Clin Med 2 - derm - Drug Reactions
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
1) Immediate reactions = less than 1 hour after first dose
2) Delayed reactions = after 1 hour, but usually more than 6 hours, or even weeks to months
Drug-Induced skin reactions are classified according to timing, what are the two types?
When do they occur?
1) Urticaria
2) Angioedema
3) Anaphylasis
What are the types of immediate drug reactions? (3)
1) Exanthematous eruption
2) Fixed drug eruption
3) Systemic reactions (SJS, TEN, DIHS)
4) Vasculitis
What are the types of delayed durg reactions? (4)
No, except for penicillin
(Skin testing of penicillin is preferred to IgE-mediated testing)
Is allergy testing effective for assessing a patients drug reaction?
1) Instilled (eye drops, ear drops)
2) Inhaled (steroids, beta adrenergic)
3) Ingested (capsules, tablets, syrup)
4) Inserted (suppositories)
5) Injected (IM, IV)
6) Incognito (herbs, non-traditional meds, homeopathic, vitamins, OTCs)
7) Intermittent (pts may not reveal meds they take on intermittent basis unless specifically asked)
A complete drug Hx should include the 7 I's. What are they?
Timing! The initiation of the medication is usually 7-10 days before the rash
What is the most important data to gather in determining a medication-related rash?
onset of rash
when determining a drug timeline, what is day 0
1) Female
2) Prior Hx of drug reaction
3) Recurrent drug exposure
4) HLA type (Human Leukocyte Antigen)
5) Certain disease states
What are risk factors for drug reactions? (5)
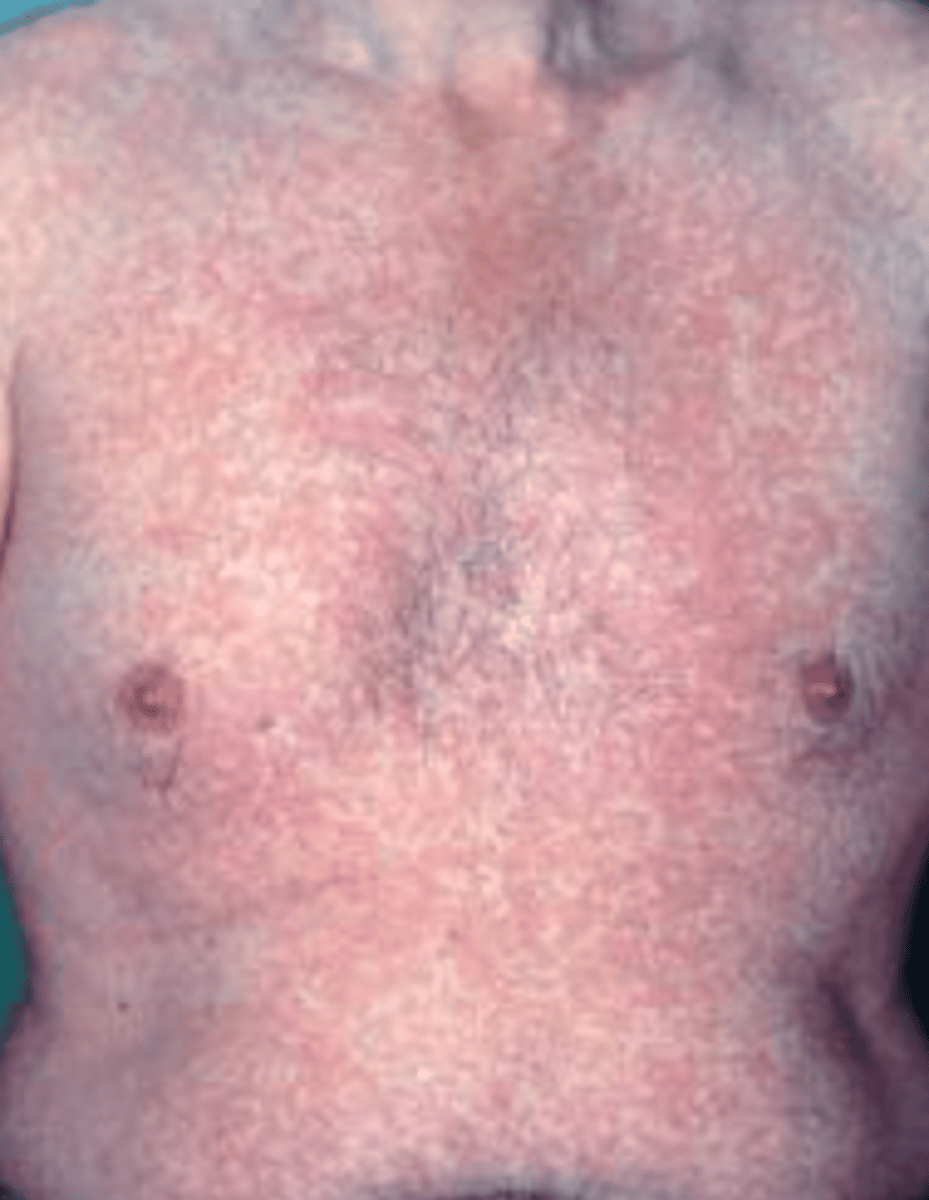
Morbilliform rash
This is a wide-spread, symmetric, erythematous macules and papules on the trunk and extremties that looks like a measles eruption.
