venous thromboembolism
1/200
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
201 Terms
DVT presentation
sx: unilateral and localized to area, swelling, pain, redness, tenderness
s: superficial veins dilated (palpable cord), unilateral leg edema (2 cm difference in diameter), homan’s sign (calf pain during dorsiflexion (backward bending) of foot
PE presentation
sx: SOB + fatigue, chest pain, palpitations, hemoptysis, syncope
s: tachypnea, tachycardia, diaphoresis, hypoxia; lungs sound clear
dx tests for dvt
d-dimer (rule out), ultrasound (non-invasive), venography (invasive)
dx tests for pe
d-dimer (rule out), computed tomographic pulmonary angiography (CTPA) [minimally invasive], ventilation-perfusion (V/Q) scan [minimally invasive], echocardiography [non-invasive]
d-dimer
measures plasma levels of d-dimers, generated when the endogenous fibrinolytic system degrades fibrin
97% sensitivity, 35-45% specificity (useful as exclusionary test for VTE
compression ultrasound
highly sensitive + specific modallity for recognition of lower extremity DVTs w/o need for radiation or contrast exposure non-invasive
computed tomographic pulmonary angiography (CTPA)
1st line testing for PE, high sensitivity and specificity
contrast dye used to visualize thrombus in lungs
ventilation perfusion (V/Q) scan
2nd line dx test for PE (esp for pts who can take contrast dye)
pt breathes in isotope nebulizing solution used to assess air flow (ventilation)
isotope inj then used to assess blood flow (perfusion)
dx: blood flow defects in presence of normal air flow
tx goals of VTE
prevent development of PE
prevent recurrence of dvt/pe
reduce post-thrombotic syndrome, chronic thromboembolic pulmonary HTN
prevent complications, mortality + morbidity
tx w/ minimal AE and cost
direct oral anticoags (DOACs)
apixaban, rivaroxaban, edoxaban, dabigatran
which DOACs are factor Xa inhibitors
apixaban, rivaroxaban, edoxaban
which DOAC is a factor IIa (thrombin) inhibitor
dabigatran
vitamin K antagonist (indirect)
warfarin
which parenteral anticoags work indirectly
UFH, LMWH (enoxaparin, deltaparin), factor Xa inhibitor (fondaparinux)
which parenteral anticoags work directly on thrombin
argatroban, bivalludin, desirudin
how does warfarin work in the clotting cascade
prevents factor 2, 7, 9, 10 production from the liver! and adds anticoag proteins C and S (→ early procoagulant effect)
which factors does unfractionated heparin inhibit indirectly
Xa and IIa equally
which factors dose LMWH inhibit indirectly
more Xa than IIa
which parenteral anticoags are given SC
fondaparinux, desirudin, UFH, LMWH (both)
which parenteral anticoags are given IV
argatroban, bivalirudin, UFH, enoxaparin
true or false: are DOACs less effective than warfarin
false they are non-inferior!
which DOACs are dosed BID
apixaban, dabigatran
which DOACs are dosed QD
rivaroxaban, edoxaban
which DOAC is more renally cleared (in order)
dabigatran » edoxaban » rivaroxaban » apixaban
are DOACs recommended in pregnancy
no! avoid!
