W13 Pathology of Peripheral Artery Disease
1/107
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
108 Terms
What is vasculitis?
Inflammation of the blood vessel wall; can affect any vessel type (small capillaries to the aorta) in any organ
What are the two most common mechanisms of vasculitis?
Immune-mediated mechanisms and direct invasion of the vascular wall by infectious pathogens
What constitutional symptoms are seen in vasculitis?
Fever, myalgia, arthralgia, and malaise — due to systemic inflammation or local manifestation of tissue ischemia.
What vessels are most likely affected in vasculitis?
Most affect small vessels such as arterioles, venules and capillaries. Several affect aorta and medium sized vessels. Some involve several sizes and/or sites. (Some patients have disorders that do not fit neatly into a single well-defined category and have overlap features)
What local consequences result from endothelial damage in vasculitis?
Thrombosis → ischemia; RBC extravasation → purpura/bleeding; transudate/exudate; vessel wall destruction → aneurysm or rupture
What are the 5 possible pathogenic mechanisms of vasculitis?
1) Immune complex formation (Type III hypersensitivity), 2) Anti-endothelial cell antibodies, 3) ANCA (anti-neutrophil cytoplasmic antibodies), 4) T-cell dependent (cell-mediated/granulomatous), 5) Direct infection of endothelial cells
Which vasculitis diseases are caused by immune complex formation (Type III hypersensitivity)?
SLE vasculitis, RA vasculitis, Polyarteritis nodosa (PAN), drug-induced vasculitis, viral infection-associated vasculitis
Which vasculitis is caused by anti-endothelial cell antibodies?
Kawasaki disease (mucocutaneous lymph node syndrome)
Which vasculitis diseases are ANCA-related?
Wegener's granulomatosis (PR3/c-ANCA), Microscopic polyangiitis (MPO/p-ANCA), Churg-Strauss syndrome (MPO/p-ANCA) - Premature activation of neutrophils > damages surrounding tissues + suicide (ANCA)
Which vasculitis diseases are T-cell dependent (granulomatous)?
Giant cell arteritis (temporal arteritis) and Takayasu arteritis (unknown but thot to be immune mediated). Typically, this can show granuloma. And also there is a minor component of humoral response as well. So, mainly we will see the cellular reaction, but this can have autoantibodies, this is kind of aftermath of local immune reaction.
What is a granuloma histologically?
Central collection of histiocytes/macrophages ± multinucleated giant cells, surrounded by lymphocytes; represents cell-mediated immune response
What does the presence of granuloma in a vessel indicate?
Cell-mediated immune response causing tissue/vessel damage
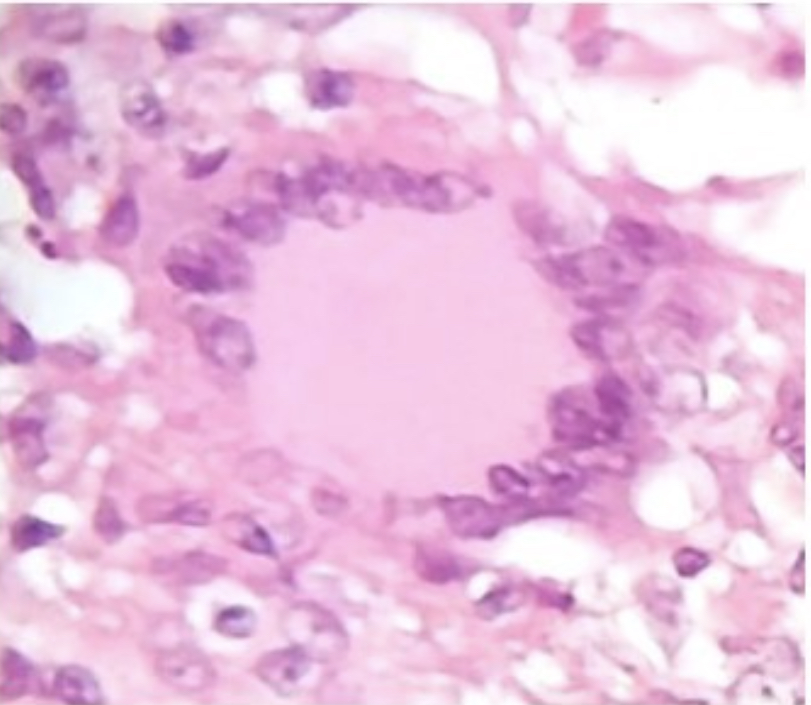
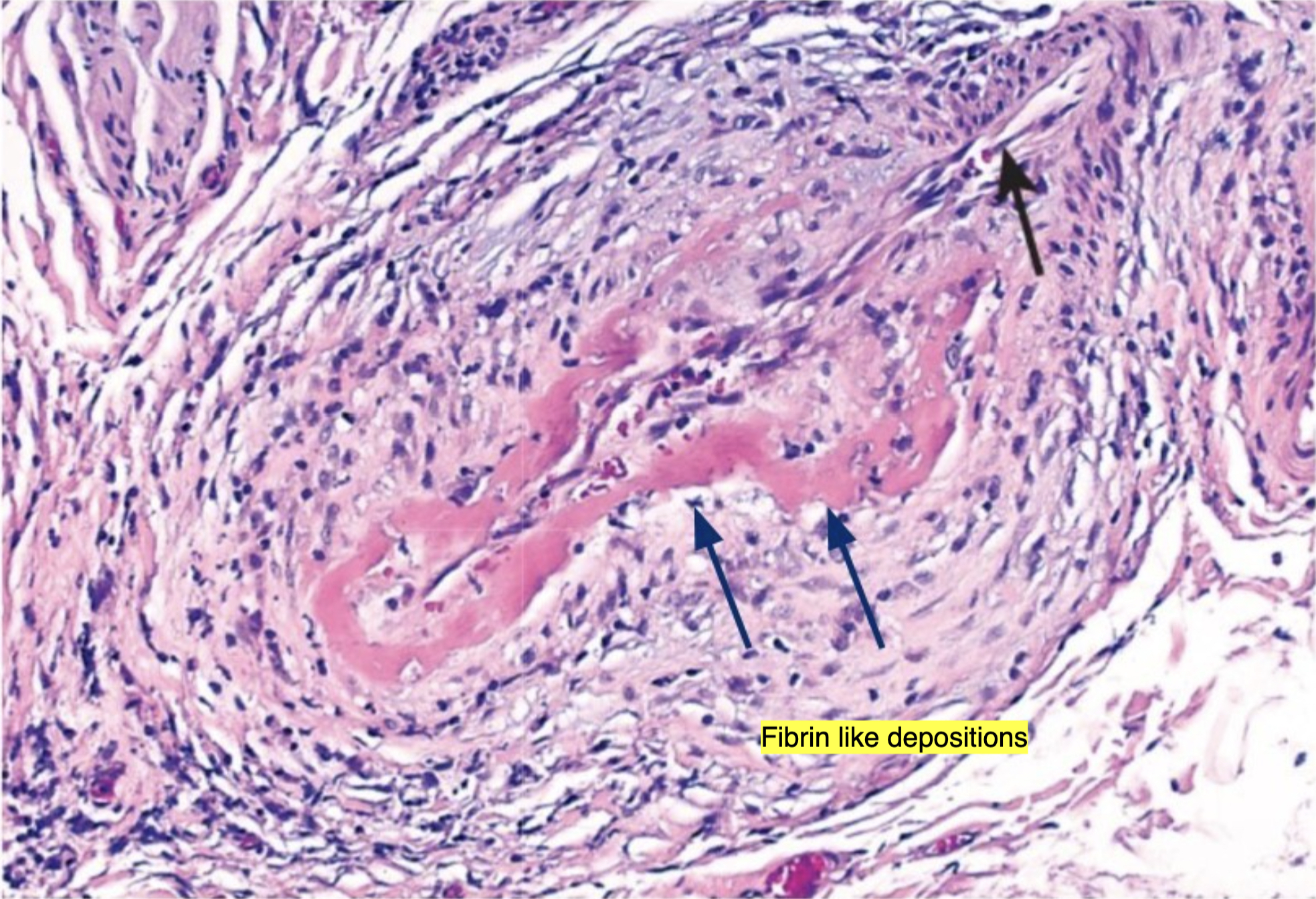
What is fibrinoid necrosis (necrotizing vasculitis)?
