Anesthetics (Khan)
1/36
Earn XP
Description and Tags
Based on Study Guide
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
What is MAC
What is Potency
Minimum Alveolar Concentration
measures the potency of an inhaled anesthetic
Lower MAC → more potent
Potency = 1/MAC
What is blood/gas coefficient
meaure of how soluble an inhaled anesthetic is in blood compared w/ alveolar gas phase
how quickly an inhaled anesthetic induces anesthesia and how quickly a pt recovers
Low b/g = anesthetic stays in lungs rather than dissolving in blood
Faster induction and recovery
High b/g = anesthetic dissolves extensively in blood
Slower induction and recovery
What are the inhaled anesthetics
Which is non-halogenated
Nitrous Oxide (non-halogenated)
Halothane
Methoxyflurane
Enflurane
Isoflurane
Desflurane
Sevoflurane
General MOA of Anesthetics
Potentiate inhibitory synaptic activity
Enhance GABA-A and glycine receptors
Increases Cl influx, activate K channels → neuronal hyperpolarization
Diminish excitatory synaptic activity
Inhibit ACh and NMDA receptors
Decreases Na and Ca influx
Net Effect: decreased CNS excitation + increased inhibition
Nitrous Oxide
MOA
Activates opioid neurons in the periaqueductal grey matter
Produces strong analgesia
Nitrous Oxide
Pharmacological Properties
Least potent inhaled anesthetic
Very rapid induction/recovery (low blood/gas)
Strong analgesic effect
Isoflurane
Pharmacological Properties
Volatile liquid at room temp w/ pungent odor
Used mainly for maintenance anesthesia
Relatively slow onset and delivery
Good safety profile (commonly used)
Desflurane
Pharmacological Properties
Rapid onset and recovery (low blood/gas)
Commonly used for outpatient surgery
Desflurane
ADRs
Pungent odor
Airway irritation/cough
Sevoflurane
Pharmacological Properties
Rapid onset and recovery
Drug of choice for pediatric anesthetic induction
Sevoflurane
ADRs
Volatile at room temp (not pungent)
Metabolized to fluoride ions
Potential nephrotoxicity
Name IV anesthetics
Propofol
Dexmedetomidine
Lorazepam
Midazolam
Ketamine
Etomidate
Propofol
MOA
Pharm Properties
MOA
Potentiates GABA-A receptors
Pharm Properties
Short acting sedative-hypnotic
Poor water solubility, formulated as an IV emulsion (pain on injection)
Causes sedation and hypnosis
Lowers BP
Respiratory depression
No analgesic effect
Propofol
ADRs
BW
ADRs
Hypotension
Apnea
Hypertriglyceridemia
Green urine/hair/nailbeds
Propofol Infusion Syndrome (PRIS); rare but fatal
BW
Risk of bacterial contamination; discard tubing and vial within 12 hours
C/I to egg or soy allergy
Dexmedetomidine
MOA
Pharm Properties
ADRs
MOA
Selective α2-adrenergic agonist
Pharm Properties
Sedation and analgesia
Minimal respiratory depression
Lowers HR and BP
High doses may cause HTN
ADRs
Hypo/Hypertension
Bradycardia
Benzo (Lorazepam & Midazolam)
MOA
Pharm Properties
ADRs
MOA
Positive allosteric modulators fo GABA-A
Increase frequency of Cl channel opening
Pharm Properties
Sedation, anxiolysis, amnesia
CNS depression limited by endogenous GABA
Respiratory depression increased when combined with opioids
ADRs
Respiratory depression
Dependence and withdrawal
Abuse potential
Midazolam Box Warning
Respiratory depression, respiratory arrest
Use lower end of dosing range in debilitated and geriatric population
Not to administer by rapid IV injection in neonates
What can happen if you take a Benzo + Opioid
Sedation
Respiratory depression
Coma
Death
Use flumazenil BZD respiratory antagonist for OD
Ketamine
MOA
Pharm Properties
ADRs
MOA
NMDA receptor antagonist
Pharm Properties
Produces anesthesia and significant analgesia
Sympathetic stimulation; Increases HR, BP, and cardiac output
ADRs
Emergence Reactions
Vivid dreams
Hallucinations
Delirium
BZDs reduce incidence of emergence reactions
Etomidate
MOA
Pharm Properties
ADRs
MOA
Produces hypnosis (no analgesia)
Pharm Properties
Ultra short acting
Minimal effects on cardiac output and peripheral resistance
Less respiratory depression
ADRs
N/V
Adrenal suppression (less cortisol production)
Monitor Hypotension and Hyperkalemia
Therapeutic uses of Local Analgesics
Abolish pain sensation in limited area of the body without producing unconciousness
Uses
Topically in burns and small cuts
Injection during dental procedure
Epidural blocks during obstetric procedure and surgery
Are LAs specific for pain fibers?
