NUR2225 EXAM PREP
1/44
Earn XP
Description and Tags
mental health
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
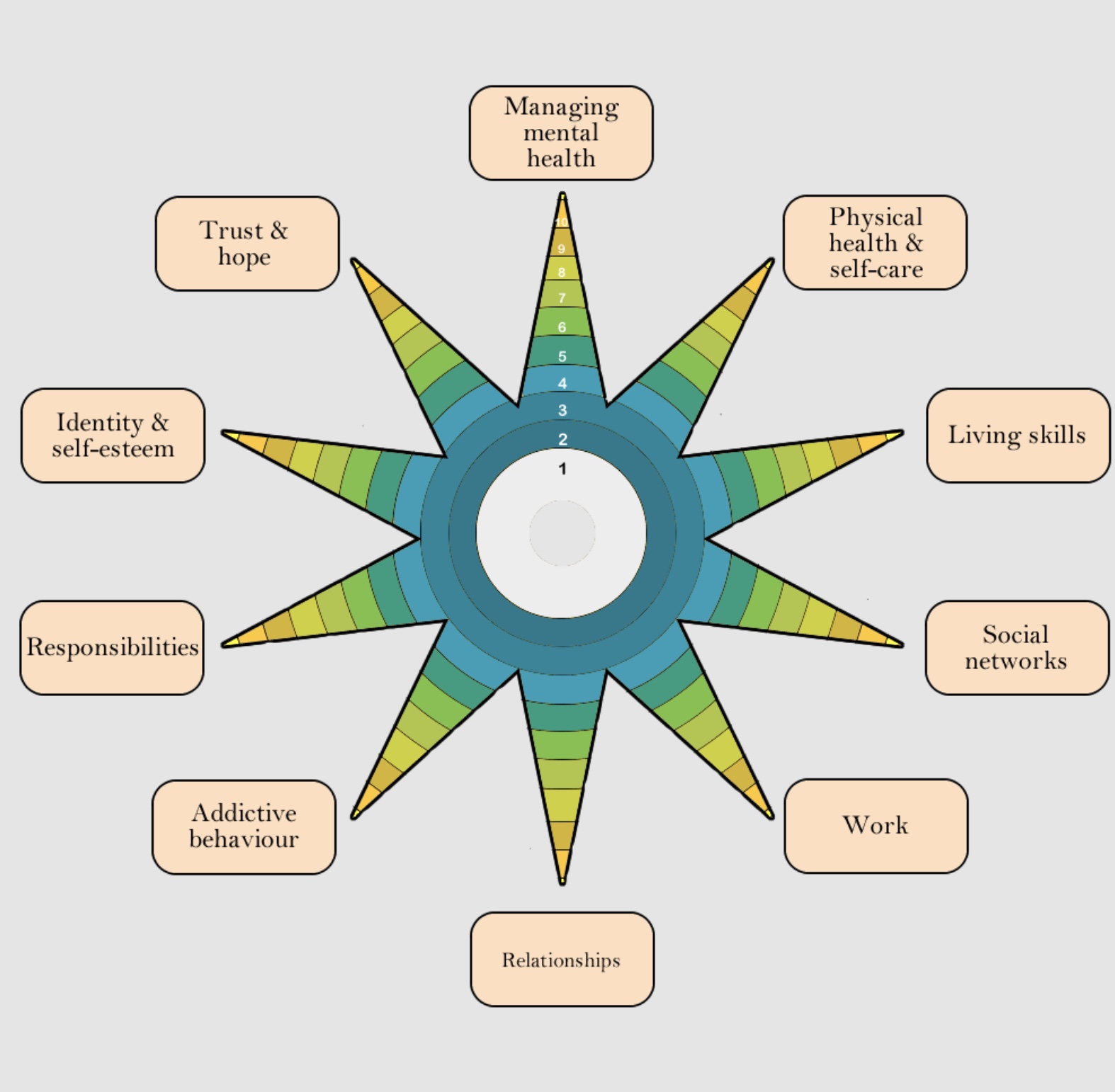
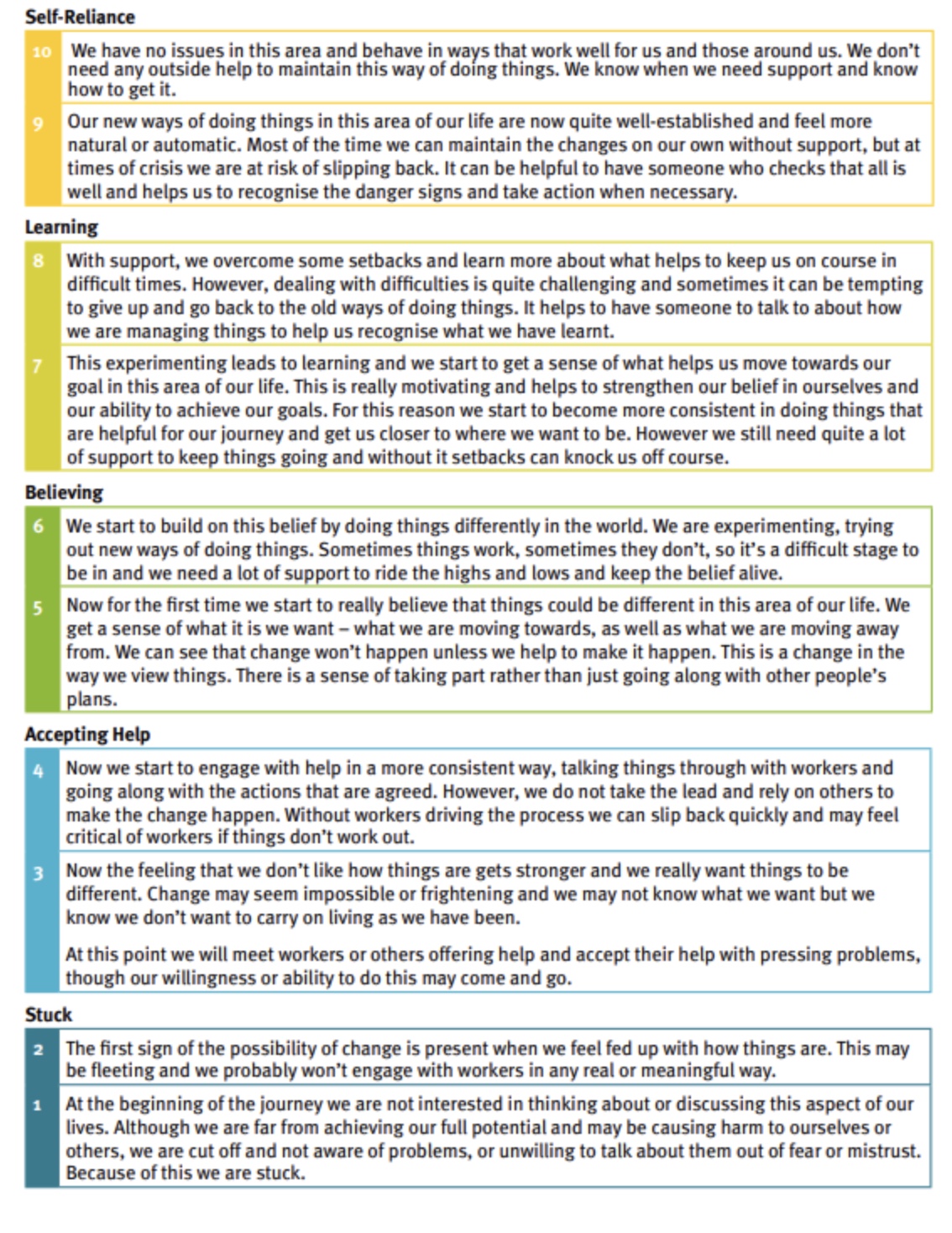
Recovery star
Biopsychosocial model
understand and treat mental illness in a holistic manner with the complex interplay of three dimensions
Personal:
Bio-
Psycho-
Society:
Social
therapeutic relationship
Establish therapeutic rapport
Remain person centred and responsive to the person’s immediate needs using active listening skills, being supportive and providing reassurance
Encourage the person to discuss their feelings and share their thoughts and associated experiences – acknowledge, validate, clarify and empathise
Person centred care
ensuring that health services are tailored to people’s needs and are provided in partnership with the patient
benefits:
improves the trust, experience and outcomes
respect cultural and regious diversity
emprowering dignity and choice
Trauma informed care
treat everyone as they have experienced trauma in their lives to prevent further harm.
provides services and support that recognises and responds to impacts of trauma on individuals’ lives
principles:
safety
empowerment
choice
collaboration
trustworthiness
Stigma
Three components:
stereotype: negative belief about a group.
prejudice: cognitive and affective response that leads to discrimination and a behavioural reaction.
discrimination: behavioural response to prejudice.
