L9 NEUROCLIN II Clinical Trials and Drug Discovery
1/105
Earn XP
Description and Tags
To know the brief history of how clinical trials were developed To recall what a clinical trial is and the key steps involved. To explain important terminology used in clinical trials To describe the roles academics, researchers, patients and institutions take in clinical trials and their responsibilities. To describe the basic principles of the drug discovery process
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
106 Terms
what is the first written documentation of a (sort of) novice clinical trial?
Book of Daniel, Old Testament, Bible
King Nebuchadnezzar ordered his ppl to eat only meat and drink only wine to keep them strong
several young men of royal blood objected as they only ate vegetables
king allowed them to eat legumes and water for only 10 days
atp vegetarians appeared more nourished than the meat eaters
→ altho not a clinical trial, first example of human experiment guiding decision abt public health
valley of death
when u go from research in lab to treatment of patients
where 95% of all promising drugs fail
after the drug discovery phase
current treatments on the market for Alzheimer’s disease
only 2
only slow Alz by 27% in a very specific population and have very bad side effects
clinical trial
medical research studies involving ppl
not just for drugs, interventions- e.g. cld be interventions to modify lifestyle or behaviour
can be done for many diff reasons
reasons clinical trials are used
prevent disease + reduce number of ppl who become ill (e.g. vaccinations)
treat illness + increase number of ppl cured
improve quality of life for ppl living with illness- reducing symptoms or side effects (e.g. currently untreatable conditions like dementia, can use technologies/robotics, assistive techn in the home)
for disease diagnosis + health problems (e.g. can a blood test to develop alz 25y earlier be developed?)
brief history of clinical trials
book of daniel, old testmanet
1747 scurvy clinical trial, james lind
Jenner, 1790-1800s
European clinical trials in hospitals + Jenner
1800s- emergence of plecebo, defined 1811
1863: USA Medic Autstin Flint used placebo in clinical study
1943: first double-blind controlled trial (Patulin, penecillin related) (MRC)
1946: first randomised curative trial- using streptomycin to treat TB (MRC)
one of the first clinical trials in the modern era
Scurvy clinical trial, James Lind, 1747
James Lind, 1747
scurvy trial
first clinical trial in modern era
scurvy terrible disease effecting sailors on ships- lesions → death
lind thought related to diet
split sailors into 6 groups with diff food and drinks
had 12 sailors w scurvy and treated them w separate food supplements
two sailors who had oranges and lemons recovered v quickly and a third who had cider was the next best
vitamin c deficiency → scurvy
James Lind, 1753
using his 1747 findings, published Treatis On Scurvy
not only first desc of a controlled trial but also a systematic review of the previous literature on scurvy
took british navy 50 years to adopt the findings in full
James Lind impacted modern clinical trials how?
first one in modern era
published lit review w his findings
still part of modern clinical trials
must to lit review to assess what been done prior to ur trial
Edward Jenner reasoning
sidestepped clinical trial process
1700s, rural England
been taking notes and making observations on patient population for years
noticed all milk maids on farms did not contract the deadly small pox disease
hwvr all milk maids reported they had all prev caught a similar milder disease called cow pox, which did not have lasting effects
he reasoned the exposure to the milder disease somehow prevented them from getting the deadly disease
Edward Jenner May of 1796
performed the first ever experimental vaccination on an 8yo boy called James Phipps
escaped small pox so far, Jenner infected him with cow pox then exposed him to small pox
experiment worked- if this was done today scientist wld face jail
hwvr, argued this experiment led to modern vaccination which has saved the most human lives in history of science
vaccinations saves millions of lives a year
Jenner’s 1700s battle
when he presented his findings he was rejected and told to collect a larger sample data set
he did this , and the set included his own son
finally published Inquiry into the Causes and Effect of Variolae Vaccinae (1798)
but finding was still wildly ridiculed in society, especially amongst religious groups
battle from renaissance (where science was invented to prove gods existence) thruought history, even today
thght against god to put smth from a cow in a human
Jenner and 1800s development
not until 1800s several major hospitals across europe began to do studies (clinical trials)
only then cld Jenner’s vax method be robustly assessed
led to development of modern vax we see today
laid down foundations for rigorous clinical trials we see around the world
Jenner’s legacy
huge → saved most lives in all science
polio, aids, MMR, covid- groundwork for these vax
(he also gave James Phipps a house)
in 1800s, emergence of a very important term…
placebo
placebo was first defined as… (+ when, by who)
an epithet given to any medicine more to please than the benefit of the patient (Hoopers Medicial Dictionary, 1811)
first use of placebo
1863
USA medica Austin Flint used a placebo in a clinical study
he gave a ‘pleceboic remedy’ for rheumatism to patients
all reported positive effects, bc they thght was working, even tho placebo did nothing to treat disease
shows importance of having placebo in clinical trials to control for placebo effects → important compound to test for when assessing therapeutic efficacy
first double blind control trial
1943, testing Patulin, related to penicillin, wanted to try and treat common cold
1943 double blind control trial
first one
testing Patulin, related to penicillin, to try and treat common cold
never cured common cold so didnt work
carried out by medical research council (MRC)
recruited 1000+ subjects from british offices and factory workers suffering from common cold- difficult in wartime
both drs and patients blinded to the treatment
→ failed to show effect
Medical Research Council
set up to promote human health
assess which clinical trials to fund
still funds lots to this day
strength of double bind
protects against bias
when was first randomised curative trial
1946, using streptomycin to treat TB, carried out by MRC
1946 first randomised curative trial
using streptomycin to treat tb
carried out by mrc
patients had systematic and randomised enrolment rather than alternating, as used in prev studies into treatment and control groups
drs looking at x ray results were blinded to diff patient groups- did not know which was treated and which not
study set group work for basis of clinical trials (randomised control ones) we see today
→ included establishment of national and international regulatory frameworks globally
why are clinical trials important?
