Peds/OB 4.3: GU/Renal
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
In general, what is hypospadias? What is this condition a contraindication to?
Urethral opening on the ventral surface of the penis; circumcision is contraindicated

What is cryptorchidism, & how long may it be considered "normal?"
Undescended testis; ~4-6 months (after this point they should be fully descended tho)

How is cryptorchidism diagnosed, & what is the preferred treatment? Why is it important we treat this?
Pelvic US to confirm location, surgery (orchidopexy) at 9-18 months of age; untreated cryptorchidism can ↑ risk of malignancy, infertility, inguinal hernia, & torsion
In general, what is hydrocele & how is it diagnosed? Does it usually require treatment?
Fluid accumulation within the remnant tunica vaginalis that appears as a soft tender swelling of the scrotum that transilluminates; US; no - usually resolves by 1 y/o

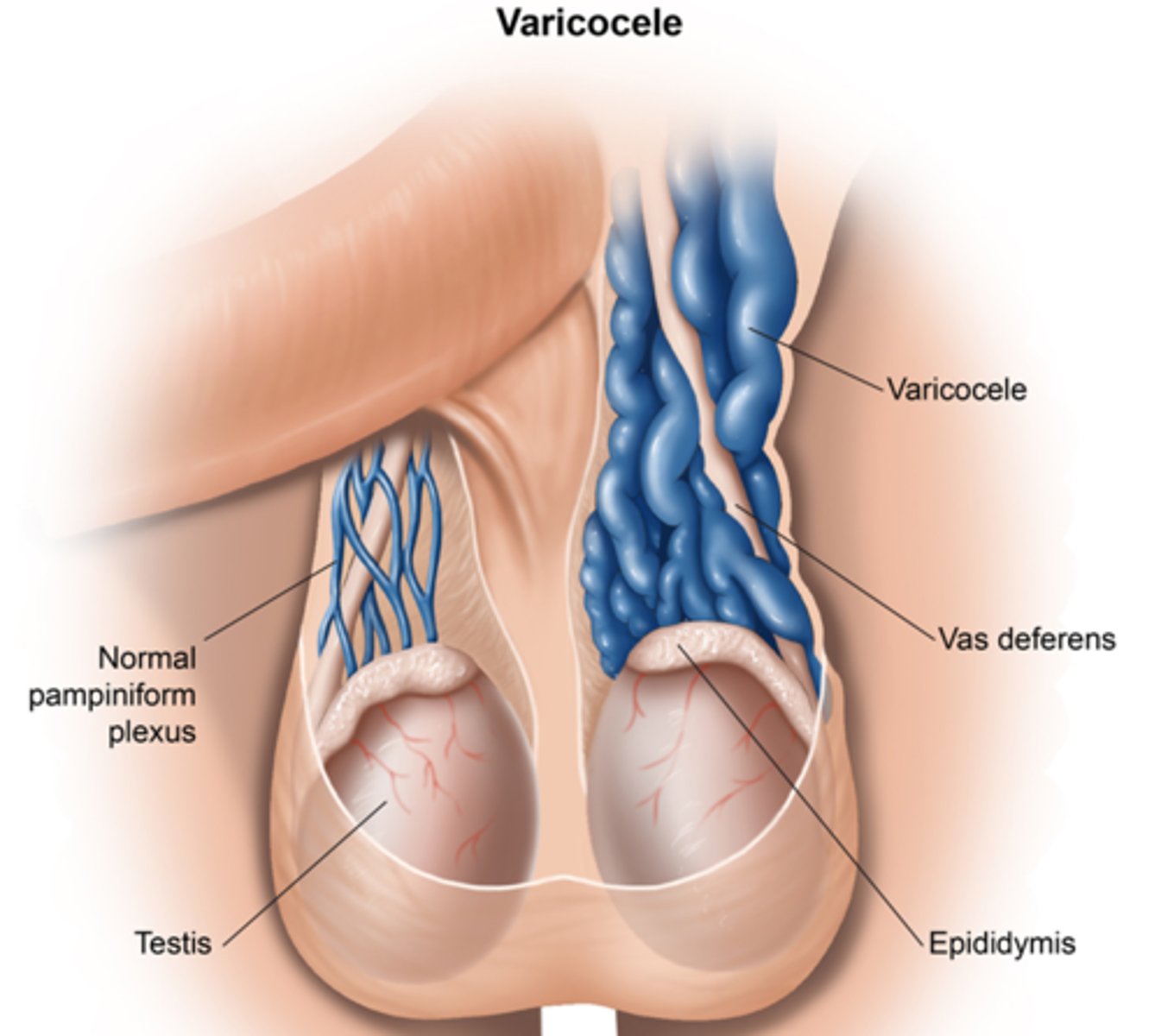
If a patient has a left-sided varicocele, what must we do? Why?
