Psychological Interventions Lecture 4
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
Risk factors for eating disorders: Biological
Genetics and family history
Neurochemical imbalances
Starvation syndrome
Risk factors for eating disorders: Psychological
Anxiety
Perfectionism
Poor emotion regulation
Risk factors for eating disorders: Social
Pressure to be thin
Stressful life events
Ballet, rowing
Eating disorder intake
Demographics information
Help request
History
Eating disorder symptom screening
Risk assessment and differential diagnosis
ED symptoms present at intake
✓ Restriction of energy intake leading to low body weight
✓ Fear of gaining weight or becoming fat
✓ Disturbances in body image and/or preoccupation with body weight
✓ Eating large amounts in a short while feeling a loss of control (binges)
✓ Inappropriate compensatory behaviours (laxatives, vomiting, exercise)
X Avoidance of eating due to a lack of interest in food
X Avoidance of foods based on sensory characteristics (slimy, seedy)
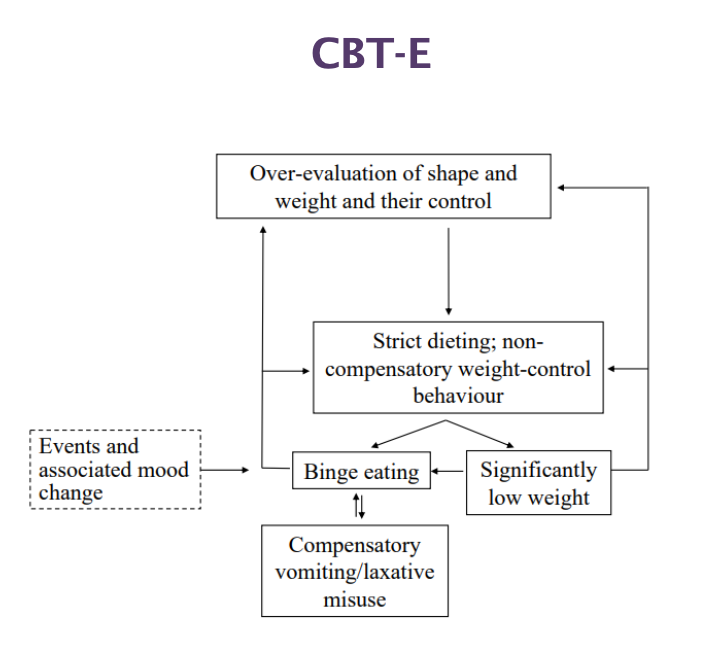
Transdiagnostic Model
Different eating disorders (e.g., anorexia, bulimia) share the same underlying processes
People can move between disorders over time
Core mechanism (cycle)
Overvaluation of weight/shape
→ Restricting food
→ Binge eating
→ Guilt/shame
→ Purging
→ Back to restriction (cycle repeats)
Symptoms are interconnected and maintain each other
Treatment targets the whole cycle, not just one behaviour
Treating an eating disorder: Choosing a focus
Stopping with binge-eating
Improving confidence in self/body
Weight re-gain
Eating more variety
Stopping laxative use
Stopping with excessive exercise
Treating OCD rituals
Somethingelse?