health professionals need evidence for best way to compare approaches
want to be able to properly test different treatments
ensure using most optimised treatment for separate patient populations
what could happen without clinical trials?
patients cld be given meds that do not work
→ wastes resources bc expensive
→ worse, meds cld be given that make patients worse or are not safe
who is in control of clinical trial process?
generally designed by doctors and other specialists but involve wide variety of people:
doctors, nurses, patients, statisticians, trial managers, and representatives from pharmaceutical companies to design the best possible trial
designed to offer least risk to patient but maximum potential new treatment/intervention being tested
what do statisticians do?
calculating the power of study, e.g. how many animals needed in preclinical aspect or patients needed to see if statistical difference
pharmaceutical companies role in clinical trials
get bad press
investing money into process
will make profit in the end
key player in it bc provide resources ans tend to be able to do things at scale re manufacturing of drugs
what are clinical trials designed to offer?
least risk to a patient plus maximise potential of intervention being test
what should be done before a clinical trial?
systematic review of previous trials
look at similar drugs, is there gap in market, is smth that can be taken further or has it been done before etc
systematic review of previous trials performed in same area of disease using similar drugs to assess firstly whether research already been done (so no need for trial)
gaining ethical approval
who is trial protocol sent to
who does this include
what do they do
what do they focus on
trial protocol sent to research ethics committee
independent group of ppl that includes doctors, nurses, other medical staff, members of public, sometimes lawyers
decide whether trial is ethical
focus on:
do the potential benefits of treatment/intervention outweigh costs?
that information provided to potential Ps is clear and satisfactory
will ppl be approached in appropriate way
emotional involvement, cannot force or promise ppl, be objective and clear, clear they may not even get treatment
is compensation in place for Ps if smth goes wrong?
often checkpoints in place in case
sometimes if trial going rly well can move placebo group onto drug but only if stats in place and proper controls in place to ensure satisfied all criteria, otherwise u cannot move onto next stage
trials often stopped early bc found side effect not anticipated even w pre clinical testing
travel expenses- are they in place?
trial can start only once ethical approval in place
what type of research is becoming funded a lot more in alzheimers + why?
patient led/ patient involved research
bc what patients to buy into what is going on, so younger ones can understand what is being tested and how it can even benefit then
can involve friends and family of those suffering bc they important voice to be heard
legal NHS perspective in UK, what do you need for a clinical trial?
a sponsor
sponsor (in context of NHS research)
nhs trust, individual, company, instituition, or group of organisations that takes on responsibility for initiation, management, and financing of research
what must all research falling under the remit of Secretary of State for Health have?
a formal sponsor
→ includes insurance provision
sponsorship of involving medicines
legal requirement for any clinical trial of aan investigational medicinal product (CTIMP) to be sponsored
this includes provision for insurance in case things go wrong
why sponsors neccessary?
mitigate any bad effects if something does go wrong
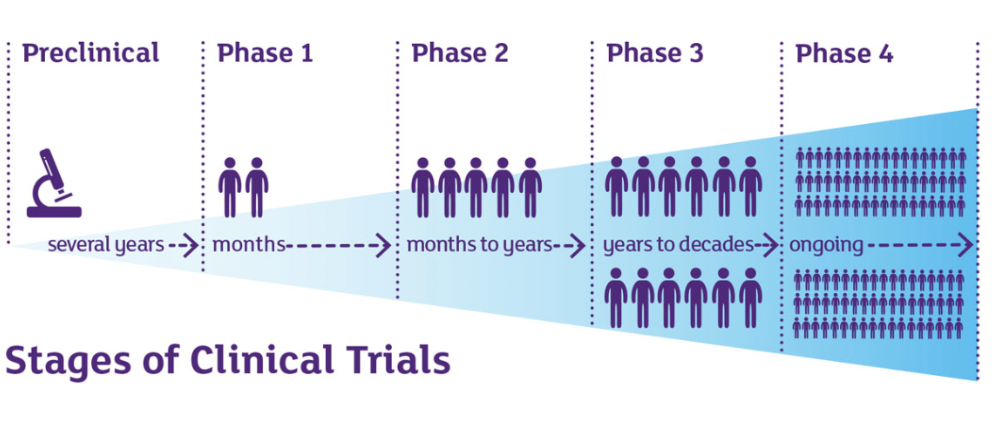
what are the distinct phases of clinical trials + their durations?
