Combined set clin skills
1/337
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
338 Terms
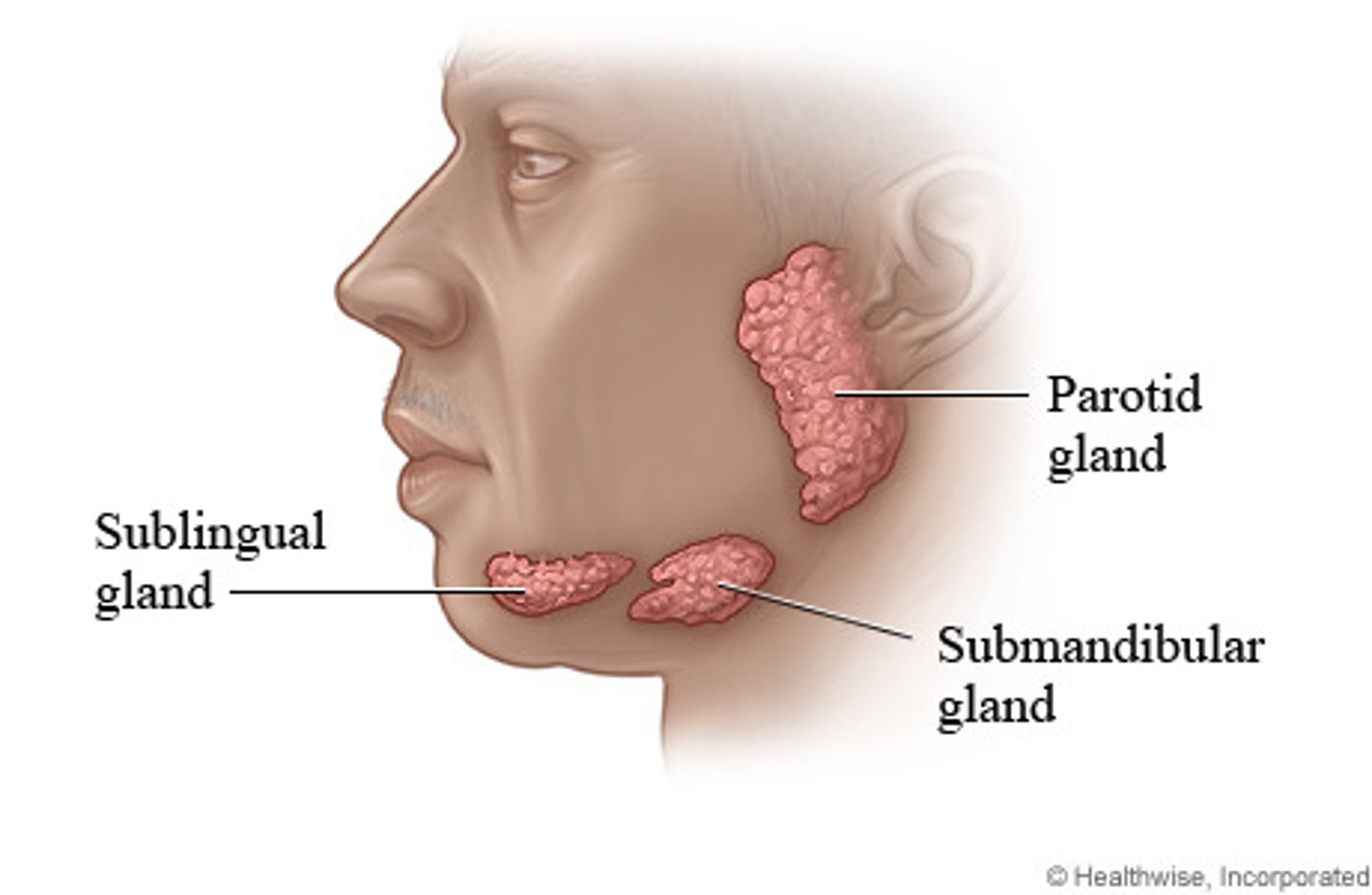
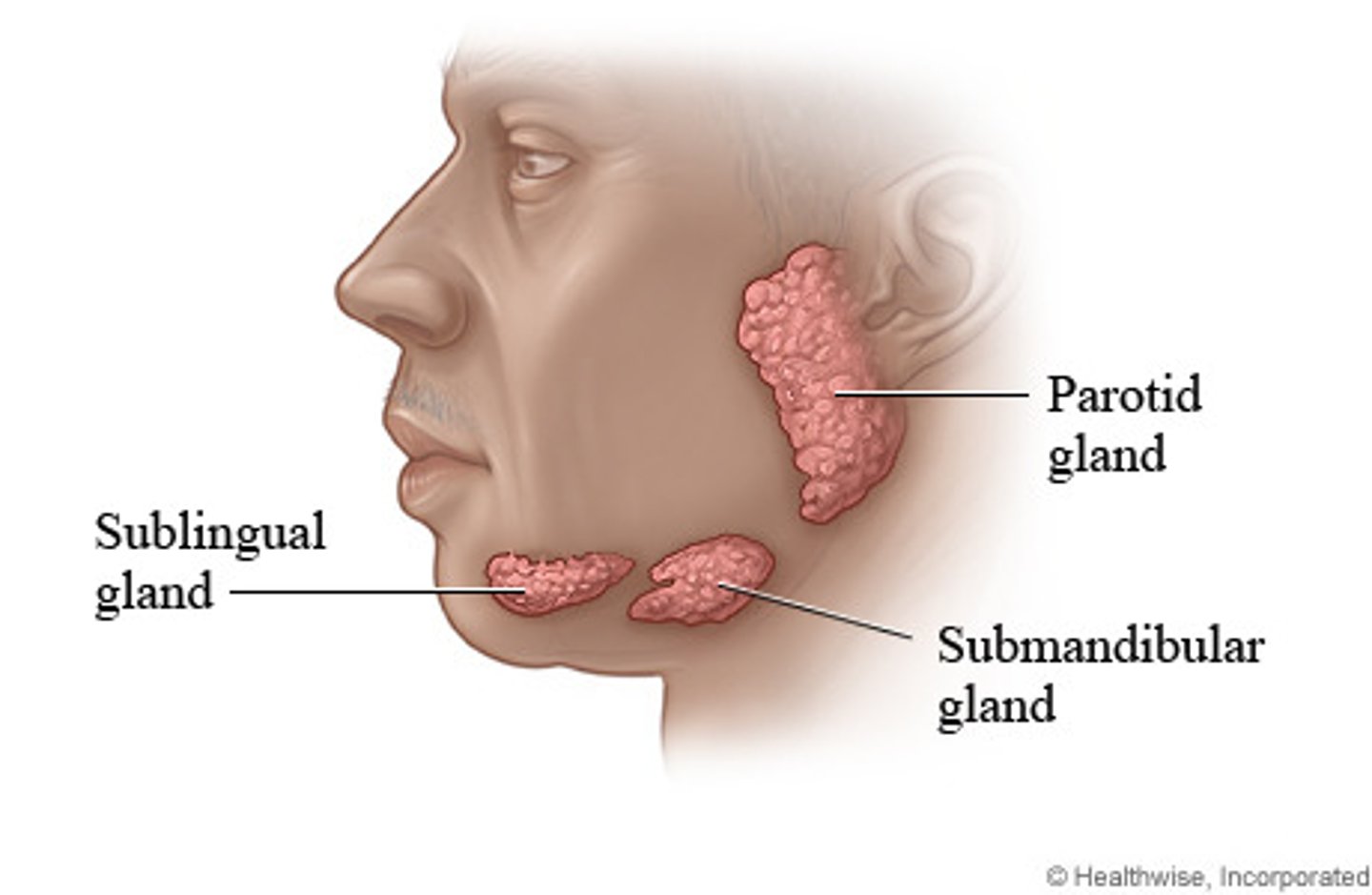
stenson's duct
parotid glands
-enters oral cavity through buccal mucosa opposite the upper second molar
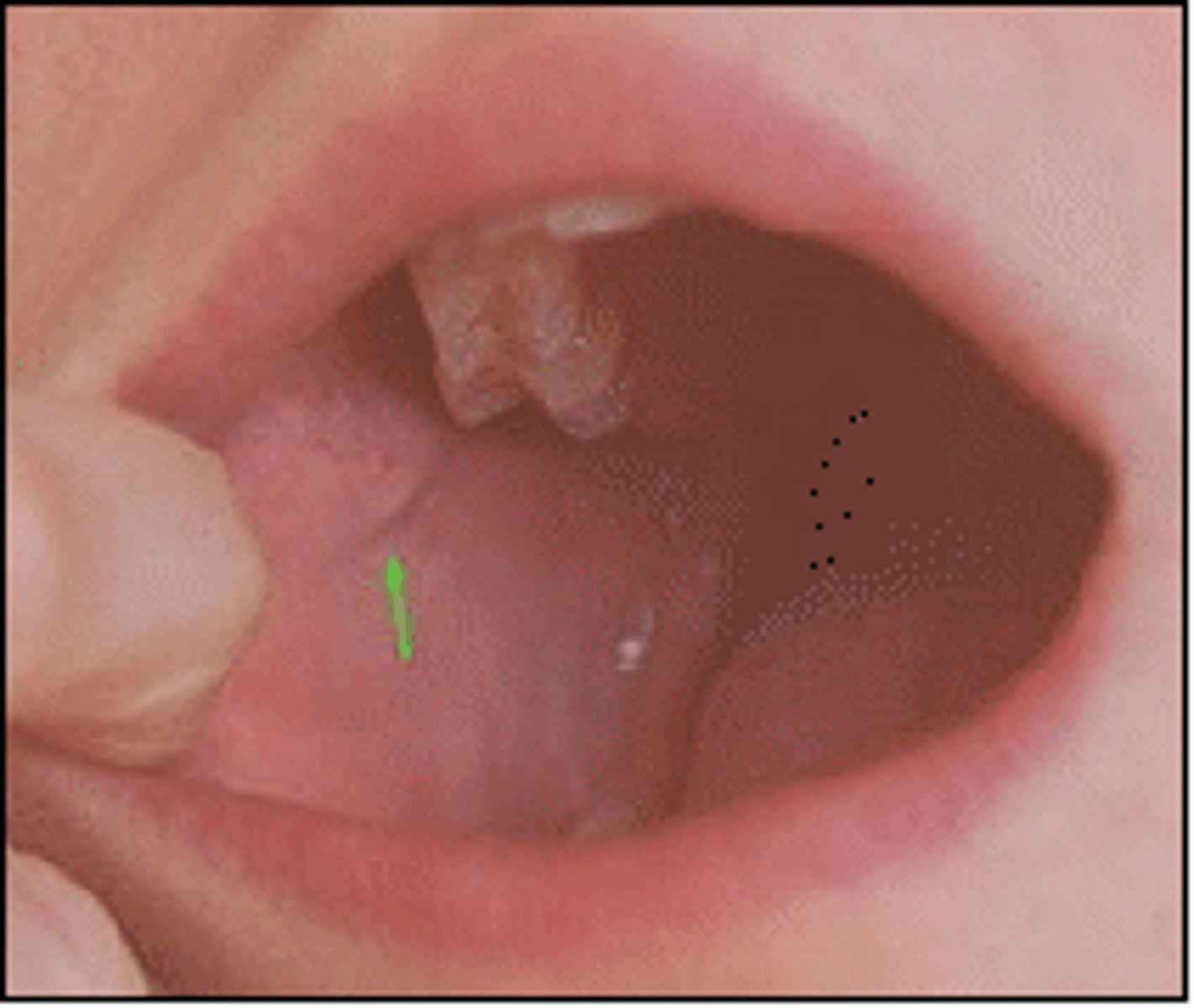
submandibular salivary glands
deep to the mandible, beneath floor of mouth
wharton's ducts
wharton's ducts
enters the floor of the mouth near the lingual frenula

sublingual glands
below mucous membranes of the floor of the mouth
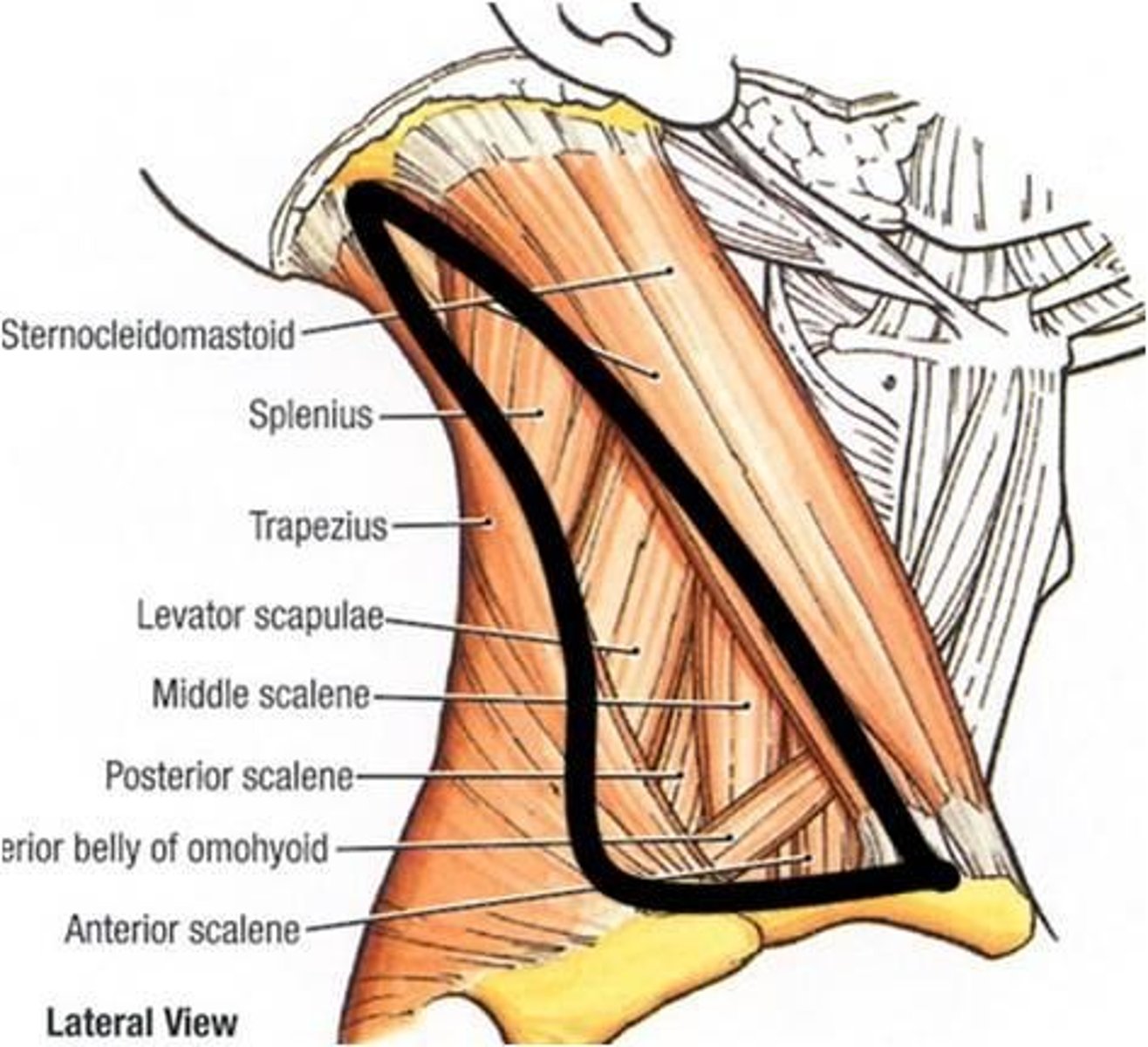
anterior cervical triangle
borders the mandible, anterior border of sternocleidomastoid, and neck midline
in front of SCM
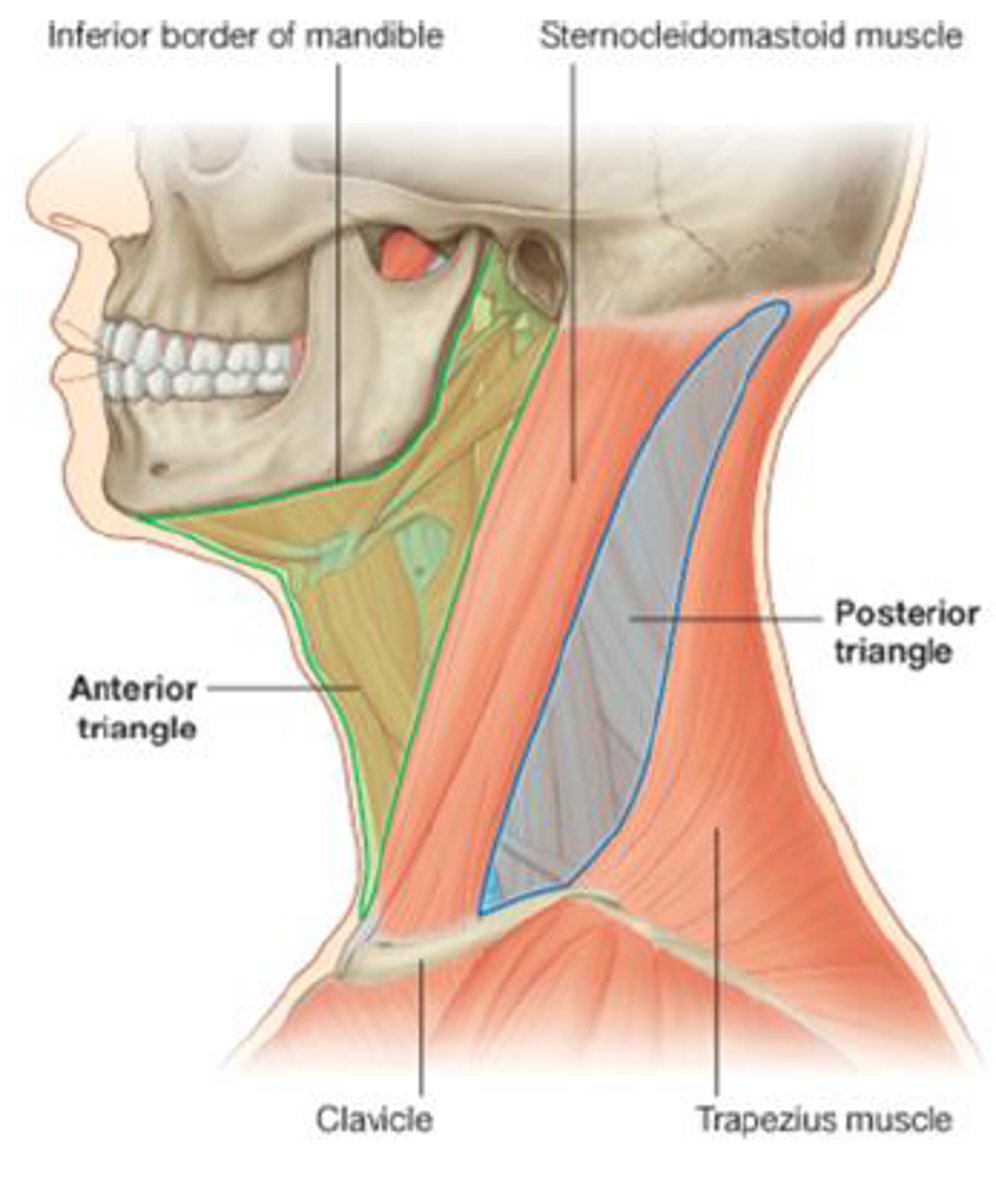
posterior cervical triangle
borders posterior border of sternocleidomastoid, trap and clavicle
behind SCM
common carotid artery (great arteries of neck)
internal carotid a. = intracranial
external carotid a. = extracranial
great veins of neck