Evidence-based/recommended care
Cognitive behavioural therapy - enhanced
Maudsley Anorexia Nervosa Treatment for Adults (MANTRA)
Specialist Supportive Clinical MAnagement (SSCM)
Cognitive behavioural therapy - enhanced
Problem-focused on behaviour and psychopathology
Highly structured protocol with stages
Core idea: The main problem is: Overvaluing weight and shape
Goal: Break the cycle of eating disorder
Two types of CBT-E
“Focused” Version:
Exclusively addresses eating disorder psychopathology
“Broad” Version:
In addition addresses one or more “external” (to the core eating disorder) processes that may maintain eating disorder
E.g. clinical perfectionism, core low-self-esteem, or marked interpersonal problems
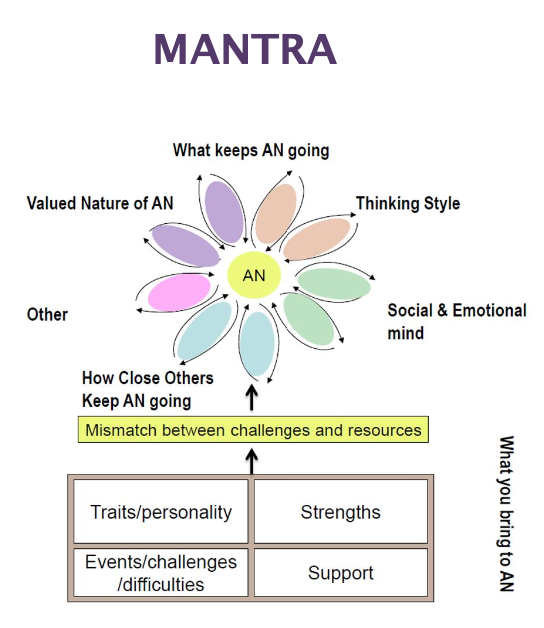
MANTRA
Cognitive and personality traits (rigidity, avoidance)
Semi-structured, workbook with tailored modules
Focus = broader personal and emotional factors
Anorexia continues because of:
Thinking style (e.g., perfectionism)
Emotional and social difficulties
Beliefs about anorexia (e.g., “it helps me cope”)
There is a mismatch between challenges and resources:
Challenges = stress, problems
Resources = support, coping skills
SSCM
Support and weight restoration
Less structured, patient led
Key pillars of treatment
Psychoeducation (risks of being malnourished, starvation syndrome)
Somatic + psychological support
Start & end well
Multidisciplinary
Consistency
Quality of life
Self-directed
Less-restrictive setting