there are 4 stages
preclinical (several years)- drug discovery process
phase 1 (months) - early stage, usually small groups of health subjects but sometimes patients, safety, large side effects
phase 2 (months to years) - lot more known, larger group of ppl, see if positive effect in patients, side effects
phase 3 (years to decades)- 100-1000s of ppl, often international, compare new drug to standard treatment, how well works/length of effects/side effects
phase 4 (ongoing)- licensed and used as treatment, large population, long term risks and benefits, rare side effects
phase 1- clinical trial
early stage
months
generally small groups of health subjects
sometimes patients
used to test how safe treatment is- are there any large side effects?
in cancer research:
small, <30ppl
designed to find safe dose of new treatment, determine how treatment shld be given, learn how it affects body
if safe dose found, move to phase 2
phase 2- clinical trial
months to years
by this stage, a lot more known about the treatment
now tested in larger group of ppl to assess safety and side effects in greater detail
first time- see if treatment has positive effect in patients
in cancer research:
more patients enrolled, usually </=100
study how treatment affects body, how treatment works for certain type of cancer
if found to be safe and have some benefit, go to phase 3
phase 3- clinical trial
years to decades
moves up to hundreds if not 1000s of ppl
often international groups of ppl
compare new drug to a standard treatment
how well drug works
how long effects last for
finds out abt any serious side effects + how long they last for
need more longitinal, cld serious side effects be in smaller groups etc, test for rarer
in cancer research:
many Ps needed, usually 100+ and sometimes thousands
compare new treatment w current to see which is better
phase 4- clinical trial
ongoing
drug now licensed and being used as treatment
get stats on how well drug is working in large pop
any long term risks and benefits
rare side effects
key terms in clinical trials
placebo
controlled trials
blind trials + double blinded trials
randomisation
informed consent
what happens during a trial?
assess whether treatment is working
also assess:
any potential side effects
any new symptoms
wider effect of treatment such as quality of life, day to day activities
mental state- is treatment making u happy/sad, anx/dep
cost effectiveness of treatment- are u able to work, how often u need to visit doctor
what happens at the end of a trial?
trials can last for years altho as seen w COVID19 process can be dramatically sped up
all Ps will have access to results if want them
results published to help other researchers in field and allow advancements to be undertaken by all
in some instances, treatment used as part of trial may not be available on NHS- at end of trial will be given standard treatment
in some cases u may be able to buy new treatment
all ur info kept confidential- key requirement
what needs to happen before start of trial?
arrangements in place incase smth goes wrong and ppl are harmed
ethical committee can refuse permission if this not in place
important for Ps to know insurance in place before trial starts
controlled trials
designed to compare different treatments
usually 2 groups
trials group - given new treatment
control group - given standard treatment
where no standard treatment, control may given none or may be given placbo
importance of controlled trial
understand if new drug better than standard
esp bc standardised more likely to be off patent, meaning cheap, whereas new one probably controlled by pharmaceutical company which cld cost fortune, so need to ensure doing smth better than standard treatment
what point have a lot of Alz drugs failed + impact?
at controlled trials
costing billions of pounds
found it works in preclinical models, e.g mice
but not translated
blind trial
Ps not told which group they are in
blind trial challenges and importance
can be very difficult on patients and families, especially if complicated and/or life threatening disease, bc dk if recieving poss treatment or placebo
protect integrity of trial
doubled blind trial
means Ps and teams treating them do not know which group they are in
→ takes away bias of treatment team treating patient in terms of hoping going to work
what is important re blind trial
for all groups not to know or guess which one they are in - treatments must look identical
randomisation
essential and usually assigned by a computer
ensures no biases and groups have similar mix of age,sex, health state
with random allocation- if one groups does better than the other, likely that treatment is working
if left to doc to assign, may be influenced by putting treatments think will respond into treatment group - biasing outcome
informed consent
researcher shld always ask ur consent and permission to enter u into a clinical trial
cannot be entered into one without consent
few exceptions
exceptional circumstances re informed consent
children and other vulnerable groups who lack capacity:
consent process may be different and ppl may be entered into trial w/o their consent, e.g.:
treatment of severe head injuries
dementia
if patient lacks ability to give consent
→ in these examples, relatives or other legal representatives play a key role to safeguard inclusion of those who cannot consent
exceptional circumstances re informed consent- children
process involving children is different and has to be fully explained by trial recruiter
in these cases the P or representative must be told:
the aim of the study- what it is trying to find out
how u will be treated
what u will need to do to stay in trial- commitments
what possible risks and benefits are
enough info needed to allow deciison to be made to give ur informed consent
questions shld be encouraged + time given to make decision + no pressuring/coercion to family or anyone, regarding time to decide or space to decide etc
→ language right when beginning recruitment
issue w post treatment
sometimes drugs are shown to work, but regulatory panel in uk- NICE, say they are too expensive for small amounts of benefits they produce
in these cases, patient shld be given option to buy it outside of NHS
problem is, e.g. w alz drugs in states, u can buy in uk but costs 50k. option is there if have resources to get it but not accessible.