If not then what muscles and fibers are blocked
Not specific for pain fibers; can block other sensory motor and autonomic fibers
Cardiac and skeletal muscles action potential
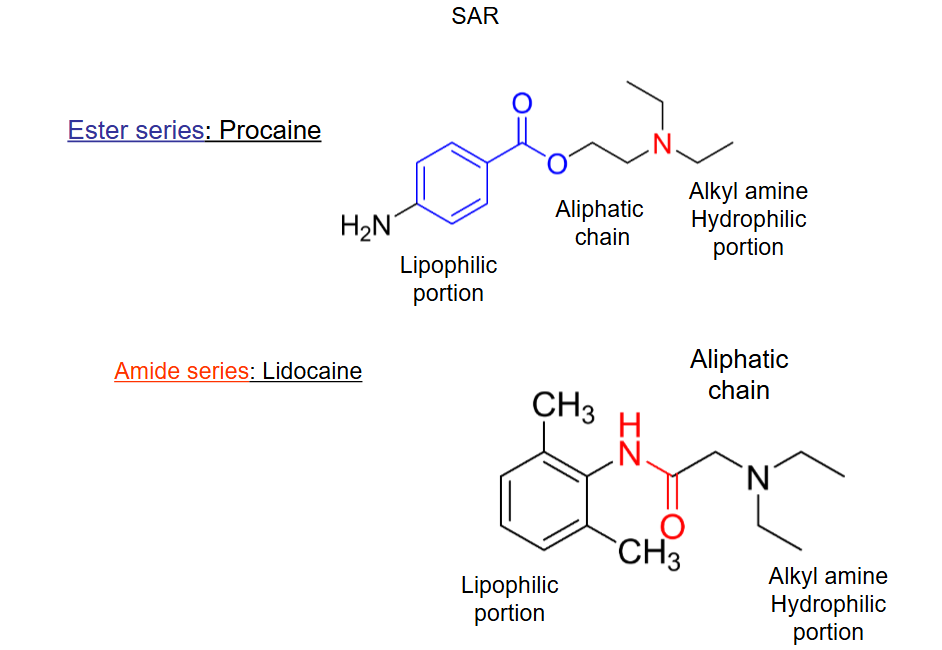
List ester and amide LA
Ester
Tetracaine
Procaine
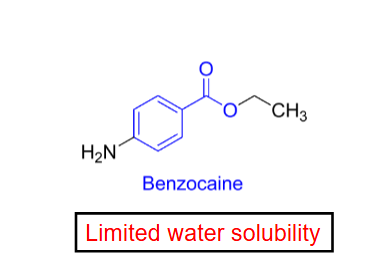
Benzocaine
Amide
Lidocaine
Mepivacaine
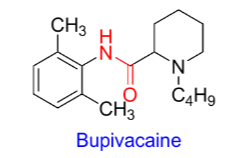
Bupivacaine & Levobupivacaine
Ropivacaine
Prilocaine
What is the importance of ionic form of LA
Most active at the receptor site because it cannot exit from closed channels
Importance of nonionic form of LA
Uncharged form is important for rapid penetration of membranes
SAR Properties
Lipophilic Portion
Essential for local anesthetic activity
Important binding to the sodium channel receptor
Di-ortho substitution protects the amide bond from hydrolysis
Increases metabolic stability and duration of action
Aliphatic Chain
Connects aromatic ring and amine
Usually 1-3 carbons long
Determines whether drug is ester or amide
Amide- more resistant to metabolic inactivation
Ester- more susceptible to ester hydrolysis
Alkyl amine Hydrophilic portion
Most local 3o alkyl amine
Increases water solubility
Protonated form binds to the receptor site inside the Na channel
Which LA lacks a tertiary amine
Benzocaine
poor water solubility
mainly used as topical anesthetic
Absorption of LA
The rate and extent of systemic absorption of LAs is greater
From densely perfused tissues (more vascularity)
Following multiple administrations (increasing concentration of LA)
Vasoconstrictor
Increases conc. and duration of action of LA at site of injection
Decreases the max systemic conc. of LA, and thereby reduces the potentials for systemic toxicity
Distribution of LA
IV bolus of amide LAs results in wide tissue distribution
Sequestration occurs in fatty tissue
Initial rapid distribution-uptake into highly perfused organs (heart, brain, liver, kidney)
Metabolism of LA
LA are converted in the liver and plasma to more water-soluble metabolites and then excreted in urine
Ester type drugs are hydrolyzed very rapidly in the blood by butyryl cholinesterase
Amide drugs are hydrolyzed by liver microsomal CYP 450
Toxicity of amide drug is more likely to occur in patients with liver disease
Why is Epinephrine given along LA
Enhances and prolongs LA induced spinal anesthesia by acting on α2 adrenoreceptor, which inhibit release of substance P and reduce sensory neuron firing
Epi-LA combo reduces systemic absorption, and enhances LA uptake
What is the MOA of LA
Block VG Na channels of the cell membrane
Prevent membrane depolarization and AP generation
Receptor is not readily accessible from the external side of the cell membrane
LA gain access to their receptors from the cytoplasm or the membrane
Cardiovascular Effects of LA
LAs can depress myocardial contractility and produce arteriolar vasodilation → severe hypotension
At high concentrations block cardiac Ca channels
Other toxicities of LA
Prilocaine in high doses causes methemoglobinemia (cyanotic and chocolate colored blood)
IV administration of reducing agents to convert to Hgb
Ester type drugs are metabolized to PAPA derivatives
These metabolites are responsible for allergic reactions in a small percentage of population
Lidocaine properties
Rapid onset of action due to high lipophilicity
Longer duration of action
Also used as Class IB antiarrhythmic agent
Extensively metabolized in liver by N-dealkylation & aromatic hydroxylation
Lidocaine ADRs
Drowsiness
Seizure
CV depression
Which isomer is responsible for Bupivacaine cardiotoxicity
R(+) enantiomer responsible for cardiotoxicity → ventricular arrhythmia