Order a renal ultrasound - Britt has seen renal cell carcinoma missed because people did not do this!!!
What is testicular torsion, & is it serious?
Testis twists on itself leading to decreased blood supply; YES - is a surgical emergency (only have ~4 hours to fix this or the person may lose the testicle)
What are some s/sxs of testicular torsion?
Acute scrotal pain, swelling, edema, erythema, absent cremaster reflex, "blue-dot" sign

How is testicular torsion diagnosed & treated?
Diagnosis: US
Treatment: manual detorsion & surgery (orchiopexy - prevents recurrence)

In general, what is enuresis?
Urinary incontinence beyond the age when the child is developmentally-capable of continence (typically ~5 y/o)
What is the difference between nocturnal & diurnal, primary vs. secondary, & monosymptomatic vs. non-monosymptomatic enuresis?
Nocturnal = during sleep, diurnal = during the day
Primary = never been consistently dry, secondary = at least 6 months of prior consecutive dryness)
Mono = uncomplicated nocturnal (no underlying disorder), non-mono = both nocturnal & daytime incontinence (indicative of an underlying disorder)
When is enuresis considered to be abnormal?
If it occurs in children > 12 y/o or is non-monosymptomatic (if it's in kids < 12 & monosymptomatic tho, it is considered totally normal & doesn't require any intervention)
How is enuresis managed (if it requires treatment)?
Education, conditioning alarms, DDAVP, TCAs (both good med options)
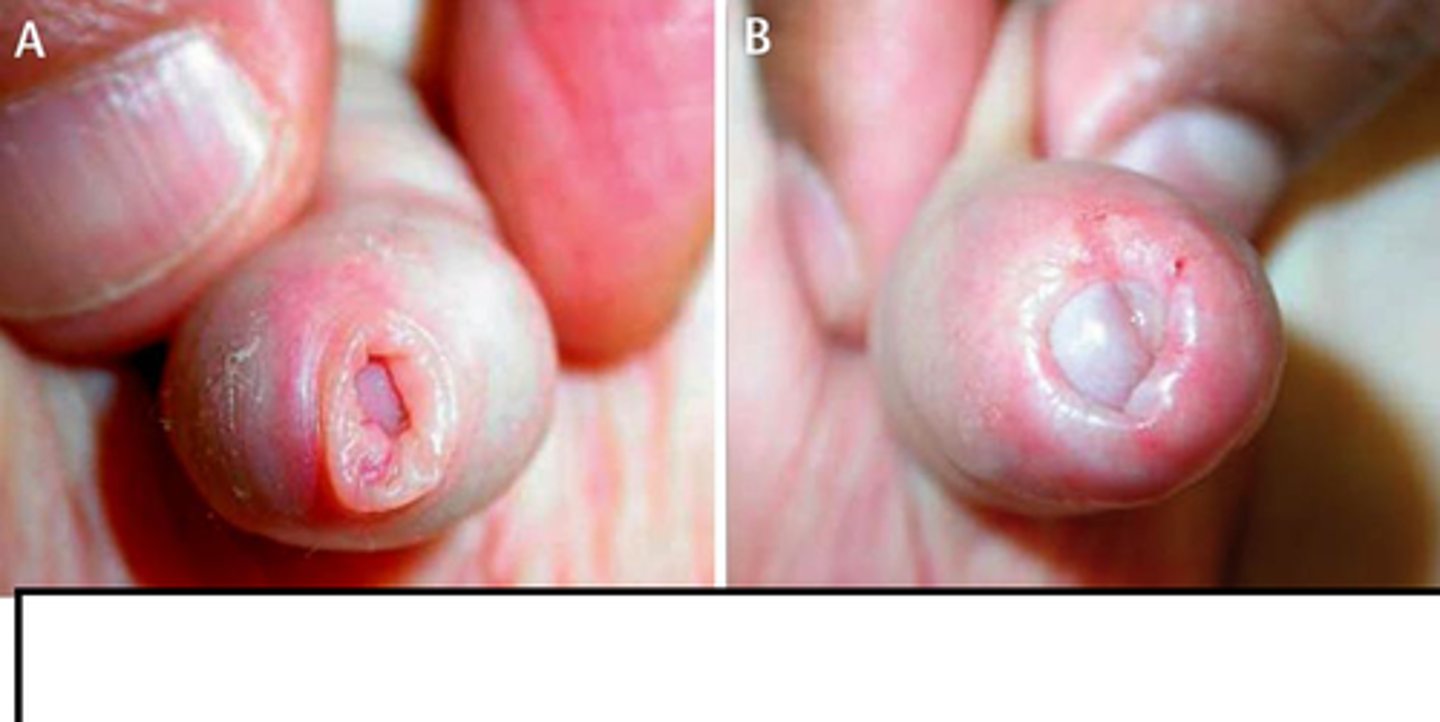
What is phimosis, & what is the most common cause?
