Type 1 Hypersensitivity
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
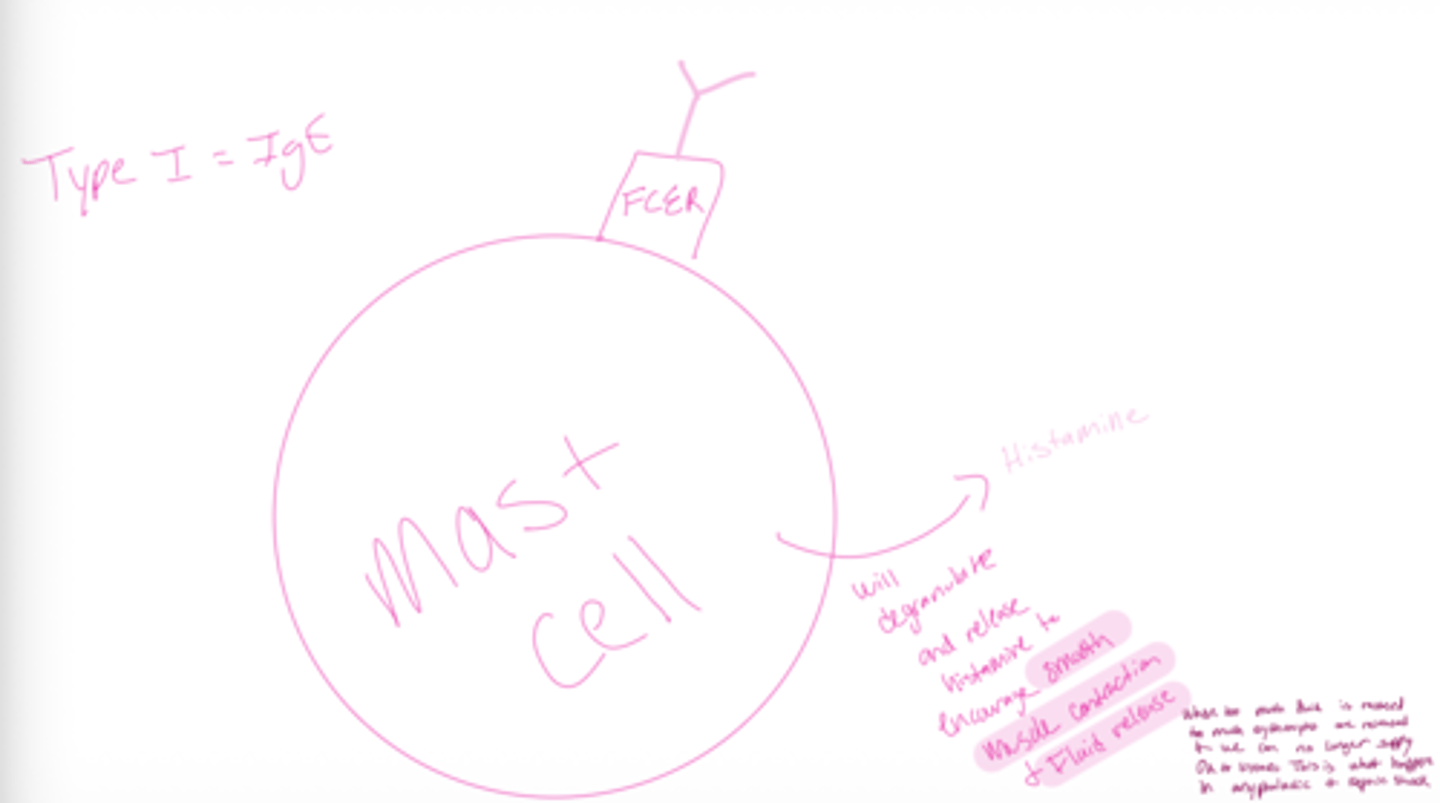
describe generally the process of anyphalactic shock and septic shock
see how the mast cell will degranulate and release histamin to encourage smooth muscle contaction and fluid release
when too much fluid is released and too much erythrocytes are released and we can no longer supply O2 to tissues. this is what happenes in anyphalatic and septic shock
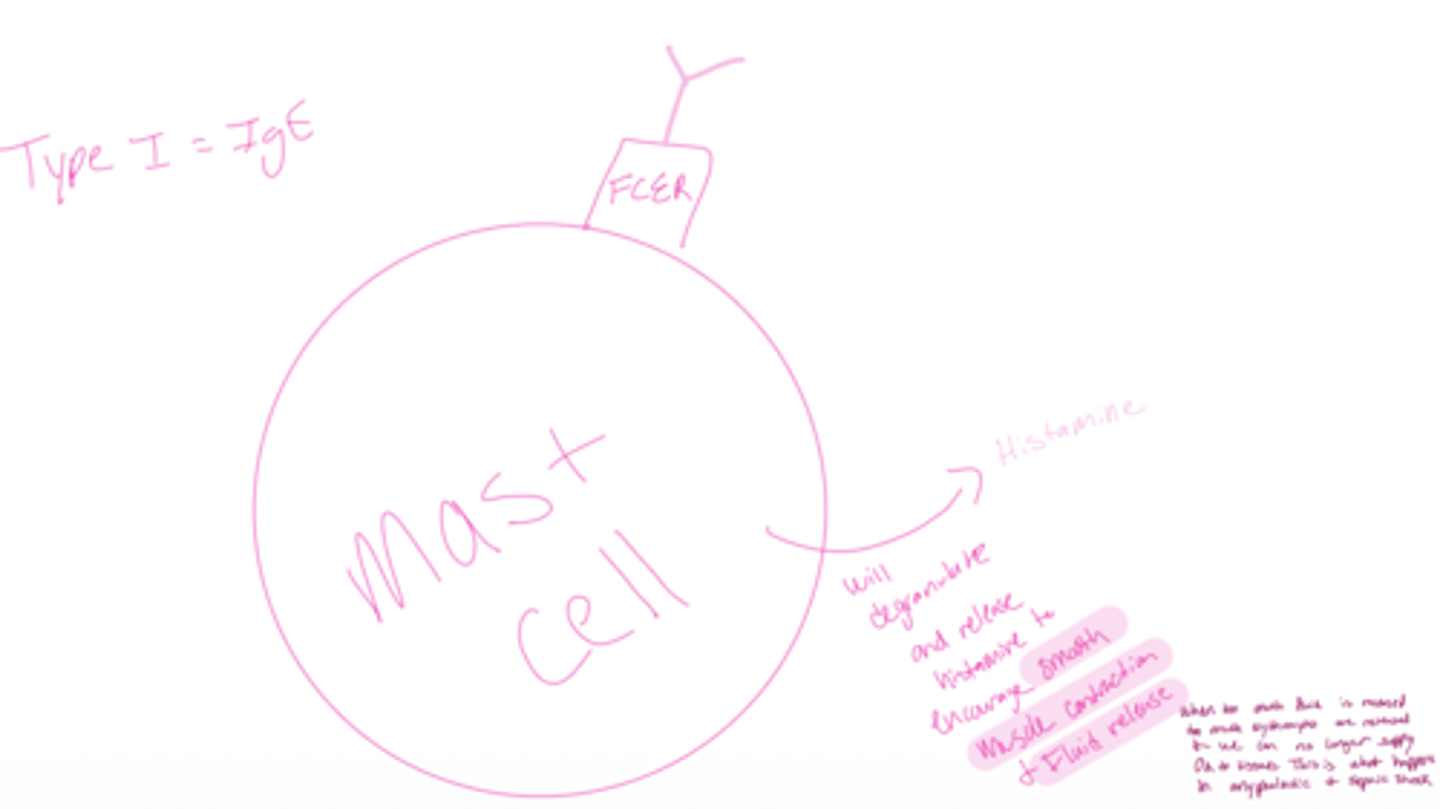
What type of hypersensitivity is associated with Type 1?
