prosthetics componentry
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
k-code levels
functional level 0: no ability to transfer w/ or w/o assistance
functional level 1: ability/potential to use prosthesis to transfer/ambulation on level surface at fixed cadence
functional level 2: ability/potential for ambulation w/ low level barriers like curbs, stairs, or uneven surfaces…typical limited community ambulator
functional level 3: ability/potential to ambulate w/ variable cadence & handle most environmental barriers…community ambulator
functional level 4: ability/potential for prosthetic ambulation that exceeds basic ambulation, exhibiting high impact, stress, or energy levels…typical for children, active adults, or athletes
what is a check socket and when would you see it?
-clear socket used to evaluate fit of prosthesis & assist in determining pressure points
-will not see outside of prosthesis office
what is the socket?
part that attaches to residual limb & places GRF back into the body
what is the rotator?
-a prosthesis will not always have this
-locks in a degree to prep for walking or decrease pull of weight when in downward position
-ex: 6’5 individual who needs to turn leg to sit comfortably on a plane
what is a pylon?
pipe that connects lower parts
endoskeletal vs exoskeletal
endoskeletal —> provides internal support through pylon & has interchangeable parts…beneficial bc it’s lighter for energy expenditure & can cover for cosmesis
exoskeletal —> will rarely seen
if a pt. has had their prosthesis for over a decade, should you change it?
no! unless pt. has requested
what is the interface of a prosthesis?
the fabric against the skin
what is the suspension of a prosthesis?
method of securing prosthetic limb to RL
*if you can connect the interface to the suspension, this is ideal
function of prosthetic sock?
-for skin protection & volume mgmt.
-nylon sock —> sweat wicking
purpose of prosthetic foam?
-barrier b/t socket & skin
-made to shape & size of pt
sleeve vs liner
sleeve: outside of socket
liner: inside socket against skin
what is the importance of correct socket design?
plays a role into how GRF are transmitted out of prosthesis back into the body
will transtibial socket designs tend to have patellar tendon bearing (PTB) bars or total surface bearing (TSB) bar?
-all will most likely have PTB…which allows more release of pressure in areas
-TSB is more rounded…more comfortable to not put high forces on certain areas
supracondylar (SC) vs supracondylar suprapatellar (SCSP)
SC: trimline above condoles where you will see impressions on medial side
SCSP: patella is covered, offering med./lat. support w/ a little bit of flexion block…will not see on its own
*both are used w/ short RL *& med./lat. ligament instability
quadrilateral brim (transfemoral design)
rectangular design where the pelvis sits on top
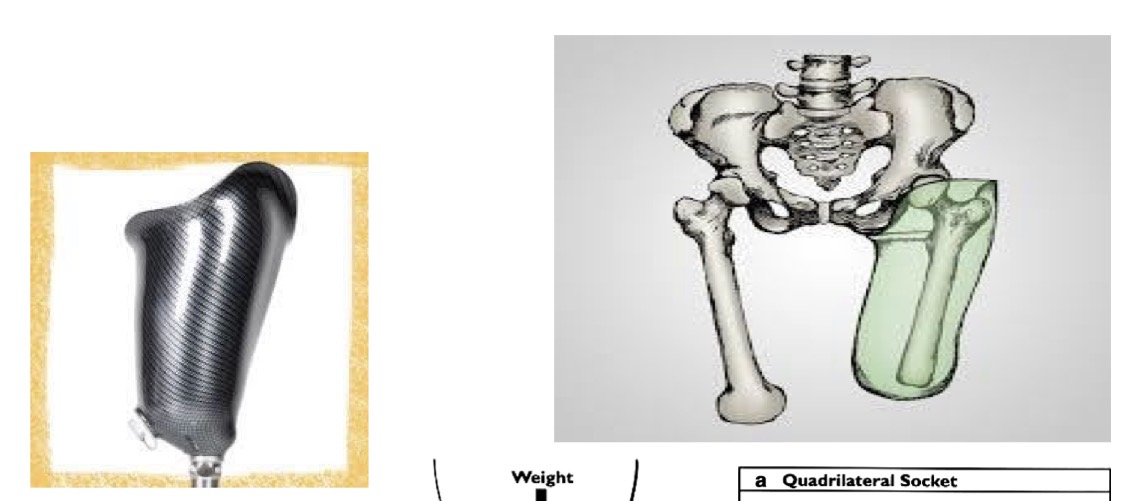
comfort flex socket (transfemoral design)
-custom made to pt
-can beep laced in quad socket
-can cut out “window” for pressure release/re-enforcement

