BIPN 152: material after midterm 3 (part of Final Exam material)
1/48
Earn XP
Description and Tags
covers LE 14-17, DI week 9-10 slides (if posted on Canvas)
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
(mostly a repeat of last card of midterm 3 set)
use syndromic ASD to study cellular mechanisms underlying ASD b/c we know the genetic causes
one of the syndromic forms of ASD and/or ID: fragile X syndrome (FXS)
fragile X syndrome (FXS) is the most common __ cause of ID and ASD
def. FXS
is caused by a __ in the gene __ that encodes for (1), SO have __ of __ expression ← is what causes Fragile X syndrome
what are the 3 states depending on the amount of the specific trinucleotide repeats?
symptoms (5)
draw out how it looks like
fragile X syndrome is the most common hereditary cause of ID and ASD
a trinucleotide repeat expansion disease of CGG
is caused by gene mutation of gene FMR1 that encodes for the Fragile X Messenger ribonuclear protein (FMRP), SO have lack of FMRP expression
^ the lack of FMRP protein expression is what causes Fragile X syndrome
typical (→ get normal FMRP expression), premutation (→ have some defects), mutation (→ lack of FMRP expression)
symptoms:
ASD
ID
enlarged testicle
flat feet
seizures (in ~10% of patients)
use syndromic ASD to study cellular mechanisms underlying ASD b/c we know the genetic causes
one of the syndromic forms of ASD and/or ID: fragile X syndrome (FXS)
FMRP is a __ binding protein that NORMALLY does what (end w/ protein synthesis)?
what happens if FMRP is absent due to FXS (← end w/ protein synthesis)?
what are some of these FMRP-regulated proteins (aka give some general categories & name 1 specific ex.)
t/f: FMRP helps regulate translation & mRNA control, and indirectly helps regulate transcription
__
summary of above:
FXS leads to the loss of __ control of specific protein translation, which is especially important in __ b/c …
FMRP is a mRNA binding protein that NORMALLY regulates translation (aka protein synthesis) specifically by causing ribosome stalling to decrease translation → to get NORMAL levels of specific FMRP-regulated proteins
SO in FXS, a full mutation (of >200 CGG repeat expansion) on the FMR1 gene → FMR1 gene silencing → decreased translation SO very little FMR1 mRNA → little to no FMRP protein is expressed/made
→ loss of ribosome stalling (that normally decreases translation) → increase translation (can think of as over-translation) → overproduction of specific FMRP-regulated proteins
^^ some FMRP-regulated proteins are proteins that regulate the cytoskeleton (like MT-ass. and actin-ass. proteins), synapse function, ion channels, metabolism, and mRNA stability
ex: MAP1b ← MT-associated protein that was made from FMRP-regulated translation
_
true (^ FMRP helps regulate translation & mRNA control, and indirectly helps regulate transcription)
_______
summary of above:
FXS leads to the loss of localized control of specific (FMRP-regulated) protein translation, which is especially important in neurons b/c neurons are compartmentalized cells, meaning that each part of the neuron has different functions/organizations (i.e. dendrites vs. soma vs. axon)
(where “abnormal mRNA” is due to the presence of pre-mutations or full mutations on the FMR1 gene)
use syndromic ASD to study cellular mechanisms underlying ASD b/c we know the genetic causes
one of the syndromic forms of ASD and/or ID: fragile X syndrome (FXS)
FMRP locally regulates protein synthesis in (2)
state the compartmentalized protein synthesis functions in each
FMRP locally regulates translation in (2)
describe (← 1 each, for 1 of them explain why)
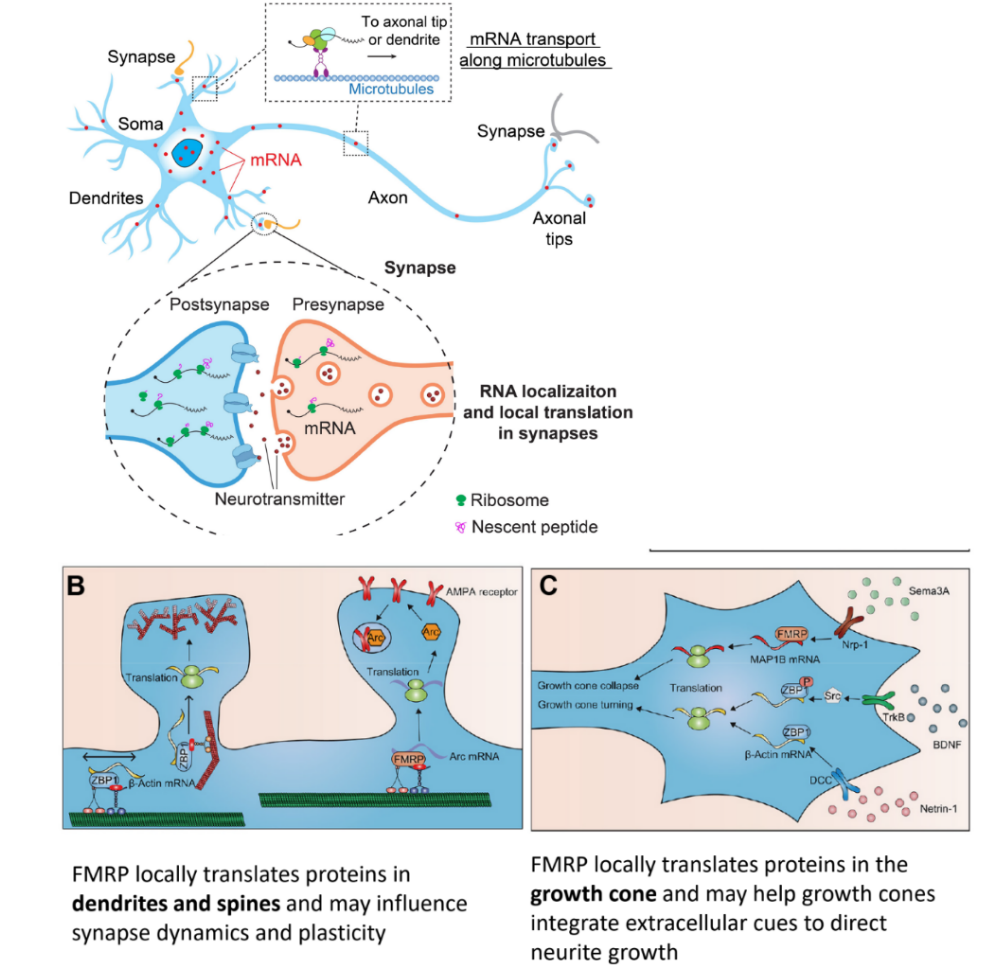
FMRP locally regulates protein synthesis in axons & dendrites
(FMRP-regulated) mRNA transport occurs along microtubules along the axon (moving in either direction: towards dendrite or towards terminal)
(FMRP-regulated) RNA localization & local translation occurs in synapses b/w pre- axon terminals & post- dendrites
__
FMRP locally regulates translation in dendritic spines & growth cones
(FMRP-regulated) local translation in dendritic spines may influence synaptic plasticity (i.e. LTP and LTD)
(FMRP-regulated) local translation in growth cones allows for faster detection of extra- cues & faster neurite growth (of axons & dendrites)
b/c local translation in growth cones means that growth cones contain mRNA, ribosomes, and FMRP/translation regulators, SO translation of proteins occurring in the soma is close, not far away
overall:
transport & local anchoring of specific mRNAs
involves MTs and actin filaments ← axons
is regulated by FMRP in response to synaptic activity ← dendrites
influences spine shape & synaptic plasticity (like LTP) ← dendritic spines & growth cones
for FXS underlying mechanisms
t/f: mRNAs are translated in and around (localized translation) dendritic spines & growth cones
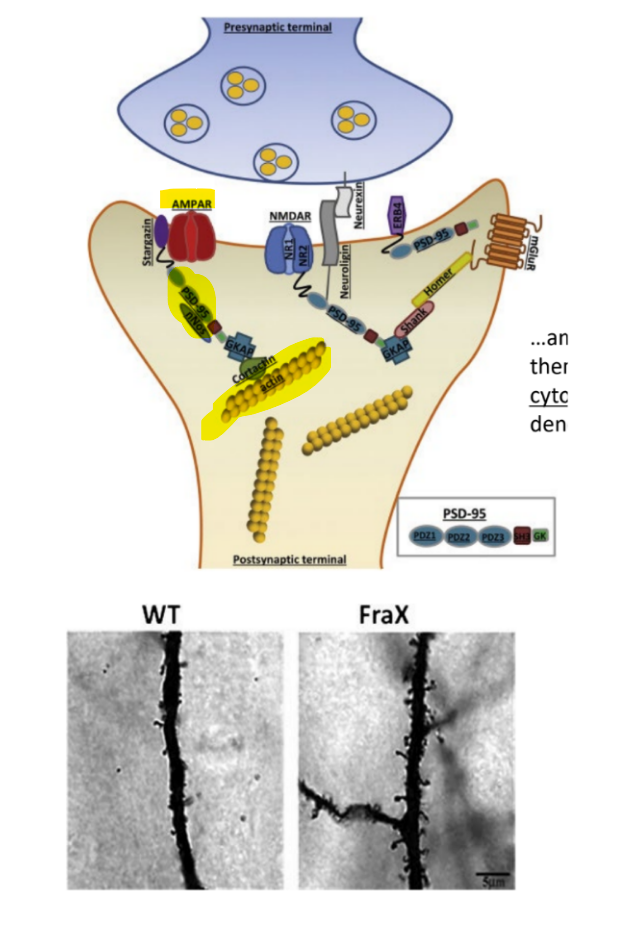
def. PSD-95 (incl. its 2 functions)
describe (~1/2)
_
SO, in wildtype vs. FXS mice, which is associated w/ increased density of dendritic spines & elongated shape of dendrites?
what is bad about this?
