kale PUD
1/85
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
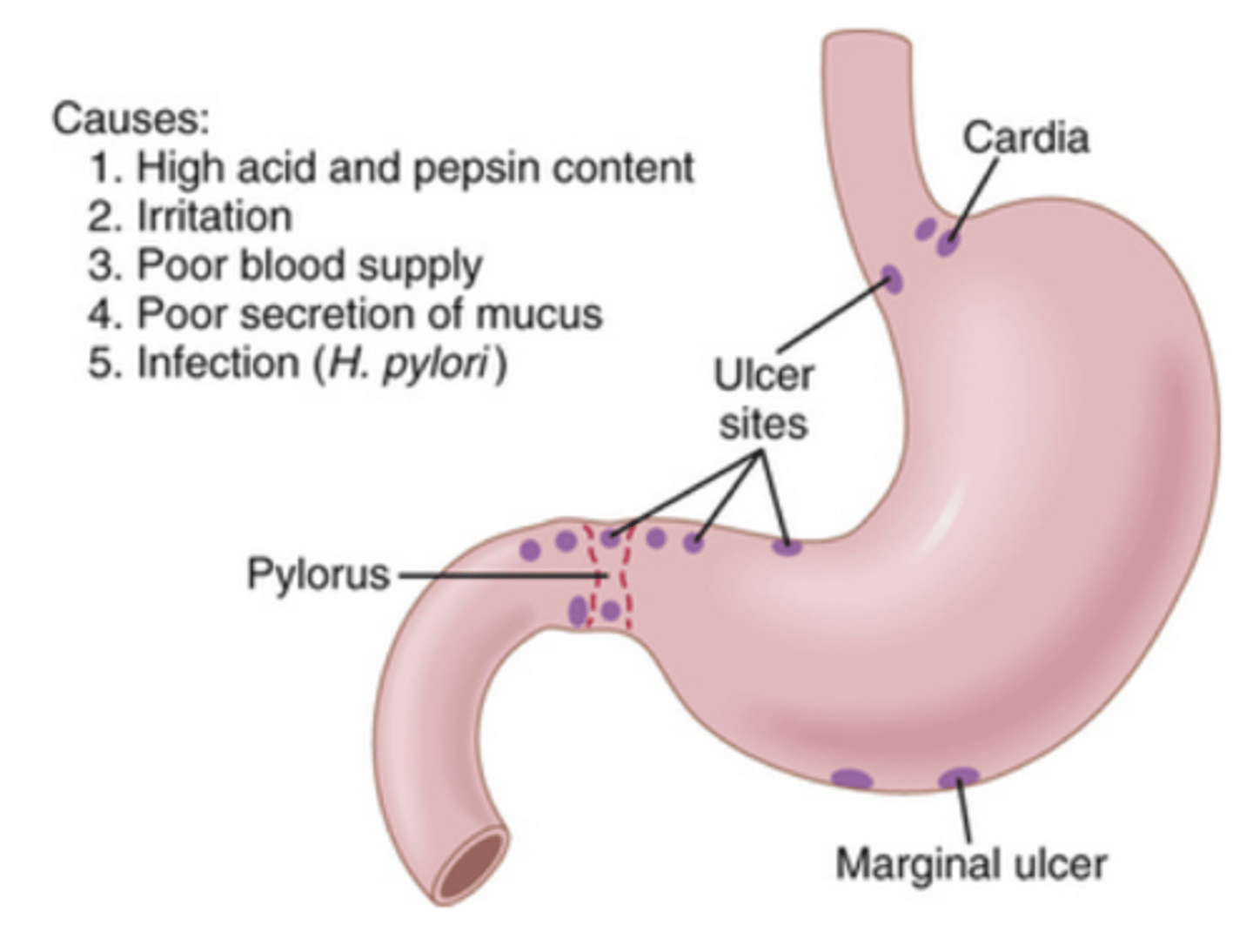
what are peptic ulcers
open sores created on the digestive system epithelium, due to inadequate mucus protection --> acid corrosion
1. duodenal
2. gastric= antrum of stomach
have ulcer rates been increasing or decreasing
duodenal ulcers: overall decline
gastric ulcers: less dramatic decline (aging pop, increased NSAID use)
-> women mortality rate INCREASING
-> men mortality rate DECREASING
describe 4 regions of stomach and 4 secreting cells
