pathology bone and salivary gland disorder
1/112
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
113 Terms

torus (plural, tori)
not a true tumor
developmental lesion or lesion with a hereditary basis
more common in women
as an asymptomatic, bony hard, or lobulated mass
no treatment is necessary, unless interfere with the fabrication of a denture

torus palatinus
usually in the midline

torus mandibularis
usually bilateral, in the premolar area

exostosis
a small nodular excrescence of normal compact bone
asymptomatic, on the buccal aspect of alveolar ridge
no treatment needed, unless any interference with denture

osteoma
an asymptomatic, benign tumor composed of normal compact bone
no sex predilection
within the bone or as a mass attached to the outer surface of the bone
within posterior mandible, as most common location
surgical excision as treatment, no recurrence

gardner symdrome
autosomal dominant disorder
presence of intestinal polyps as most serious feature
possible malignant transformation into adenocarcinoma

symptoms of gardner syndromes
mutiple osteomas
mutiple odontomas
supernumerary teeth
idiopathic osteosclerosis
a focal area of increased bone density that cannot be attributed to any specific cause
common
also seen in other bones
teens and young adults
mandible (90% of cases) : premolar and 1st molar area
adjacent teeth are vital

idiopathic osteosclerosis differential diagnosis
contrast with condensing osteitis
if the tooth is non vital - condensing osteosis
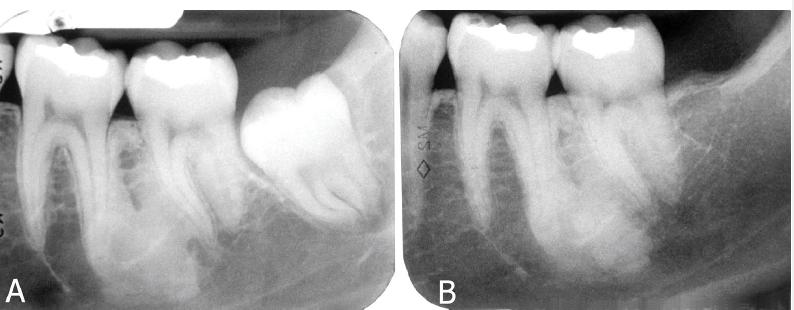
condensing osteitis
features of condensing osteitis
non-vital tooth or presence a source of inflammation
widened PDL
sclerosis of bone around roots in response to chronic inflammation
may mimic idiopathic osteoscerosis
multiple osteomas and odontomas (supernumerary teeth)
which of the following is associated with gardner syndrome

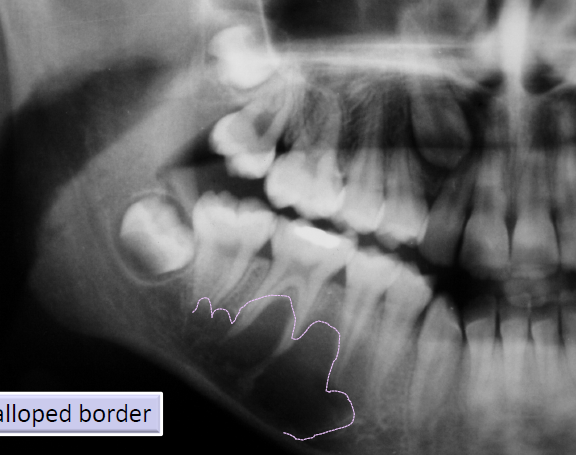
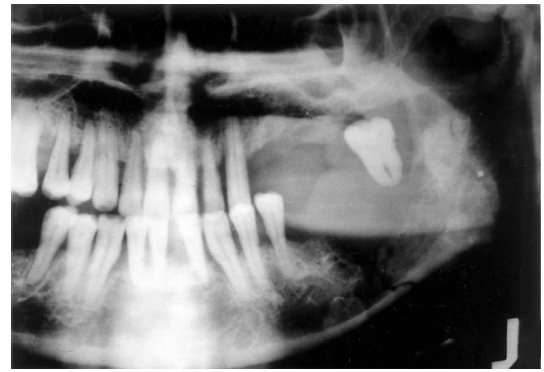
traumatic bone cyst (simple bone cyst)
asymptomatic intra-osseous empty cavity
not a true cyst
may be associated with trauma, patients commonly young
pseudocyst
lined by a thin loose connective tissue, scalloped borders

aneurysmal bone cyst
not a true cyst, caused by increased venous pressure with resultant dilation and rupture of the local vascular network
“blood soaked sponge” as surgical finding
arising in a pre-existing bone lesion
may cause pain and swelling
large unilocular or multilocular radiolucency

central giant cell granuloma
a non neoplastic lesion
more common in females
mandible> maxilla
more common in the anterior segment of the jaws
unilocular or mutilocular radiolucency
may be associated with jaw expansion and divergence of the adjacent teeth roots. inflammatory reaction
“within the jaw” type of giant cell granuloma
“central” in central cell granuloma suggests

central giant cell granuloma occlusal radiograph of mandible
may demonstrate CGCG as cause of expansion of internal and external cortical bones

central giant cell granuloma maxillary occlusal radiograph
demonstrates CGCG as cause of divergence of roots of maxillary central incisors