_
t/f: cytoskeleton changes that lead to growth cone shape, direction, and turning & neurite growth are the underlying mechanisms of neuronal network formation
true
PSD-95 — a scaffolding protein that regulates AMPARs (which are glutamate Rs) at post- synapses/junctions AND connect glutamate Rs to actin cytoskeleton
there is more PSD-95 translation in dendritic spines of FMR1 knockout (KO) neurons (← as seen in FXS) compared to neurons that contain FMR1 genes
in these FMR1 knockout neurons, there is too much translation of PSD-95 mRNA
_
SO FXS mice are associated w/ increased density of dendritic spines & elongated shape of dendrites
b/c there is loss of FMRP-controlled/regulated translation in dendritic spines & growth cones that causes for abnormal protein synthesis → faster neurite growth (of axons & dendrites)
however, it is TOO MUCH loss of FMRP-controlled translation → which causes HIGH density of dendritic spines & TOO MANY synapses → which causes the brain to NOT function properly (problems in memory, learning, and LTP) → that will cause changes in behavior
__
true
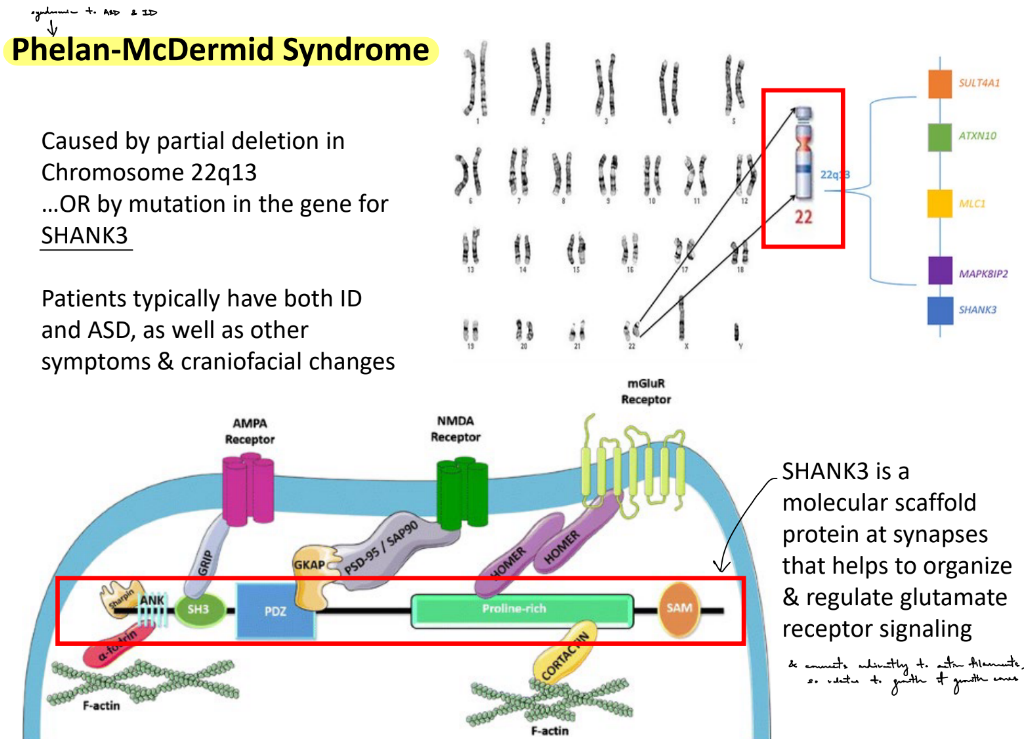
def. Phelan-McDermid syndrome
is syndromic to (2)
def. SHANK3
_______
mechanisms of ASD can involve either __ or __activation of normal development biochemical cascades
the main idea is that ASD mechanisms are due to __
Phelan-McDermid syndrome — a genetic disorder caused by partial deletion in Chr 22q13 OR caused by mutation in the gene for the SHANK3 protein
syndromic to ID (intellectual disabilities) & ASD (autism spectrum disorder)
SHANK3 — a scaffolding protein at synapses to help regulate glutamate R signaling
___________
mechanisms of ASD can involve either under or overactivation of normal development biochemical cascades (← think how ASD individuals can range from having extreme ID to developing extraordinary talents)
the main idea is that ASD mechanisms are due to imbalance
overall:
t/f: FXS & Phelan-McDermid syndrome are monogenic genetic disorders (FMR1 gene + SHANK3 gene), while ID and ASD are due to a combination of genetics & environment
_
t/f: proper & tightly-regulated responses to external cues at growth cones & dendritic spines are necessary to form neuronal network & regulate synaptic plasticity (i.e. LTP and LTD) and synaptic activity
t/f: SO when it is dysregulated (like in FXS), these small changes can lead to large changes in the brain & behavior
__
overall, ASD phenotype depends on what 4 factors?
true for all
__
overall, ASD phenotype depends on:
genes
CNVs
environment
epigenetics
def. neuromodulation
review:
what mediates fast vs. slow neurotransmission
which type of neurotransmission can act spatially limited vs. spatially distant
_
similarities & diff b/w the general naming of fast-acting NTs and/or slow-acting neuromodulators
__
3 things that determine if something is a NT
neuromodulation — changing the response of fast-acting NTs
_
review:
ACh, glutamate, GABA, glycine med. fast neurotransmission
neuromodulators med. slow neurotransmission
…
fast is spatially limited (specific/restricted to 1 synapse)
slow is spatially distant (has paracrine effects
b/c are released into the bloodstream & affect many synapses)
__
fast-acting NTs & slow-acting neuromodulators (specifically monoamines: serotonin, NE, EPI, DA) can be referred to as NTs b/c their release is vesicular & synaptic (aka act locally & are usually the main ligand)
BUT other neuromodulators (like purines, neuropeptides, enkephalins) can be called NTs but are usually called neuromodulators b/c they aren’t the main ligand, aren’t always released from vesicles, and have paracrine or endocrine effects
__
is a NT if:
exists in terminals
released when there’s depolarization
acts on target cells via ligand-activated Rs
all vesicularly-released NTs are packaged into vesicles via (1) ← explain how using DA as the NT
name & describe the 3 major DA systems/pathways
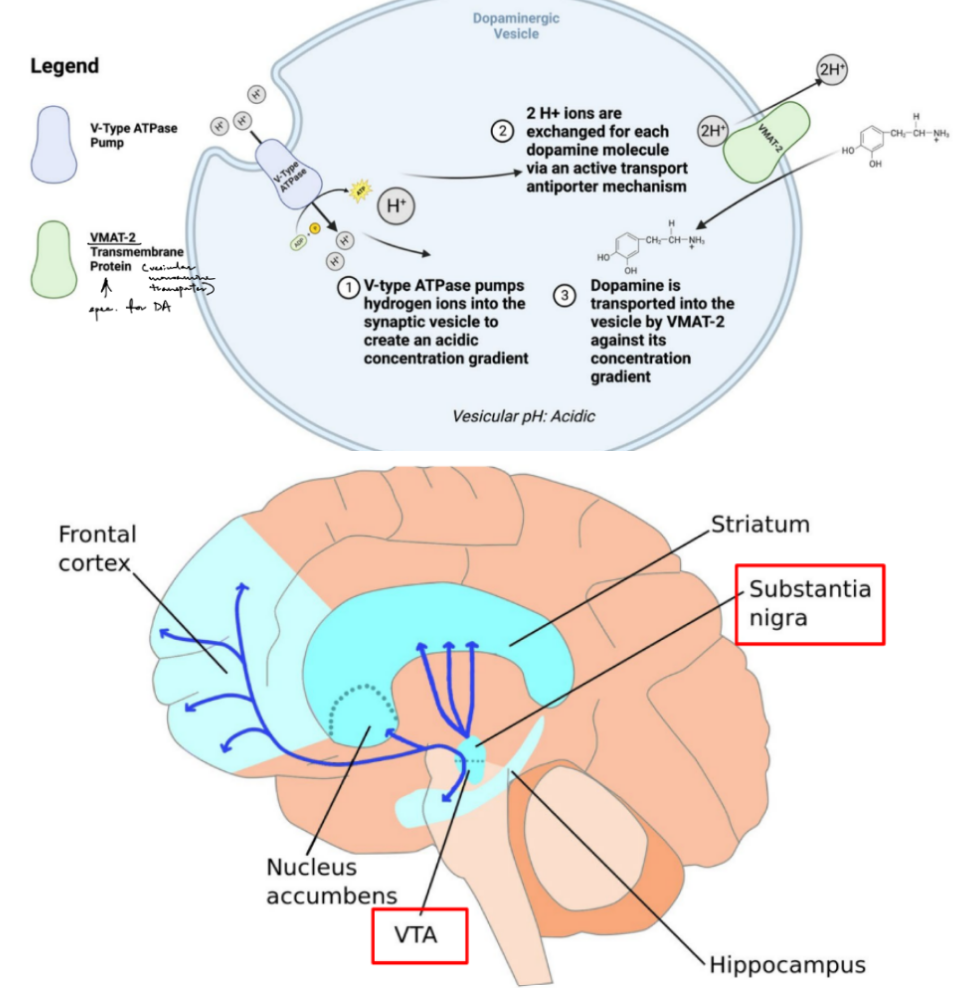
all vesicularly-released NTs are packaged into vesicles via proton-driven exchangers, works by:
Vesicular/V-type H⁺-ATPase pumps protons into vesicle
This creates a proton/acidic electrochemical gradient
That gradient powers vesicular neurotransmitter transporters, like VMAT-2 antiporter, to pump 2 H+/protons out & pump 1 DA into the vesicle (against its concentration gradient)
__
for vesicularly-released NTs, specific to monoamines:
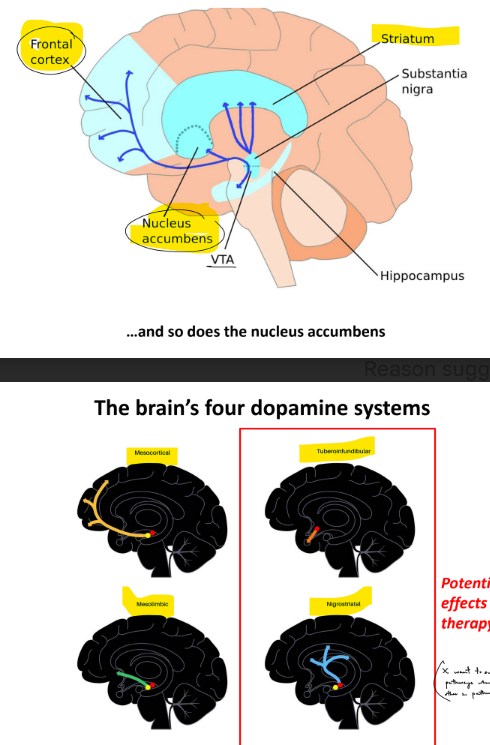
3 major DA systems/pathways:
nigrostriatal pathway — DA from SN (substantia nigra) → striatum
mesocortical pathway — DA from VTA (ventral tegmental area) → cortical areas
mesolimbic pathway — DA from VTA (ventral tegmental area) → nucleus accumbens
for vesicularly-released NTs, specific to monoamines
function of NE (norepinephrine) in CNS vs. PNS
all noradrenergic transmission in the brain came from the __ __
__
epinephrine can be considered both a (2)
EPI is mainly produced by the __ __
__
state order of catecholamines w/ enzymes
__
serotonin is made in 2 steps from __
serotonin is packaged into vesicles by (1), degraded by (1), and taken up by (1, which is the target of __)
