A&P 3: Exam 1
1/109
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
110 Terms
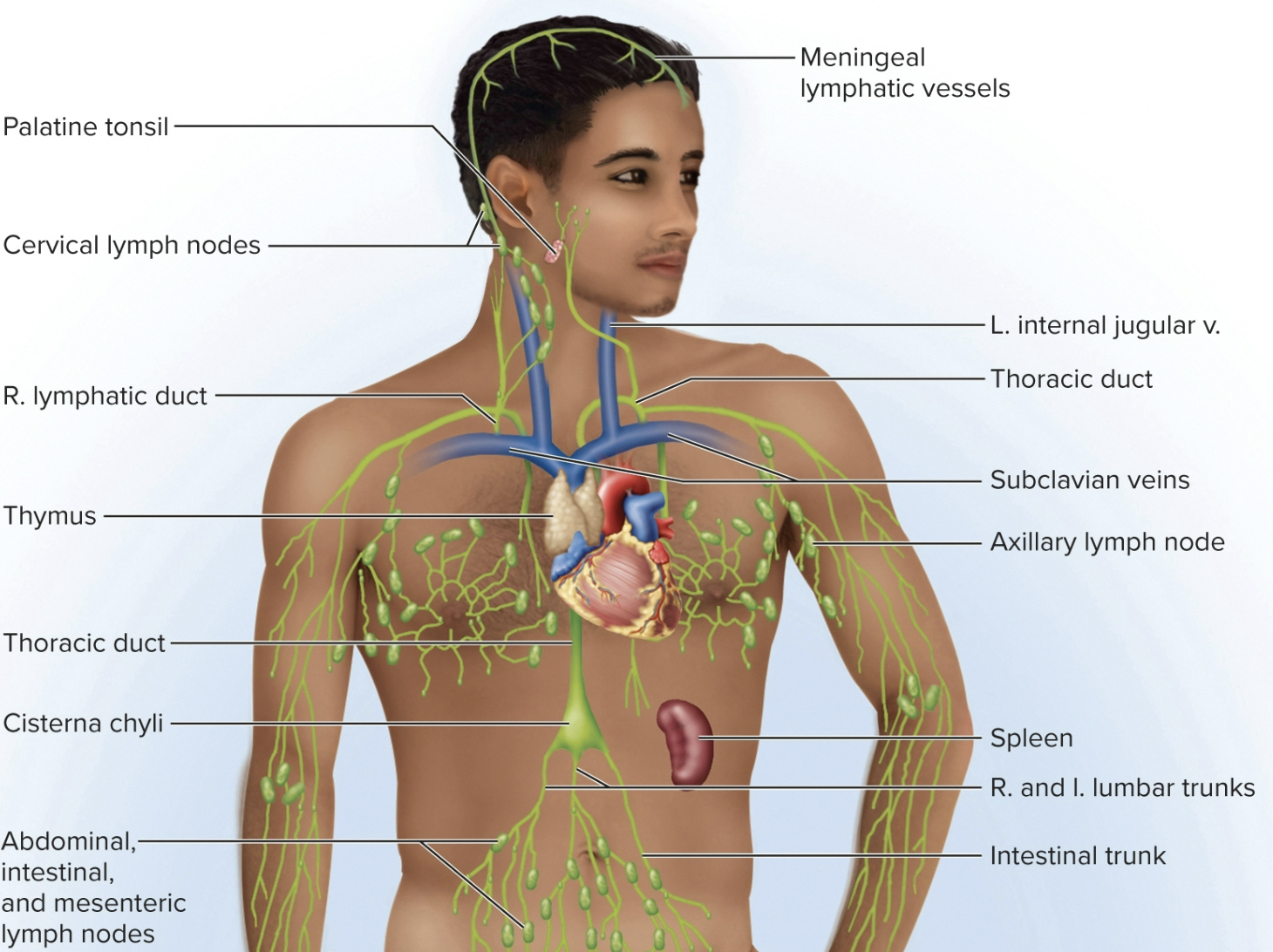
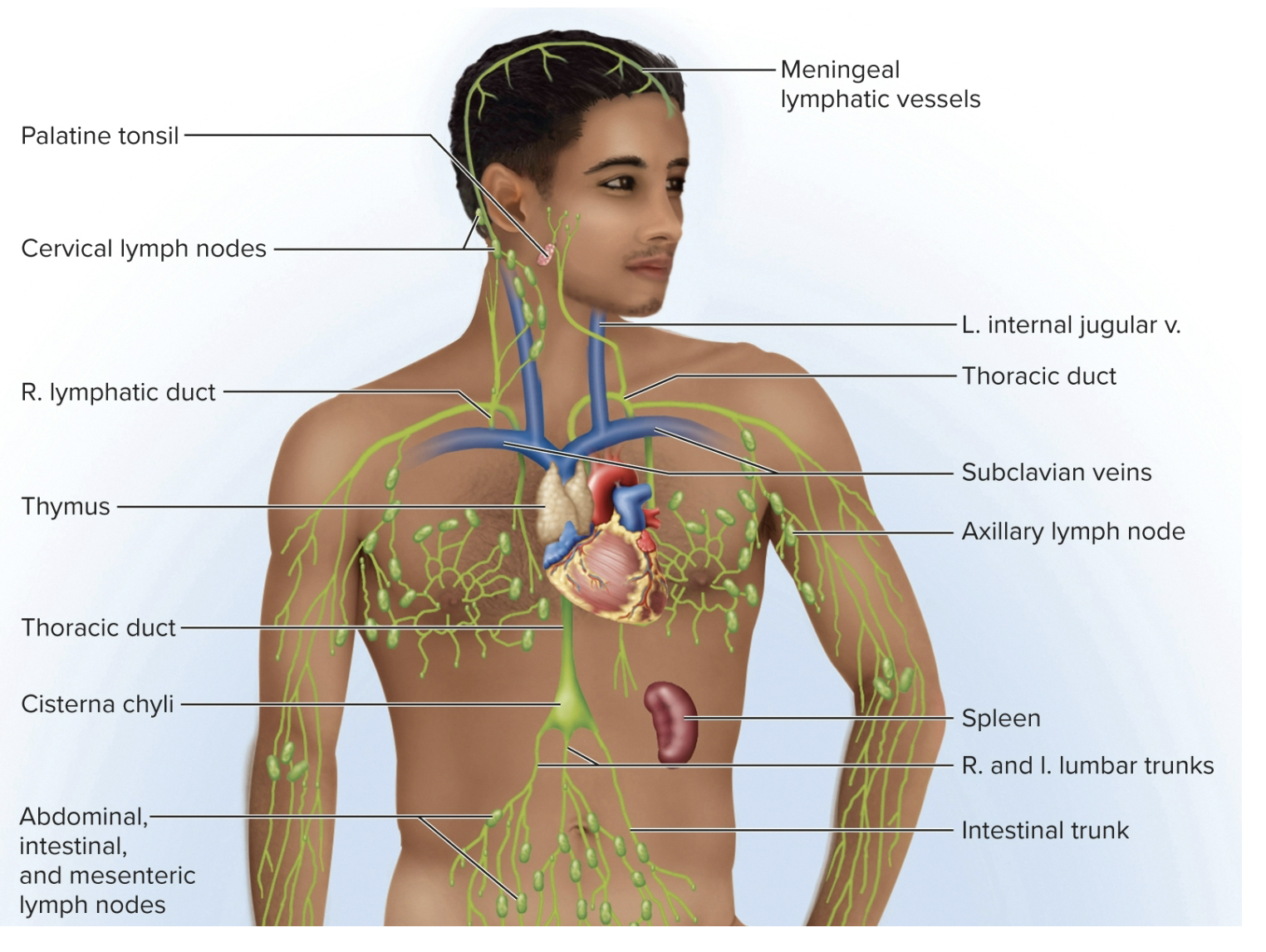
Lymphatic (lymphoid) system
(A set of tubes) circulatory system that drains and removes excess interstitial fluid (prevents edema)
includes lymphatic vessels that penetrate most tissues, with lymphoid tissues/organs that produce immune cells
prevents fluid accumulation in tissues
the immune system is it’s second part (immune surveillance)
Lymphoid system: lymph (fluid)
clear, colorless fluid, similar to plasma, but low in protein
can help return plasma proteins to the blood
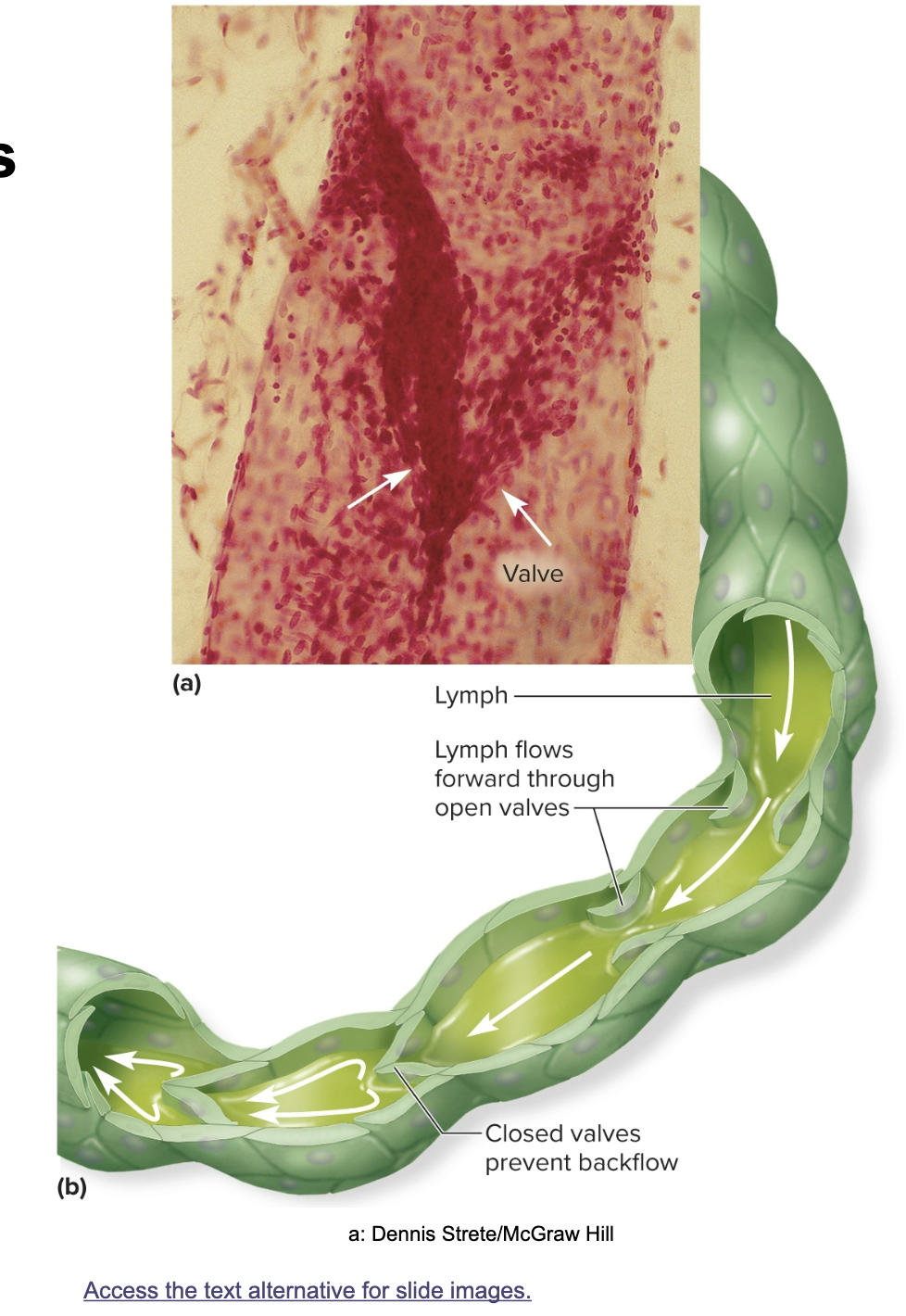
flows at low pressure
stretching - stimulates contraction
moved down the tubes by rhythmic contractions of lymphatic vessels, squeezing of skeletal muscles, rhymthic pulsations of nearby arteries, a thoracic (respiratory pump; breathing in/out), and rapod blood in subclvain veins draws lymph down the tubes
Fluid Recovery:
interstitial fluid that enters the lymphatic capillaries (fluid comes out of capillaries into interstitium, then goes from intersititum into the lympathic system)
classified as ECF (extracellular fluid)
ultimately returned to venous circulation (venous system)
1) maintains fluid balance between the blood and interstitial space
2) returned to the blood at the same rate it is produced
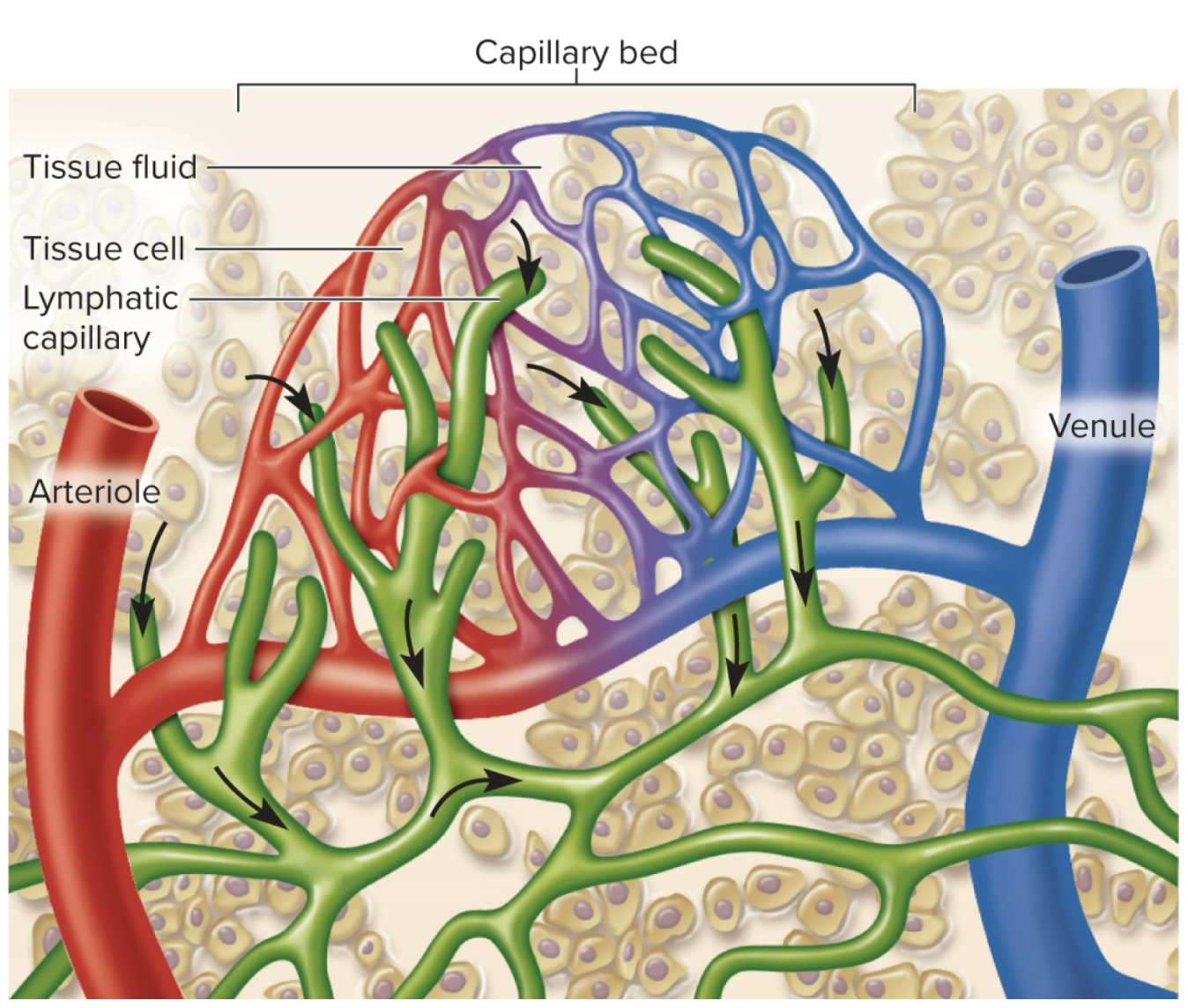
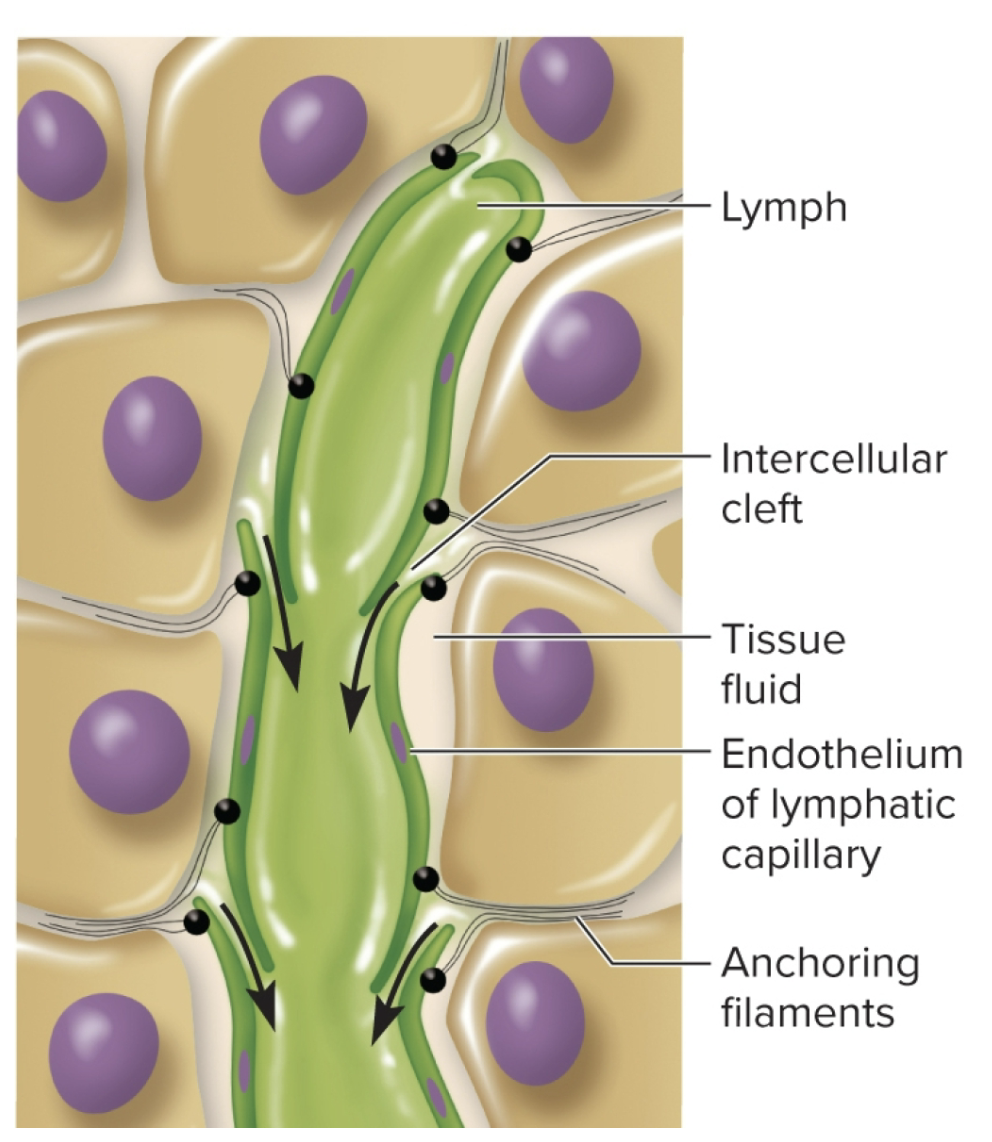
Lymphoid system: lymphatic capillaries
microscopic vessels that penetrate nealry every tissue, taking interstitial fluid by it’s gaps
flow like the venous system (driven by skeletal mmuscle pump)
contains one way valves (keeps flow in one direction)
High pressure causes valves to shut pushing interstital fluid to the lymph nodes. low pressure opens them allowing fluid to come in (not on exam b/c confusing)
assisted by the tunica media
Absent from cartilage, cornea, osseous tissue, and bones/bone marrow (b/c they dont have lymphatic draining)
very similar to how blood moves thru veins (skeletal muscle squeezing it)
fluid comes out of gaps (some sources call it intercellular clefts)
arteriole/venule capillaries secrete fluid and enter these capillaries
Lymphoid system: lymphatic vessels
made from lymphatic capillaries that penetrate nearly every tissue by transporting lymph to the lymph nodes. These vessels converge to form larger (11) lymphatic trunks (on test)
made of: tunica interna, media and externa (thinner) much weaker structure compared to veins/can barely see them
Converges into two collecting ducts:
1) Right lymphatic duct: half of the system drain into the subclavian veins ( right arm, right thoracic region, and right side of the head, and a little bit of the liver) and lymph them become plasma, and empties into the subclavian vein (right side)
right upper wuadrant of body drains to right subclavian vein via lympahtic duc
2) Thoracic duct: larger and longer, begins as a sac in abdomen called (cisterna chyli) receives lymph node from digestive system & rest of the body (whole bottom of the body, left side of the body, left side of the head, neck, and thorax) drain into the left subclavian vein via thoracic duct
lympahtic system: immune system & lymph nodes
lymph nodes flow thru lympathic nodes ( important for immune function)
full of reticular tissue: helps filter out, trap, and detect foreign matter found in the lymph
nodes are loaded with lymphocytes & macrophages *forms a gauntlet