Impacts:
societal exclusion.
denied access to life opportunities, employment, education, community acess.
The Mental Health and Wellbeing Act (2022)
mental health law that reforms approaches to mental health treatment aiming to provide an diverse, compassionate and responsive care plan.
support dignity
ensure collaboration with their treatment of care
recognist role of family and carers
responds to diverse needs and preferences
assessment order: when psychiatrist intiates compulsory treatment when assessing severe declination if treatment if not provided to person.
Assessment order
person appears to have a mental illness and appears to need immmediate treatment to prevent:
serious deterioation
serious harm to self and others
Temporary Treatment Order (28 days)
Compulsory treatment criteria are:
person (>18 years) has mental illness, and
because needs immediate treatment to prevent:
serious deterioation, serious harm and
and there are no less restrictive methods for person to recieve treatment.
Comprehensive holistic assessment
This advances person-centered care approaches by providing appropriate services relevant to the person's individual needs and treating them as a whole.
past mental history
family history
medications
substance history
foresensic history
premorbid personality
Mental Health Examination (MSE)
Appearance: hygiene, weight, hair style/colour.
Behaviour/motor activity: posture, hyperactivity, movement.
Speech: volume, tone, paste, quality.
Mood: rating scale, emotions.
Perception: auditory, visual, olfactory, gustatory, tactile…
Thought content: obessions, delusions, magical thinking, harm.
Thought form/process: thought broadcasting, insertion…
Insight: personal belief about ones’ condition
Judgement: ability to make reasoned decisions
Memory
Orientation
Cognition: general intelligence, orientated to place/time/person.
BARRIERS TO:
Mental Health Examination (MSE)
Lack of therapeutic relationship
physical environment
age
health literacy
cultural and language barriers
stigma
cognitive state or untellectual impairment
mood altering substances.
Risk Assessment
Risk assessment is an process that identify and evaluate the potential risks that an individual may propose upon themselves or others. The primary goal is to enhance safety and well-being of the individual and their surroundings.
harm to self/others
suicidal tendencies
suicidal history
vulnerability
S: staring
T: tone of voice
A: anxiety
M: mumbling
P: pacing
management of psychosis:
ANTIPSYCHOTICS
role of MHN:
education on benefits.
education on side effects: weight gain, headache, sedation.
administer and monitor the effect of treatment.
Types of irrational beliefs
thought broadcasting:
inner thoughts are heard to external environments
persecutory ideation:
fixed thoughts of one is being targeted, harmed, conspired against.
thought insertion:
delusions and thoughts aren’t their own.
ideas of references:
random, unelated external events are meant for them.
Interventions for:
ANXIETY
NON-PHARMACOLOGICAL:
Breathing exercises
Mental exercises
Physical movement
Mindfulness
Sensory Modulation
Reframing unhelpful thoughts
Psychoeducation
PHARMACOLOGICAL:
antidepressants
selective serotonin reuptake inhibitors
Diagonostic & Statistical (DSM) criteria for:
Major Depressive Disorder
depressed mood, most & nearly everyday.
diminished interest and pleasure
significant weightloss (>%5 in a month)
insomnia or hypersomnia
agitation, restlessness
fatigue
worthlessness or guilt
diminished thinking and concentration
recurrent thoughts of death
DSM criteria for:
Bipolar Disorder Manic Episode
A. increase activity & energy lasting at least 1 week.
B. three (or more) of the following symptoms:
inflated self esteem or grandiosity
decreased need for sleep
flight of ideas
distractibility
increase goal-directed activity
excessive involvement in activities with painful consequences.
C. mood disturbance sufficiently severe that cause marked impairment
D. listed episodes are not attributed to substance abuse
DSM criteria for:
Bipolar Disorder hypomanic Episode
A. abnormal elevated, expansive, or irriritable mood lasting at least 4 consecutive days.
B. three or more of the following symptoms:
Inflated self-esteem or grandiosity.
Decreased need for sleep (e.g., feels rested after only 3 hours of sleep).
More talkative than usual or pressure to keep talking.
Flight of ideas or subjective experience that thoughts are racing.