IgE → Type I hypersensitivity (allergies)
for example anaphylatic shock and septic shock
immeditae hypersensitivity
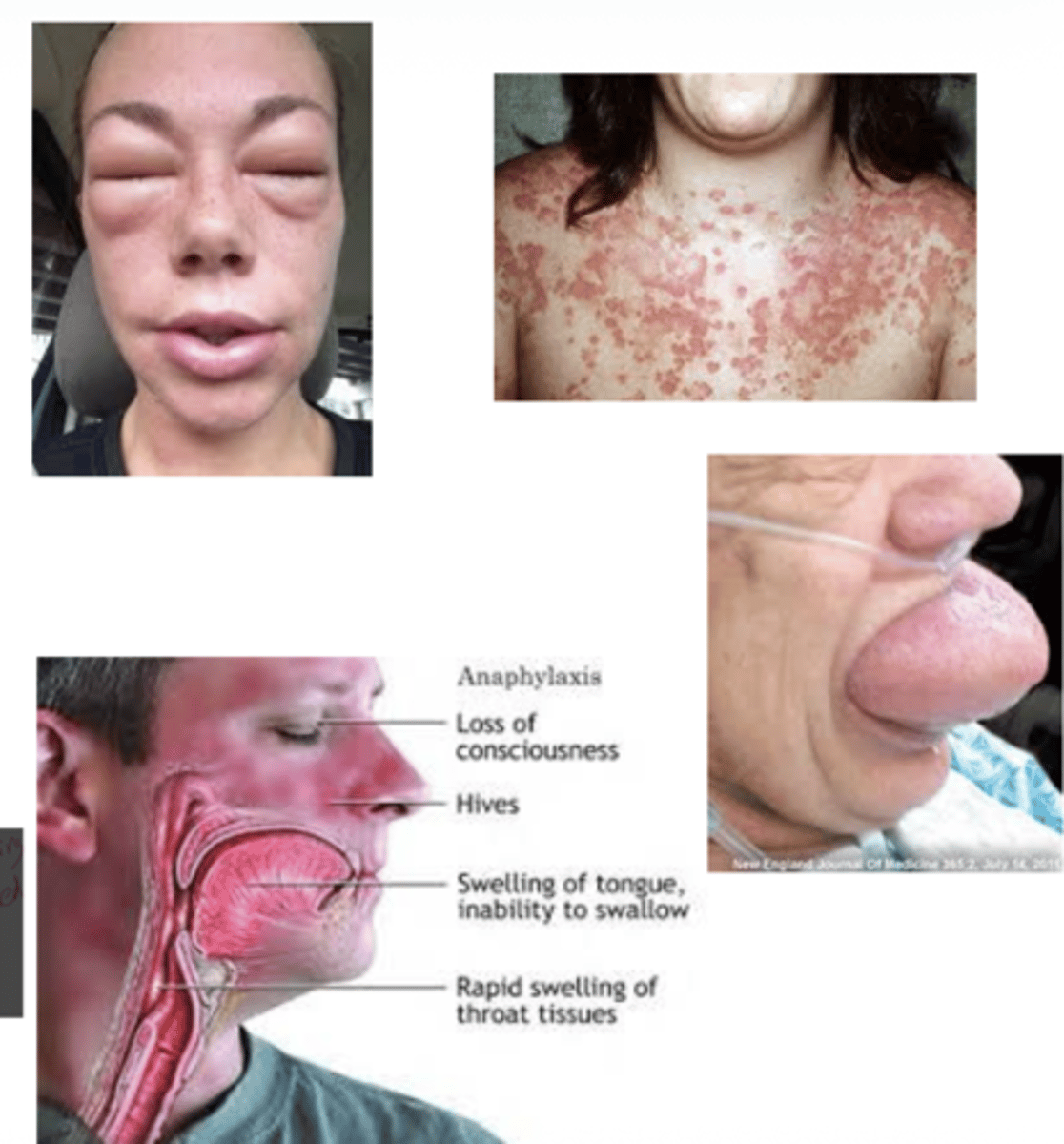
irritation (runny nose) to tissue damage (bronchospasm) to death (asphyxiation)
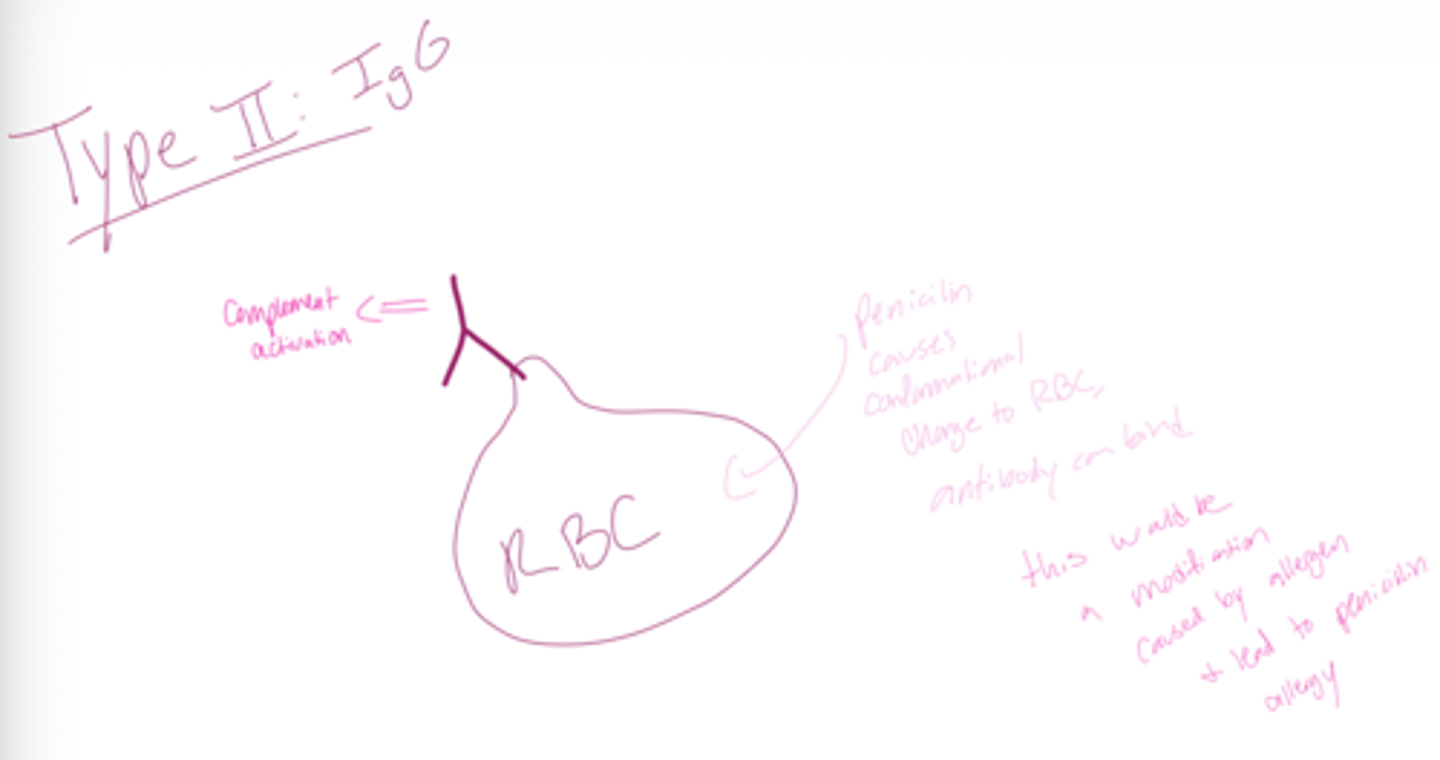
What type of hypersensitivity is associated with Type 2?