post surgical hyperostosis
tumor like (reactive) growth of bone at the surgical site
in periosteum following periodontal surgery such as a gingival graft
female patients, anterior mandible
central giant cell granuloma is more common in
an intraosseous cavity without epithelial lining
a traumatic bone cyst is best described as
benign fibro-osseous lesion of the jaws
a group of diseases characterized by the replacement of bone with abnormal fibrous connective tissue interspersed with varying amounts of calcification
fibrous dysplasia
central ossifying/cementifying fibroma
cemento-osseous dysplasia
fibrous dysplasia classification
unknown, maybe a developmental disease
central ossifying/cementifying fibroma classification
neoplasm
cemento-osseous classification
reactive lesion
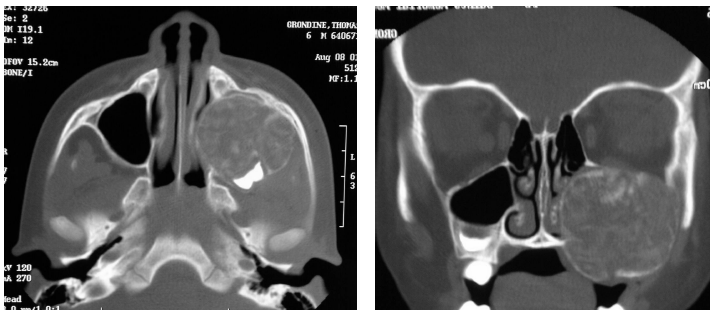
fibrous dysplasia
benign fibro-osseous lesion of the jaw
uncommon, benign, chronic bone disease
replacement of bone by fibrous connective tissue intermixed with delicate bony trabeculae
monostatic type is most common, polyostotic type
maxilla > mandible
painless, gradual enlargement of the affected bone
children and young adults
monostatic type of firbous dysplasia
most common type
affects only 1 bone

polyostotic type
type of fibrous dysplasia
involvement of more than one bone

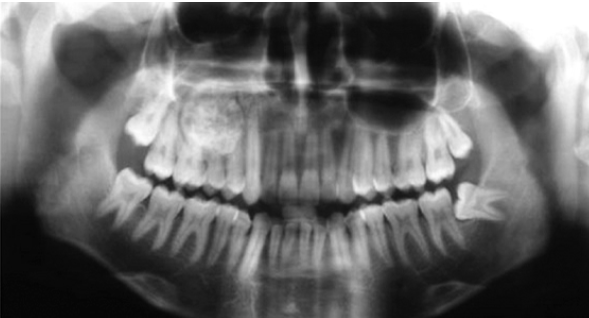
fibrous dysplasia radiographic characteristics
“ground glass” appearance on radiograph
abnormal bone blends into the normal adjacent bone
ill-defined borders
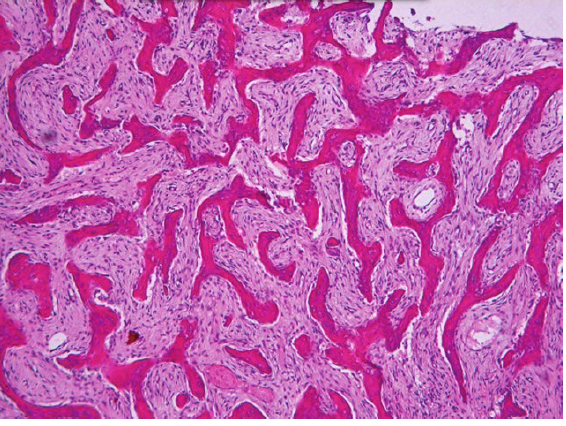
fibrous dysplasia histopathologic features
chinese letter appearance

central ossifying/ cementifying fibroma
a benign fibro-osseous lesion of the jaw
a true benign neoplasm composed of fibrous tissue containing bone, cementum-like material, or both
most patients are in 3-4th decades of life
female predilection
mandible> maxilla
radiographically, a well-defined unilocular radiolucency with varying degrees of radiopacity
juvenile ossifying fibroma
unilocular or mutilocular radiolucencies
mixed radiolucent/radiopaque
radiopacity depending on amount of cacification
cemento-osseous dysplasia
a benign fibro-osseous lesion of the jaw
a common fibro-osseous lesion that occurs in the tooth-bearing areas of the jaws
in this setting “dysplasia” does not imply that the lesion if precancerous
periapical
focal
florid
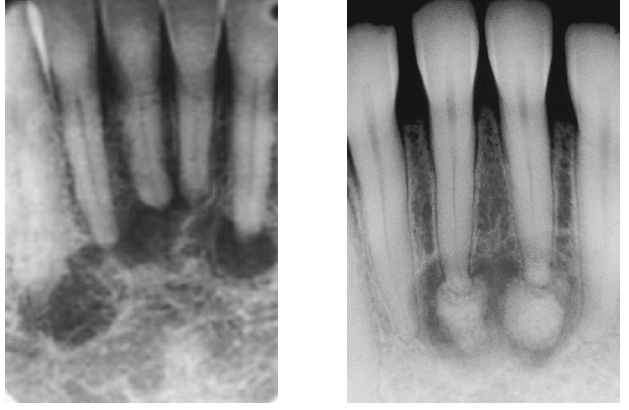
periapical cemento-osseous dysplasia
not a neoplasm
adult females
black population (70% of cases)
periapical region of anterior mandible
asymptomatic
early lesions mimic periapical inflammatory pathology (early is radiolucent)
involved teeth are vital

