Basal ganglia & cerebellum
1/21
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
22 Terms
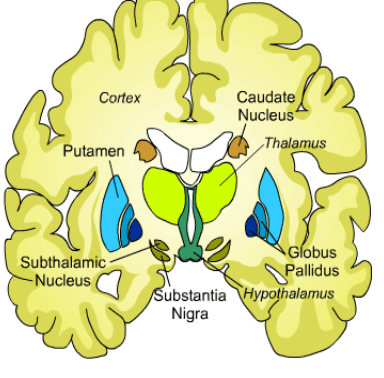
what are the components of the basal ganglia
straitum, globus pallidus, subsantia nigra, subthalamic nucleus
functions of the basal ganglia?
-voluntary behaviour & movements
-inhibiting inappropriate involuntary movements
-extensive connections in frontal cortex- therefore indicated involvement in memory, cognition, emotion
symptoms of parkinsons?
rigidity, reduced arm swing, tremor at rest & shuffling gait
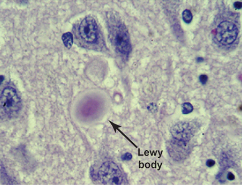
what are a histological hallmark of PD
fibrillar aggregates- lewy bodies (similar to inclusion formation in Huntington’s ) (by the time motor symptoms appear, approx 60% dopamine neurons are lost)
whats some treatment for PD
Levadopa- tablet or liquid form
converted to dopamine & often combined w other meds e.g. benserazide/ carbidopa
why are additional meds often given in addition to Levodopa to treat PD?
-stop levodopa being broken down in bloodstream b4 gets to brain
can reduce levodopa’s side effects (e.g. feeling sick, tiredness, dizziness)
what is long term levodopa use linked to?
-uncontrollable, jerky muscle movements (dyskinesias)
-’on-off’ effects- the person rapidly switched being able to move (on) & being immobile (off)
(even tho initial dose is very small & gradually increased& can cause dramatic improvement in symptoms)
how does deep brain stimulation work (treating PD)
surgically implanting a pulse generator (like a heart pacemaker) into the brain
describe huntingtons
Neurodegenerative condition
Autosomal dominant – trinucleotide CAG repeat
Incidence 1 in 10,000-12,000
Selective loss of medium spiny neurons in striatum
mood disturbances, depression, impulsiveness/ aggression, dystonia/ myoclonus, chorea
differences between early & late stage Huntingtons?
early- indirect path affected (striatum not as effective) (picture seen)
late- both indirect and direct path dysregulated
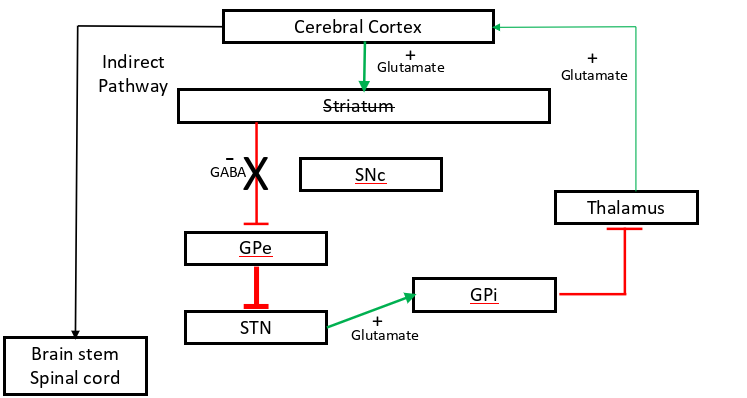
SAQ: Describe the primary cause of Huntington’s disease, in the early stages of the disease, state which specific cells of the striatum are impacted, and which pathway of the basal ganglia is primarily affected [4 marks].
CAG repeats in the huntingtin gene causing selective loss of (GABAergic) medium spiny neurons in the striatum and the indirect pathway is mostly affected (in caudate nucleus & putamen?)
how many copies of CAG usually means HD onset?