internal and external jugular veins
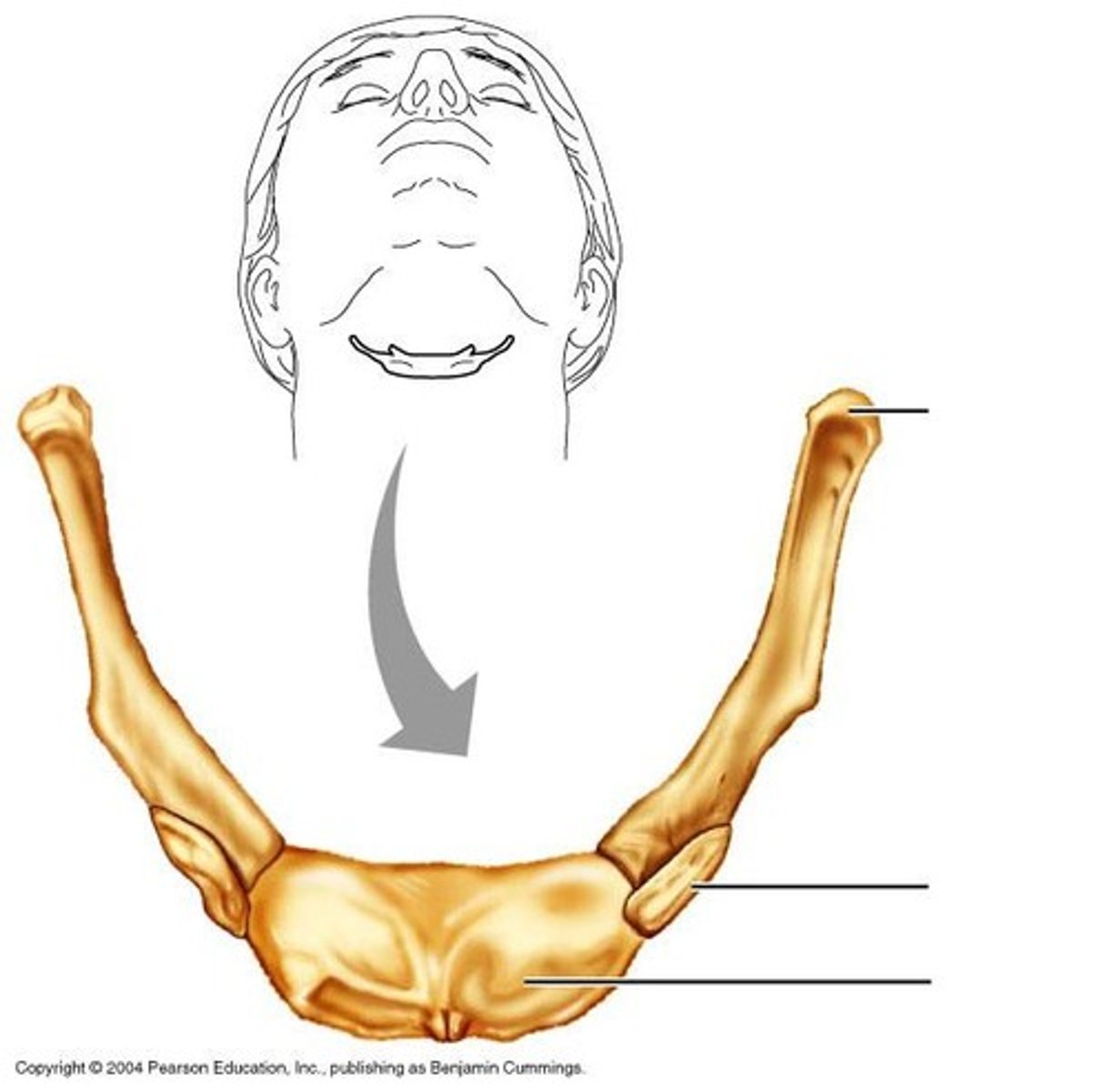
hyoid bone
mobile bone right below mandible
thyroid cartilage
adams apple - notch on superior edge
thyroid gland
just above suprasternal notch and isthmus
spans 2, 3, and 4 tracheal rings
order of midline neck cartilage
thyroid cartilage
cricoid ligament
cricoid cartilage
submental lymph node
directly behind mandible
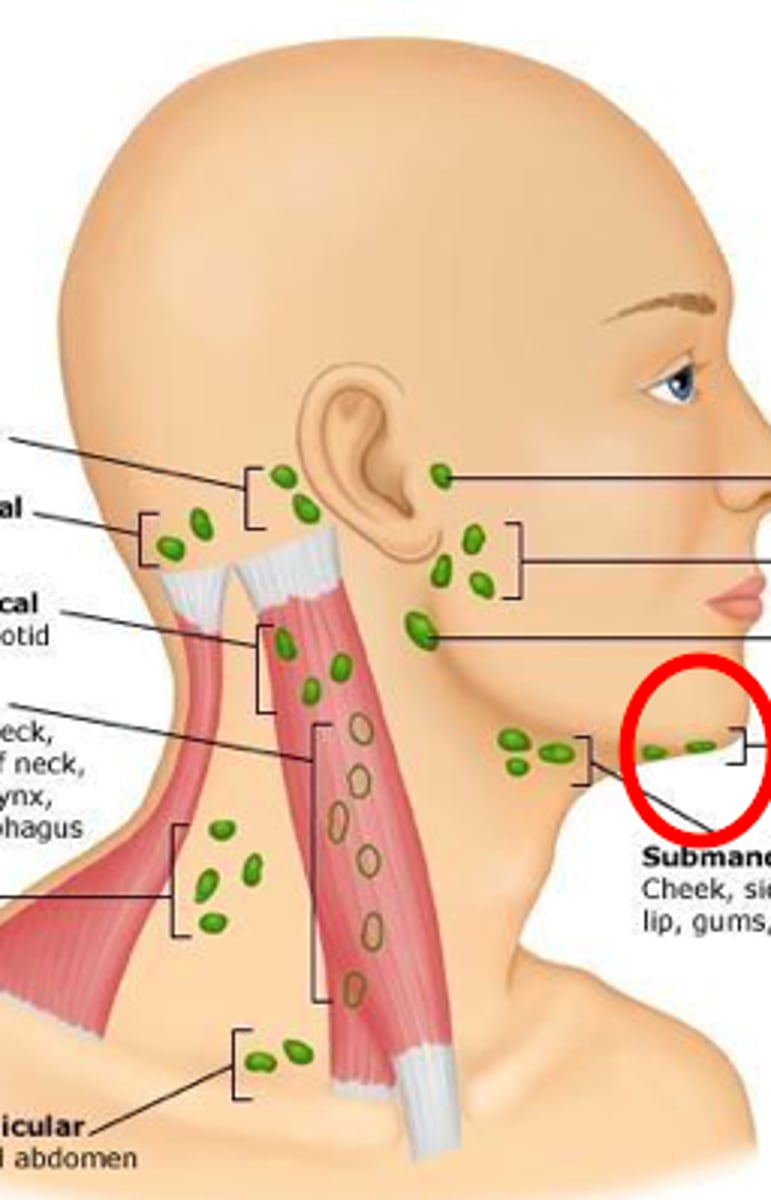
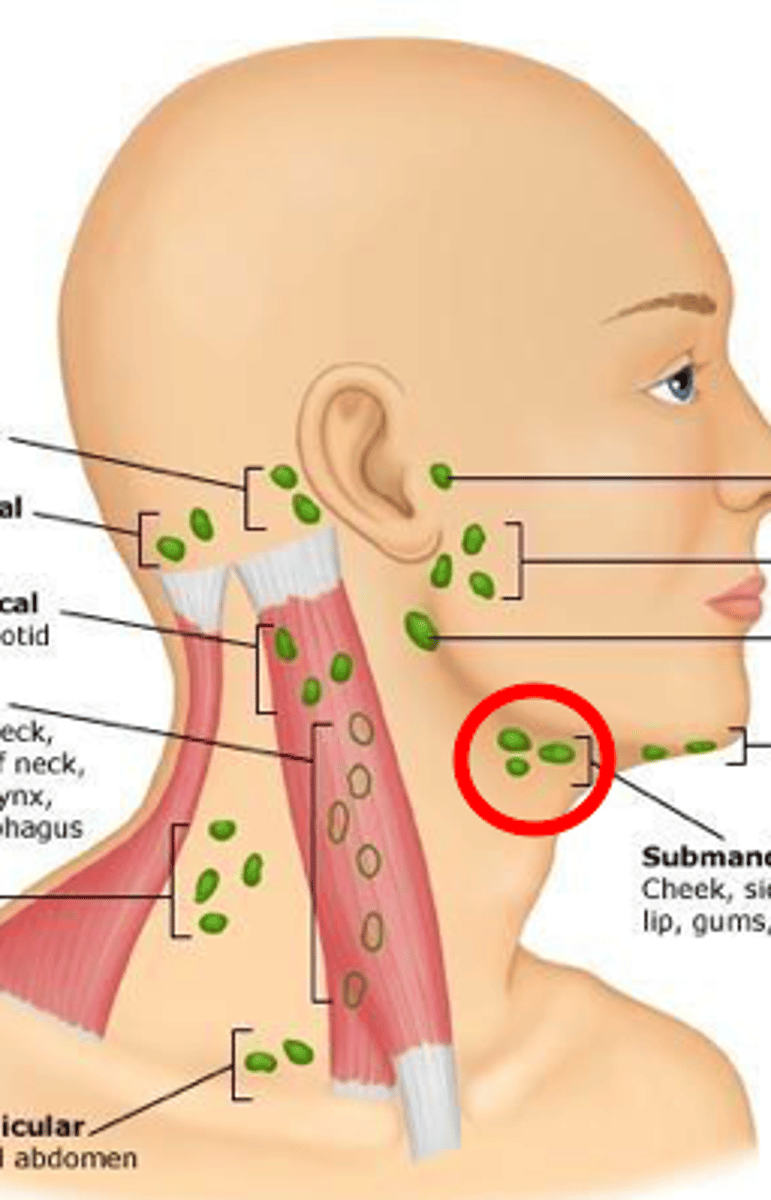
submandibular lymph node
midway point between mandible tip and angle
tonsillar lymph node
angle of mandible
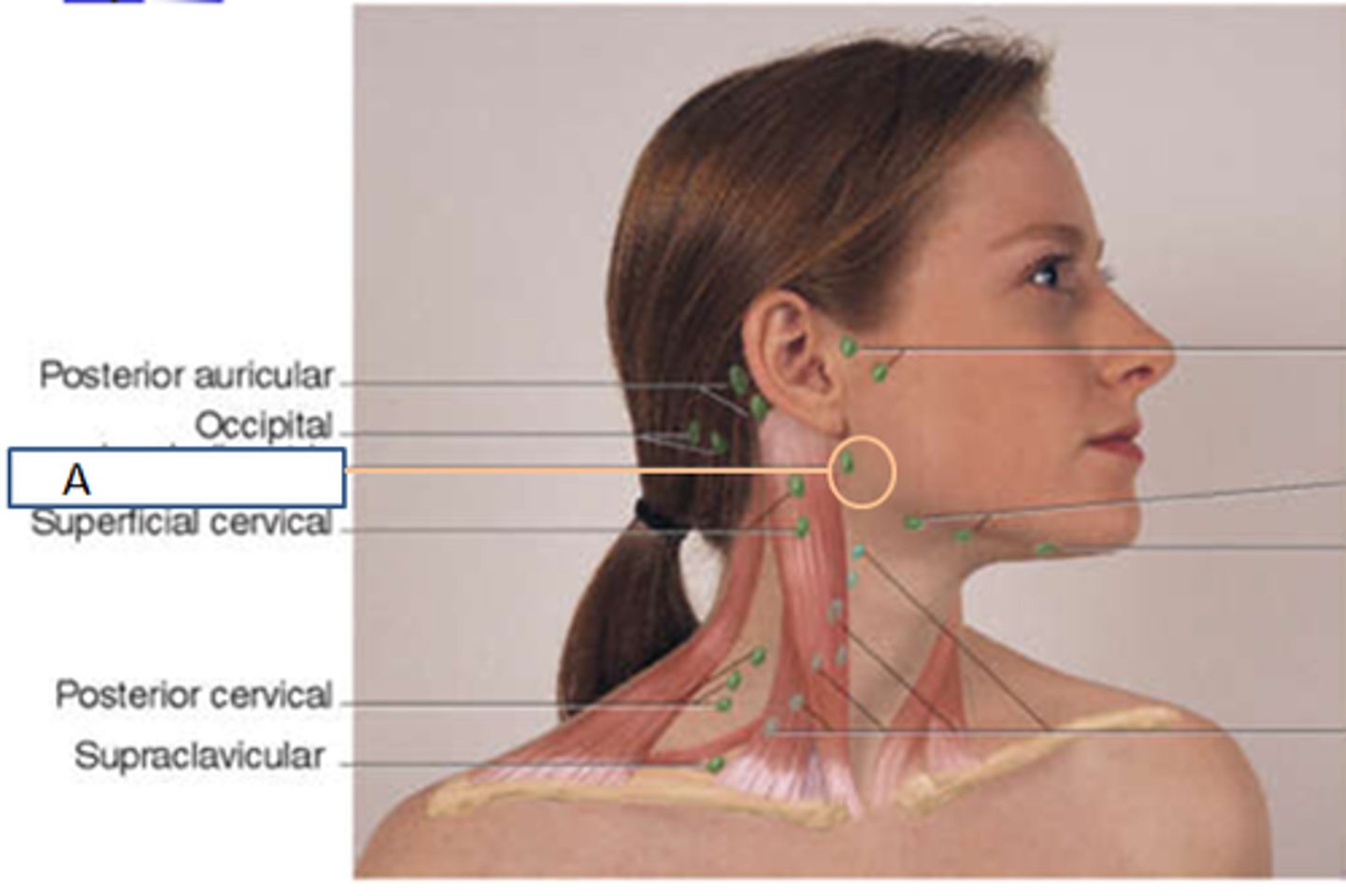
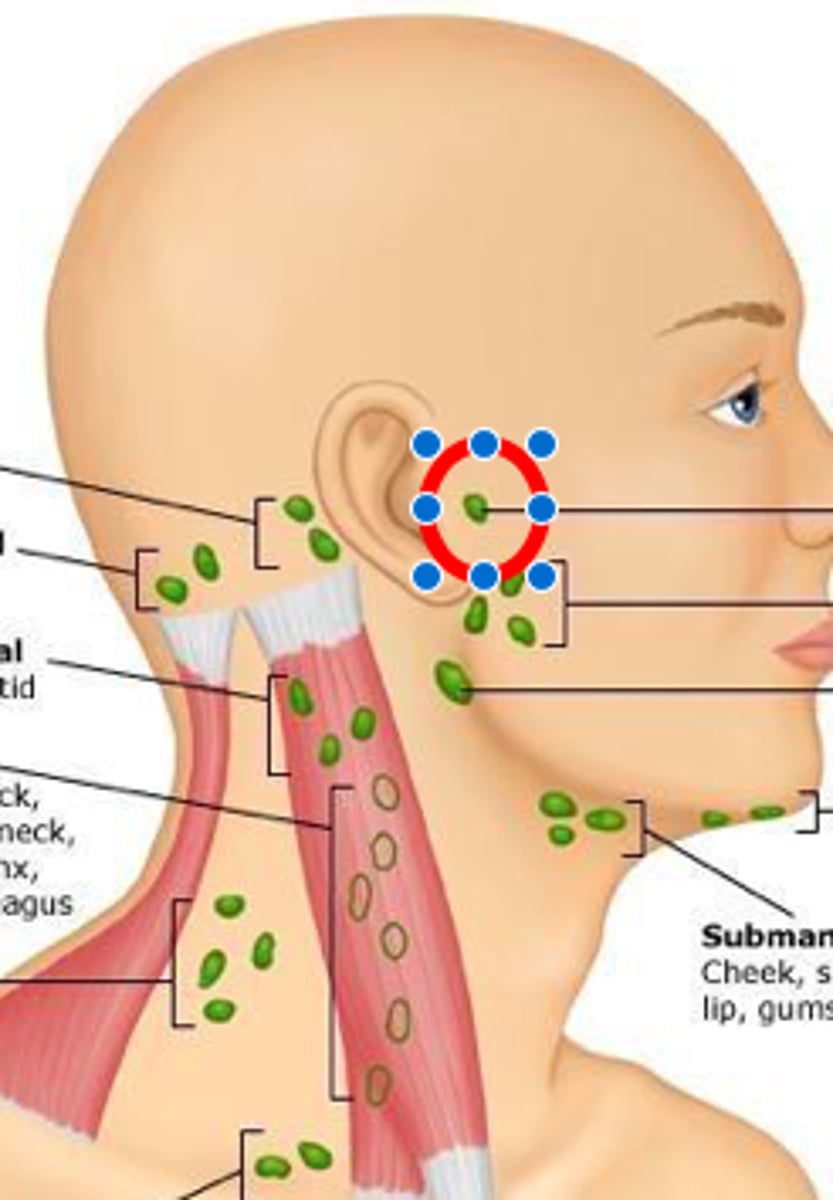
preauricular lymph node
in front of ear
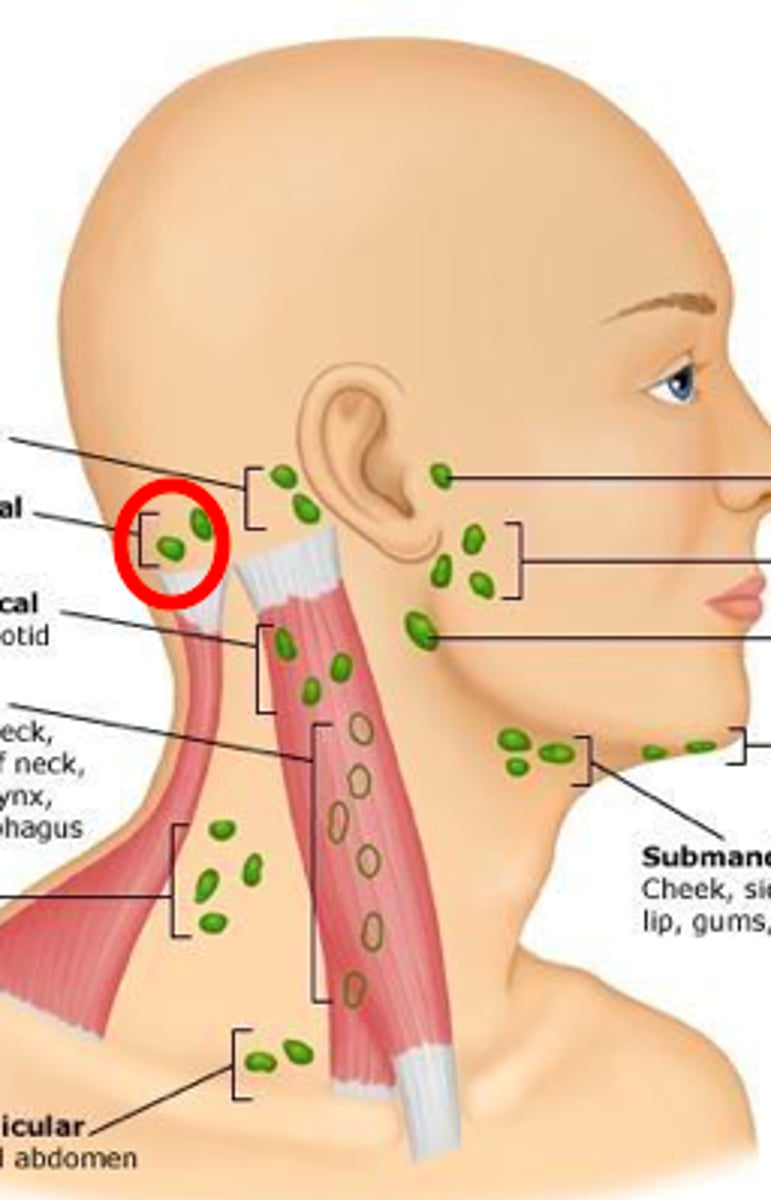
posterior auricular lymph node
behind ear
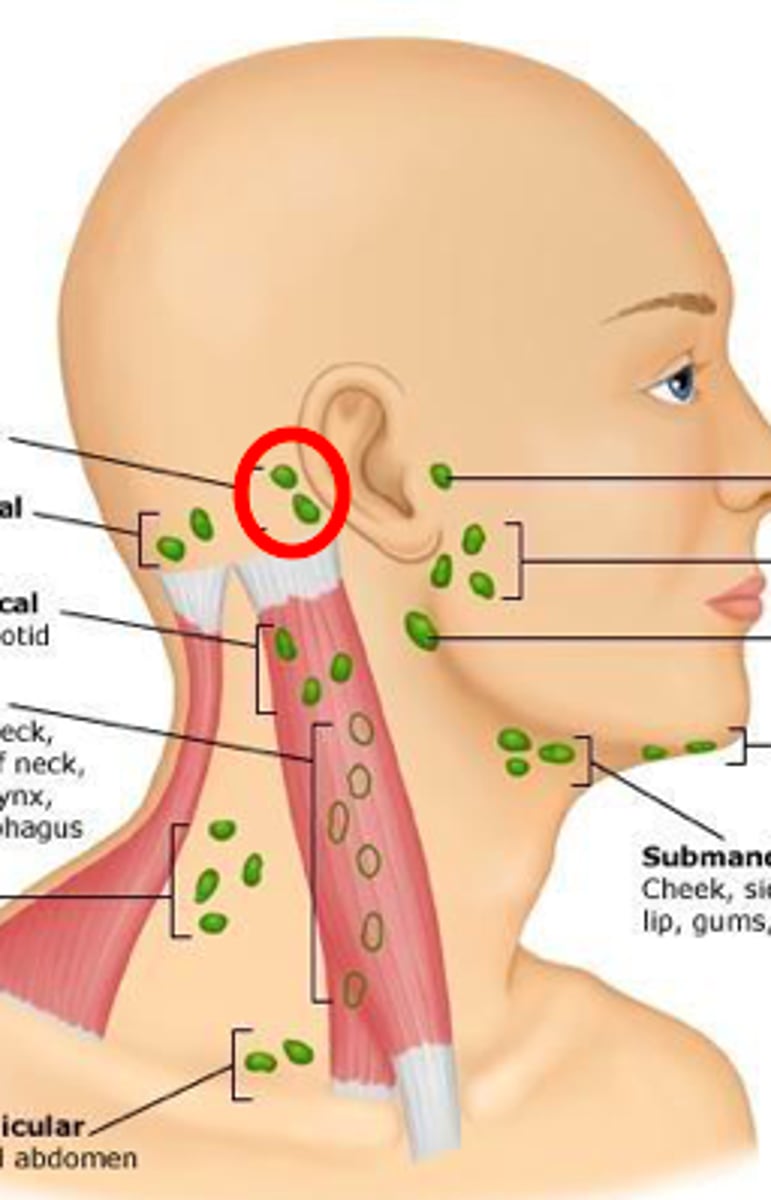
occipital lymph node
base of posterior skull
superficial anterior cervical lymph node
superficial to SCM muscle
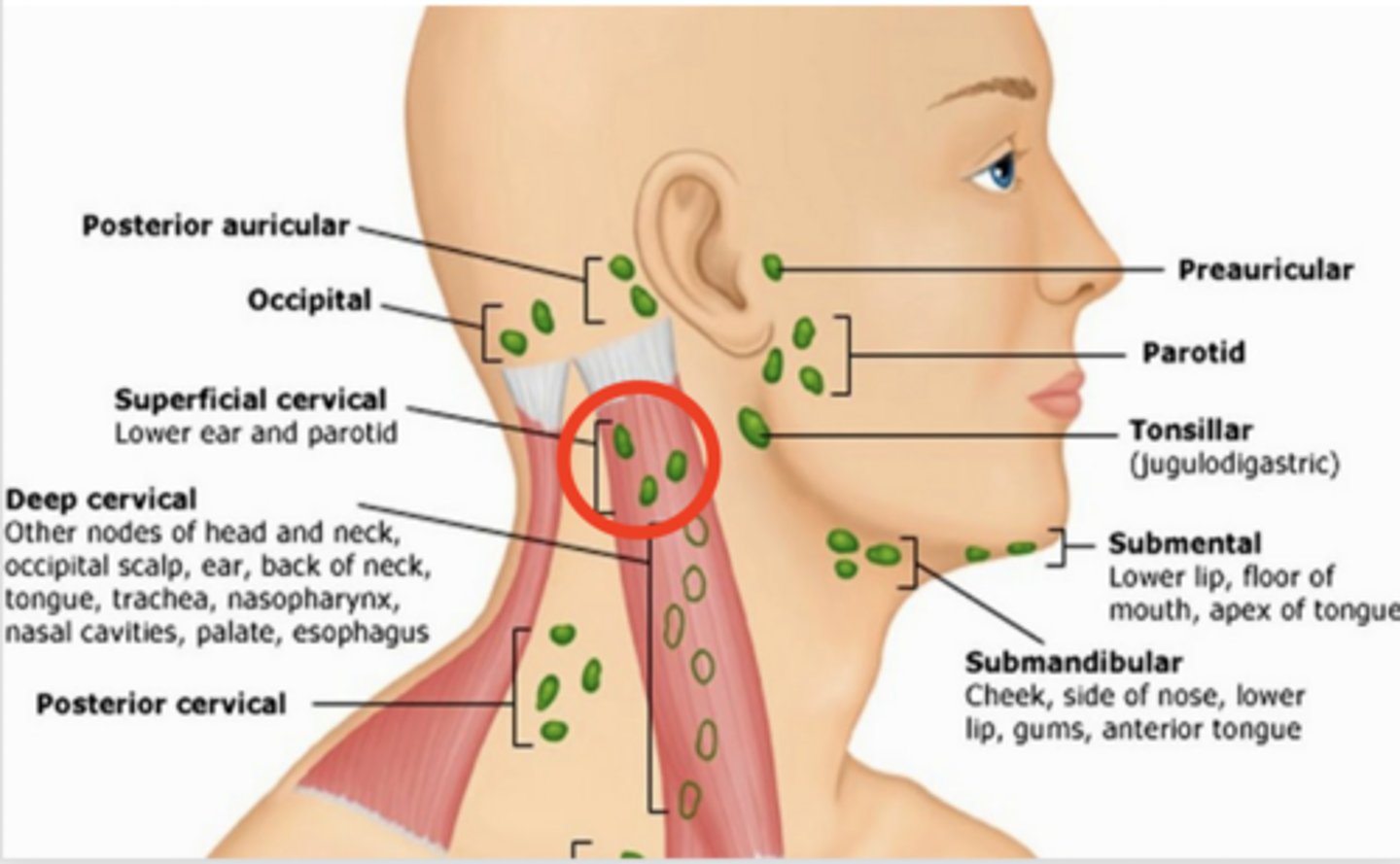
superficial posterior cervical lymph node
