Parts of the Nephron E3
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
Identify
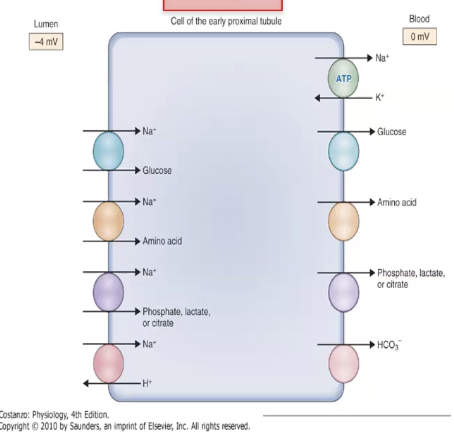
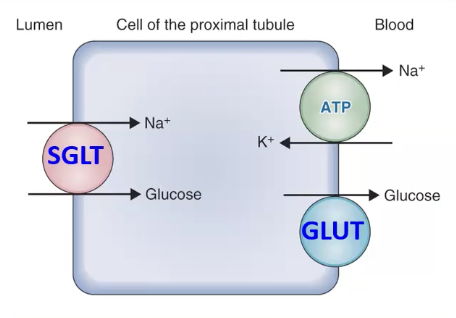
Early proximal tubule cell (PCT)
Key identifier: If you look and see a ton of secondary symporters in the apical membrane and the reabsorption of glucose and amino acids, you definitely have this cell type
Note: Na+, Cl-, and urea will cross paracellularly
There are no transport processes for urea in the PT
Identify.
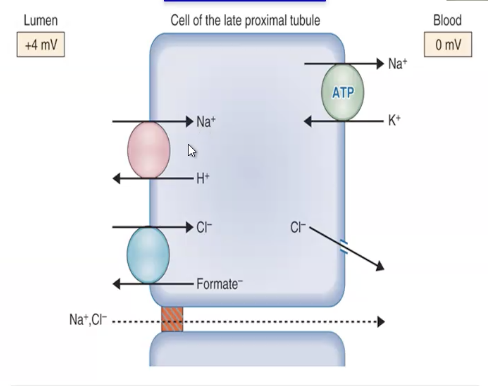
Late proximal tubule (PST)
Key identifier: Secondary active chloride transport. There are NO chloride transport proteins in the early proximal tubule. If you see formate. Chloride moves passively AND actively
Note: Na+, Cl-, and urea will cross paracellularly
There are no transport processes for urea in the PT
SGLT2 and GLUT2 transporters have low affinity and high capacity. T/F
TRUE
Remember —> in the early PT, glucose concentrations are really high! Affinity isn’t an issue, it is just responsible for rapid movement for reabsorption. Responsible for 90% of the filtered load of glucose by the mid-length of the proximal tubule
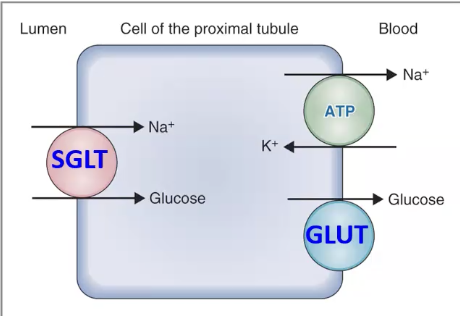
Where are SGLT2 and GLUT2 found?
Apical membrane of early proximal tubule
Basolateral membrane of early proximal tubule
Where are SGLT1 and GLUT1 found?
Apical membrane of late proximal tubule
Basolateral membrane of late proximal tubule
GLUT1 and SGLT1 are describe as high affinity, low capacity transporters. T/F
TRUE
This means they can’t move a lot of glucose, but they can pick up small amounts and move them across the membranes
How do SGLT2 inhibitors work?
