BIOM - In semester (weak areas)
1/84
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
85 Terms
Golgi Apparatus
Modifies, sorts, and packages proteins and lipids for transport to different parts of the cell or for secretion outside the cell.
Lysosomes and peroxisomes
Membrane bound organelles
Lysosomes:
Break down of organic material inside the cells
Peroxisomes:
Degrade toxic molecules inside the cell
What molecules can penetrate and not through the plasma membrane
Penetrating molecules:
Gases (O2 & CO2)
Water
Ethanol
Non-penetrating molecules
Ions
Glucose & proteins
Difference between simple and facilitated diffusion
Simple diffusion:
Where small molecules move directly through the cell membrane (O2, CO2)
Facilitated diffusion:
Molecules move from high to low, however uses the help of proteins such as channel and carrier proteins.
Osmosis
Diffusion of water across a partially permeable membrane.
Isotonic solution - No net movement of water (does not change shape)
Hypotonic solution - water moves into the cell, lower solute concentration outside of the cell (cell will swell)
Hypertonic solution - Water moves out of the cell, higher solute concentration outside of the cell (cell will shrink)
Compare and contrast primary and secondary active transport.
Similarities
Both move substances against their concentration gradient
Both require membrane transport proteins
Both are essential for maintaining cellular homeostasis
Differences
Energy source:
Primary → Direct ATP use
Secondary → Indirect (ion gradient energy)
Protein type:
Primary → ATPase pumps
Secondary → Carrier proteins
Dependency:
Primary → Independent
Secondary → Relies on primary transport
Examples:
Primary → Na⁺/K⁺ pump
Secondary → Na⁺–glucose symporter
Myelination
Myelin protects and electrically insulates the axon, making it increase the speed of electrical signals
Created by:
Schwann cells (PNS)
Oligodendrocytes (CNS)
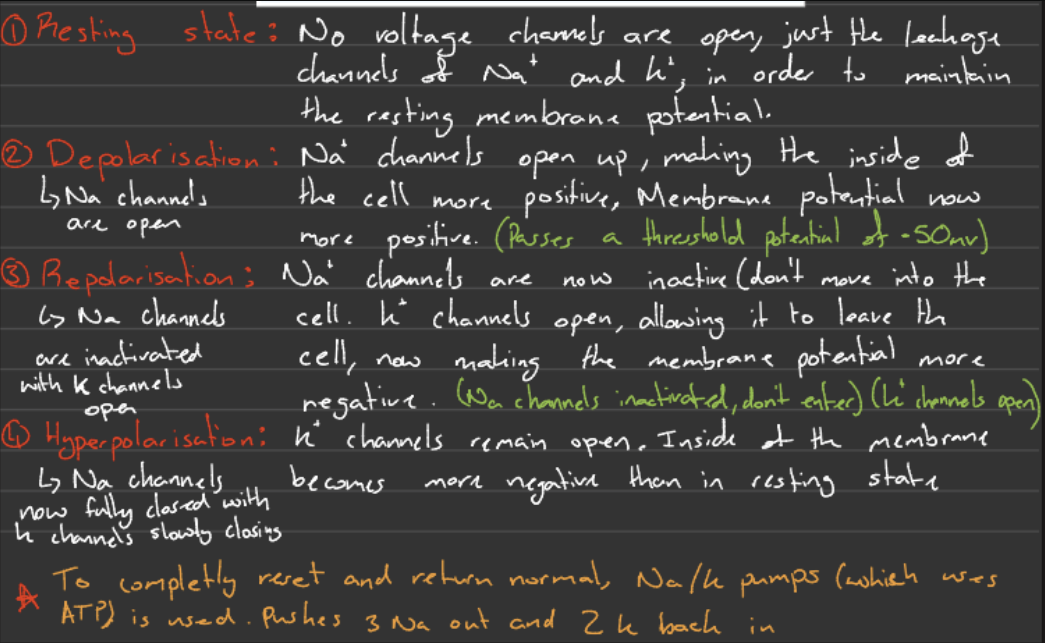
Stages of action potentials
Important:
The threshold must be reached in order for an action potential to even occur
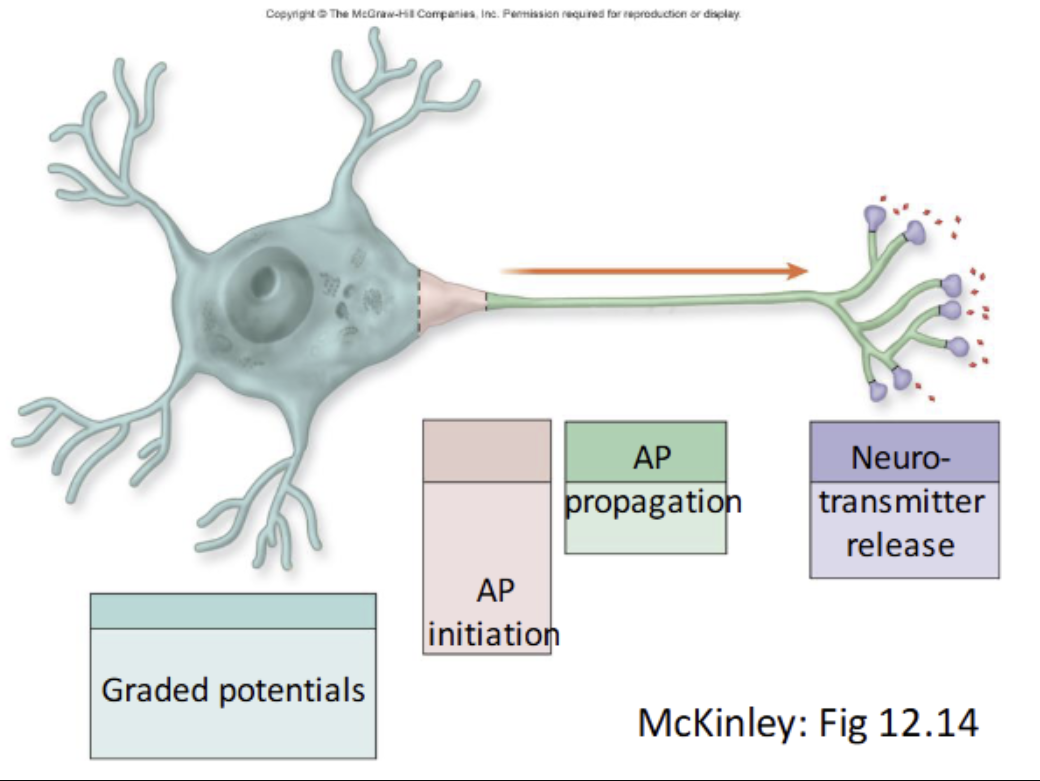
Compare and contrast graded potentials and action potentials.
Similarities
Both are changes in membrane potential
Both involve movement of Na⁺ and K⁺ ions
Both are used for neuronal communication
Differences
1. Location
Graded: dendrites & cell body
Action: axon
2. Type of channels
Graded: chemically-gated (stimulus-controlled)
Action: voltage-gated
3. Direction
Graded: spreads in multiple directions
Action: one direction along axon
4. Type of signal
Graded: can be depolarising OR hyperpolarising
Action: always follows the same pattern (depolarisation → repolarisation)
5. Distance
Graded: short, decreases with distance
Action: long, does not decrease
Compare and contrast the functions of the sympathetic and parasympathetic divisions of the autonomic nervous system (ANS).