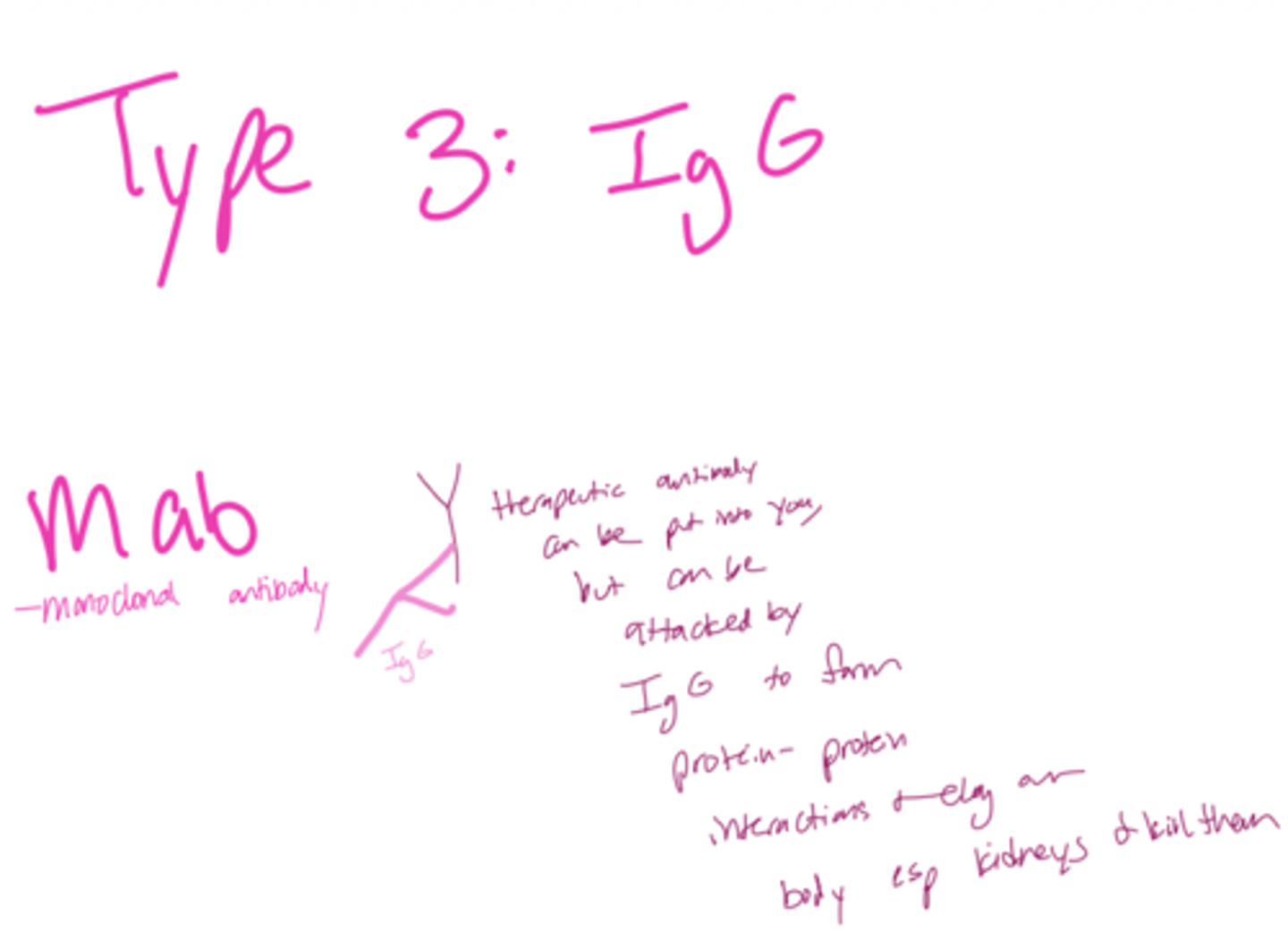
What type of hypersensitivity is associated with Type 3?
What type of hypersensitivity is associated with Type 4?
Q: What are hypersensitivity reactions also called?
A: Allergies or autoimmune hypersensitivities
Q: What do hypersensitivity reactions occur in response to?
A: Innocuous substances (normally harmless) called allergens.
Q: What is the main consequence of hypersensitivity reactions?
A: Inflammation and tissue damage, which in severe cases can lead to death.
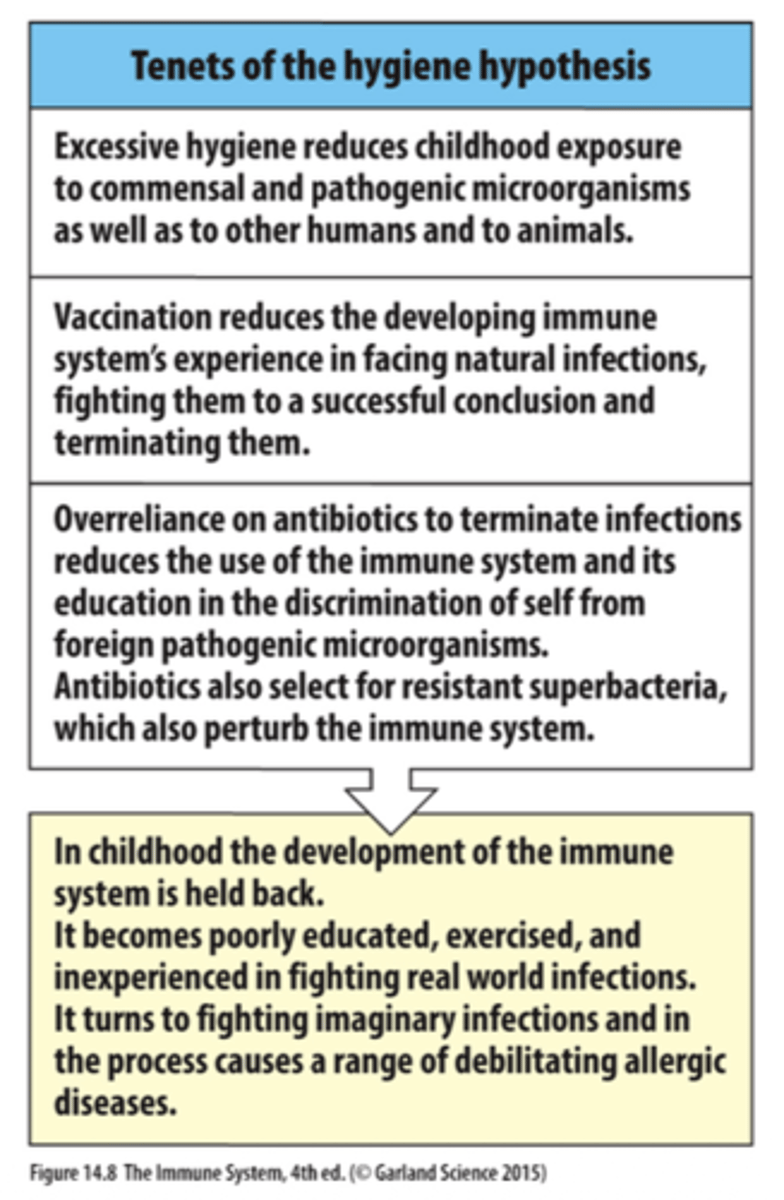
Q: What is the Hygiene Hypothesis?
A: The idea that overly clean environments and reduced exposure to microbes during childhood impair immune system training, increasing allergy risk.
note that in the past 30 years allergies have more than doubled, and now 10-40% of the developed world suffer from allergies
Q: What is Type I hypersensitivity?
A: The most common form of hypersensitivity, also called immediate hypersensitivity.
Q: Which antibody is involved in Type I hypersensitivity?
A: IgE
Q: Why is Type I called “immediate” hypersensitivity?
A: Symptoms occur rapidly after exposure to the allergen.
what are the sympotms of type 1 hypersensitivity
Irritation (runny nose) to tissue
damage (bronchospasm) to
death (asphyxiation)
Q: What receptor does IgE bind to?
A: IgE binds rapidly to the high-affinity FcεR receptor.
Q: Which cells express FcεR and bind IgE?
A: Mast cells, basophils, and eosinophils
Q: What is the normal protective role of IgE?
A: Defense against parasitic infections.
Q: What happens when IgE is cross-linked by an allergen?
A: Mast cell degranulation occurs.
Q: Result of mast cell degranulation?
A: Inflammatory reactions and physical expulsion (mucus, coughing, vomiting, diarrhea).
Q: Why is IgE problematic in developed countries?
A: Few parasites → IgE instead reacts to harmless allergens → increased allergies.