focal cemento-osseous dysplasia
asymptomatic, found incidentally on radiographs
female predilection (30-50 years of age)
more common in white population
posterior mandible, most common location

florid cemento-osseous dysplasia
involvement of multiple quadrants in the maxilla and mandible
most often seen in black women
treatment is often unnecessary
osteomyelitis as one complication in edentulous patients
mandibular anterior region
periapical COD primarily affects
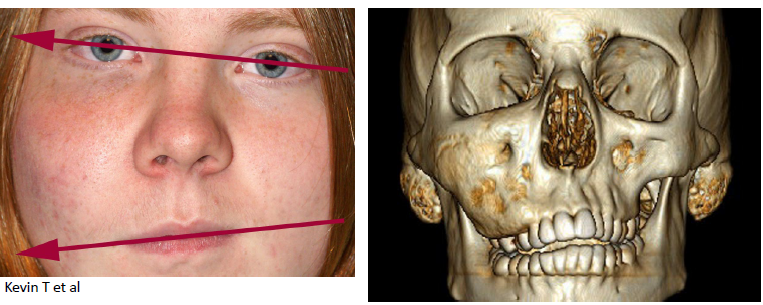
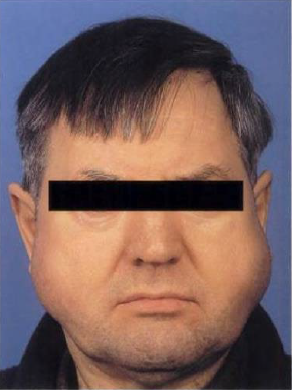
paget disease of bone
another name: osteitis deformans
a chronic metabolic bone disease
most common in men over the age of 50
pelvis and spinal column
jaws: maxilla> mandible
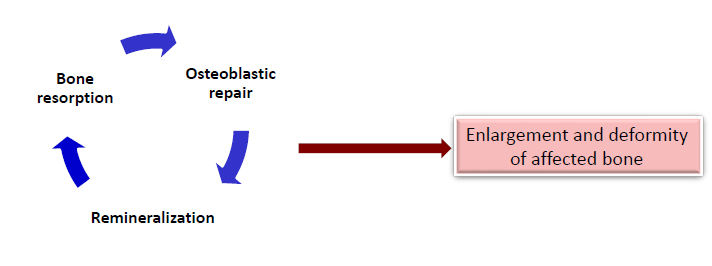

paget disease of bone clinical manifestations
enlargement, deformity, and pain of affected bone
jaws: spacing between the teeth, complaining of current denture
involvement of skull bones: headache, dizziness, and deafness
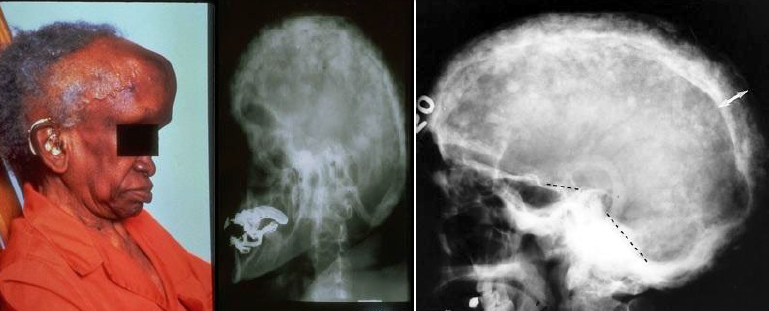
cotton-wool appearance
paget disease of bone radiographic features
hypercementosis
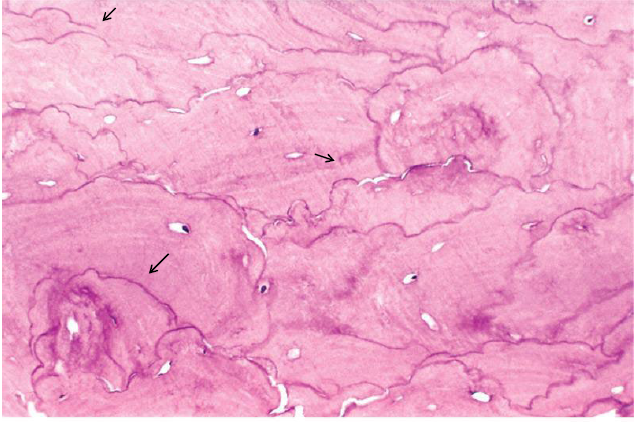
histopathologic feature of paget disease
mosaic pattern due to prominent reversal lines
paget disease of bone diagnosis
laboratory evaluation is important in establishing the diagnosis of paget disease
significant elevation of the level of serum alkaline phosphatase
osteoblastoma
a benign tumor with cells showing osteoblastic differentiation
a bone-forming tumor, but the bone as not as mature seen in osteoma
mixed radiolucent/radiopaque

osteosarcoma
a malignant tumor of bone-forming tissue
most common primary malignant tumor of bone in patients under 40 years of age
gnathic
extragnathic
treatment: surgery, adjuvant chemotherapy, radiotherapy
gnathic osteosarcoma
3rd and 4th decades
extragnathic osteosarcoma
long bones
10-20 year olds

