STM Exam Review
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
Soft Tissue
Tissues that connect, support, or surround other structures/organs
- Muscles + Tendons + Ligaments + Fascia
- Nerves, fibrous tissues, blood vessels, synovial membrames
Microadhesions
Small areas of restriction in tissues w/ decreased ground substance + presence of fatty fibro-infiltrates
Macroadhesions
Larger areas of restricted tissue under conditions of long/large amounts of immobility
- With or Without injury/trauma
What causes microadhesions?
Decrease of ground substance + presence of fatty fibroinfiltrates
What causes macroadhesions?
Long / large amounts of immobility, with or without injury/trauma
What does ground substance provide
Tissue glide
Microtrauma
From repetitive, low-force stressors over time
- Leading to chronic overuse injuries
Macrotrauma
Single, high-force event causing immediate acute injury
Fascia
Soft tissue, continuous 3D matrix of structural support
- Dynamic sensory network
- Supports everything in body
- Superficial + Deep
Superficial Fascia
Houses superficial vessels (blood, nerves, lymph)
Deep Fascia
Envelops all muscle in body
- Fxn is to transmit muscular forces at a distance
What does fascia transmit/transfer?
FORCE
Does fascia have a sensory component?
YES -- DYNAMIC SENSORY NETWORK
- Muscle spindles activate when fascia is stretched --> Inform CNS
- Allows smooth and safe movement
Normal Healing
LINEAR WITH DISTINCT END POINT
- Local response (inflammation, fibroblasts, maturation)
- Decreased mobility due to space reduction
Effects of Immobilization
1. Loss of ground subtance
2. Fibrofatty infiltrates --> MACROADHESIONS
Both contribute to microadhesions
Injury/Trauma + Immobilization
- Macroadhesions (shortens tissues, decreases play, restricts ROM)
- Homogenous change in entire fabric (shrinking)
Cyclical --> Continues if irritant is present
Fibrosis
Too much healing --> Limits mobility, elasticity, force transmission
STM Mechanical Model
Tissue deformation changes soft tissue
- Changes to hyaluronic acid --> Decreased ground substance
- Decrease ECM space
- Inflammation response
- Compensations
STM Neurological Model (Dermoneuromodulation)
Changes in soft tissue are primarily due to NS
- NOT from reshaping tissue
- Stimulation of muscle spindles + GTOs --> NS Modulation
- Reduction in activation (relax)
STM Biotensegrity Model
Change in tension anywhere is instantly signaled everywhere in body
- Muscles dynamically adjust as fascia distributes force
- Spine = Tensegrity tower --> Integrates w/ system
Current thought as to why STM is effective
ALL THREE MODELS PLAY A ROLE
How to assess tissue play
Perpendicular Formation
How to assess tone
Strumming
FABQ
Fear Avoidance Beliefs Questionnaire
What is the importance of outcome measures such as FABQ?
Yellow flags can influence outcome of PT, must address!
CPG - Category A
Strong Evidence that STM is beneficial for:
1. Hip OA
2. Lateral Ankle Sprain (recurrent)
3. Plantar Fasciitis
CPG - Category B
Moderate Evidence that STM is beneficial for:
1. Acute LBP (< 3 months)
2. Chronic Neck Pain
3. Patellofemormal Pain Syndrome
STM Indications
- Loss of mobility and ROM
- Scar tissue + tissue adhesions
- Play and Tone distruptions
- Poor quality of movement
STM Contraindications
- Active infection
- Acute circulatory disorders
- Systemic infection (cellulitis)
- Obstructive edema
- Acute RA
- Broken skin / open wound
- Hematoma
- Healing fx
- Cancer
- Skin conditions
- Anti-coagulants
STM Precautions
- Psycosocial yellow flags (anxiety, pain catastrophizing, fear)
- Pregnant
- Hypersensitive
- Hyper/hypotension
- Acute/inflammatory stage of healing
Trigger Point
Localized area of increased sensitivity in tight area
- Taut, local pain, restricted ROM
Active Trigger Point
Spontaneously painful, pain at rest
- Specific referred pain patterns
Latent Trigger Point
Pain only on compression
Trigger Point - Signs + Symptoms
- Tightness
- Local pain
- Asymmetries
- Decreased ROM
- Muscle weakness
What is the most effective treatment for trigger points?