apixaban: category B
rivaroxaban, edoxaban, dabigatran: category C
contraindications for DOACs
active bleeding, mechanical heart valves, severe hepatic impairment
adrs for apixaban, rivaroxaban, edoxaban
bleeding
adrs for dabigatran
bleeding, dyspepsia, gi upset (gastritis)
what should you monitor for when pt is on DOAC
no efficacy lab monitoring
monitor renal fxn (for dosing adjustment), hgb, hct for safety
what antidote/reversal agent is used for apixaban, rivaroxaban, and edoxaban
factor 4-PCC (Kcentra)
what antidote/reversal agent is used for dabigatran
idarucizumab (Praxbind)
DOAC black box warning
increased risk of thrombotic events when discontinued prematurely
risk of epidural or spinal hematoma if receiving neuraxial anesthesia or undergoing spinal puncture
edoxaban specific black box warning
reduced efficacy in nonvalvular a-fib if crcl is >95 ml/min
apixaban tx for dvt/pe
10 mg BID x 7 days then 5 mg BID
rivaroxaban tx for dvt/pe
15 mg BID x 21 days then 20 mg daily with food
avoid use if crcl <30
edoxaban tx for dvt/pe
60 mg daily, start after 5-10d of parenteral anticoag
reduce to 30 mg if crcl 15-50, wt ≤ 60 kg, or on certain P-gp inhibitors
not recommended if crcl <15
dabigatran tx for dvt/pe
150 mg BID, start after 5-10d of parenteral anticoag
avoid if crcl <30
apixaban ppx for dvt (after knee/hip replacement)
2.5 mg BID x 12 d after knee or x 35d after hip surgery
1st dose 12-24h after surgery
rivaroxaban ppx for dvt (after knee/hip replacement surgery)
10 mg QD x 12d after knee or x 35d after hip surgery
1st dose 6-10h after surgery
avoid if crcl <30
is edoxaban used for ppx of dvt
no
dabigatran ppx for dvt (after knee/hip replacement surgery)
110 mg on day 1, then 220 mg QD
avoid if crcl <30
when should pt take rivaroxaban if taking it for nonvalvular afib stroke prevention
with their evening meal
avoid if crcl<15
15 mg qd if crcl 15-50
30 mg qd if crcl >50
which DOACs need renal adjustment
rivaroxaban, edoxaban, dabigatran
which DOAC does not need renal adjustment
apixaban, but dose adjust for afib! (reduce to 2.5mg bid if they have ≥2 of age≥80y, wt ≤60kg, or scr ≥ 1.5 mg/dl)
which DOAC has less bleeding than the other DOACs
apixaban
which DOAC has the least DDIs
dabigatran
which DOAC do you keep in the original bottle/blister pack/dont add to pill box (d/t humidity)
dabigatran
DOAC DDIs that should generally be avoided
p-gp inhibitors + cyp3a4 inhibitors
p-gp inducers + cyp3a4 inducers
which cyp3a4 inhibitors should be avoided w/ DOACs
azole antifungals, macrolides, protease inhibitors, non-dhp ccbs, amiodarone etc (g-pacman)
what cyp3a4 inducers should be avoided
rifampin, phenytoin, smoking, phenobarbital, carbamazepine, oxcarbamazepine, st.johns wort
initial management tx duration
5-21d
primary tx duration
3-6 months
extended tx (2ndary prevention) duration
beyond 3-6 months
apixaban initial tx
10 mg bid x 7 days
rivaroxaban initial tx
15 mg bid x 21 d
avoid if crcl <30
which anticoags are not used in initial treatment?
edoxaban and dabigatran
warfarin initial tx
combo!
warfarin + UFH/LMWH
heparin (UFH) initial tx
80 units/kg iv bolus
18 units/kg/hr infusion
or
5000 units iv bolus
1000 units/hr infusion
enoxaparin initial tx
1 mg/kg SC bid
1.5 mg/kg SC qd only for inpt vte tx
if crcl <30 : 1mg/kg SC qd
apixaban primary tx
5 mg bid
rivaroxaban primary tx
20 mg qd
avoid if crcl <30
edoxaban primary tx
60 mg qd
if crcl 15-50 or wt ≤ 60 kg: reduce to 30 mg qd
dabigatran primary tx
150 mg bid
avoid if crcl <30
warfarin primary tx
monotherapy! target INR 2-3
is heparin used for primary tx
no!
is enoxaparin used for primary tx
not usually, some pts w/ cancer may use it for 3-6 months
apixaban extended tx
2.5 mg (or 5mg) bid
rivaroxaban extended tx
10mg (or 20 mg) qd
avoid if crcl <30
is edoxaban used for extended tx?
no!
dabigatran extended tx
150 mg bid
avoid if crcl <30
is heparin or enoxaparin used for extended treatment?
no!
apixaban ppx (primary prevention)
2.5mg bid
rivaroxaban ppx (primary prevention)
10 mg qd
avoid if crcl <30
is edoxaban used for ppx (primary prevention)
no!
dabigatran ppx tx (primary prevention)
110 mg on day 1 then 220 QD
avoid if crcl <30
warfarin ppx tx (primary prevention)
monotherapy, target INR 2-3 (less evidence)
heparin ppx tx (primary prevention)
5000 units SC q8-q12
enoxaparin ppx tx (primary prevention)
30 mg SC bid (or 40 mg SC daily)
if crcl <30 → 30 mg SC daily
how is warfarin dosed
daily
indications of warfarin
vte tx and ppx
ppx of stroke in afib
ppx of acute MI in pts w/ pad
ppx of stroke, recurrent infxn
how many days of warfarin therapy is necessary before a pt is completely anticoagulated?