cardia, fundus, body, pylorus
1. parietal cells: HCl
2. chief cells: pepsinogen
3. mast cells: histamine
4. G cells: gastrin
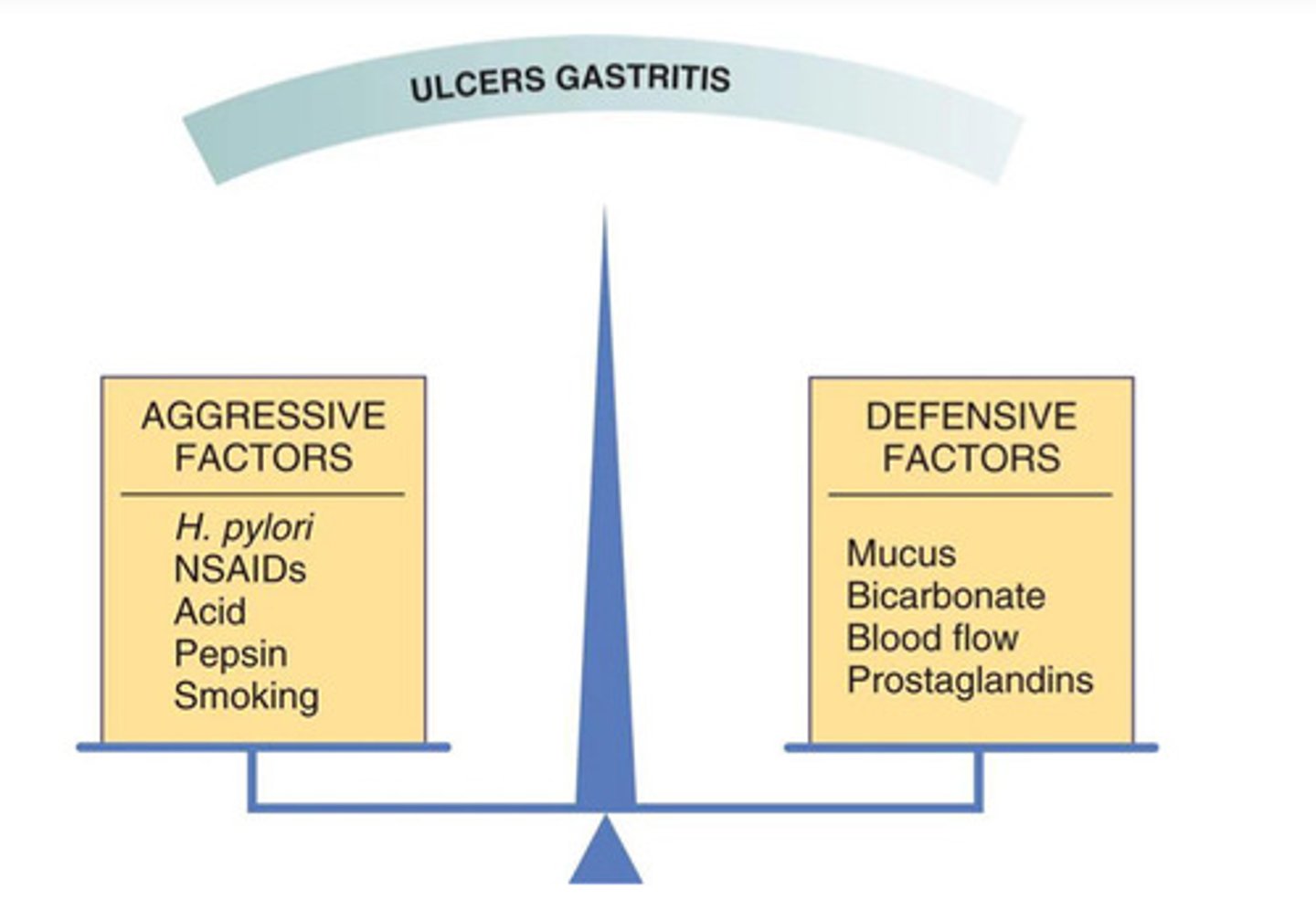
pathogenesis of peptic ulcers
aggressive vs defensive factors
aggressive: acid, pepsin, gastrin, bile acid
defensive: mucosal blood flow, bicarb, cellular regeneration, prostaglandins
(remember prostaglandins were actually aggressive factor in GERD bc lower LES pressure!!)
where are drug induced peptic ulcers more likely to occur (stomach vs duodenum)? which drugs?