Infection in the lympathic sysmtem?
infection occurs in the tissue first
pathogens will go into the lymph nodes and flow thru a lymph node
provides surveillance of the interstital fluid draining tissue that allow immune system to mount a defense against the infection
Edema in tissues
where rate of capillary filtration is greater than lymphatic removal causing accumulation of excess interstitial fluid
Two main causes:
1) Too much filtration (inflammation/trauma):
increased Filtration coefficient (Kf) b/c increase in hydraulic conductivity of capillarly wall → capillaries become “leaky”
increase Net filtration pressure (NFP) due to vasodilation and increase capillary pressure
Seen in inflammation (“inflammatory soup”) and tissue injury
2) Lymphedema (next slide)
ALSO helps with tissue clean up:
swelling compresses veins/reduces venous drainage
forces open valves of lymphatic capillaries, promoting lymphatic drainage of bacteria, dead cells, and debris
immune system
not an organ system, but cell population that defends against pathogens/diseases and in concentrated in the lymphoid system
Two divisions:
four primary categories of pathogens: bacteria, viruses, fungi, parasties
system must differentiate from “self” to “non-self” in order to destroy potential pathogens (based on surface proteins/cells/free substances that are normall found in our “self” cells/body fluids)
include foreign markers called “antigens (immunogens)
Important: helps guard between mutations of our own cells (ex; tumors; cancer)
everywhere in the body except avascular tissue
confines infection to one region (smart) makes it easier to battle w/
lymph nodes
bean/kidney shaped struture that cleanse lymph (debris), are is site of lymphocyte activation.
enclosed w/ fibrous capsule w/ trabeculae tha devide inferior into compartments
parenchyma divided into cortex & medulla
has ferminal center in cortex: where b-cells multiple and differencial in plasma cells
several afferent lymphatic bessels lead into the mode along its convex surface
lymph leaves node thru 1-3 efferent lymphatic vesells thay leave the hilum
simplest organ and we see them in the neck, armpits, groin, gut!
most numerous organ (apprx. 450 in trypical adult)
picks up foreign chemicals in tissues that passes thru the nodes (organ), samples to see if theres anuthign fangerous
helps isolate infections! (doesn;t allow infections to spread)
contains lymphocytes and macrophages
lymphatic tissue
high density of lymphocytes (but scattered) in connective tissues of mucous membranes/organs
ex of mucosa membranes: respiratory, digestive, urinary, and reproductive tract
MALT: mucosa-associated lymphoid ___ or GALT if in gut
macrophages are found densely here too (helps ingest & clean up (destory) pathogens, sending debris to the general circulation)
lymphocytes
lymph cells that have 11 of three branches?
one of the top 5 WBC
more associated w/imme system than other WBC
Lines of defenses against pathogens (immune system)
this division prevents pathogens (viruses, bacteria, fungi, & parasites) from producing diseases in body initially by physical barriers like…
1) First line defense: skin/mucous membranes as a barrier
2) Second line defense: protects when pathogens break thru skin/mucous membrane barriers (leukocytes & macrophages, antimicrobial proteins, natural killer cells, fever, & inflammation)
3) Third line defense: adaptive immunity, mechanisms that defeat a specific pathogen & leave body with memory of it.