ethical issue re inequalities in healthcare bc only rich can afford the treatments
big problem going forward too
NICE is there to keep level playing field so if something is effective even if it costs mills it will go on NHS
but bc not endless money, NICE difficultly balance and weigh up between drugs worth it for population of uk as a whole
leaves some without support
confidentiality
all info kept confidental
reason partially for ethics application
is data on subjects going to be anonymised, how to store it, any chance of data leaks etc?
if funded by MRC, have criteria for gov funded research where must keep data secure in its original format for over 10 years and also make that accessible to anybody else that wants it
open science
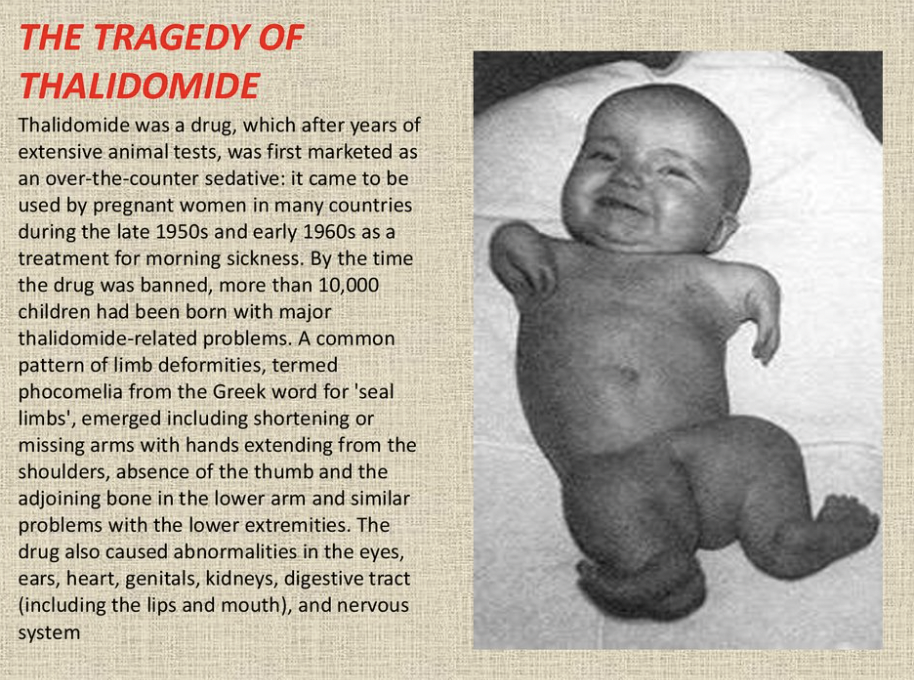
case where clinical trial went terribly wrong everywhere (except the usa)
thalidomide 1960s
thalidomide 1960s
“one of darkest episodes of pharmaceutical research history”
drug marketed as a mild sleeping pill safe for even pregnant women in late 1950s
as it seemed to reduce morning sickness, many pregnant ppl took it
caused thousands of babies worldwide to be born with malformed limbs
during testing process on animals, no tests were included to look at effects on pregnancy
damage revealed in 1962- before then, every new drug was seen as beneficial
hwvr, thalidomide been shown to reduce the symptoms of leprosy and still used to treat it
in usa: boss of FDA, frances kelsey, despite huge pressure from pharma industry refused a license bc she felt insufficient evidence for its safety- john f kennedy praised her as national heroine
big issue w thalidomide
preclinical testing
not tested on pregnant animals
missing chance to identify if something very wrong with drug
in usa- thousands of baby saved but only by one strong woman, needed more robust clinical trials
cost of clinical trials
very expensive
calculated that avg cost of a 5.5 year non pharmacological clinical trial involving collecting data across 20 centres in uk (stage 2 or 3) wld cost on avg, £1 million to administer
staff needed were highest costs, including managers, researchers, statisticiains, around 30% costs for non-staffing expenses like ethical approval
in uk, price of taking a drug from development to market is £1.1 billion
1/10 drugs make it thru to stage 4 in clinical trials
partially explains why drugs developed are so expensive- bc companies have so many failures
calculated that avg cost of a 5.5 year non-pharmacological clinical trial involving collecting data across 20 centres in uk (stage 2 or 3) wld cost on avg…
£1 million to administer
in uk, price of taking a drug from development to market is
£1.1 billion
how many drugs make it thru to stage 4 in CTs?
1/10
highest cost in clinical trials
staff needed, including managers, researchers, statisticiains,
around 30% costs for non-staffing expenses like ethical approval
also reducing dropout rate- big issue
what is changing in uk re pharmaceutical research and why?