name of serotonin Rs & its types
most serotonin transmission in the brain came from the __ __
NE function in CNS:
sleep and arousal, attention, feeding, emotional state
NE function in PNS:
sympathetic function (fight-or-flight) of autonomic/involuntary systems
all noradrenergic/NE transmission in the brain came from/started at the locus coeruleus
__
epinephrine can be considered both a NT & hormone (b/c helps neuronal communication & acts in peripheral systems/PNS)
EPI is mainly produced by the adrenal glands
_______
tyrosine —(tyrosine hydroxylase/TH)→ L-DOPA —(DOPA decarboxylase/DDC)→ DA —(DA beta-hydroxylase/DBH)→ NE —(phenylethanolamine N-methyltransferase)→ EPI
______
serotonin is made in 2 steps from tryptophan
serotonin is packaged into vesicles by VMAT degraded by MAO, and taken up by SERTs (serotonin transporters), which is the target of SSRIs
serotonin Rs are 5-HT Rs: 5HT1, 5HT2, 5HT3
most serotonin transmission in the brain came from the raphe nucleus
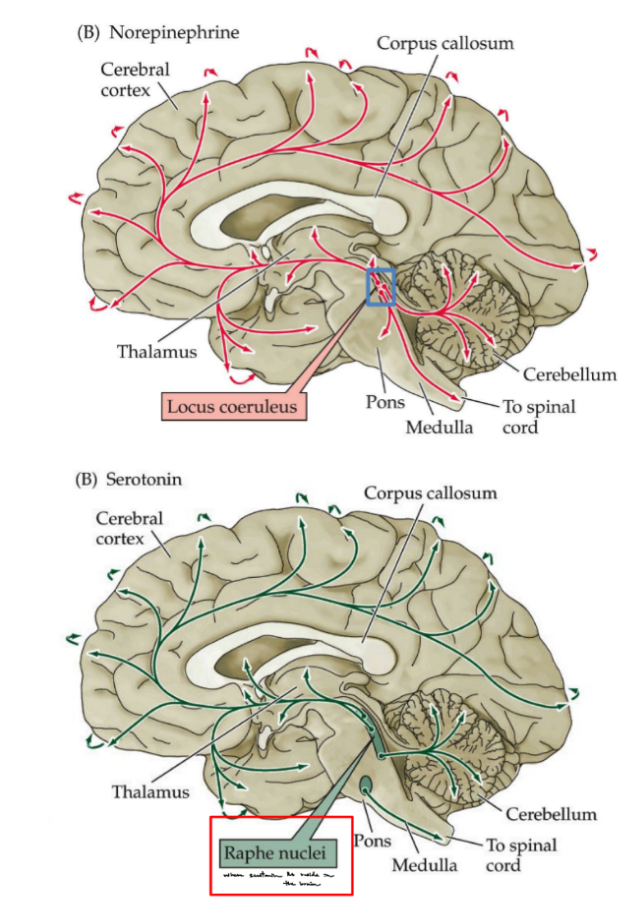
t/f: tiny clusters of neurons/nuclei have big influence
__
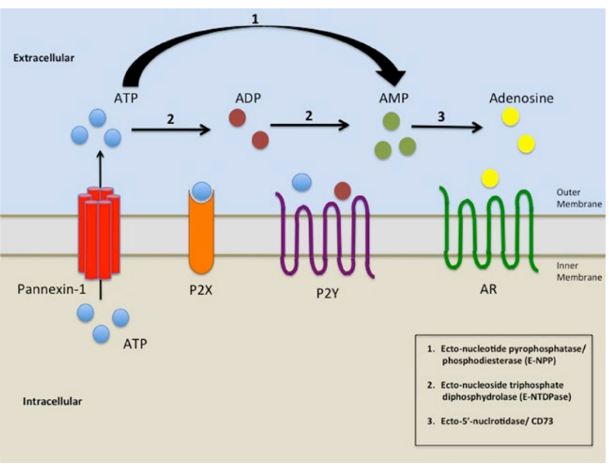
for NOT vesicularly-released NTs (aka neuromodulators), specific to purines: ATP and adenosine
t/f: all synaptic vesicles have ATP
ATP is released via (1)
_
adenosine is released from (2), not from (1)
__
^^ purines activate specific Rs called __ __, where ATP’s Rs are (2) & adenosine’s Rs are (1)
true (all synaptic vesicles have ATP)
ATP is released via pannexin channels
_
adenosine is released from neurons & glia, not from vesicles
__
^^ purines activate specific Rs called purinergic Rs, where:
ATP’s Rs are channels (P2X) & GPCRs (P2Y)
adenosine’s Rs are adenosine Rs / ARs
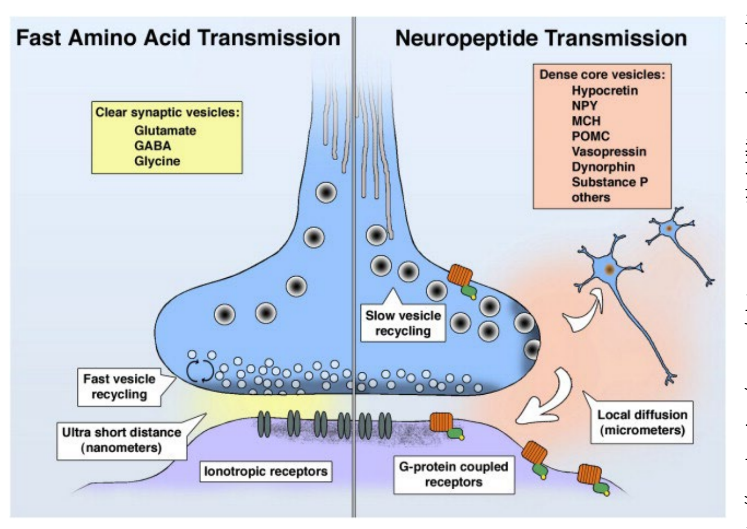
for NOT vesicularly-released NTs (aka neuromodulators), specific to neuropeptides
like all peptides/proteins, neuropeptides are encoded by __ and synthesized by __
how are neuropeptides synthesized (← specific term, def. it, describe process)?
most neuropeptides act on what type of Rs?
are degraded by (1)
_
t/f: neuropeptides have many functions, like metabolism, appetite, analgesia, mood, hormone regulation, brain/gut, hypothalamic-releasing hormones, etc.
__
neuropeptides work together with small molecule NTs (like amino acids: glutamate, GABA, glycine) but on different time & spatial scales
explain
like all peptides/proteins, neuropeptides are encoded by mRNA and synthesized by ribosomes
…synthesized via proteolytic processing — cleave inactive proteins into active proteins using enzymes…
pre-propeptides (have a signal sequence that allows them to cross into the ER)
→ peptidases cut them into propeptides
→ propeptide is packaged into vesicles & processed into individual ACTIVE peptides
__
most neuropeptides act on metabo- Rs
neuropeptides are degraded by extra- peptidases
_
true
neuropeptides have many functions, like metabolism, appetite, analgesia, mood, hormone regulation, brain/gut, hypothalamic-releasing hormones, etc.
__
neuropeptides work together with small molecule NTs (like amino acids: glutamate, GABA, glycine) but on different time & spatial scales
^ fast-acting NTs have fast vesicle recycling & work short distances (i.e. in synapse)
^ neuropeptides have slow vesicle recycling & local diffusion (released in the brain’s extra- space)
for NOT vesicularly-released NTs (aka neuromodulators), specific to neuropeptides
general location of human hypothalamus
__
one of the functions of neuropeptides is regulating appetite (hunger, cravings, and satiety) & metabolism
give 1 ex. of such neuropeptides, and what general type of molecule is it?
__________________________________________________________________
name some unconventional NTs (2)
deep in the center of the brain
__
one of the functions of neuropeptides is regulating appetite (hunger, cravings, and satiety) & metabolism
ex: Ozempic, which is a GLP-1 receptor agonists
__________________________________________________________________
unconventional NTs:
endocannabinoids
gasotransmitters
for unconventional NTs: endocannabinoids
def. endocannabinoids
synthesized from __ __
signal terminated how?
cannabinoid receptors are __ (& state 2 endocannabinoid Rs)
are found… & are activated by …
currently, we are developing endocannabinoid __, __, and __ __ as potential therapeutic agents
endocannabinoids — endogenous ligands at cannabinoid Rs
synthesized from fatty acids
signal terminated when uptake into post- cell & hydrolyzed by FAAH (fatty acid amide hydrolase)
cannabinoid receptors are metabotropic, like CB1 and CB2
these Rs are found throughout the body & are activated by natural compounds in cannabis plants
currently, we are developing endocannabinoid agonists, antagonists, and FAAH blockers as potential therapeutic agents
(^ “FAAH blockers” b/c don’t want these NTs to be terminated / want continuous effects)
for unconventional NTs: gasotransmitters
def. gasotransmitters
state 3 examples
why are they unconventional / its unusual activity (4)
for the gasotransmitter: NO
made by (1), which is stimulated by (1)
2 mechanisms of signaling
how is signal terminated?