along anterior edge of trapezius
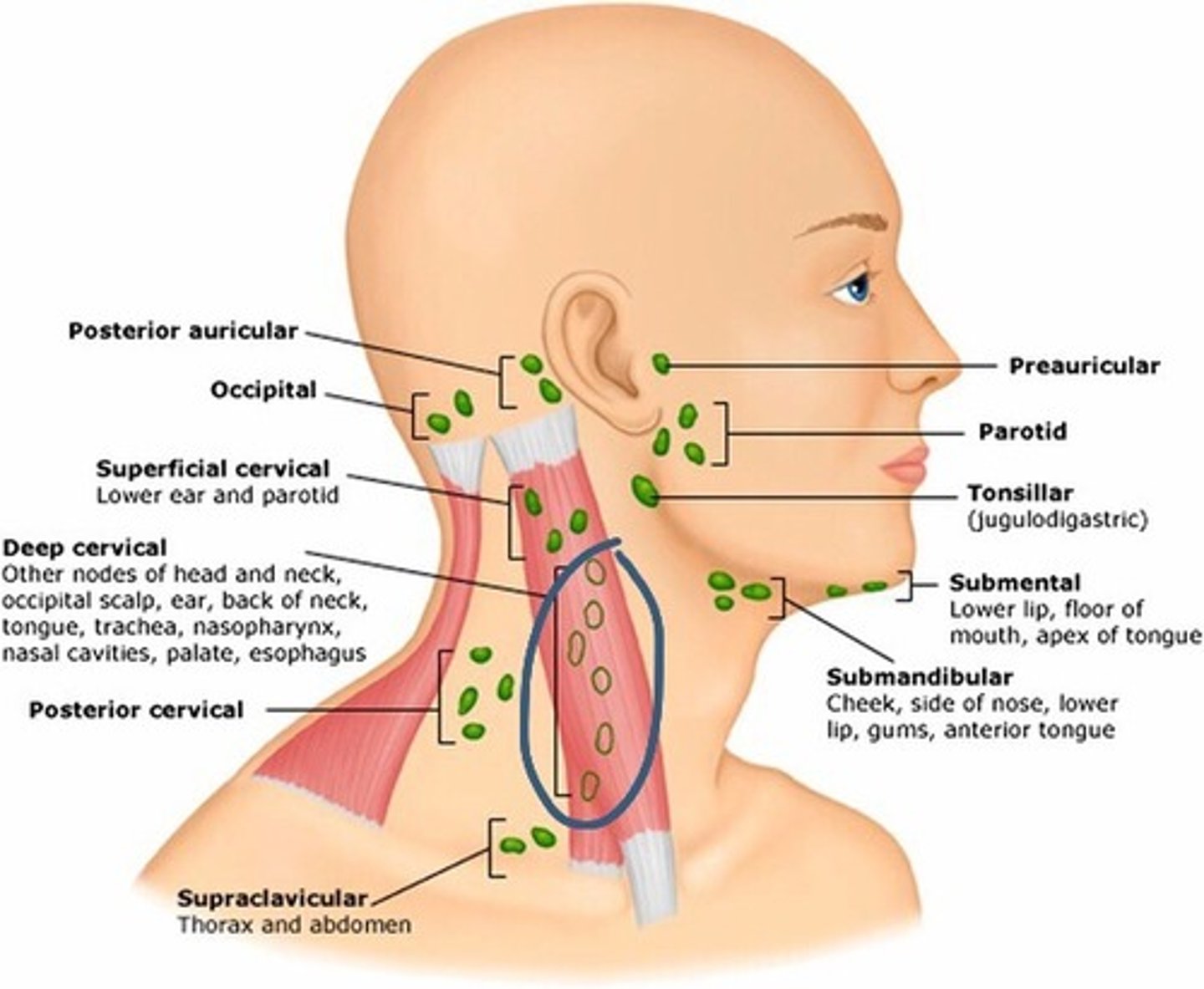
deep cervical chain lymph node
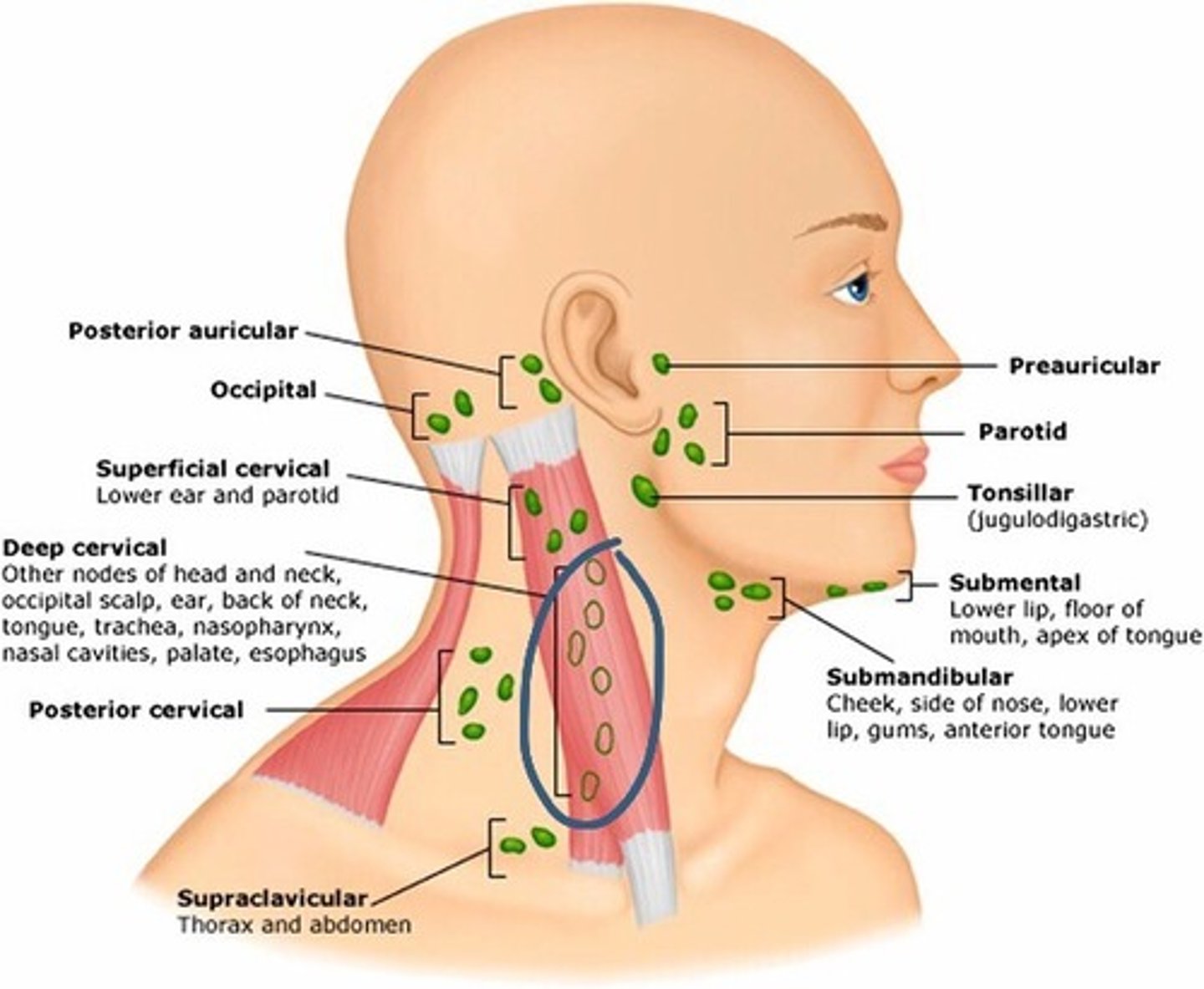
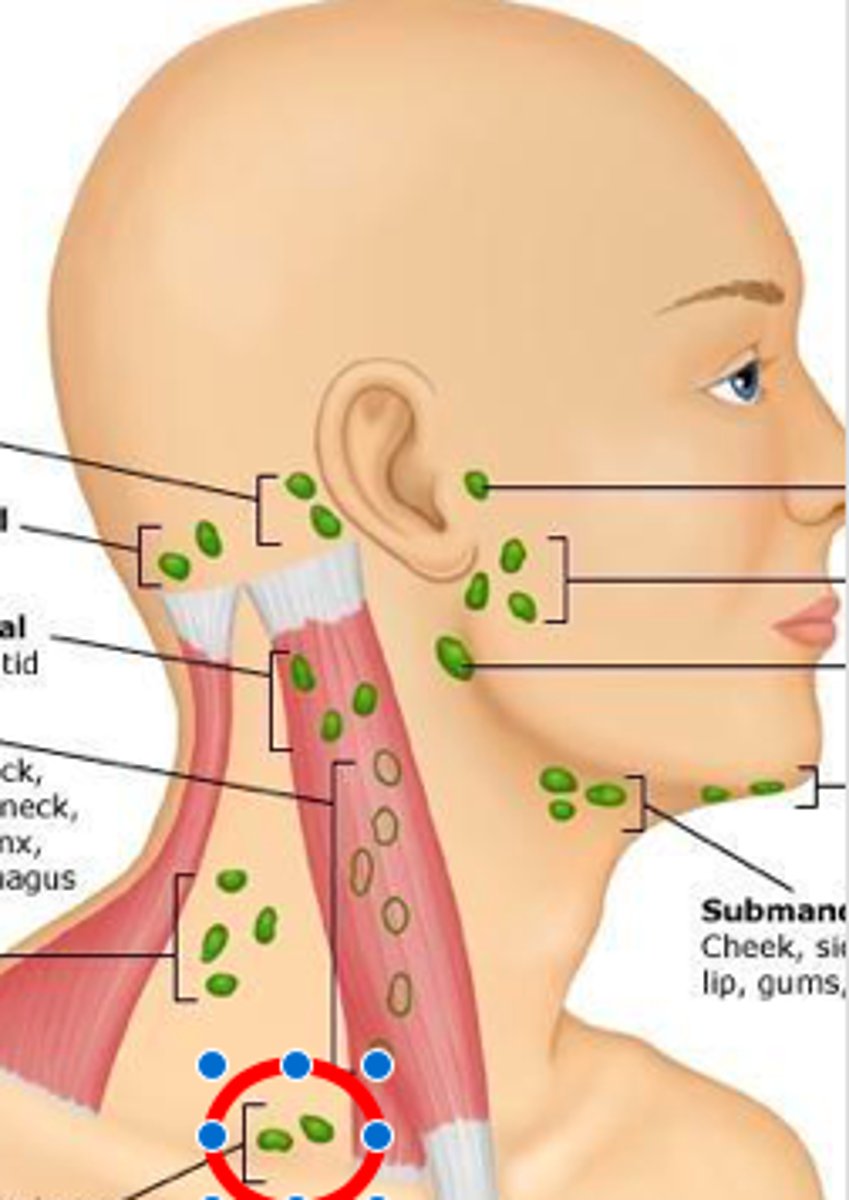
supraclavicular lymph node
deep in angle formed by clavicle and SCM
head ROS
hair loss/changes
h/o headaches
-frequency, location, associations
h/o head injury
neck ROS
masses
enlarged or tender glands
goiter
h/o thyroid disease
painful areas
neck stiffness
what to inspect for in hair
quantity
distribution
texture
patterns of hair loss
dandruff
what to inspect for on scalp
scaliness
masses
lesions
what to inspect for on skull
size
contour
deformities
depressions
masses
what to inspect for on face
facial expression
contours
symmetry
involuntary movements
masses
edema
examination for skin on face
color
texture
thickness
hair distribution
lesions
rashes
acne
how to palpate lymph nodes
-gently in circular motion w/ pads of index and middle fingers b/l
-pt should be relaxed w/ neck flexed forward