the whole pharmaceutical research structure has changed bc it nearly bankrupted them
what they r changing to now, a lot of the big companies like Pfizer, AstraZeneca- they are actually closing down
was a massive site in Alley Park, one of biggest non-uni scientific centres in country all owned by AstraZeneca- now moved to cambridge
so now moving closer to big unis, bc unis can do a lot of the research, the preclinical stuff, and potentially for cheaper than a pharmaceutical company
and if that collaboration is better, that will ensure that the drugs won’t cost 1.1billlion
bc seen that it is too big a gamble for the pharma companies sometimes, bc once the drug comes thru, they have abt 10 years when they have the patents to make as much money as poss from that one drug and then fund the other drugs coming up
taking a step back- crucial process linked to clinical trials
drug discovery
→ important essential bc otherwise wld not have compounds/meds to test
valley of death
process of going from drug discovery to developing a new medicine
drug discovery vs clinical trials re cost
DD almost as expensive, esp getting data, and also has high failure rate
controversy + overview of current debates in field of drug discovery
problems where it has gone v wrong, how to make better
current play of field cld mean end of research done with mouse models of disease
cld not be a bad thing in terms of moving towards more patient cell-based systems- modern way
organ on a chip , brain organoids
things done now at SITran
gearing up for drug discovery process
part of research taking cell from forearm of MND or PD or Alz , take cell, and repurpose it back into a stem cell, differentiate it in a dish into a neuron/astrocyte - do research on cell based systems or even grow into mini brains if want to
sidestepping animal research bc human based cellular research
big advantages to that
one argument for value of animal research is in Jason research for example bc cannot get nice blood flow or cerebral blood flow in cell based system on a chip
altho ppl trying to build those too- artificial blood vessels based on human tissue
dynamic area of research + lots changing
pressures - lots of cmpanies developed to stem cell based research
Animal Rights lobby do not believe animal research shld progress
tensions which cld mean in NIH if doing prelin like him, must link to some human researchers → he thinks good think bc helps drug discovery and clinical trial process get more accurate results that do relate to humans
in gov, trying to reduce animal research by 30% in next 10 years
mistakes made via animal reseach, e.g. thalimode
big debate
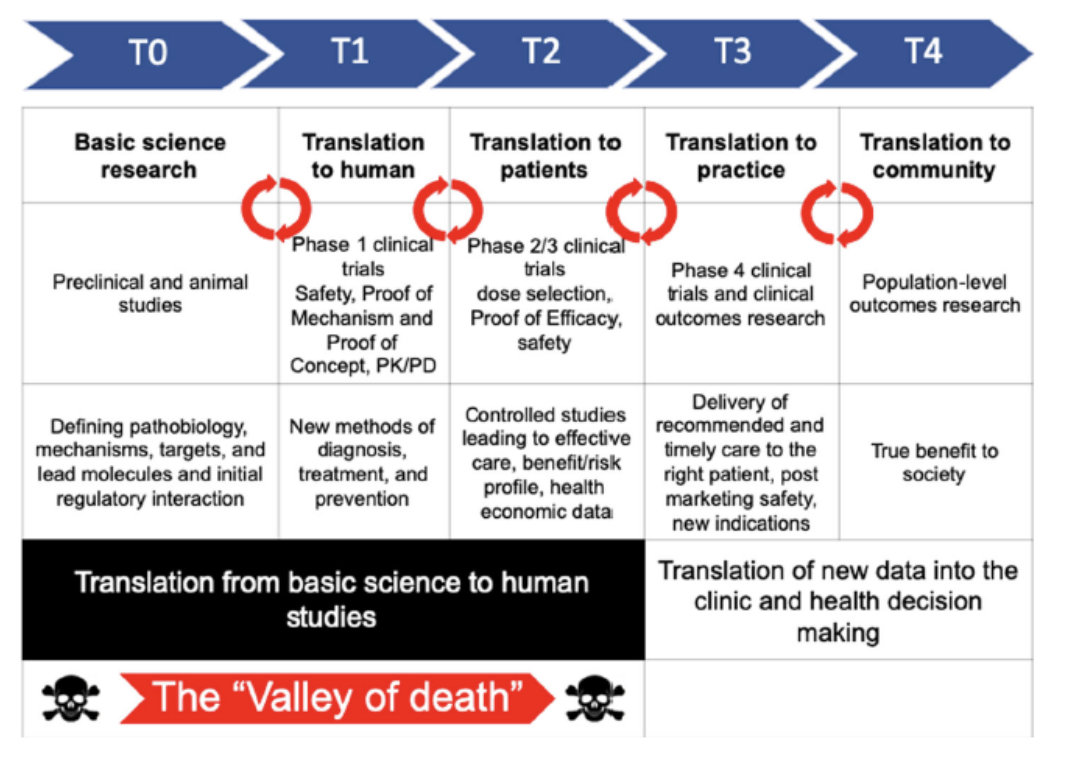
research process
T0: Basic Science Research
preclin and animal studies
defining pathology, mechanisms, targets, lead molecules, initial regulatory interaction
T1: Translation to Human
phase 1 clinical trials
safety, proof of mechanism, and proof of concept, pk/pd
new methods of diagnosis, treatment, and prevention
T2: Translation to Patients
phase 2/3 clinical trials
dose selection, proof of efficacy, safety