gastric
drugs: NSAIDs, adrenocorticosteroids, chemo
where are infection-induced ulcers more likely to occur (gastric or duodenal)? which organisms?
duodenal
H. pylori, CMV
RISK FACTORS FOR PUD
(not direct causes)
1. cigarette smoking= decreased response to H2RAs, ulcer reoccurrence
2. alcohol: mucosal irritant, bleeding
3. caffeine: gastric acid stimulant, dyspepsia
4. spicy food: dyspepsia
5. stress: ulcer pain and disability, induces behavior risks (smoking)
how does epigastric pain present in PUD
- usually nocturnal
- DU: episodic and clusters
- pain may radiate to back
antacids provide relief
food might relieve or increase pain
what effect can PUD have on bp/hr/hgb/hct
bleeding causes decreased intravasc volume
- lower bp
- higher HR
- lower hgb/hct [<13/50% ish]
radiography dx
- uses barium and xray to see ulcer crater
- can result in false negative for small ulcers
esophago-gastro-duodeno-graphy (EGD)
- use endoscope to see GI mucosa directly
- MOST ACCURATE AND CONCLUSIVE. not gold standard tho (histology)
what is the most accurate diagnostic test for PUD? gold standard?
most accurate=
esophago-gastro-duodeno-graphy (EGD)
gold standard= histology/ microbio examination for H/ pylori
histology dx for PUD
GOLD STANDARD
-microbio examination for various strains
- patchy distribution of HP results in false negatives
a __________ diagnostic tool is used to test for antibiotic resistance
culture
urease (biopsy)
CLO test
campylobacter-like organism test (CLO test)/ urease biopsy
TEST OF CHOICE DURING ENDOSCOPY
-rapid screening test to detect the presence of the bacterium Helicobacter pylori
- HP ammonia causes a color change= rapid results show active infection
t/f: a CLO test/ urease biopsy only shows an inactive infection
false. it shows active infection bc HP produce ammonia which leads to color change
what is the test of choice for H. pylori during endoscopy
urease (biopsy)
CLO test
dx tests:
_________= gold standard
________= most accurate and conclusive
__________= test of choice at endoscopy; H. pylori active infection
_________= test to confirm HP eradication [non endoscopic]
histology= gold standard
EGD= most accurate and conclusive
urease (biopsy)= test of choice at endoscopy; H. pylori active infection
urea breath test= test to confirm HP eradication
which test can be used to confirm HP eradication? describe what it entails
urea breath test (non-endoscopic)
- ingest urea with labeled carbon: C13 nonradioactive or C14 radioactive
- HP produces urease which will break down the urea, and you will find labeled C in breath via CO2
no bacteria= no labeled C in breath
which non-endoscopic technique can be used to tests for the presence of HP but will NOT differentiate btwn an active or inactive infection
serology= tests for Igs against HP [will be in blood for 6-12months]
what is shock
drop in bp <90 systolic
chronic complications of PUD
- GI bleeding (melena, hematemesis, shock)
- perforation (ulcer eroded through lining)
- gastric outlet obstruction (scarring of pylorus)
- gastric cancer (NOT direct complication)
t/f: gastric cancer is a direct complication of PUD
false
H. pylori characteristics
gram neg spiral
flagella
acid labile!!! needs pH>4 to survive
secretes urease to form NH3 and CO2 from acid
class 1 carcinogen
infects gastric antrum and is carried into duodenum via peristalsis
t/f: H. pylori primarily infects the duodenum
false. infects gastric antrum and is carried into duodenum via peristalsis. most duodenal ulcers are H. pylori cases
non-pharm measures for HP PUD
1. avoid irritating foods (spicy, fried)
2. avoid caffeine and alcohol
3. stop smoking
4. stress management
what were old 2017 guidelines for h. pylori PUD
MOC= metronidazole, omeprazole, clarithromycin
COA= clarithromycin, omeprazole, amoxicillin
for 14 days
levofloxacin triple therapy
levofloxacin 500mg qd, amoxicillin 1000mg bid, PPI bid for 10-14 days
not fda approved, and low quality of evidence
fluoroquinolone sequential therapy
PPI + amoxicillin for 5-7 days
then
PPI + fluoroquinolone + metronidazole for 5-7 days
low quality of evidence!!