what to note about lymph node exam
size
shape
delimination (single or matted together)
mobility
consistency
tenderness
any overlaying skin changes
mobile vs. fixed lymph node
mobile = benign
fixed = malignant
virchow's node
enlargement of supraclavicular nodes
esp in L side - suggest metastasis from thoracic or abdominal cancer
tender lymph nodes
inflammation
hard/fixed lymph nodes
suspicious for malignancy
generalized lymphadenopathy
include infection, inflammation, or malignancy
HIV, IM, lymphoma, leukemia, sarcoidosis
inspect trachea for
deviation from midline
deviation = tension pneumothorax
palpate trachea for
tracheal deviation by placing one finger on side of trachea and note space between it and SCM
compare b/l spacing
auscultating trachea
stethescope diagram over trachea and note breath sounds
note stridor
stridor
high-pitched musical sound indicating respiratory emergency
how to inspect thyroid gland
tip head back and feel while they swallow
note contour, symmetry, and swelling of gland
how to palpate thyroid gland
-behind neck, position head forward
-place pads of both fingers below cricoid cartilage
-ask to swallow
-displace trachea and palpate lobes
note size, shape, and consistency
what to do if thyroid is enlarged
auscultate over lateral lobes for potential bruit (turbulent blood flow)
diffuse thyroid enlargement
indicated thyroid disease like graves, hashimotos, goiter
single nodule in thyroid
determine if benign or malignant
multinodular goiter
enlarged gland w/ multiple nodules
review of head and neck exam
-inspect hair
-inspect scalp
-inspect skull
-inspect face
-inspect skin of face
-palpate lymph nodes
-palpate trachea
-palpate and auscultate thyroid
battle sign
ecchymosis over the temporal bone, behind the ear
indicates head trauma and possible basilar skull fracture
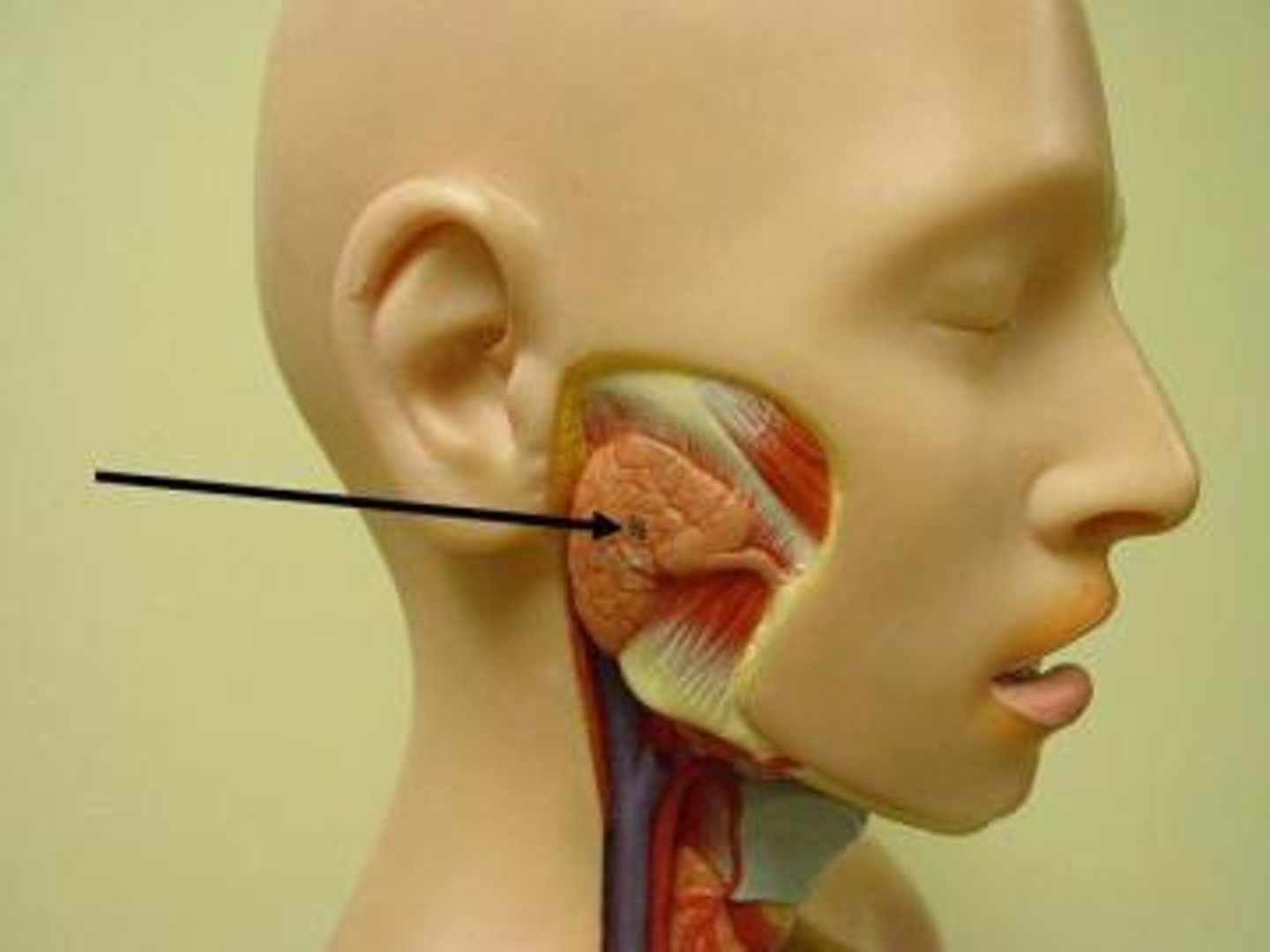
parotid gland
near the ear
contains stenson's ducts
auricle
outer ear
-helix, antihelix, lobule, tragus
helix
prominent curved outer ridge
antihelix