Similarities
Both are divisions of the autonomic nervous system (ANS)
Control involuntary functions
Act on the same organs
Work together to maintain homeostasis
Differences
Role
Sympathetic: fight or flight
Parasympathetic: rest and digest
Overall effect
Sympathetic: prepares body for activity
Parasympathetic: calms and restores body
Heart rate
Sympathetic: increases
Parasympathetic: decreases
Digestion
Sympathetic: inhibits (redirects energy away from it)
Parasympathetic: stimulates
Pupils
Sympathetic: dilate
Parasympathetic: constrict
Energy use
Sympathetic: uses energy
Parasympathetic: conserves energy
Three Sympathetic preganglionic neurons
Sympathetic chain ganglia
Collateral ganglia
Adrenal medullae
Receptor that responds to ACh
Nicotinic receptors
Receptor at the ganglionic neuron
Muscarinic receptors
Receptor at all of the parasympathetic target organs
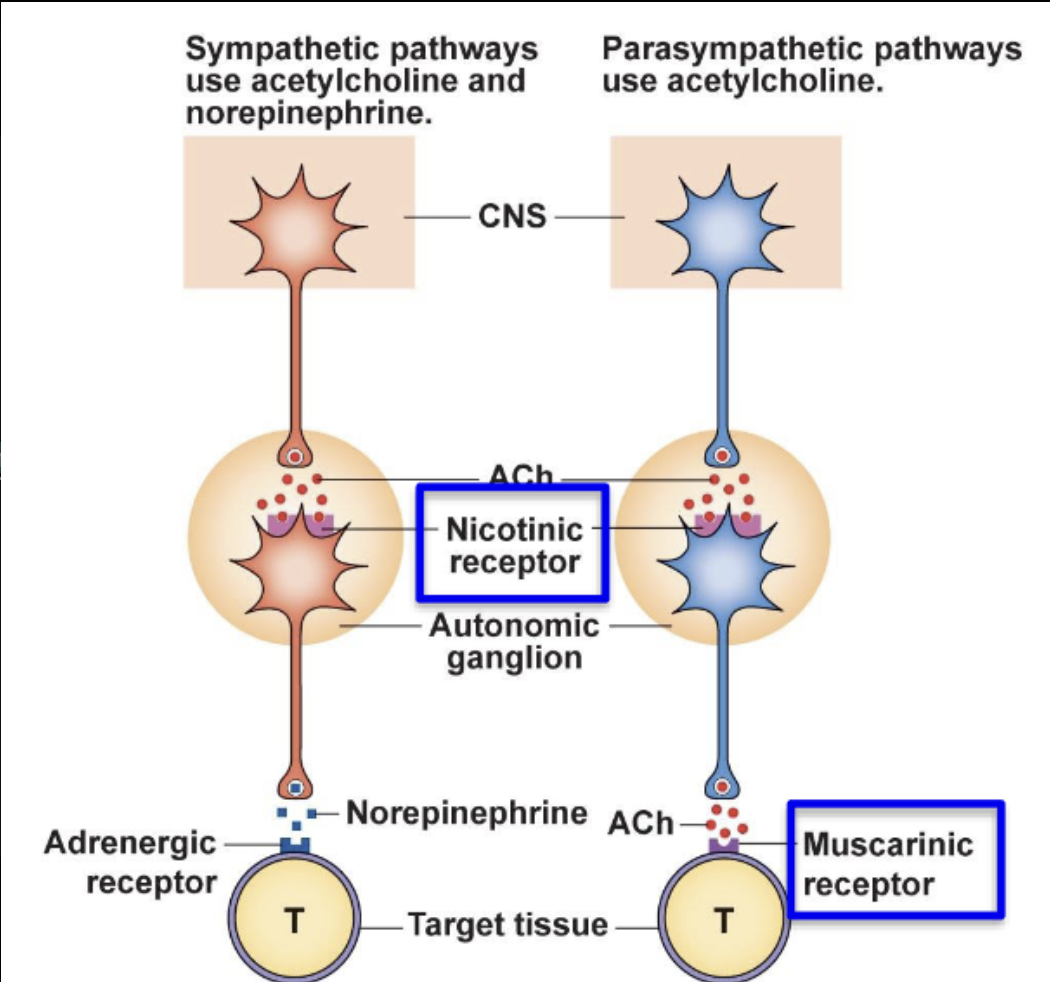
Receptor that responds to NE
Adrenergic receptors
Receptor that is found at all the sympathetic target organs
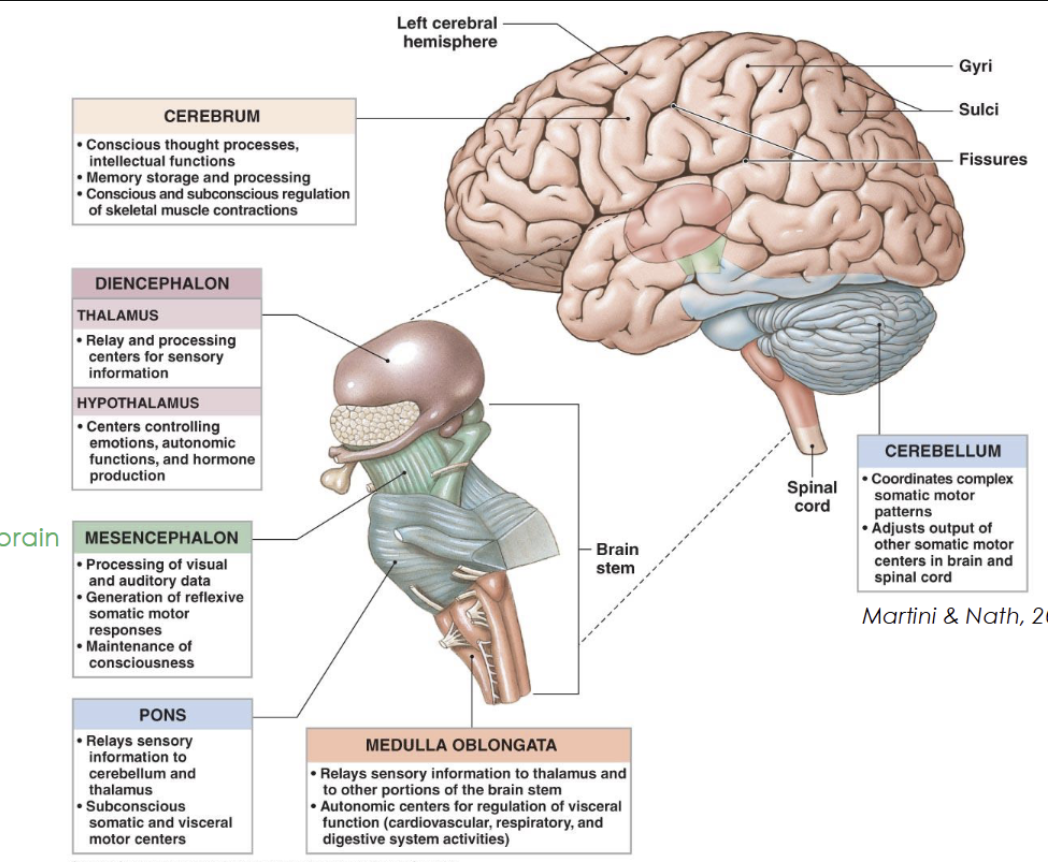
Name the various divisions/regions of the brain and their functions.
Diencephalon
Thalamus → relays sensory information to the cortex
Hypothalamus → maintains homeostasis, and regulates emotions
Epithalamus (pineal gland) → day and night cycles (melatonin produced in response to darkness)
Brainstem
Midbrain → visual and auditory reflexes
Pons → Relays signals between brain regions and regulates sleep and breathing
Medulla oblongata → Controls autonomic functions
Cerebellum
Coordinates movement, balance, and posture (works subconsciously)
Describe the structure and function of the spinal cord.
Function
Provides two-way communication (sensory info and motor commands) between brain and body
Acts as a major reflex centre (reflexes are processed in the spinal cord)
Key features
Filum terminale: anchors spinal cord to coccyx
Cauda equina: spinal nerve roots
Spinal nerves
Connect to spinal cord via two roots:
Dorsal root: sensory input
Ventral root: motor output
Functions of Cerebrospinal fluid (CSF)
Supports the brain and spinal cord (provides buoyancy)
Cushions/protects the CNS against shock and injury
Maintains a stable chemical environment for neurons
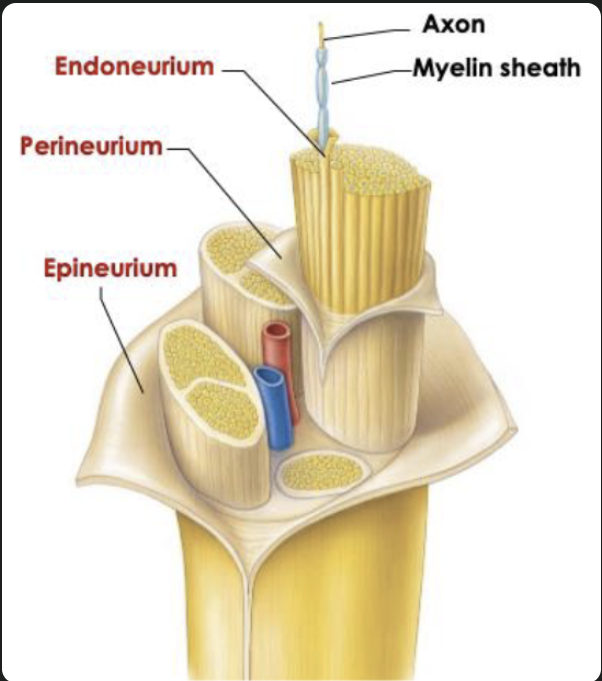
Peripheral nerve structure
It is a bundle of axons (these are composed of dendrites, axon hill, cell body, axon and myelin sheath)
Peripheral nerve structure
Endoneurium: around each axon
Perineurium: around bundles of axons
Epineurium: outer covering of whole nerve
To describe the 5 components of a reflex arc.
Receptor – site of stimulus action.
Sensory neuron (afferent) – Carries the afferent impulses to the CNS.
Integration centre – Processes the information in the spinal cord via synapses, with or without interneurons
Motor neuron (efferent) – Carries the efferent impulses from the integration centre to the effector organ.
Effector – Produces a response to the efferent impulses (e.g., muscle contracts or gland secretes).
Stimulus → Receptor → Sensory → CNS (integration centre)→ Motor → Effector → Response
Usually occurs in the spinal cord of the CNS
To understand the function of muscle spindles
Muscle spindles are sensory receptors located within skeletal muscle that monitor muscle length and the speed of stretch.
Core functions:
Detect muscle stretch
Sense changes in muscle length
Maintain muscle tone
Provide continuous feedback to the spinal cord to keep muscles slightly contracted even at rest
Enable the stretch reflex
Muscle contraction to prevent overstretching.
Pathway of stretch reflex
The stretch reflex is a fast, automatic, monosynaptic spinal reflex that resists sudden muscle stretch.
Muscle is stretched
Muscle spindle is activated
Sensory neuron (Ia afferent) sends signal to spinal cord via dorsal root
Direct synapse with alpha motor neuron at integration centre
Motor neuron activates muscle through ventral root
Muscle contracts (opposes stretch)
Key term often required:
Monosynaptic reflex (one synapse)
la afferent - a fast sensory nerve fibre that carries information from muscle spindles to the spinal cord about muscle stretch.