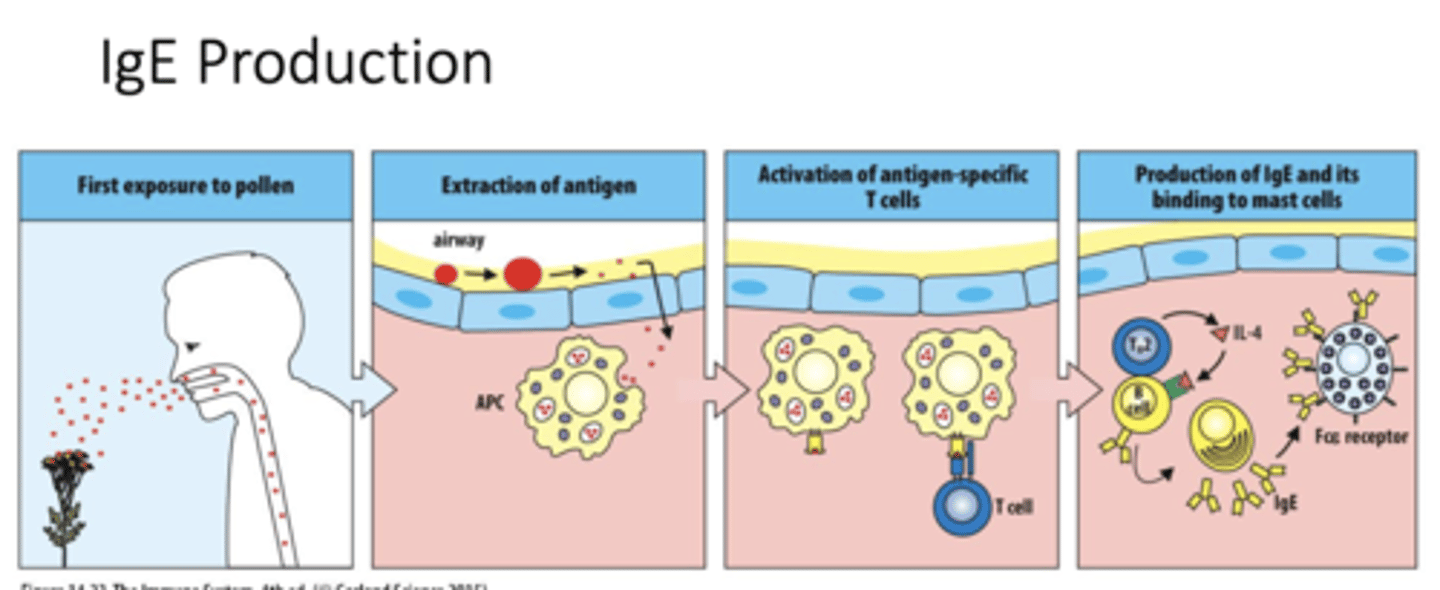
Q: What occurs during the first exposure to pollen in Type I hypersensitivity?
A: Pollen enters the airway and acts as an allergen, starting the sensitization phase of the immune response.
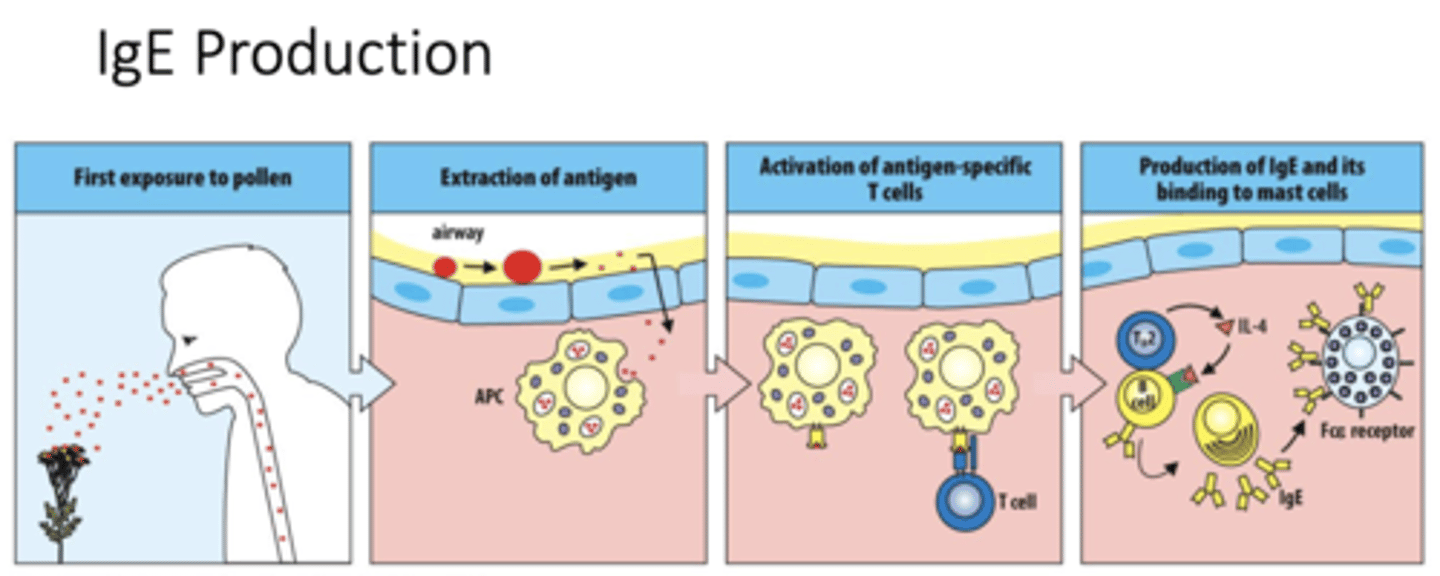
Q: What does “extraction of antigen” mean in an allergic response?
A: Antigen-presenting cells (APCs) capture and process pollen allergens from the airway lining.
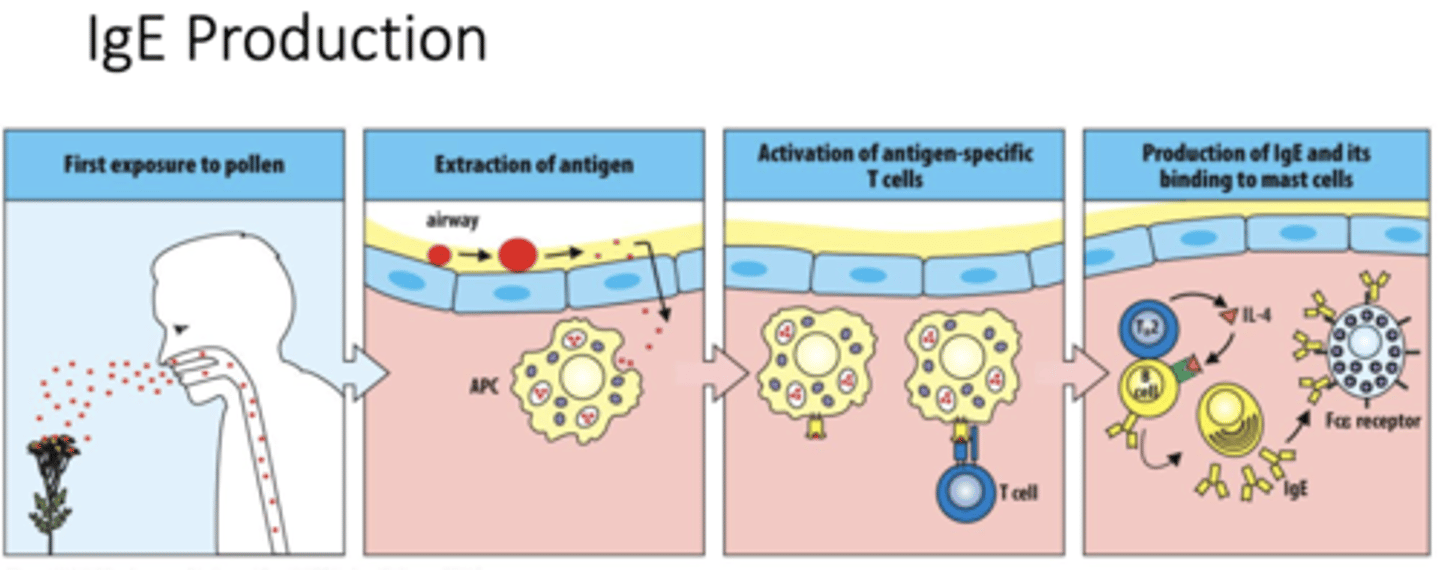
Q: How are antigen-specific T cells activated in Type I hypersensitivity?
A: APCs display the processed allergen on their surface to naive T cells, activating them.
