Pancreatic Conditions
1/85
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
what does the pancreas release?
1. digestive enzymes - amylase, lipase, protease
2. endocrine hormones - glucagon, insulin, somatostatin, pancreatic polypeptide
what is acute pancreatitis?
1. inflammation of the pancreas
2. can resolve itself if mild
3. can become critically ill if severe
4. some develop chronic pancreatitis
what are some consequences of pancreatitis?
1. fluid volume deficit and e-lyte imbalances (#1 issue)
2. peritonitis and abdominal compartment syndrome
3. pseudocysts, abscess formation, infection
4. hemorrhage and necrotizing pancreatitis (SEVERE issue)
5. pleural effusion and ARDS potential (fluid moving into the pleural cavity
6. DVT and DIC
what are the two most prevalent causes of acute pancreatitis?
1. gallbladder stones
2. alcohol use
what are some other causes of acute pancreatitis?
G - gallstones
E - ETOH
T - trauma
S - steroids
M - mumps
A - autoimmune
S - scorpion/spider bite
H - hypercalcemia/hyperlipidemia
E - ERCP
D - drugs (diuretics, sulfa drugs, estrogen, cannabis)
what is the primary manifestation of acute pancreatitis?
severe pain (PRIORITY, after airway and fluid resuscitation)
what values are elevated in the presence of acute pancreatitis?
1. serum amylase - up within 24 hours of onset, normalized within 72 hours
2. serum lipase - up after 48 hours of onset, and stays up for 5-7 days at least
what is the go to test for acute pancreatitis?
elevated serum lipase
what are the pain characteristics?
1. epigastric, LUQ, mid-abdominal
2. radiation to back and shoulders
3. deep, sharp, intense after eating
4. guarding, rebound tenderness, rigid muscles
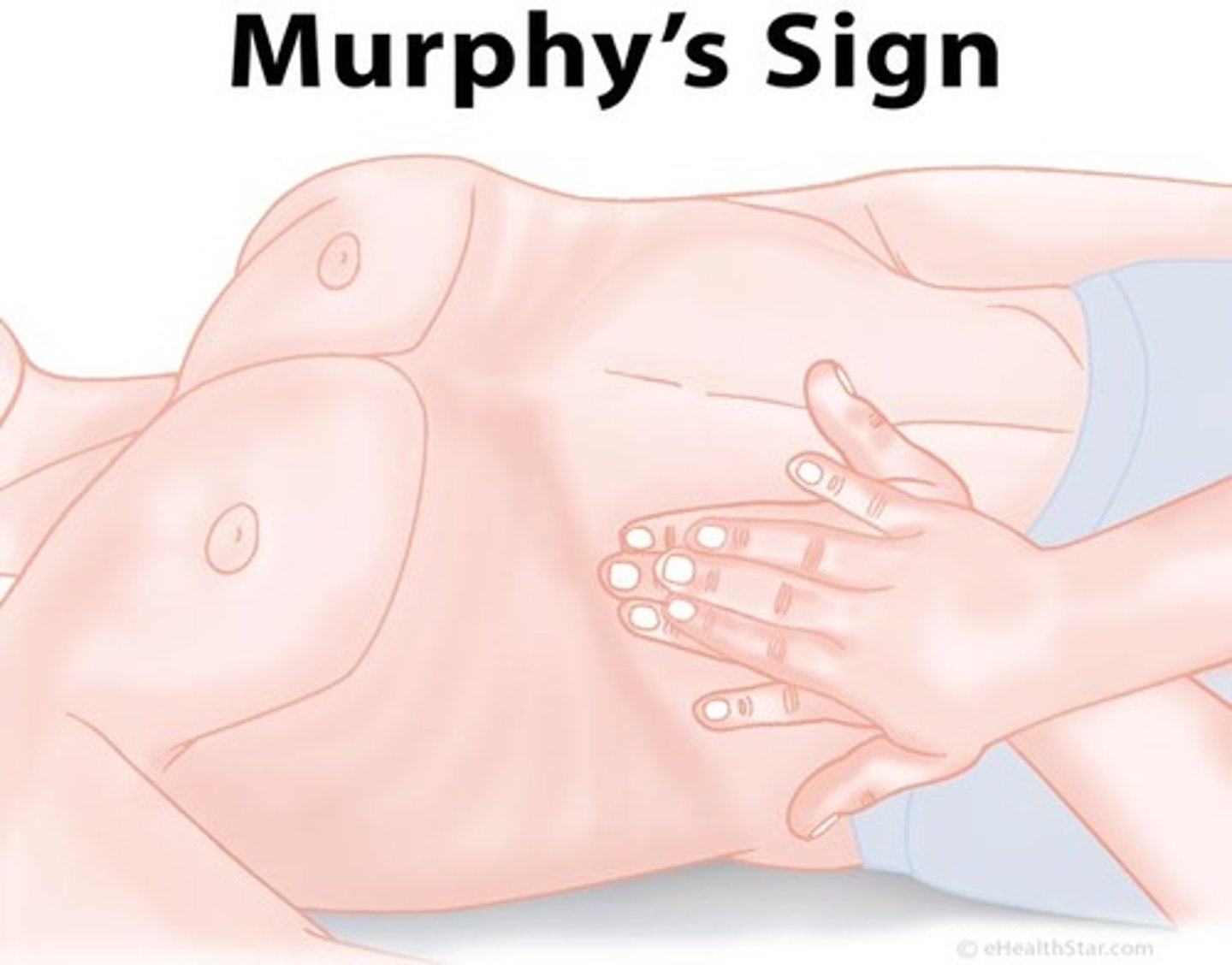
5. gallbladder involvement (Murphy's sign, RUQ pain radiating to shoulder)
6. distended, rigid, board-like abdomen, decreased bowel sounds, decreased UOP, shallow breaths, N/V (peritonitis potential)
what is murphy's sign?
deep palpation of RUQ under the rib during inspiration
how can we manage pain in a patient with acute pancreatitis?
1. rest
2. semi fowler's
3. possible fetal position (in the absence of breathing issues)
4. narcotics - hydromorphone (Dilaudid), sublimaze (Fentanyl) - AVOID MORPHINE