fluoroquinolones
-floxacin
macrolide
-mycins
t/f: in 2024 guidelines, clarithromycin and levofloxacin (fluoroquinolone) is no longer first line
true. antibiotic resistance
optimized bismuth quadruple therapy
indication and dose
recommended first line for HP PUD
- used in pts with PCN allergy or macrolide exposure
PPI BID
Bismuth subsalicyate 300 or subcitrate 120-300 QID
tetracycline 500mg QID
metronidazole 500mg TID or QID
can pt with aspirin allergy be given optimized bismuth quadruple therapy
yes. switch bismuth subsalicylate 300mg to bismuth subcitrate 120-300mg
rifabutin triple therapy for tx naive
NOT FOR PCN ALLERGY (amoxicillin)
omeprazole 20-40mg BID
amoxicillin 1000mg BID
rifabutin 50-300mg QID
4 capsules TID of combo Talicia
vonoprazan dual therapy
vonoprazan 20mg BID
amoxicillin 1000mg TID [NOT FOR PCN ALLERGY]
for 14 days
vonoprazan triple therapy
vonoprazan 20mg BID
amoxicillin 1000mg BID [NOT FOR PCN ALLERGY]
clarithromycin 500mg BID
for 14 days
reserve for clarithromycin sensitive strains!
for treatment naive pts with H. pylori infection,
recommended first line?
2 alternates?
1. optimized bismuth quadruple
2. rifabutin triple
2. vonoprazan dual
2. vonoprazan triple
for a pt previously on PPI-clarithromycin triple or non-optimized BQT with persistent HP infection, what is next tx
-optimized BQT
- rifabutin triple
[high dose PPI or PCAB dual if above arent options]
for tx-experienced pts who underwent antibiotic susceptibility testing, what would you give for clarithromycin and levofloxacin-sensitive strains
- clarithromycin triple [omit if clarithromycin resistant]
- optimized BQT
- rifabutin triple
- levofloxacin triple [omit if levofloxacin resistant]
for tx-experienced pts who underwent antibiotic susceptibility testing, what would you give for clarithromycin and levofloxacin-resistant strains
- optimized BQT
- rifabutin triple
- high dose PPI or PCAB dual
for treatment-experienced pts with H. pylori infection,