includes processes that react to a lot of “common markers”
includes the 4 types of WBCs (myeloid): neutrophils, eosinophils, basophils, and monocytes as well as the macrophages (monocytes)
lymphoid organs
organs where lymphoid cells/tissues are concentrated
1) Primary organs: thymus, and bone marrow
site where B & T cells become immunocompetent (able to recognize and respond to antigens)
2) Secondary organs: tonsils, lymph nodes, and spleen
locations where immunocompetent cells migrate and populate (these take place in early embryonic development and move around to other sites living ur whole life)
ex: mucosa (invaginations of the body) where pathogens are most likely to enter (ex: digestive tract, respiratory tract, and urogenital; urinary and reproductive tracts)
Lymphedema
A blockage in lymphatic system (lymphatic insufficiency) due to external compression and closing of lympathic vessels
ex: when tumor grows and squishes lymphatic vessel
primary lympathic insufficiency: congenital malformation
secondary lymphatic insufficiency: due to trauma, tumor, surgery, etc
immune cells
found in the lymphatic tissues distributed to many areas of the body
circulate thruout bloodstream and tissues of the body
can move back and forth between capillaries & surrounding interstital fluids of the tissues into the lympathic circulation
found everywhere except avascular tissues
Adaptive immunity: (immune system)
third line defense system that, recognizes and reacts to very specific pathogens, developed only w/ exposure and maintains immune memory (systemic effect)
two types cellular and humoral
ex: getting measles
important to combat pathogens not removed by the innate immune system
B & T cells are associated
other two (non-myeloid) type of lymphocytes
cellular (cell-mediated) adaptive immunity
specfic defense where T lymphocytes directly attack/destory foreign cells/diseased host cells
rids body of pathogens that reside inside human cells (parasitic worms, cance cells, transplanted cells) where theu are inaccessible to antibodies
4 classes of T-cells: Cytotoxic, Helper, Regulatory, Memoru
General stages: recognition, attack, and memory
cytotoxic T (tc) cells
carry attack out on another cell when the cell displays its antigen
when it recognizes the complex of antigen/MHC-1 protein on the diseased/foregin cell it “docks” on that cell
after docking it delivers a lethal hit of chemicals: perforin and granzymes (kill cells)
interferons: inhibit viral replication activating/recruiting macrophages
tumor necrosis factor (TNF) aid in macrophage activation and kills cancer cells
only respond to MHC - 1 proteins
once it finishes its job it turns into a memory cell
Helper T (Th) cells
promote activites of other immune cells
only respond to MHC-2 proteins
Regulatory T (Tr) cells
limit the immune response
Memory T (Th) cells
responsibe for immune primary response in celllular imunity
long-lived
more numerous than naive T cells
fewer steps to be activated so they respond faster (T cell recall response)
humoral (antibody-mediated) adaptive immunity
mediated by antibodies that do not directly destory a pathogen but tag it for destruction
useful for extracellular viruses, bacteriam yeasts, protzoans, and molecular (noncellular) disease agents like toxins and venoms
ex: B-cells
Has Primary and Secondary responses
Normal Immune Physiology
when operating normally, pathogens are found and eliminated successfully
Natural active immunity
Production of one’s own antibodies/T-cells as a result of infection or natural exposure to antigen
catching a cold
innate immunity
Artifical active immunity
Production of one’s own antibodies or T-cells as a result of vaccination against disease
Vaccine
consists of dead/attenuated (weakened) pathogens that stimulate the immune response without causing the disease
booster shots: given to restimulate immune mmeory to maintain high level of protection
Natural passive immunity
temporary immunity that results from antibodies produced by another person
fetus acquires antibodies from mother thru placenta, baby acquries thru breast-feeding
no memory
Artificial passive immunity
Temporary immunity that results form the injection of immune serum (antibodies) from another person or animal
emergency treatment for snakebite, botulism, tetanus, rabies, etc.
no memory
Pathological Immune Physiology
involve either excess activity or insufficient activity
excess activity: exemplified by autoimmune disorders (system over-reacts/attacks itself) ex: allergies
Insufficient activity: excess disease. ex: immunosuppression: immune function is unnatrually supresed and pathogens get out of control (ex: glucocorticoids; cortisol causes immunosuppression and excess secetion/administration causes pathogen invasion)
ex: bone marrow stem cell disorder: lack of WBC production (leukopoiesis)
Physical barriers of the innate immune system
The epithelia (skin) is the first defense to prevent pathogenic entry into the tissues of the body
integument made of a thick stratified epidermis that is kertinized (tough) have tight junctions and desmosomes making it difficut to be penetrated
if penetrated, we have adipocytes of the hypodermis that secete anti-pathogenic secretons for prevention of pathogens
weak barriers (not as thick): epithelial linings of the GI, respiratory or urogenital tracts (good target for pathogens)
nose hairs, glandular secretions (antibacterial eye secretions): help filter out pathogens
etc: mucus, coughing, or sneezing
Inflammation
a local defensive response to infection from pathogen.
Due to trauma (physical damage, burns, etc)
purposes:
helps remove debris from damaged tissue to initiate tissue repair
