breast and female GU review
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
glandular tissue
15–20 lobes of mammary glands
drains
lactiferous duct → lactiferous sinus → nipple
cooper ligaments
Suspensory ligaments tethering breast to skin & chest wall
tumor infiltration = SKIN DIMPLING
areola
Pigmented ring around nipple
contains Montgomery glands (keep nipple supple)
tail of spence
Axillary extension of breast tissue
UOQ
Upper Outer Quadrant
contains MOST glandular tissue = site of ~60% of breast carcinomas
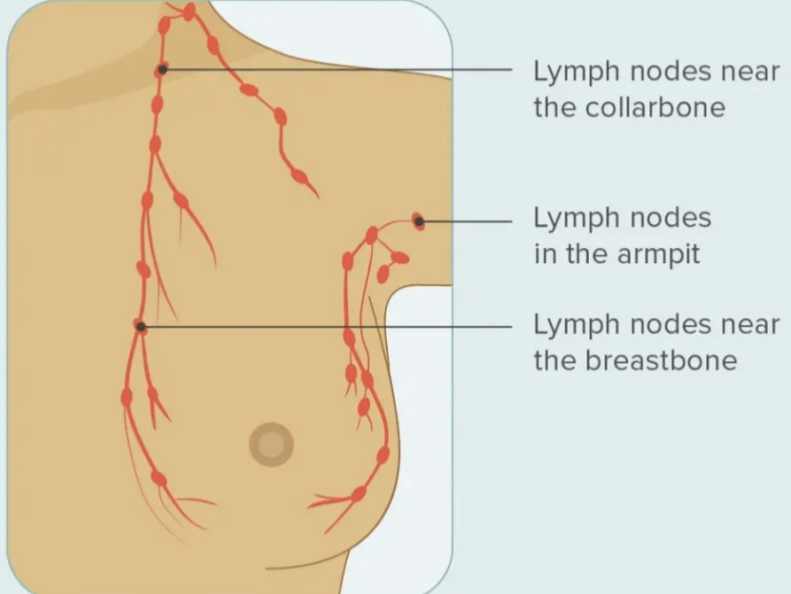
axillary lymph nodes
75% of breast lymph drainage
anterior
posterior
lateral
central
apical nodes

thelarche
breast bud
tanner stage 2
first sign of puberty
menarche
1st period
follows 2-3 years later
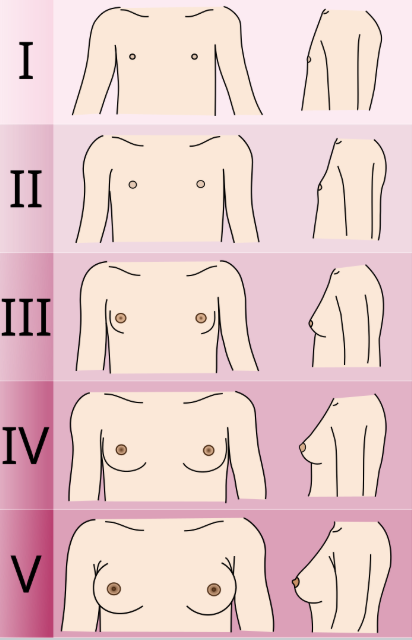
tanner stage
stage 1
prepubertal
Flat
no palpable breast tissue
stage 2
breast bud (thelarche)
Elevation of papilla + areola
avg age 8–13
stage 3
enlargement
Breast & areola enlarge together
often asymmetric
stage 4
Areola & papilla project ABOVE breast
double-mound appearance
stage 5
Areola recedes to breast contour
papilla projects
mature adult breast
infant breast change
transient enlargement from maternal estrogen
witch milk possible
resolve in weeks
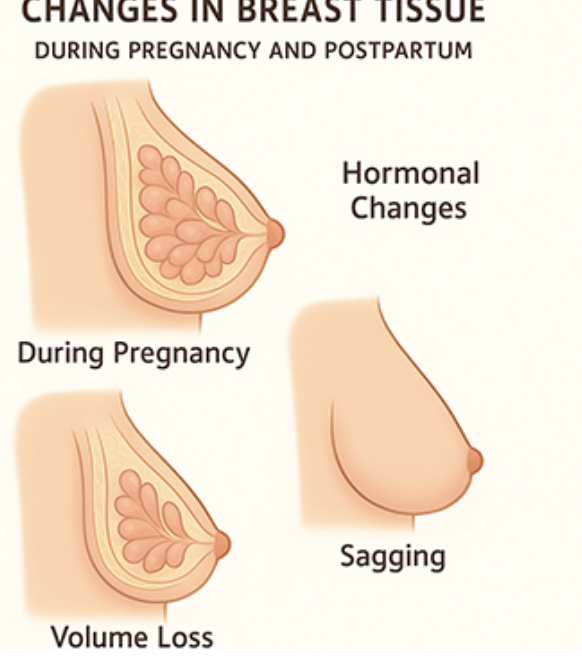
pregnancy breast change
enlarge vein, visible
nipple/areola darken
colostrum
montgomery gland prominent
lactation breast change
maximal enlarged/firm
milk production
nipple tender/cracked
menopause/aging breast change
glandular tissue replaced…
fat
lobule atrophy
breast sag
nipple small/prominent
breast cancer risk factors
increasing age
Female sex
Family history of breast cancer
BRCA1, BRCA2, PALB2, TP53 mutations
Personal history of breast cancer
Dense breast tissue (mammographically)