Sustained Pressure ~ 10-100 seconds
- Aim for intensity of 4-7, start gentle
Trigger Point Treatment - Technique Options
ALL IN COMBO WITH EXERCISE / STRETCHING
- Sustained pressure
- Small kneading strokes (friction)
- Parallel strokes (know direction of fibers)
- Pinching compression
- Dry needling
Trigger Point Treatment - Duration
10 - 100 seconds
Trigger Point Treatment - Intensity
4-7 on pain scale
- Start gentle
- Augmentation techniques to make less aggressive
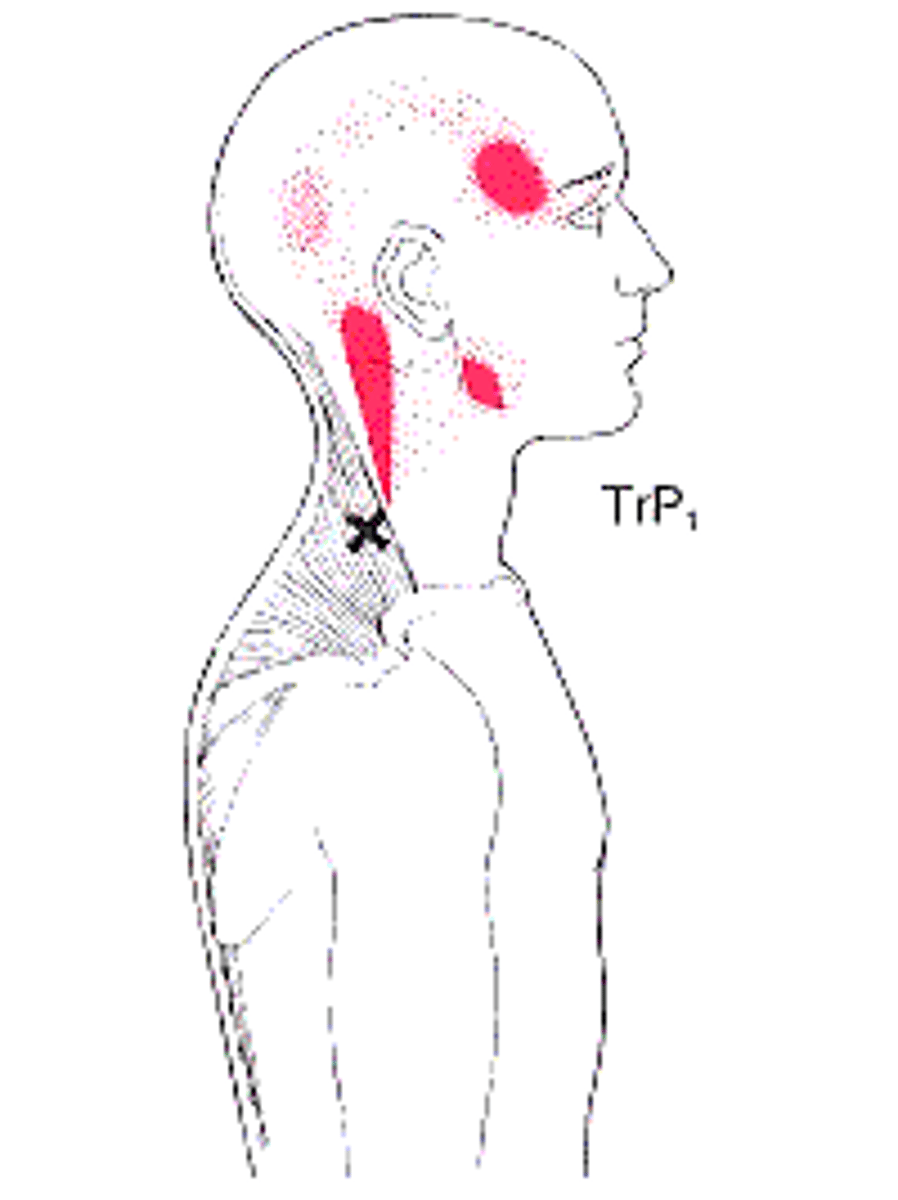
Upper Trap - Muscle Referral Pattern
RAM'S HORN
Psoas - Muscle Referral Pattern
LBP
- L3 dermatomal pattern
Visceral Referral Pain - Characteristics
- BP changes
- Nausea
- Sweating
- Deep/inside pain (not superficial)
Fibromyalgia
Chronic Pain Syndrome; Differential dx for myofascial pain syndrome
- Sleep disturbance
- Systemic
- Psychosocial factors
- Fatigue
- dx with 18 specific points, 11/18 painful for dx
Myofascial Pain Syndrome
Chronic pain disorder affecting muscles and fascia
- Treatment goal = reduce TP irritability
- Restricted ROM + Muscle weakness
- Feeling of "knots"
How soon can you mobilize a scar?