_______
also, in general, unconventional NTs can act as __ signals that move from … to … to …
gasotransmitters — endogenously-produced/produced in body gaseous signaling molecules
nitric oxide (NO), carbon monoxide (CO), hydrogen sulfide (H2S)
unusual activity:
not stored in vesicles
diffuse freely across membranes
and also act locally by diffusion, not by synaptic release
made on demand
for the gasotransmitter: NO
made by NO synthase, which is stimulated by calcium
2 mechanisms of signaling:
activating guanylyl cyclase
nitrosylation (adding NO) of specific proteins
don’t need signal termination b/c decays spontaneously by reacting w/ O2
_____________________________________
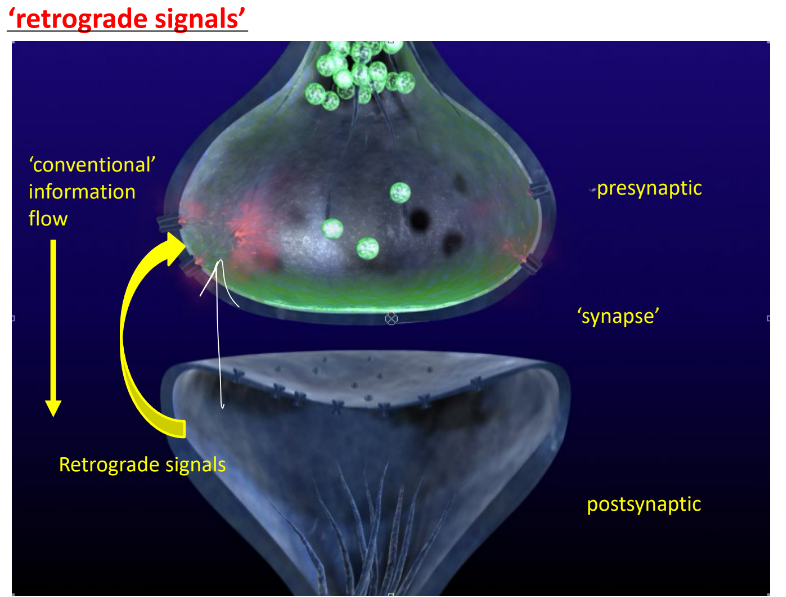
also, in general, unconventional NTs can act as retrograde signals
by diffusing backwards from post- → synapse → pre- cell
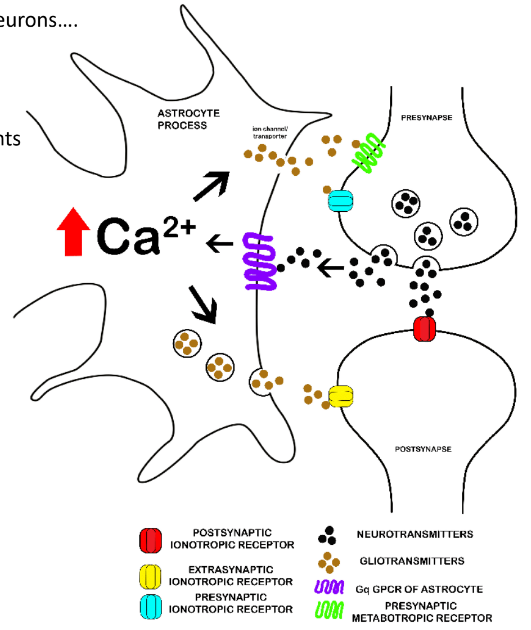
tripartite synapse consists of (3)
describe (2)
tripartite synapse: pre-, post-, astrocytes
(neuro)transmitters & (neuro)modulators from pre- cells can act on Rs on astrocytes & post- cells
(neuro)transmitters & (neuro)modulators are released from astrocytes & pre- terminals
for neuromodulators: steroid hormones
give ex. of steroid hormones that can act as neuromodulators (4)
where does each come from
what is the mech. of steroids?
_
def. neurosteroids
ex. of steroid hormones as neuromodulators:
estrogen (from ovaries)
progesterone (from ovaries)
testosterone (from testes)
cortisol (from adrenal cortex)
mech: Rs in the cytoplasm will become TFs once the steroid ligands bind to it
__
neurosteroids — type of steroids made in the mitochondria & can act in many places in the CNS and periphery/PNS
review: many neuromodulators function via __ Rs
state steps of GPCR signal transduction (5)
name & describe the diff types of G-protein pathways (3)
and these steps can be generalized as …
what are the 2 most common 2nd messengers?
which 2nd messengers are made or inhibited in each G-protein pathway?
what “steps”/stages does amplification occur vs not occur?
review: many neuromodulators function via metabotropic Rs (aka GPCRs), which affect the function of ion channels, NT Rs, NT release, etc.
__
the R binds to the G-protein (that is heterotrimeric w/ alpha, beta, gamma subunits that are bound to GDP) → causes GDP to leave & GTP to bind to alpha subunit
alpha subunit dissociates from beta-gamma subunits
alpha subunit binds & activates an effector protein, which is usually adenylyl cyclase or phospholipase C
GTP is hydrolyzed to GDP on the alpha subunit, while GAP (GTPase activating protein) is speeding up the rate of this hydrolysis
alpha subunit dissociates from effector protein & binds to beta-gamma → to become inactive state
__
Gs (w/ Gs protein): activates adenylyl cyclase → cAMP → PKA → (target effect)
Gi (w/ Gi protein): inhibits adenylyl cyclase → cAMP → PKA → (target effect)
Gq (w/ Gq protein): activates phospholipase C → DAG & IP3, where DAG → PKC → (target) and IP3 → Ca2+ release → (target)
^^
NT → R → G-protein → effector protein → 2nd messenger → effector protein → (target)
__
most common 2nd messengers: cAMP & Ca2+
Gs - makes cAMP
Gi - inhibits cAMP
Gq - makes IP3, DAG, and Ca2+
__
amplification occurs at all stages EXCEPT from 2nd messenger → effector
G-protein → effector protein → 2nd messenger
effector protein → (target)
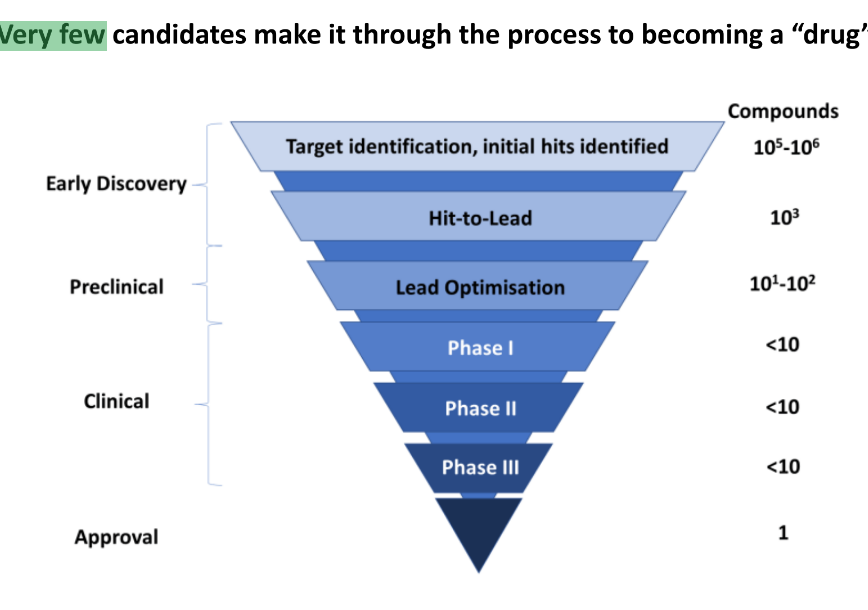
what are the 5 drug discovery & development phases/pipeline
describe the first 3
discovery & development
get information about PK (pharmacokinetics) ← how drugs are absorbed, metabolized, and excreted (aka how it works w/in the body)
& PD (pharmacodynamics) ← dosage, benefits, side effects, interaction with other drugs, etc. (aka usage & effects)
preclinical research
before testing drug in people, need to find potential toxicity via in vitro & in vivo (in animals)
clinical research
studies/trials done with people, including deciding who, how many, time, etc. of how the study will be designed
there are 3 phases of clinical trials
(#695 video)
FDA review
FDA post-market safety monitoring
(aka FDA review the safety of drugs after being introduced to the market)
why does the brain have Rs for opiates?
3 things opiates do
__
def. nociception
describe how pain is good vs. how pain is bad (3 each)
diff. b/w acute & chronic pain in terms of cause, duration, treatment
b/c endogenous opiates are part of the natural system to reduce pain (aka analgesia), where endogenous opiates are neuropeptides & exogenous opiates are small molecule drugs (not small molecule NTs)
__
opiates reduce pain, lessen anxiety, create euphoria
____
nociception — perception of noxious/painful stimuli
pain is good b/c:
pain evolved to help organisms sense danger/threat
pain is normal
pain occurs when body’s alarm system alerts the brain to actual or potential tissue damage
pain is bad b/c:
chronic pain might indicate disease, where it’s pain that lasts longer than normal time it takes to heal
chronic pain might be caused from psychological states, has no biological purpose, and no end-point
acute & chronic pain are big problems in the US
__
acute pain:
known cause
short duration, where know the expected time of how long pain lasts
can solve the underlying cause & interrupt nociceptive signals
chronic pain:
usually unknown cause
lasts after healing, of at least 3 months
can’t resolve underlying cause and pain, so treatment is pain control with a multidisciplinary approach
t/f: it is ALWAYS the brain that decides whether or not something is painful
t/f: the severity of pain does not necessarily relate to the severity of tissue damage
t/f: some injuries that result from slowly evolving body changes (i.e. age-related arthritis) don’t produce pain
t/f: pain is personal & subjective
t/f: loss of consciousness ALWAYS results in loss of pain perception (i.e. anesthesia, coma)
__
for the hypothesis demonstrated by the ex: people who had major surgery while hypnotized & no medical anesthesia don’t feel pain
what is the conclusion?
true for all
__
conclude that pain relies on BOTH consciousness & context
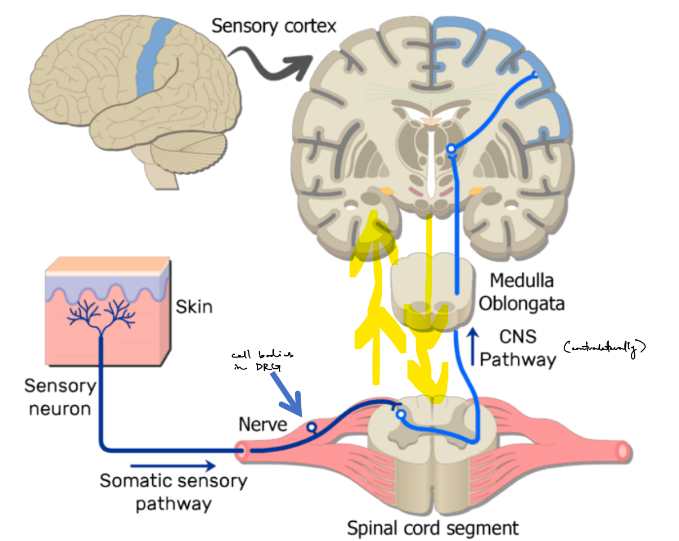
pain is perceived in the __ __ on the __ side (meaning? aka what is the path of pain perception)
pain perception is usually modulated (to either be __ or __) by the __, where there is (1)
what are the 5 general steps of the brain circuitry of pain perception?
pain is a combination of what 3 things?
pain is perceived in the sensory cortex on the contralateral side
meaning that pain goes from the skin → (somatic) sensory nerve → DRG → SC, where crossing over happens → brain, specifically sensory cortex
pain perception is usually modulated (to either be enhanced or reduced) by the CNS, where there is bidirectional communication b/w the brain & spinal cord (← aka b/w parts of the CNS)
__
detection: nociceptors in the body detect potentially damaging stimuli
transmission: pain signals travel to the SC
ascending pathways: signals go up to the brain via 2 major pathways: spinothalamic tract (cross over in SC, always for pain) & dorsal column tract (cross over in brain)
brain processing: brain processes pain signals
perception: brain integrates pain signals to produce the conscious experience of pain
__
pain is a combination of:
sensory (discriminative: where, how intense, quality)
affective (motivational: distress, unpleasantness)
cognitive (evaluative: context, meaning, expectations)
nociceptors are a type of sensory neuron with __ nerve endings that respond to __ stimuli, like (4 types w/ ex.)
t/f: nociceptors are a heterogenous group of neurons (no single anatomic, biochemical, etc. criteria can identify a nociceptor)
what 2 things deter. if pain perception is slow or fast?