helps promote repair and healing, preventing infection (b/c body is notifiyinh you to treat it).
limiting spread of pathogen (then destroys)
basophils and mast cells are activated
involves LOTS of cytokines including interferon, interleukins, chemotactic factors, etc
Inflammation & fibrinogen
it filters into tissue fluid, clots to forma a sticky mesh that walls of microbes
heparin prevents clotting at injury site
here, pathogen is in a fluid pocket surorunded by clots
it is then attacked by antibodies, phagocytes & other defenses
after an hour, neutrophils come exhibiting chemostaxis when they leave: attracts bradykinin and leukotrienes
Cardinal signs of inflammation ON EXAM.
1) Redness (ruber): due to hyperemia
2) Swelling (tumor/edema): due to increased fluid filtration from capillaries
3) Heat (calor): due to hyperemia
4) Pain (dolor): injury to nerves creating prostaglandins
Inflammatory soup
includes heparin and histamine
mobilization of inflammation
The immediate requirement after tissue injury is to get defensive leukocytes to the site quickly (bc capillary gaps increase)
due to hyperemia (increase in blood flow meaning more WBC & washes toxins/metabolic waste from site rapidly)
vasoactive chemicals causes = local vasodilation (more WBC/filtration)
includes histamine, leukotrienes, and other cytokines which are secreted by basophils, mast cells, & cels damaged by trauma, toxins, or organisms, triggering inflammation
Diapedesis (emigration) inflammation
leukocytes crawl through gaps in the endothelial cells *that are widened and enter tissue fluid
extravasated: cells and chemicals that have left the blood stream
margination (inflammation
the ability of WBC to stick to the capillary wall easily, where it senses that inflammation is going on and near source of infection
Cytokines
small proteins that function in chemical communications between cells
alter physiology of receiving cell (both local and systemic)
includes interferons, interleukins, chemotactic factors
Basophils (leukocyte)
activated during inflammation, and reside in every tissue, they secrete most of the inflammatory “soup” (grp of mediators: cytokines) more associated with mucosa
1) local effects they secrete include:
Prostaglandins: causes elevated sensitivity to paid (hyperalgesia)
Bradykinin: causes pain directly (color)
Histamine: causes vasodilation of local arterioles, increasing blood flow causing redness and heat, can lead to edema
Heparin: inhibits coagulation (clot formation). Causes leakyness of capillary plasma (increase in hydraulic conductivity).
leukotrienes: activate/attract neutrophils/eosinophils when infection involved
cytokines: increase immune activity (stimulation of non-specific WBCs, macrophages & defenses) lots of positive feedback
Mast cells have similar functions to basophils but found in connective tissue and ARENT leukocytes!
Resolution: immune system
when the battle is won and damaged has repaired, inflammation shuts down.
if this fails, chronic inflammation can occur leading to long lasting pathologies
Chemotaxis
ability of WBCs to move (taxis) torwards a source of infection where signals are concentrated (chemo)
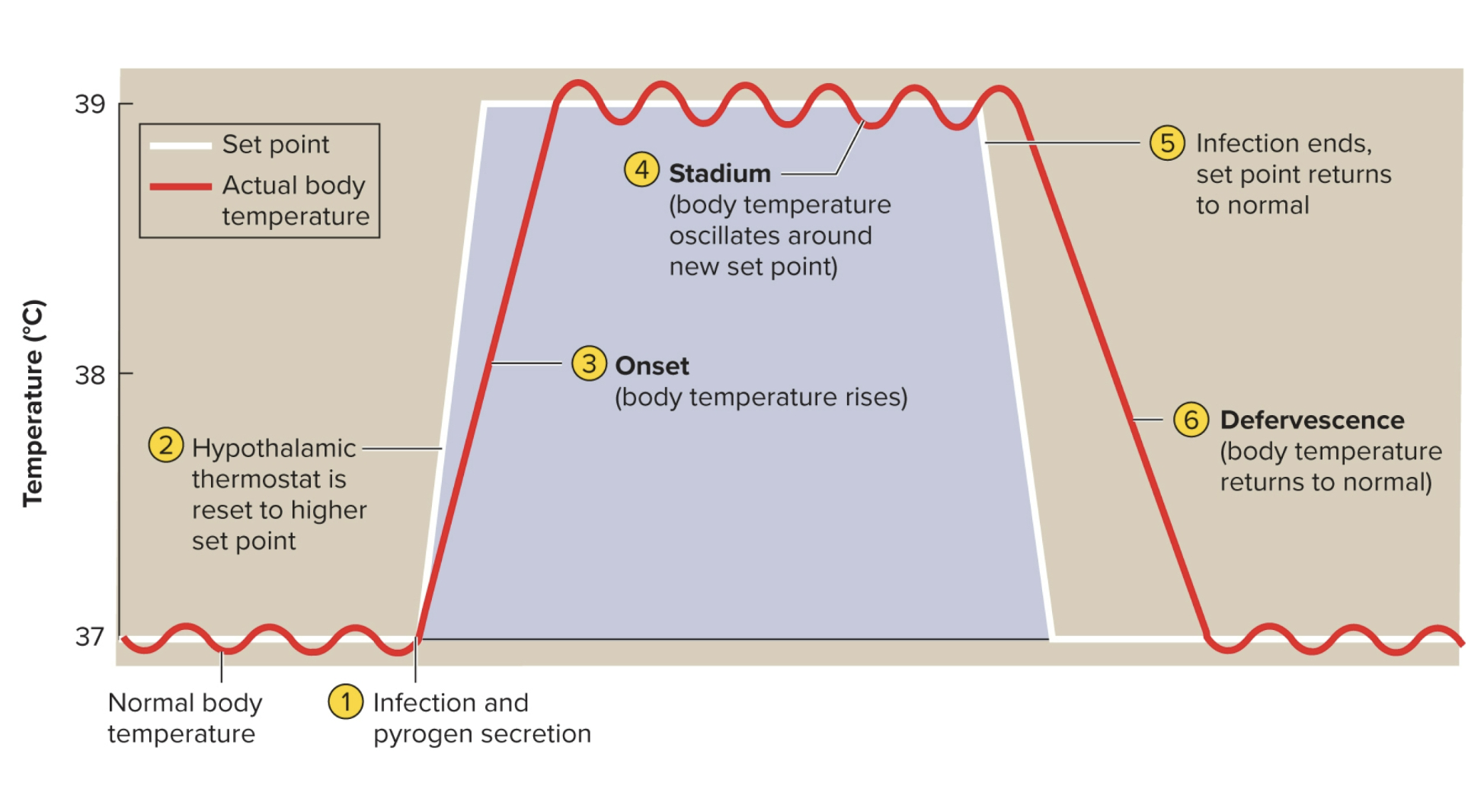
Fever (pyrexia)
an abnormal elevation of body temperature due to a release of endogenous (produced from within) pyrogens targeting hypothalamus, a cytokine from an inflamed area, that circulate and target the hypothalamic thermoregulator
due to trauma, infections, drug reactions, brain tumors, etc
promotes interferon activity
elevates metabolic rate to accelerate tissue repair
inhibits reproduction of bacteria/viruses
Interleukins-1: a cytokine that contributes to this effect
stages are “onset”: temp begins to rise and “stadium” where it remains elevated
exogenous pyrogens, byproduct of bacterial infection can cause same increase in temp (however, not adaptive)
recovery is faster when not taking fever reducing medications (antipyretics)
Endogenous pyrogens
fever-producing agents originating from within body (peptides secreted by neutrophils, macrophages)
• These raise hypothalamic set point for body temperature
Exogenous pyrogens
fever-producing agents originating outside the body
• Examples: glycolipids on bacterial and viral surfaces
• Stages of fever: onset, stadium, defervescence
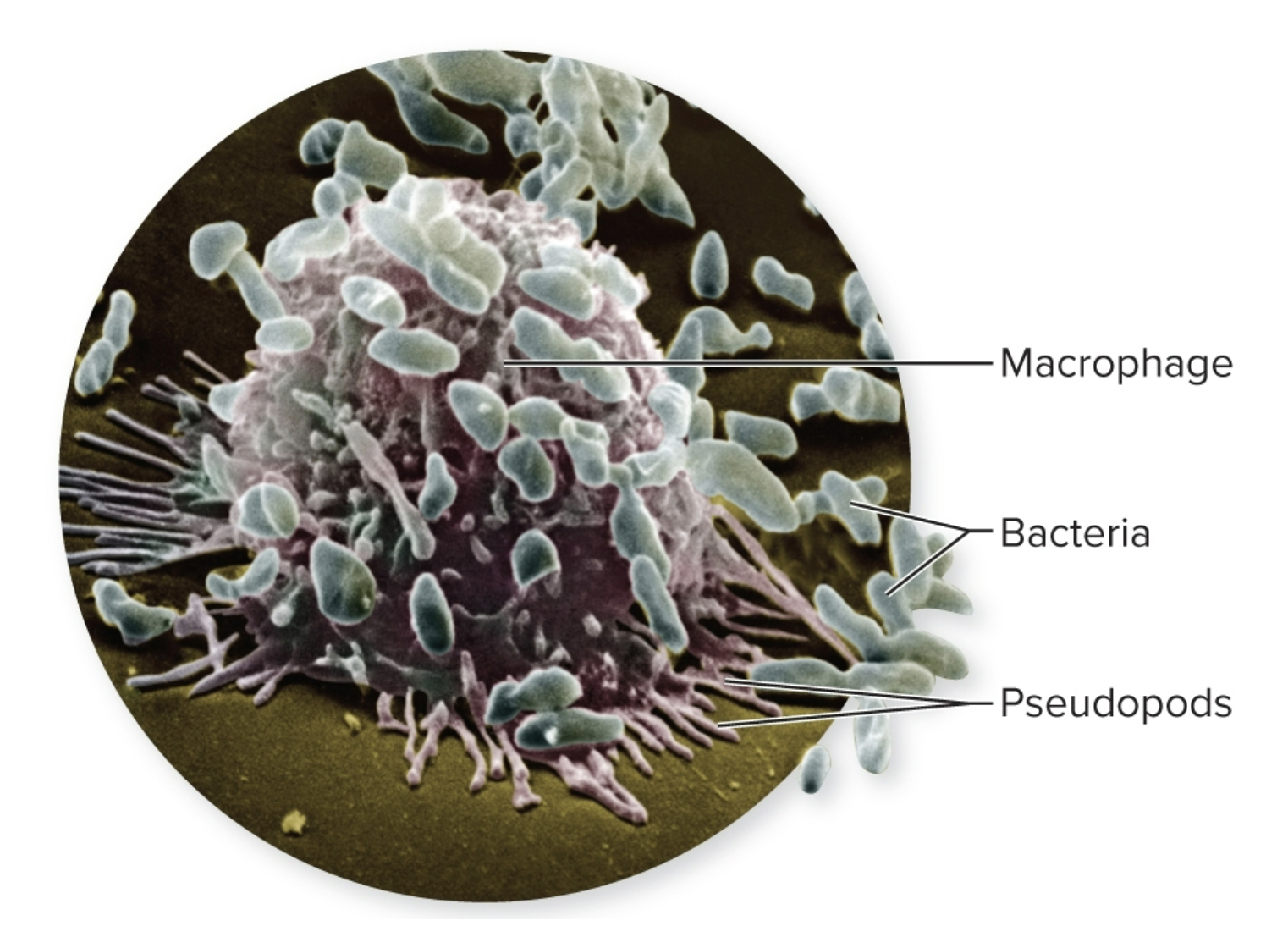
Phagocytes
A cellular defense, includes 2 types: microphage/macrophage cells that ingest foreign cells/debris by phagocytosis (internalized and broken down).
attracted by inflammatory cytokines
functions when leukocytes/macrophages don’t do their thing
microphages
Attack and engulf smaller pathogens and takes/cleanup debris
ex: defined as neutrophils and eosinophils (2/5 WBC)
microfaded (can’t engulf)
part of the innate system
macrogphages
These larger cells attack larger pathogens (parasites)
Larger phagocytes derived from monocytes (a type of WBC)
1) Two types: Wandering & Fixed
wandering: freely move thru tissues, patrolling for pathogens (attracted by cytokines signaling for an infection)
fixed (dendritic cells): remain in a specific tissue (waits for pathogens to come) most dense at points of entry into the body (ex: Kupffer cells(stellate); liver, Langerhans cells; skin, histiocytes; connective tissue, microglial cells; central nervous system, microfold cells: gut)
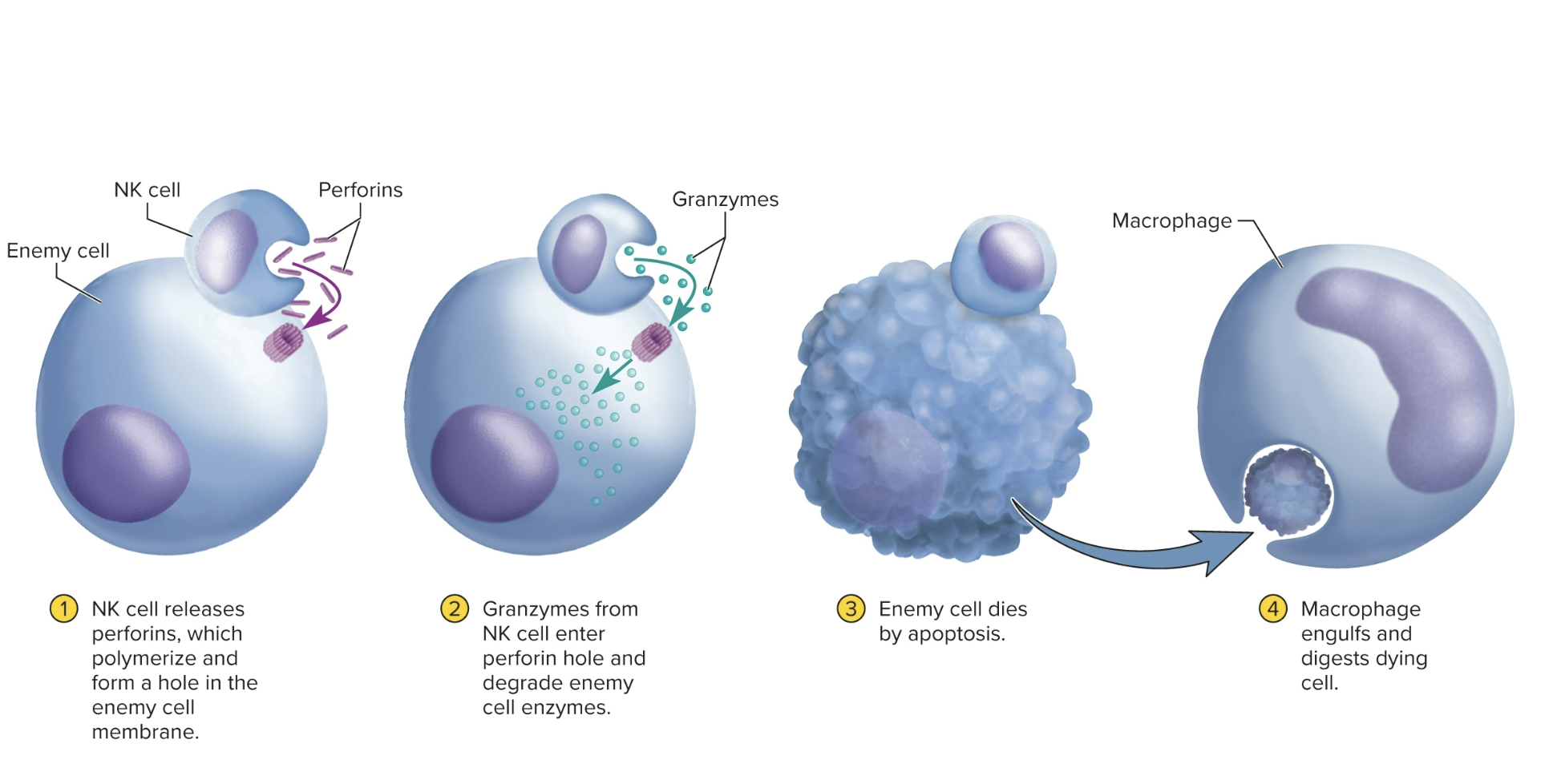
Natural Killer (NK) Cells
Cells patrol body for pathogens/diseased host cells by attacking/destroying microbes, transplanted cells, cells infects by virus, cancer cells.
attacks by secreting perforins (grp of proteins that lyse “punch a hole in” the plasma membrane of bacteria or pathogen)
perforins inject granzymes into cell that help degrade cellular machinery & speed cell’s death.