Prior chest radiation (e.g., Hodgkin Tx)
Early menarche (<11 y)
Nulliparity / First pregnancy after age 30
Never breastfed
Obesity (especially postmenopausal)
Alcohol consumption
Physical inactivity
Combined HRT (estrogen + progesterone)
Recent hormonal contraceptive use
Weight gain in adulthood
Type 2 diabetes
High endogenous estrogen (postmenopausal)
Proliferative breast disease with atypia
protective factor of breast cancer
breastfeeding
warning signs of breast cancer
painless lump/thick
skin dimpling/puckering
nipple retraction
nipple discharge
redness/scaliness skin
change size/shape breast
enlarged lymph nodes
persistent breast pain
clinical breast exam inspection
pt seated/supine
› Arms relaxed at sides → baseline symmetry & skin
› Arms pressed on hips → contracts pectoralis → reveals dimpling
› Arms raised above head → elevates breast; reveals tethering
› Lean forward (large breasts) → hangs freely; check symmetry
notings of breast exam
inspect for: asymmetry, contour changes, skin color
look for: edema (peau d'orange), dimpling, puckering
check: nipple position, retraction, discharge, skin changes
note: visible masses, axillary fullness, erythema
palpate BSE
3 middle fingers with finger pads — dime-sized circular motions
pressure levels at EACH spot: Light → Medium → Deep (to chest wall)
Systematic pattern — vertical strip (lawnmower), concentric circles, or wedge
Cover ENTIRE breast including Tail of Spence — sternum to mid-axilla, clavicle to inframammary ridge
Patient SUPINE with small pillow under ipsilateral shoulder
lump found: document
location - quadrant + clock position
size - cm x 3 dimension
shape - round, oval, irregular
consistency - soft, firm, hard, rubbery
mobility - freely movable vs fixed
tenderness - present or absent