_
for the 4 types of specialized nerve endings in skin, name & what each senses (← is review)
nociceptors are a type of sensory neuron with free nerve endings that respond to intense stimuli, like
mechanical (strong pressure, sharp objects)
thermal (burning heat, painful cold)
chemical (pH extremes, environmental irritants)
polymodal aka multiple things
_
true (are heterogenous)
_
deter. if pain perception is slow or fast are:
if axons are myelinated or unmyelinated
axon diameter
(i.e. small diameter has slow flow/transmission of signals down the axon, so will perceive throbbing, long-lasting pain)
__
Meissner’s corpuscle — senses touch
Pacinian corpuscle — sense pressure
thermoreceptor — senses temp (heat or cold)
nociceptor (are free nerve endings) — senses pain
for pain
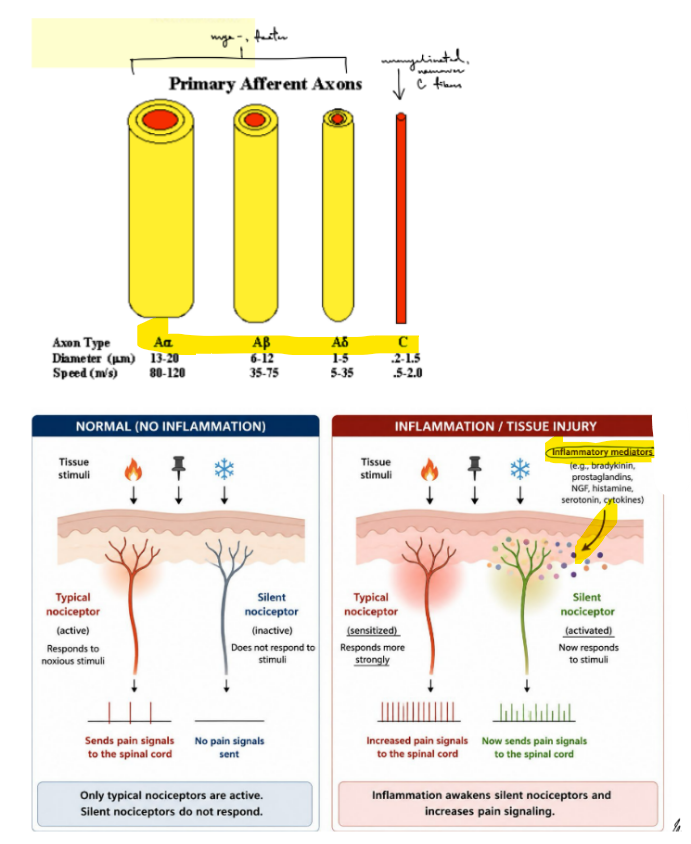
PERIPHERAL nerves have different classes of __ that carry different info at different __
name the 2 types & names of axons types in each
__
what type of info is carried by A-delta & C nerve fibers
__
nociceptors have a high threshold for activation (← relate to GPs and APs)
do A-delta or C fibers have better localized sensation? why?
PERIPHERAL nerves have different classes of axons that carry different info at different speeds
primary afferent axons that are mye- and faster axons
A-alpha, A-beta, A-delta fibers (← where A-alpha is largest diameter to smallest diameter of A-delta fibers)
unmye-, slower axons (← slower b/c have narrower axon diameter)
C fibers
__
A-delta fibers carry mechanical & thermal pain
C fibers carry mechanical, thermal and chemical pain (← what most nociceptors sense)
__
nociceptors have a high threshold for activation, so a very intense stimuli can increase the amplitudes of GPs, which can increase the frequency of APs
_
A-delta fibers have better localized sensation (b/c A-delta fibers are myelinated) vs. C fibers w/ poor localized sensation (b/c C fibers are unmye-)
for pain
def. silent nociceptors / silent nociception
^ where __ ___ of inflammation can increase pain perception
__
cellular/tissue damage will cause the release of diffusible __ of inflammation (& name 4 ex.)
t/f:chemical mediators of inflammation act synergistically to increase the transmission of nociceptive impulses along sensory neuron axons
____________
whereas the cellular mediators of inflammation are __ __ that work by (1)
silent nociceptors / silent nociception — pain signals are only activated +increase when the presence of inflammation activates silent nociceptors
^ where chemical mediators of inflammation can increase pain perception
__
cellular/tissue damage will cause the release of diffusible mediators of inflammation
histamine
bradykinin
prostaglandins
cytokines
true
_________________
whereas the cellular mediators of inflammation are immune cells that work by secreting signals & activate Rs in the nociceptive nerve terminal
for pain
name the 4 classes of analgesics/pain relievers (w/ ex. of 3 of them)
describe how 2 of the examples work
t/f: but we are still learning more about acetaminophen
opioids
steroidal anti-inflammatory (cortisone)
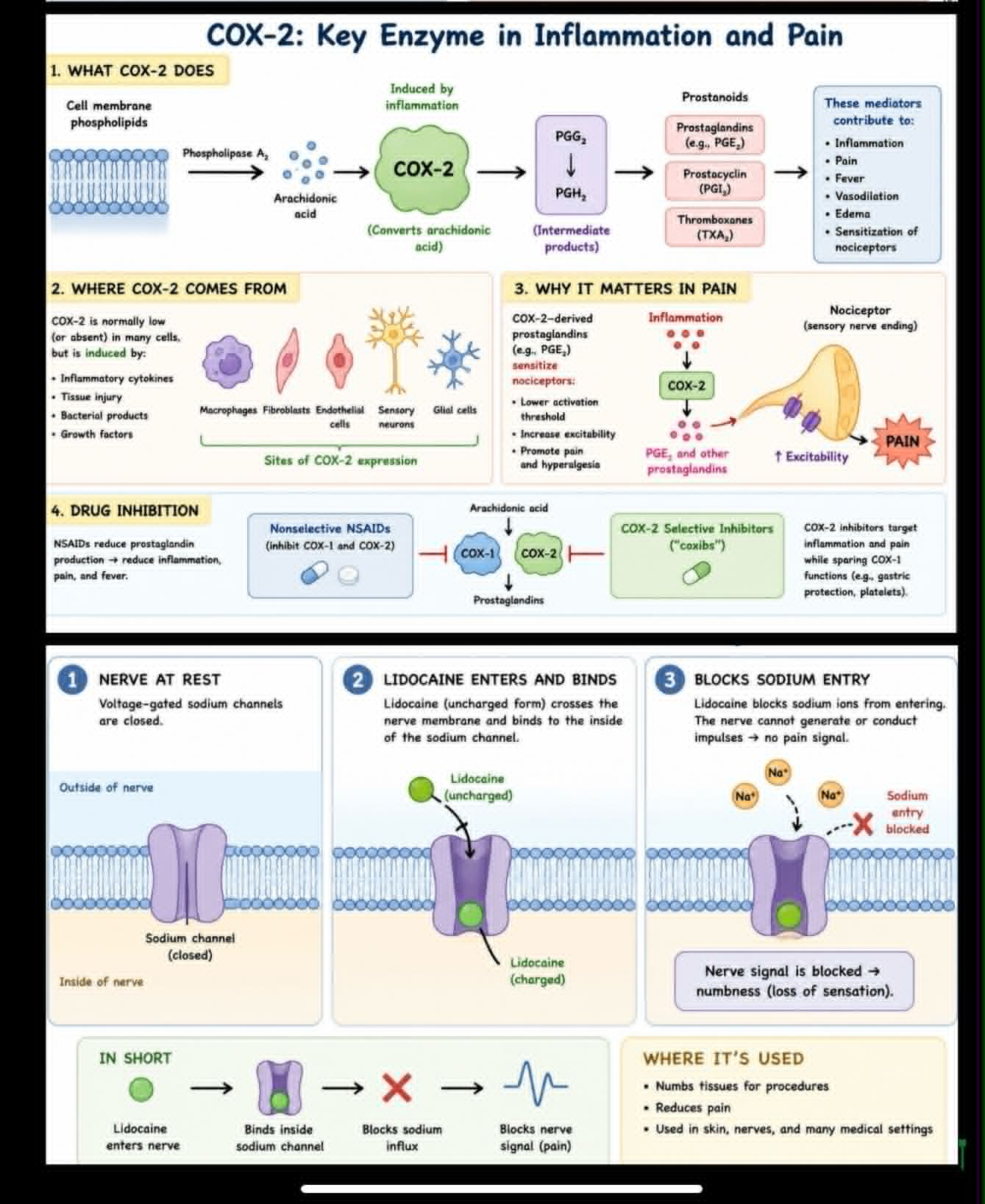
non-steroidal anti-inflammatory (NSAIDs like ibuprofen inhibit COX2 activity of making prostaglandins which cause inflammation & pain)
(where COX2 lowers pain activation threshold in nociceptors)
local anesthetics (lidocaine, which is a VGSC antagonist
that works by binding to the inside of the VGSC to block Na+ influx → SO can’t conduct impulses (no dep- to reach pain threshold) → SO no pain signal)
describe how does acute pain become chronic pain (3 parts w/ 3 certain terms)
__
pain sensitization (← def.) can occur at the level of (1)
t/f: in neuropathic pain, non-noxious/non-tissue damaging stimuli can become noxious/tissue-damaging due to (1)
__
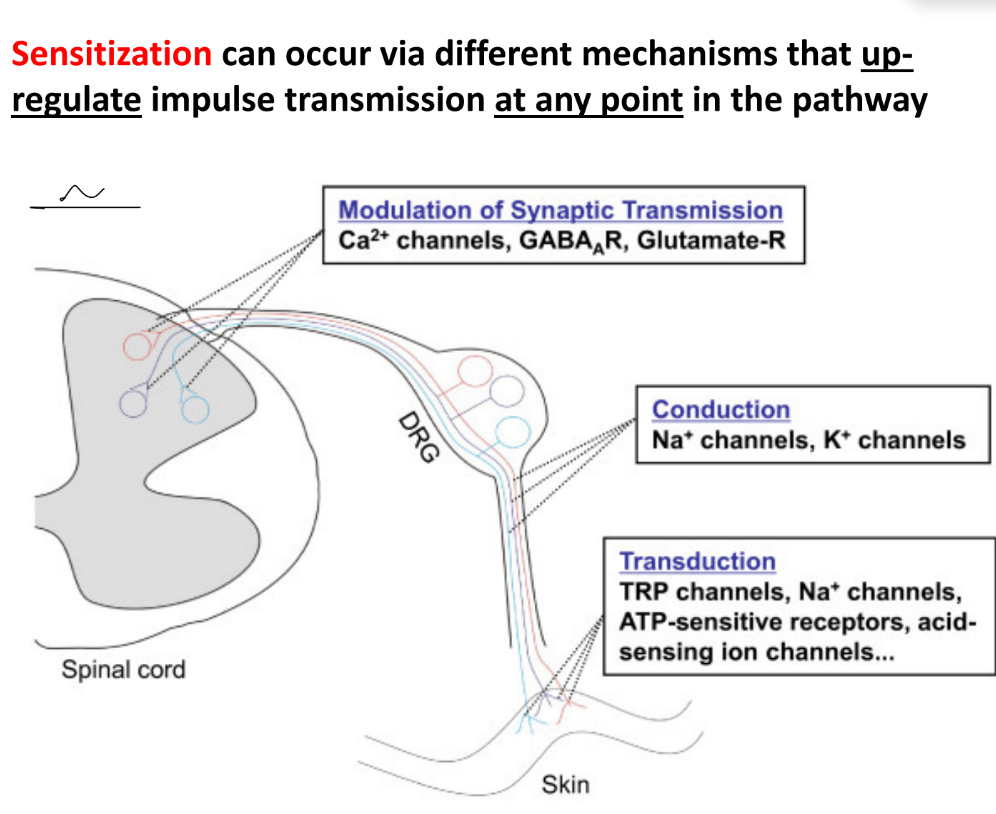
sensitization can occur in different mechanisms that all __ the transmission of pain impulses/signals at ANY point in the pathway
hypersensitivity can develop in the CNS, which remodels synaptic connections in the brain (synaptic plasticity) especially in the somatosensory cortex, which will increase spread of __ & __ in time
________________
t/f: stress, anxiety, mood, hormonal states can all contribute to pain perception from acute to chronic
and, these chronic pain experiences can alter __ to be mostly __ __
^^ overall, this creates a cycle of a __ feedback loop b/w (3)
acute pain begins as nociceptive pain (← damage to tissue due to inflammation or trauma)
persistent nociception can lead to sensory hypersensitivity (← pain w/o identifiable nerve or tissue damage)
if have damaged peripheral or central nerves, then it leads to neuropathic pain
__
pain sensitization can occur at the level of peripheral sensory nerves
pain sensitization — amplified pain signals cause hyperactive CNS
_
true
in neuropathic pain, non-noxious/dangerous stimuli can become noxious/tissue-damaging due to lower AP / pain activation thresholds
__
sensitization can occur in different mechanisms that all up-regulate/increase the transmission of pain impulses/signals at ANY point in the pathway
hypersensitivity can develop in the CNS, which remodels synaptic connections in the brain (synaptic plasticity) especially in the somatosensory cortex, which will increase spread of pain & persistence in time
_________________
true
stress, anxiety, mood, hormonal states can all contribute to pain perception from acute to chronic pain perception
and, these chronic pain experiences can alter behavior to be mostly maladaptive behavior
(^^ clinical status of chronic → psychological states, like stress → behavior)
^^ overall, this creates a cycle of a negative feedback loop b/w chronic pain, maladaptive behavior, and psychology
best way to treat chronic pain is using a __/__ approach (← briefly explain/give ex.)