Transparency
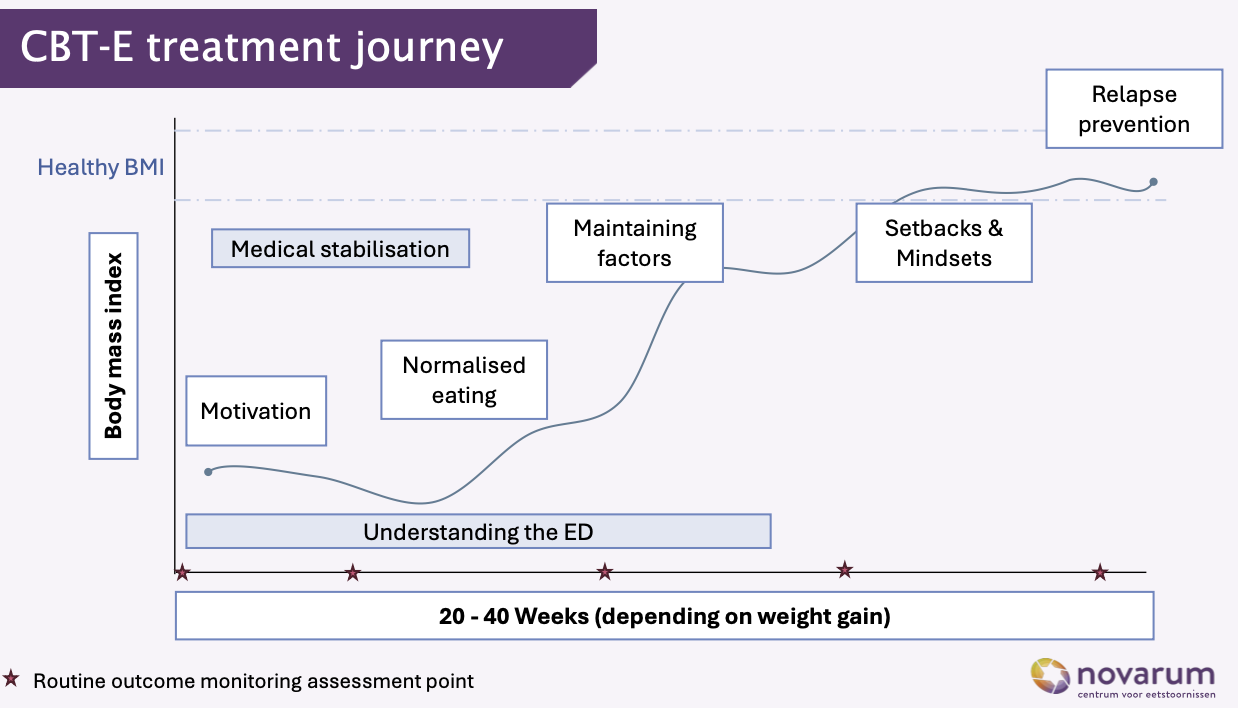
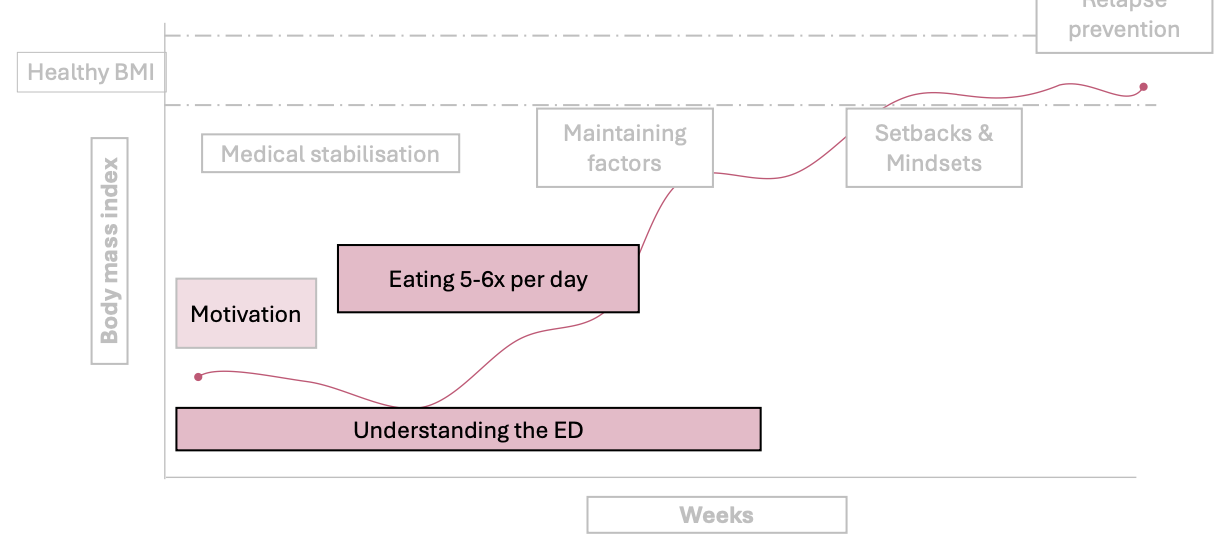
CBT-E treatment journey
Motivation + understanding the eating disorder (ED)
Medical stabilisation
Normalised eating
Address maintaining factors (thoughts & behaviours)
Setbacks & mindset work
Relapse prevention
20-40 weeks (depending on weight gain)
Weight/BMI and recovery improve gradually (not in a straight line)
Important features
Focus on understanding the ED throughout treatment
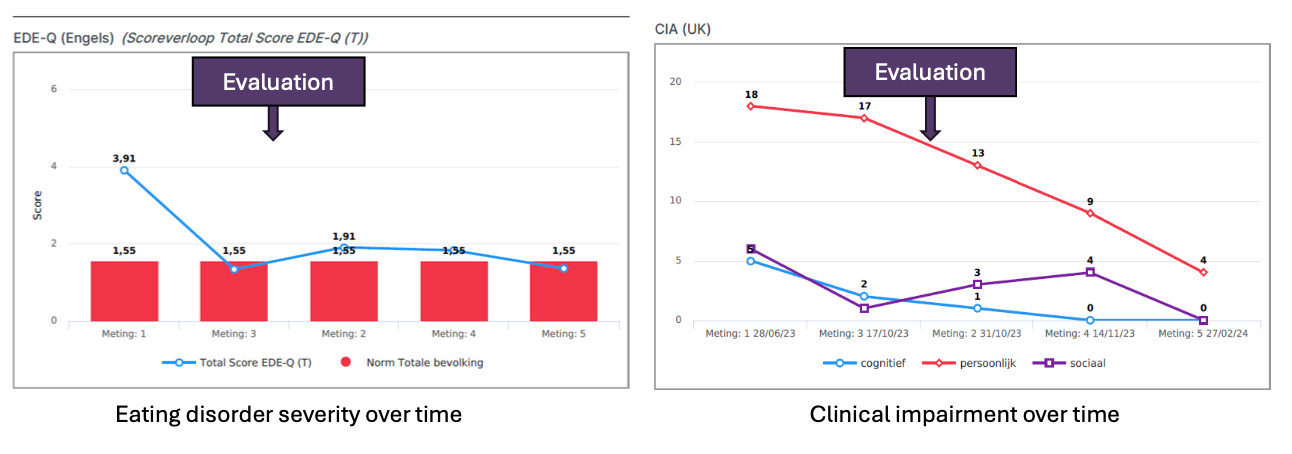
Regular monitoring of progress
Expect ups and downs
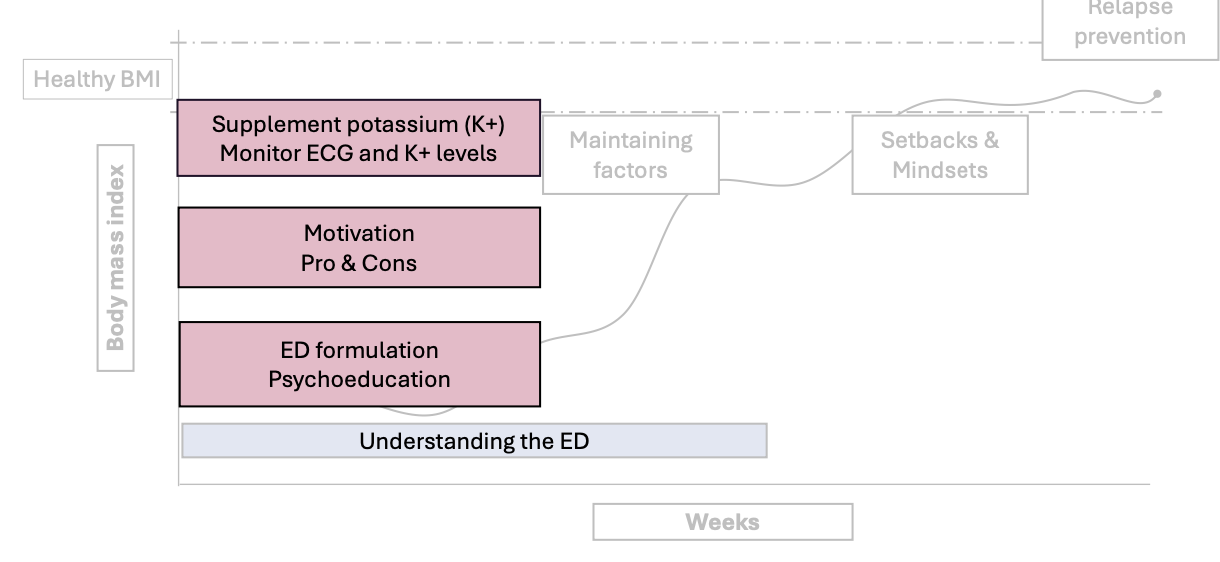
CBT-E Stage 0: Motivation
Very first stage of treatment, before real behaviour change starts: getting the person ready and safe to begin treatment
Physical safety first
Check health
Monitor heart (ECG) and potassium (K+)
Give supplements if needed
Build motivation
Talk about pros and cons of the eating disorder
Understand the eating disorder
Psychoeducation (learning about the disorder)
Create a personal explanation (formulation) of what keeps the problem going
Other potential barriers should be explored
Cost/benefit of an ED
Pro
Feeling of control
Sense of accomplishment
Temporarily lowers anxiety
Affirmation from some people
Predictable future
Con
Out of control binges
Always thinking about food
Less focus in class
Tired
Hair loss and weak nails
Isolated from friends
Cost/benefit of recovery
Pro
Better focus
More spontaneous and social
Hair re-growth