To differentiate between the stretch reflex and tendon reflex.
Stretch reflex
Receptor: Muscle spindle
Stimulus: Muscle is stretched (length increases)
Response: Muscle contracts
Pathway: Monosynaptic (direct sensory → motor neuron)
Function: Maintains posture and muscle tone
Example: Knee-jerk reflex
Tendon reflex (Golgi tendon reflex)
Receptor: Golgi tendon organ
Stimulus: High muscle tension (force)
Response: Muscle relaxes
Pathway: Polysynaptic (via interneuron)
Function: Prevents muscle/tendon damage
Example: Dropping a heavy weight causing muscle relaxation
Key difference
Stretch reflex = contract when stretched
Tendon reflex = relax when too much force is applied
Classifications of bones
Long bones
Longer than wide
Help with movement
Examples: femur, humerus
Short bones
Small and cube-shaped (equal length, width, and thickness)
Give stability
Examples: wrist (carpals), ankle (tarsals)
Flat bones
Thin, flat, and usually curved
Protect organs
Examples: skull, ribs, sternum
Irregular bones
Odd-shaped
Have special jobs (support/protection)
Examples: vertebrae, pelvis
Sesamoid bones
Small bones in tendons
Help reduce friction
Example: kneecap (patella)
Gross structure and key anatomical features of long bones
Compact bone: Dense outer layer
Spongy bone: Honeycomb like bone found within
Connective tissue:
Periosteum covers outside of the impact bone
Endosteum covers the inside portion
Long Bone structure:
Diaphysis: Forms long axis, tubular shaft
Epiphyses: The end of long bones, made up of compact bone and spongy bone
Metaphysis: Region between diaphysis and epiphysis and contains the growth plate
The axial skeleton
1. Cervical: 7 vertebrae
2. Thoracic: 12 vertebrae
3. Lumbar: 5 vertebrae
4. Sacrum: one bone formed from fusion of
several (5) bones, articulates with hip
5. Coccyx: fused (4) bones
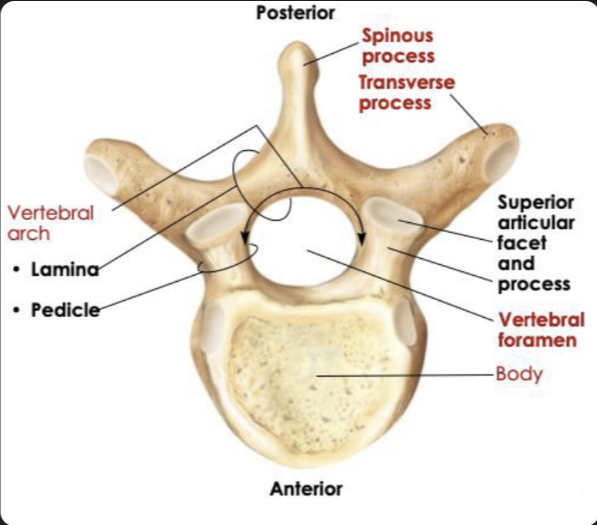
Common structure of all vertebrae
Cervical: Small oval body, large triangular vertebral foramen, small transverse process
Thoracic: Heart shaped body, smaller circular vertebral foramen, large transverse process
Lumbar: Very large, thick oval body, smaller triangular vertebral foramen but bigger than thoracic, short and flat transverse process
Joints of the vertebral column
Intervertebral discs – cushion-like pad between vertebrae that act as shock absorbers
Upper limbs
Arms: Hummeruss
Forearm: radius and ulna
Hand: carpals (8 - wrist), metacarpals (5 - palm), phalanges (14 - fingers)
Lower limbs
Thigh: Femur and patella
Leg: Tibia and Fibula
Foot: tarsals (7 - hind foot), metatarsals (5 - midfoot), phalanges (14 - toes)
Understand changes to the skeleton during development, ageing, and disease.
Bone Development
Starts as cartilage → ossifies in embryo
Long bones: ossification ~8–25 weeks
Growth continues until ~25 years
Age-Related Changes
Children: formation > resorption → growth
Young adults: formation = resorption → stable
Adults: resorption > formation → bone loss
Osteoporosis
Resorption > formation → low bone mass
Common in elderly (especially women)
Prevention: weight-bearing exercise
Functional classifications of joints (degree of movement)
Synarthrosis (none to very little movement)
Amphiarthrosis (slight movement)
Diarthrosis (freely movable)
Fibrous
bones joined by collagen fibres
No joint cavity
Synarthrosis, Amphiarthrosis
Cartilaginous
Bones joined by cartilage
No joint cavity
Synarthrosis or Amphiarthrosis
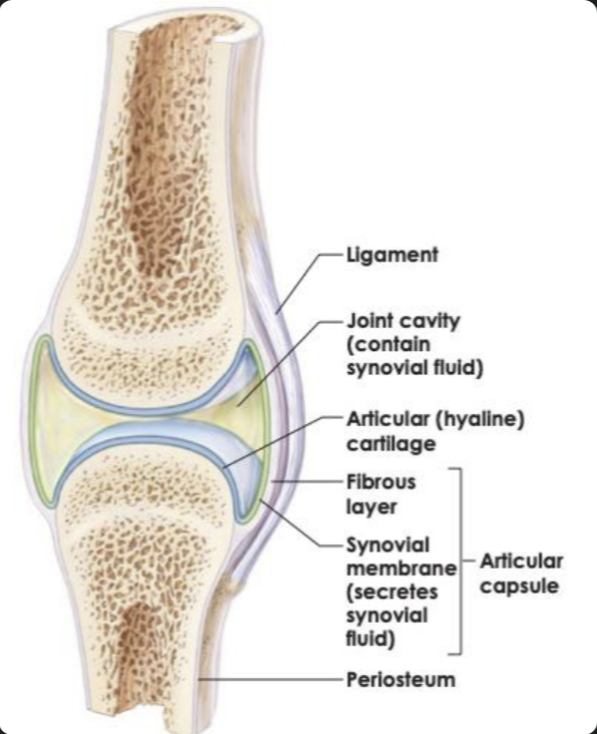
Synovial
Bones are separated by fluid filled cavity
Contains synovial fluid and a joint capsule
Diarthrosis
Synovial joint structure
Articular cartilage → reduces friction
Joint cavity → allows movement
Synovial fluid → lubrication
Joint capsule → encloses the joint
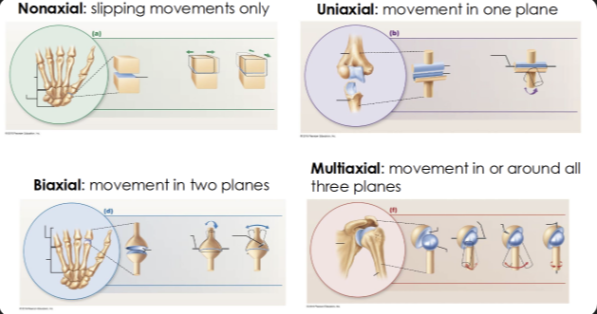
Types of range of motion
Nonaxial: intercarpal joints
Uniaxial: elbow
Biaxial: knuckle
Multiaxial: shoulder
Types of synovial joints
Plane/gliding
Hiinge
Pivot
Condylar/Saddle
Ball-and-socket
Plane/gliding
Slight movement along relatively flat surfaces
Nonaxial
Intercarpal joints
Hinge
Cylinder nests in trough
Uniaxial
Elbow
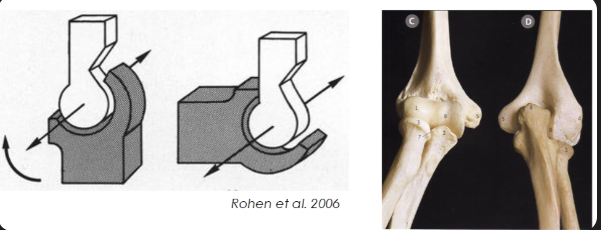
Pivot
Axle fits into a sleeve
Uniaxial
Neck
Condylar/saddle
Biaxial
Wrist (C) and base of thumb (S)

Ball and socket
Multiaxial
Shoulder
Hierarchical organisation of skeletal muscle
Muscle (organ)
Whole muscle (e.g. biceps)
Surrounded by epimysium
Fascicles (bundles)
Bundles of muscle fibres
Surrounded by perimysium
Muscle fibres (cells)
Long muscle cells
Surrounded by endomysium
Myofibrils
Tiny rods inside muscle fibres
Made of repeating units (sarcomeres)
Sarcomeres (functional unit)
The smallest working units of muscle that make it contract
3 levels of connective tissue
Epimysium: dense irregular connective tissue surrounding entire muscle
Perimysium: fibrous dense connective tissue surrounding bundles of fascicles
Endomysium: fine areolar connective tissue surrounding each muscle fiber
Different muscle architecture types
Pennate
Parallel
Circular
Parallel
Fascicles lie parallel to muscles line of action
• Strap
• Fusiform
Pennate
Fascicles at angle relative to the line of action
• Unipennate
• Bipennate
• Multipennate
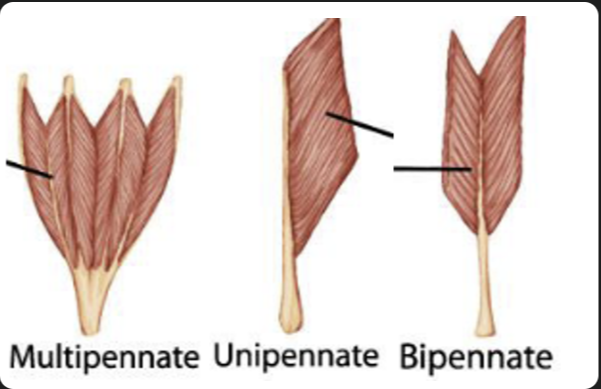
Fascicle architecture linked to function
Pennate muscles have fascicles arranged at an angle which produces a reduced range of motion, due to shorter fibre lengths. Whereas, parallel muscles have fibres running parallel to the line of pull with longer fascicles, allowing for a larger range of motion through its longer muscle fascicles.