Fibrin-like deposition of pink (eosinophilic) material or debris after vascular cell death(endothelial cell death); caused by immune complex deposition (or chemical damage)
What causes fibrinoid necrosis in vasculitis?
Immune complex deposition → necrosis of endothelial and smooth muscle cells → replacement with fibrinoid material
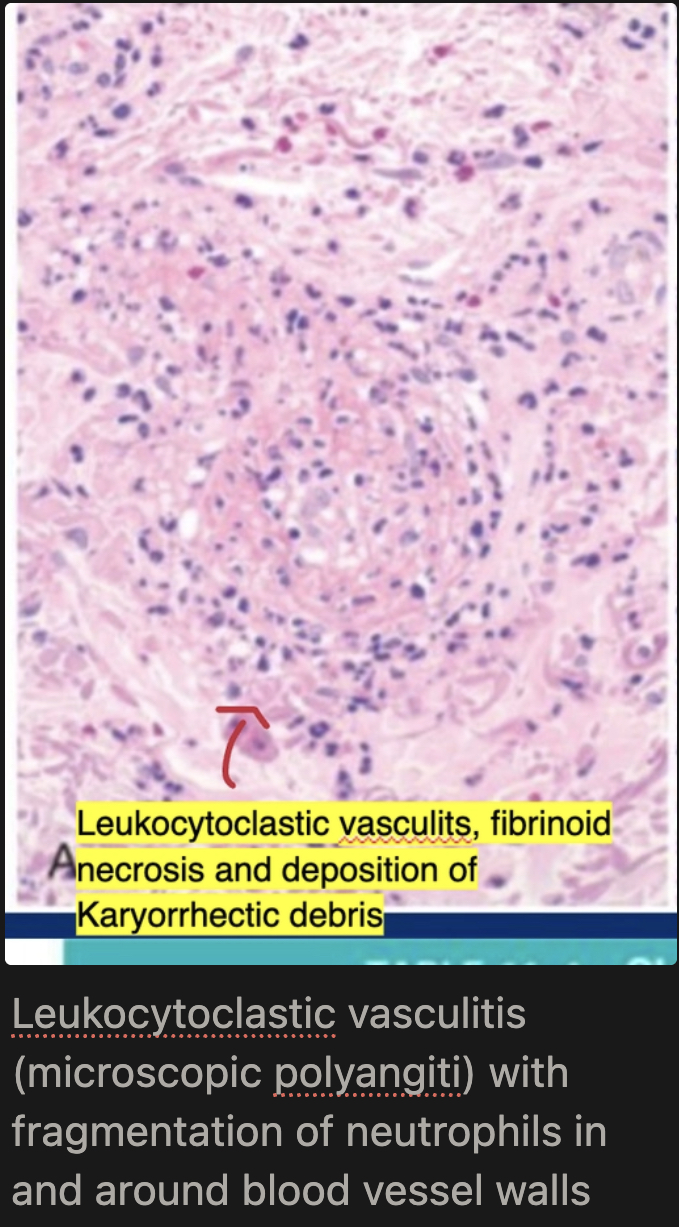
What is leukocytoclastic vasculitis?
basically means inflammation driven by neutrophils (“leuko”) that break apart (“clastic”). In this condition, neutrophils become highly activated—often due to antibodies like Antineutrophil cytoplasmic antibodies—and release toxic enzymes that damage vessel walls. As these neutrophils die, their nuclei fragment into tiny pieces called karyorrhectic debris, which appear as small dark dots under the microscope. So the name reflects the key feature: blood vessel damage with broken-down neutrophil debris deposited in the tissue.
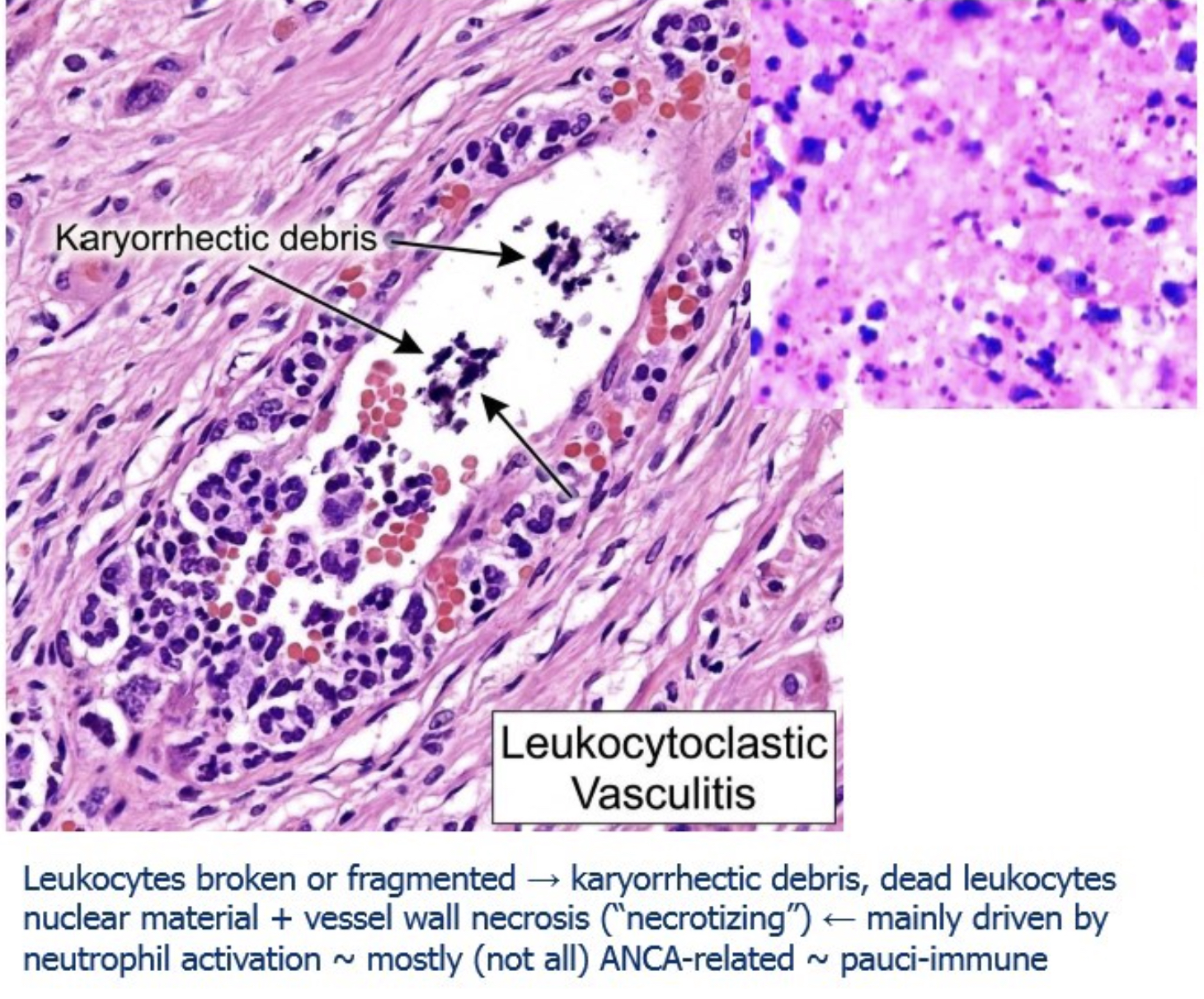
What is karyorrhectic debris?