They are used in the treatment of type II diabetes mellitus
Examples: Glifozins, Invokana
MOA: They selectively inhibit SGLT2 because it is a low affinity, high capacity transporter that’s responsible for reabsorbing majority of glucose. So if you inhibit that transporter, you end up not reabsorbing all of the glucose, and the glucose shows up in the urine. So, you end up excreting glucose and that helps lower glucose concentrations in the plasma
—> BUT this isn’t great because glucose in the urine is good incubator for bacteria. Yeast infections and UTIs are super common while on this medication
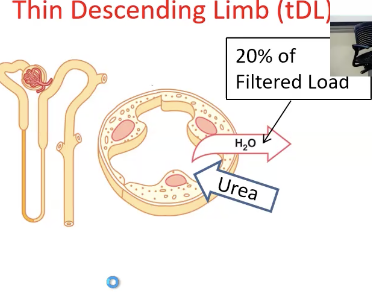
What is the thin descending limb responsible for?
Highly permeable to water, no solute permeability
Contains AQP-1 channels that play a major role in concentrating the urine
Reabsorption of water
Urea secreted here via facilitated diffusion
What is the tAL responsible for?
Impermeable to water
Does not reabsorb significant amounts of any solutes
Urea secreted here via facilitated diffusion
—> Does nearly nothing
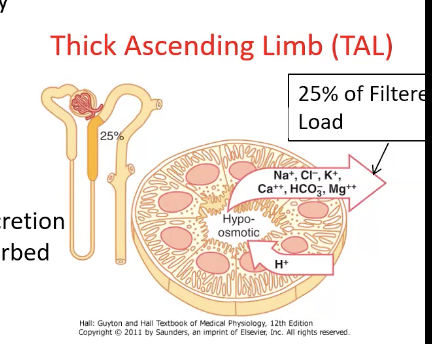
What is the TAL responsible for?
Impermeable to water AND urea
Permeable to solute —> major site of Na+/K+/Cl- reabsorption
Site of H+ secretion
By the end of the LOH, more solute is reabsorbed than water = filtrate hyposmotic
Distal end forms part of the JGA = has macula densa that mediates TGF response
Reabsorbs 25% of solutes!!
Identify.
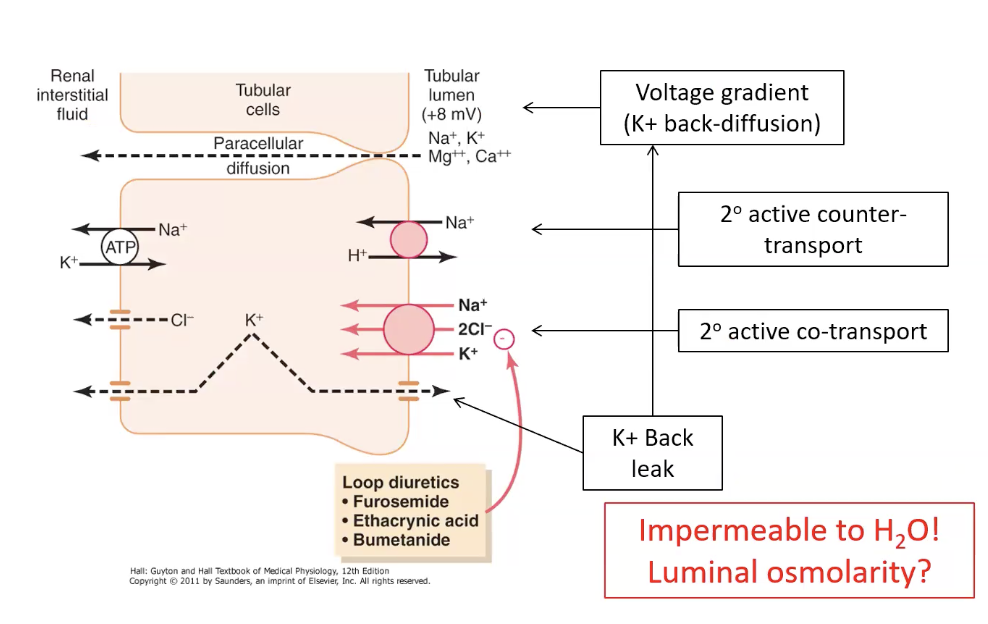
TAL cell
Key identifiers: The Na+/K+/2Cl- symporter on the apical membrane. This transport processes senses the sodium/chloride concentration in the filtrate. Secretion of H+ via transporter placed on the apical membrane
What influence does the K+ back leak have in the TAL?