BSE: menstruating women
5–7 days AFTER start of period
breasts least tender & swollen
BSE: pregnant/menopausal
Same day each month (e.g., 1st of month)
monthly, consistent date
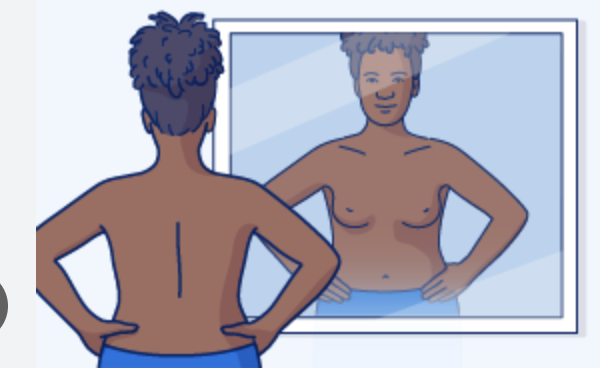
BSE: mirror inspection
Arms at sides → hands on hips → arms raised
look for asymmetry, dimpling, nipple changes
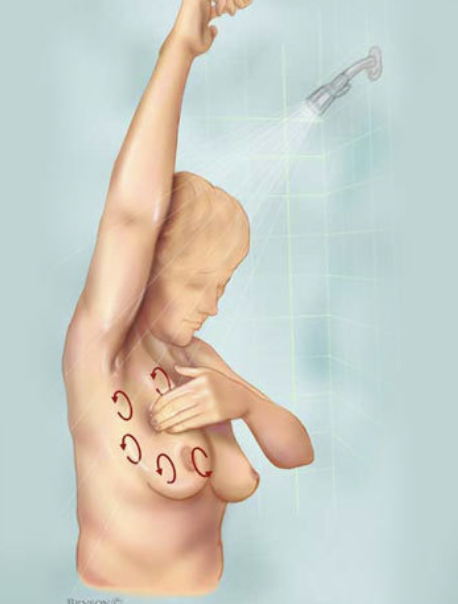
BSE: shower
Soapy skin makes lumps easier to detect
palpate with flat fingers
BSE: supine
Arm raised above head on side being examined
pillow under shoulder
3-finger dime-sized circles
BSE: nipple check
Gently squeeze each nipple
note any discharge
color, consistency, unilateral?
BSE: methods
Vertical strip (lawnmower)
Concentric circles
Wedge
choose ONE, stay consistent
screenings: avg women risk
40-44 → OPTION to begin annual mammogram (shared decision-making with provider)
45-54 → Annual mammogram RECOMMENDED
55+ → May switch to every 2 years OR continue annually; continue while healthy & life expectancy ≥10 yrs
all women → Know your normal! Report breast changes to provider immediately
screenings: high risk women
18+ → Breast self-awareness education begins
25+ → CBE every 6–12 months
25-29 → Annual breast MRI with & without contrast
30-75 → Annual mammogram PLUS annual breast MRI with & without contrast
male → BSE education age 35+; CBE annually age 35+; consider annual mammogram starting age 50
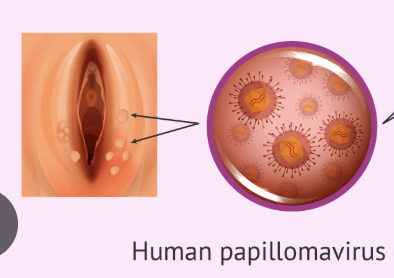
HPV
cervical cancer
type 16/18
risk factor
HPV infection — high-risk strains 16, 18, 31, 33, 45
Early sexual debut
Multiple sexual partners
Smoking
immunosuppression (HIV, transplant meds)
Other STIs (chlamydia, HSV-2)
Long-term OCP use (slight increase)
No HPV vaccination
Missed Pap screenings
AA/Hispanic — higher incidence
Pap smear