Small dark dots in tissue representing fragmented nuclear material from dying/dead neutrophils; hallmark of leukocytoclastic vasculitis
What are the two ANCA staining patterns and their targets?
c-ANCA = cytoplasmic staining, targets PR3 (proteinase 3); p-ANCA = perinuclear staining, targets MPO (myeloperoxidase)
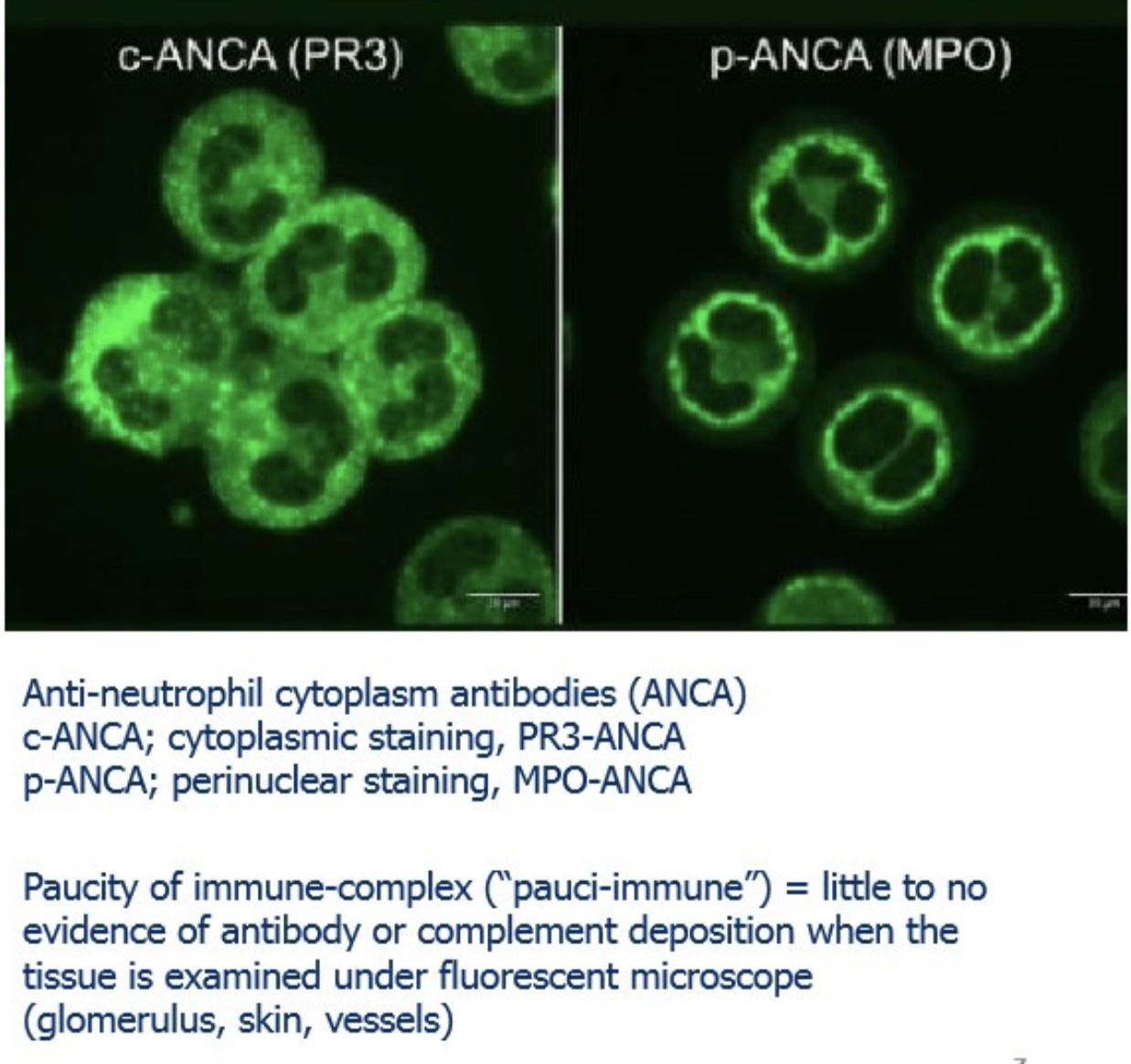
What is "pauci-immune" vasculitis?
Vasculitis with little to no evidence of antibody or complement deposition on immunofluorescence; seen in ANCA-related vasculitides (main mechanism is neutrophil activation, not immune complex deposition)
Why is ANCA-related vasculitis called pauci-immune?
Because the primary mechanism is neutrophil hyperactivation by ANCA antibodies — not immune complex deposition — so immunofluorescence shows no/minimal immune deposits in tissue
What is thromboangiitis (thrombo-angiitis)?
Combination of thrombosis + vascular inflammation with neutrophils within the same vessel
Which vasculitides affect large vessels and what is their key pathological feature?
Large vessel vasculitis affects the aorta and its major branches and is typically granulomatous inflammation seen on histo. Main types are Giant cell arteritis and Takayasu arteritis.
"What are the main types of medium vessel vasculitis and their mechanisms?
"Medium-sized arteries are affected. Two main types:
Immune complex–mediated: Polyarteritis nodosa
Anti-endothelial antibodies: Kawasaki disease"
How is small vessel vasculitis classified and what is the role of immune complexes?
Arterioles, venules, capillaries, occasionally small arteries; examples: Wegener's (PR3-ANCA), Churg-Strauss (MPO-ANCA), Microscopic polyangiitis (MPO-ANCA)
What is Giant Cell Arteritis (GCA) and who does it affect?
Chronic granulomatous inflammation of large to small arteries; most common systemic vasculitis in adults; affects patients >50 years old.
What are the local symptoms of Giant Cell Arteritis?
Facial pain/headache along superficial temporal artery (painful to palpation); ocular symptoms (~50%) including diplopia and vision loss (Amaurosis Fugax); rarely aortic involvement → thoracic aortic aneurysm
What is Amaurosis Fugax and how does it relate to GCA?
Transient monocular vision loss due to involvement of ophthalmic artery branches in GCA; can become permanent
What is the immune mechanism of Giant Cell Arteritis?
Segmental (“skip lesion”) granulomatous vasculitis of large arteries driven mainly by a T-cell–mediated immune response (trigger unknown), with cytokines like TNF playing a key role. It may also involve anti-endothelial antibodies and is associated with certain HLA types, and it typically responds well to steroids + some contribution from anti-endothelial cell humoral responses
What supports an immune etiology in Giant Cell Arteritis?
Granulomatous reaction histology, association with HLA class II haplotypes, and therapeutic response to steroids
What is the macroscopic appearance of Giant Cell Arteritis?