reliant on the expression of external markers to detect problems, bacteria
type of lymphocyte a component of the innate immune system
Deficiency in these cells: higher rates of cancer & viral infections
innate immunity
Interferons (antimicrobial Proteins)
class of cytokines that act locally (paracrine effector) and are secreted with two situations
1: common) secretes when a cell is infected by a viral infection (causes nearby cells to upregulate their antiviral defenses that interfere with viral replication) doesn’t prevent entry of viruses
attract and increase activity of NK cells and macrophages to destroy cells/nearby cells that are also infected
Interferons: cancer
Secretes when fighting against certain cancers by promoting inflammation which promotes healing
destroy the cell WE DO NOT HEAL IT
Complement activation
group of 30 or more globular proteins that contribute to both innate/adaptive immunity
synthesized mainly by liver
circulate in the blood when inactive (soluble) but turns (insoluble) when performing a pore that punches thru a cell (loses lots of electrolytes and H2O will get into the cell)
can be activated by antibodies bound to antigens (helps indicate a foreign cell:inflammation) or common markers
not normally confined to plasma but can enter interstital spaces during inflammation
Complement activation pathway
Includes:
1) classical pathway
2) Alternative pathway
3) Lectin pathway
Outcomes of complement activation
1) Inflammation: C3a stimulates mast cells/basophils to secrete histamine/other inflammatory chemicals
activates and attracts neutrophils/macrophages
2) Immune clearance: C3b binds w/ antigen-antibody (Ag-Ab) complexes to RBC that circulate thru liver and spleen
macrophages of those organs strip off and destroy the (Ag-Ab) leaving RBCs unharmed
3) Phagocytosis: C3b coats microbial cells (opsonization) & attract and serve as binding sites for phagocyte attachment
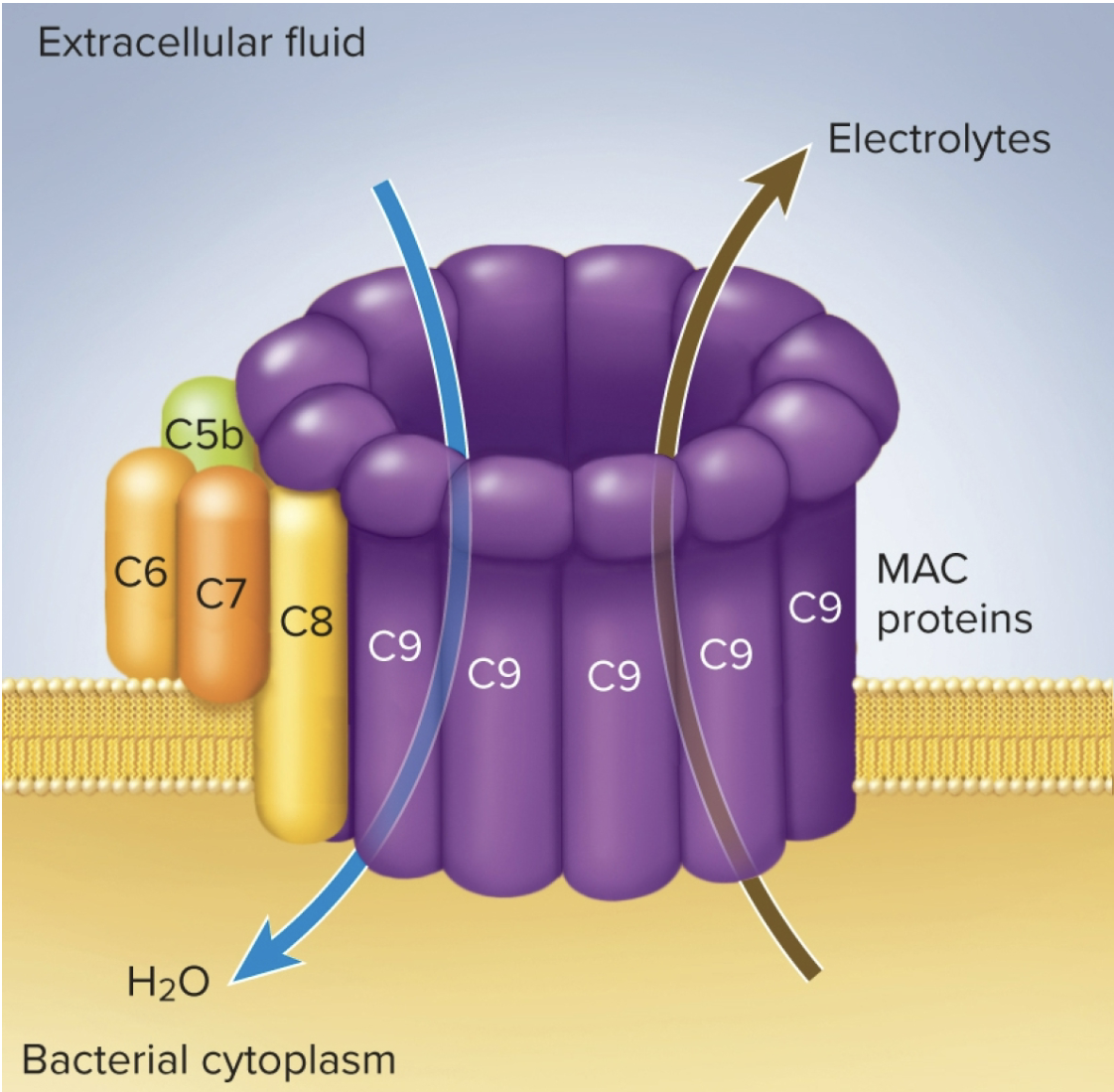
3) Cytolysis: complement C3b initiates formation of C5b
C5b aggregrates w other complement proteins within plasma membrane of microbe
form membrane attack complex (a hole in the target cell membrane where elctrolytes leak out and water fows in rapidky, cell then ruptures: cytolysis)
MAC (Membrane Attack Complex) forms this
classical pathway (complement activation)
Antibody binds to microbe, which changes antibodys shape exposing compleemt-binding sites
binding of the complement C1 sets off a reaction cascade called “complenent fixation”
macrophage punches hole into the ex: “bacterium”
Alternative pathway (complement activation)
complement C3b binds to microbe surface, activating reaction cascade
Lectin pathway (complement activation)
Lectins are plasma proteins that bind to carbohydrates
iin the blood they bind to certain sugars on microbe surface, activating reaction cascade
B & T lymphocytes
A very small minority of cells that ciriculate in the bloodstream in order to exchange between lymphatic tissues and to access all vascular tissues
found in the primary lympathic organs: Thymus and Red Bone Marrow
limited in blood but we do blood test to figure out the amt #
eflects the overall activity of the adaptive immune
system.
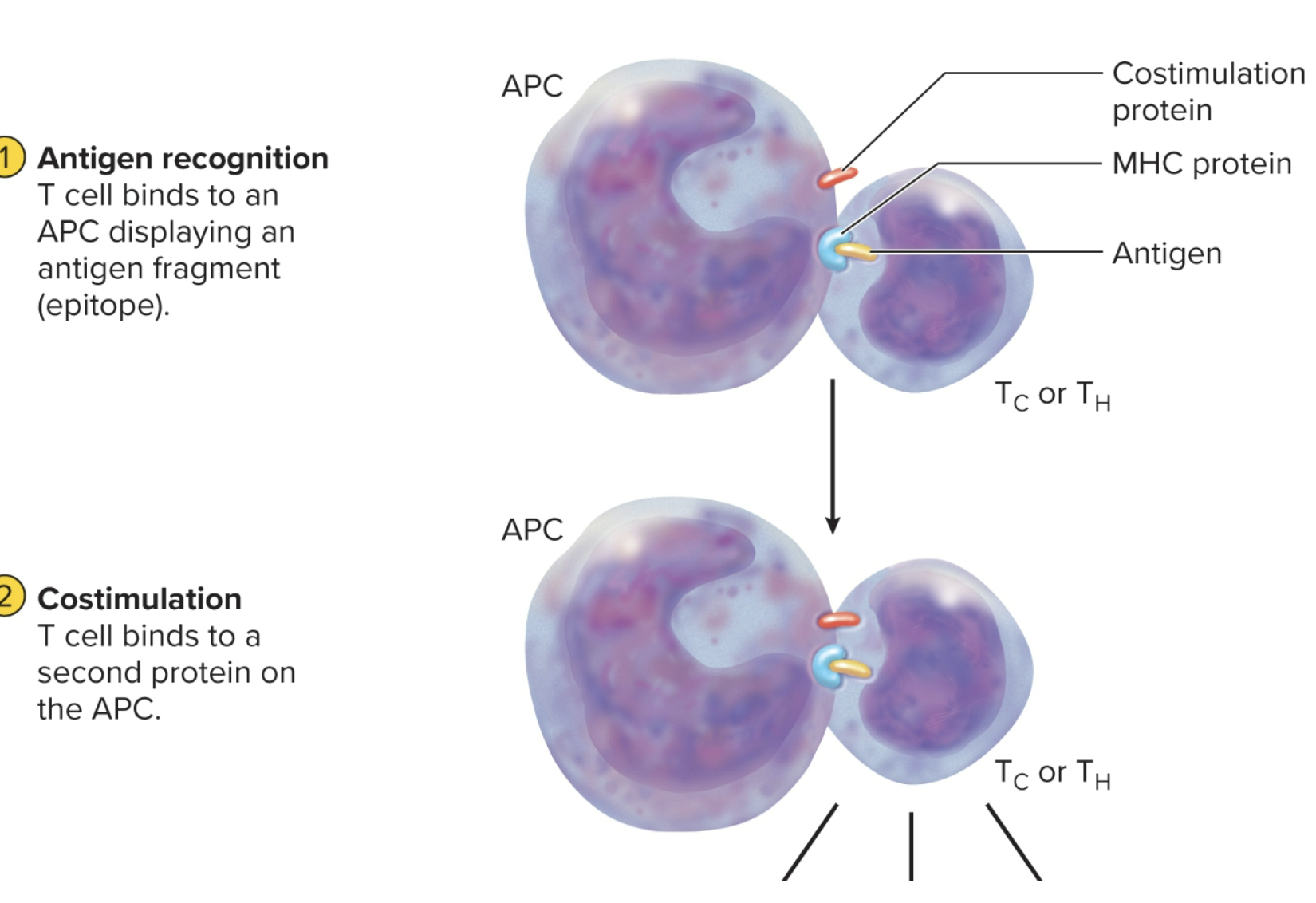
antigen presenting cells (APCs) IMPORTANT
antigen cells that only present T cells interact with and can only recognize antigens on here (so T-cells disregard it)
present via dendritic cells, macrophages, and B cells
if ABC displays a non-self antigen the appropriate T cell will intiate an immune response against the source of the antigen.
function depends on MHC proteins encoded by major histocompatability (MHC) complex genes
acts as cell “identification tags” that label every cell of your body as belonging to you
structurally unique to each individual, except for identitcal twins
Never let monkeys eat bananas (NLMEB)
only these cells have MHC-2
Antigen processing
APC encounters antigen, internalizes it by endocytes, and digests it into fragments
display fragments (epitopes) in the grooves of the MHC protein
MHC molecule/protein
interleukins
how APCs, T-cells and lymphocytes communicate with cytokines
T-cells recognizes Ag-MHC complex then secretes it which then…
1) attract neutrophils and NK cells
2) Attract macrophages, stimulate their phagocytic activity, and inhibit them from leaving the area
2) stimulate T and B cell mitosis and maturation
Primary lymphatic organs: Thymus and Red Bone Marrow
involved in maturation of lymphocytes where they develop immunocompetence
Red Bone Marrow: responsible for production of all formed elements of blood, including B & T lymphocytes (they mature here)
T - cells exit and circulate and taken up by thymus where they undergo their final maturation
Secondary Lymphatic Organs and Tissues: Lymph Nodes
destinations for already immunocompetent lymphocytes
lymph filters for detection of pathogens within interstital fluid. Infections generally occur in tissues and lympathic overflow from these regions
indirectly monitor all tissues drained by lymphatics (ex: nervous tissue drained by lymphatics) everywhere! except avascular tissues
approx. 450 nodes in a typical human
placed on groin, axilla, and neck are extended to confine any infection to the limb or head and can’t expand to other regions
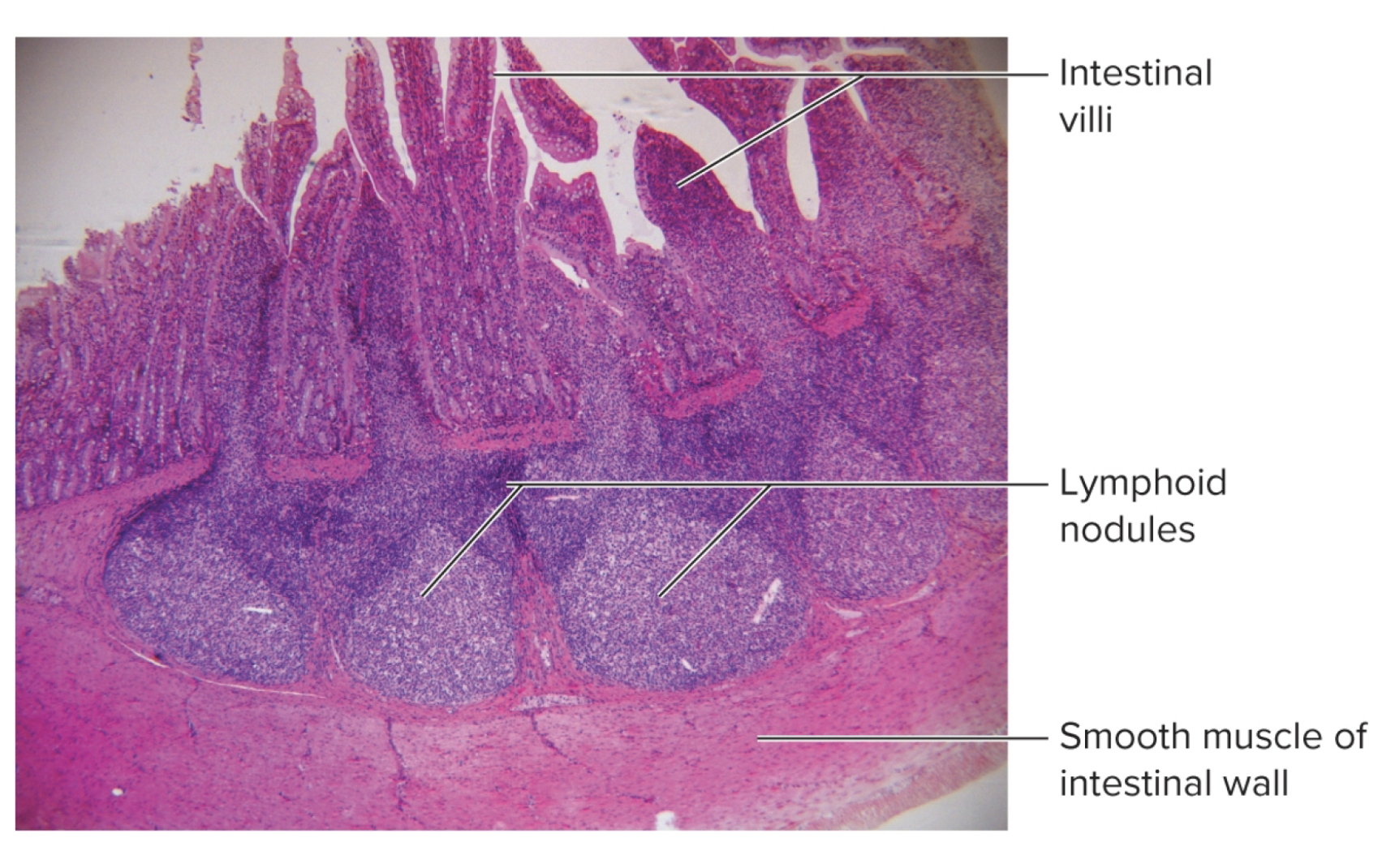
A LOT found in the digestive organs to protect against pathogens (most vulnerable)
swelling indicates exposure to a pathogen and response includes active division of the lympocytes within (hence why increase in size)
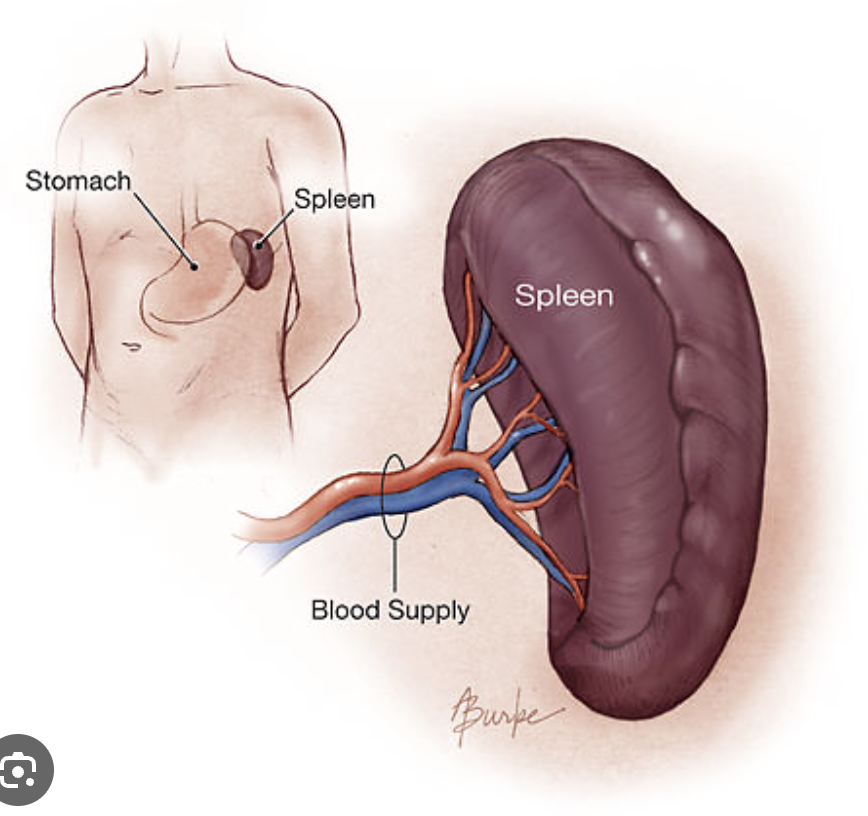
Spleen: Lymphatic system
The body’s largest lymphoid organ. It’s a lymphatic filter to monitor blood passing through.