Fibrous constriction of the foreskin that prevents its retraction; poor hygiene
How is phimosis managed?
Topical corticosteroids + educate on good hygiene, NSAIDs, APAP, gentle manual retraction, circumcision if all else fails
What is paraphimosis? Is this serious?
Foreskin is unable to be retracted into its natural position; yes - is a urological emergency

How is paraphimosis managed depending on if its complicated (ischemia and/or necrosis of the glans) vs uncomplicated?
Complicated: emergent surgery
Uncomplicated: attempt manual compression of ring & glans under anesthesia to reduce swelling, circumcision last resort
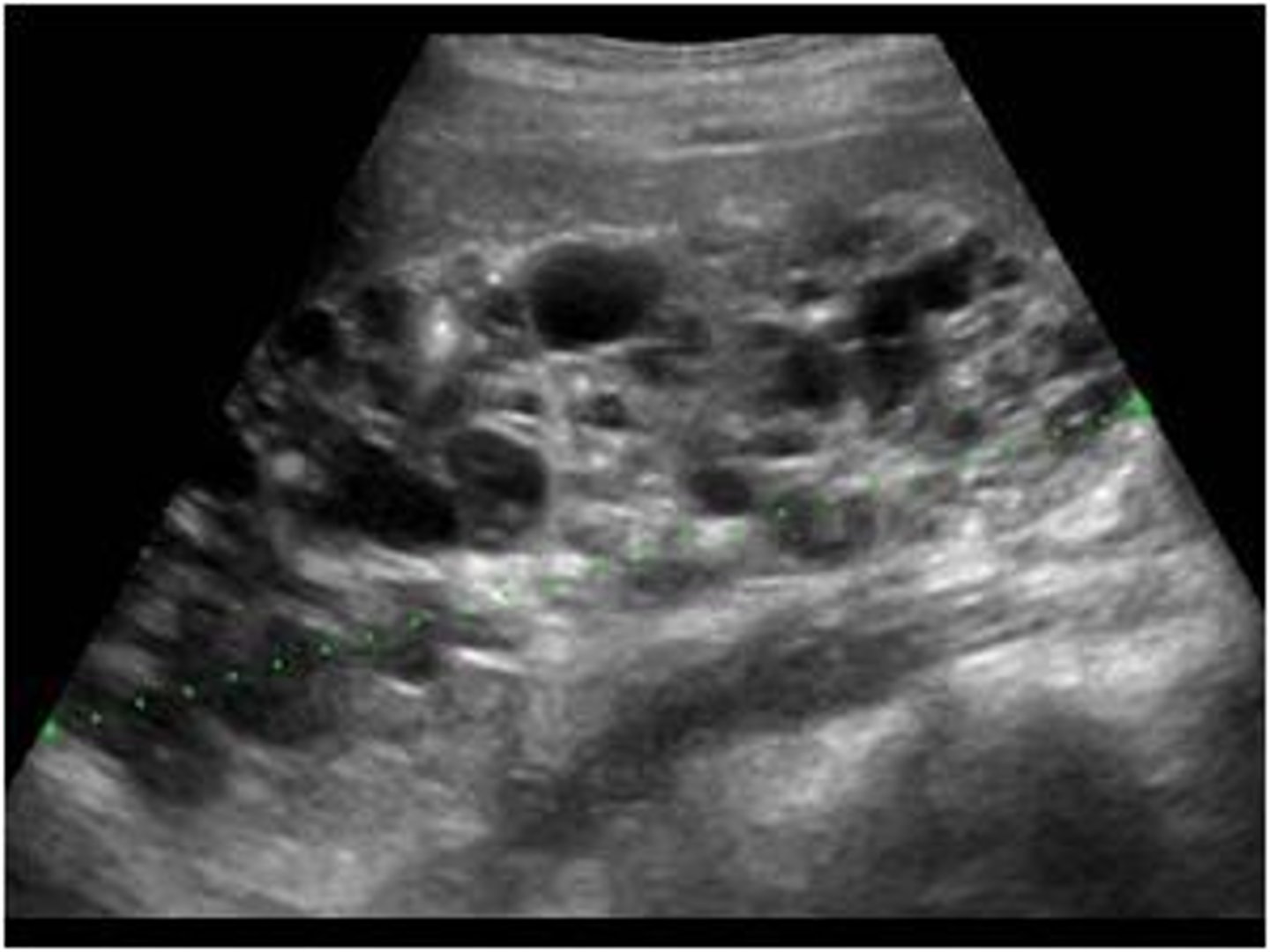
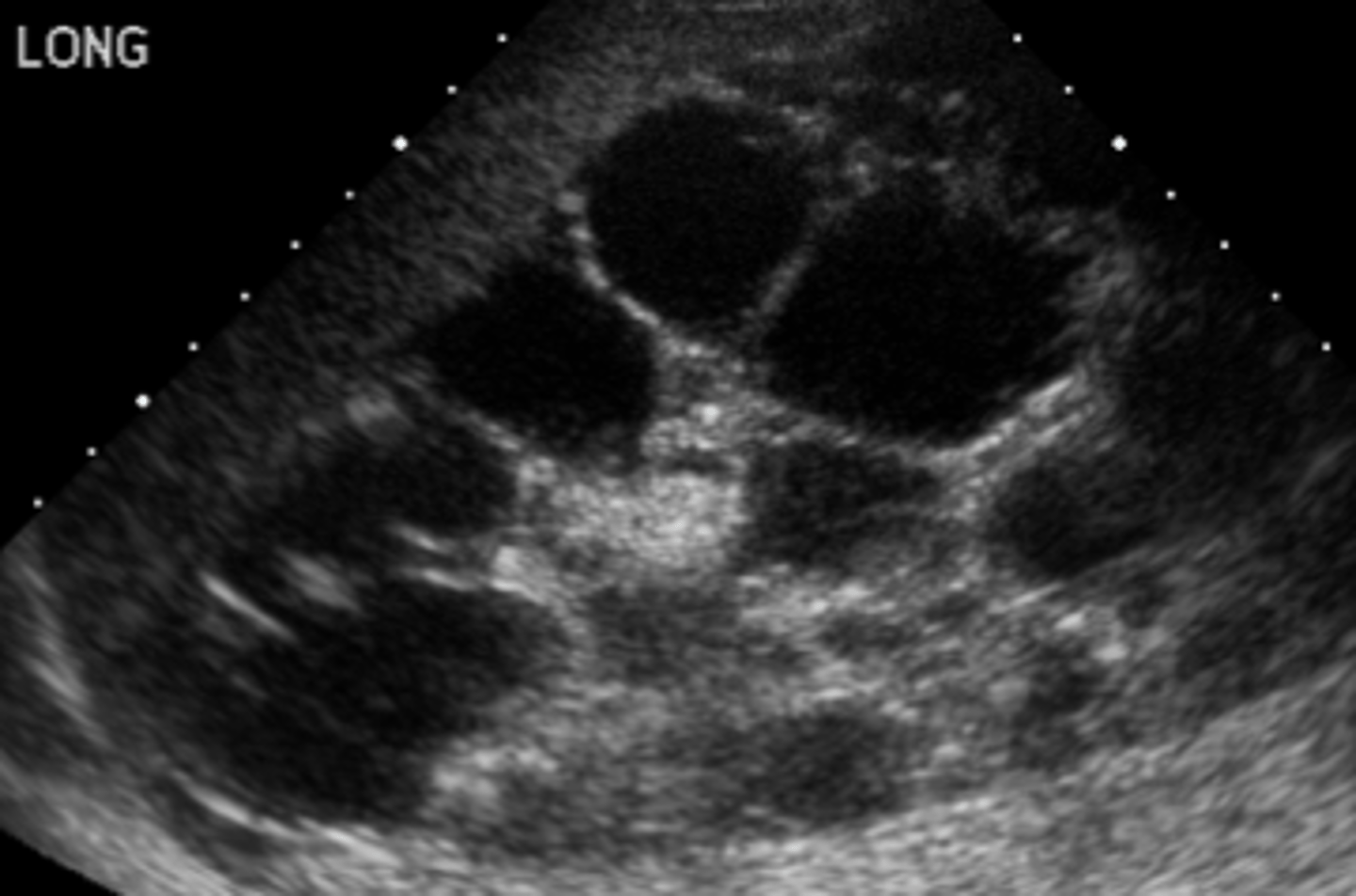
When does autosomal dominant polycystic kidney disease (PCKD) typically present? What are some common s/sxs?