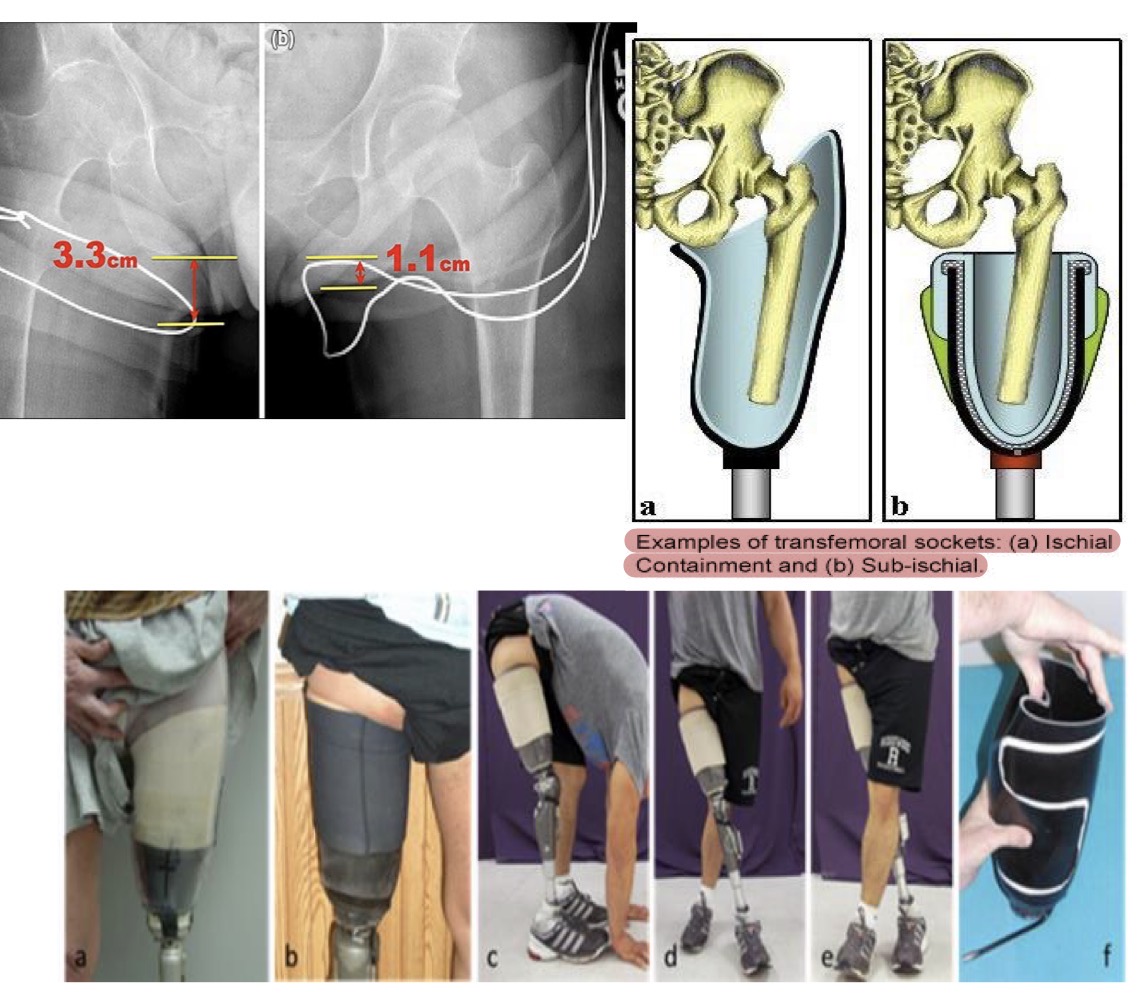
ischial containment (transfemroal design)
-ischium is contained within socket…gives control d/t contact
-can place a flexible brim for comfort…”comfort flex socket”
sub ischial socket (transfemoral design)
-pt needs adequate hip strength for this since there is not bony block
-need long enough RL to be suspended
-if less than 50% of femur, this is not a good idea
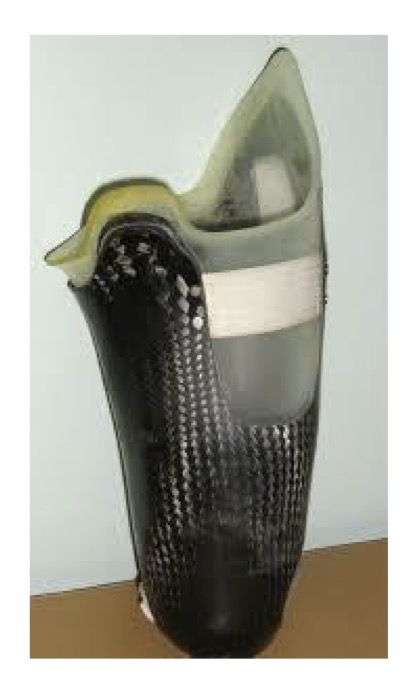
marlo anatomical socket (M.A.S) (transfemoral design)
-grabs ischial tub. & pelvic ramus to create bony block for control
-good for s/o w/ short RL but needs med./lat. control since it makes greater connection w/ pelvis
‘socketless’ & strut style socket (transfemoral design)
-good but pt does not normally keep for long since it does not distribute forces well and needs to be really tight to stay on