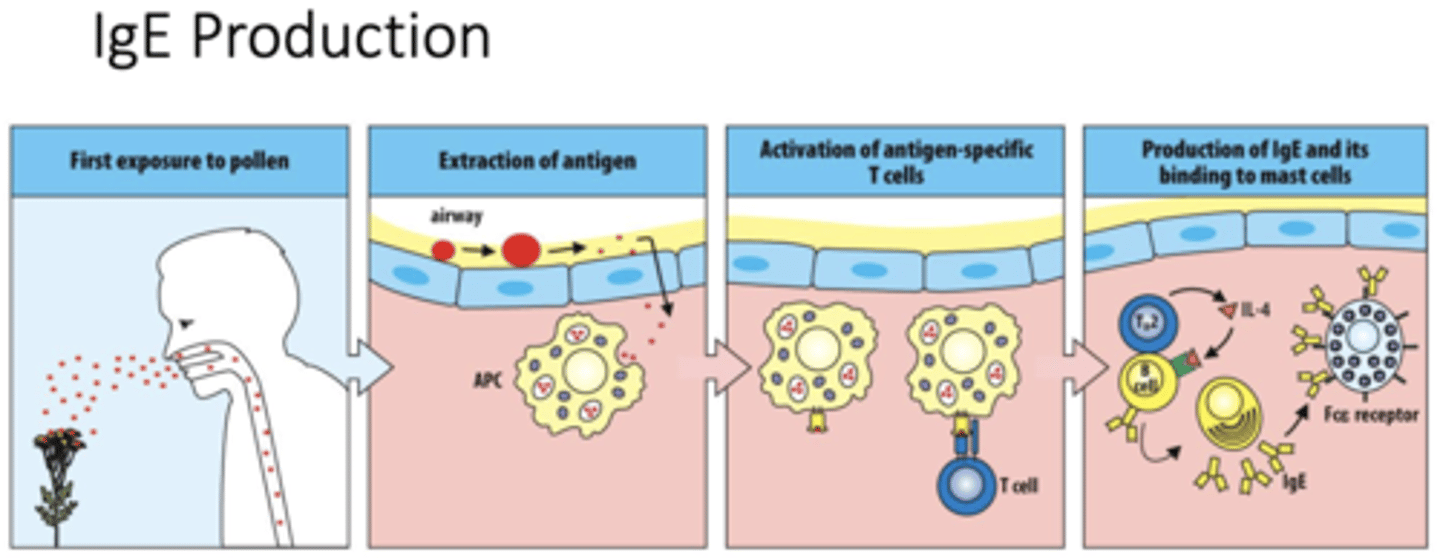
Q: What role does IL-4 play in Type I hypersensitivity?
A: IL-4 released by TH2 cells signals B cells to switch antibody production to IgE
Q: Which leukocytes act together during allergic inflammation?
A: Mast cells, eosinophils, and basophils work together to drive the allergic response
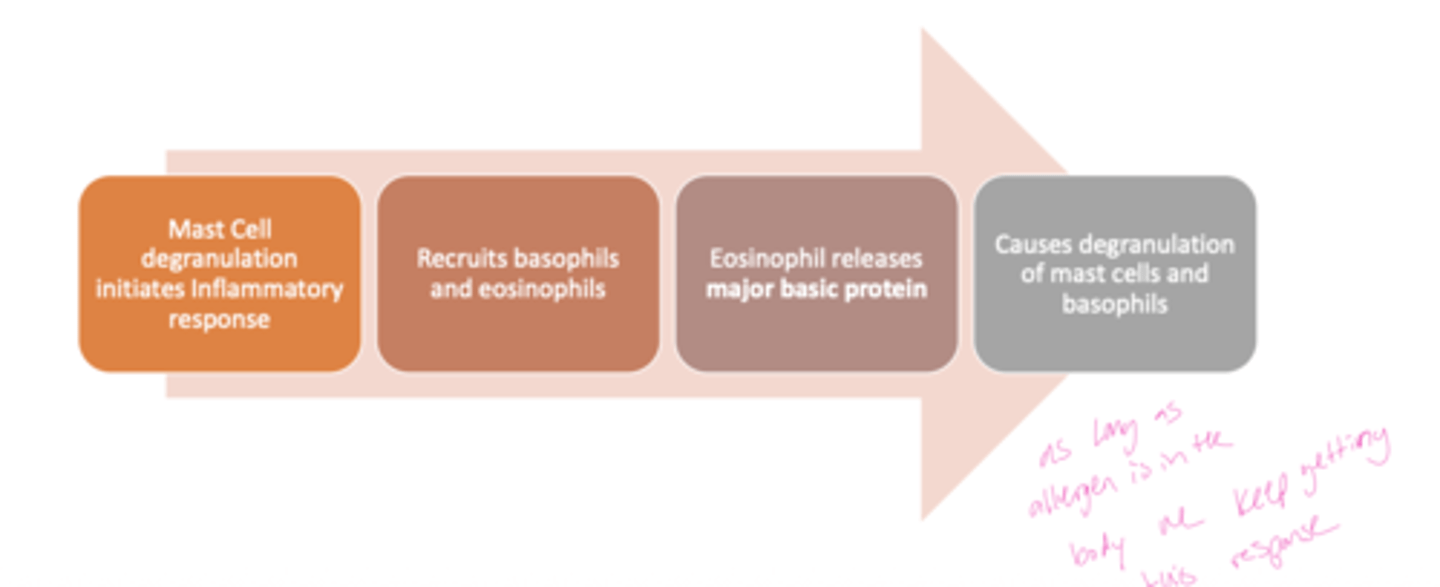
Q: What role do mast cells play in an allergic reaction?
A: Mast cell degranulation initiates the inflammatory response by releasing histamine and other mediators.
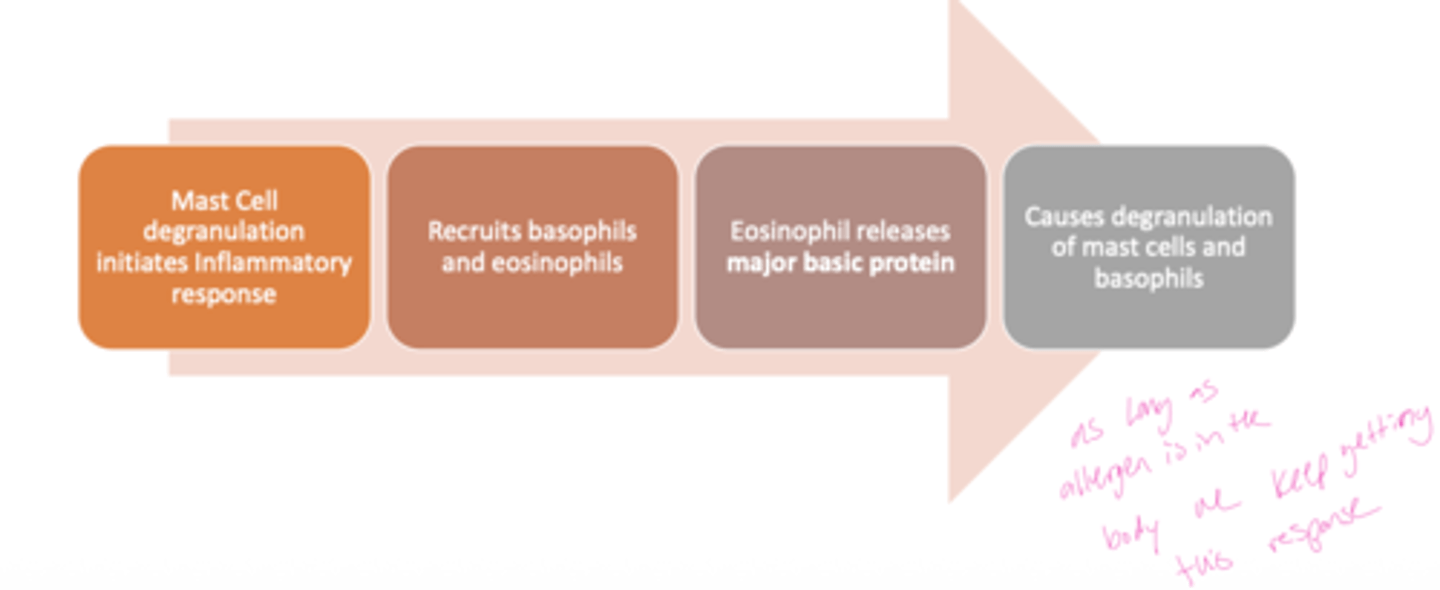
Q: What happens after mast cell activation during allergy?
A: The inflammatory signals recruit basophils and eosinophils to the site of exposure.