The sinusoid capillaries here are very leaky
surrounding immune cells detect pathogens (infections) in blood
also occasionally removes/recycle RBC (red pulp)
first place to detect blood infection!!
more organized than other diffuse lymphatic tissue (tonsils, lymph nodes)
Parenchyma *two types of tissue:
red pulp: sinuses filled w/ erythrocytes
white pulp: lymphocytes, macrophages surrounding small branches of splenic artery (monitors foreign antigens)
medial hilum for passage of the BIG splenic artery, vein and lymphatic vessels
if you lose this organ the liver can take over bc it has similiar functions (BUT highe risk of immune system failure)
Diffuse Lymphatic tissue
found within the mucosal that lines the lympathic tissue (MALT) of the gut, respiratory, and urogenitcal tracts
dividing lymphocytes found here
minimal organization here
Tonsils
patches of lymphoid tissue near the entrance of the pharynx that guard against inhaled/ingested pathogens (food/air), encapsulated by limited connective tissue
considered an organ however less complex and organized
covered by epithelium and lined by lymphoid nodules
three main sets: single pharyngeal, palatine, and lingual
Antigen (immunogen) receptors
Any molecule (protein) that can bind an antibody
most have large molecular weights (over 10,000 amu) and some structural complexity
basis of the specific immune system (SIS) associated with B &T lymphocytes
it is antigenic (immunogenic) when it provokes an immune response from the SIS
markers that have a unique shape nd form that usually involves a
protein component (may involve carbs/lipids)
provoke an immune response b/c it is “non-self”
expressed on external surfaces of pathogens/byproduct (excretion) of a pathogen)
neutral debris (ex. animal hair, pollen) not harmful, can also provoke an immune response (allergic response)
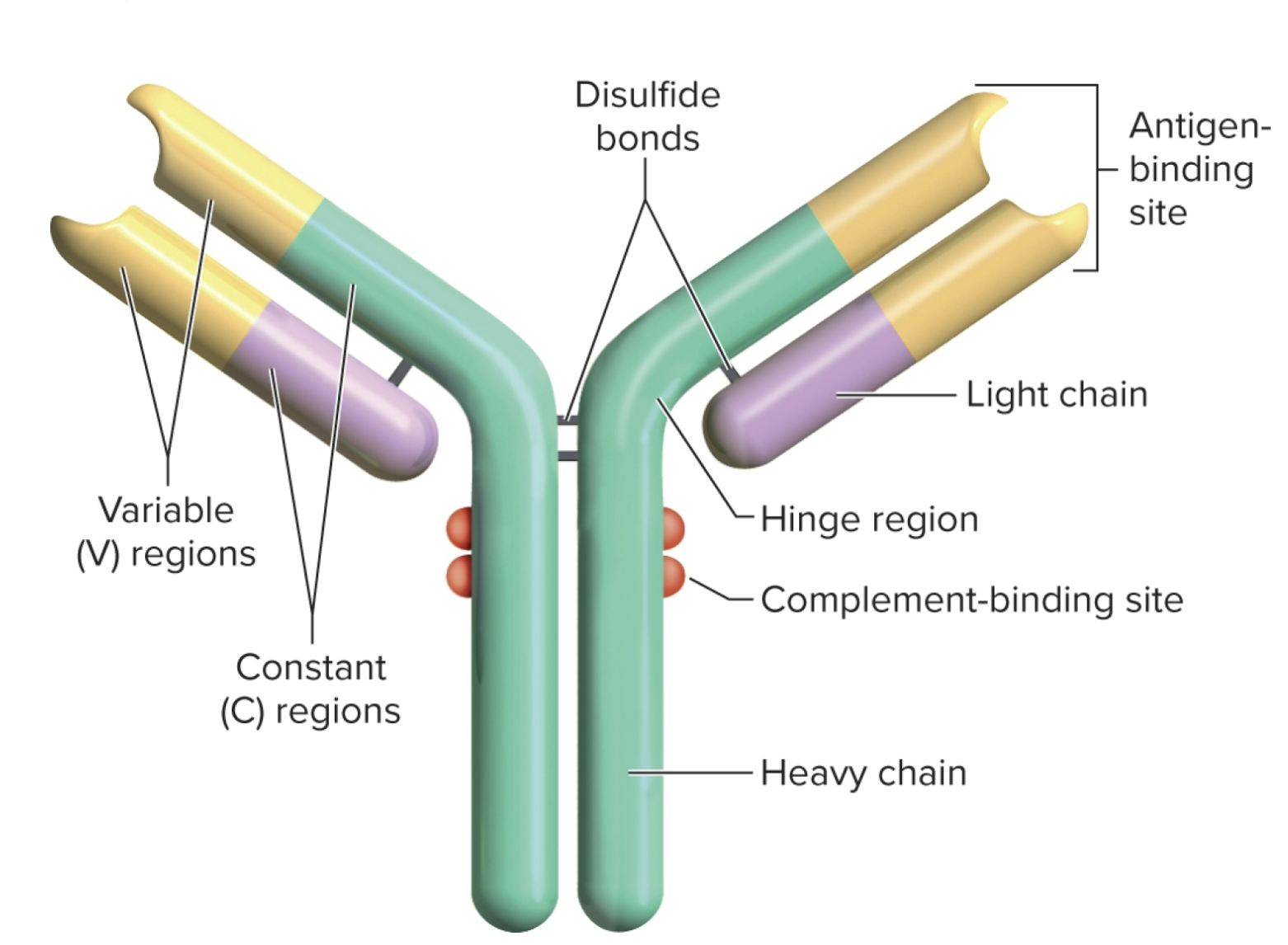
Epitopes (antigenic determinants):
expressed by B & T lymphocytes and consist of proteins thay bind to antigens w/ a “lock and key” specifivity based on shape and charge distributions of the antigen to enable an immune repsonse. (huge diversity of antigen receptors derived from DNA)
only the light chain and part of the heavy chain has a antigen binding site
antibody classes
called GAMED five classes of antibodies
anti-G’s
anti-A’s
anti-M’s
anti-E’s
anti-D’s
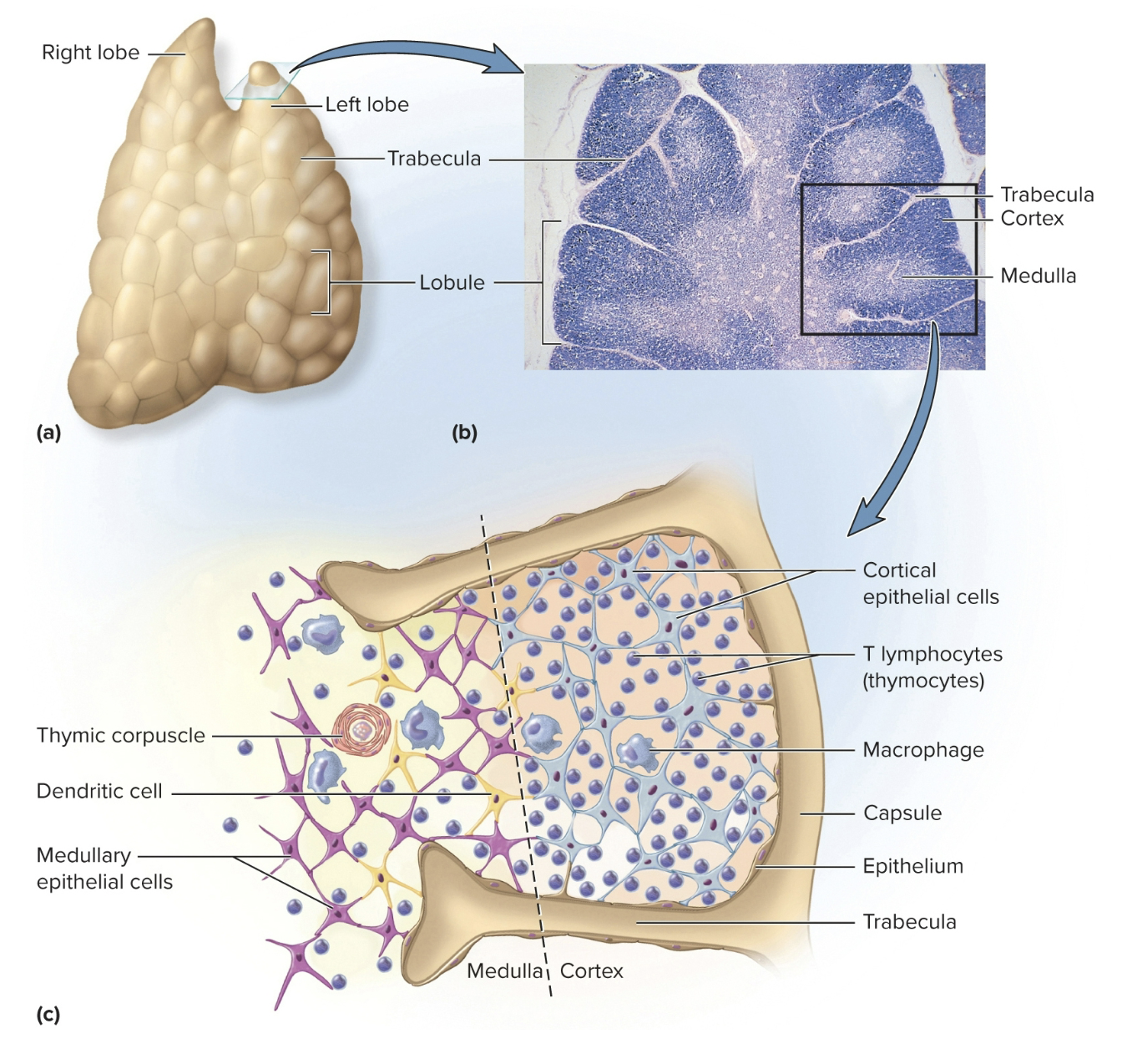
Thymus: Lymphoid Organ
Where t-cells mature in the epitherlial cells: secretes signaling molecules like thymosin, thymopoietin, thymulin, interleukins, and interferon (on exam)
the 2nd lymphoid organ
practically degenerates/gone by age 65 (b/c it’s js a bunch of fatty cells) meaning u stop producing t-cells (immune system decreases)
has a fibrous capsule, gives off trabeculae that divides glands into several lobes
lobes have cortex and medulla populated w/ t cells
Antigen receptor maturation
After maturation, immunocompetent cells travel through the blood stream and lymphatics to “seed” the
lymphatic tissues. From there further division can produce more copies of each clone containing that
unique antigen receptor and those copies can continue to mobilize and travel via the bloodstream to seed
other lymphatic tissues
final cell lines are referred as “immunocompetent” (usually completed by 6 months of age; fetal stage)
B & T lymphocyte activation
1) Encounter and Recognition: antigen receptor binds to matching antigen; due to expression of the pathogen
when lymphocyte binds it is activated
starts dividing repeatedly. some copies form memory cells to enchance memory to recognize future antigen of the pathogen in the future (a repeated invasion)
contribute to evenetrual response to pathogen (varies by type)
B - lymphocytes (B-cells)
responsible for antibody mediated aka humoral (adaptive) immunity
develop in red bone marrow
antibodies that maybe be free or bound to B-cells (also called immunoglobulins)
composed of multiple proteins
has specifice shape and charge distribution for non-self antigens
self-tolerant cells synthesize antigen surface receptors, divide rapidly, produce immunocompetent clones
leave bone marrow and colonize same lymphoid tissues and organs like T-cells