why do we want to shift attention? do so through what 3 techniques? BUT shifting attention is not the same as __ pain, which just worsens the subjective pain perception
best way to treat chronic pain is using a multimodal / biopsychosocial approach
biological (medication, PT), cognitive (goal is to shift attention), social (support networks, life meaning)
want to shift attention b/c:
neuroplasticity: constantly focusing on pain can strengthen that pathway, so it basically increases the brain’s sensitivity to chronic pain
psychology: stress, anxiety, etc. can amplify/increase pain perception
distraction shifts attention, which can reduce subjective pain intensity
shift attention w/:
cognitive behavioral therapy (CBT)
acceptance & commitment therapy (ACT)
mindfulness-based stress reduction (MBSR)
BUT shifting attention is not the same as suppressing pain, which just worsens the subjective pain perception
def. anesthesia
name & describe the 4 types of anesthesia
is insensitivity to pain
general anesthesia — use a medications called anesthetics to put a patient into a sleep-like state before surgery/medical procedure, where they can’t breath on their own
regional anesthesia — numbs an area of the body to prevent pain sensation, like nerve blocks, epidurals
sedation — monitored anesthesia to make the patient drowsy and relaxed, but not sleepy & they can still breath on their own, like with propofol
local anesthesia — numbs a small area of the periphery, like with lidocaine
for general anesthesia
general anesthesia is a drug-induced __ state defined by 5 endpoints (← name & def.)
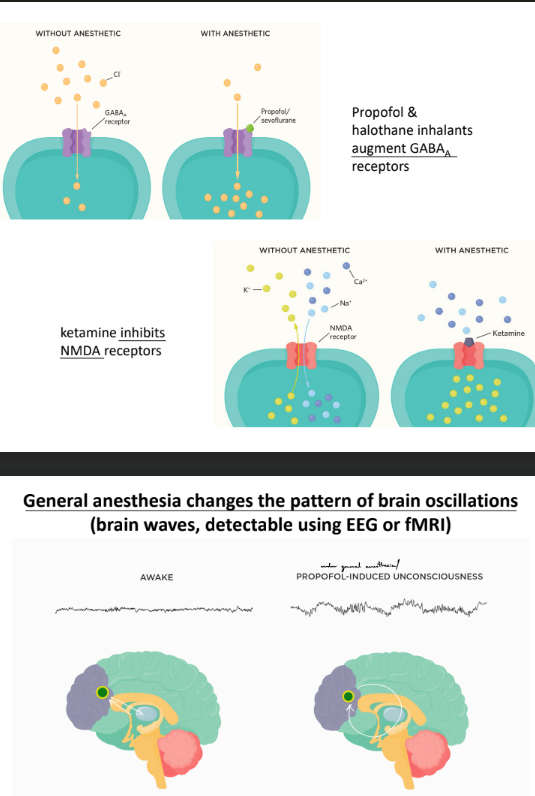
how does propofol & ketamine affect specific Rs and ion flow?
this shows that general anesthesia will change brain patterns b/c …
general anesthesia is a drug-induced reversible state defined by 5 endpoints:
unconsciousness — lack of awareness of sensory input
analgesia — lack of pain
akinesia — lack of movement
amnesia — lack of recall
physiological stability — maintaining normal levels of all important physiological functions
_
propofol excites/increases GABAA Rs (so increases Cl- influx)
ketamine inhibits NMDARs (so inhibit Ca2+, Na+ influx and K+ influx)
^^
this shows that general anesthesia will change brain patterns b/c GABAA Rs and NMDARs affect excitatory & inhibitory neurons
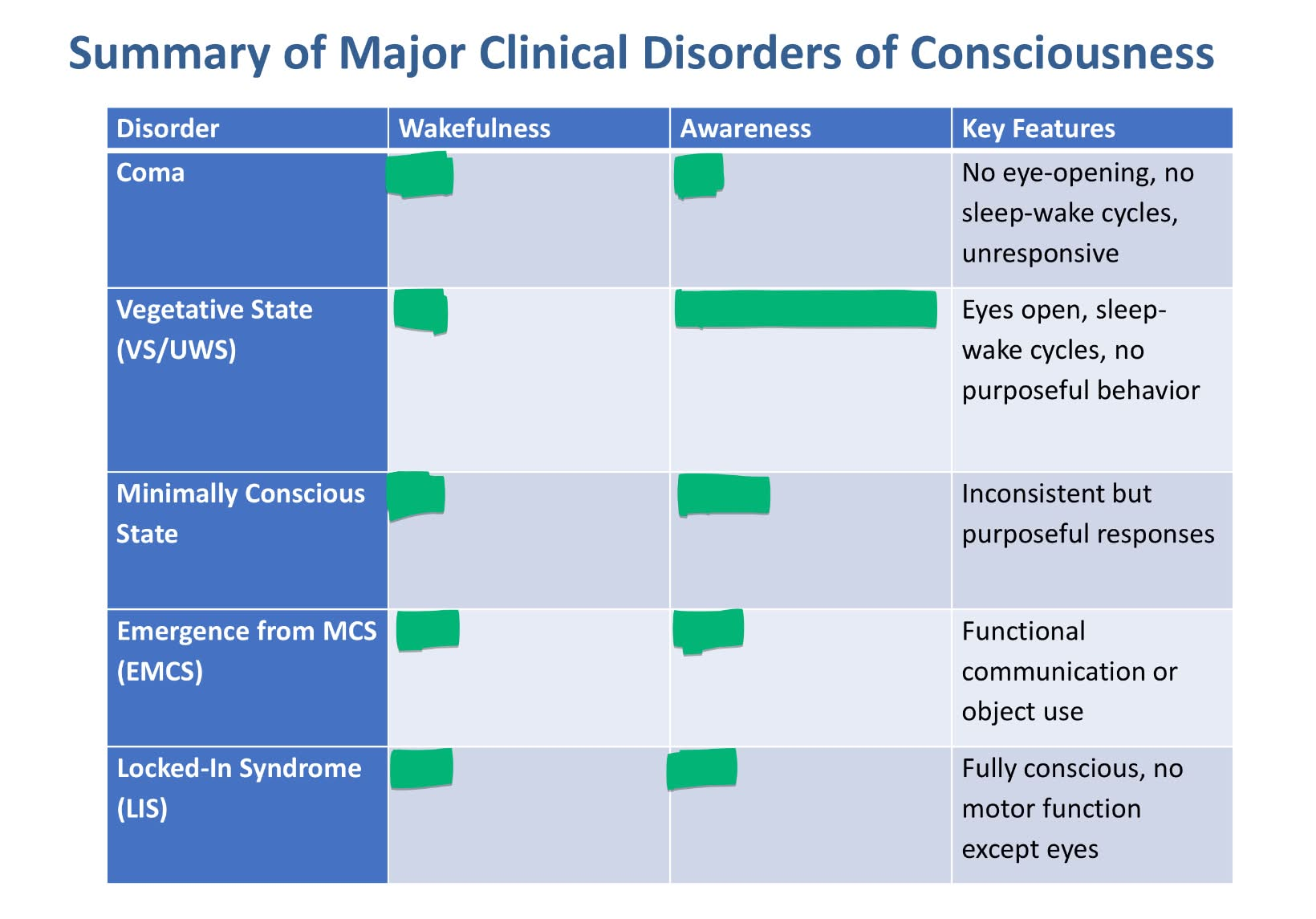
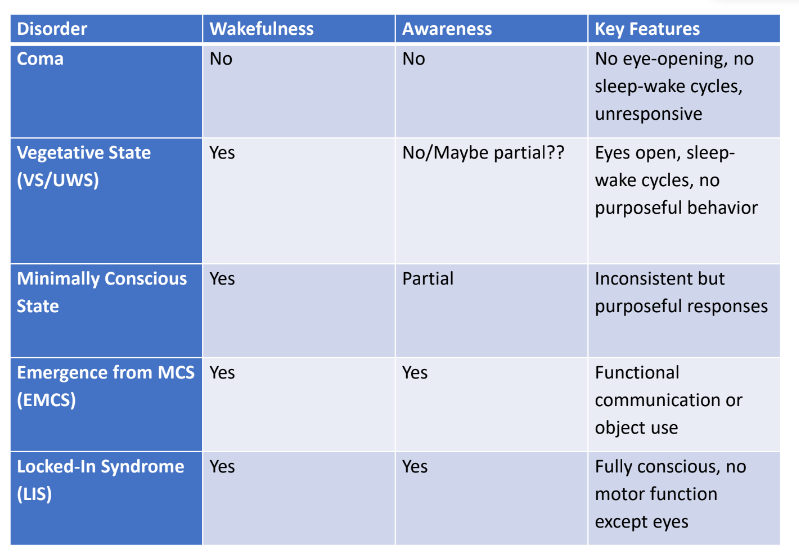
state & describe the 5 disorders of consciousness (2, 2, 2, 2, 3)
answer pic w/ yes, no, or partial
coma
no wake or awareness
no sleep-wake cycles or reflexes
vegetative state / unresponsive wakefulness syndrome
has wakefulness, BUT no awareness
may have random reflex behaviors
minimally conscious states (MCS)
wakefulness w/ inconsistent awareness
divided into MCS- (low level responses) & MCS+ (high level responses)
emergence from MCS ← is b/w MCS and fully conscious states
regain ability to communicate, which shows recovery of awareness & already have wakefulness
can do object use, where choose appropriate object to use given 2 choices
locked-in syndrome
fully conscious & aware
almost complete paralysis, except for eye movements
is often misdiagnosed
def. neuropsychiatric disorders (w/ 3 specific terms ← def.)