what are 2024 tx options for no antibiotic sensitivity
- optimized bismuth quadruple
- rifabutin triple
possibly vonoprazan dual if above arent options
for treatment-experienced pts with H. pylori infection,
what are 2024 tx options for pts with proven antibiotic sensitivity
- optimized bismuth quadruple
- rifabutin triple
- vonoprazan triple (clarithro sensitive)
- levofloxacin triple (levo sensitive)
possibly vonoprazan dual if above arent options
what is the only possible tx regimen for HP PUD for those with penicillin allergy
optimized bismuth quadruple
rifabutin triple therapy for pts who have already tried BQT
PPI BID
amox 1000mg BID or TID
rifabutin 50-300mg QID
orrrrrrrr
combo Talicia 4 caps TID
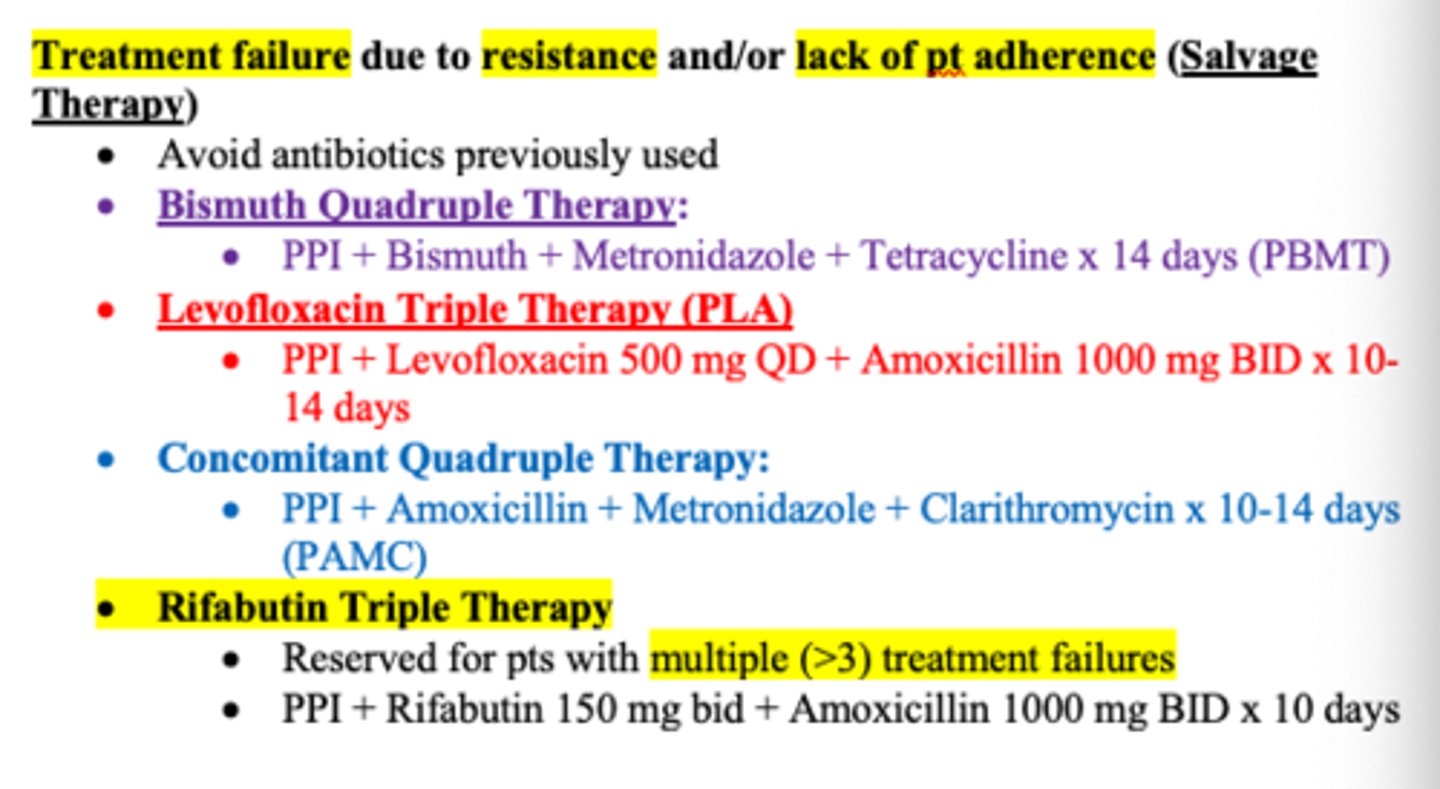
levofloxacin triple therapy for pts w known levofloxacin-sensitive HP and when BQT and rifabutin failed
PPI BID
Levofloxacin 500mg QD
amox 1000mg BID or metro 500mg BID
can you interchange antibiotics for HP PUD tx
no
can you interchange bismuth preparations for HP PUD tx
no
can you interchange PPIs and H2RAs in HP PUD tx
- may interchange PPIs
- may sub PPI in place of H2RA but u CANNOT use H2RA in place of a PPI
t/f: probiotics are a low cost alternative that may increase HP eradication rates
true
describe how NSAIDs correlate to erosions/ulcers
locally= direct damage to mucosa bc acidic
systemic= NSAIDs inhibit COX which is needed for prostaglandin synthesis (defensive factor)
COX 1 vs COX 2
COX1: protective PG that are always expressed (stomach, intestines, kidney, platelets)
COX2: stops PG at site of infalmmation
-> so using COX2 selective NSAIDs is less damaging
t/f: aspirin is more selective for COX2 than naproxen
false. naproxen is more selective for COX2, followed by ibuprofen, and then aspirin
celecoxib
Celebrex
NSAID that is selective for COX2
what did the VIGOR and APPROVE trials/studies determine regarding selective COX 2 inhibitors? CLASS trial?