if these cells react to self-antigens (they are go thru clonal deletion)
T lymphocytes (T cells)
cell in adaptive immunity
Three developmental stages:
Birth in bone marrow
Training in the thymus
Deployment = to locations to carry out immune function ( shuffle thru bloodstream to lymphnodes, spleen, etc)
Proper development = immunocompetent: capable of recognizing antigens presented to them
however can fail by reacting to the self-antigen whcih they are then eliminated (ensures that it’s “self-tolerant” meaning it wont attack one’s own tissue)
Responds to two classes of MHC protein:
1) MHC-1 Protein
2) MHC-2 Protein
T-cell activation
Beings when Tc or Th cell binds to a MHC protein displaying an epitope that the T cell is programmed to recognize
Constimulation: additional signaling process required for this activation
MHC and antigen binding, T cells must also bind signaling proteins on surface of APC’s in damged, infected tissues
helps ensure the immune system does not launch an attack in the absense of an enemy
Successful costimulation: triggers clonal selection
activated t cell undergo mitosis
creates identical T cell programmed against the epitope
some cells become effector cells and carry out the attack
other cells become memory cells
MHC-1 Protein
Occur on all nucleated cells, internal peptides are presented on cell surface
ex: a liver cell (b/c it can easily get infected)
RBC do not have MHC-1 bc not nucleated
test question
MHC-2 Protein
occur on APCs, external (phagocytosed, foregin antigens are presented on cell surface
test question
naive lymphocytes
T-cells that migrate to secondary lymphoid tissues and await their antigen
haven’t been tested yet (not exposed to the real *bloodstream etc thing)
Free Type antibodies
these are release from extracellular fluids (humors) and bind to antigens causing: Neutralization, Agglutination, Antibody Opsonization, and Complement Activation
humans have approx. 100 million floating in the body (ask) (we need this b/c a lot of things attack us our entire life)
accomplished by: somatic recombination & tolerated hypermutation (bc we only have 20,000 genes)
somatic recombination: antibody
DNA segments shuffled and form new combinations of base sequences to produce antibody genes
Tolerated hypermutation: antibody
B cells in lymphoid nodules rapidly mutate creating new sequencies
Neutralization
A bound pathogen is often a disabled pathogen that cannot perform its pathogenic function.
(toxin, virus, microbial cell)
Agglutination
Some types especially bind (clump) many pathogens together and these large clusters are easier to remove by the spleen and liver and the macrophages within the tissues.
Antibody Opsonization
When bound, the constant region of the antibody changes configuration
and allows macrophages to more easily recognize, bind, and ingest the antigenic pathogen or toxin (similar to complement opsonization).
Unbound antibodies are invisible to the macrophages.
Antibody Classes: IgG
dominant monomer form, include approx. 80% of the circulating free antibodiesmin the body.
found primarily in plasma and heavy region is excellent at activating complement and opsonizing bacteria. They are the class that is most able to transfer across the placenta into fetal tissue from maternal blood.
dominate in secondary immune response, capable of complement fixation
donating plasma to ppl who don’t have a lot
Antibody Classes: IgE
monomer associated w/ activation of basophils/mast cells and initiating and amplifying inflammation.
IMPORTANT: involved pathologically in allergies and hypersensitivity reactions.
stimulates release of histamine/chemical mediators of inflamamtion & allergies
stimulates eosinophils defensive actions against parasites
Antibody Classes: IgM
forms a pentamer of antibodies (10 antigen binding sites) and are especially good at agglutination (causes things to stick tgt)
This class also activates complement well.
Antibody Classes: IgA
associated with secretions (tears, saliva, vaginal, prostatic, bronchial, and gut secretions, mothers’ milk; coats internal digestive tract of newborn providing protection before the infant’s immune system is fully functional.
