1.07 Topical Anaesthetics
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
types of anaesthetic
general - whole body
local - temporarily numbing a specific area of the body (can be administered by injection, or can diffuse across a mucous membrane (topical))
analgesia definition
pain relief without a total loss of sensation
can still move that part of the body
anaesthesia definition
pain relief with associated loss of sensation (and perhaps loss of motor control and consciousness)
uses for topical anaesthetics for optoms
anaesthetia of the anterior ocular surface (topical) to enable diagnostic procedures
contact tonometry (GAT)
gonioscopy/fundus cls (view anterior angle)
ultrasonography (measure axial length)
ocular blood flow measurement
superficial foreign body removal
impressions for scleral cls
insertion of punctal plugs/lacrimal syringing (treating dry eye)
increases the efficacy of other ophthalmic drugs by increasing permeability of the cornea (controversial)
legal aspects -
how many topical anaesthetics do optoms have access to
what medicine classification are they
optoms have access to 4 topical anaesthetics
they are all POMs USE only - must never be supplied to pts under any circumstances
why is the overuse of topical anaesthetics bad
slows down corneas ability to self heal
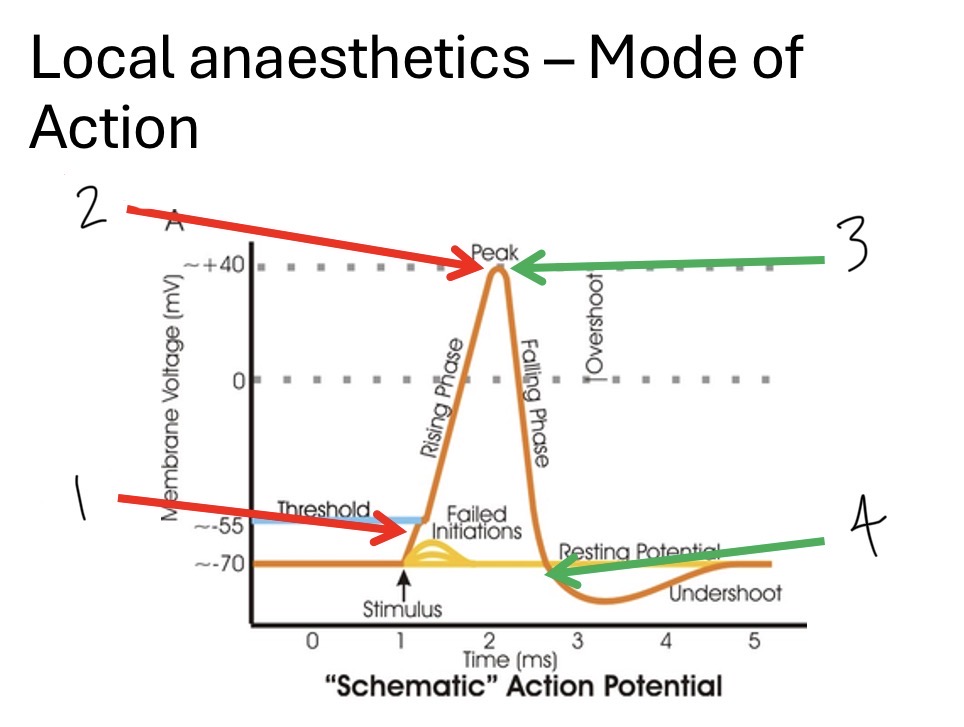
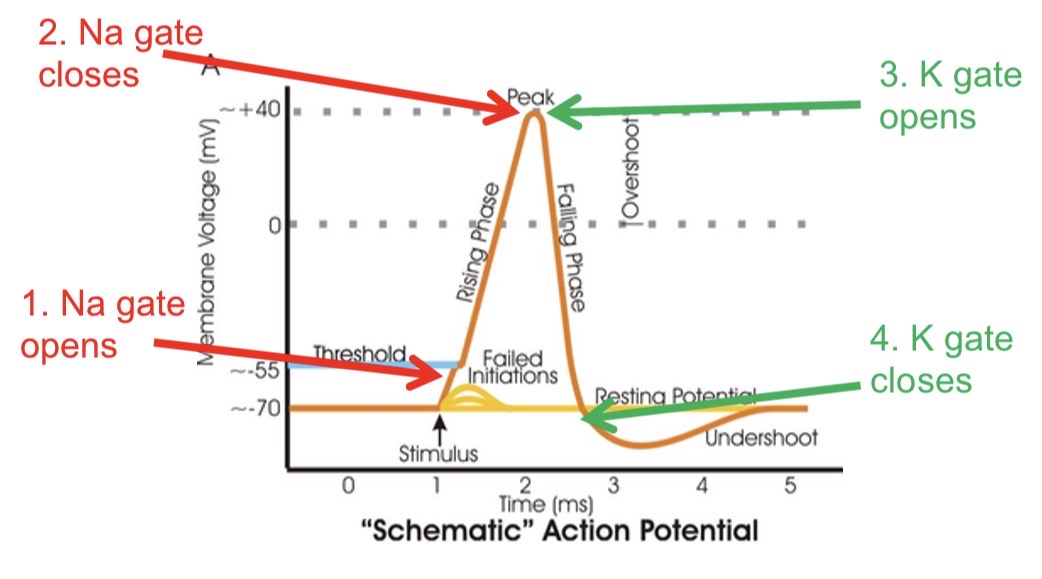
describe what gates are opening/closing at each part of the graph
Na gate opens
Na gate closes
K gate opens
K gate closes
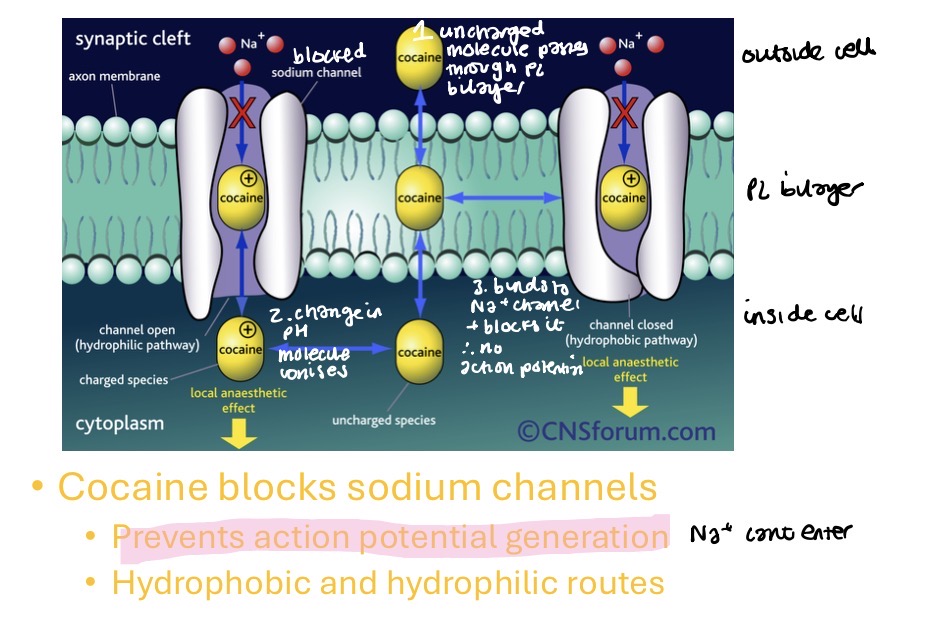
how do topical anaesthetics work
the active agent is a weak base (it is administered in an acidic solution - hydrochloride) increases solubility and stability in water
uncharged molecule passes through phospholipid bilayer
change in pH. molecule becomes ionised (therefore easier to pass membrane)