This results in the Pennate muscles to pack a higher volume of muscle fibres, allowing for higher power (higher PCSA), but less range of motion. With the parallel muscles, its longer muscles makes it where there is less volume of it, reducing its power (lower PCSA), giving it a higher range of motion.
Physiological Cross-Sectional Area - PCSA
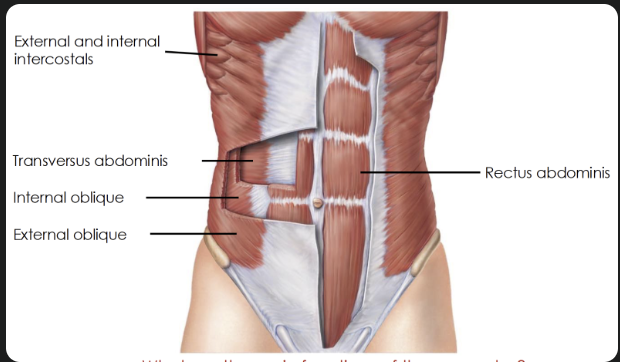
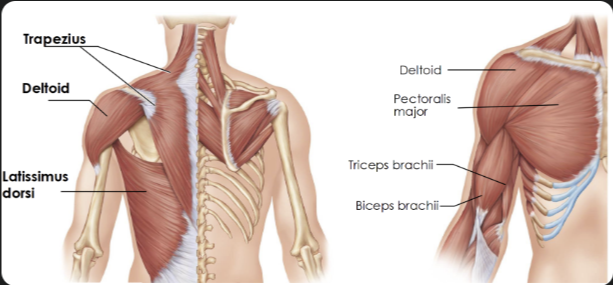
Major muscle compartments
Thorax and abdomen
Shoulder and upper arm
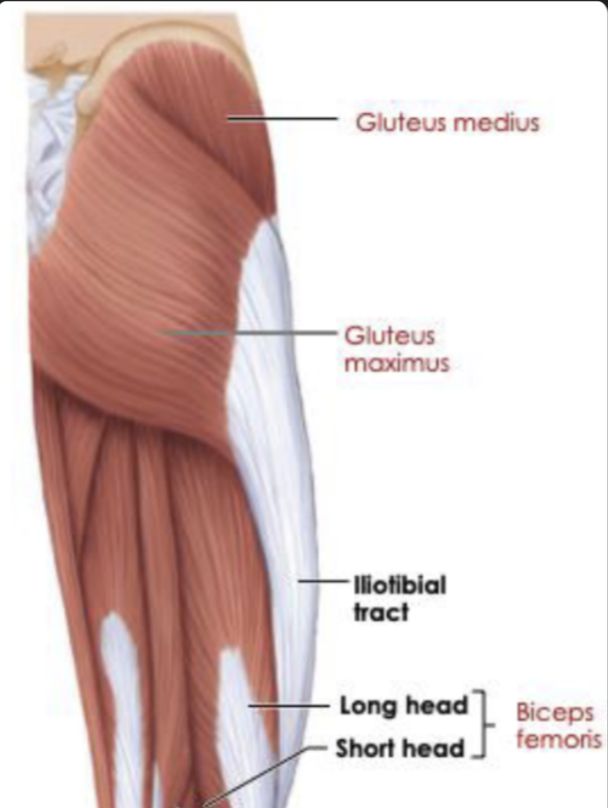
Thigh (anterior)
Thigh (posterior)
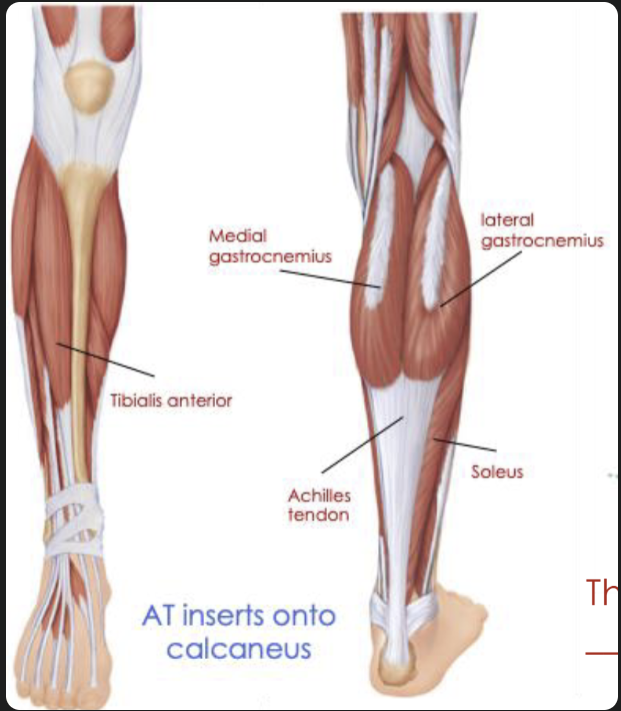
Lower leg
Thorax and abdomen
Shoulder and upper arm
Thigh anterior

Thigh posterior
Lower leg
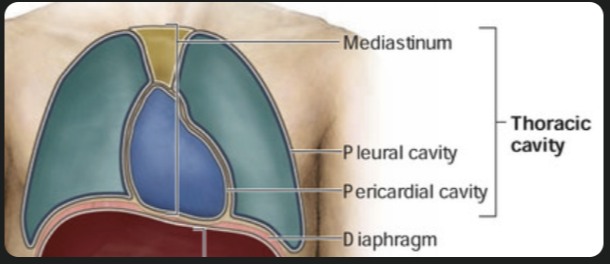
Main body Cavities
Thoracic cavity
luns, heart, trachea and esophagus
Abdominopelvic cavity
intestines, live,stomach, spleen ect
Pelvic cavity
bladder, rectum and reproductive organs
Where exactly does the heart sit
Thoracic cavity → mediastinum (central region)
Mediastinum → pericardial cavity
Pericardial cavity → heart
Structure that makes up the wall of blood vessels
1. Tunica intima (inner layer)
Endothelium (smooth epithelial lining)
Thin connective tissue layer
Function: smooth blood flow, reduces friction
2. Tunica media (middle layer)
Smooth muscle + elastic fibres
Function: controls vessel diameter (vasoconstriction/vasodilation) and blood pressureThickest in arteries
3. Tunica externa (outer layer)
Connective tissue (collagen + elastin)
May contain small blood vessels (vasa vasorum)
Function: support and anchoring
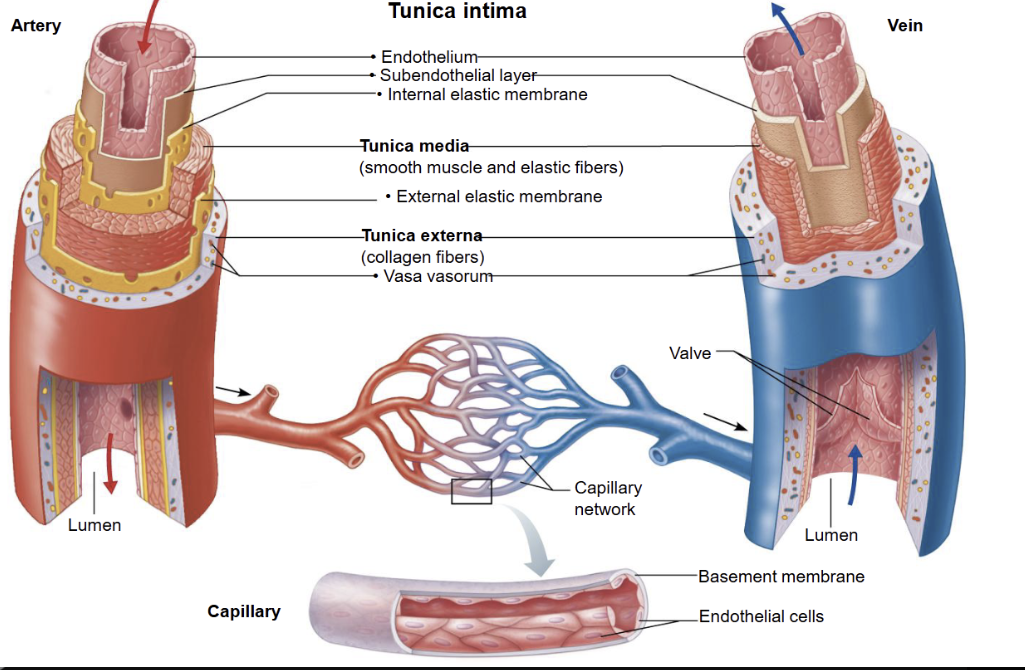
Compare arteries, veins and capillaries
It should be noted:
The pressure is high in arteries as it needs to be pumped throughout the whole body.