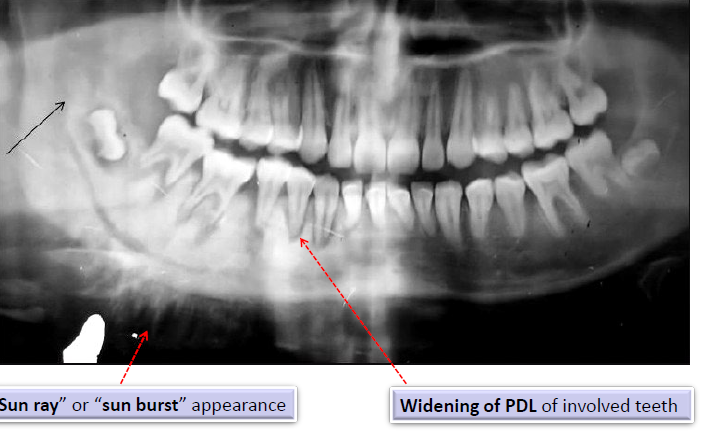
osteosarcoma radiographic features
“sun ray” or “sun burst” appearance
widening of the PDL of involved teeth
metastatic tumors of the jaws
the most common form of malignancy involving bone
mandible as the most frequent intraoral site for metastatic tumors of the jaws
primary tumors: breast, lung, thyroid, prostate, and kidney
clinical features of metastatic tumors of the jaws
pain, paresthesia or anesthesia of the lip
swelling and expansion of the affected bone and loosening of the teeth
radiographic features of metastatic tumors of the jaws
usually poorly-defined and radiolucent
metastatic tumors from the breast, prostate gland, and lungs may form bone
radiopaque
sun-ray or sun-burst appearance
radiographically, osteosarcoma of the jaws may show
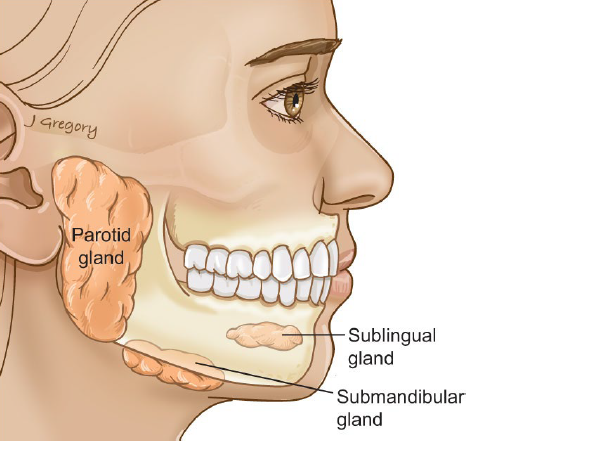
major salivary glands
parotid
submandibular
sublingual
minor salivary glands
distributed in the oral cavity
xerostomia
subjective sensation of dry mouth
in 25% of older adults, but not a normal aspect of aging
systemic diseases associated with xerostomia
sjrogen syndrome
diabetes mellitus
diabetes insipidus
sarcoidosis
HIV infection
graft-versus-host disease
psycogenic disorders
developmental causes of xerostomia
salivary gland aplasia
water/metabolic loss causes of xerostomia
impaired fluid intake
hemorrhage
vomitting/diarrhea
latrogenic causes of xerostomia
medications
radiation therapy to the head and neck
local factors that contribute to xerostomia
decreased mastication
smoking
mouth breathing
medications that may induce xerostomia
antihistamines
decongestants
antidepressants
antipsychotic
antihypertensives
anticholinergics
treatment of xerostomia
stay hydrated with water throughout the day
sugarless candy (stimulates flow)
daily fluoride application
biotene products
artificial saliva
systemic drugs
pilocarpine (salagen)
cevimeline (evoxac)