Creates a +8mv and stimulates the movement of Na+, K+, Mg++, and Ca++ into the interstitial fluid through paracellular diffusion = too much positive charge accumulating!
Which segment of the nephron reabsorbs the most water?
Proximal tubule (70%)
—> most water is reabsorbed here!
What is the early distal tubule responsible for?
SAME AS TAL: permeable to solute, impermeable to water and urea
Called the “diluting segment” = reabsorbs another 5% of water making the filtrate even more hyposmotic
Identify.
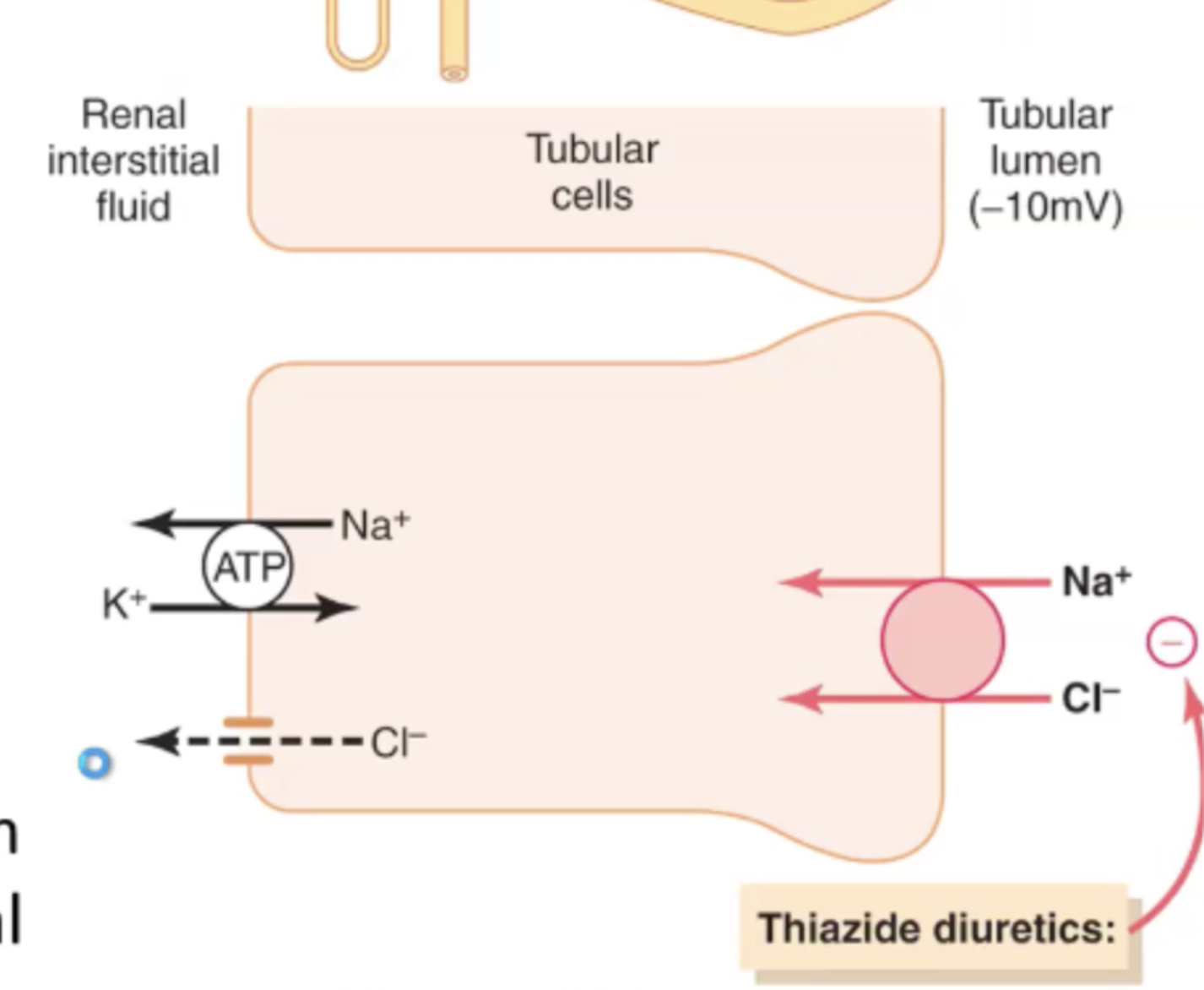
Early distal tubule
Key identifier: it’s ONLY job is to reabsorb Na+ and Cl-. Sodium/ Chloride secondary active symporter
What are the two different cell types found in the late distal tubule and cortical collecting duct?