parallel and anterior to helix
lobule
ear lobe
tragus
nodular protrusion covering entrance of ear canal
ear canal
begins at external auditory meatus and extends to TM
function of middle ear
connect nasopharynx to Eustachian tube
-drains ear to help with pressure regulation
-sinuses and nose drain into the eustachian tube to cause ear pain
ossicles
malleus, incus, stapes
-hands of malleus and short process of malleus seen on TM
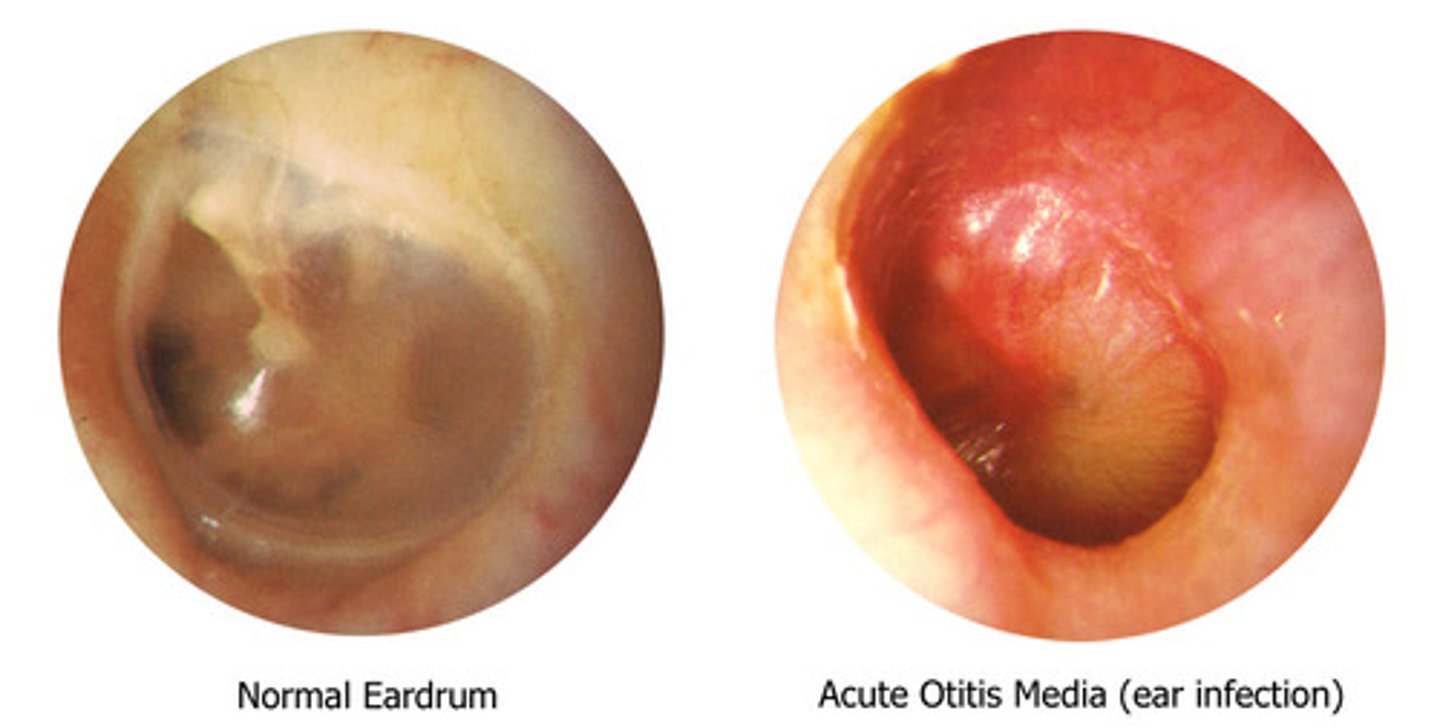
cone of light
light reflection fans down and anterior from umbo
-in OM, you can't see it
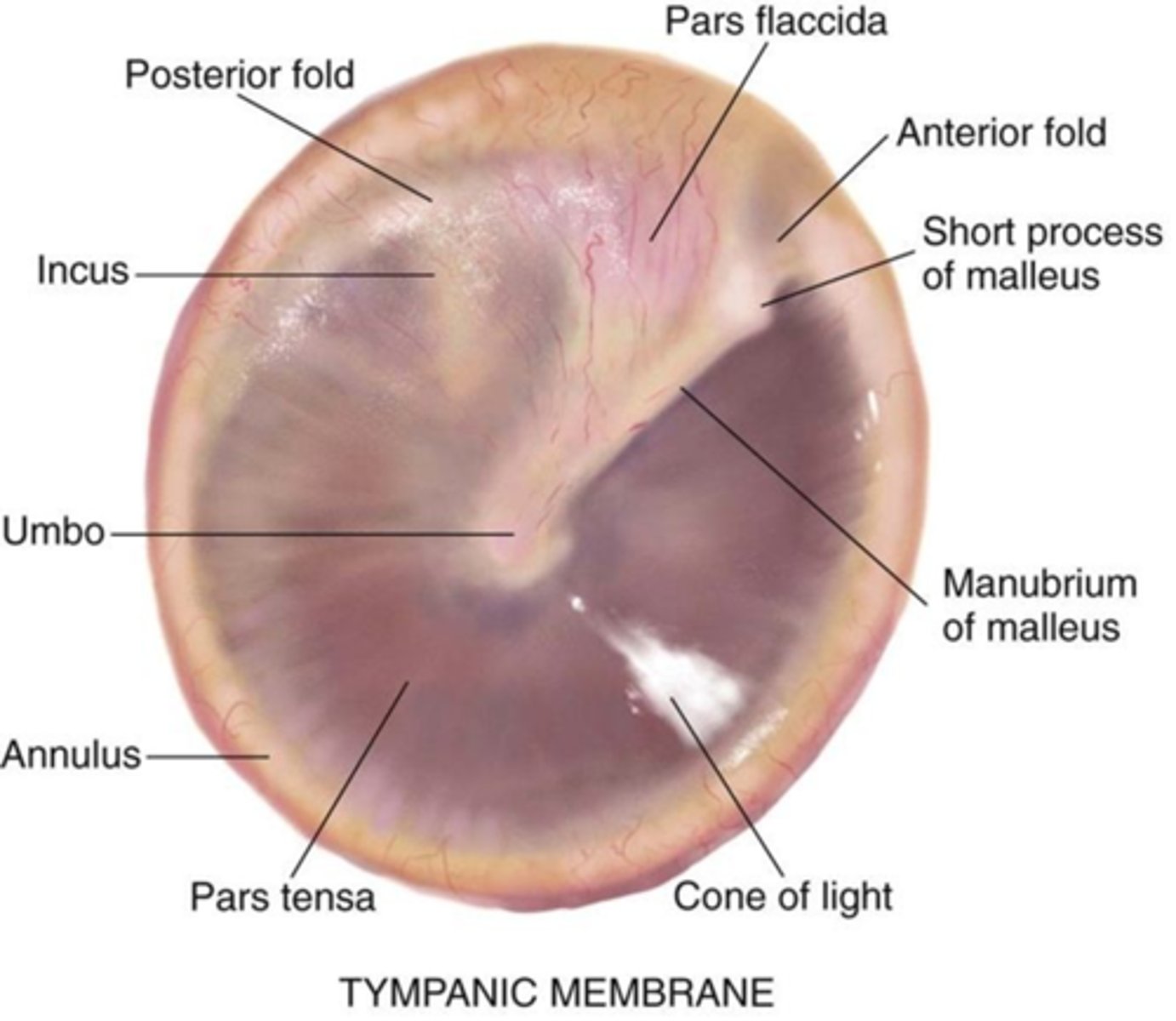
pars flaccida
part of eardrum above short process of malleus
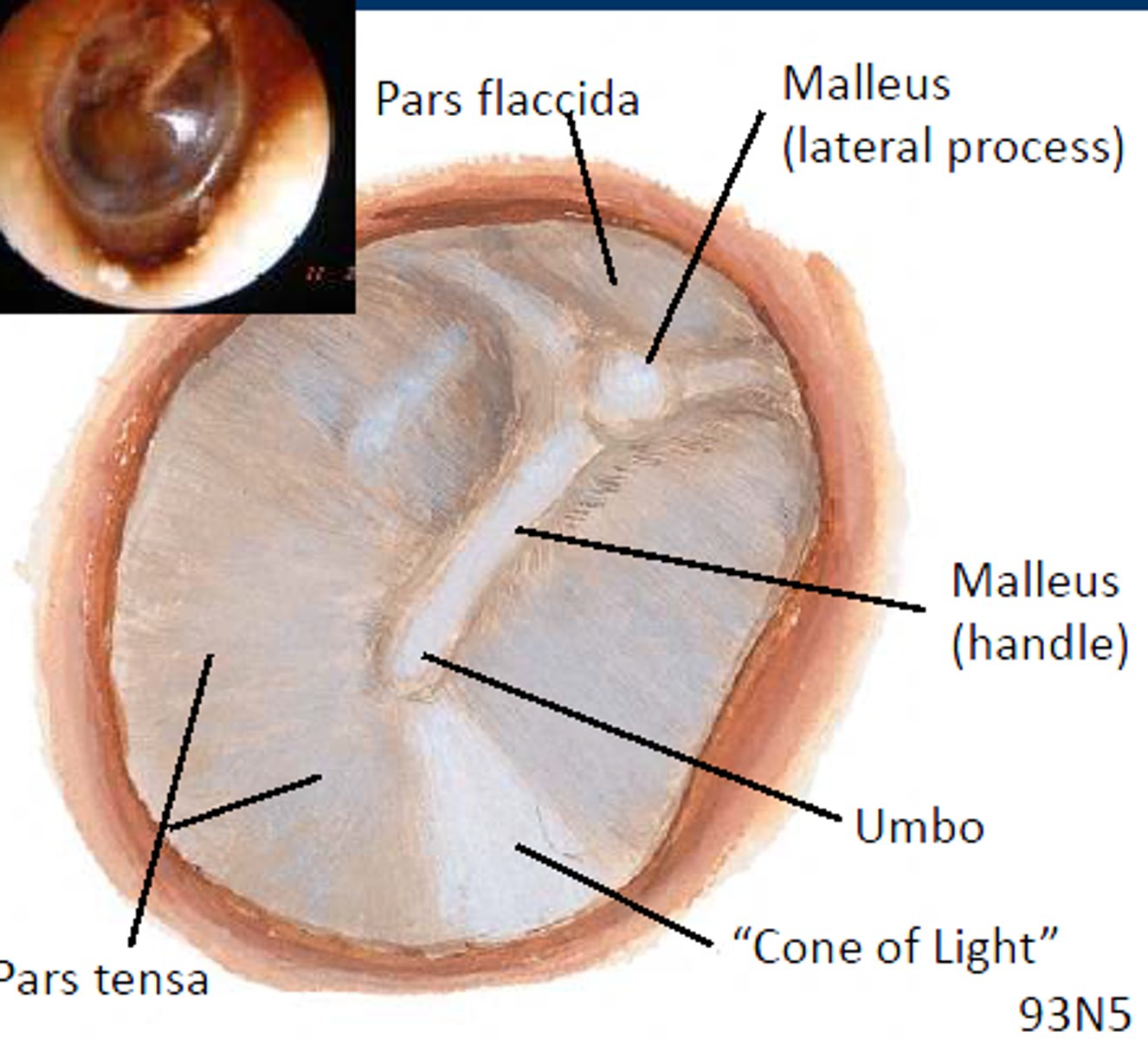
pars tensa
remainder of eardrum

labyrinth
inner ear
-cochlea
-semicircular canals
-vestibule
semicircular canals
rotational movement
vestibule
linear movement
vestibulocochlear nerve (CN VIII)
sends nerve impulses to brain to be interpreted
conductive phase
external to middle ear