Wall thickness is important in arteries as it needs to withstand all that pressure, whereas in veins its doesn’t face such pressure and in capillaries it needs to be thin to allow diffusion.
Lumen affects flow speed, so in arteries it’s narrow to maintain high pressure whereas in veins its wide in order to carry large volumes of blood, and very narrow in capillaries, however due to being arranged in a large cross-sectional area it slows blood down to giving it time for exchange.
The reason valves are present in veins is to prevent backflow.
And as for function, in capillaries especially its is used to exchange gases, nutrients and wastes

How does veins transport blood
Through the use of one way valves
Skeletal muscle contractions
Respiratory pump
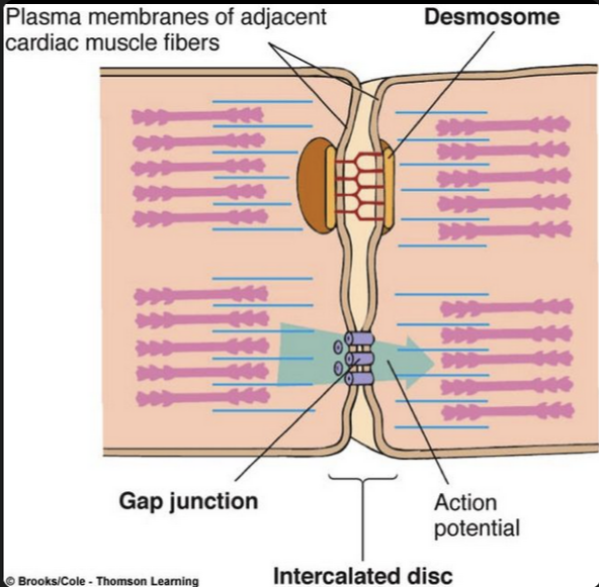
Structure of cardiac muscle its relationship to its function
Structure
Striated cells → contain proteins that cause contractions
Short, branched cells → form a connected network
Intercalated discs (join cells):
Desmosomes → hold the myocytes together
Gap junctions → allow ions & electrical signals to pass through the membrane
Cardiac cells can contract simultaneously due to rapid flow of action potentials between the cardiac myocytes
Relationship to Function
Striations → strong contractions to pump blood
Branching network → rapid spread of contraction
Desmosomes → prevent cells pulling apart during forceful beats
Gap junctions → fast electrical communication, so cells contract together
Important: Cardiac myocyte = cardiac muscle cells
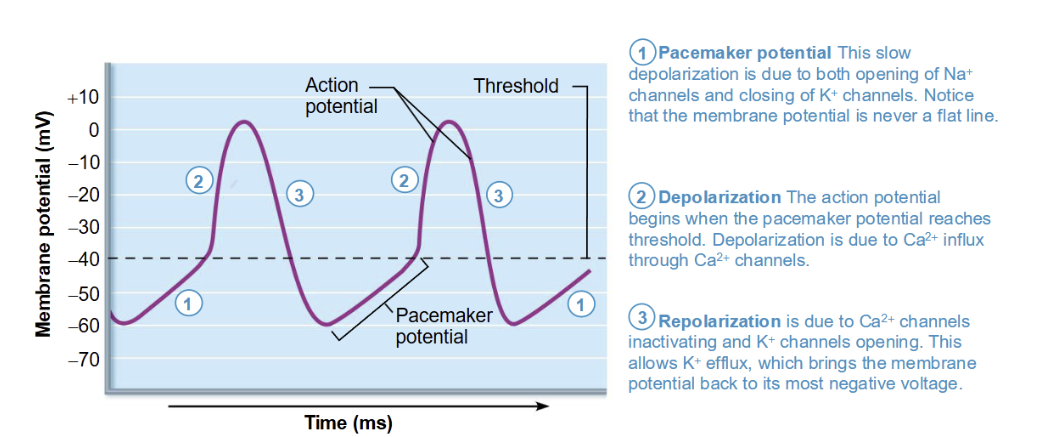
Action potentials in Cardiac Pacemaker cell
No stable resting potential
1) Leaky sodium channels (funny current), slow rise with the potassium channels closed. Pacemaker potential
2) Once threshold is achieved calcium (influx) comes in, more positive than sodium, so depolarises faster reaching the action potential
3) The repolarization of this is the calcium channels inactivating and the potassium channels opening (efflux)
This is the firing that is repeated over and over at the SA node
SA node to the AV node there is a pause of 0.1 second to allow the ventricles to fill
Function link
Generate rhythmic impulses automatically
Set heart rate and timing (natural pacemaker activity)
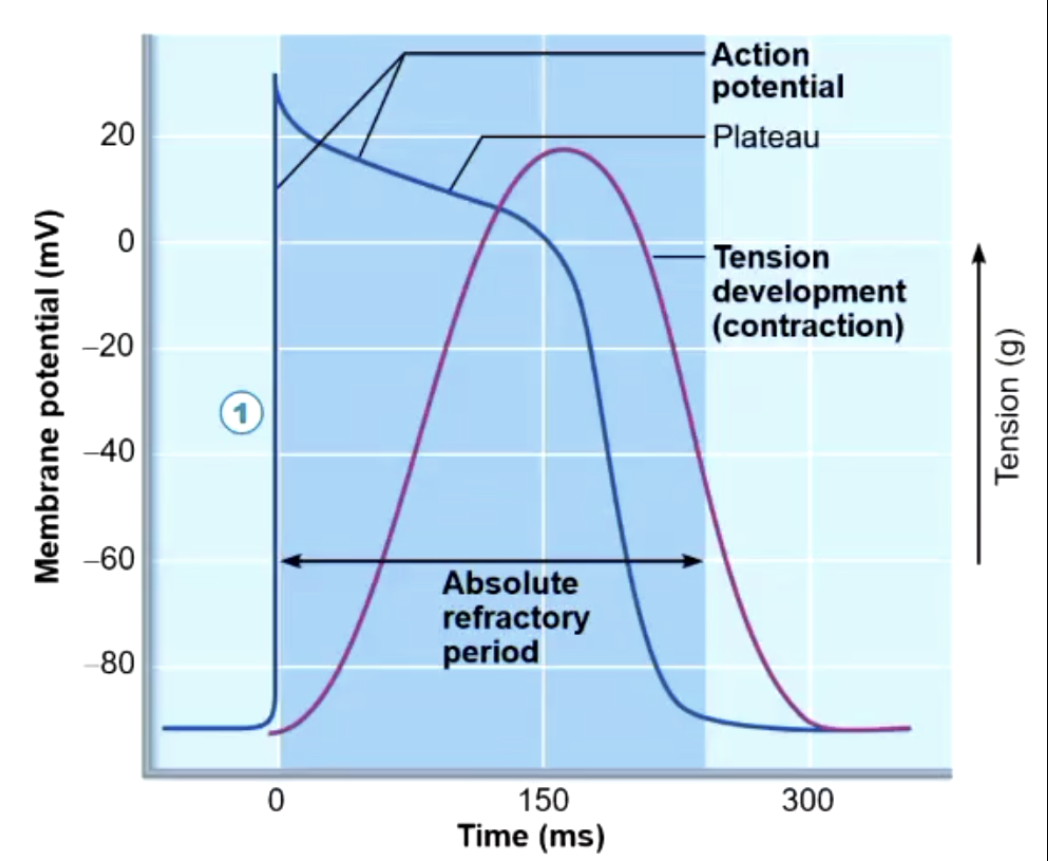
Action potentials in cardiac muscle cells
Stable resting membrane potential
1) Rapid depolarisation of Na influx through fast voltage gated Na channels
2) Plateau phase of where there is a slow influx of calcium keeping the cell depolarised. THIS IS WHERE THE CONTRACTION TAKES PLACE
3) Repolarisation is when the calcium channels becomes inactivated, opening the potassium channels, and resting to the resting voltage
Long Absolute refractory period
Function link
Produces strong, coordinated contractions
Plateau allows sustained force for blood ejection
Prevents continuous contraction → ensures relaxation between beats
Similarities and Differences of Autorhythmic cells and Contractile cells
Similarities
Both involve Na⁺, Ca²⁺, and K⁺ ions
Both propagate electrical signals in the heart
Both are essential for coordinated heartbeat
Differences
Autorhythmic cells → initiate impulses (no resting potential, automatic firing)
Contractile cells → produce force (plateau phase, strong contraction)
Autorhythmic = set the rhythm of the heart
Contractile = execute the pumping of blood
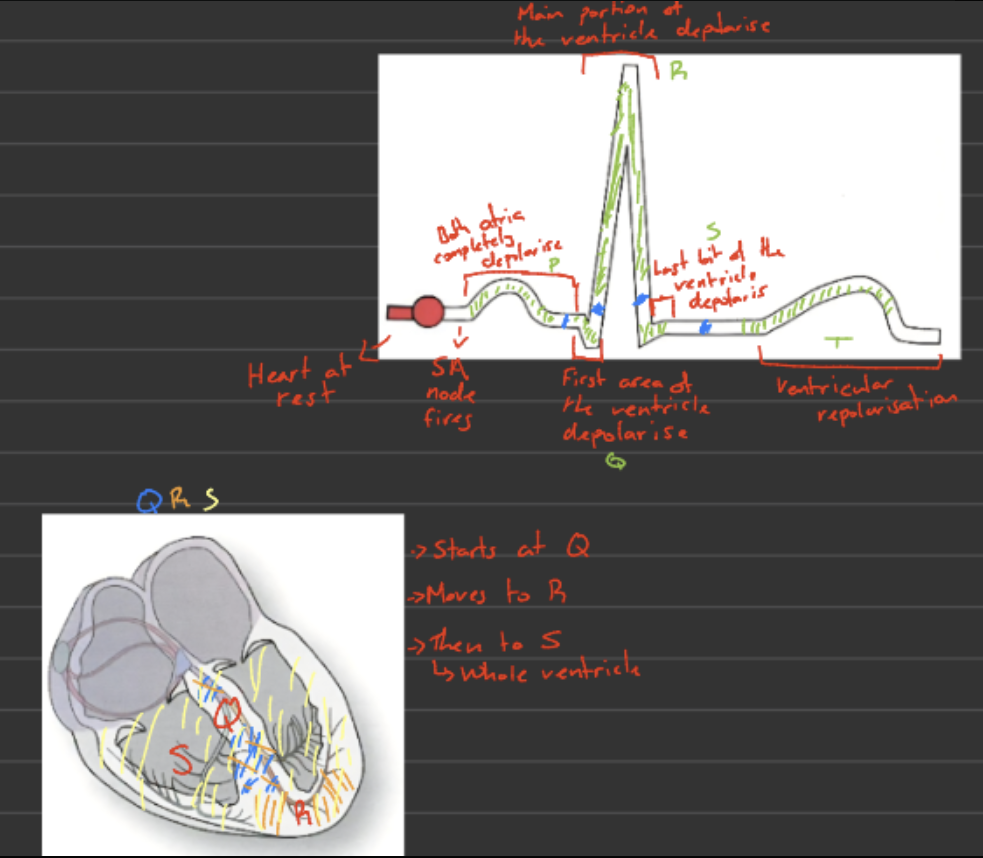
Flow of electrical activity
SA node fires
Impulse spreads across both atria
Causes atrial contraction
AV node (atrioventricular node)
Receives impulse
Delays it briefly (allows ventricles to fill)
Bundle of His and bundle branches
The bundle of His separates into right and left bundle branches, carries the electrical to the apex.