binds to Na+ channel and blocks it. therefore no action potential (Na+ cant enter so nerve cell cant depolarise)
relationship between blockage of conduction and concentration of drug
blockage of conduction within a nerve is related to nerve diameter - higher concentration of drug required to block thicker nerves
sensory nerves of the cornea are thin (dont have a myelin sheath) so its easy to induce a blockade using a topical drug
neural block occurs in what order
pain blockade
touch blockade
temperature blockade
pressure blockade
motor blockade (paralysis)
ideal properties of topical anesthetics
rapid onset of a depth of anaethesia sufficient to enable procedure to take place comfortably eg applanation of the cornea
sufficient duration
rapid recovery
complete recovery
no adverse reaction to the drug
cheap
easy to store
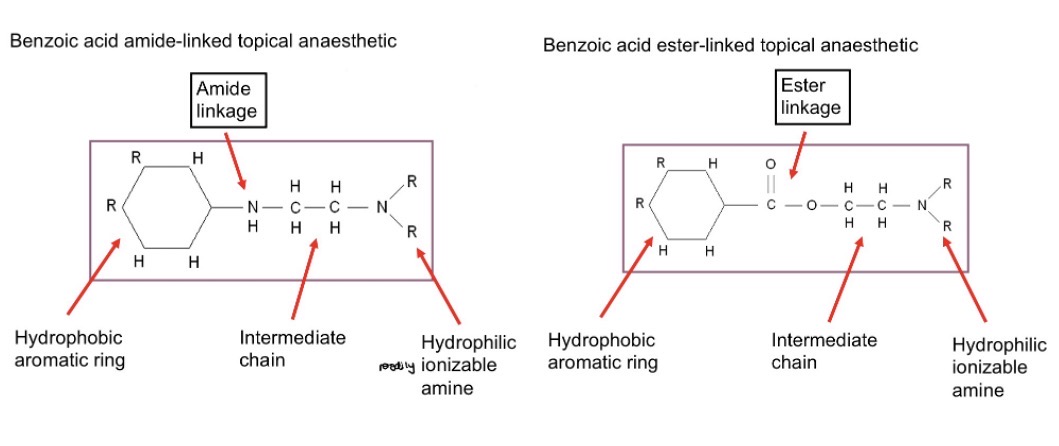
molecular structure of topical anaesthetics
a hydrophobic aromatic ring structure
and
a hydrophilic amine structure, with intermediate chain
linked by either:
(lidocaine) an amide linkage
drug is resistant to break down
longer duration of action than ester linked TAs
allergic reaction much rarer
(other TAs) an ester linkage
drug is rapidly broken down
therefore short duration of action
allergic reaction is common (due to products when drug is metabolised)
why do we want TA molecules to be charged or uncharged
uncharged for passing through cornea
charged when storing to keep it stable and so it can bind to Na+ channels
what are the topical anaesthetics available to optoms
benzoic acid amide linkage
lidocaine hydrochloride
benzoic acid ester linkage
proxymetacaine hydrochloride
oxybuprocaine hydrochloride
tetracaine hydrochloride
what is lidocaine hydrochloride available as and the concentration
available as
minims lidocaine and fluorescein (pre mixed with fl)