36-39 with reduced penetrance, 40+ full penetrance
whats genetic anticipation and how does it work (HD genetic)
increasing severity of disease or decreasing age of onset in successive family generations
-instability of CAG repeat during spermatogenesis
-paternal transmission
-juvenile inheritance from father
what are some treatments for HD
treats symptoms-
mood disturbances -antipsychotic
depression- anti-depressants
impulsiveness/ aggression- anti-epileptics
dystonia, myoclonus- anti-spasticity/ anti-parkinsonian drugs
chorea- dopamine blocking agents (DA can reduce effect indirect pathway)
or cell transplantation/ antisense oligonucleotide/ uniQure
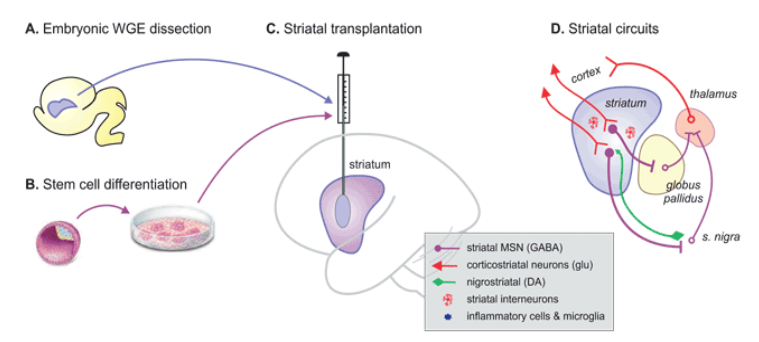
review the effectiveness of HD treatments cell transplantation/ antisense oligonucleotide/ uniQure
cell transplantation- improvements in motor function & cognition seen but small scale
antisense oligonucleotide- showed reduced mutant HTT in CSF (gene silencing working) but this trial discontinued due to benefit/ risk profile not good enough
uniQure- still under review of results but showed after 3yr avg 75% slowing of disease & generally safe but some pt developed inflammation (from the virus) causing headaches & confusion (was resolved or needed steroid treatment)
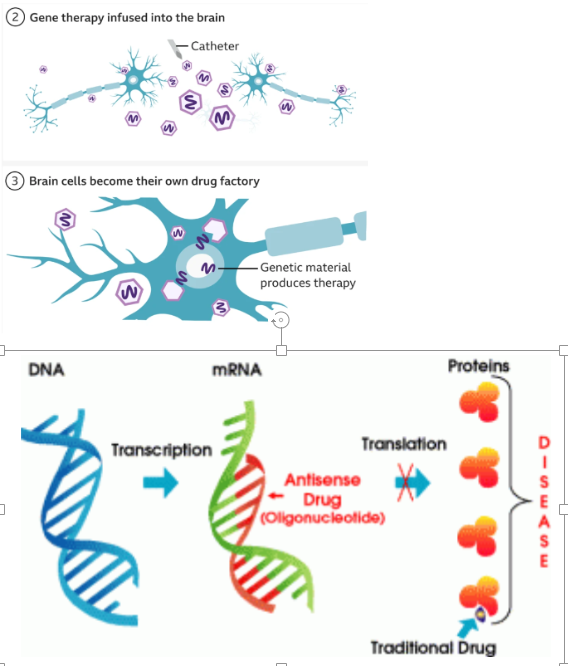
how do HD treatments antisense oligonucleotide/ uniQure work?
antisense oligonucleotide - gene silencing via antisense drug binding DNA stopping translation
uniQure- virus containing specially designed seq of DNA, virus infused into brain using RT-MRI to guide a microcatheter to Caudate nucleus & putamen (12-18hr surgery) -> cells produce miDNA designed to intercept & disable mRNA for mHTT (=lower lvl mHTT)
whats the vestibulo-ocular reflex
maintain eyes on a visual target when the head is rotated
how do prism goggles affect the vestibulo-ocular reflex
after consecutive days the direction of the reflex progressively reduces, eventually reversing direction (lesions of vestibulocerebellum stops this adaption)
Babinski (1900s) & Holmes (1920s) - what are the distinctive symptoms and signs of cerebellum disorders
-hypotonia (low lvl of muscle tone)
-ataxia (lack of co-ordination- voluntary movement)
-action or intention tremors (tremor at the end of a movement)
describe Firedrich Ataxia
-most common of the inherited ataxies
-autosomal recessive (expansion of GAA repeat in intron 1 of FRDA gene) - decreases fraxin protein
-iron accumulates in mitochondria -> excess production of free radicals
-fibre loss in dorsal column & spinocerebellar tracts & cellular damage & death
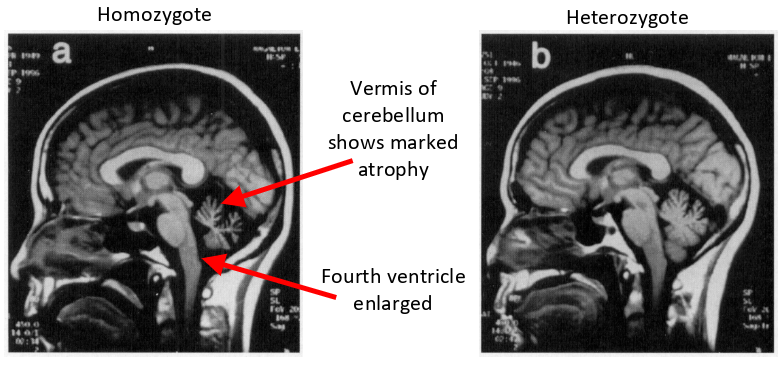
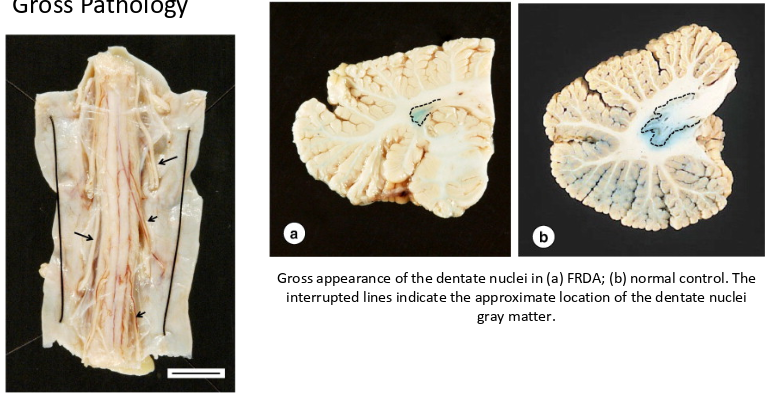
whats the gross pathology of friedrich ataxias
-reduced transverse diameter of the thoracic spinal cord
-reduced dendate nuclei in cerebellum
describe spinocerebellar ataxia type 1
-autosomal dominant (expanded CAG repeat in chromosome 6 containing SCA1 locus)
-cAG repeat size correlated with siza and age of onset
-neurodegeneration of cerebellum, spinal cord & brain stem