Exanthematous rash
What type of drug reaction is this?
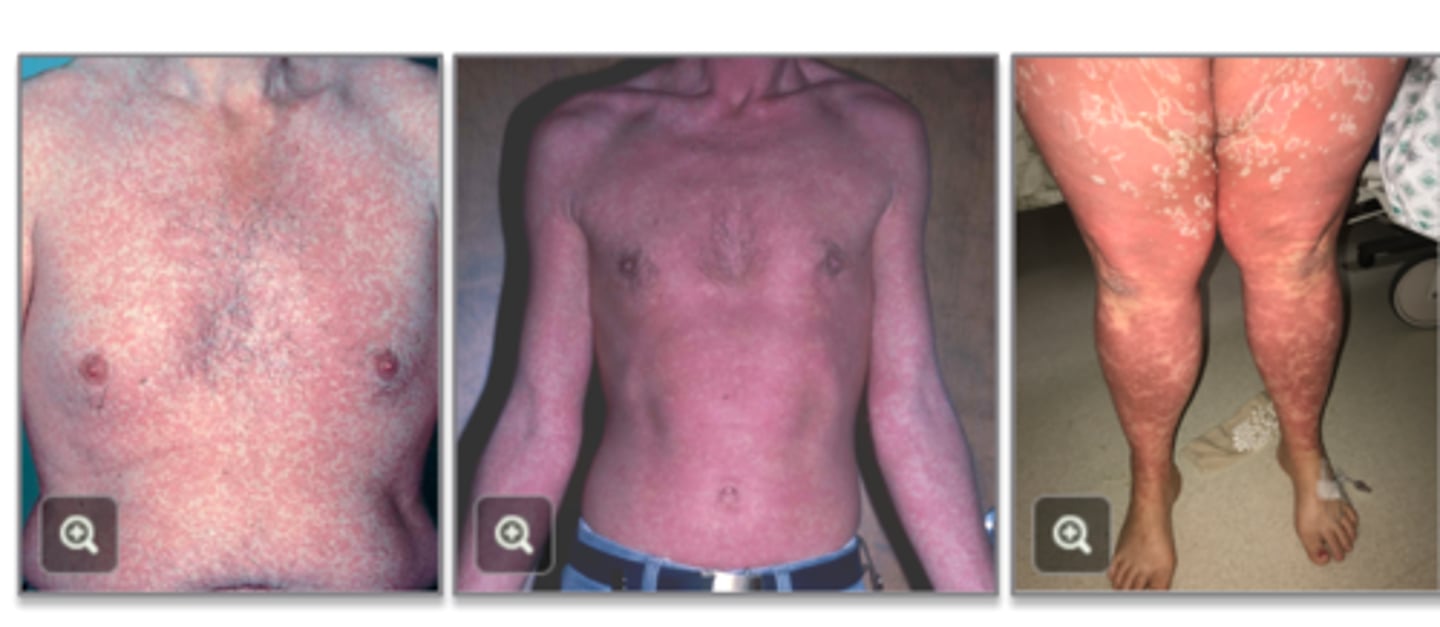
Exanthematous eruptions
What type of eruptions are the MC of all the cutaneous drug eruptions?
Exanthematous eruptions
This type of eruption has lesions that initially appear on the trunk and spread centrifugally to the extremities in a symmetric fashion and may have pruritus and mild fever.
Rash appears 7 to 10 days after drug initiation if it is the first episode, or 24 to 48 hours after repeat drug initiation.
resolves in a few days to a week after the medication is stopped (resolves w/o sequelae though extensive scaling/desquamation can occur)
On average, how long before exanthematous drug eruptions occur?
Yes, the medication can safely be continued if the eruption is not too severe and the medication cannot be substituted
Can a patient continue taking a medication after an exanthematous eruption?