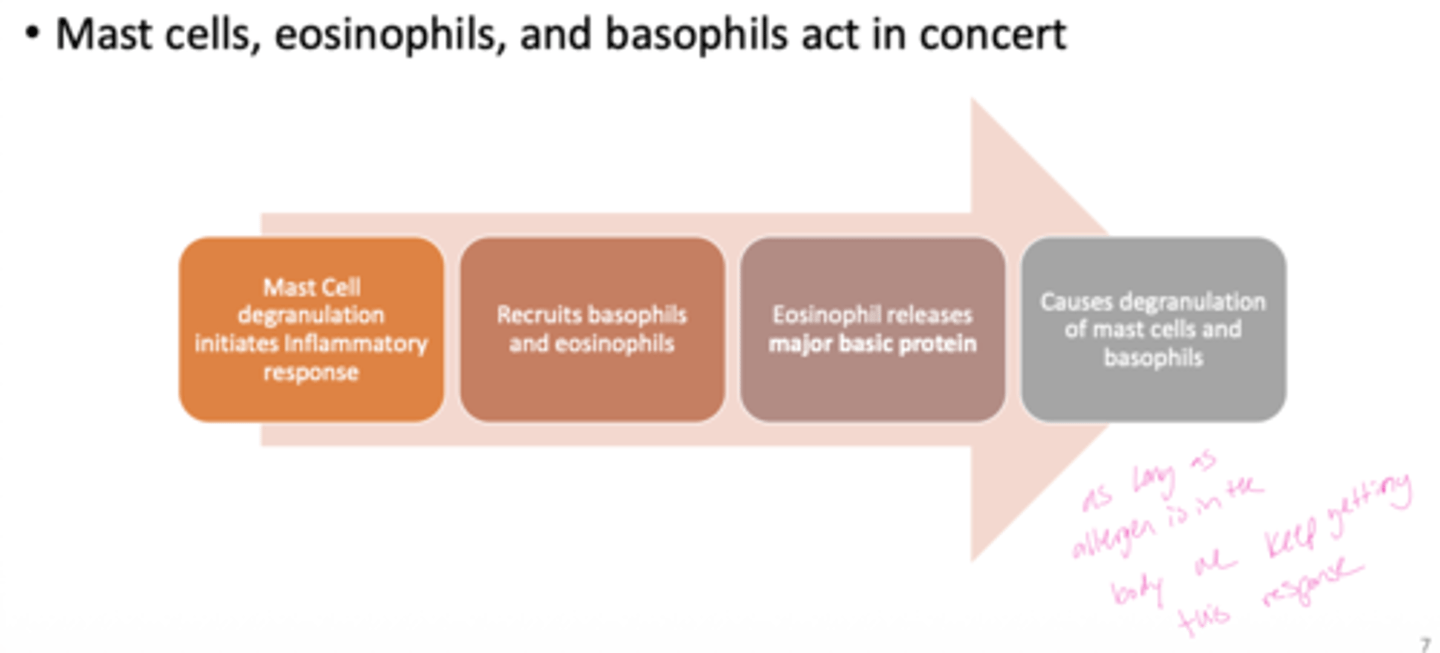
Q: What is the main effector function of eosinophils in allergy?
A: Eosinophils release major basic protein, which contributes to tissue damage and inflammation.
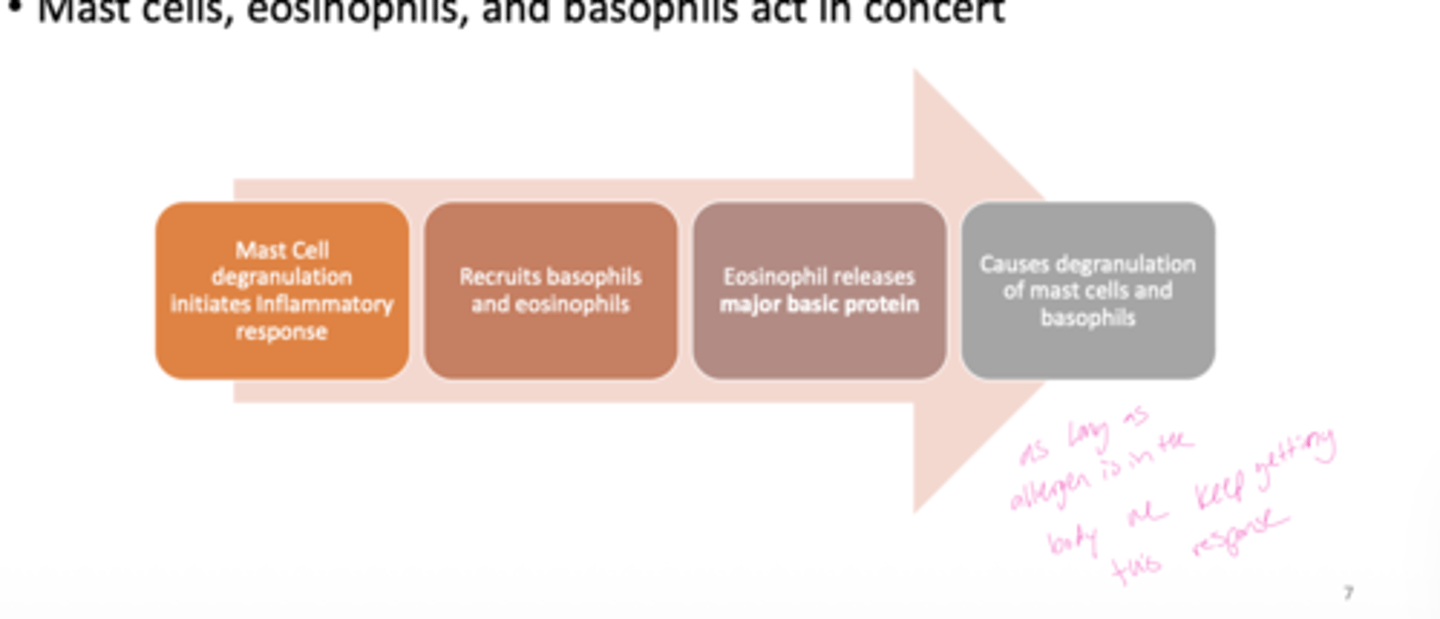
Q: How do eosinophils and basophils amplify the allergic response?
A: Their activity causes further degranulation of mast cells and basophils, intensifying inflammation.
Q: How is the allergic reaction amplified over time?
A: Continuous allergen presence causes repeated degranulation of mast cells and basophils, creating an escalating inflammatory cycle.
Q: Where are mast cells primarily located in the body?
A: Mast cells are resident in mucosal tissues, epithelial tissues, and vascularized tissues.
Q: What are the main functional roles of mast cells in body tissues?
A: Mast cells maintain tissue integrity, alert the body to infection or trauma, and participate in repairing tissue damage.
Q: What are pre-formed granules in mast cells?
A: Mast cells contain 50–200 pre-formed granules in the cytoplasm that store inflammatory mediators.
Mast cell granules contain histamine, a key mediator of inflammation and allergic responses
Q: What is the lifespan characteristic of mast cells?
A: Mast cells are long-lived immune cells that remain in tissues for extended periods.
Q: How do mast cells interact with IgE antibodies?
A: Mast cells retain IgE antibodies on their surface via high-affinity FcεR receptors, allowing rapid response upon allergen exposure.
Q: How do mast cells respond to antigens besides releasing histamine?
A: They synthesize cytokines, chemokines, and eicosanoids to respond to antigens
Q: What are leukotrienes, and how do they compare to histamine?
A: Leukotrienes have the same effects as histamine but are 100× more potent
Q: What effect do prostaglandins from mast cells have on blood vessels?
A: They cause vessel dilation and increase permeability. the combination of vasodilation and fluid leakage can cause rapid cardiovascular collapse and airway obstruction, which are hallmarks of anaphylactic shock.

what is the effects of mast cell activation and granule release on the GI tract?
increased fluid secretion, increased peristalsis (stomach contraction)
leads to expulsion of gi tract contents (v/d)
what is the effects of mast cell activation and granule release on the airways?
decreased diameter, increased mucus secretion
leads to expulsion of airway contents (phelgm, coughing)
what is the effects of mast cell activation and granule release on the blood vessels?
increased blood flow, increased permeability, leads to edema, inflammation, increased lymph flow and carriage of antigen to lymph nodes
Q: What type of protein makes eosinophils highly cytotoxic?
A: Major basic protein, this is used to kill worms, but pollen and dander is so small when it is seen as foreign and attacked it will likely kill our own tissues.
eosinophils can cause damage when migrating.
Q: Are eosinophils normally found in high or low numbers?
A: Low numbers
Q: What triggers an increase in eosinophil numbers?
A: Th2 activation
Q: what type of allergies are linked to eosinophils
A: Chronic allergic reactions and chronic asthma
Q: What types of granules do eosinophils have?
A: Preformed granules followed by synthesized granules
Q: Do eosinophils typically express FcεR?
A: No, they do not typically express FcεR
if this was induced, people could have severe allergic response
Q: What cell type induces eosinophil activation?
A: Mast cells
Q: Which cytotoxic protein is a hallmark of eosinophils?
A: Major basic protein
Q: What effect do eosinophils have on mast cells?
A: They promote more mast cell degranulation
Q: How are basophil granules similar to other immune cells?
A: Their granules are similar to those of mast cells
Q: What percentage of leukocytes are basophils?