sialadentitis
inflammation of the salivary glands
can be due to a variety of infections and non infectious causes
mumps, as most common viral cause
staphylococcus aureus is the most common bacterial cause
most bacterial infections are the result of reduced salivary flow or ductal obstruction, allowing retrograde spread of bacteria
mumps
most common viral cause of sialadenitis
staphylococcus aureus
most common bacterial cause of sialadentitis
most bacterial infections are the result of reduced salivary flow or ductal obstruction, allowing retrograde spread of bacteria
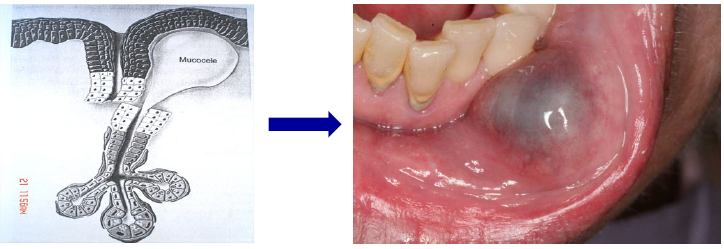
mucous extravasation phenomenon (mucocele)
mucous spillage into the soft tissues due to rupture of a minor salivary gland duct
causes by local trauma (common in kids)
fluid-filled lesions that is often blue or translucent in color
lower lip is the most common location
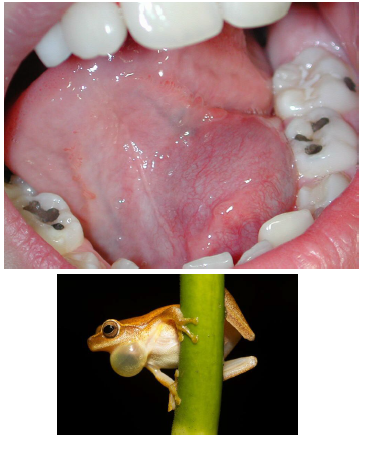
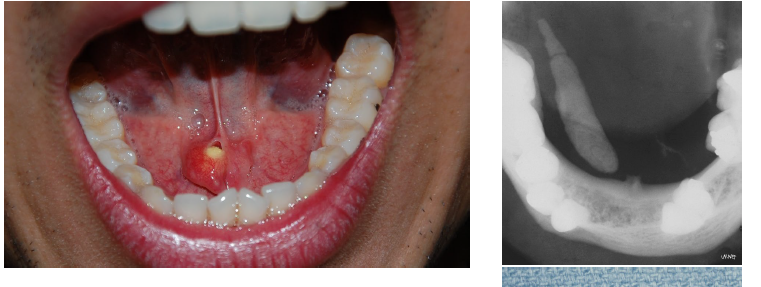
ranula
a mucocele in the floor of the mouth

superficial mucoceles
minor gland ducts close to mucosal surface involved
cause by mucosal inflammation rather than rupture of duct
tiny, clear, and bubble-like
soft palate, retromolar region, and the posterior buccal mucosa as the common sites
more common in patients with xerostomia
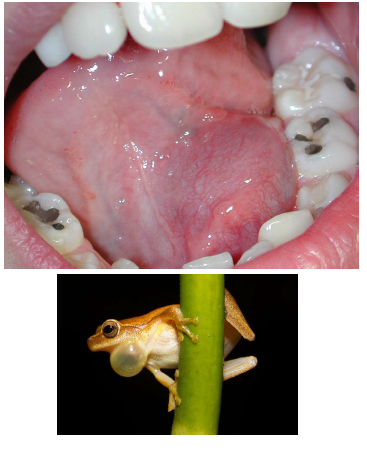
ranula
mucoceles in the floor of the mouth, trauma induced
lateral to the midline, painless swelling
appearance similar to the underbelly of a frog (rana)
possible displacement of the tongue
cervical or plunging
oral
oral ranula
superior to the mylohyoid muscle
cervical or plunging ranula
below the mylohyoid muscle
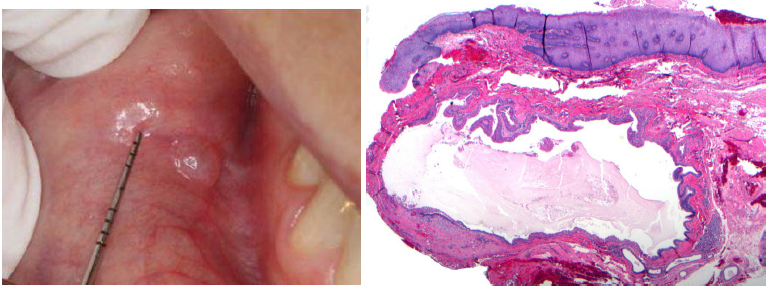
salivary duct cyst
a mucous retention phenomenon, called mucous retention cysts or sialocyst
a true cyst
similar to mucocele clinically
blockage of the salivary duct (by salivary gland stone) → cystically dilation of the duct
surgical excision as treatment
stress
most common cause of xerostomia