what are the additional concerns of acute pancreatitis?
1. fluid volume deficit
2. pulmonary involvement (pleural effusion, ARDS potential)
3. bleeding potential
4. clotting concerns
5. GI assessment and nutrition status
6. signs of bile duct obstruction
7. infection potential
8. hypocalcemia
what are the manifestations of fluid volume deficit?
1. decreased BP (may have a normal BP at first)
2. increased HR
3. increased RR (shallow breaths)
4. decreased UOP (GOAL UOP = > 0.5-1 mL/kg/hr)
5. increased temp
6. dry mucous membranes
7. delayed cap refill
8. poor skin turgor
9. HD changes (decreased CVP, PCWP, CO)
10. lab changes (widened BUN:CR, increased H/H)
what is included in the patient care for fluid volume defecit?
1. IV fluids (LR, maybe colloid)
2. electrolyte management (draw labs)
3. monitor for volume overload with correction
what are we looking for with volume overload?
1. pulmonary signs (crackles)
2. abdominal compartment syndrome (sustained bladder pressure > 20 mm Hg)
what is the best indicator that fluid volume status is being corrected?
increased UOP (through, BP will be the first sign)
what are the manifestations of pulmonary involvement, which include the potential for pleural effusion and ARDS?
1. left lung most vulnerable
2. dyspnea, hiccups, pleuritic chest pain
3. adventitious sounds (diminished lung sounds)
4. O2 sat and ABG changes (respiratory acidosis, usually starts out with alkalosis)
how should we respond to hiccups?
it could indicate diaphragm and phrenic nerve irritation (get a CXR)
what is included in the patient care for pulmonary involvement?
1. oxygenation
2. positive pressure ventilation
3. thoracentesis
4. chest tube placement
5. diuretics
what diuretic is used to aide in pulmonary involvement associated with acute pancreatitis?
furosemide (Lasix)
what should we keep in mind with Lasix?
1. don't push too fast
2. monitor for ototoxicity (tinnitus)
3. monitor K+
what are the manifestations of bleeding?
1. VS changes (decreased BP, increased HR)
2. lab changes (decreased H/H)
3. cullen's sign
4. grey turner's sign
what is cullen's sign?
bleeding in the abdominal cavity

what is grey turner's sign?
retroperitoneal bleeding

what is included in the patient care for bleeding?
