Diagnosis and treatment of necrotising periodontal disease
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
necrotising gingivitis
Painful bleeding gums, ulceration and necrosis of interdental papilla - punched out appearance

Necrotising periodontitis
gingivitis that progresses to attachment loss

Necrotising stomatitis
Progression of NP into tissue beyond the mucogingival junction characterizes necrotizing stomatitis - mostly in malnutrition and HIV infection - may result in denudation of the bone leading to osteitis and oro-antral fistulas
What are the symptoms of necrotising periodontal disease?
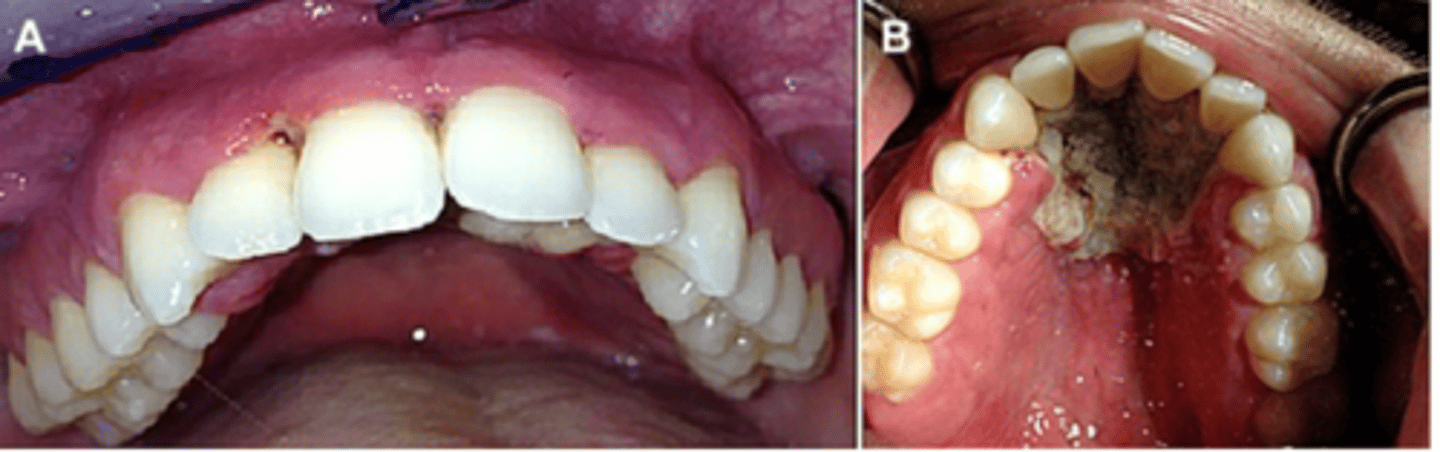
Ulcerated and necrotic papillae and the gingival margin resulting in a characteristic punched-out appearance.
What covers the ulcers in necrotising periodontal disease?
The ulcers are covered by a yellowish, white, or greyish slime, often misleadingly termed pseudo membrane.
What happens when the 'membrane' over the ulcers is removed in necrotising periodontal disease?
The underlying connective tissue becomes exposed and bleeds.
How quickly do lesions develop in necrotising periodontal disease?
Lesions develop quickly.
What is the level of pain associated with lesions in necrotising periodontal disease?
Lesions are very painful, causing severe pain.
What can provoke bleeding in necrotising periodontal disease?
Bleeding is readily provoked.
Where are the first lesions most often seen in necrotising periodontal disease?
The first lesions are most often seen interproximally in the mandibular anterior region.
What is a characteristic breath symptom of necrotising periodontal disease?
Halitosis
What is a key diagnostic feature of necrotising stomatitis?
Bone denudation extends through the alveolar mucosa.
What may occur in necrotising stomatitis besides bone denudation?
Larger bone sequestrates may occur.
What are the associated lesions in necrotising stomatitis?
Large areas of osteitis and oral-antral fistulae.
In which patients are lesions of necrotising stomatitis more severe?
Patients with severe systemic compromise, including those with AIDS, severe malnutrition, or after chemotherapy.
which diseases should NP be differentiated from
•Oral mucositis
•HIV-associate periodontitis
•Herpes simplex virus (HSV)
•Scurvy
•Gingivostomatitis
•Desquamative gingivitis
•Invasive fungal disease
•Illicit-drug related gingival disease
•Agranulocytosis
•Leukemia
•Chronic periodontitis
Risk factors of NP
in developed counties
- mostly young adults
- physiological stress
- sleep deprivation
- Immunosuppression
- poor OH
- Smoking
Developing countires
young malnourished children
Main objective of acute treatment
1)to arrest the disease process and tissue destruction;
2) to control the patient′s general feeling of discomfort and pain that is interfering with nutrition and oral hygiene practices
acute treatment phase 1
- Careful superficial debridement
- remove soft necrotic deposits
- debridement should be daily
- stage lasts 2 -4 days
- chlorhexidine based mouthwash
- Mechanical OH measures should be limited - like brushing directly
- including professional prophylaxis and/or scaling and root planing.
- Oral hygiene instructions and motivation should be enforced.
- Existing predisposing local factors, such as overhanging restorations, interdental open spaces and tooth malposition, should be carefully evaluated and treated
control of the systemic predisposing factors, including smoking, adequate sleep, reduction of stress, dietary advice ( vitamin supplementation) or treatment of involved systemic conditions.
corrective treatment of disease
The correction of the altered gingival topography caused by the disease should be considered because gingival craters may favour plaque accumulation and disease recurrence. Gingivectomy and/or gingivoplasty procedures may be helpful for treatment of superficial craters; periodontal flap surgery, or even regenerative surgery, are more suitable options for deep craters
Supportive or maintenance phase
the main goal is compliance with the oral hygiene practices and control of the predisposing factors.
HIV and NP
HIV-positive patients may not be aware of their serologic status. The occurrence of necrotizing periodontal disease in systemically healthy individuals without any predisposing factors in the background is suggestive of HIV infection and, therefore, the affected individuals should be screened for HIV.