Purkinje fibres
Spread impulse through ventricular walls
Ventricles contract
Blood is pumped to lungs and body
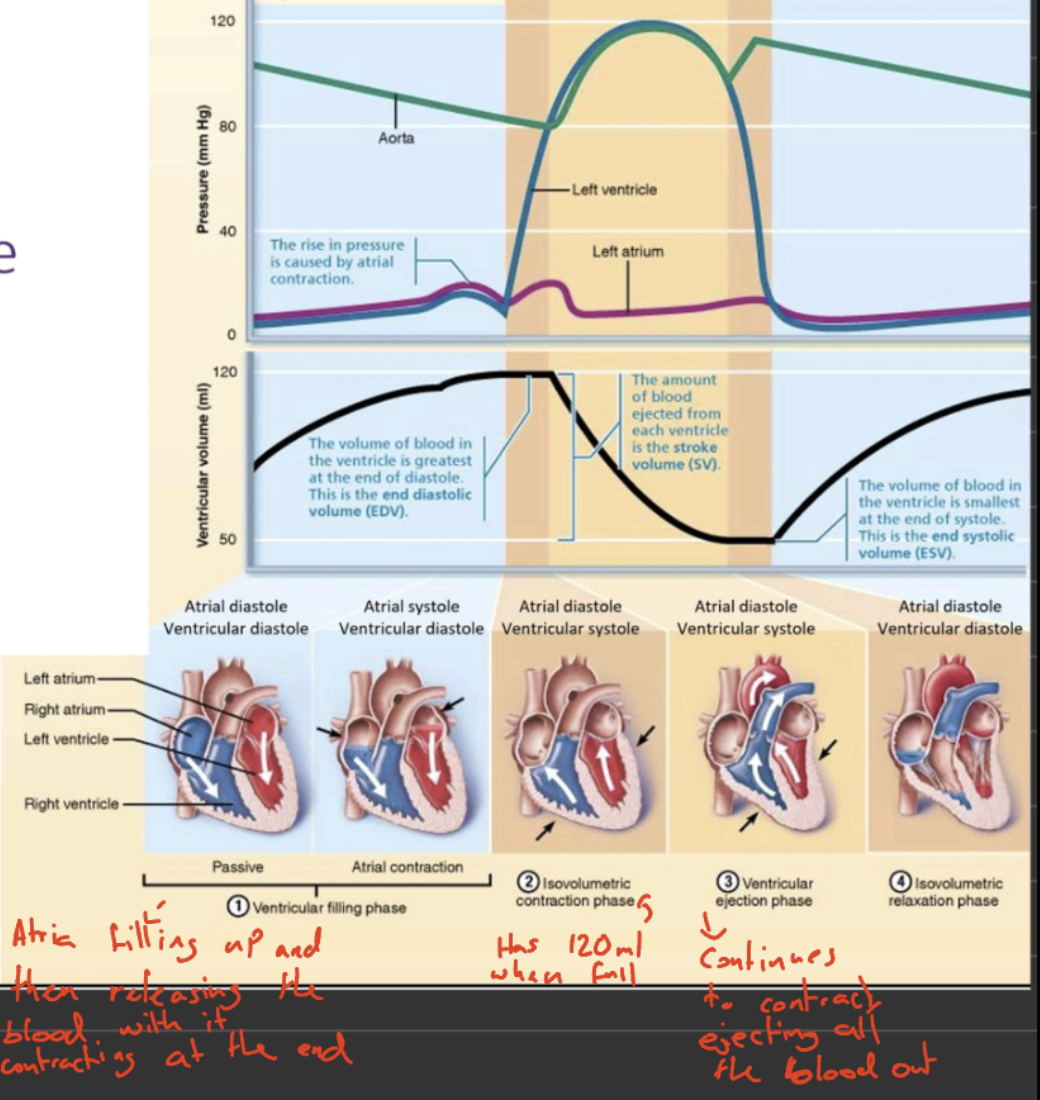
The five volume stages of the cardiac cycle
Ventricular and atrial diastole
Passive filling of ventricles and atria with blood
Atrial contraction (atrial systole)
Blood is moved from the atria to the ventricles
Isovolumetric ventricular contraction (ventricular systole)
Ventricles contract but don’t yet eject blood (done to close the AV vales)
Ventricular ejection (ventricular systole)
Blood is ejected into arteries
Isovolumetric ventricular relaxation (ventricular diastole)
Ventricles relax and remaining blood stays in ventricles
Mean Arterial pressure
Mean arterial pressure = cardiac output x total peripheral resistance
Cardiac output → Blood coming out of the heart into the arteries
Total peripheral resistance → Diameter of the blood vessels
Cardiac Output

Heart rate
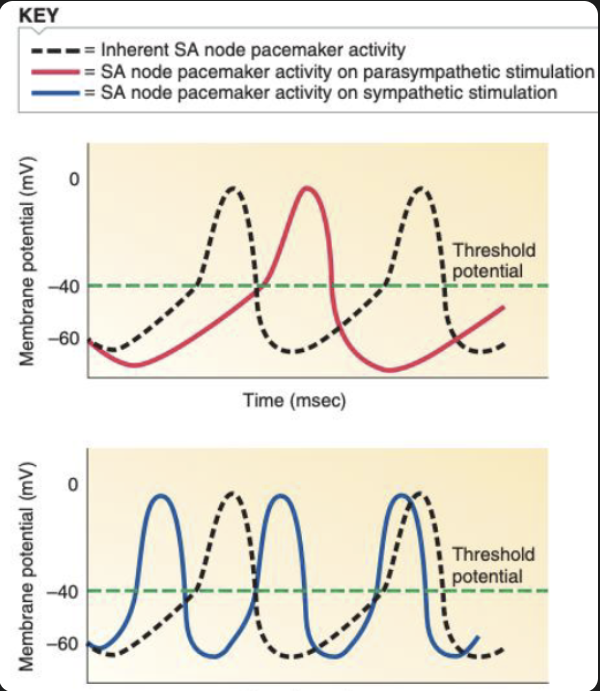
Parasympathetic nervous system
Slows down action potential firing in the SA node - pacemaker activity
Causes hyperpolarisation, slowing time to reach threshold, thus starting an action potential
Sympathetic nervous system
Increases rate of action potential firing in the SA node - pacemaker activity
Causes depolarisation, reducing time to reach threshold, thus starting an action potential
This is how heart rate is regulated
Stroke Volume
Stroke volume (SV) = EDV - ESV
End diastolic volume → Volume of blood in the ventricles before contraction or end of diastole
End systolic volume → Volume of blood that is left in the ventricles after contraction
This is how Stroke Volume is regulated
Factors affecting stroke volume
Venous Return
Amount of blood returning to the heart
Higher venous return INCREASES EDV, thus increase cardiac output
causes a greater stretch for the heart muscle
Sympathetic NS increases venous return
Contractility of the heart
How hard the heart is contracting
Harder contraction means more blood ejected thus DECREASES end systolic volume, ESV
Sympathetic NS increases contractility of the heart
Total peripheral resistance
Resistance to blood flow is determined by:
Blood viscosity (usually constant)
Blood vessel length (Usually constant)
Blood vessel diameter
What determines the total peripheral resistance (TPR)
Radius of arterioles can be increased or decreased
• Increase radius → vasodilation → reduced TPR
• Decrease radius → vasoconstriction → increased TPR
Describe two pathologies that result from abnormal blood pressure
1. Hypertension (high blood pressure)
Chronically high pressure damages vessel walls
Leads to heart strain, stroke risk
2. Hypotension (low blood pressure)
Low pressure reduces blood flow to organs
Causes dizziness and fainting
Baroreceptor reflex and the autonomic nervous systems role
Detects changes in blood pressure via stretching of blood vessel walls
Sends signals to the medulla
↑ Blood pressure
↑ firing (too much pressure) → ↑ parasympathetic, ↓ sympathetic
Leads to, ↓ heart rate, vasodilation → BP decreases
↓ Blood pressure
↓ firing (not enough pressure) → ↑ sympathetic, ↓ parasympathetic
Leads to, ↑ heart rate, vasoconstriction → BP increases
The autonomic nervous system adjusts heart rate and vessel diameter to keep blood pressure stable.