pros & cons of socketless systems
pros: adjustable & reduces heat
cons: mvt. b/t limb & socket, pistoning, rotation, inability for prosthetist to adjust
sub-ischial w/ flexible intersocket (transfemoral deisgn)
good if pt has significant flexion contracture

what are the transtibial suspension straps?
-supracondylar strap
-hip belt w/ y-strap
-velcro strap @ proximal sleeve
supracondylar strap
-goes above condoles
-not ideal for s/o with poor circulation

hip belt w/ y-strap
-common w/ IPOP
-not very effective d/t pistoning issues

velcro strap @ proximal sleeve
-used w/ children & small circumference of thighs
transfemoral suspension belt
-good as secondary suspension for runnner
-don under underwear
3 types of transfemoral suspension braces
-TES belt
-silesian belt
-pelvis belt w/ hip joint
-TES belt —> comes around socket & over contralat. iliac crest…good for those who have decreased abd. strength and decreased ability to control add…good for short RL
-silesian belt —> more intimidate fit, has clothe & velcro w/ D-ring going over contralat. iliac crest
-pelvis belt w/ hip jt. —> circumferential pressure to pelvic fossa, adds lat. hip stability for trendeleberg gait and short RLs…cumbersome
what is the most common below knee suspension?
the below knee locking suspension system
-imp. to ensure pins are correctly aligned
what can be an issue with an above knee locking suspension for a pt who has a longer RL?
-it will make it very hard to nearly impossible to maintain alignment
what are lanyard suspensions and KISS straps most often used for?
transfemoral prostheses
what are some benefits of the above knee lanyard suspensions?
-allows for shrinkage
-easy to done & secure
*note: does not have as much rotation as a pin lock
what’s the most common: suction ring suspension (creates seal on socket) or suction suspension (creates a suction seal)
suction ring is most common
however
suction suspension is good if pt wears a liner a lot