Not thinking about food all the time
More confident
Con
Facing fear of weight gain
Loss of tight control
Letting go of ED identity
Fear of judgment
Fear that noting will change mentally
CBT-E Stage 1: Starting well
Keep motivation
Understanding the ED
Eating 5-6x per day
What factors should be included in the progress review
Frequency of ED symptoms
Regularity of meals
Medical stability
Changes in clinical impairment
Changes in overall functioning
Readiness for change
CBT-E Stage 2: Taking stock
Review progress
Eating diaries
Symptom severity
Frequency of laxative use
Impairment and functioning
Medical stability
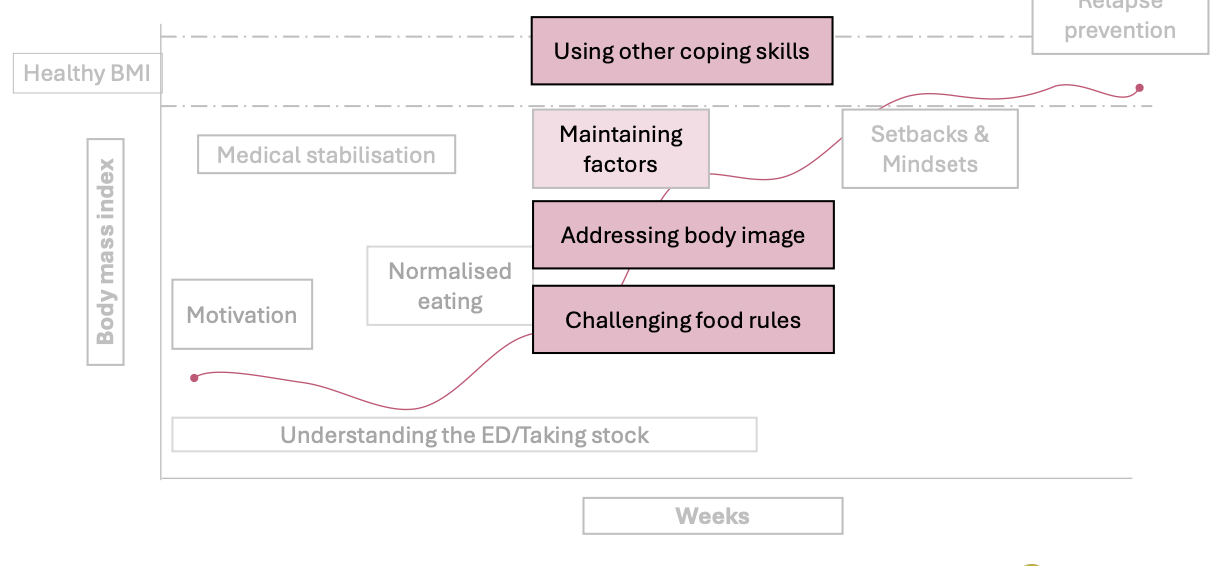
CBT-E stage 3: Maintaining mechanisms
Learn better coping skills
Handle difficult feelings (e.g., stress, sadness, loneliness)
Instead of using eating behaviours to cope
Break strict food rules
Challenge beliefs like:
“If I eat this, I will lose control”
Start eating feared foods in a flexible way
Work on body image
Reduce:
comparing yourself to others
checking your body all the time
Use exposure (e.g., looking in the mirror without judgment)
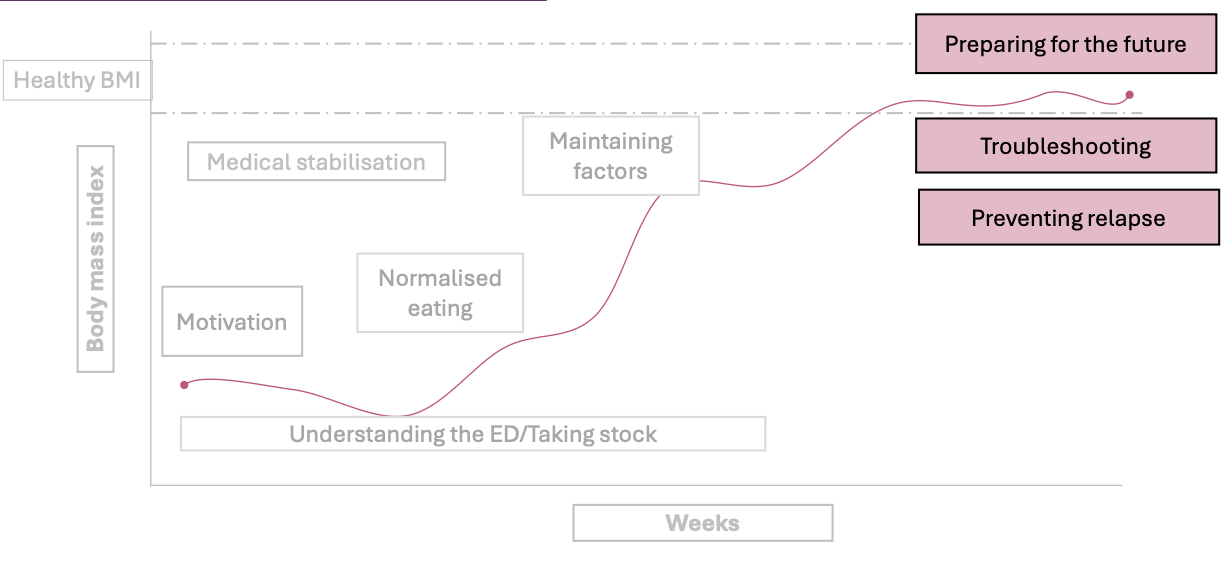
CBT-E Stage 4: Ending well
Preparing for the future: Create personalised plan for the future
Further work on body checking, food avoidance, and practice problem solving
Continue develop new interests and activities
Troubleshooting
Preventing relapse: Patient needs to have realistic expectations for the future
CBT-E throughout
Keeping and reviewing eating diary