Childhood or adulthood; early-onset HTN, mild polyuria, hematuria, episodic flank pain, nephrolithiasis, UTI, hepatic cysts, & intracranial aneurysms
What is the best initial diagnostic test for autosomal dominant PCKD? What is the best overall?
Initial: renal US
Overall: MRI
How is autosomal dominant PCKD managed? What is the prognosis like for these patients?
Symptomatic: tolvaptan (slows disease progression), ACEi/ARBs for HTN, NSAIDs for flank pain, low sodium diet, etc.; patients will go on to develop ESRD & eventually require transplant or dialysis
When does autosomal recessive polycystic kidney disease (PCKD) typically present? What are some common s/sxs?
Often found on the prenatal ultrasound (readily apparent at birth); anatomical abnormalities, HTN within first few months of life, CHF s/sxs, prenatal oligohydramnios (can produce anomalies such as pulmonary hypoplasia, Potter facies, etc.)
How is autosomal recessive PCKD managed? What is the prognosis like for these patients?
Symptomatic: ACEi/ARBs for HTN, NSAIDs for flank pain, low sodium diet, etc.; very high mortality here (30% do not survive infancy, 45% have ESRD by age 20)
What are some characteristic features of Potter facies, & what is this condition often secondary to?
Wide-set eyes, prominent inner canthus, beaked nose, large low-lying ears, spine/limb contractures, pulmonary hypoplasia; oligohydramnios

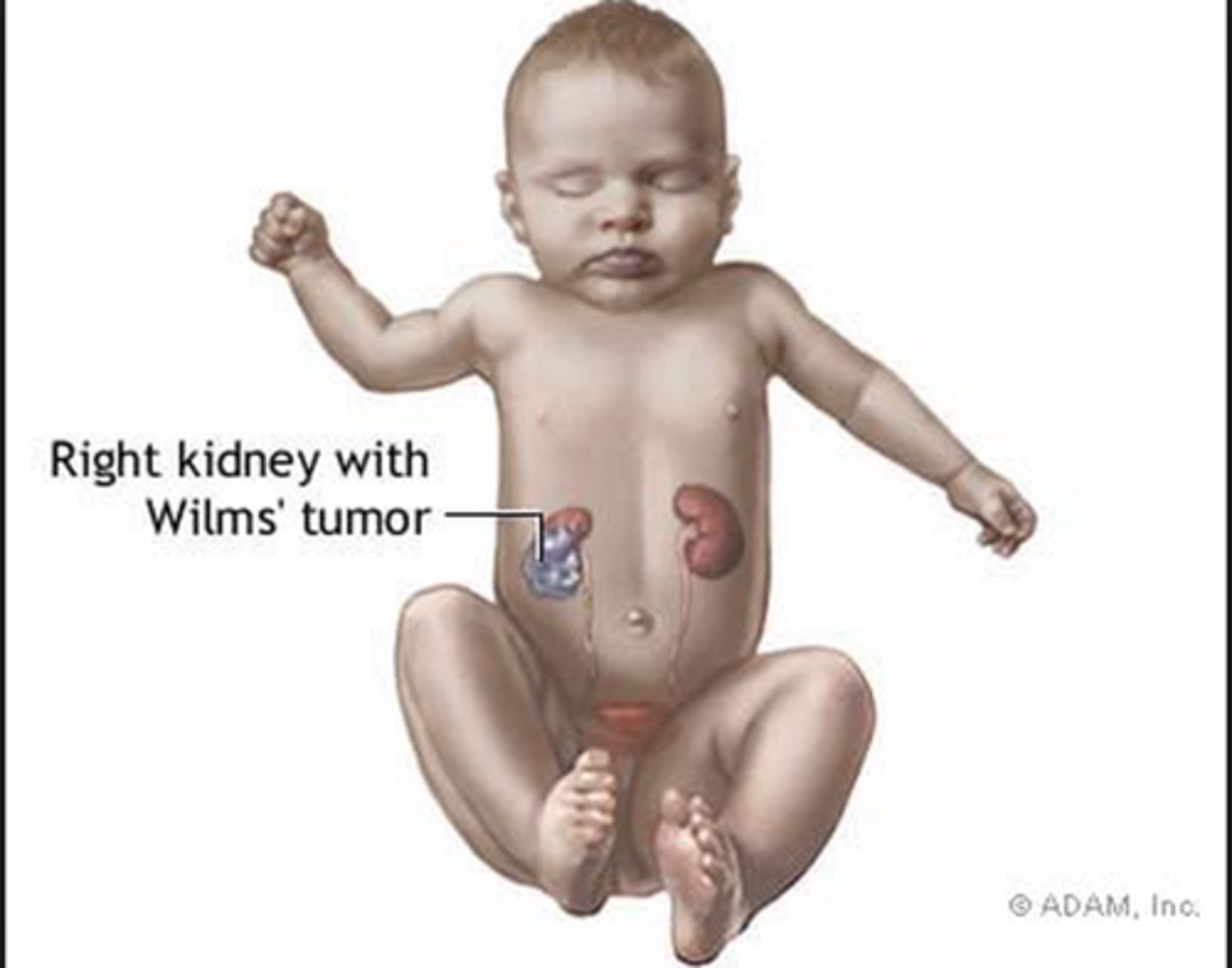
What is a Wilm's tumor (nephroblastoma), & what is it often associated with? What is the most common presentation?
Most common childhood renal tumor; WAGR syndrome (Wilm's tumor, aniridia, GU abnormalities, range of developmental delays); an incidental flank mass & possible hematuria
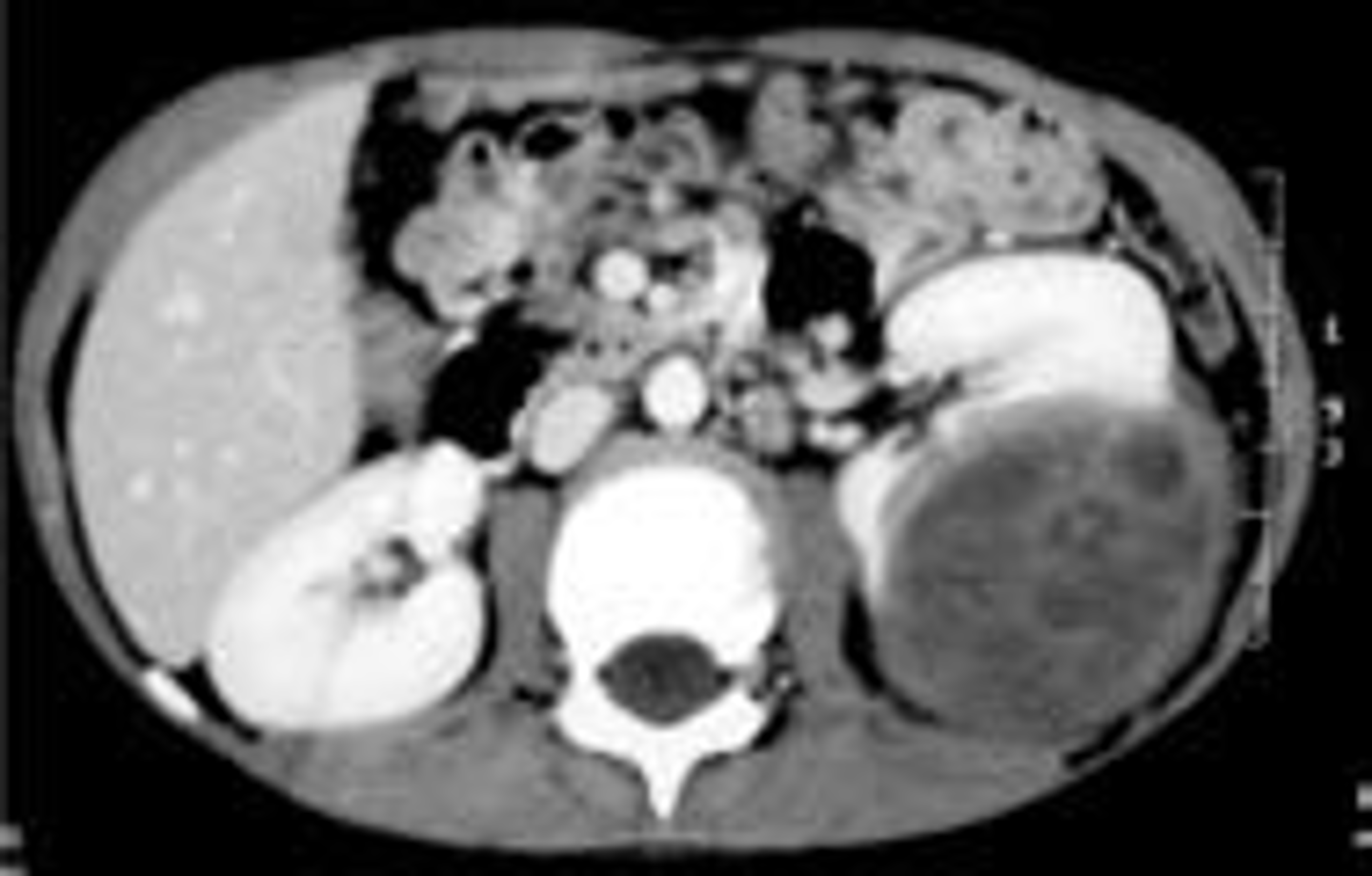
What is the best initial test to diagnose a WIlm's tumor? If this is positive, what should we follow this up with? How is it treated?
Diagnosis: abdominal CT, F/U w/ explorative laparotomy for biopsy if CT suggestive of a mass
Treatment: surgery & chemo (radiation for later stages)
What is unilateral renal agenesis often associated with?