Arterial segments develop nodular intimal thickening (with occasional thrombosis) that reduces luminal diameter that can lead to ischemia; can appear as palpable nodules on the scalp

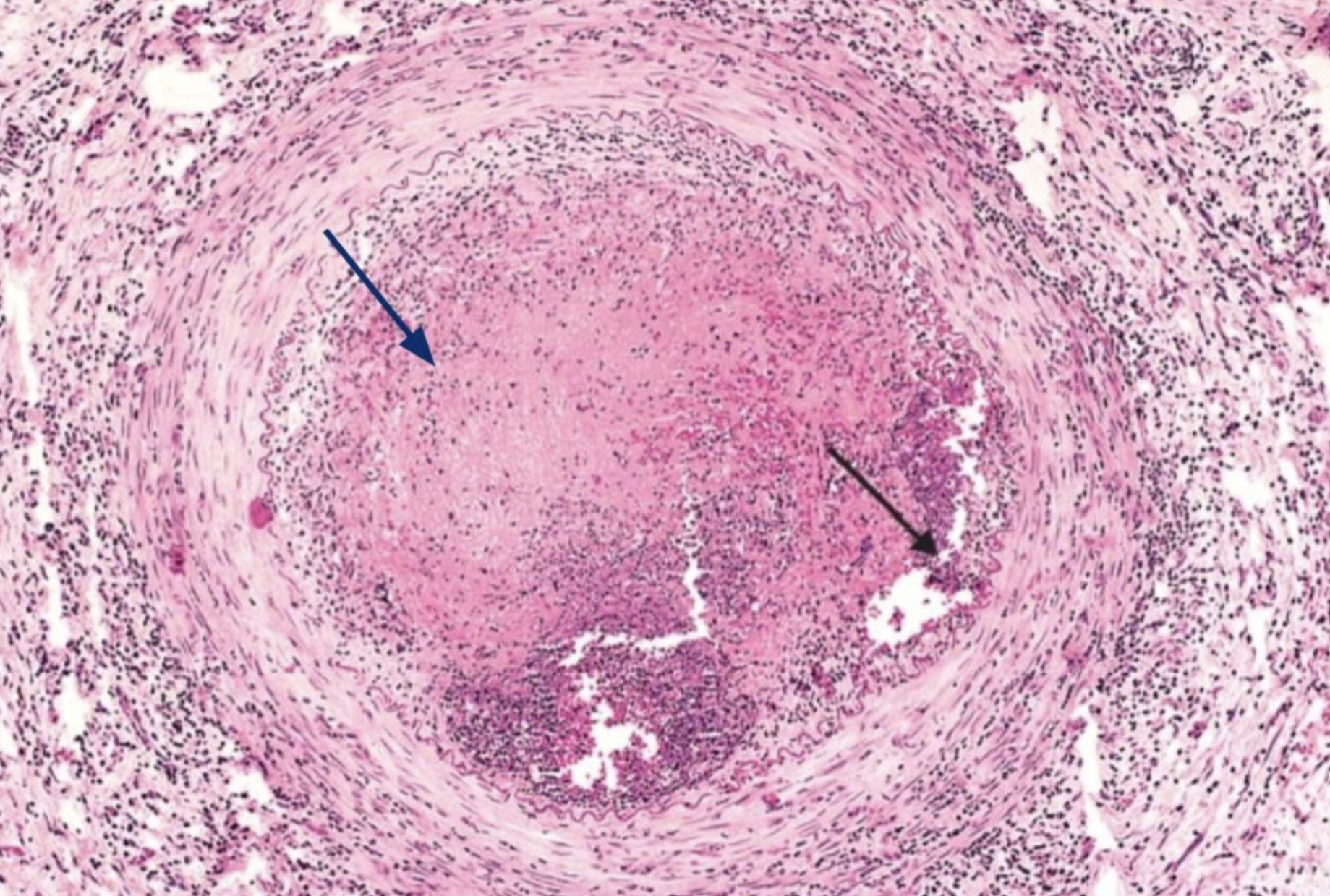
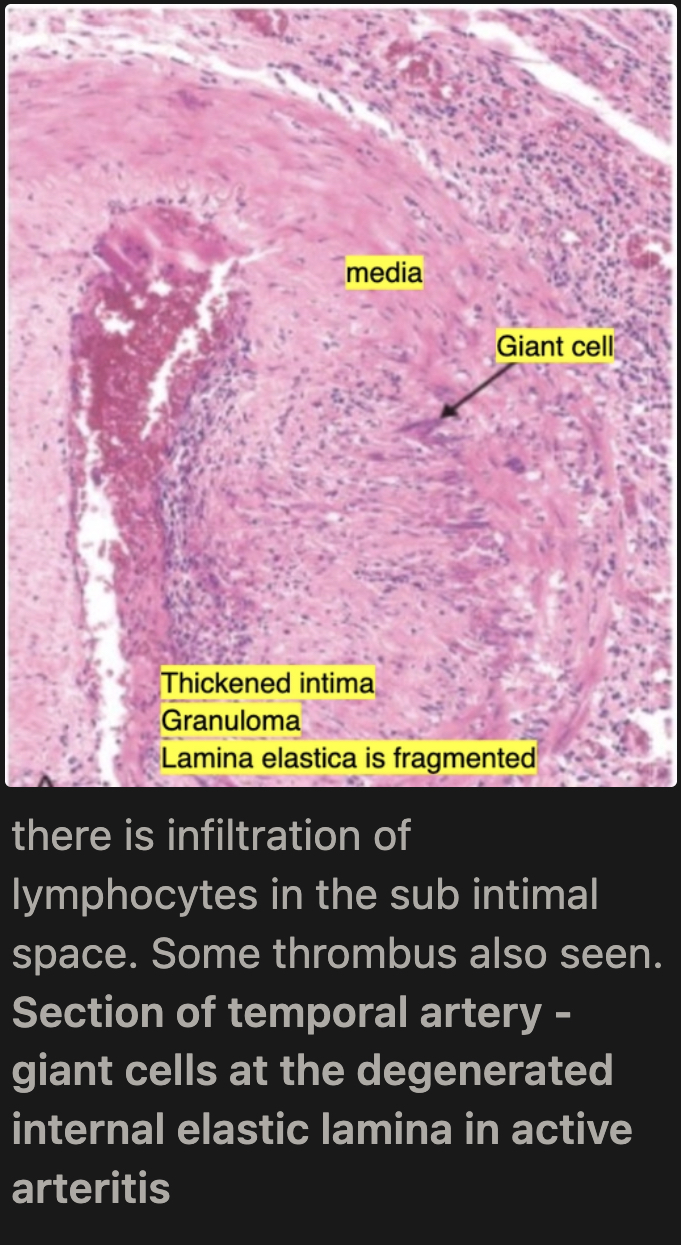
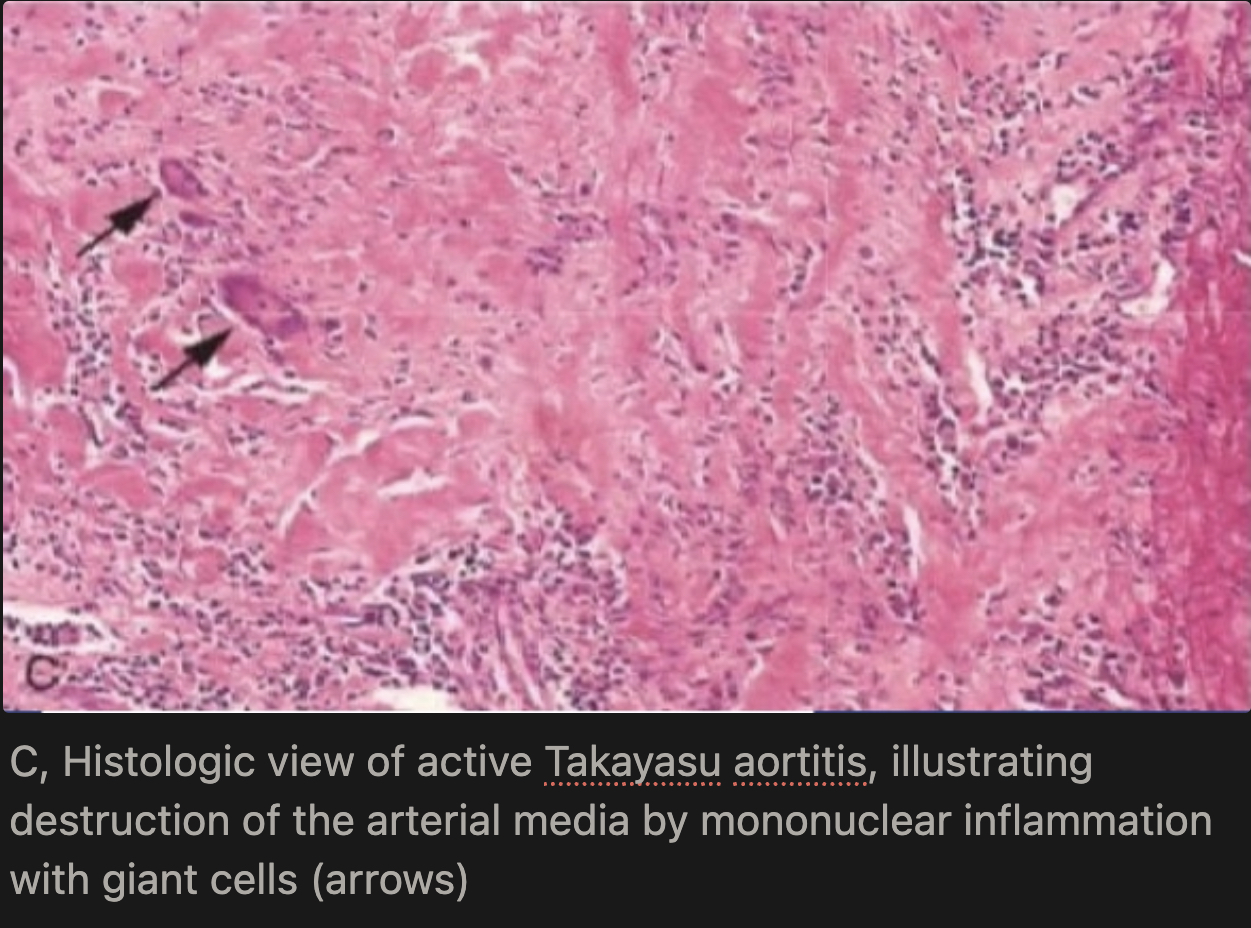
What is the microscopic appearance of Giant Cell Arteritis in the active phase?