controlled studies leading to effective care, benefit/risk profile, health economic data
T3: Translation to Practice
phase 4 clinical trials and clinical outcomes research
delivery of recommended and timely care to the right patient, post marketing safety, new indications
T4: Translation to Community
population level outcomes research
true benefit to society
T0
Basic Science Research
preclin and animal studies
defining pathology, mechanisms, targets, lead molecules, initial regulatory interaction
T1
Translation to Human
phase 1 clinical trials
safety, proof of mechanism, and proof of concept, pk/pd
new methods of diagnosis, treatment, and prevention
T2
Translation to Patients
phase 2/3 clinical trials
dose selection, proof of efficacy, safety
controlled studies leading to effective care, benefit/risk profile, health economic data
T3
Translation to Practice
phase 4 clinical trials and clinical outcomes research
delivery of recommended and timely care to the right patient, post marketing safety, new indications
T4
Translation to Community
population level outcomes research
true benefit to society
where do the valleys of death fall
translation from basic science to human studies
between T0 and T1, T1 and T2, T2 and T3, T3 and T4
gap between academia and industry in translational science, education, academic drug discovery centres, business incubators/accelerators, academia, industry consortia where research dies-
causes of the valley of death
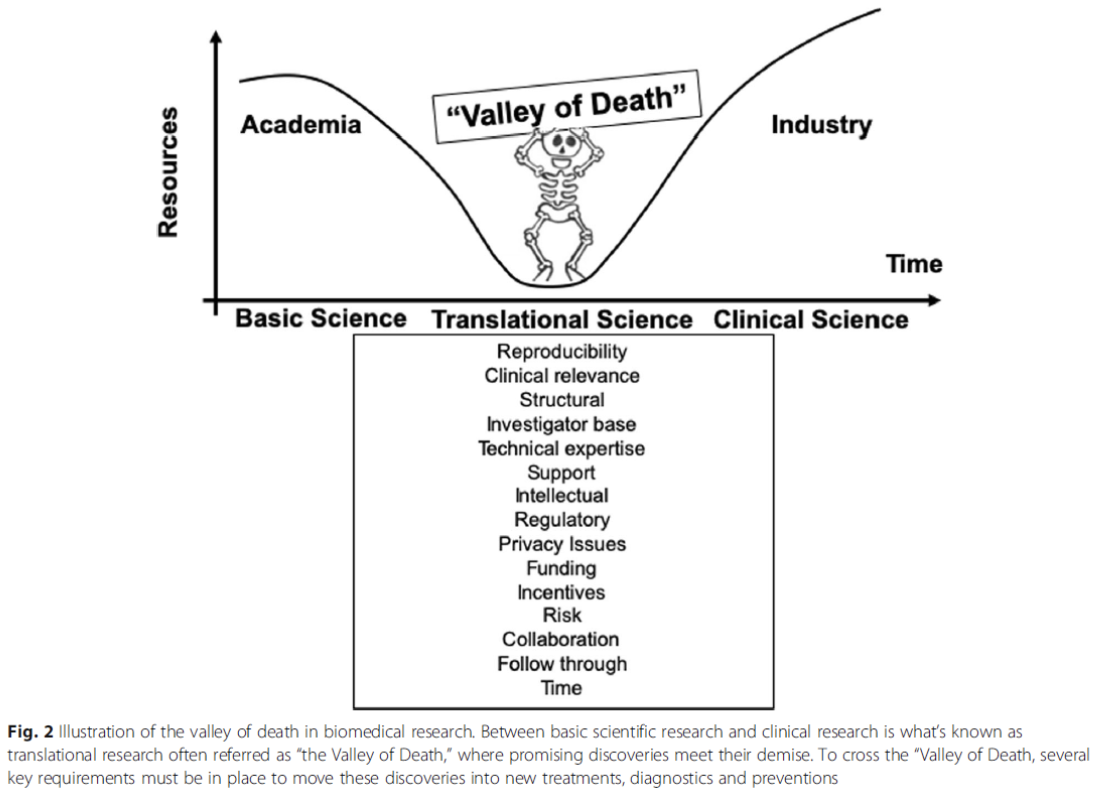
reproducibility
clinical relevance
structural
investigator base
technical expertise
support
intellectual
regulatory
privacy issues
funding
incentives
risk
collaboration
follow through
time
steps in the drug discovery process
discovery
→ screening
development
→ in vitro and in vivo testing
drug discovery - discovery
typically, researchers discover new drugs thru:
new insights into a disease process that allow researchers to design a product to stop or reverse the effects of disease
many tests or screening of compounds to find the possible beneficial effects against diseases
repurposing/orphan drugs: existing treatments that have unexpected effect against new disease → cld be quick route to clinic as often these drugs been safely tested already
proved true for potential covid19 treatments- vaccine methods that r already proven to be safe
new technologies- e.g. those providing new ways to target the medicine to specifics sites within the body, i.e. across BBB
at this stage- thousands of compounds may be potential candidates for development
after early testing, only a small number of compounds deemed promising + req further study
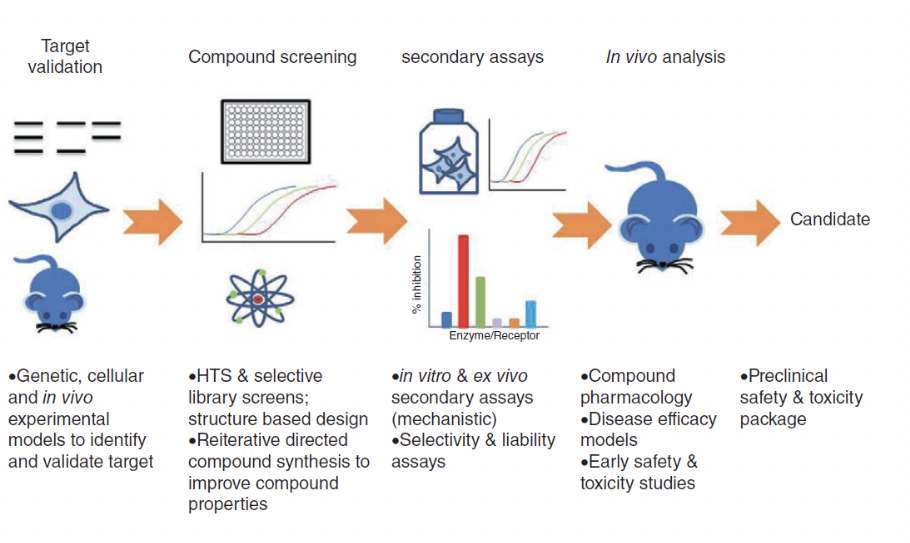
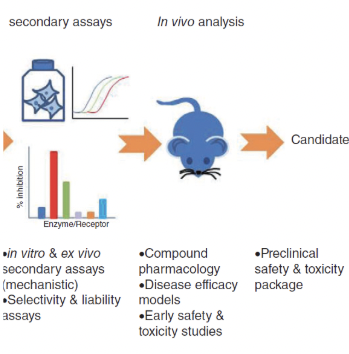
example method of drug screening
target validation: genetic, cellular, and in vivo experimental models to id and validate target
compound screening: HTS and selective library screens; structure based design. reiterative directed compound synthesis to improve compound properties
secondary assays: in vitro and ex vivo secondary assays (mechanistic). selectivity and liability assays.