1. anticipate prep for surgery
2. maintain HD status
3. transfusion with volume replacement (RBCs, FFP, fluid, cryoprecipitate - concentrated clotting factors)
what are the manifestations associated with clotting?
1. DVT assessment (red, swelling, warmth)
2. DIC assessment (bleeding and clotting at the same time that warrants both Heparin and a transfusion)
what is included in the patient care for clotting?
1. prophylactic anticoagulant
2. SCDs
3. hydration
4. ambulation
what are the manifestations of GI and nutrition alterations?
1. N/V
2. distention, indigestion, anorexia
3. ileus (decreased sounds, distention, N/V)
4. low serum albumin, pre-albumin (analyzes if fluid can be held in the cells)
5. increased blood glucose (insulin may not be working, stress response)
what is included in the patient care for GI and nutrition alterations?
1. NPO initially BUT resume diet ASAP
2. possible TPN or enteral feeding
3. possible NGT (rest and decompress)
4. ondansetron (Zofran)
5. compassionate care for nausea
6. GI protection (PPIs, H2 blockers)
7. insulin
what would prevent us from resuming the diet ASAP?
1. N/V
2. pain
3. ileus
how should we resume the diet?
1. clears to solids
2. LOW FAT (trigger for gallbladder issues)
what do we want to monitor for with Zofran?
QT interval (potential for torsades)
what is included in compassionate care for nausea?
1. coordinate care
2. remove smells
3. cool towel on neck
what are the manifestations of a bile duct obstruction?
1. pain ("biliary colic" in the RUQ)
2. jaundice
3. oily, pale colored, foul smelling STOOLS THAT FLOAT
4. liver enzyme elevation (increased AST, ALT)
5. elevated bilirubin
what is included in the patient care for a bile duct obstruction?
1. laparoscopic cholecystectomy
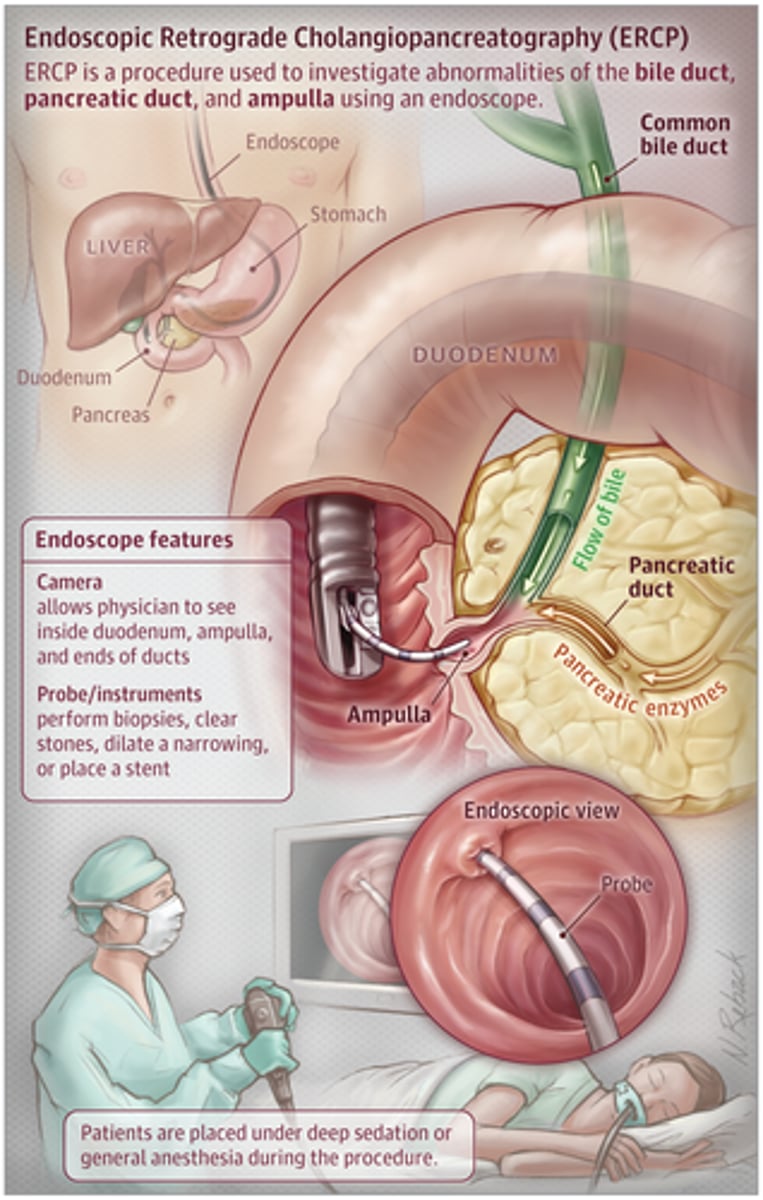
2. endoscopic cholangiopancreatography (ERCP)
what is an ERCP?