Medial granulomatous inflammation (T cells and macrophages) leading to elastic lamina fragmentation/destruction
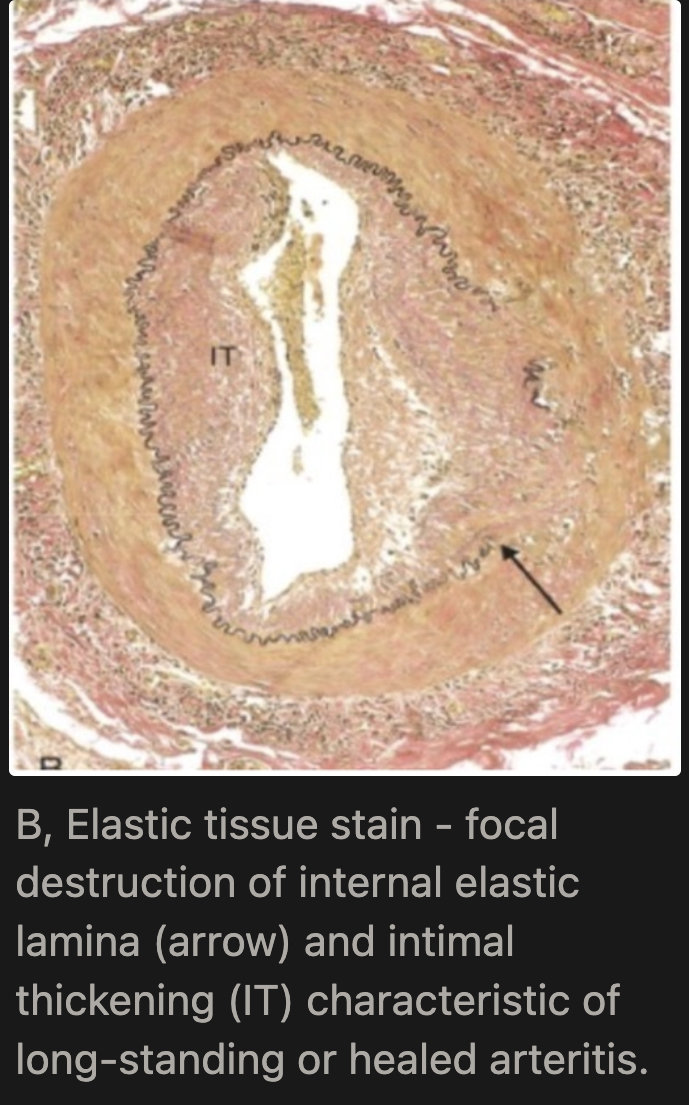
What is the microscopic appearance of Giant Cell Arteritis in the healed phase?
Medial scarring, intimal thickening, and residual elastic tissue fragmentation (seen on elastic tissue stain), followed by fibrosis → permanent vessel wall changes
What is the key histological feature distinguishing active vs. healed GCA?
Active: Multinucleated giant cells are present → these are large inflammatory cells formed by fused macrophages.
They are usually found near the internal elastic lamina (the elastic layer between the intima and media of the artery).
This elastic lamina becomes fragmented and degenerated because the inflammation is attacking it.
Healed: The internal elastic lamina is focally destroyed (parts of it are broken/lost)
The intima becomes thickened (intimal thickening) due to healing/scarring
No giant cells are seen because the active inflammation is gone
What is Takayasu Arteritis and who does it affect?
Granulomatous vasculitis of large and medium arteries (aorta and major branches); predominantly affects females younger than 40 years
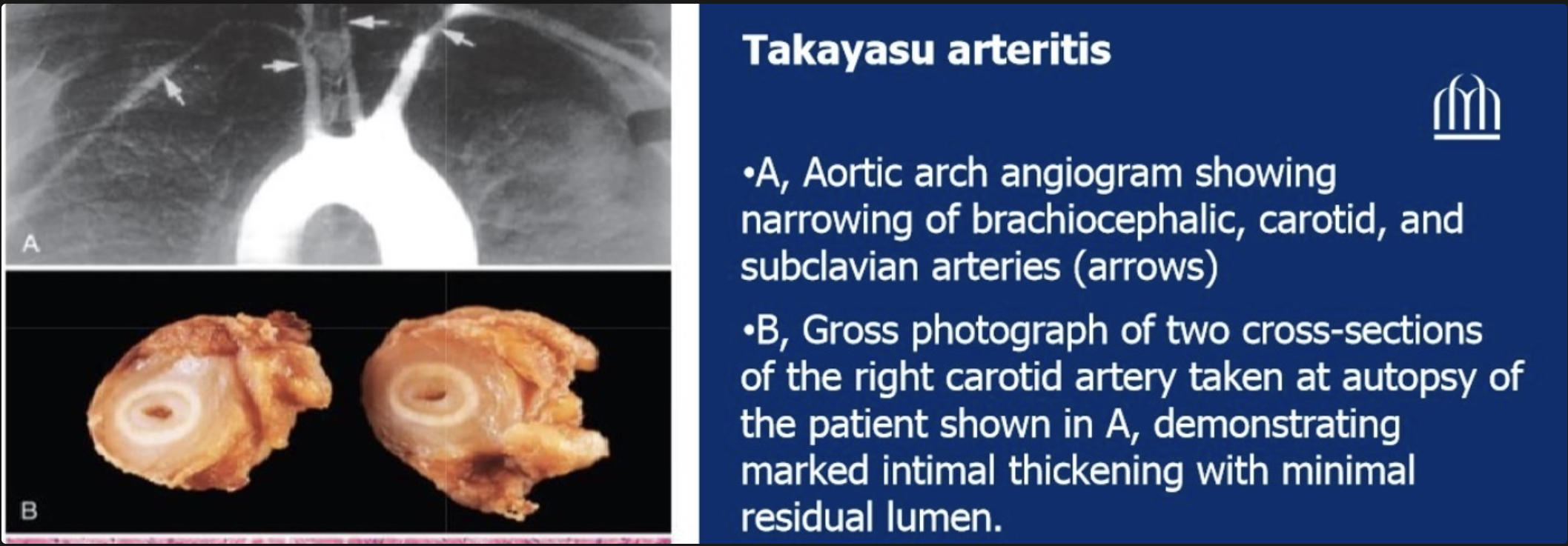
Why is Takayasu Arteritis called "pulseless disease"?
Inflammation and subsequent fibrous thickening narrow the aortic arch and brachiocephalic/subclavian arteries → markedly weakened or absent upper extremity pulses + ocular disturbances
What is the etiology of Takayasu Arteritis?
Unknown, but autoimmune mechanism suspected based on clinical features
What are the clinical manifestations of Takayasu Arteritis?
Reduced BP (in the limbs) and weak pulses in upper extremities, cold/numb fingers, ocular disturbances (carotid artery), neurologic deficits, hypertension (renal artery), leg claudication (distal aorta/femoral artery), pulmonary hypertension, myocardial infarction (coronary artery)
What is the macroscopic appearance of Takayasu Arteritis?
Irregular thickening of vessel wall with intimal thickening; great vessel lumens markedly narrowed or obliterated
What is the microscopic progression in Takayasu Arteritis?
Early on, inflammation starts in the outer layer (adventitia) with mononuclear cells clustering around the small vessels (vasa vasorum), then spreads into the media, where it becomes granulomatous with giant cells and causes patchy necrosis. Later, as healing occurs, the vessel wall develops collagen scarring with chronic inflammation affecting all three layers (adventitia, media, and intima), leading to permanent structural damage.
What cardiac complication can occur in Takayasu Arteritis involving the aortic root?
Aortic valve insufficiency (due to distortion and damage of aortic valve)
How do Giant Cell Arteritis and Takayasu Arteritis differ clinically?
GCA: age >50, external carotid branches (temporal), headache/jaw claudication/scalp pain, vision loss common; Takayasu: age <40, female, aorta + major branches, "pulseless disease" (weak limb pulses), visual loss rare
How do Giant Cell Arteritis and Takayasu Arteritis compare histologically?