Distractibility
Increase in goal-directed activity
Excessive involvement in activities with high potential for painful consequences.
C. uncharacteristic of individual when not symptomic.
D. disturbance in mood and functioning observable by others
E. not severe enough to cause impairment in social or hospitalisation
F. not attributed to drug or substance usage.
MSE:
person experiencing mania
Appearance
dishevelled, provacative, flamboyant
Behaviour
restless, disorganised, innappropriate
Speech
rapid, loud, increased
Mood
euphoric, elevated, irritable
Affect
euphoric
Thought content
delusions, inflated self-esteem
Thought form
flight of ideas, increased thought stream
Perception
nil unless psychosis
Cognition
short attention, racing thoughts
Judgement
poor
Insight
poor
Low mood, depression, mania, and bipolar disorder
Low mood:
short period/temporary response to specific stressors or life events.
Depression:
clinical diagnoses mental health condition that impacts daily functions, chronic period (>2 weeks) of low mood.
Mania:
intense abnormal high energy, euphoric, impulsivity lasting (>7 days)
can cause psychosis unliked hypomania (<4 days)
Bipolar Disorder:
extreme mood swings, emotional highs such as mania and hypomania and extreme lows such as depression.
depression and mania are associated symptoms of bipolar affective disorder.
Emotional dysregulation
difficulties regulating painful emotions
unable to control intense arousal and problems turning attention away from stimuli, cognitive distortions and failures in nformation processive and unable to control impulsive behaviours relating to strong emotions.
DSM for:
Borderline Personality Disorder (BPD)
instability of interpersonal relationships, self-image, and marked impulsivity beginning in adulthood.
frantic efforts to avoid real or imagined abandonment
identity disturbance.
impulsivity (self-damaging)
recurrent suicidal behaviour
affective instability due to reactivity of mood
chronic feelings of emptiness
innapropriate response to anger
transient, stress-related paranoid ideation or severe disassociative symptoms
BPD:
Transference & Countransference reactions
Transference:
transferring feelings, thoughts or behaviours that occured in the past to a situation that is happening in their present
Countertransference:
your response to the patient
Nursing considerations:
BPD
Mental Health Safety Plan:
identify triggers to crisis
link strategies to cope with triggers
Medications
should not be primary treatment therapy
high dosage can lead to overdose (high-risk patients)
substance dependance (e.g. benzodiazepines)
acute crisis if psychological therapy is insufficent
Psychotherapy
Cognitive Behavioural TherapY (CBT)
DSM 5:
Personality Disorder (Cluster A)
odd, eccentric thinking or behaviour
Paranoid Personality Disorder
distrust and suspiciousness of others & their motives are interpreted as harmful and against them
Schizoid Personality Disorder
detachment from social relationships and restricted range of expression of emotions in interpersonal settings
Schizotypical Personality Disorder
social and interpersonal deficits, accompanied by cognitive or perceptual distortions.
DSM 5:
Personality Disorder (Cluster B)
dramatic & erratic behaviours
Narcissistic Personality Disorder
grandiosity (in fanatsy or behaviour), need for admiration, lack of empathy.
Borderline Personality Disorder
instability of self-image, relationshps and marked impulsivity.
3. Histrionic Personality Disorder
attention-seeking, excessive emotionality
Antisocial Personality Disorder
pattern of disregard and violation of rights of others
DSM 5:
Personality Disorder (Cluster C)
anxiety and fear-driven behaviours
Avoidant Personality Disorder
social inhibitation, feelings of inadequency and hypersensitivity to negative feedback.
Dependant Personality Disorder
excessive need to be taken care of, clinging, fear of serperation
Obssessive Compulsive Personality Disorder (OCPD)
preoccupation with orderliness, perfectionism and mental and interpersonal control
nursing management:
BPD
Mental Health Care Plan
Identity triggers
create coping strategies to alleviate negative promoting behaviour
Medication
overdose for high suicide risk patients
not the primary treatment therapy
acute crissis if psychological therapy is insufficent
medication dependancy
Psychotherapy
CBT (cogtive behavioural therapy):
reframe negative thinking patterns and achieve stability and strategies to cope with emotions.
DBT (dialectical behavioural therapy)
incoperaties cbt and talk therapy into understandign the relationship between emotions and behaviours
nursing management:
Personality Disorder
get what you want from another person
Describe the current situation, stick to the FACTS.