4% lidocaine hcl with 0.25% fl in a 0.5 ml single unit
what link does lidocaine have
amide
what temperature should we store lidocaine at
below 25 degrees c
pros and cons of lidocaine
pros - lower risk of adverse reaction to the drug (corneal desquamation)
stings more than benoxinate and proxymetacaine
what is proxymetacaine hydrochloride available as
available as
minims proxymetacaine
0.5% proxymetacaine hydrochloride
what temperature should we store proxymetacaine hcl
2-8 degrees c
in the fridge
what is the link in proxymetacaine
ester
what is the most commonly used TA in optometry
proxymetacaine hcl
what is oxybuprocaine hcl available as
minims oxybuprocaine
0.4% oxybuprocaine hcl
temperature to store oxybuprocaine
below 25 degrees c
what is the link in oxybuprocaine
ester
what is tetracaine hcl available as
minims tetracaine
0.5% and 1.0% tetracaine hcl
what temperature should tetracaine hcl be stored at
below 25 degrees c
what link is in tetracaine hcl
ester
why is tetracaine unpopular
it stings
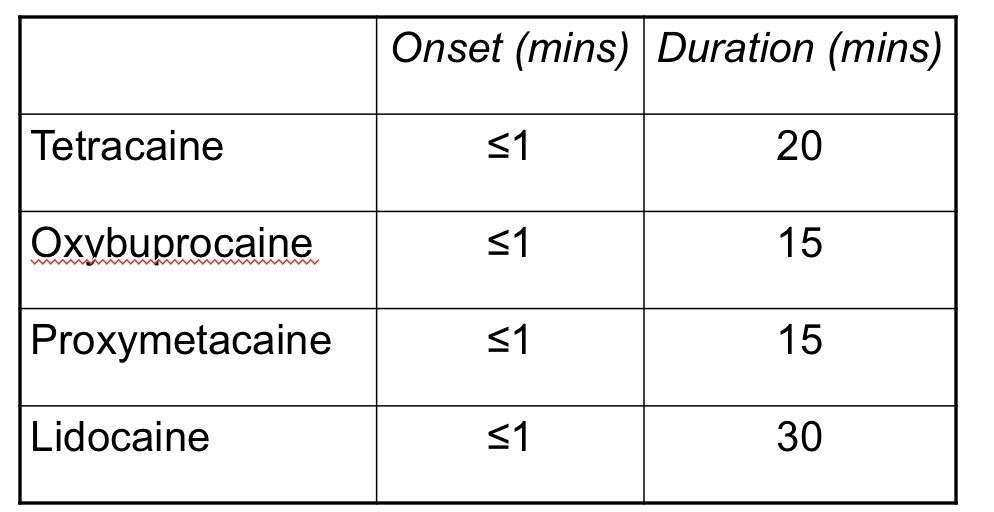
onset and duration of the 4 anaesthetics (slide 24)
adverse reactions to topical anaesthetics
stored in acidic solution so causes side effects
conjunctical hyperaemia
corneal oedema
punctate keratitis
transient blurred vision
stinging/burning sensation
decreased tear secretion
inhibition of blink reflex - eye vunerable to trauma
allergic reaction - can be delayed - 6-12 hrs following instillation
reaction at the corneal epithelium
loss of microvilli
localised or diffuse epithelial desquamation (accelerated loss of epithelium cells) - VA 6/60. spontaneous resolution (ocular lubricants may help)
severe reaction (melting cornea) rarely occurs - antibiotic prophylaxis
delayed wound healing
What should we measure before instillating anaesthesia
Visual acuity