scope goes down to the small bowel and can retrieve stones if present
what are the manifestations of an infection with acute pancreatitis?
1. WBC and differential trends up
2. increase in pain
what is included in patient care for an infection?
1. standard measures
2. possible antibiotics
3. monitor for sepsis (increased lactate, abnormal cultures, prolactin)
what are the manifestations of hypocalcemia?
1. trousseau sign (BP cuff)
2 chvotek's sign (cheek)
what is included in the patient care for hypocalcemia?
calcium chloride or calcium gluconate IV
what should we be alert for from the moment of admission?
signs of alcohol withdrawal
what is delirium tremens (DT)?
most severe form of withdrawal
what are the symptoms associated with delirium tremens (DT) manifestations?
1. shaking
2. vomiting
3. increased HR
4. increased BP
5. increased temp
6. sweating
what is included in the management of alcohol withdrawal and DTs?
1. quiet environment
2. patient safety
3. nutrition and hydration
4. banana bag and benzos (Lorazepam)
5. hospital protocol
what is the antidote for benzos?
flumazenil (Romazicon)
what is chronic pancreatitis?
1. persistent inflammation
2. periods of remission and exacerbation
3. scarring and damage to the pancreas and surrounding tissues
4. not reversible!
5. leads to decreased function in both exocrine and endocrine pancreas
what is the primary risk factor of chronic pancreatitis?
alcohol abuse
what does decreased exocrine function lead to?
1. decreased enzyme production
2. malnutrition potential
what does decreased endocrine function lead to?
hyperglycemia and diabetes
what are the manifestations of chronic pancreatitis?
1. upper abdominal pain (radiating to the back, worse after eating, or drinking alcohol)
2. N/V
3. weight loss
4. pale or clay colored stools
5. steatorrhea
6. ascites
7. elevated amylase and lipase
8. elevated alkaline phosphatase (ALP)
9. elevated bilirubin
what should we keep in mind with chronic pancreatitis and elevated amylase and lipase levels?
recognize that chronic could NOT have increased amylase and lipase over time
what is included in the patient care emphasis for chronic pancreatitis?
1. nutritional support
2. blood glucose control (DMII, type 3C diabetes)
3. pain control
4. prevention of exacerbations
5. risk of pancreatic cancer
what is included in the nutritional support for chronic pancreatitis?
1. high calorie, high protein, high complex carb
2. low fat (some healthy fat if tolerated - avocados, olives, nuts)
3. possible TPN or J tube for enteral feeding
4. pancreatic enzyme replacement
5. hydration maintenance
what is type 3C diabetes?
beta cells and alpha cell dysfunction (risk for increased and decreased BG)
what is a whipple procedure?
pancreaticodueodenectomy in order to restore bile flow from the liver
what is included in the routine post-op care for a whipple procedure?
1. assess VS, UOP, e-lytes
2. hydration
3. pulmonary care
4. DVT prevention
5. pain control
6. blood glucose and insulin therapy
7. possible NGT
what is included in NGT care if indicated?
1. rest and decompress, remove gastric acid
2. a DO NOT MANIPULATE NGT sign needs to be placed above the patient's bed
3. if the patient removes the tube, the nurse CAN NOT replace the NGT and a member of the surgical team needs to be notified
what is included in the assessment findings associated with exocrine insufficiency?
1. abdominal pain
2. gas
3. bloating
4. change in bowel habits
5. fatty stool (pale, oily, floats, foul-smelling)
what is included in the management for exocrine insufficiency?