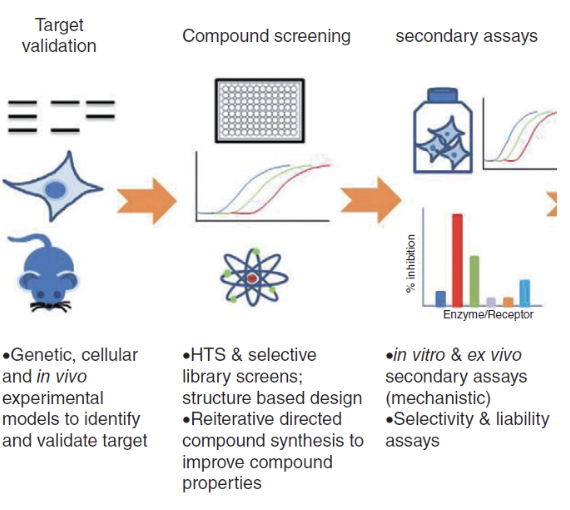
what does this show?
where is the point between discovery and development?
shows example of steps in drug discovery process
first three steps- example method of a drug screening (discovery)
last two steps- development
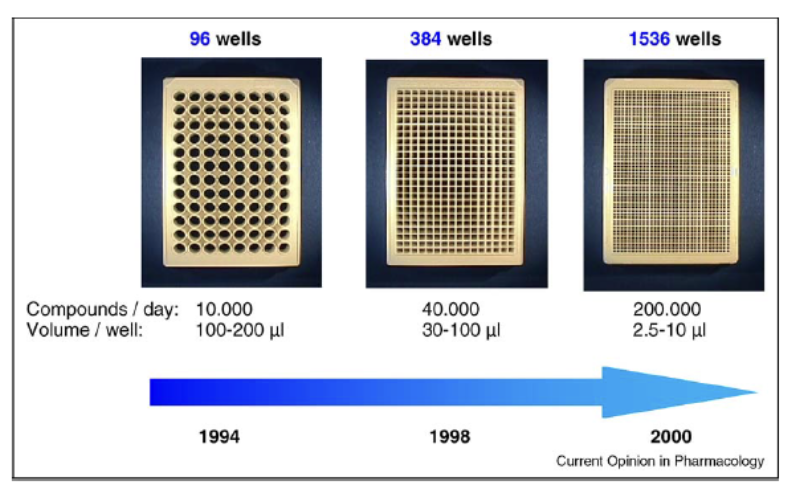
what is HTS
high throughput screening
test 100,000s of compounds against ur cell/animal model of choice
see which ones have effect u want without causing any toxicology problems
assess function of ur cell of choice e.g. astroyctes, measure activity, see which drugs have toxic effects
minaturisation of screening
development- drug discovery
once researchers ID’d promosing compound for development, conduct experiments to gather info on:
how it absorbed, distributed, metabolised, and excreted
potential benefits and mechanisms of action
best dosage
best way to give drug
how toxic the drug is
how it interacts w other drugs and treatments
how it compares to existing drugs
toxicity
potential (of a drug) to cause serious harm
two types of preclin research used to assess toxicity
in vitro
in vivo
in vitro
often looking at how cells in a test tube are effected by the treatment
in vivo
often involving small animals (usually mice, but some studies, esp brain diseases, non human primates may be used in later stages)
GLP
good laboratory practices
strict guidelines for preclin labs to adhere to
aims to standardise approaches and method
GLP sets minimum basic requirements for…
Study Conduct
personnel- training of staff
Facilities
equipment- safe and rigorously checked
written protocols for all experiments
standard operating procedures- minimising experimenter error
clearly writing study reports
quality assurance oversite for each program of work - ethical approval
preclin studies- size, info, etc
usually not large
must provide detailed info on dosing and toxicity levels
after preclin testing, review findings and decide whether to proceed to clinical trials
why do clinical studies fail? example from stroke research
accurate and repeatable strokes can be caused in rodents
hwvr, systematic review of literature showed that:
over 800 drugs been tested on animal models → 500 work in reducing stroke effects →100 went to clinical trials → only one become treatmentrandomised and blinded experiments had less favourable results
of 100 studies examined in a diff study, only 36% were randomised and 11% blinded- these are routine in clinical trials
why do clinical studies fail? example from alzheimer’s disease therapy research
billions £s investment - no disease-modifying alz drug has been developed, just 2 drugs slowing it down on market
many clinical trials failed, cld be bc:
wrong targets- most focus on beta amyloid plaques, cld be smth else, e.g. blood supply
interventions cld be too late- damage already done
early biomarkers needed- existing treatments cld be re-examined
clinical trials often <5 years- for alz, might not be long enough, but longer trial far more expensive
complex and difficult problems to solve
large cohort human studies may help esp in early biomarker detection
what era are we entering?