-air conduction: normal hearing where sound travels through air to middle ear to cochlea
sensorineural phase
transmission from cochlea to CN VIII
-bone conduction: bypasses external and middle ear by sending vibration from skull to cochlea
conductive hearing loss
-conductive pathway impacted
-external or middle ear dysfunction
-impaction of ear due to cerumen or infection
sensorineural hearing loss
cochlear nerve damage
-little-to-no hearing in affected ear
turbinates
superior, middle, and inferior bony structures with highly vascularized mucous membranes
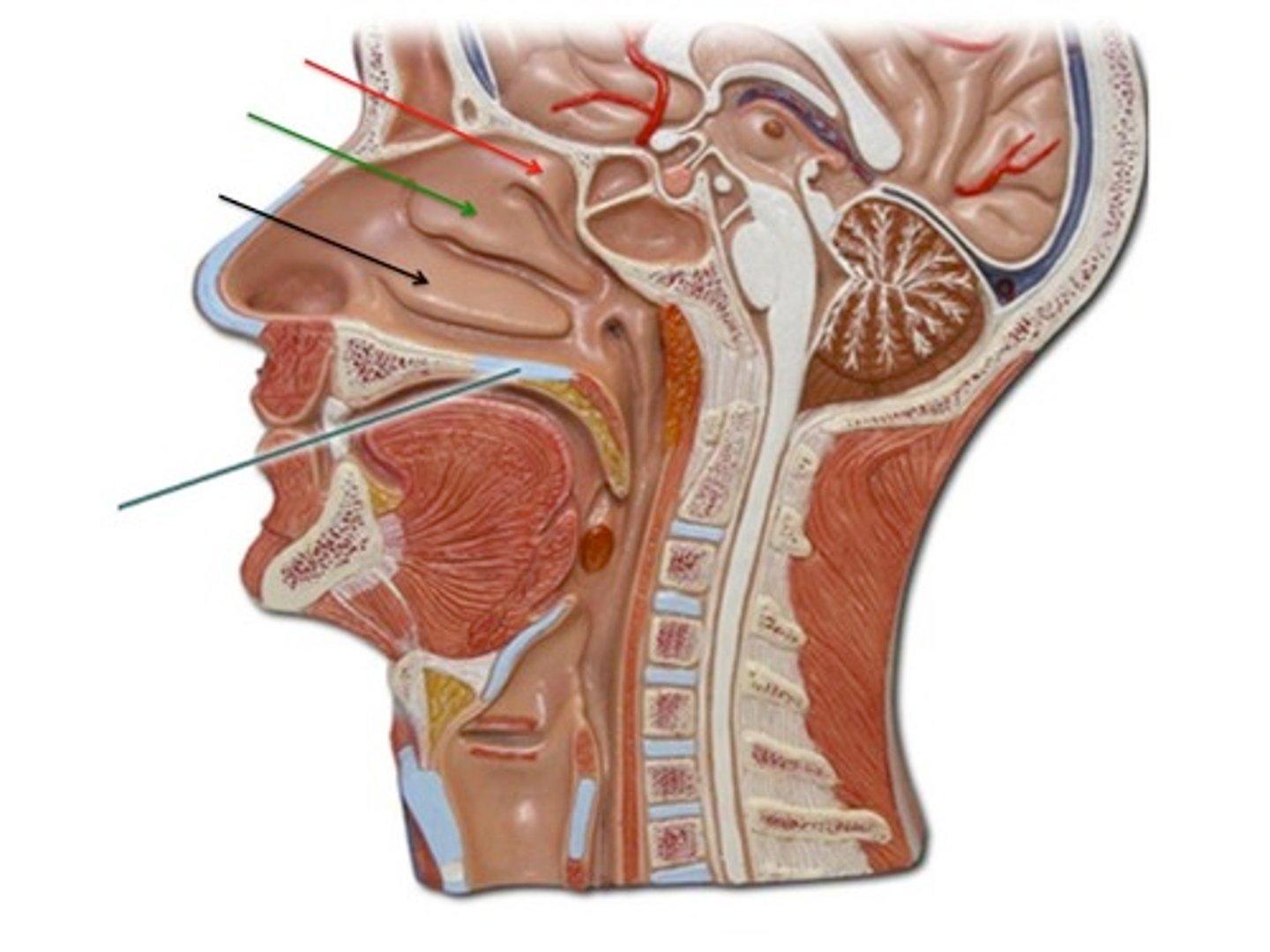
middle turbinate
drains paranasal sinuses
inferior turbinate
drains nasolacrimal duct
paranasal sinuses
maxillary, ethmoid, frontal, sphenoid
-only front and maxillary accessible on PE
-palpation can determine location of sinus infection
labial frenulum
connects lip to gingiva
ear ROS
hearing loss - sudden or gradual
hearing aid use?
ear pain
ear discharge
tinnitus
vertigo
presyncope
disequilibrium
meiniere's hx?