As early as 2 weeks
- Once surgical incision is closed
How late can you mobilize a scar?
Up to 2 years
- Can still make some impact after
Acute Scar Treatment
Approximation
Scar Treatment > 2 Weeks / once scar is closed
Half circles using 2 fingers
- WITHOUT SEPARATING INCISION
- Periwound area first, then over length of scar
- Lateral pulls perpendicular to scar
Scar Treatment > 4 Weeks
Cross friction
- Perpendicular to line of scar
Scars - Superficial STM Interventions
- MFR (shearing + torsion)
- Skin rolling
- Cupping
Scar Mobilization - Goals
1. Put beneficial stress through new tissue
2. Improve Sensations (sensitivity, itchiness)
3. Improve Circulation
Scar - Phases of Healing
1. Inflammatory Phase (1-10 days)
- GOAL = Protect fragile tissues
2. Proliferative Phase (3-21 days)
- Collagen guides alignment
- Capillaries bud + granulation tissue fills wound
3. Maturation Phase (7 days - 2 years)
- Remodeling! Fiber reorganization + scar contraction
- Load progressively
- Pale, flat, pliable
What do you pair with self myofasical release (MFR)?
Stretching
Theragun Surface Area
Smaller = MORE INTENSE
Larger = LESS INTENSE
Myofascial Meridians - Treatment Benefits
Can impact a sensitive area by manipulating elsewhere
Regional Interdependence
Point of restriction may be away from point of pain
How do you put tension on the superficial back line?
Downward Dog position
What physical activity loads the functional line?
Cross-body rotational movements
- Throwing
Deep Frontal Line - Function
Myofascial Core; Provides stability + Position changes to core structure
- Lifts inner arch of foot
- Stabilizes legs, pelvic floor, chest
- Supports lumbar spine from front
- Balances neck and head
Deep Frontal Line Dysfunction
Causes fxnl restriction over time which may appear elsewhere
- NOT acute change, but chronic
Proximal stability = Distal mobility
MFR Progression
External to internal
1. Manual application
2. Myofascial Rebounding
3. Myofascial Unwinding
What happens when you increase the instrument angle during IASTM?
Increased angle = Increased intensity
IASTM - Indications
- Limited motion
- Pain during motion
- Motor dysfunction (poor patterns)
- Lack of tissue glide
Wet vs Dry cupping
Wet = Incisions and blood
Dry = No incisions / blood
What cupping technique is used when working with a new patient?
Stationary Cupping
What cupping technique can be stimulating?
Fast moving cupping
Cupping - Treatment Time
3-5 minutes
Cupping - Treatment Intensity
< 7/10
- Start with 1-2 pumps
Cupping - Indications
- Decreased ROM / flexibility
- Inflammation
- Pain
- Headaches
- TPs
- Poor scar healing
Cupping - Goals
- Improve circulation
- Alleviate adhesions
- Clear congestion + stagnation
- Lift, rehydrate, manipulate fascia
- Neovascularization
- Reduce pain by alleviating pressure on sensory organs
Cupping - Contraindications
- Dry / Cracked skin
- Contagious skin condition
- Open wound
- Compromised joints
- Over umbilicus
- Bleeding disorders
- Anemia
- Muscle dystrophy
- Excessive swelling
- DVT
- Varicose veins
- NEW tattoos
Lymphedema - What happens to transport capacity?