A: Less than 1%
Q: How do basophils influence the Th2 response?
A: They drive the Th2 response by secreting IL-4
Q: How can basophils be activated?
A: Through Toll-like receptors (TLRs)
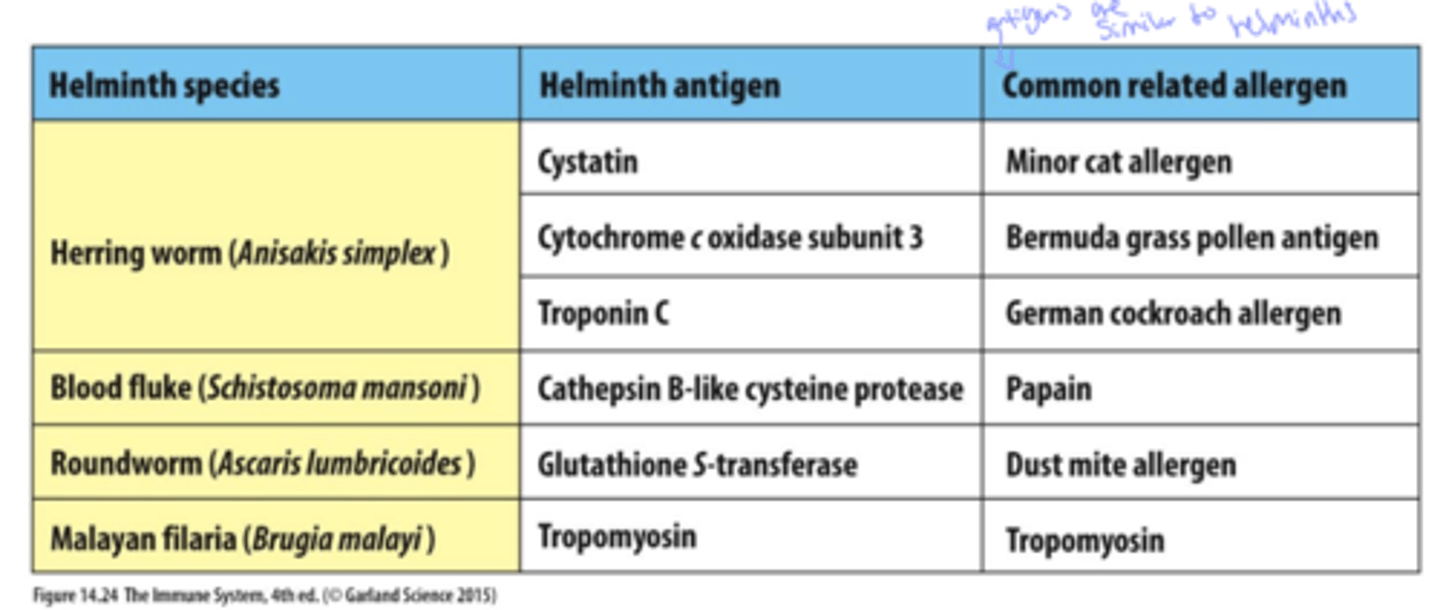
Q: What can cause allergies due to similarity between antigens?
A: Cross-reactivity of similar antigens
in simple terms, common allerens tend to be chemically similar to helminths (ex: peanuts)
Q: How does genetics influence allergies, and give examples?
A: Genetic predisposition increases the likelihood of developing allergies
ex: Some allergy genes are more common in Caucasians, making their immune system more likely to overreact.
also Many genes can make you more likely to have allergies, not just a single gene
Q: How can mothers pass allergy risk to their child after birth?
A: 1. IgE is present in amniotic fluid which the fetus ingests
and
2. Through breast milk
Q: What is the immediate skin reaction used in allergy diagnostics called?
A: Wheel and flare
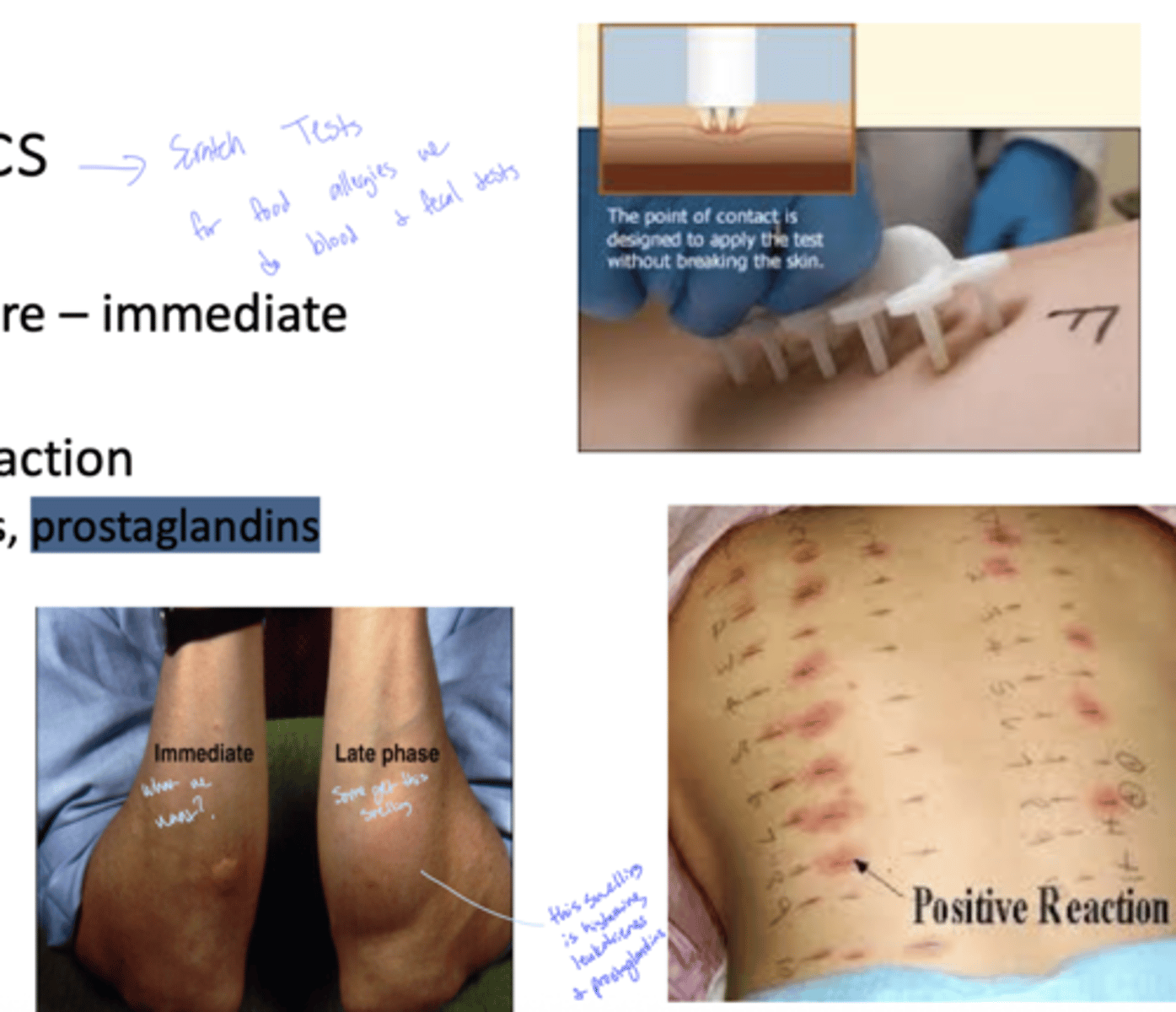
Q: Which molecule is primarily responsible for the immediate wheel and flare reaction?