what is the only type of prostheses that direct skin suction used on?
transfemoral prostheses
what population are good candidates for the above knee total suction?
-very elite!
-very few can tolerate
purpose of vacuum pin?
-reduce pistoning & promotes security
-reduces friction
-helps manage RL’s swelling
-easy to use
below knee vac-pin suspension
-combo of pin & suction
-pro: eliminates all pistoning & secure
-con: reduces knee flexion
what should you be caution of when using a below knee elevated vacuum suspension?
getting air inside liner bc it can lead to blisters
what is important to note when using joints & corsets
prolonged use leads to quad atrophy
when are joints & corsets used?
with transtibial protheses for short RLs or severe ligamentous instability
BOA system
-for below & above knee
-can be secondary system
-twist dial to tighten
K codes apply to what body parts
feet & knee
K1 foot types
-S.A.C.H
-single axis
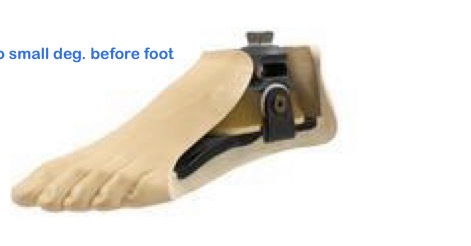
K2 foot types
-flexible keel
-multiaxial
-single axis
-S.A.C.H
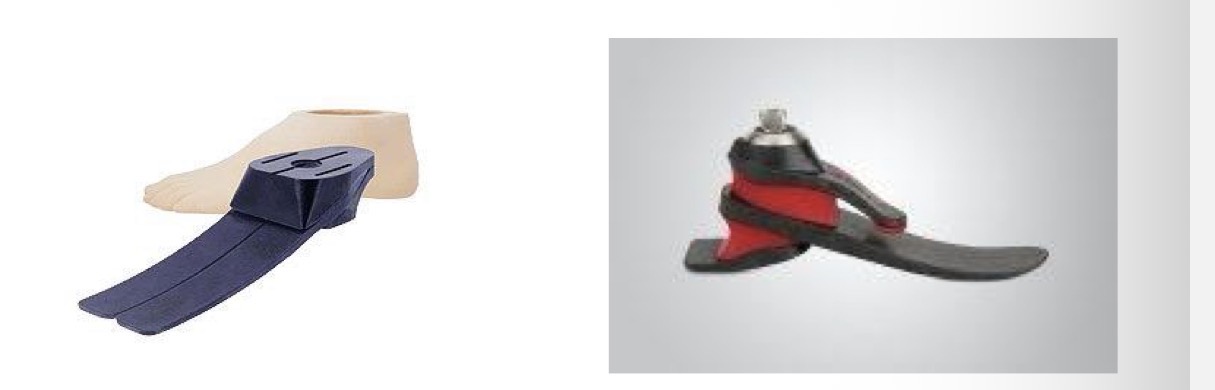
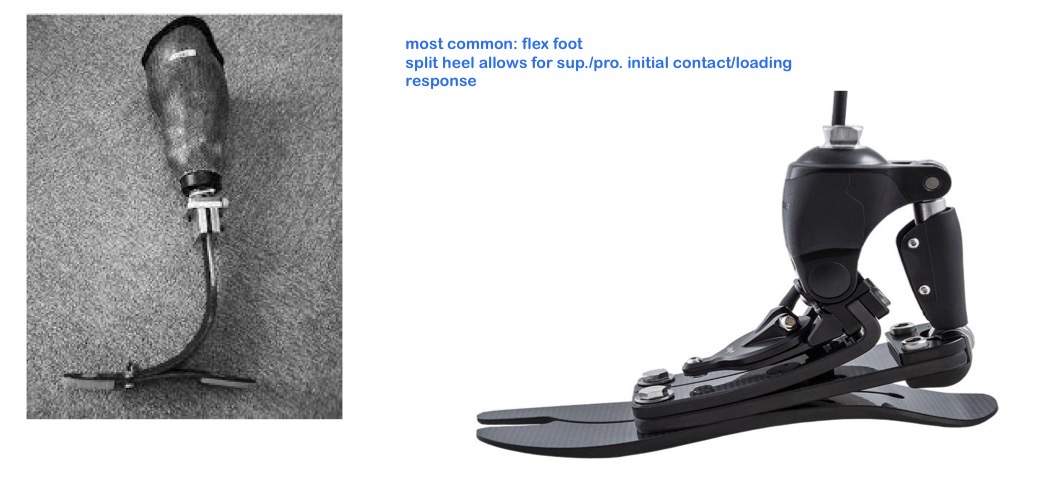
K3 foot types
-carbon feet
-microprocessor feet
K4 foot types
-all K3 feet
-running feet
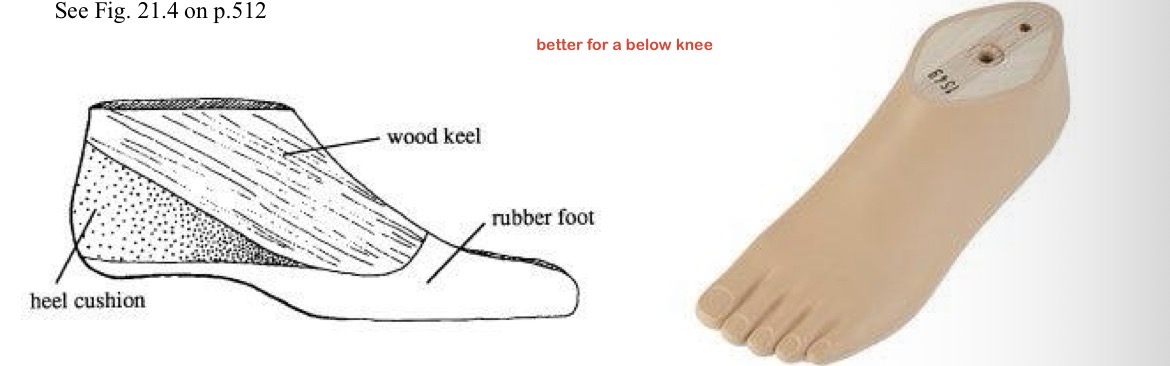
purpose of heel in prosthetic foot
-shock absorption w/ heel flexion during loading w/ TTA
-uses heel chusion/bumper/lever to achieve heel rocker in loading response
purpose of keel in prosthetic foot
-uses semi-rigid lever arm to control limb advancement in midstance replicating ankle rocker
-excessive keel ridigity/flexibility = gait disturbance
-compresses during loading & springs back during terminal —> “energy storing” forefoot rocker
S.A.C.H
-rigid combo of rubber & wood
-compressed under BW to simulate PF @ heel strike
-better for below knee
single axis
-has ankle jt w/ DF & PF controlled by interchangeable bumpers
-better for transfemoral
-“works like a seesaw”