good at blocking ability of a pathogen to adhere to epithelia
tougher and more resistant to damage that might occur in these areas where they are secreted (pH fluctuations for example).
Antibody classes: IgD
expressed on the surface of B cell transmembrane antigen receptor - lymphocytes (cells)
an immunoglobulin
B-cell activation
has antibodies attached to their cell surfaces (IgD) and when a matching antigen binds to these membranebound antibodies, the cell is “activated”.
when activated, cell begins to divide and produce two cells of the same clonal cell line
1) Memory Cells
2) Plasma Cells
Also activate “Helper” T-Cells aplifying processes (secretes interleukins)
acts as antigen presenting cells (APCs) simialar to macrophages when they encounter a pathogen.
has thousands of surface receptors for one antigen
antigen binds to several of these receptors, links them tgt, and is taken into the cell b yreceptor-mediated endocytosis
cell processes (digests) the antigen, then displays antigen fragments with MHC-II on its surface
DOESNT KILL CELL triggers clonal selection
B cell mitosis gives rise to clons of identical B cells programmed agains same antigen
mosy differentiaye into plasma celss
plasma cells secrete antibodie sat a rate of 2,000 molecules per second during their life span of 4 to 65 days
- firs exposure to antigen triggers production og IgM antibodies later exposures to the same antigen, IgG
antibodies travel thru body in blood other body fluids
Memory Cells: B cells
These are copies of the same cell line that do not do anything immediately.
may respond more immediately to more of the pathogen and amplify the other effects below after being
activated, or they may wait for another invasion of the same pathogen. They may remain dormant
for more than 20 years providing enhanced “memory” of that pathogen which is the basis of
acquired immunity (below).
secreted from B-cells
Plasma Cells: B cells
These copies begin production of the antibodies that match the encountered
pathogen. Many antibody copies will be formed and secreted to the tissue and enter the
bloodstream for distribution throughout the body, though they will be most concentrated in the
same region where the pathogen was encountered. The free antibodies will attack that pathogen as
above through neutralization, etc.
secreted from B-cells
microbiome
microorganisms that reside on/in the body
can be beneficial/harmful
constantly exposed to potential harmful microrganisms from external/outside environment
protected by the immune system
Lymphoid system: Lacteal
these are in the small intestines and absorbs dietary lipids (vitamins and fat-soluble ADEK) that aren't absorbed in blood capillaries
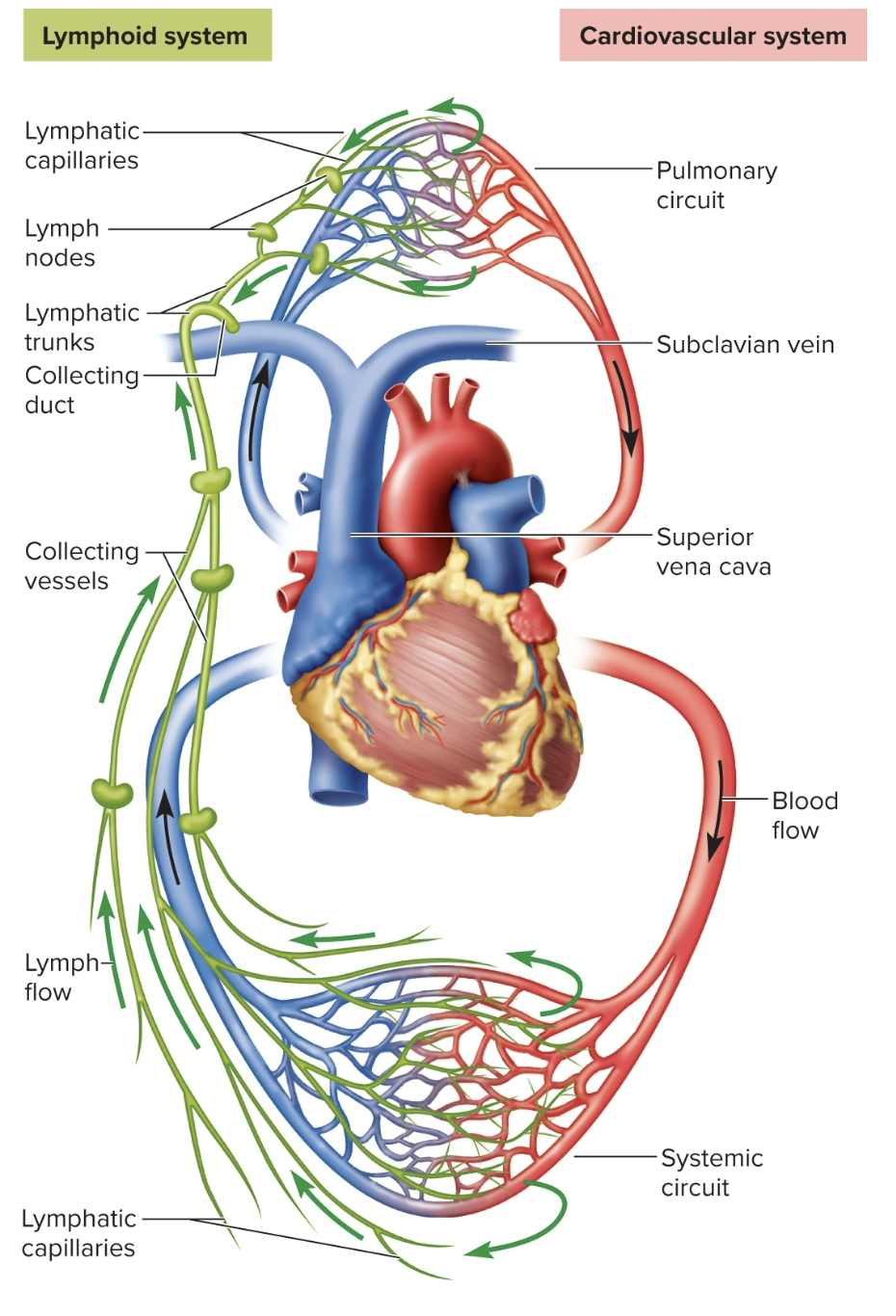
subclavian veins: lymphatic vessels
where the fluid gets funneled from collecting ducts into the subclavian vein
low pressure system
one way flow builds up (gets pushed) fluid to get from vessels to veins
lymphoid nodules (follicles): lymphoid tissue
where lymphocytes and macrophages gather in dense masses
can be temporary/permanent on some tissues
pyres matches: lymphoid nodules in the small intestine
Red Bone Marrow: Lymphoid Organs
soft, loosely organized, high vascular material seperated from osseous tissue by endosteum of bone
involved in hematopoiesis (blood formation) and immunity
blood-forming cells attached to reticular cells/other elements of marrow stroma
secretes colony-stimulating factors that stimulate stem cells to produced formed elements (erythropoietin)
as blood cells mature (B-cells), they push their way thru the reticular/endothelial cells to enter sinu and flow away in blood stream
doesn’t have lymphatic draining
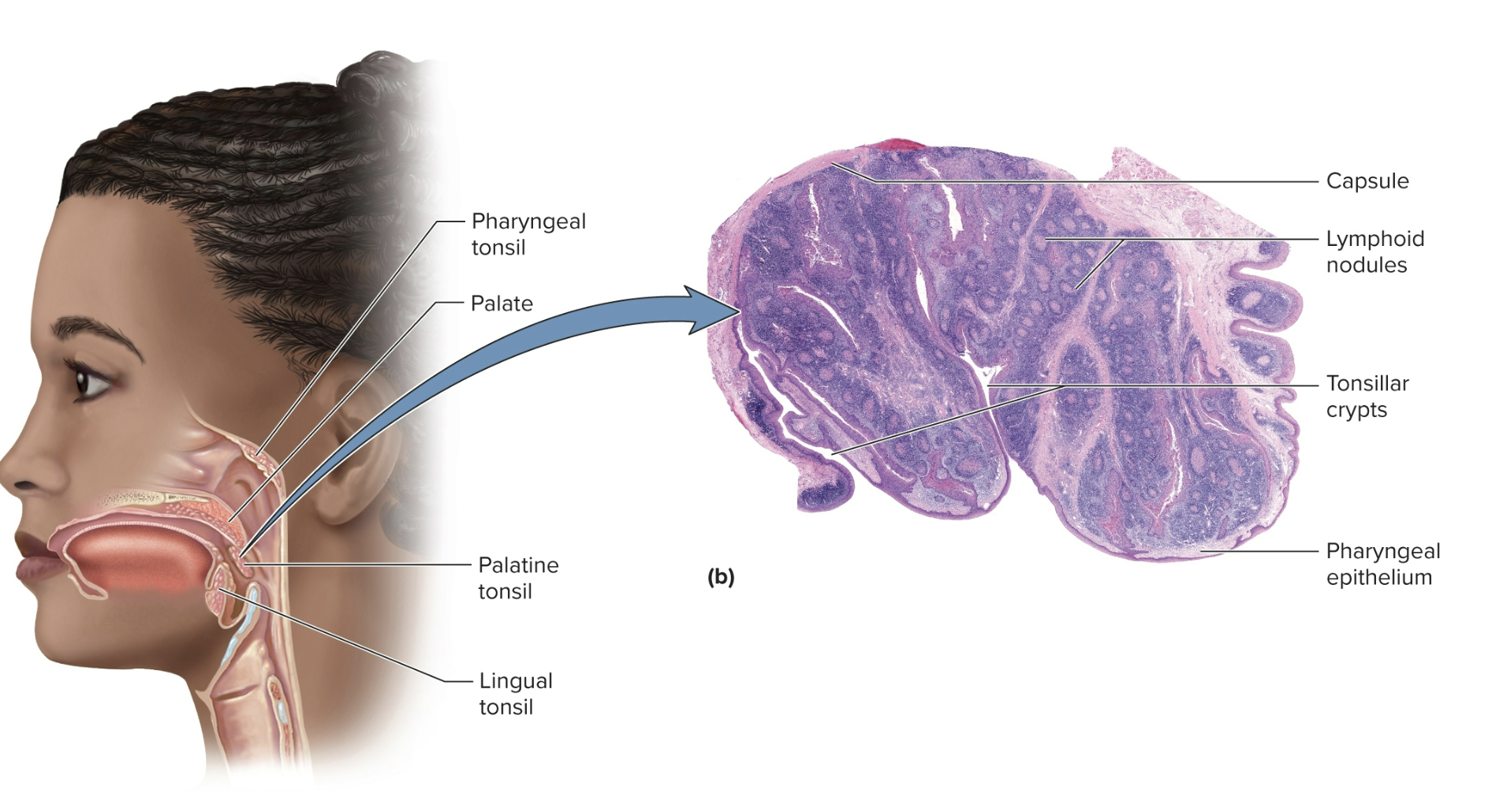
Pharyngeal tonsil (adenoids)
A single tonsil on the wall of the pharynx
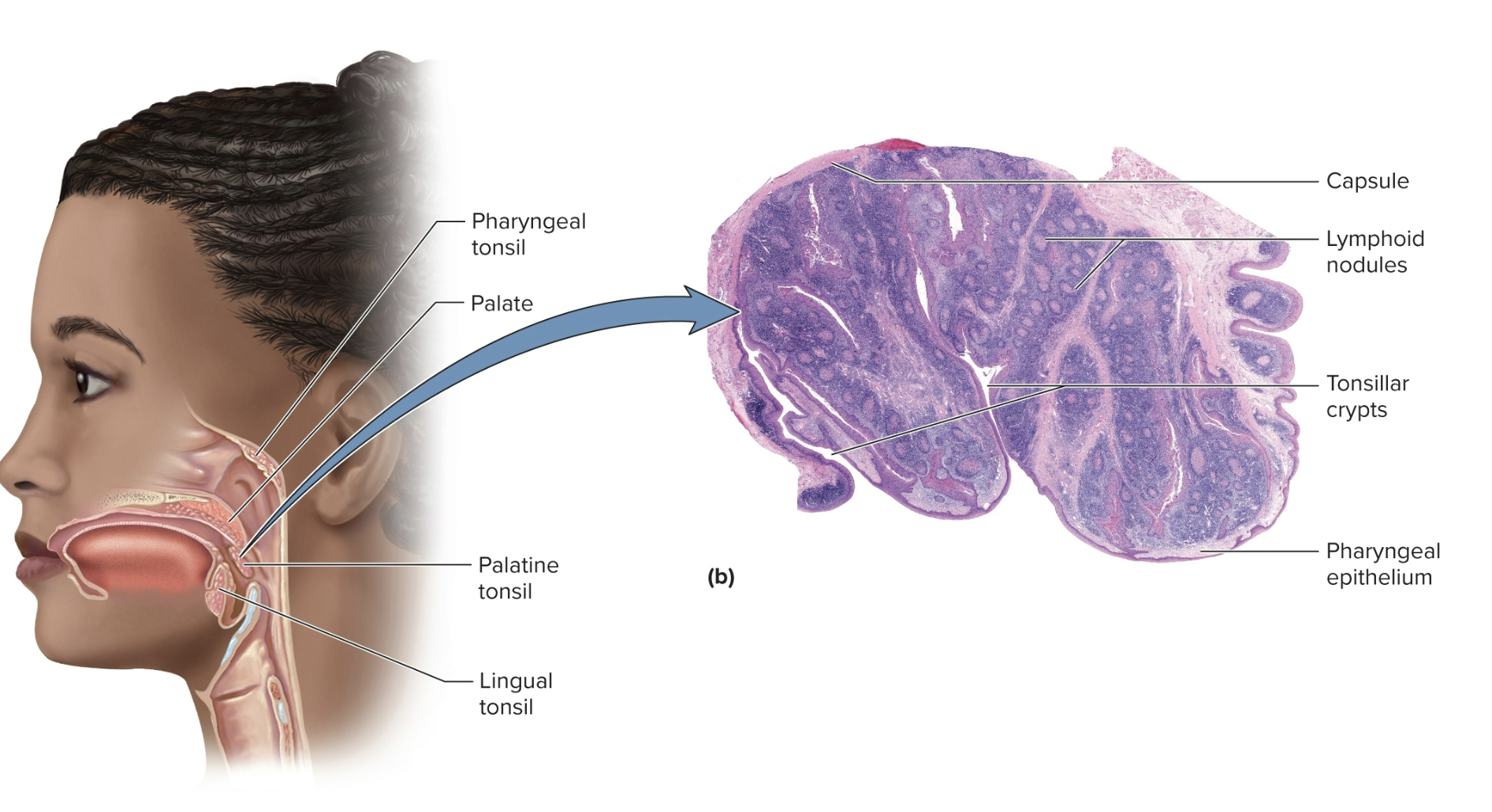
Palatine tonsils
a pair of tonsils at the posterior margin of oral cavity
the standard tonsils you get removed if you have a tonsillectomy/adenoidectomy
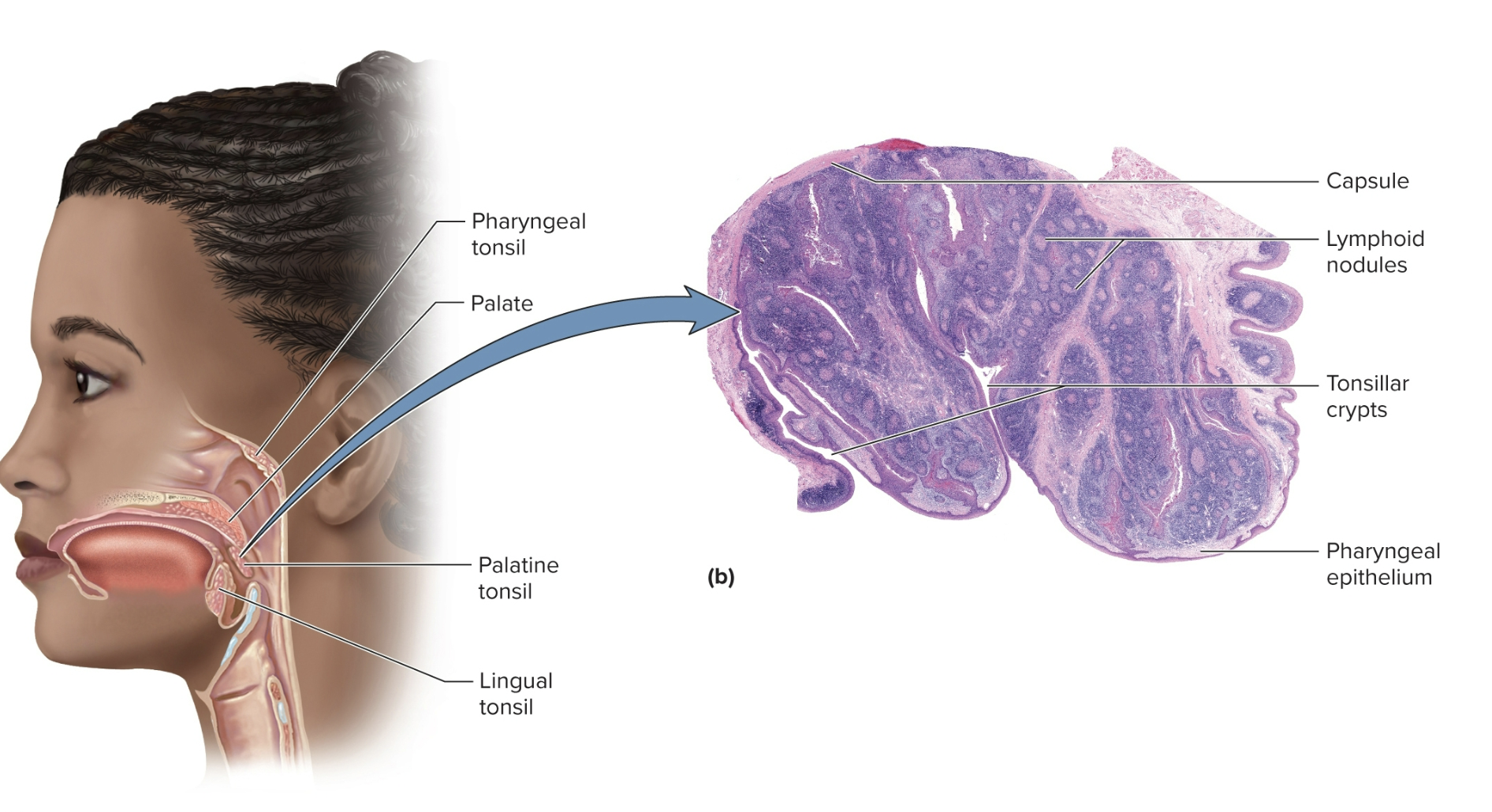
Linguinal tonsils
numerous tonsils concentrated on each side of the base of the tongue
Tonsillitis
acute inflammation of palatine tonsils