relate it to genetic and environment
give 2 examples of neuropsych disorders that
about __% of Americans 18+ suffer from a mental/behavioral disorder
name some of these neuropsychiatric disorders (2, 1 of them w/ ~3)
the most effective treatment for neuropsychiatric disorders are …
disorders about affect, cognition, and behavior due to abnormal brain function or disease outside the brain
affect — observable signs of emotional state
cognition — conscious intellectual thinking
behavior — external reactions to environment
neuropsych disorders are both genetic & environment (like ASD), BUT has many genetic risk genes that include CNVs
high genetic risk factors are bipolar disorder & schizophrenia
__
about 25% of Americans 18+ suffer from a mental/behavioral disorder
schizophrenia
mood disorders
bipolar disorder
major depression
anxiety-related disorders, like OCD (obsessive-compulsive disorder)
the most effective treatment for neuropsychiatric disorders are combination of medication & psychotherapy
def. schizophrenia (SCZ)
symptoms (3)
usually appear in __ __ (← age for men vs. women)
is rarely diagnosed in __ __, BUT is believed to originate in early brain development
is a __ brain disorder
t/f: has high prevalence (aka affects large part of global population 0.5%)
strong __ risk of __%
describe (2)
what is 1 modifiable risk factor for SCZ?
a long-term mental/psychiatric disorder that involves a breakdown b/w though/cognition, emotion/affect, and behavior
symptoms:
hallucinations, disordered thinking, lack of motivation
^ usually appears in early adulthood (men early 20s, women late 20s-early 30s)
^ rarely diagnosed in children, BUT is believed to originate in early brain development
is a CHRONIC brain disorder
true: has high prevalence (aka affects large part of global population 0.5%)
strong GENETIC risk of 80%
there is no monogenic diagnostic gene / no single gene that determines SCZ risk, but have multiple risk genes
people w/ SCZ, bipolar disorder, and ASD share many risk genes
modifiable risk factor for SCZ is heavy THC cannabis use, b/c it increases the risk of SCZ in individuals who are already at high risk
for SCZ
name the 3 categories of symptoms w/ ex. in each category of such symptoms
t/f: these symptoms / the key pathological features of SCZ are NOT unique to SCZ
positive symptoms / psychosis
hallucinations
delusions
disordered thinking
negative symptoms
decreased motivation
social withdrawal
extreme case is catatonic state of immobility & unresponsiveness (like a stupor)
impaired cognition
problems w/ attention, memory, etc.
(^^^ think of “+” as abnormal behaviors, and “-” as decreased behaviors)
__
true (i.e. also seen in bipolar disorder, substance abuse, ASD, ADHD, neurodegenerative diseases)
name the 3 hypotheses for SCZ w/ brief description of each
dopamine hypothesis
hyperfunction in mesolimbic pathway
hypofunction in mesocortical pathway
DA alters the salience (aka degree/effectiveness) of stimuli
glutamate hypothesis
hypofunction in NMDAR-mediated plasticity
muscarinic (cholinergic system) hypothesis
hypofunction in CNS muscarinic Rs
for SCZ
def. dopamine hypothesis
is charac. as hyperfunction of DA in __ & hypofunction of DA in __ __
evidence for (3) vs. evidence that limits/doesn’t fully support (3) the hypothesis
DA hypothesis — certain dopaminergic pathways are overactive, specifically hyperactivity in dopamine D2 R signaling in subcortical & limbic brain, which leads to the “positive" symptoms of SCZ
is charac. as hyperfunction of DA in prefrontal cortex & hypofunction of DA in nucleus accumbens
evidence for:
antipsychotics work by blocking D2 Rs
DA-enhancing drugs can cause psychosis-like symptoms (← positive symptoms)
DA dysregulation relates to abnormal salience aka positive symptoms (b/c “+” is abnormal, “-” is decreased)
evidence that limits/doesn’t fully support the hypothesis:
blocking D2 Rs doesn’t really treat negative & cognitive symptoms
DA can affect striatal, mesolimbic, mesocortical, and nigrostriatal circuits in different ways
the Cobenfy drug shows that you don’t need to block D2 Rs to treat SCZ
for SCZ: DA hypothesis
def. antipsychotic medications/antipsychotics
def. in terms of “typical” vs. “atypical” antipsychotics (& give ex. of each)
__
what are the 2 main classes of DA Rs?
ALL DA Rs are __
__
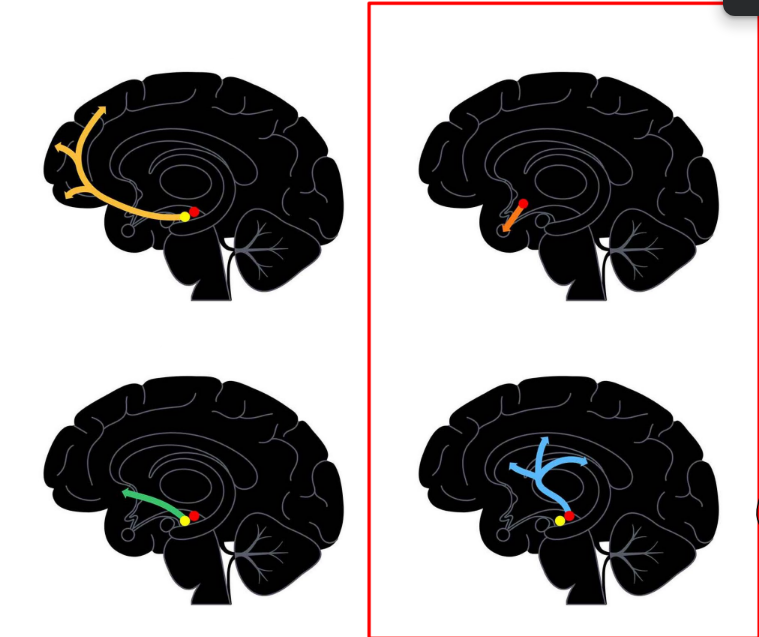
name the brain’s 4 DA pathways
each pathway does what general function?
which 2 relate to SCZ and mood disorders? how does this info relate to how to address SCZ & bipolar disorder treatment?
label the picture w/ the brain’s 4 DA pathways
antipsychotics — are used to manage psychosis (positive symptoms) in SCZ & bipolar disorder
typical antipsychotics — 1st gen drugs that block dopamine D2 Rs
ex: Haldol, Thorazine
atypical antipsychotics — 2nd drugs that block BOTH DA Rs & serotonin Rs
ex: clozapine
__
D1 and D2 dopamine Rs
all DA Rs are metabotropic
__
nigrostriatal pathway — DA from SN (substantia nigra) → striatum
motor pathways
mesocortical pathway — DA from VTA (ventral tegmental area) → cortical areas, like prefrontal cortex (PFC)
cognition
mesolimbic pathway — DA from VTA → nucleus accumbens
reward-seeking behavior & motivation
tuberoinfundibular pathway — DA from hypothalamus → pituitary
normally reduces hormone release, which reduces lactation
^ mesocortical & mesolimbic pathways rel. to SCZ and mood disorders
SO for treatment, we would want to suppress the tuberoinfundibular & nigrostriatal pathways W/O affecting the 2 meso- pathways
for SCZ: DA hypothesis
describe the altered salience hypothesis (which is part of the dopamine hypothesis for DA) (← 2)
what is the mech. (1 short statement ← explain how)
hypothesis formed from this
__
altered salience hypothesis
overfocus on neutral stimuli, so that coincidences appear meaningful (not as chance like we usually do)
may cause hallucinations & delusions
mech:
hyperactive mesolimbic pathway causes abnormal salience
the mesolimbic pathway regulates the “salience” of events, where DA tags an event as “positive” or “negative”
the nucleus accumbens is involved w/ motivation & reward-seeking behavior
hypothesis:
excess DA will assign salience to insignificant/neutral events, which leads to psychotic state/psychosis
(reminder that the DA hypothesis relates to psychosis/”+” symptoms of SCZ)
for SCZ
glutamate hypothesis is charac. by (1), which causes (1)
how does this hyp. relate to pharmacology, autoimmunity, genetics?
for autoimmunity, def. PANDAS/PANS
for genetics, explain GRIN2A
glutamate hypothesis is charac. by hypofunction of NMDAR-mediated plasticity, which causes E/I imbalance (which disrupts cortical microcircuits, esp. inhibitory interneuron control of pyramidal neurons)
pharmacology: PCP & ketamine are NMDAR antagonists that can cause psychosis-like symptoms & cognitive impairment (antagonists which cause hypofunction)
autoimmunity: makes anti-NMDAR antibodies in autoimmune encephalitis (aka make antibodies against NMDARs to cause hypofunction)
genetics: have rare monogenic causes for SCZ related to producing glutamate (i.e. in GRIN2A and GRIA3 subunits of NMDARs)
for autoimmunity:
PANDAS/PANS — pediatric acute neuropsychiatric syndrome, that is seen with OCD or tics occurring after infection
for genetics:
rare monogenic causes of psychiatric disorders (i.e. SCZ) are ass. w/ rare NULL mutations in the GRIN2A subunit of NMDARs
for SCZ
muscarinic (cholinergic system) hypothesis is charac. by (1)
def. Cobenfy / KarXT
is a combination of what 2 drugs, that each do what? how do they work together?