flexible keel
-simulates ankle mvt. through entire length of foot w/ flexible inner keel and rubber foots heel
-lighter than multi-axial
multiaxial
-similar to single axis but uses inversion, eversion, & torsion
-good for walking on uneven surfaces but is heavy
carbon
-for energy storing or dynamic response feet
-returns energy during 3rd rocker (forefoot)
running feet K4
-specific for high activity, not for everyday walking
-set in PF
-attaches to bottom of shoe

stubbies/foreshortened prostheses
-for bilateral transfemoral amputations…will start w/ foot on bottom of socket to get use to CoM
-less energy & more stable
single axis knee
-transverse hinge for flexion & extension

multi-axial knee (polycentric)
-gives stability in stance
-appropriate for short RL or weak hip extensors
-allows longer RL to have knee axis and be more symmetrical

K1/2 knees
-non-hydraulic —> bc you have a fixed cadence
-locked
-single axis
-multi-axis
*probably a limited community ambulator
K3/4 knees
-hydraulic or pneumatic —> can vary cadence to help knee to keep up when walking fast
-single axis
-multi-axis
-swing only resistance
-swing-n-stance resistance
-microprocessor
locked knee K1-K2
-max. stability in stance

non-hydraulic knee K1/2
-lightweight
-stability is primary attribute
-extension assist
hydraulic knee K3/4
-adds resistance to motions
-mimics natural gait pattern
-adaptable & adjustable
-swing only resistance & swing and stance resistance
“knee with no hydraulics” has what kind of resistance
none!
swing only hydraulics emphasizes what muscle?
hamstrings
swing & stance hydraulics emphasizes what muscle?
quads in stance
microprocessors are better for what population?
-higher level pts.
-allows for smooth gait and rapid response to changing surfaces