Histologically almost identical — both show granulomatous inflammation with giant cells; differentiated by age, sex, and anatomy location
What is Polyarteritis Nodosa (PAN)?
Systemic vasculitis of medium-sized and small muscular arteries; typically involving renal and other visceral vessels; spares pulmonary circulation
Who is typically affected by PAN?
Young adults primarily, but can occur in pediatric and geriatric populations
What are the key clinical features of PAN?
Malaise, fever, weight loss; renal artery involvement → rapid hypertension (major cause of death); abdominal pain and melena due to vasc lesions in the GI; diffuse muscle aches; multiple skin nodules (nodosa); peripheral neuritis
Why does PAN cause hypertension but NOT glomerulonephritis?
PAN involves medium/small muscular arteries but does NOT involve capillaries (glomerular capillaries are spared); thus hypertension results from renal artery disease but glomerulonephritis does not occur
What is the macroscopic appearance of PAN?
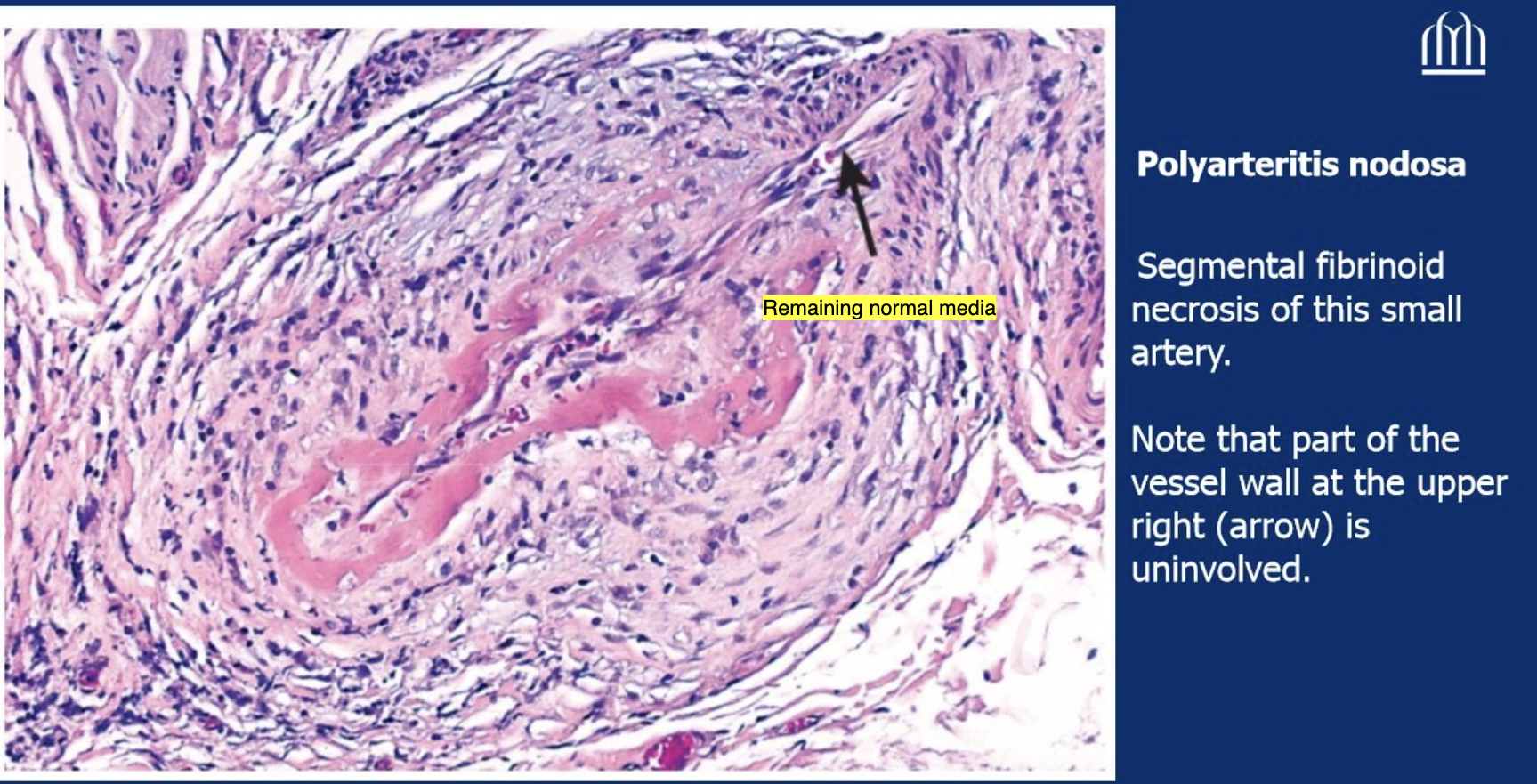
Segmental transmural necrotizing inflammation of vessel wall; lesions affect only part of circumference (segmental); Prefers branch points of vessels; weakens the vessel wall → can cause aneurysm or rupture, leading to infarction, ulcers, and bleeding.
What is the microscopic appearance of PAN in the acute phase?
there is fibrinoid necrosis with neutrophil-rich inflammation (sometimes with eosinophils), followed by mononuclear cell infiltration
What is the microscopic appearance of PAN in the chronic phase?
Fibrous thickening of vessel wall extending into adventitia
What is the characteristic temporal feature of PAN lesions?
All stages of activity (early to late) coexist in different vessels or even within the same vessel — lesions of DIFFERENT ages (unlike microscopic polyangiitis where lesions are same age)
What is the treatment of PAN and its prognosis?
Untreated: usually fatal; Treated with corticosteroids + cyclophosphamide → remissions or cures in ~90% of cases
Describe the image
Lumen is totally obliterated, neutrophils + chronic inflammatory cells are infiltrating the lumen; certain segments are necrotized but there is also remaining normal component.
What is Kawasaki Disease?
Acute febrile, usually self-limited illness of infancy and childhood (80% <4 years); arteritis affecting large to medium-sized, and even small vessels; also called mucocutaneous lymph node syndrome
What are the clinical features of Kawasaki Disease (muco-cutaneous-lymph node breakdown)?
Muco: conjunctival and oral erythema/erosion; Cutaneous: edema of hands/feet, erythema of palms/soles, desquamative rash (excessive shedding, peeling, or scaling of the skin's top layer (stratum corneum)); Lymph node: cervical lymphadenopathy
What is the major feared complication of Kawasaki Disease?
About 20% of patients have coronary artery involvement: the arteries dilate (ectasia) → can form large aneurysms (7–8 mm) → which may rupture or form clots → leading to heart attack and possible sudden death.
What is the pathogenesis of Kawasaki Disease?
Likely triggered by a viral infection in genetically susceptible children → activates T-cells and macrophages → cytokine release and B-cell activation → autoantibodies attack blood vessel endothelial and smooth muscle cells → causes acute vasculitis.
What is the histological appearance of Kawasaki Disease vs. PAN?
Kawasaki: inflammation of entire vessel wall thickness with necrosis, BUT fibrinoid necrosis is less prominent than in PAN; Kawasaki also involves the FULL circumference (transmural), not segmental like PAN. Healed lesions may have obstructive intimal thickening
What happens after the acute vasculitis in Kawasaki Disease subsides spontaneously?
Aneurysm formation + thrombosis can occur; healed lesions may develop obstructive intimal thickening
What is Microscopic Polyangiitis (MPA)?
Pauci-immune, leukocytoclastic vasculitis affecting small vessels (arterioles, capillaries, venules); associated with MPO-ANCA (p-ANCA)
How does Microscopic Polyangiitis differ from PAN?
MPA affects smaller vessels (arterioles, capillaries, venules) vs. PAN (medium arteries); MPA has pauci-immune pattern; MPA lesions are all the SAME age vs. PAN lesions are DIFFERENT ages; MPA causes necrotizing glomerulonephritis (90%), PAN does not
What are the clinical features of Microscopic Polyangiitis?
Hemoptysis (pulmonary capillaritis), hematuria and proteinuria (necrotizing glomerulonephritis in 90%), bowel pain/bleeding, muscle pain/weakness, palpable cutaneous purpura; renal or brain involvement = severe/fatal disease
What is the histological appearance of Microscopic Polyangiitis?
