiration of vomit
Delayed administration of opiates
Would disruption after abdominal surgery
Dehydration/electrolyte disturbances
Delay in mobilisation and recovery
Patient discomfort, distress and fear
20-30% of patients experience it
What are the risk factors of PONV?
Patient - age, gender, anxiety, history of PONV
Surgery - GI surgery, long surgeries
Anaesthestic - general has a higher risk than local
Post op
Cyclosine are first line agents used
What advice are patients given to prepare for knee replacement surgery?
Losing weight, watching her diet to reduce strain
Moving ankle, leg, knee exercises for circulation, pain and discomfort
Making sure home environment is easy to live in after surgery
Remember to bring in medication
For a patient having knee replacement surgery what does NICE say about reducing venous thromboembolism risk?
Offer VTE prophylaxis to people undergoing elective knee replacement surgery whose VTE risk outweighs their risk of bleeding
Aspirin (75 mg or 150 mg) for 14 days.
LMWH (Low molecular weight heparin) for 14 days combined with anti-embolism stockings until discharge.
Rivaroxaban
What is a common LMWH given to reduce VTE risk?, include dose
Enoxaparin sodium
40mg injection to be given 12 hours before surgery then 40mg every 24 hours
How can pain be managed after knee surgery?
Manage pain so she’s not in bed all day - reduces risk of VTE
Oral medications
Paracetamol
NSAIDs
Opioids for moderate to severe pain
What surgery/medication side effects can happen and how can it be fixed?
Side effect of opioids is constipation - prescribe laxative
Respiratory depression as well - prescribe naloxone
Post op nausea - prescribe cyclizine
Infections after surgery - prescribe antibiotics