1. high calorie, protein, complex carb diet
2. some healthy fat if tolerated
3. lack of fat soluble vitamin concern (supplement)
4. enzyme replacement (PERT)
what fat soluble vitamins should be supplemented?
1. vit A
2. vit D
3. vit E
4. vit K
what are the functions of vit A?
1. vision
2. reproduction
3. bone health
4. immune system
5. skin
what are the functions of vit D?
1. bones
2. calcium absorb
3. immune system
what are the functions of vit E?
1. immunity
2. flushes toxins
what are the functions of vit K?
1. blood clotting
2. bone health
what are the nursing implications for pancreatic enzyme replacement therapy (PERT)?
1. take with meals, snacks, milky drinks (after a few bites, not after the meal is over)
2. swallow capsules whole with sips of a drink (cold drinks, not hot drinks)
3. do not chew capsules (could cause mouth ulcers)
4. taking > 1 or meal lasts for > 20 min (spread out)
5. if you forget, just take the usual dose with the next meal
6. do not store in a hot place
7. do not take with a splash of milk, fruit squashes, fizzy drinks, alcohol drinks, small amount of fruits, dried fruit, small amount of veggies, sugary sweets)
what are the exceptions in which one can take the enzyme with?
1. bananas and avocados
2. potatoes, beans, and lentils
what GI issues are people post-whipple procedure at risk for?
1. gastroparesis
2. dumping syndrome
what are the manifestations of gastroparesis?
1. N/V
2. bloating
3. cramping
4. unpredictable BG
what is included in the patient care for gastroparesis?
1. small, more frequent meals
2. chew food thoroughly
3. well-cooked fruits and vegetables
4. avoid fibrous fruits and vegetables
5. mostly low-fat foods
6. hydrate well
7. walk after meal
8. avoid lying down for 2 hours
9. metoclopramide (Reglan)
what are the manifestations of dumping syndrome?
1. N/V
2. cramping
3. bloating
4. unpredictable BG
5. signs of fluid shift (tachycardia, dizziness)
what is included in the patient care for dumping syndrome?
1. smaller, more frequent meals
2. increase protein and complex carbs
3. increase fiber
4. fat as tolerated
5. fluids between meals (not with meals)
6. limit sugar and dairy
7. rest after a meal
8. octreotide (Sandostatin)
what is used to measure the severity of alcohol withdrawal?
CIWA
if the patient receives a score of 0-7, how often must we assess?
q8h
if the patient receives a score of 8-14, how often must we assess?
q1h
if the patient receives a score of 15 or greater, how often must we assess?
q30m
what precautions must we place the patient in alcohol withdrawal on?
seizure and aspiration precautions
what are the medications used for primary treatment for alcohol withdrawal?
1. lorazepam (Ativan)
2. phenobarbital IV - MUST be in the ICU
3. dexmedetomidine (Precedex) infusion - MUST be in the ICU
4. midazolam (Versed) infusion - MUST be in the ICU and intubated
how can we give Ativan?
1. 2-4 mg IV or IM (if no IV access)
2. dosing based on CIWA score
what should we monitor for with Ativan?
1. BP (hold if less than 90 SBP or 60 HR)
2. RR (hold if less than 10 bpm)
3. SpO2 (hold if less than 92 or with a change in LOC)
4. potential for RESPIRATORY DEPRESSION
what are the adjunctive medications that we give along with benzos?
1. clonidine (Catapres) PO - central acting alpha 1 agonist that shuts down the SNS
2. metoprolol (Lopressor) IV PRN
3. haloperidol (Haldol) IM PRN for delirium - antipsychotic
what do we want the BP to look like before giving Catapres?
SBP > 100 or DBP > 100
what should we monitor for with Catapres?
hold if SBP < 100 or HR < 60
what do we want the BP to look like before giving Lopressor?
SBP > 100 or DBP > 100
what should we monitor for with Lopressor?
hold if SBP < 100 or HR < 60
what are the considerations when giving Haldol?
1. obtain a baseline ECG
2. avoid use with prolonged QT interval
what are the nutritional considerations with alcohol withdrawal?
1. thiamine (vitamin B1) PO or IV
2. folic acid (Folvite) PO or IV
3. multivitamin PO