< 21 → No screening — regardless of sexual activity
21-29 → Pap smear ALONE every 3 years (no HPV test)
30-65 → PREFERRED: Pap + HPV co-test every 5 years Acceptable: Pap alone q3y OR HPV alone q5y
65+ → DISCONTINUE if adequate prior screening history
post-hysterectomy → Discontinue if no cervix & no history of CIN 2+
HPV vaccine
Protects against HPV types
6, 11, 16, 18, 31, 33, 45, 52, 58
Recommended:
age 11–12 (can start at 9)
catch-up through age 26
2-dose series
<15 y3-dose
3-dose series
≥15 y or immunocompromised
Does NOT replace Pap screening — vaccinated women still need Paps
chlamydia
asymptomatic
S/S
mucopurulent cervical
discharge
cervical friability
pelvic pain
dysuria
diagnose: urine/vagina/cervical swab
treat: doxycycline
gonorrhea
Mucopurulent discharge
dysuria
pelvic pain
often
co-infects with chlamydia
frequently asymptomatic in women
diagnose: culture resistance
treat: ceftriaxone
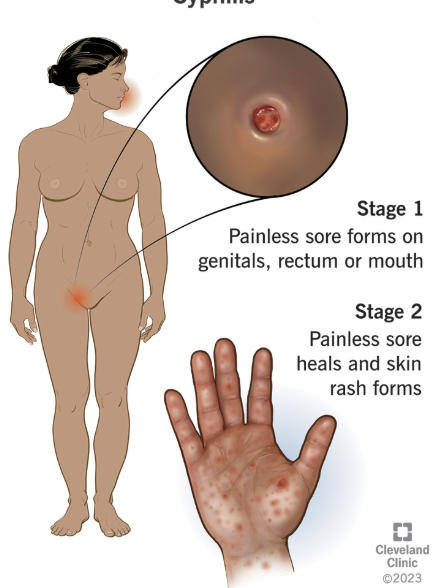
syphilis
Primary: painless chancre
Secondary: rash palms/soles, condyloma lata
Latent: asymptomatic
Tertiary: gummas, CV, neuro
treat: benzathine penicillin G
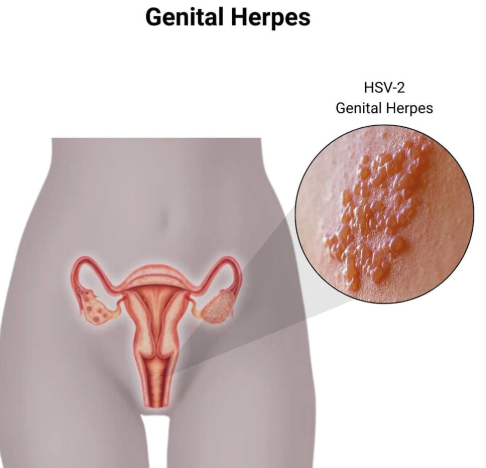
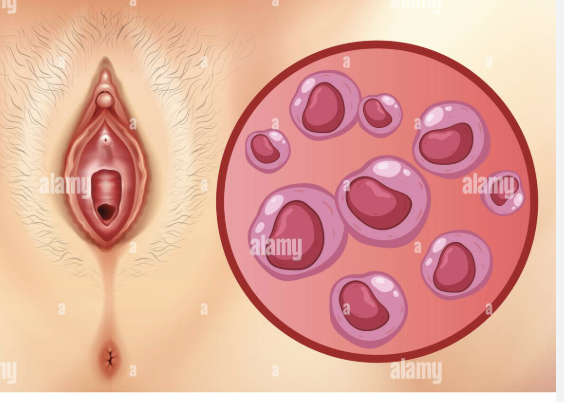
herpes HSV 1/2
Painful vesicles/ulcers genitalia
primary: fever,lymphadenopathy
recurrent less severe; asymptomatic
shedding
treat: acyclovir or valacyclovir
HPV
genital warts
asymptomatic
high risk → cervical/anal/oral cancer
diagnose: Papsmear/HPV test
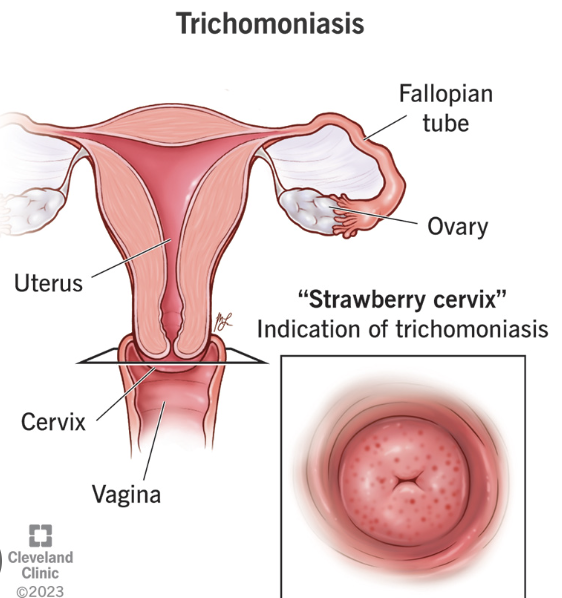
trichomonas
Frothy yellow-green discharge
pruritus → itch skin
dyspareunia → genital pain
strawberry cervix
up to 70% asymptomatic
bacterial vaginosis
Thin gray-white discharge
fishy odor (especially after sex)
vaginal itching
pH >4.5
diagnose: Whiff test +; clue cells; pH >4.5; Amsel criteria (3 of 4)