Co-existing Mullerian agenesis in females (should also do a full VACTERL workup on these patients)
Is bilateral renal agenesis significant? What is often seen with this?
Yes - it is incompatible with life due to severe pulmonary hypoplasia (baby will either be stillborn or have severe respiratory distress & die shortly after birth); often shows oligohydramnios in utero
What is hemolytic uremic syndrome (HUS), & what is it often caused by?
Acute condition characterized by microangiopathic anemia (MAHA), acute renal insult/injury, & thrombocytopenia; typically follows an E. coli O157:H7 (EHEC) infection

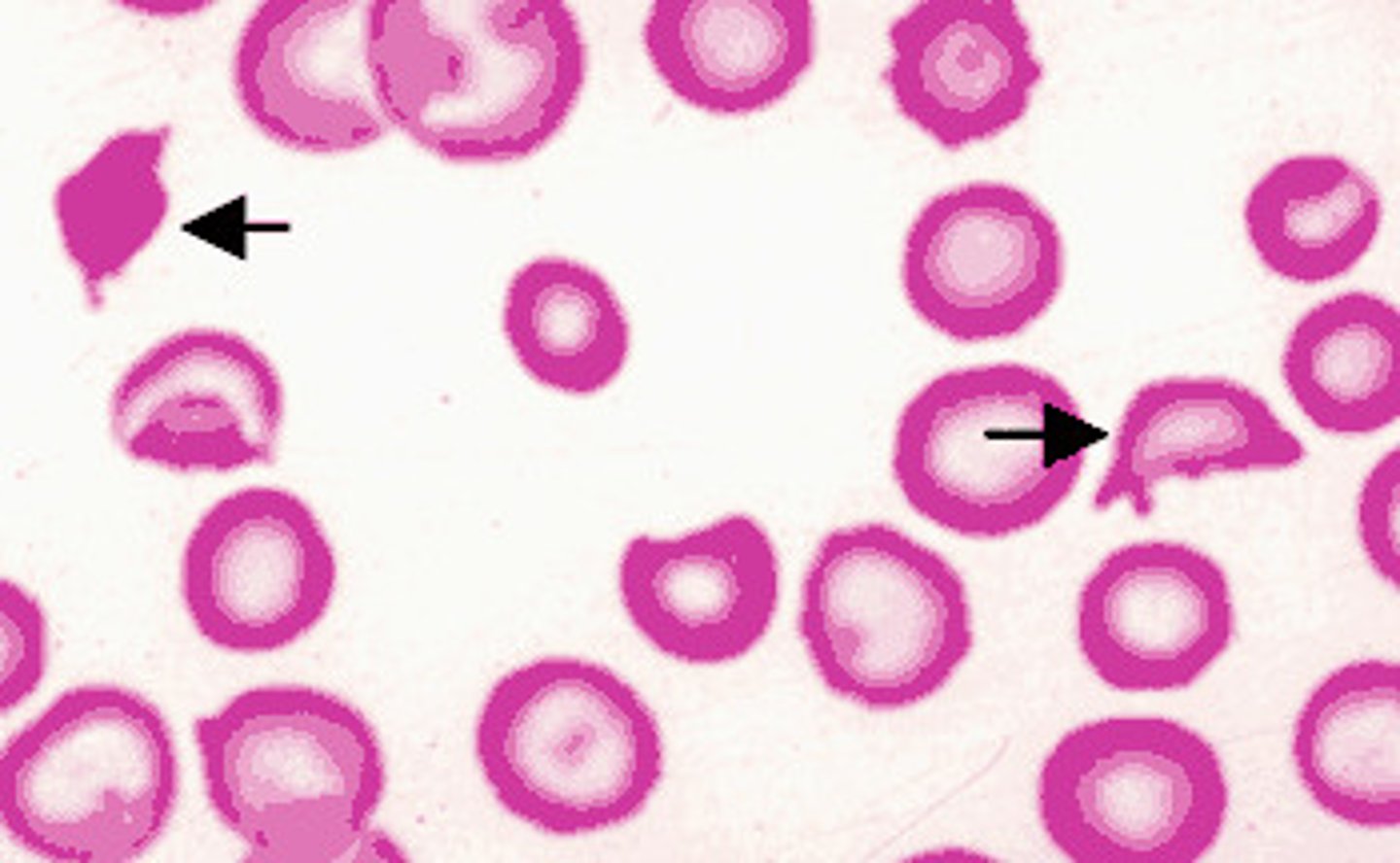
Again, what is responsible for producing shiga toxin (a cause of HUS)? What are some s/sxs?
E. coli 157:H7 (EHEC); bloody diarrhea, MAHA (schistocytes, Burr cells, helmet cells), thrombocytopenia, & acute renal failure
Are antibiotics a good idea in shiga toxin HUS?
NO - can cause patient to actually shed more tissue - don't use!
What are some possible causes of atypical HUS? How can we differentiate this from infectious causes of HUS such as shiga toxin?
Medications (OCPs, cyclosporine, tacrolimus); diarrhea is typically absent (other HUS signs are still present tho: MAHA, TTP, ARF, etc.)
As a whole, how is HUS managed?
Fluid restriction to balance UO
admission
packed RBCs for anemia
platelets only if < 20,000
dialysis if renal function continues to worsen
What is Henoch-Schoenlein purpura, & what is it characterized by?
Small vessel vasculitis of unknown cause characterized by arthralgia, non-blanching red-violet purpura (esp. on buttock), & prominent abdominal pain; also can have fever, HA, & nausea prodrome

How is Henoch-Schoenlein purpura diagnosed? Is treatment usually required?
Clinical, confirm w/ UA (shows microscopic hematuria (is a nephritic disease); no, is usually self-limited as long as there is no renal involvement
As a reminder, what is the difference between nephritic & nephrotic diseases?
Nephritic: inflammation of the glomerulus, blood is present in the urine
Nephrotic: holes in the GBM, blood is not present in the urine