Monitoring weight weekly with therapist
Ethical dilemmas in eating disorder treatment
Eating disorders can directly affects a patient’s ability to recognize the need for treatment
Does the patient have adequate decision-making capacity?
How immediate and severe are the risks?
Is there a less coercive option?
Forced treatment saves lives, but it can also be traumatic and damage trust
Areas of treatment innovation
E-health
Guided self-help
Integrated care
PTSD + anorexia treatment
Brain stimulation
Deep brain stimulation
rTMS
Psychedelics
Ketamine
MDMA
Online Guided Self-Help for Binge-Eating Disorder
Most common eating disorder (3–4%)
Often underdiagnosed and undertreated
Study Design
N = 187 patients
Compared:
Online guided self-help (12 weeks)
CBT-E (20 weeks, therapist-led)
Results: Both treatments reduced binge eating significantly
No difference in:
Treatment effectiveness
Therapeutic alliance
Dropout rates
Advantages of E-health
Shorter (12 vs 20 weeks)
Cheaper
More accessible
Combine treatment for anorexia nervosa and PTSD
~23% AN patients have PTSD
~55% have childhood trauma
PTSD can worsen and maintain the eating disorder
Problem with usual care
Treat AN first, trauma later
→ PTSD remains → risk of relapse
New approach
Treat AN + PTSD at the same time
Inpatient AN treatment + trauma therapy
Findings
Feasible: 7/10 completed
Safe but challenging: ↑ anxiety, sleep issues, some self-harm