Topical steroids, oral antihistamines, and reassurance
What is the treatment for exanthematous eruptions?
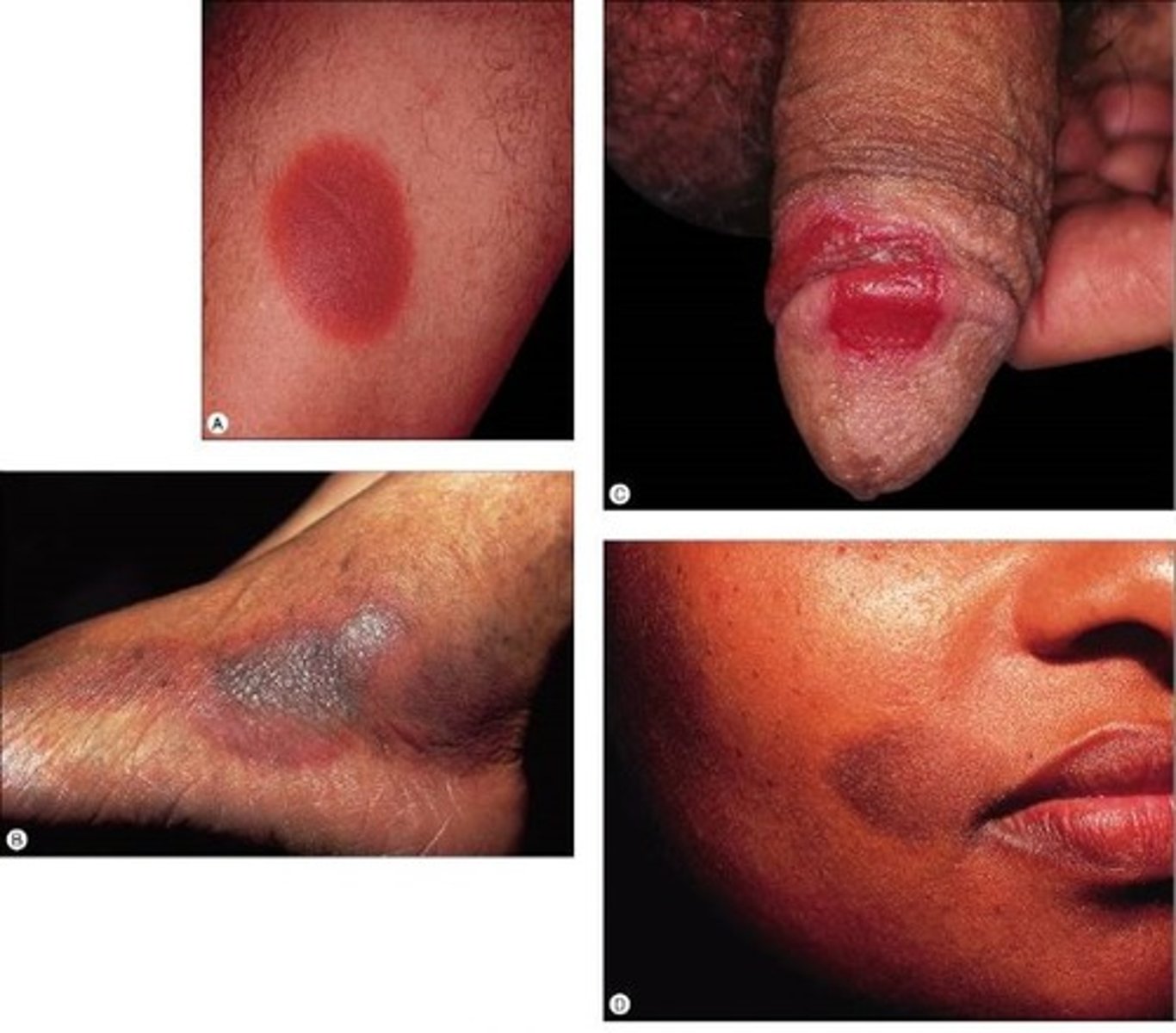
Fixed Drug Eruption
A patient comes in after this "spot" develops on her thigh (oval erythematous plaque with a central bulla). She was taking metronidazole for bacterial vaginosis. She had the same lesion 1 year ago. What is your DX?

Fixed Drug Eruption
This is a type of adverse drug reaction characterized by the formation of a SOLITARY erythematous patch or plaque that will recur at the same site with re-exposure to the drug.