cysts of blandin-nuhn
mucoceles or mucous duct cysts forming in blandin-nuhn glands as mixed glands located in anterior ventral tongue
usually pedunculated and dome shaped
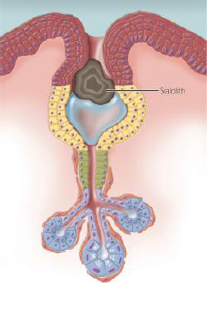
sialolithiasis (salivary stones)
calcified structures, develop within the salivary ductal system
proposed etiology: deposition of calcium salts around a nidus of debris (bacteria, foreign body, epithelial cells, mucous plug, etc)
chronic sialadenitis and partial duct obstruction promotes stone formation
submandibular gland duct as most common location
salivary stones (sialolithiasis) clinical signs
episodic pain or swelling of the affected gland at midline
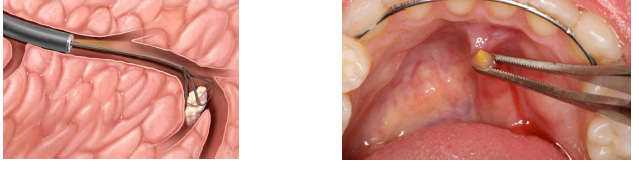
sialolithiasis (salivary stone) treatment
can sometimes be worked toward the orifice and “passes” by heat, increased fluid intake, and milking/massaging of the gland
lithotripsy (shock waves break up stone into smaller pieces that can be passed)
surgical removal is often indicated
the associated gland may also need to be removed if significant inflammatory damage has occured
sialadenosis
nonneoplastic, noninflammatory salivary gland enlargement, usually involving the parotid gland
cause by peripheral neuropathy of the autonomic nerve supply
50% of cases associated with underlying systemic factors, including diabetes, hypothyroidism, bulemia, malnutrition, alcohol abuse, and drugs
as a side effect of certain antihypertensive or psychotropic drugs
adenomatoid hyperplasia
increase in the number of gland acini in minor salivary gland
seen as firm, nontender mass, mimicking a minor salivary gland tumor
hard palate as the most common location
nectrotizing sialometaplasia
an inflammatory process
caused by ischemia → infarction → necrosis and ulcer → sloughing necrotic tissue → healing
potential/suggested predisposing factors
injury (trauma, dental injection, previous surgery)