A: Histamine
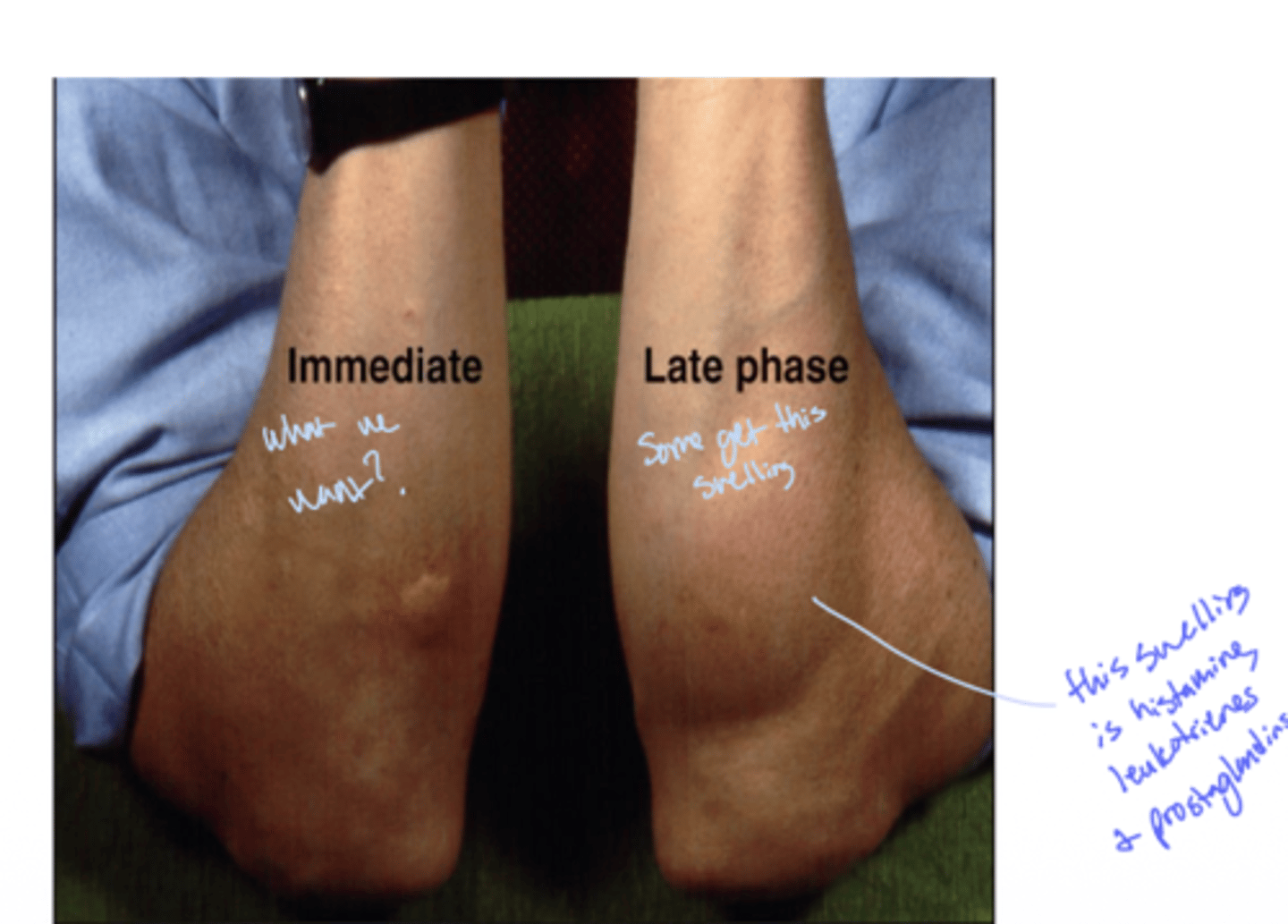
Q: What is the reaction called that occurs hours after the initial allergic response?
A: Late-phase reaction
see how the late phase is histamine, leukotrienes and prostaglandins
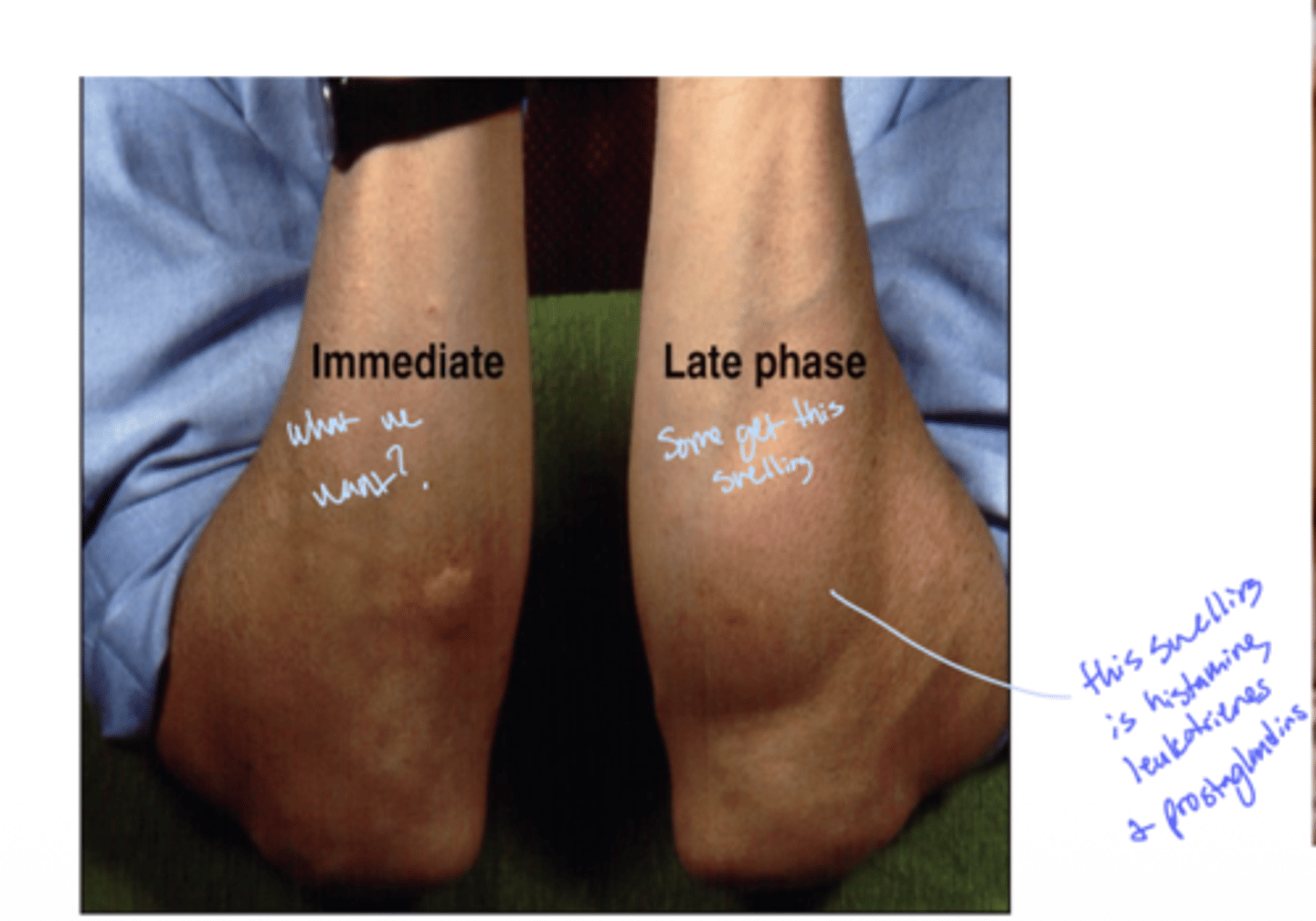
Q: Which molecules are associated with the late-phase reaction in allergies?
A: Leukotrienes and prostaglandins
Q: What are the main approaches to allergy therapy?
A: Prevention, pharmacological treatment, and desensitization
Q: Name two common pharmacological treatments for allergies.
A: Anti-histamines and corticosteroids
more preventative
Q: What is Omalizumab and what does it target?
A: An anti-IgE antibody
this is monoclonal antibody therapy, it can prevent mast cells from occuring and blocks eosinophils reaction
Q: What is Mepolizumab and what does it target?
A: An anti-IL5 antibody that targets eosinophils
Q: What is desensitization therapy commonly called?
A: "Allergy shots"
-this should decrease the sensitivity of IgE
-will NOT get rid of allergens
-this is done by putting very minor antigens right under the skin for IgE to respons, we want to avoid mast cells if possible.
Q: What happens to IgE during desensitization therapy?
A: IgE is converted to IgG4
Q: How does IgG4 help in desensitization therapy?
A: It forms complexes with the antigen but does not activate effector cells
Q: What is the most common allergic condition affecting the nose and eyes?
A: Allergic rhinitis (sneezing) and conjunctivitis(eyes)
-hay fever
Q: Which cells in the nasal mucosa are mainly involved in allergic rhinitis?
A: Mast cells
Q: What do mast cells release during allergic rhinitis?
A: Histamine
Q: What happens in the nose and eyes due to histamine release?
A: Fluid leakage, mucous discharge, and localized edema
Q: What complications can result from the swelling in allergic rhinitis?
A: Blocked sinuses and Eustachian tubes (inner ear)