nose ROS
rhinorrhea
color
laterality and odor (bad smell in kids = obstruction)
pruritus
allergies/meds
nasal stiffness or congestion
associated symptoms: cough, fever, ear pain, dental pain, sore throat
epistaxis
sinus pain
h/o sinusitis
throat ROS
sore throat or tongue
bleeding of gums
last dental exam
dentures, endentulous, partials or implants
hoarsness/voice change (epiglottitis or peritonsilar abscess)
swelling of lips or throat
lesions of gums, lips, mucous membranes
dry mouth
key components of an ear exam
-inspect auricle and surrounding tissue
-palpate and move auricle, tragus, and mastoid
-inspect ear canals and TM w/ otoscope
-test auditory acuity and gross hearing (if hearing loss is present, test with tuning forks)
mastoid pain
mastoiditis
auricle pain
otitis externa (will also have ear discharge)
auricle exam
inspect for deformities, discharge, lumps, lesions
palpate tragus
move auricle up and down
palpate mastoid process
acute mastoiditis
painful mastoid process
redness, swelling, tenderness
"protrusion of the auricle"
otoscope technique
-straighten ear canal by pulling up, back, and away
-hold like pencil, brace fingers against face
-gently direct otoscope down and forward
-bilaterally
otitis externa
-swollen ear canal, moist and erythematous
-drainage known as otorrhea
ask if they've swam recently

ear exam of tympanic membrane
describe structures: handle of malleus, short process of malleus, pars flaccida, pars tensa
inspect for: color, contour, cone of light
tympanic mobility: assess w/ pneumatic otoscope
perforation of TM
tympanosclerosis
scarring of eardrum

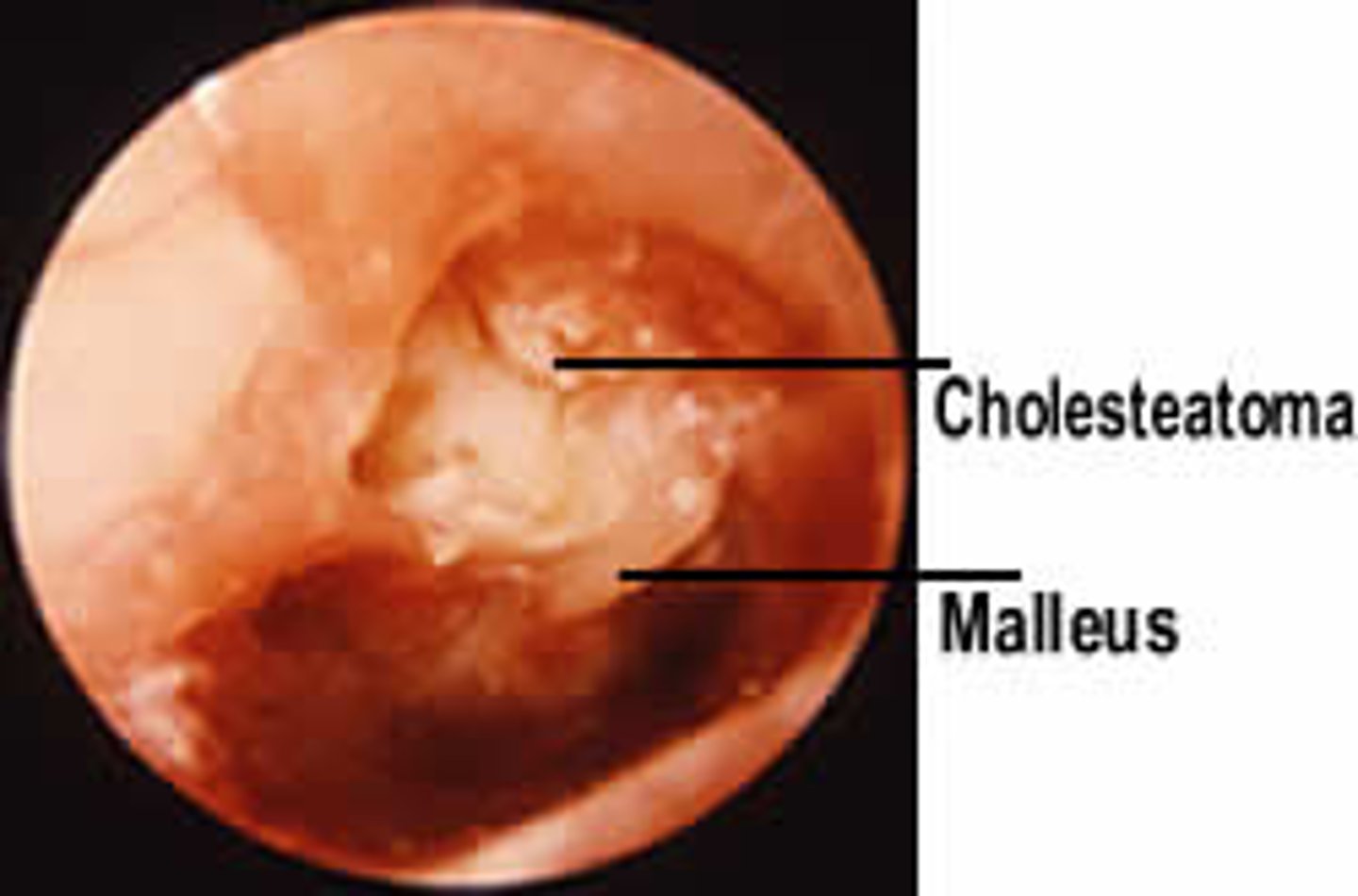
cholesteatoma
accumulation of skin cells in the middle ear that can destroy surrounding tissue
is a growth
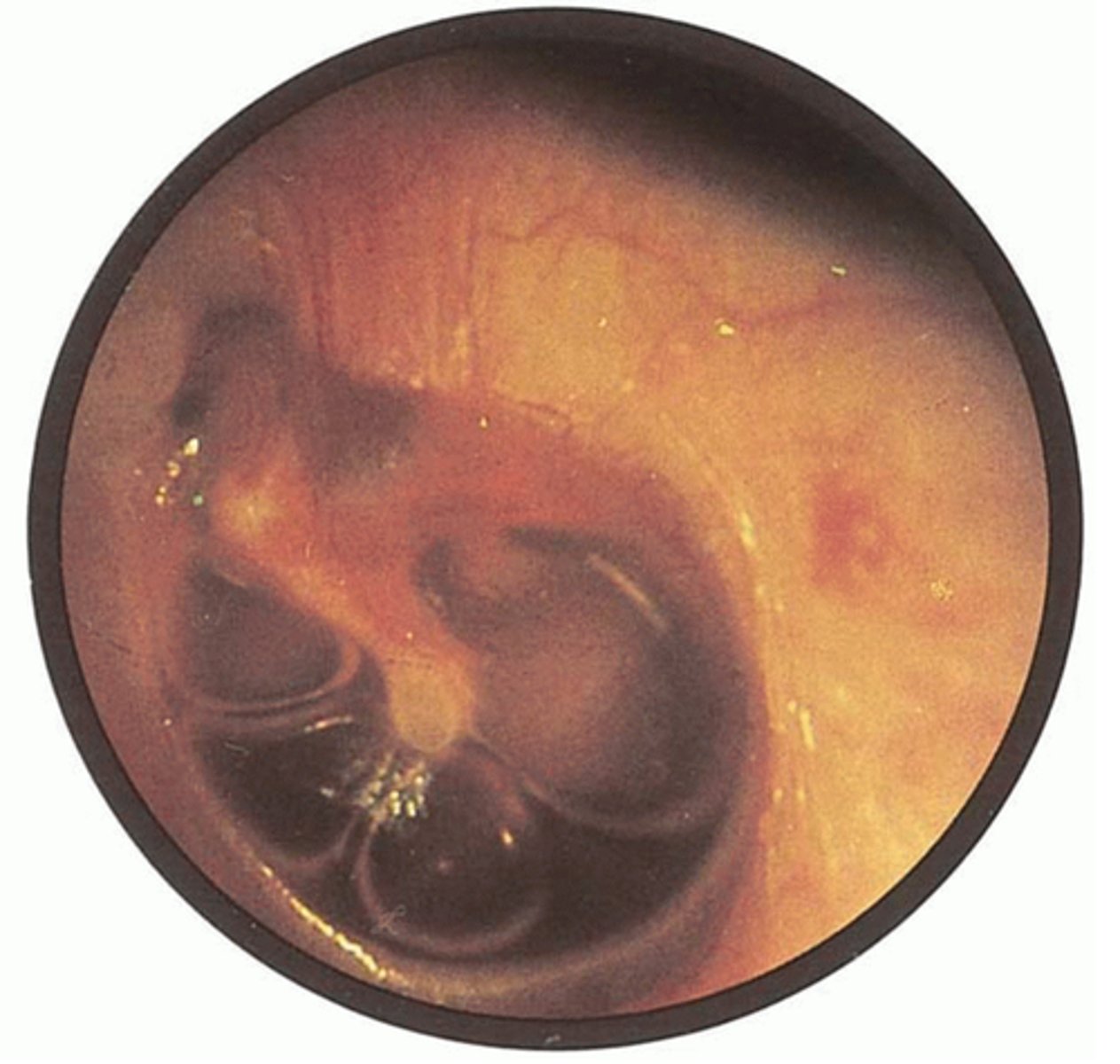
serous effusion
collection of amber serous fluid behind the TM
-associated with URI, can lead to acute OM
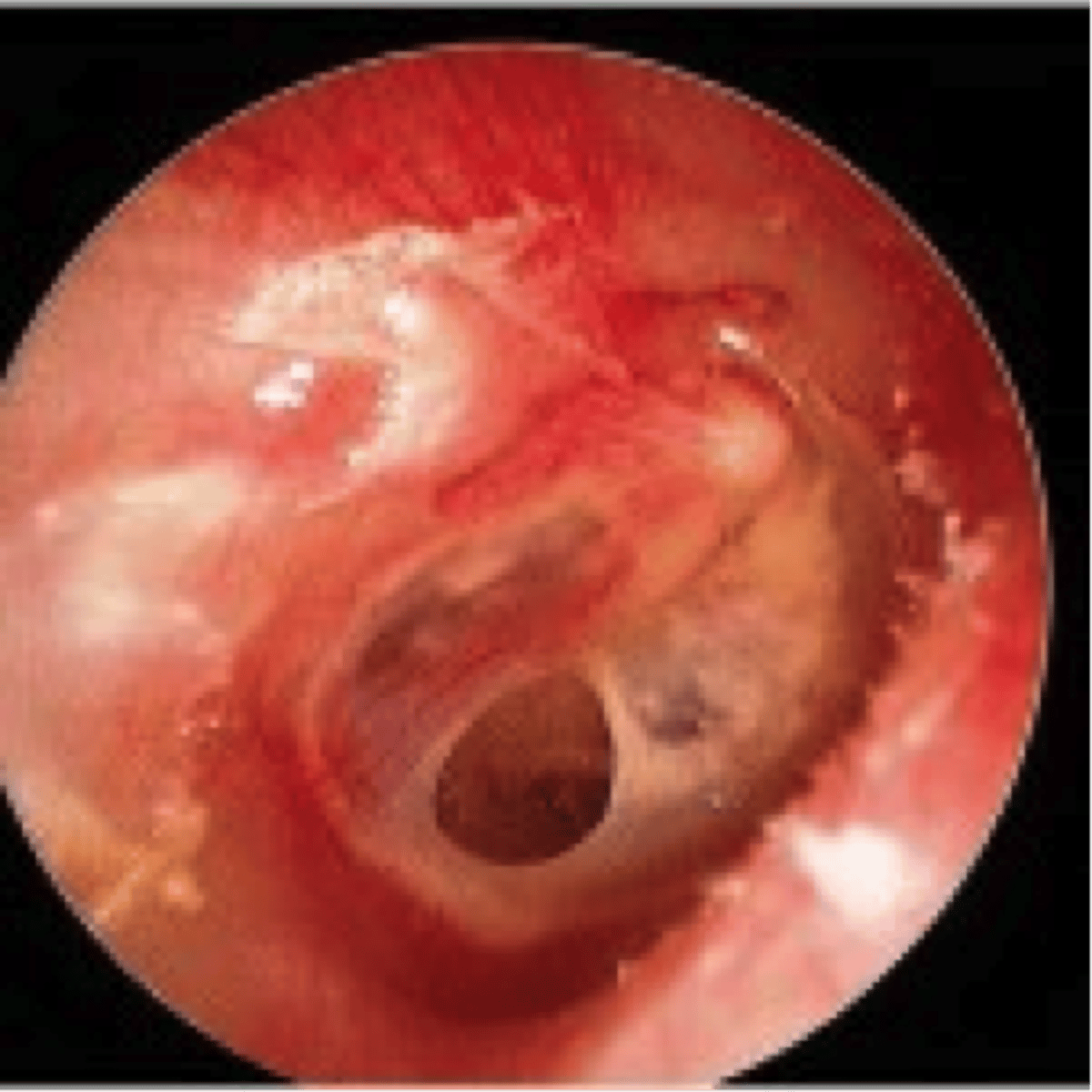
acute otitis media
AOM
bulging and erythematous TM

bullous myringitis
painful hemorrhagic vesicles on TM

whispered voice test
-inform pt you will state a sequence of numbers and letters
-stand 2 ft behind pt
-occlude and rub tragus of R ear
-whisper combination of 3 numbers/letters
-correct = normal hearing
-incorrect = repeat
-3/6 combinations correct = passed test
rinne test
-compared AC and BC
-vibrate tuning fork and put on mastoid bone
-when pt can't hear it anymore, take off and hold near external auditory canal
-AC should be > BC
Abnormal: AC=BC or AC
weber hearing test
-tests for lateralization
-vibrate fork, put on top of pt head
-ask where its heard best
normal = sound in both ears
abnormal = one or the other
weber test conductive hearing loss
sound goes to the bad ear
b/c it travels faster due to air block
weber test sensorineural hearing loss
sound goes to good ear b/c inside is messed up
nose exam
-inspect anterior surface
-test for obstruction
-inspect nasal mucosa, nasal septum, inferior and middle turbinates
-palpate frontal and maxillary sinuses
what can cause deviated nasal septum
hematoma
how to do nose exam
inspect for: asymmetry, deformity, obstruction
nasal obstruction test: occlude one ala nasi and have them breathe in, do b/l
inspection of nares
-place otoscope in nares, ask to tilt head back
-inspect mucosa for: color, edema, bleeding, exudate
-inspect septum for: deviation, inflammation, perforation, ulcers, polyps
mouth inspection
-inspect lips
-inspect and palpate oral mucosa
-inspect gingiva and gum margins
-inspect teeth
-inspect hard palate and floor of mouth
-inspect all surfaces of tongue
-inspect soft palate, anterior and posterior pillars, uvula, tonsils, pharynx
-note rise of soft palate