less GI toxicity but higher chance of MIs
CLASS trial-> long term data showed no difference btwn celecoxib and other NSAIDs in rate of ulcer complications. so gastric effects still occur
t/f: typical PUD symptoms do NOT occur in NSAID ulcers
true. may have ASYMPTOMATIC bleeding and perforation
there is poor correlation btwn sx and endoscopic findings
RISK FACTORS FOR NSAID INDUCED GI TOXICITY
-Age >65
-previous peptic ulcers/ ulcer related complications
- high dose or a lot of NSAID use
- aspirin
- chronic disorders: cardiovasc, rheumatoid arthritis
- HP infection
- cigs and alcohol
DRUGS:
NSAID with aspirin, bisphosphonates, corticosteroids, anticoags, antiplatelets, SSRIs
the concomitant use of which drugs is a risk for NSAID induced GI toxicity
NSAID with low dose aspirin
bisphosphonates (alendronate)
corticosteroids
anticoags
antiplatelets
SSRIs
NSAID induced ulcers treatment
1. stop NSAID-> give H2RA or PPI
2. if cant stop-> give PPI
strategies to minimize NSAID injury
- take w food/antacid
- enteric coated aspirin
- use tylenol
misoprostol
moa
dose
prostaglandin analog used to prevent NSAID-induced DU and GU
MOA: enhances mucus, bicarb, and blood flow. some antisecretory
dose: 200mcg QID w food
misoprostol CIs
1. PREGNANT
- stimulates uterus== abortions
2. Mg coated antacids
- increases diarrhea and cramps
tx used to prevent NSAID ulcers
1. misoprostol (prostaglandin analog)
2. concomitant PPIs
t/f: PPIs are superior to H2RAs in preventing NSAID induced ulcers
true
how should the following pts be treated according to GI risk [over 60, use of asp/steroids/antiplatelet and coag/ SSRIs]
and CV risk [CV, diabetes]
(summary)
low GI and low CV: nonselective NSAID
high GI and low CV: nonselective NSAID and PPI [may sub for celecoxib if hx of ulcer]
low GI and high CV: naproxen
[ if on aspirin then naproxen + PPI]
high GI and high CV:
1. avoid NSAIDs
2. naproxen + PPI
3. celecoxib + asp + PPI
what NSAID is recommended if pt has high CV risk
naproxen
(can add PPI if taking aspirin or has high GI risk)
-> low CV risk, give nonselective NSAID
t/f: naproxen is preferred over non-selective COX2 inhibitors in CV
true
omeprazole and esomeprazole inhibit CYP_____ and affects these meds:
CYP2C19
phenytoin, warfarin, carbamazepine, diazepam [increases effect]
clopidogrel [attenuates/decreases]
which antiviral can PPIs reduce and why
atazanavir-> pH dependant
risk of rebleeding
- over 65yo
- shock (BP <90)
- poor overall health
- initial low Hb
- melena/ emesis
- transfusion requirement
why is acid suppressant therapy recommended with NSAIDs for high GI risk pts? optimal pH?
pepsin inhibits clot formation
gastrin impairs ulcer healing
platelets aggregate at pH 7.4
impaired at pH <6!!
t/f: tolerance only occurs with H2RAs and NOT PPIs (need more of med over time)
true
dosing of PPI for bleeding peptic ulcers
pantoprazole or esomeprazole 80mg IV bolus then 8mg/hr
PPIs are formulated to be released when pH is
pH is above 7 (intestine)
exposure to gastric acid degrades the PPI
PPIs can lower absorption of drugs such as ______ by increasing gastric pH
ketoconazole, itraconazole, cefpodoxime proxetil
FDA warning for PPIs
1. increases risk of fractures of hip, wrist, and spine
- pts at risk of osteoporosis should take VItD/ Ca supplement
- monitor bone status
2. C. diff diarrhea
3. pneumonia
t/f: both H2RAs and PPIs are associated with pneumonia risk
true
t/f: vonoprazan therapies are at least as effective as PPI-based therapies, and can be given to pts on drugs metabolized by CYP2C19 or those who failed on PPI
true
what is sucralfate approved for
tx of acute and maintenance DU
[NOT approved for GU or NSAID GI injury]
sucralfate moa
aluminum salt that binds to ulcers forming a protective barrier, inhibits pepsin's actions, stimulates PGs
sucralfate dosing for active DU and maintenance
active: 1gm QID or 2gm BID for 4-8 weeks
maintain: 1gm BID
take on empty stomach!!! can bind to protein and phosphates in diet
sucralfate ADEs
constipation, hypophosphatemia, increased Al concentrations in renal impairment
which drugs should be taken 2hrs before sucralfate
- tetracycline
- digoxin
- theophylline
- fluoroquinolones (floxacin)
abx tolerability
all:
drug interactions:
pregnancy:
children:
other:
all: diarrhea, c. diff colitis, hypersensitivity
unpleasant taste: metro and clarithro
drug intrxns: metro and clarithro
AVOID in pregnant: clarithro and TCN
AVOID in children: TCN
t/f: tetracyclines, macrolides, and fluoroquinolones are known for QT prolongation
false. macrolides (mycins) and fluoroquinolones (floxacins) yes. not tetracyclines