4-5 days
how is warfarin metabolized and what does that mean
hepatic metabolism meansssss → NO renal adjustment!
can you use warfarin in pregnancy
no! contraindicated (crosses placenta but not secreted in breast milk)
adrs of warfarin
purple toe syndrome: dark blue-tinged discoloration of the feet that occurs rarely 3-8 wks after warfarin initiation
warfarin-induced skin necrosis rare but serious adverse effect (begins within 10 days of initiation)
what do you monitor for warfarin
PT, INR (shows reduction in clotting factors II, VII, and X)
antidote/reversal agents for warfarin
vitamin K and 4-factor PCC (Kcentra)
which genes are tested with warfarin
VKORC1 and CYP2C9
VKORC1
vitamin K epoxide reductase complex subunit 1 gene
AA genotype : sensitive to warfarin
GG genotype : resistant to warfarin
CYP2C9
presence of variant alleles cyp2c9*2 and *3 results in slower clearance of warfarin
mneumonic for warfarin tablet colors
Please → pink → 1
Let → lavender → 2
Granny → green → 2.5
Brown → brown → 3
Bring → blue → 4
Peaches → peach → 5
To → teal → 6
Your → yellow → 7.5
Wedding → white → 10
what initial dose of warfarin will bring INR to around 2.0 in 4-5 days for most pts
5 mg QD
initiating warfarin with UFH/LMWH
take both together, stop UFH/LMWH when ≥5 days of combo therapy AND INR ≥ 2.0 for ≥ 24h
target INR of 2.5 and therapeutic range of 2-3 is indicated for
pts treated for VTE, afib, mechanical aortic valve, bioprosthetic valve, or antiphospholipid syndrome
target INR of 3.0 and therapeutic range of 2.5-3.5 is indicated for
pts treated for mechanical mitral valve or both mechanical aortic and mitral valves
what is used to monitor heparin
efficacy: aPTT (activated thromboplastin time), ACT (activated clotting time), anti Xa levels
safety: platelet, hgb, hct, s/sx of bleeding
warfarin maintenance dosing
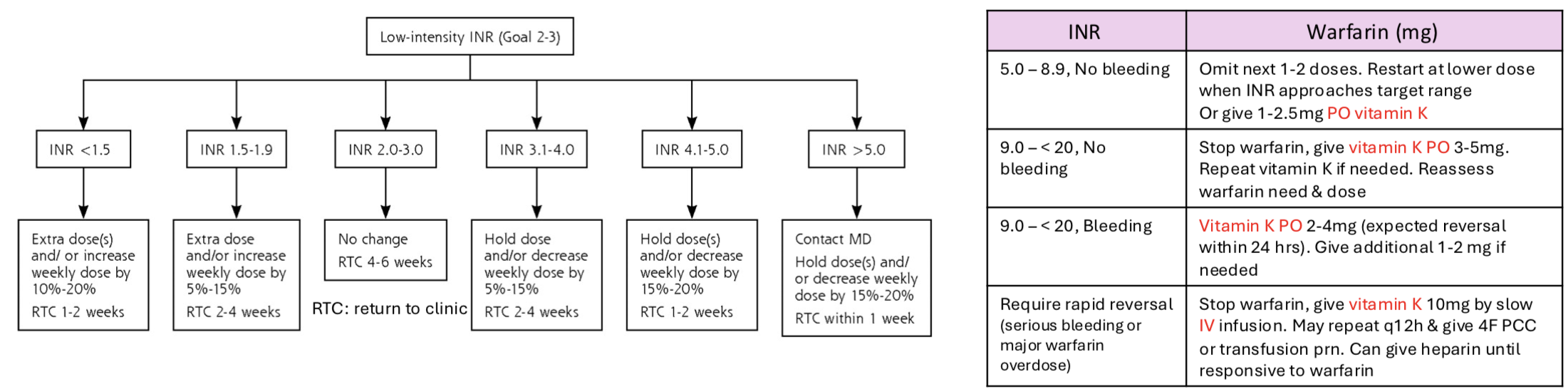
when is IV vitamin K used
only for pts with serious bleeding
warfarin DDIs
has NTI so must monitor INR
many DDIs ☹
drugs that inhibit or induce cyp2c9 or 3a4 can potentiate or reduce anticoag effect
S-isomer is more active!
which drugs increase PT/INR
metronidazole, bactrim, cimetidine, omeprazole, fluconazole, voriconazole, ciprofloxacin, erythromycin, miconazole, simvastatin, amiodarone, cephalosporins w/ NMTT side chains, aspirin + nsaids
which drugs decrease PT/INR
cholestyramine, barbiturates, rifampin, carbamazepine