Express your feelings and opinions about the situation
Assert yourself and say no clearly
Reinforce (reward) person ahead of tim by explaining positive effects
Mindful: keep focus of goals and dont be distracted
Appear confident
Negotiation
DSM 5:
Substance-use disorders
mild = 2/3
moderate = 4/5
severe = > 6
taking substance in high doseses
wanting to cut down but unable to
spending alot of time using, recovering from use
cravings and urges
inability to function in daily life
continious usage even if problems arise in relationships
giving up on important events
continual usage despite dangerous circumstance
psychological/physical problems dont discourage use
needing more of the substance (tolerance)
experience withdrawal symptoms
Substance-related disorders
INTOXICATION & WITHDRAWAL
Intoxication
any change in person’s perception, mood, cognition or behaviour after drug usage.
Withdrawal
occurs afte stopping drug usage, or reducing amount
range from mild to life-threatening
Substance-related disorders
CATEGORIES OF DRUGS
stimulants
speeds up function of CNS
depressants
decreases function of CNS
hallucinogens
distort senses and change of experience
cannabinoids
multiple effects and can fall in all three categories listed above;
Nursing Management OF Substance-related disorders:
PHARMACOLOGICAL
Opoid Substitution Therapy
used for patients with dependancy on opoids (e.g. herion)
prevents withdrawal
Nicotene Replacement Therapy (NRT)
releases slow/lower doses of nicotene compared to smoking
Naltrexone
used to patients who withdrawn from opoids and stop person from achieving “high”
also alchohol abstainance to reduce cravings
Benzodiapenes:
reduce and protect withdrawal signs
modulates CNS activity
doses depend on severity
OTHERS:
antipsychotics, paracetemol, metoclapramide
Nursing Management:
ALCOHOL WITHDRAWAL
Alchohol withdrawal scale:
mild: hypertension, headache, sweating
severe: hallucinations, disorientation, confusion
minising progression to severe withdrawal
reducing risk to self and others
reduce/elimination physical health problems
identify co-occuring illnesses that are masked
DSM 5:
Eating Disorders
Orhtorexia
Anorexia Nervosa
Bullimia Nervosa
Binge-Eating Disorder (BED)
Other Specified Feeding or Eating Disorder (OSFED)
Obesity
Pica
Diagnostic criteria
BULLMIA
large amounts of eating in discrete period of time
compensatory behaviours (purging, exercising)
lack of self-control
occurs at least once a week for (>3 months)
PHYSICAL - fainting, dizziness, damaged teeth, swollen face
PSYCHOLOGICAL - obession w/ food, intense fear of gaining, irritability surrounding meals,
BEHAVIOURAL - social isolation to avoid eating, secretive, laxatives, repititive behaviour, fasting, compulsive exercising, frequent bathroom trips
Diagnostic criteria
BINGE EATING DISORDR\ER
PHYSICAL - lethargy, poor sleep, constipation, bloating, w
PSYCHOLOGICAL - obsessive about food, guilt after binge, depression, suicidal tendencies
BEHAVIOURAL - food hoarding, secretive behaviour, discomfort regarding weight, isolation, shop-lifting, mass buying food products
Nursing management:
EATING DISORDER
ECG monitoring
vital signs
meal support
blood collection for electroyte monitering
psychoogical support
monitor weight
regular MSE & risk assessments
nasogastric tube for re-feeding
medication and education
Counseling Technique (SOLER)
Sit squarely
Open body
Lean slightly
Eye contact
Relax
Atypical antipsychotics
(schizophrenia)
atypical medications:
olanzapine
clozapine
quetiapine
aripiprazole
risperidone
acuphase
factors of risk assessments
protective: reduce negative outcomes of risk (e.g peer support).
static: unchanging, baseline of probability of risk (e.g. criminal record).
dynamic: conditions that slowly change (bipolar mania/low periods)
psychosis
non-pharmacological interventions
CBT therapy - increase function and wellbeing by reducing psychotic and affective symptoms.
Music therapy - utilizing music as an method to express, reducing negative symptoms and improve quality of life
Family support/education - provide education to interpersonal relationships to enhance treatment and strategies outside of healthcare settings, improving daily functioning.
mood stabilisers
(bipolar)
lithium carbonate
sodium valproate
antidepressants
(anxiety, depression)
escitalopram
diazepam