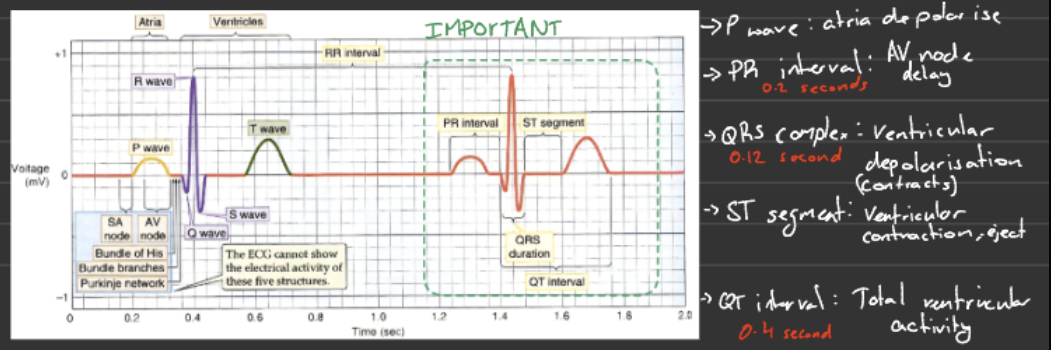
Understand what ECG measures and what creates the different ECG waveforms
ECG measures electrical activity (voltage changes: depolarisation and repolarisation) of the heart
Waveforms you must know:
P wave → atrial depolarisation
QRS complex → ventricular depolarisation
T wave → ventricular Repolarisation
Describe how the ECG correlates with the cardiac cycle
P wave → atria depolarise → atria contract (atrial systole)
PR interval → delay at AV node → ventricles fill with blood
QRS complex → ventricles depolarise → ventricles contract (ventricular systole) - AV valves close
ST segment → ventricular contraction → blood is ejected
T wave → ventricles repolarise → ventricles relax (diastole)
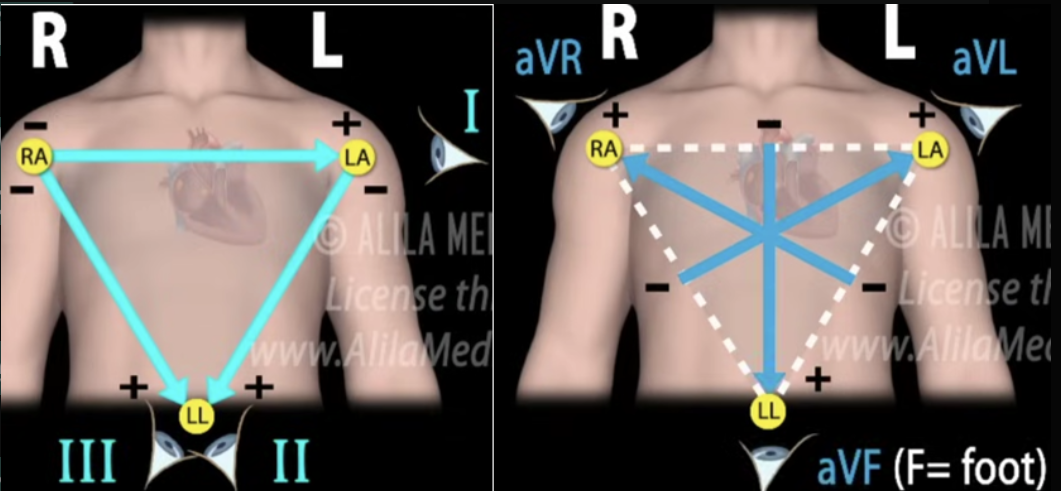
Explain how the ECG is measured using leads
A lead is not a wire, but a view of the heart’s electrical signal (looking from positive to negative) created by comparing voltage between two electrodes.
Limb leads (I, II, III): Measure heart activity in the frontal plane using arms and legs. BIPOLAR LEADS
Lead I: Right arm → Left arm
Lead II: Right arm → Left leg
Lead III: Left arm → Left leg
Augmented leads (aVR, aVL, aVF): Provide additional frontal-plane views. UNIPOLAR LEADS
aVR: Right arm perspective
aVL: Left arm perspective
aVF: Foot (inferior) perspective
Chest leads (V1–V6): Measure activity across the chest in the horizontal plane.
V1–V2: Right heart / septum
V3–V4: Anterior wall
V5–V6: Lateral wall
Explain common causes of heart rate changes that can be measured with ECG
Tachycardia: Faster heart rate
Exercise
Stress / adrenaline
Fever
Bradycardia: Slower heart rate
Sleep
High fitness (athletes)