Transport Capacity is REDUCED
- Lymph load remains normal
What happens to osmotic pressure with increased altitude?
INCREASES
- Pushes fluid out --> EDEMA
- Wear compression on airplane
What causes dynamic insufficiency (edema)?
- CHF
- Chronic venous insufficiency
- Immobility
- Pregnancy
- Pressure from tight jewlery, bandages, garments (tourniquet effect)
What is strictly contraindicated with edema caused by cardiac insufficiency?
Compression therapy and manual lymphatic drainage
Lymphedema - Exam Findings
- Chronic swelling
- Localized pain / "heaviness"
- Atrophic skin changes
- Secondary Infections (cellulitis, lymphangitis, erysipelas)
Cellulitis
Acute infection of skin and deep tissues
- May be life threatening
Lymphangitis
Infection of lymphatic vessels
- Often results from cellulitis
- May be life threatening
Erysipelas
Acute dermal infection impacting skin + subq tissues
- Includes lymph vessels + nodes
What typically causes primary lymphedema?
Congenital malformations
- Hypoplasia (most common; less lymph vessels)
- Hyperplasia (larger than normal lymph vessels)
- Aplasia (absence of lymph vessels
Lymphedema - Stages
Stage 0 (Latency) = No Signs/Symptoms, cannot see or measure
- Patient education
- Automatic after surgery
Stage 1 (Reversible) = Edema only, visible swelling
- Soft + pitting
- Reduce w/ elevation overnight
Stage 2 (Spontaneously Irreversible) = Fibrosis
- Constant pressurw to break up fibrotic tissue over time
- Must wear garments, complete decongestive therapy
- Positive stemmer's sign
Stage 3 = Lymphostatic Elephantiasis = Skin Changes + Increased Vol.
- Papillomas
- Positive stemmer's
- Frequent infections
What dictates lymphedema stage?
Tissue quality, NOT size
Lymphedema Diagnosis - Gold Standard
Lymphoscintigraphy (LAS)
- Maps lymphatic system
Stage 0 Lymphedema - Priority
Patient education
Stage 1 Lymphedema - Priority
Reverse to latency stage via elevation overnight
Stage 2 Lymphedema - Priority
Constant pressure to break up fibrotic tissue over time
Stage 3 Lymphedema - Priority
Prevent further infection, reduce size + tissue hardening
When do you see a positive stemmer's sign?
Lymphedema Stages 2 + 3
- Skin cannot be lifted on dorsum of toe
What procedure is recommended for measuring a lymphedema pt's limb?
Circumferential
- Taken in intervals of 4-6 cm along extremity
- Summing measurements
- Volumetric is more cumbersome
Lymphedema - Augmentation Techniques
- Deep abdominal technique
- Diaphragmatic breathing (at least 10x am and 10x pm)
- Decongestive exercises
Short Stretch Bandaging
Used to manage lymphedema
- Maintain decongestive affect achieved from MLD session
- Prevent re-accumulation of fluid into tissues
Exercise for patients in complete decongestive therapy (CDT)
Light exercise progressing appropriately
- Encourages movement of lymph fluid out of limb
Where is the highest density region for lymph nodes in the body?
Abdominal Region
Which kinesiotaping application is used for lymph correction / swelling?
"Fan" Strip, channeling technique
- Lifting effect on skin, decreasing pressure + facilitating fluid flow
- 10-15% tape stretch
What info does muscle play assessment give?
- Functional strength
- Flexibility
- Imbalances
- Neuromuscular control
What info does muscle tone assessment give?
Muscle's underlying tension + resting resistance to passive movement
Kinesiotaping - Proposed Effects
SKIN
- Decrease painful, abnormal sensations
MUSCLE
- Assists or inhibits function
JOINT
- Improves alignment + proprioception
LYMPHATIC
- Facilitates local circulation + lymphatic flow