ill-fitting denture
adjacent tumor
heals spontaneously over a period of 4-6 weeks
posterior palate (75% of all cases)
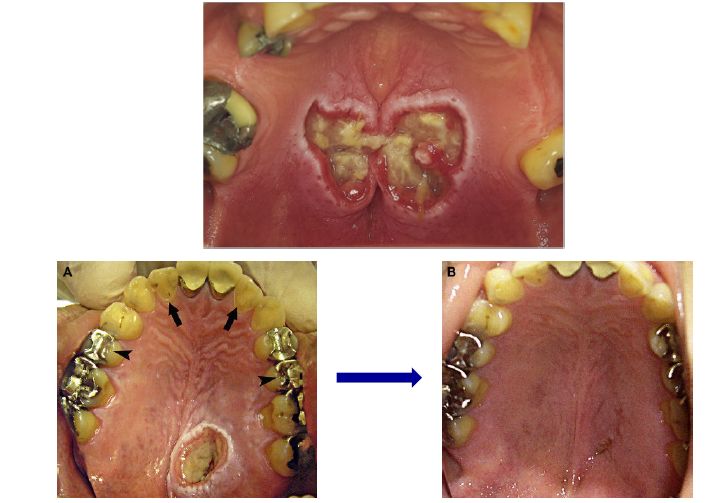
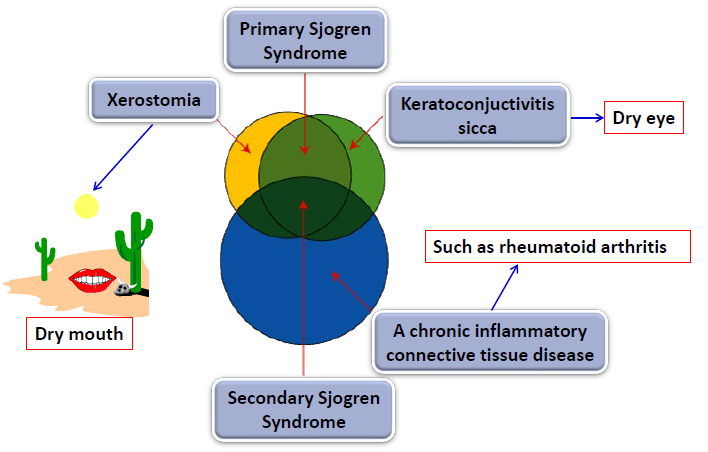
sjogren syndrome
an autoimmune disease
affects the salivary and lacrimal glands
typically leads to xerostomia
keratoconjunctivitis → dry eye
chronic inflammatory connective tissue disease → rheumatoid arthritis
raynaud phenomenon (white fingers) → triggered by cold and emotional stress
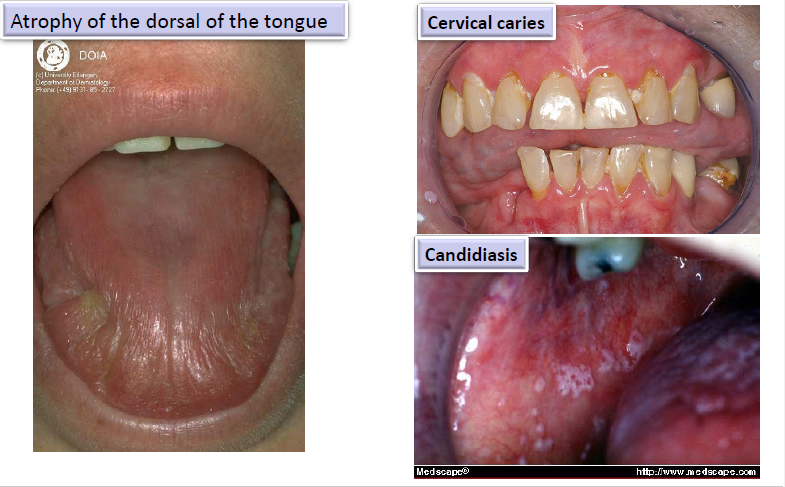
oral manifestations of sjogren syndromes
atrophy of the dorsal surface of the tongue
cervical caries
candidiasis
treatment for sjogren syndrome
symptomatic
artificial saliva, artificial tears
sugarless gum or lozenges
maintaining good oral hygiene, using fluoride toothpaste
corticosteroids and immunosuppressive agents for severe cases
sublingual gland tumor prevalence
1% of all tumors
70-90% malignant
parotid gland tumor prevalence
most common site
64-80% of all salivary tumors
15-32% malignant
submandibular gland tumor prevalence
8-11% of all salivary tumors
37-45% malignant
minor salivary gland tumor prevalence
9-25% of tumors
50% malignant
general clinical features of salivary gland tumors
female predilection
painless swellings as most common presentation
malignancies may mimic benign tumors or be ulcerated
pain need not indicate malignancy
paresthesia suggestive of malignancy
most common sites for minor salivary gland tumors in order
palate
upper lip
buccal mucosa
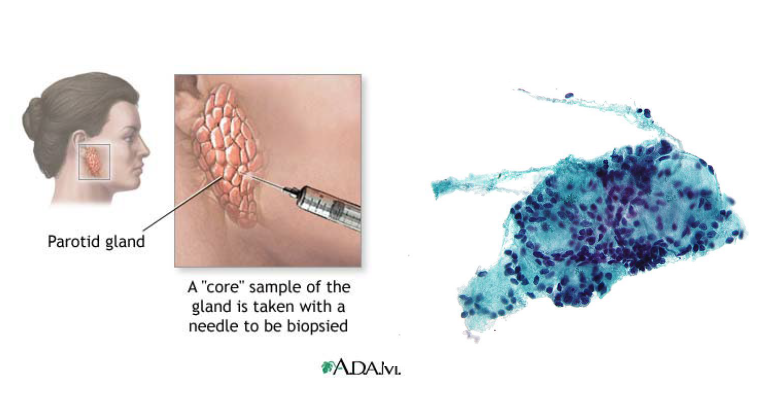
diagnosis of salivary gland tumor
physical examination
CT
MRI
ultrasound
fine needle aspiration (FNA) - core sample of gland is taken with needle
biopsy
benign salivary gland tumors
pleomorphic adenoma
warthin tumor (papillary cystadenoma lymphamatosum)
canalicular adenoma
basal cell adenoma
salivary ducts papillomas