Segmental necrotizing vasculitis of capillaries/arterioles/venules; fibrinoid necrosis of media; leukocytoclastic vasculitis (karyorrhectic debris of neutrophils); all lesions are SAME age; pauci-immune on immunofluorescence
What is the treatment of Microscopic Polyangiitis?
Cyclophosphamide + steroids → induces remission and improves long-term survival
What is Churg-Strauss Syndrome (CSS)?
Also called allergic granulomatosis and angiitis; small vessel necrotizing vasculitis classically associated with asthma, allergic rhinitis, lung infiltrates, peripheral hypereosinophilia, and extravascular necrotizing granulomas
What are the three major components of Churg-Strauss Syndrome?
1) Allergic (asthma, allergic rhinitis, hypereosinophilia), 2) Granulomatous inflammation, 3) Microscopic PAN-like small vessel necrotizing vasculitis (leukocytoclastic)
What ANCA is associated with Churg-Strauss Syndrome?
MPO-ANCA (p-ANCA); present in less than 50% of cases
What are the clinical features of Churg-Strauss Syndrome?
Cutaneous palpable purpura, GI bleeding, renal disease (focal and segmental glomerulosclerosis), eosinophilic myocardial infiltrates → cardiomyopathy (heart involved in 60%; accounts for ~50% of deaths)
What is the pathogenic trigger hypothesized in Churg-Strauss Syndrome?
Hyperresponsiveness to an allergic stimulus; in asthmatics, leukotriene receptor antagonists have been reported as a trigger
What is the histological appearance of Churg-Strauss Syndrome?
Similar to PAN or microscopic polyangiitis PLUS granulomas and abundant eosinophils in vessel wall and soft tissue
What is Wegener's Granulomatosis (GPA) and what is its classic triad?
Now called Granulomatosis with Polyangiitis (GPA); classic triad: 1) necrotizing granulomatous angiitis, 2) necrotizing granulomas of upper and/or lower respiratory tract, 3) renal disease (focal necrotizing glomerulonephritis) [nose, lungs and kidneys)
Who is typically affected by Wegener's GPA?
Males > females; average age 40 (peak in fifth decade)
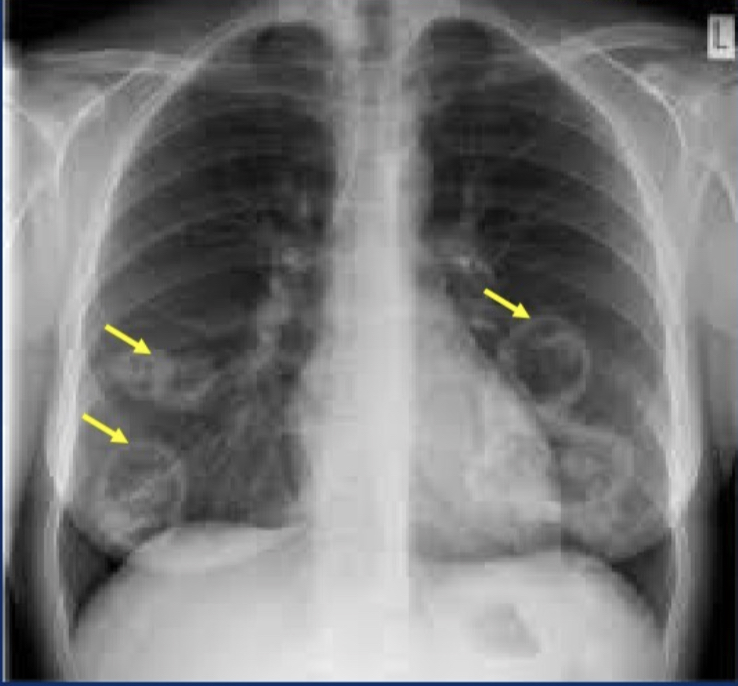
What are the typical clinical features of Wegener's GPA?
Persistent pneumonia with bilateral nodular/cavitary infiltrates (95%), chronic sinusitis (90%), mucosal ulcerations of nasopharynx (75%), evidence of renal disease (80%); also skin rash, muscle pain, joint and nerve involvement, mononeuritis or polyneuritis
What ANCA is associated with Wegener's GPA?
c-ANCA (PR3-ANCA); present in up to 95% of cases; useful marker of disease activity
What is the pathogenesis of Wegener's GPA?
T-cell mediated hypersensitivity reaction, likely triggered by inhaled infectious or environmental agent in upper respiratory tract → granuloma formation; c-ANCA may participate in pathogenesis
What is the microscopic appearance of Wegener's GPA in the sinuses/airways?
Inflammatory sinusitis with mucosal granulomas → ulcerative lesions of nose, palate, pharynx rimmed by granulomas with geographic patterns of central necrosis + vasculitis (must distinguish from mycobacterial/fungal infections) [Necrotizing vasculitis + granulomatous inflammation + giant cells]
![<p>Inflammatory sinusitis with mucosal granulomas → ulcerative lesions of nose, palate, pharynx rimmed by granulomas with geographic patterns of central necrosis + vasculitis (must distinguish from mycobacterial/fungal infections) [Necrotizing vasculitis + granulomatous inflammation + giant cells]</p>](https://assets.knowt.com/user-attachments/3091869d-dbb4-43a7-987b-4b7977d2fcda.jpg)
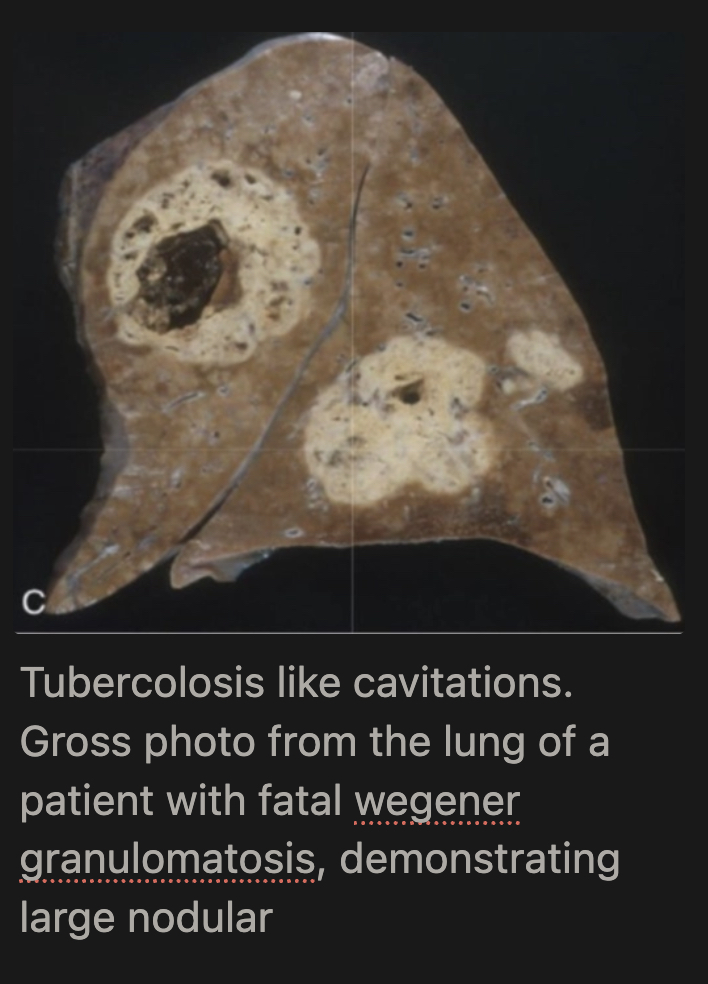
What happens to lung granulomas in Wegener's GPA?
Multiple granulomas coalesce → radiographically visible nodules that can cavitate; late stage = extensive necrotizing granulomatous involvement of parenchyma
What are the renal lesions in Wegener's GPA?
Focal and segmental necrotizing glomerulonephritis; crescentic glomerulonephritis
What is the prognosis of untreated Wegener's GPA?
80% of patients die within 1 year if untreated; rapidly fatal
What is the treatment of Wegener's GPA?