KarXT indirectly influences __ AND __ neurotransmission
t/f: is thought to address all 3 types of SCZ symptoms (+, -, cognitive impairment)
mech. of how KarXT/Cobenfy acts in the brain:
does __ via muscarinic Rs, where xanomeline activates (2) which are __
why doesn’t trospium simply negate the effects of xanomeline?
muscarinic (cholinergic system) hypothesis is charac. by hypofunction in CNS muscarinic Rs
Cobenfy/KarXT — first antipsychotic drug to treat SCZ by targeting cholinergic (ACh) signaling, instead of dopaminergic (DA) signaling
combination of xanomeline & trospium
xanomeline is a muscarinic R agonist
trospium is a muscarinic R antagonist that reduces peripheral side effects
^ together, xanomeline stimulates muscarinic Rs all over the body and brain, while trospium will block muscarinic Rs ONLY in the periphery/body
KarXT indirectly influences glutaminergic AND dopaminergic neurotransmission
true: is thought to address all 3 types of SCZ symptoms (+, -, cognitive impairment)
mech:
does neuromodulation (controlling response of fast-acting NTs, like glutamate) via muscarinic GPCRs
where xanomeline activates M1 and M4 Rs (which are GPCRs b/c they are muscarinic/metabotropic)
trospium can’t cross the BBB in the brain, so it can’t completely negate effects of xanomeline
for neuropsychiatric disorders: mood disorders
def. bipolar disease (BD)
is ass. w/ dysregulation of __ modulation
typically diagnosed during (2), is atypical if diagnosed in __
relate to genetic and environment
t/f: genetic risk overlaps w/ SCZ and major depression
t/f: recurrent mech. are limbic-PFC regulation, reward salience, cognitive control
t/f: the treatment of BD is dependent on the phases/bipolar states, like acute mania, BD, psychosis, suicidality, etc.
BD — brain disorder that causes unusual shifts in mood, energy, activity levels, and ability to do daily tasks
is ass. w/ dysregulation of monoamine modulation
typically diagnosed during late adolescence/teens & early adulthood, is atypical if diagnosed in children
strong genetic factor
__
true for all
for neuropsychiatric disorders: mood disorders
def. major depression disorder (MDD) ← incl. symptoms
depression, PTSD, and substance abuse are all __ __ (← def.)
__-__% of cases can resolve w/o treatment
t/f: depression is complex, but common and treatable
estimated __-__% will suffer from MDD some point in their lives
MDD is the leading cause of __ in the US b/w ages 15-44
MDD mech. involves what 3 things?
4 steps for MDD treatment
for severe MDD: treat w/ (2)
MDD — mental health disorder charc. by low mood, low self-esteem, and loss of pleasure and motivation in things they used to enjoy
depression, PTSD, and substance abuse are all internalizing disorders — debilitating/disabling experiences that result from persistent negative thoughts
10-20% of cases can resolve w/o treatment
true: depression is complex, but common and treatable
estimated 8-12% will suffer from MDD some point in their lives
MDD is the leading cause of disability in the US b/w ages 15-44
MDD mech. involves:
monoamines, where serotonin transporters (SERTs) are targeted by SSRIs
stress & inflammation
plasticity & circuits
MDD treatment:
assess
start evidence-based treatment
measure effects for 6-12 weeks
switch treatments if ineffective
^ where severe MDD treated w/ combination of psychotherapy & medications (compared to first-line treatment of either medications or psychotherapy)
for neuropsychiatric disorders: mood disorders, specifically MDD
for first-line MDD treatment, __ are commonly taken medications
ex. of this (5)
mech. of this type of medication/drug
__
what is the traditional vs. current view of MDD?
for current view, give hypothesis on ketamine mech. to treat MDD
ex. of 3 things/methods for MDD treatment (brief)
there is ongoing research to see if __ can be used to treat MDD, PTSD, etc.
for first-line MDD treatment, SSRIs (selective serotonin reuptake inhibitors) are commonly taken medications
ex: Prozac, Lexapro, Zoloft, Paxil, Celexa
mech:
5HT (serotonin Rs) synapse activity of serotonin reuptake is terminated by SSRIs, which prolongs serotonin being in the synaptic cleft, which increases activation of 5HT Rs
(aka SSRIs inhibit serotonin reuptake by 5HT Rs, so increases 5HT R activation)
__
traditional: depression = serotonin deficiency
current: depression is due to impaired plasticity & dysfunctional neural circuits
hyp: ketamine may restore synaptic connectivity by blocking NMDARs on specific neurons (to reduce LTD)
ex. of 3 things/methods for MDD treatment:
ketamine, esketamine
ECT (electroconvulsive shock therapy, which rapidly solves MDD BUT impairs memory)
there is ongoing research to see if psychedelics can be used to treat MDD, PTSD, etc.
for neuropsychiatric disorders: mood disorders
def. anxiety disorders
name 4 types of common anxiety disorders & briefly def. each
__
anxiety medications provide __ __ from acute symptoms (← give 1 ex.)
treatment for chronic anxiety is (2)
…
how do benzodiazepines work / its mech.?
anxiety disorders — feel anxious that goes beyond than temporary worry or fear, which doesn’t go away, can get worse over time, and interferes w/ daily activities
general anxiety disorder (GAD) — future worries
social anxiety — fear of judgment
panic disorder — fear of panic attacks
OCD — intrusive thoughts & compulsive actions
__
anxiety medications provide short-term relief from acute symptoms (i.e. benzodiazepines)
treatment for chronic anxiety is combination of SSRIs (medications) & psychotherapy like CBT
…
benzodiazepines mech:
GABA & benzodiazepine have to simultaneously bind to GABAA Rs to cause Cl- influx & hyperpolarization
t/f: ASD, BD, and SCZ has shared risk genes
true
__% of US pop. have drug or alcohol addictions
any __ can become a __, and any __ can become a __/__
how do addictions form? ← answer
where NORMALLY, reinforcement of these brain pathways are thought to be related to plasticity (__), BUT with ADDICTION, chronic exposure to drug cues create even stronger __ that have negative effects of addiction
substance use disorders have a highly __ risk
commonly-abused substances include (list a few)
10% of US pop. have drug or alcohol addictions
any behavior can become a habit, and any habit can become a dependency/addiction
addictions arise when:
habits of drug use, which is highly rewarding, are reinforced by enhancing brain pathways related to the reward system, i.e. the mesolimbic DA pathway
where NORMALLY, reinforcement of these brain pathways are thought to be related to plasticity (LTP), BUT with ADDICTION, chronic exposure to drug cues create even strong LTP that have negative effects of addiction
substance use disorders have a highly genetic risk
commonly-abused substances include: opiates, cocaine, methamphetamines, alcohol, tobacco, benzodiazepines, marijuana
for substance use disorders & addiction
chronic use of substances can lead to __ & __
def. tolerance, physical dependence, psychological dependance, withdrawal
__
t/f: there were 4 waves of US opioid overdose epidemic, where 1st ass. w/ prescription opioids, then heroin, then illicit fentanyl, now fentanyl + stimulants. saw an increase from COVID & decline in 2024, where total overdose deaths trend started declining in 2022 and since
most of these overdose deaths (__%) were due to __
3 possible reasons on this decline
chronic use of substances can lead to tolerance & dependence/addiction
tolerance — require more of the substance to feel the effects
physical dependence — experiences physical discomfort w/o the drug
psychological dependance — doesn’t feel like themselves w/o the drug
withdrawal — psychological or physical reactions to absence of drug
__
true
most of these overdose deaths (70%) were due to opioids
decline possibly b/c:
increased access to Naloxone aka NARCAN (used to reverse opioid overdoses)
better treatment availability for substance use disorders
teach harm reduction strategies
for substance use disorders & addiction
about __% of patients prescribed opioids for chronic pain misuse them
2 most known opiates
opioid Rs are __, where (how do the 3 subunits behave?)
t/f: opioid Rs are present in most brain areas
__
why did fentanyl become an overdose problem?
__
nicotine spec. acts on what type of Rs?
about 25% of patients prescribed opioids for chronic pain misuse them
2 most known opiates: heroin & morphine
opioid Rs are GPCRs, where alpha subunit binds to Gi-protein & beta-gamma subunits directly regulate other effector proteins like ion channels
true (opioid Rs are present in most brain areas)
__
pure fentanyl powder is very potent & hard to dilute properly, so fentanyl in street drugs are way too strong & dangerous
__
nicotine spec. acts on nicotinic ACh Rs (nAChRs)
for substance use disorders & addiction
drugs → __ → __
where reward system is heavily influenced by DA from the __ b/c …
__
t/f: MALADAPTIVE recruitment of certain brain memory circuits/systems can drive addiction b/c normally, DA Rs (D1 and D2) and glutamate Rs are involved in normal learning
t/f: CREB and other TFs help convert early LTP + memory into late LTP
__
repeated activation of the same pathways __ & __ the addiction feelings & behaviors, just like with other types of __
a key factor in addiction is that learning __ the __ __ of the brain, which causes feelings of __ from __ stimuli
t/f: behavior circuits that experience LTP have even stronger LTP when DA is released from VTA
drugs → DA → reward
where reward system is heavily influenced by DA from the VTA b/c the release of DA from VTA converges onto neurons in the nucleus accumbens to increase LTP-like glutamate signaling, which causes excitation & reinforcement/strengthening of neural circuits → leading to strong LTP
(reinforces the internal “reward sensation” aka the positive salience of the experience)
_
true
true
_
repeated activation of the same pathways reinforces & strengthens the addiction feelings & behaviors, just like with other types of learning
a key factor in addiction is that learning (involving excitation from increased glutamate signaling) enhances the reward behavior/circuitry of the brain, which causes feelings of pleasure from harmful stimuli (like drugs of abuse)
_
true
for substance use disorders & addiction
def. relapse
triggered by (3)
the __ __ mediates the bidirectional communication of stress b/w the body & brain
moderate levels of stress can be __, but strong and/or persistent stress is __ b/c …
relapse — drug-seeking habit is reactivated by drug-related cues, like:
stress
exposure to conditioned stimulus (i.e. environment w/ drug use)
consuming the drug
the HPA axis (hypothalamic-pituitary-adrenal) mediates the bidirectional communication of stress b/w the body & brain
moderate levels of stress can be adaptive, but strong and/or persistent stress is maladaptive (b/c trend of drug-use to relieve excess stress)