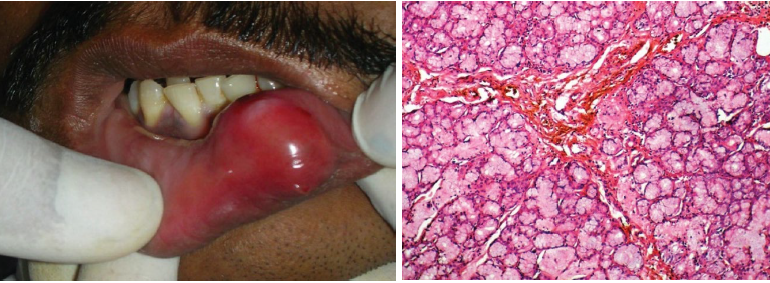
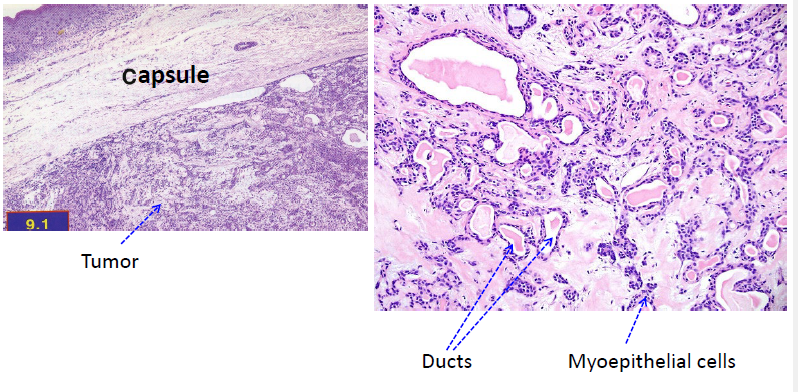
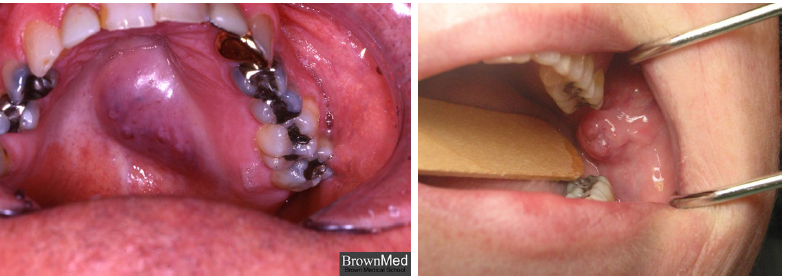
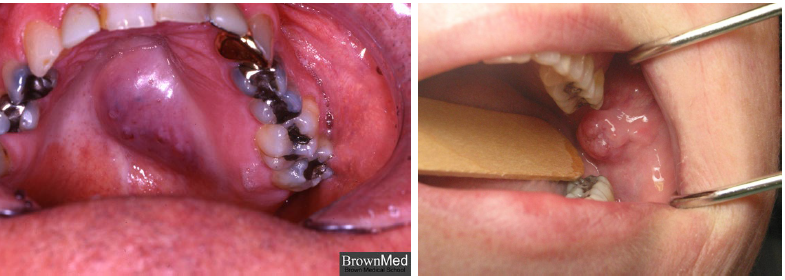
pleomorphic ademona
benign salivary gland tumor
most common salivary neoplasm
painless, slow-growing firm mass, intraorally is commonly seen on palate
female predilection
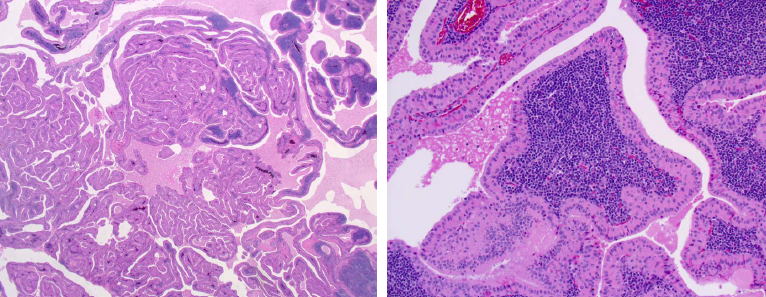
pleomorphic adenoma histopathologic features
mixture of ductal and myoepithelial elements
well-circumscribed, encapsulated
ducts and cystic structures
myoepithelial cells
stromal changes: myxoid, hyalinized, focal areas of fat, chondroid, and osteoid
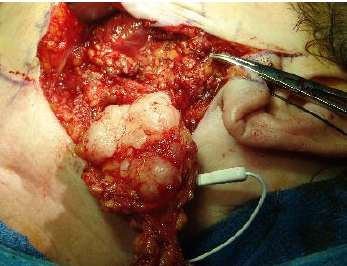
pleomorphic ademona treatment and prognosis
surgical excision
recurrence in multifocal cases
small risk of malignant transformation (5% of all cases)
warthin tumor (papillary cystadenoma lymphomatosum)
benign
second most common benign partoid tumor
almost exclusively in the partoid gland
strong association with smoking
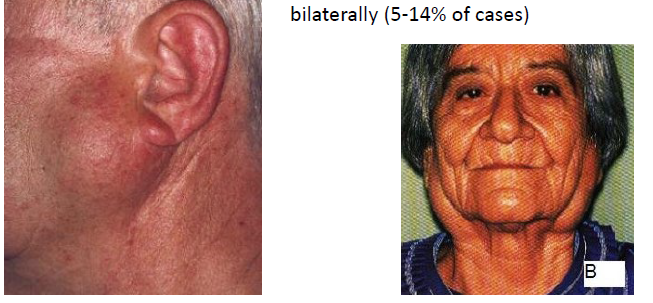
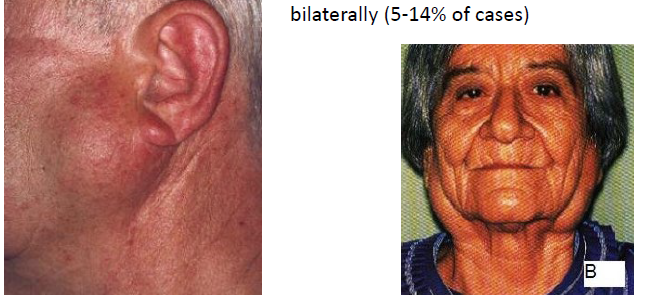
warthin tumor (papillary cystadenoma lymphomatosum) clinical features
slowly growing painless mass
MALE predilection, 6-7 decades of life
most likely salivary gland tumor to appear bilaterally (5-14% of all cases)
warthin tumor histopathologic features
cystic spaces lined by ductal oncocytic epithelium in papillary configuration
lymphoid stroma with frequent germinal center formation
warthin tumor treatment and prognosis
surgical removal
6-12% recurrence

canalicular adenoma
benign salivary gland tumor
exclusively in the minor salivary glands
75% in upper lip
buccal mucosa, second most common site
female predilection
surgical excision as treatment
malignant salivary gland tumors
may appear clinically innocuous
may appear histopathologically innocuous
may be associated with paresthesia, tumor fixation, or ulceration
types of malignant salivary gland tumors
mucoepidermoid carcinomas
polymorphoud low-grade adenocarcinoma
adenoid cystic carcinoma
acinic cell carcinoma
carcinoma ex-pleomorphic adenoma
mucoepidermoid carcinoma
most common malignant salivary neoplasm in adults and children
second most common salivary tumor
in US, 10% of all major gland tumors and 15-21% of minor gland tumors
variable biologic potential (low, intermediate, and high grades)
mucoepidermoid carcinoma clinical features
seen in wide age range
female predilection
parotid, most common site
an asymptomatic swelling