Steroids + cyclophosphamide + TNF antagonists → turns it into a chronic remitting/relapsing disease
How does Wegener's GPA differ from Churg-Strauss syndrome?
Both have granulomas + small vessel necrotizing vasculitis + ANCA; Churg-Strauss has allergic component (asthma, hypereosinophilia, eosinophilic infiltration); Wegener's has no eosinophilia/allergy but has prominent upper/lower respiratory destruction and c-ANCA vs. p-ANCA in CSS
What is Thromboangiitis Obliterans (Buerger's Disease)?
Distinctive disease of segmental, thrombosing, acute and chronic inflammation of medium-sized and small arteries, principally tibial and radial arteries; with secondary extension into surrounding veins and nerves
What is the strongest risk factor for Thromboangiitis Obliterans?
Cigarette smoking — the most consistent association; abstinence in early stages often brings dramatic relief
What is the pathogenesis of Thromboangiitis Obliterans?
Unknown — thought to be an idiosyncratic reaction/genetic predisposition to cigarette smoke; NOT autoimmune or infectious
Who typically develops Thromboangiitis Obliterans?
Young male heavy smokers; affects lower leg/foot/toes and hand/fingers
What are the early clinical features of Buerger's Disease?
Superficial nodular phlebitis, cold sensitivity/Raynaud-type phenomenon in hands, instep claudication (pain in arch of foot on exercise)
What are the late/chronic clinical features of Buerger's Disease?
Severe resting pain (from neural involvement), chronic ulcerations of toes/feet/fingers → frank gangrene
What is the microscopic appearance of Buerger's Disease in the acute stage?
Lumen occluded by thrombus containing microabscesses (neutrophilic); vessel wall infiltrated with leukocytes
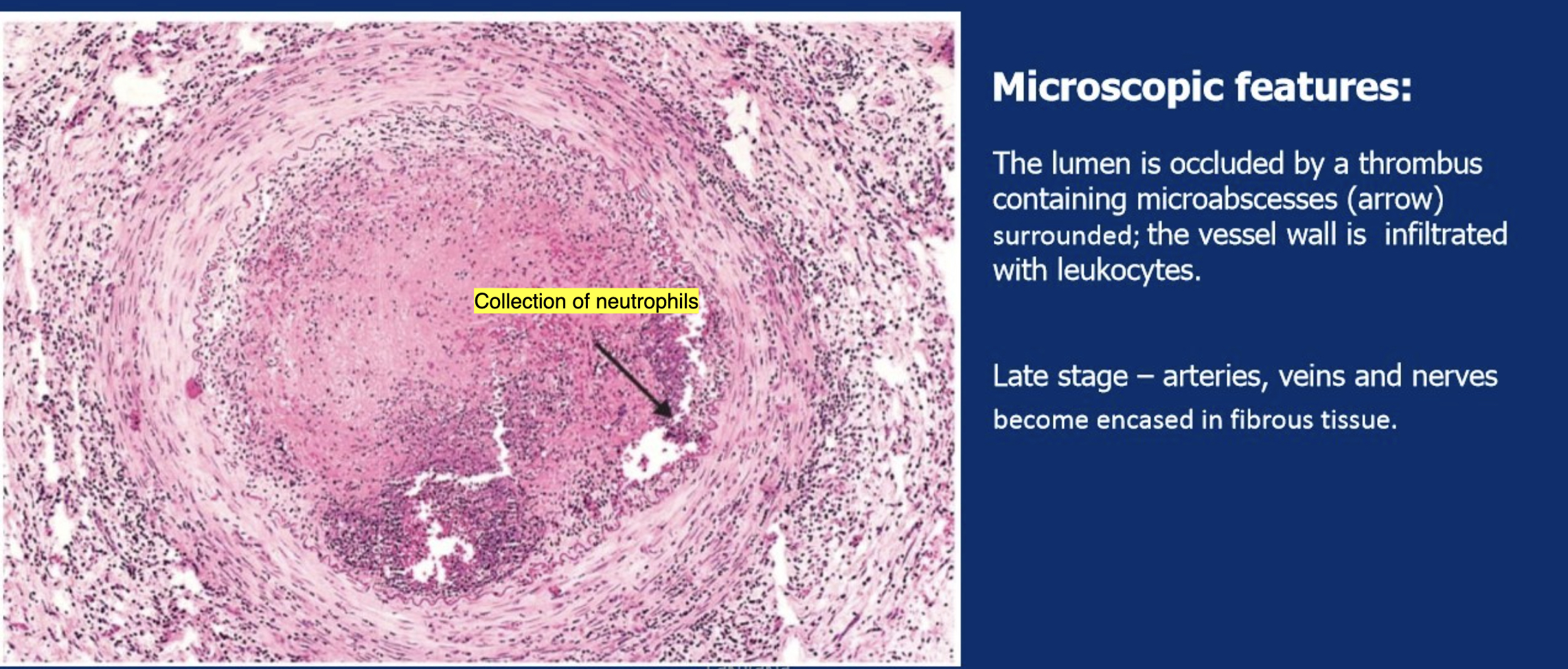
What is the microscopic appearance of Buerger's Disease in the late stage?
Arteries, veins, and nerves become encased in fibrous tissue; lumen obliterated by fibrosis
What is the key clinical difference between Buerger's Disease and atherosclerotic peripheral artery disease?
Buerger's affects young smokers, involves tibial/radial arteries + secondary venous and neural involvement; atherosclerosis affects older patients with conventional risk factors
What is the clinical summary clue for Giant Cell Arteritis?
Elderly patient + constitutional symptoms + headache/facial pain/scalp tenderness/visual symptoms + granulomatous inflammation with giant cells in external carotid artery branches (temporal artery)
What is the clinical summary clue for Takayasu Arteritis?
Young woman + multiple symptoms from aortic branches (extremities, ocular symptoms, etc.) + granulomatous inflammation with giant cells in aorta and major branches
What is the clinical summary clue for PAN?
Young adult + multiorgan symptoms (acute hypertension, abdominal pain, melena, skin nodules) + segmental fibrinoid/necrotizing transmural necrosis of medium arteries in DIFFERENT stages
What is the clinical summary clue for Kawasaki Disease?
Children + cervical lymphadenopathy + mucosa/skin involvement + 20% cardiac complications + transmural necrosis of artery (especially coronary)
What is the clinical summary clue for Microscopic Polyangiitis?
Elderly + acute renal failure/hematuria/proteinuria + hemoptysis + skin lesions + transmural necrosis of small vessels with karyorrhectic debris (leukocytoclastic) + pauci-immune + p-ANCA (MPO)
What is the clinical summary clue for Churg-Strauss Syndrome?
Adults + asthma/sinusitis/hypereosinophilia (allergic) + skin/peripheral nerve/heart symptoms + acute GN + p-ANCA (MPO) + necrotizing vasculitis in small vessels WITH granuloma + eosinophilic infiltration + pauci-immune
What is the clinical summary clue for Wegener's GPA?
Adults + upper and lower respiratory symptoms with tissue destruction (cavitations) + acute GN + c-ANCA (PR3) + granuloma and geographic tissue necrosis with necrotizing vasculitis in small vessels + pauci-immune
What is the clinical summary clue for Thromboangiitis Obliterans (Buerger's)?
Young heavy smoker + lower leg/foot/toe or hand/finger symptoms + neutrophilic vasculitis with thrombus containing microabscesses in medium-to-small arteries
What immunofluorescence pattern is seen in ANCA-related vasculitides (MPA, GPA, CSS)?
Pauci-immune = little to no deposition of IgG/IgM/IgA or complement in tissue on immunofluorescence (because mechanism is neutrophil activation, not immune complex deposition)
What immunofluorescence pattern is seen in immune complex vasculitides (SLE, IgA, cryoglobulin)?
Bright deposition of immune complexes (IgG, IgA, IgM, complement) seen on immunofluorescence in affected vessels/glomeruli
How does the age of lesions differ between PAN and Microscopic Polyangiitis?
PAN: lesions are of DIFFERENT ages (temporal heterogeneity — early, mid, and late stage coexist); MPA: all lesions are the SAME age
Which vasculitis spares the pulmonary circulation?
Polyarteritis Nodosa (PAN)