Principal Cells
Intercalated Cells
Alpha
Beta
What are principal cells responsible for?
The site of ALDOSTERONE and ADH action!
Reabsorb Na+ and H2O
Secrete K+
Identify
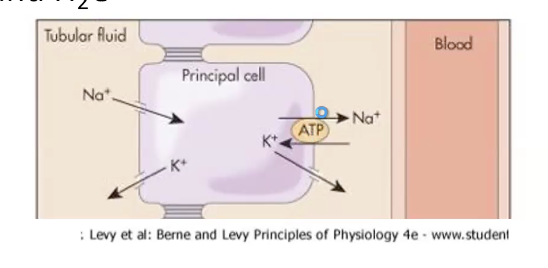
Principal Cell
Key Identifiers: The Na+/K+ ATPase is on the basolateral membrane that keeps the sodium concentration low and potassium gradient high inside the cell. This promotes the passive movement of Na+ into cell to be actively pumped out. K+ is secreted into the lumen. Processes are regulated by aldosterone
Is the late distal tubule/ cortical collecting duct permeable to urea?
No
What are alpha intercalated cells responsible for?
Function is important during ACIDOSIS
Secrete H+ into the lumen, reabsorb K+ and HCO3-
Excrete acid from the body via urine
SECRETING ACID, ABSORBING BASE
Identify.
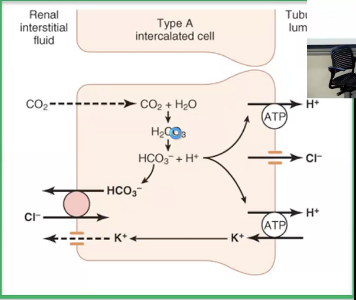
Alpha intercalated cells
Key identifier: Secreting acid H+, and reabsorbing base HCO3- and K+
What are beta intercalated cells responsible for?
Function important for alkalosis
Secrete K+ and HCO3-
Reabsorb H+
Opposite to alpha intercalated cells
Identify.
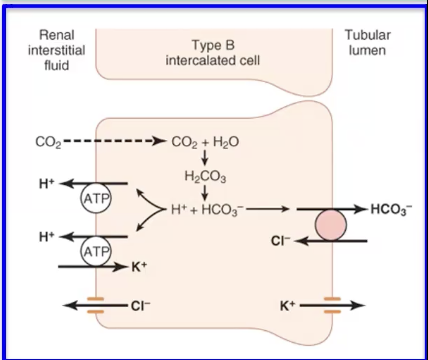
Beta intercalated cells
Key identifiers: Primary active H+ transporters in the basolateral membrane, and bicarb secreted on apical membrane. B cells secrete base.
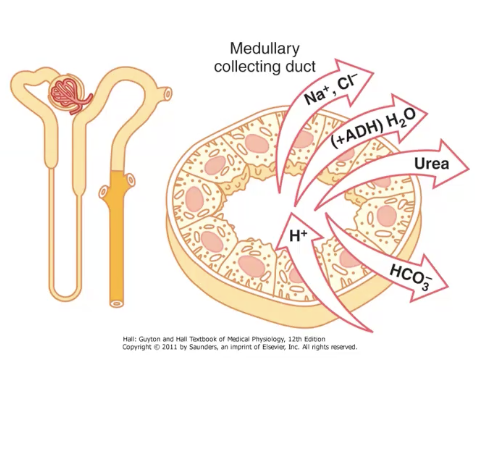
What is the medullary collecting duct responsbile for?
Contains principal cells and alpha intercalated cells
Processes less than 10% of Na+ and H20 but still very important
Site of Aldosterone and ADH action
Urea is REABSORBED via facilitated diffusion
Secretes H+ using the same mechanism as the alpha intercalated cells
Where balance is created