Acceptability: patient report benefit, healthcare workers emphasise the need, engagement and focus across sessions was high
Neuromodulation
= Changing brain activity to help treat eating disorders
Non-invasive (rTMS / iTBS)
Magnetic stimulation (no surgery)
Targets self-control & emotion areas
Effects:
↑ eating in anorexia
↓ impulsivity in bulimia/BED
Safe and well tolerated
Invasive (DBS)
Brain surgery (electrodes)
For severe, treatment-resistant cases
Findings
rTMS/iTBS: promising and safe
DBS:
Small studies
Some side effects
Improvements in BMI, mood, anxiety
Psychedelics and their effects in therapy
Psilocybin
Cognitive flexibility
Anorexia and binge-eating disorder (Sweden Lund University)Binge-
eating disorder (University of Florida)
Long-standing anorexia nervosa (UCSF)
MDMA
Shame and fear
ED + PTSD: where trauma may be an underlying factor
Ketamine
Rapid effect on mood
Anorexia + MDD (EDEN Study at King’s College)
Ayahuasca / DMT
Neuroplasticity, interoception and emotional processing
Mostly speculative and self-report
Psychedelic-assisted therapy: MDMA
Randomised controlled trial
N = 90 with PTSD & ED symptoms (no purging)
n = 15 with BED or OSFED
n = 13 with history of anorexia or bulimia
80-180mg MDMA + psychological support
Findings
Dropout n = 7
Reduction in disordered eatingat titudes
No change in BMI within or between groups
More to explore
Brief and online treatments
Guided self-help for other eating disorders
Treatments for severe overweight and obesity
Neuromodulation
Medications and off-label prescribing