1) Phenolphthalein (laxatives)
2) Barbiturates
3) Tetracyclines
4) NSAIDs
5) Metronidazole
6) Salicylates
7) Sulfonamides
8) Food coloring (yellow)
What are the common drugs that cause a Fixed Drug Eruption? (8)
Mouth, genitalia, face, and acral areas -(distal portions of limb: e.g. hand, foot, ears, nose)
What are the common areas that are affected by Fixed Drug Eruption?
30 min to 8 hours
If a person has had previous exposure to the same drug causing an Fixed Drug Eruption, how long will it take for the new lesion to occur?
Fixed Drug Eruption
This type of drug reaction will have early lesions that are sharply demarcated erythematous macules, they can then form a plaque which may turn into a bulla , then an erosion. Once healed it will be dark brown to violet colored.
Non-eroded: potent topical corticosteroid ointment
Eroded cutaneous: protective or antimicrobial ointment and dressing until the site has reepithelialized
Pain must be addressed, especially for mucosal lesions
How are Non-eroded Fixed Drug Eruption lesions treated?
Eroded cutaneous Fixed Drug Eruption?
Days to weeks
How long does it take for a Fixed Drug Eruption to resolve?
CBC and LFTs
What labs should be ordered if a patient presents with a combination of rash and facial edema?

Drug-Induced Hypersensitivity Syndrome (DIHS)
Also called DRESS = Drug Reaction with Eosinophilia and Systemic Symptoms
**Note 70% of pt have an eosinophilia
A patient present with an skin eruption and systemic sx of exanthem, erythematous dentrofacial swelling, fever, malaise, lymphadenopathy, and involvement of other organs (liver, kidneys). What do you suspect?

Typically 3rd week but may range 1-12 weeks
(this helps to distinguish DIHS from exanthematous drug eruption, which appears in up to 10 days.)
s/sx may persist and recur for many weeks even after cessation of drug treatment.
How long after a patient takes medications do the signs and symptoms begin?
1) Allopurinol
2) Antibiotics
3) Anti-TB
4) Anticonvulsants
5) NSAIDs
5) Anti-HIV
What are typical medications that can cause drug-induce hypersensitivity syndrome?
Stop or substitute all suspect medications and discontinue non-essential medications
What should your initial step be after determining a patient has drug-induce hypersensitivity syndrome?
Consult dermatology
NON-SEVERE can use topical steroids and systemic antihistamines.
SEVERE = start systemic steroids (prednisone 1mg/kg/day) and very gradually taper
After stopping all medications, when you suspect a drug-induced hypersensitivity syndrome how do you treat the patient? For both severe and non-severe reactions.
SJS Stevens-Johnson Syndrome/TEN (Toxic Epidermal Necrolysis)
This patient comes to the ER with a painful, expanding, and "sloughing" rash. They were recently treated for a UTI with sulfamethoxazole and trimethoprim. What is the likely Dx?

Stevens-Johnson Syndrome/TEN
This type of drug rash has erythematous erosions mainly localized on the face, upper trunk, and hands with lesions that begin as flaccid blisters.

1) Consult dermatology
2) Discontinue all non-life-sustaining medicatios
3) Request a tissue biopsy to confirm suspected dx.
4) Transfer to burn unit for >25/30% BSA involvement
How do you manage a patient with Stevens-Johnson Syndrome/TEN?
The amount of body surface area involved
What is the difference between Stevens-Johnson Syndrome and TEN?
SJS < 10%
SJS/TEN 10-30%
TEN > 30%
What are the 3 groups for TEN and SJS based on the total body surface area?
SATAN is the mneumonic
S = Sulfa antibiotics, sulfasalazine
A = Allopurinol
T = Tetracyclines
A = Anticonvulsants
N = NSAIDS
N = nevirapine
What are the medications that have been associated to SJS/TEN?
SJS/TEN begins within 8 weeks of drug exposure.
1-3 days before pt may have fever, HA, rhinitis, and myalgias
Mucous membrane improvement can precede skin eruptions (buccal, ocular, and gential mucosa)
How may days after the onset of the drug does SJS/TEN begin and is there any signs or sx before the skin eruptions?
Pain!
Which is more common with SJS/TEN - pain or itching?
1) Corneal damage
2) Oral cavity
3) GU damage
4) Pulmonary damage
5) Fluid and electrolyte problems
6) Secondary infection
What are possible complications from SJS/TEN?
HLA-B*1502 genetic screening for all southeast Asian patients starting carbamazepine (anti-epileptic)
HLA-B*5701 genetic screening for all patients starting abacavir (treatment of HIV infection)
How can SJS/TEN/DIHS be prevented in southeast Asian patients?