Explain the concept of the mean electrical axis (cardiac axis), what it measures, and how it changes with physiological and pathological factors
The cardiac axis (mean electrical axis) is the average direction of the heart’s ventricular electrical activity during contraction, shown as an angle on an electrocardiogram (ECG).
What it measures:
The net direction of the heart’s electrical activity during ventricular contraction
Represented as an angle in degrees
Key idea:
It summarises all ventricular electrical forces into one main vector
Why it matters:
Helps detect cardiac enlargement or hypertrophy
Identifies conduction defects and some cardiac pathologies
Describe some pathologies that can be detected by ECG
Extrasystoles and sinus arrhythmia → irregular heart rhythms
Supraventricular tachycardia (starts at the atria) and ventricular tachycardia (starts in the ventricles) → abnormally fast heart rates
Heart block → delayed or blocked electrical conduction
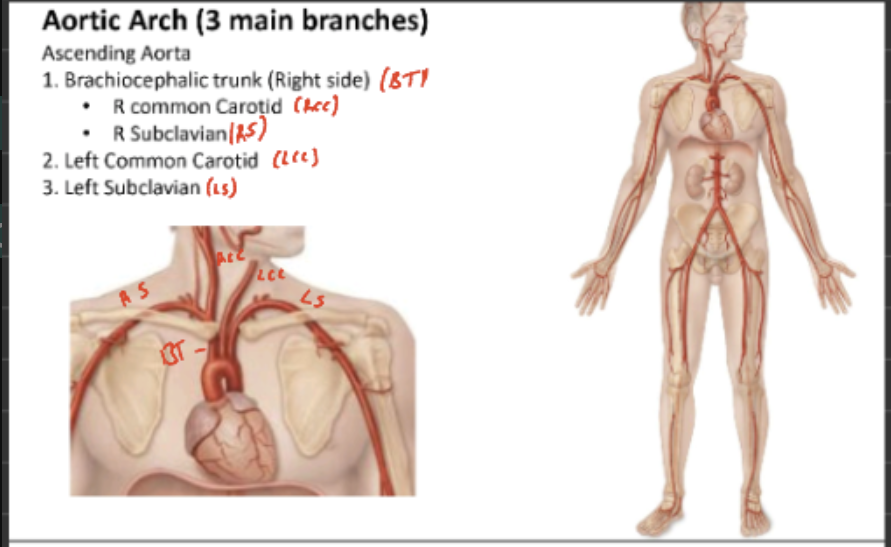
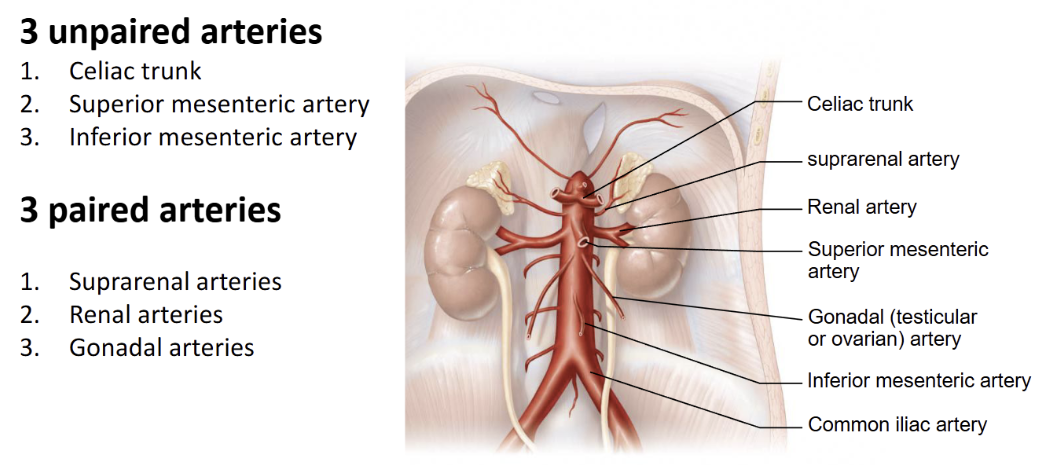
Name the arteries which branch off the Aorta to give rise to the arteries in different regions of the body
Aorta
Ascending Aorta
Descending Aorta
Aortic arch
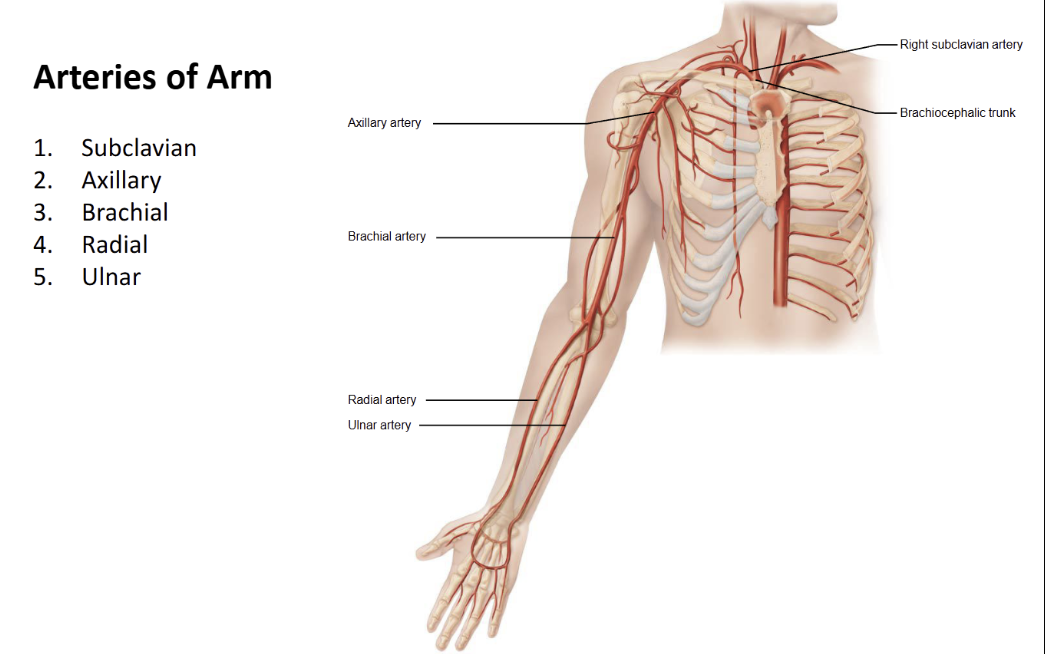
Name the arteries of the arms
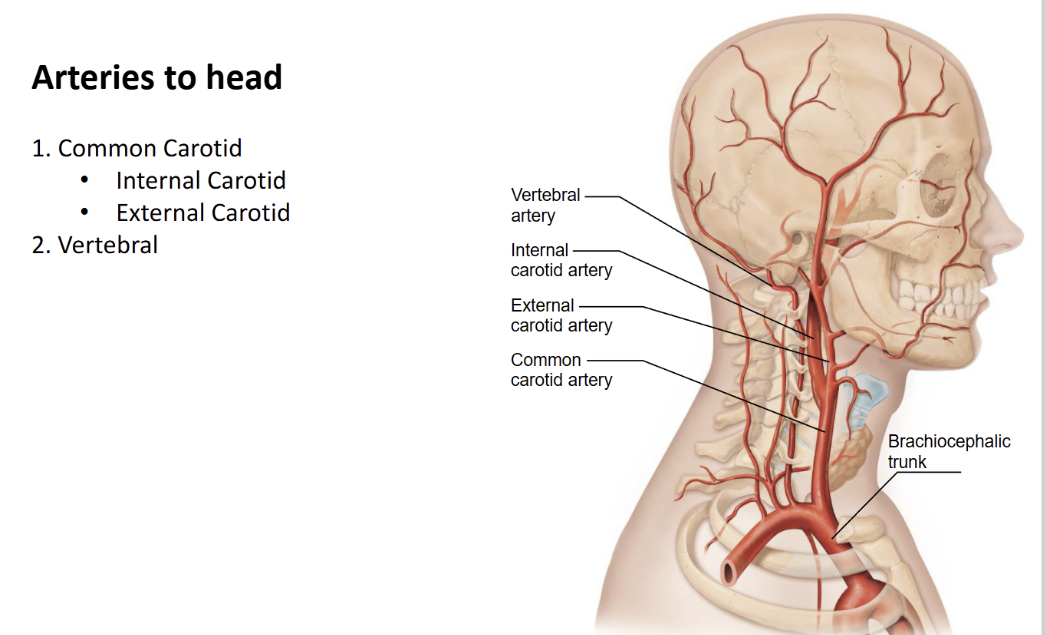
Name the arteries of the head
Internal Carotid = for the brain
External Carotid = for the face and neck
Vertebral = Goes through the cervical holes and up to the head
Name the arteries of the torso (paired and unpaired branches from Aorta)
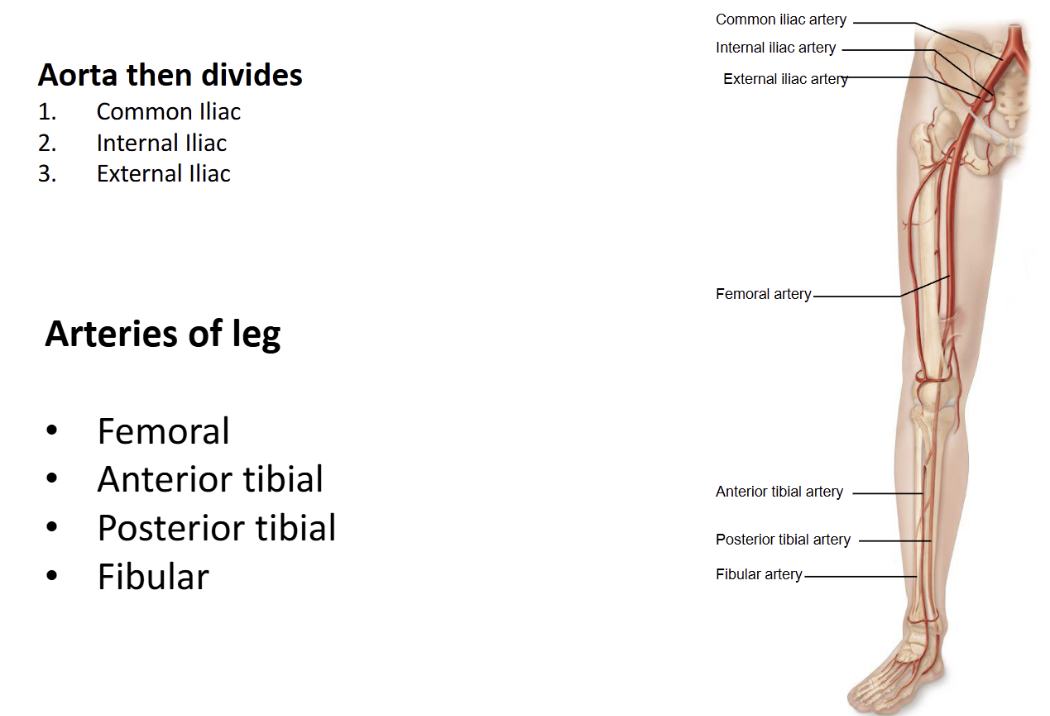
Name the arteries of the legs
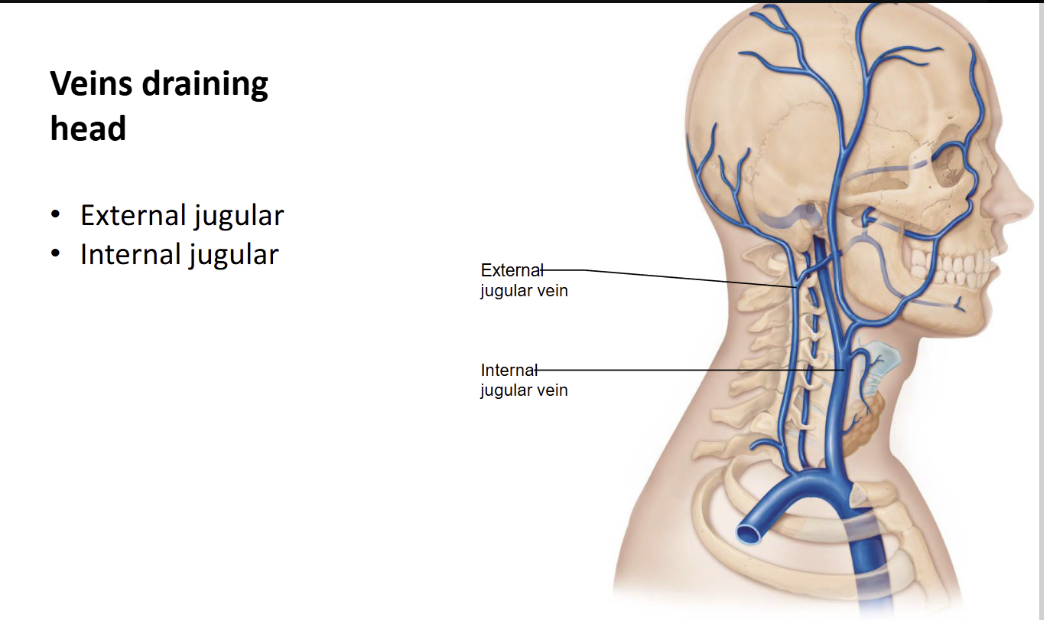
What vein drains the head