dig data era + its powers
large cohort human studies in AD
many underway
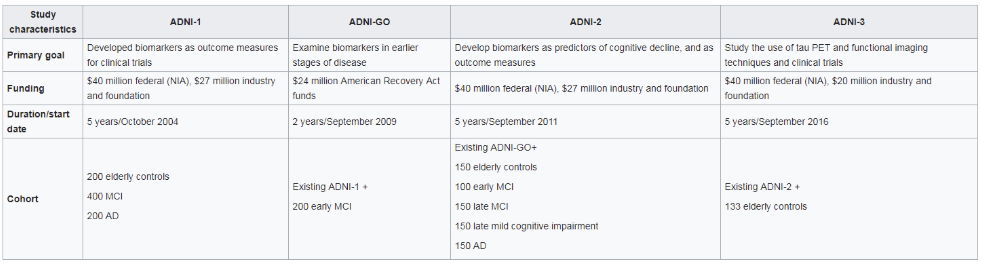
one of largest is Alzheimer’s Disease Neuroimaging Initiative - ADNI (USA)
ADNI
what is it
budget
what does it collect
tests include
large cohort study in AD
alzheimers disease neuroimaging initiative
astronomical budget
so far, $218m: multi modal data from elderly controls and AD patients
tests include:
detailed history of each patient and assessment of health and education
neuropsychological tests
genetic testing for risk factors- APOE4
lumbar puncture- CSF measurement
MRI + fMRI
PET for glucose consumption, tau, and beta amyloid
post mortem histology
does the ADNI approach work?
yes
Clifford Jack Diagram- theoretical figure of what shld be produced by all the ADNI studies: a complete time line of disease progression and potential to donate early biomarkers at critical time points for intervention
3393 papers been published from ADNI studies and keeps growing
a: Clifford Jack Diagram- theoretical/hypothetical model of late onset alzheimers disease progression
b: data driven model of late onset alzheimers disease progression
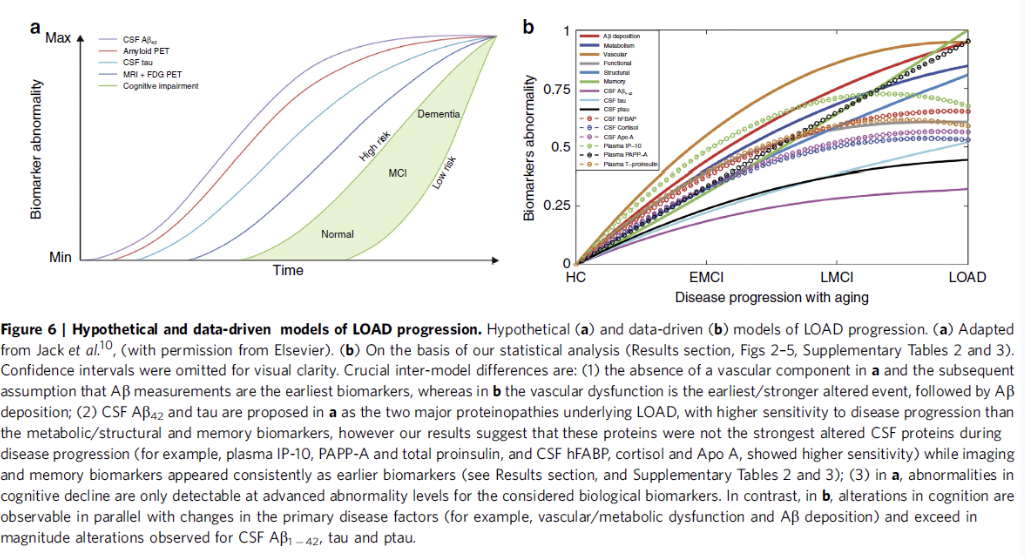
hc - healthy control
emci- early mild cognitive impairment
lmci- late mild cognitive impairment
load- late onset alzheimers disease