NR118 Musculoskeletal Problems (Unit 5)
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
osteomylelitis
Severe infection of the bone, bone marrow, and surrounding soft tissue
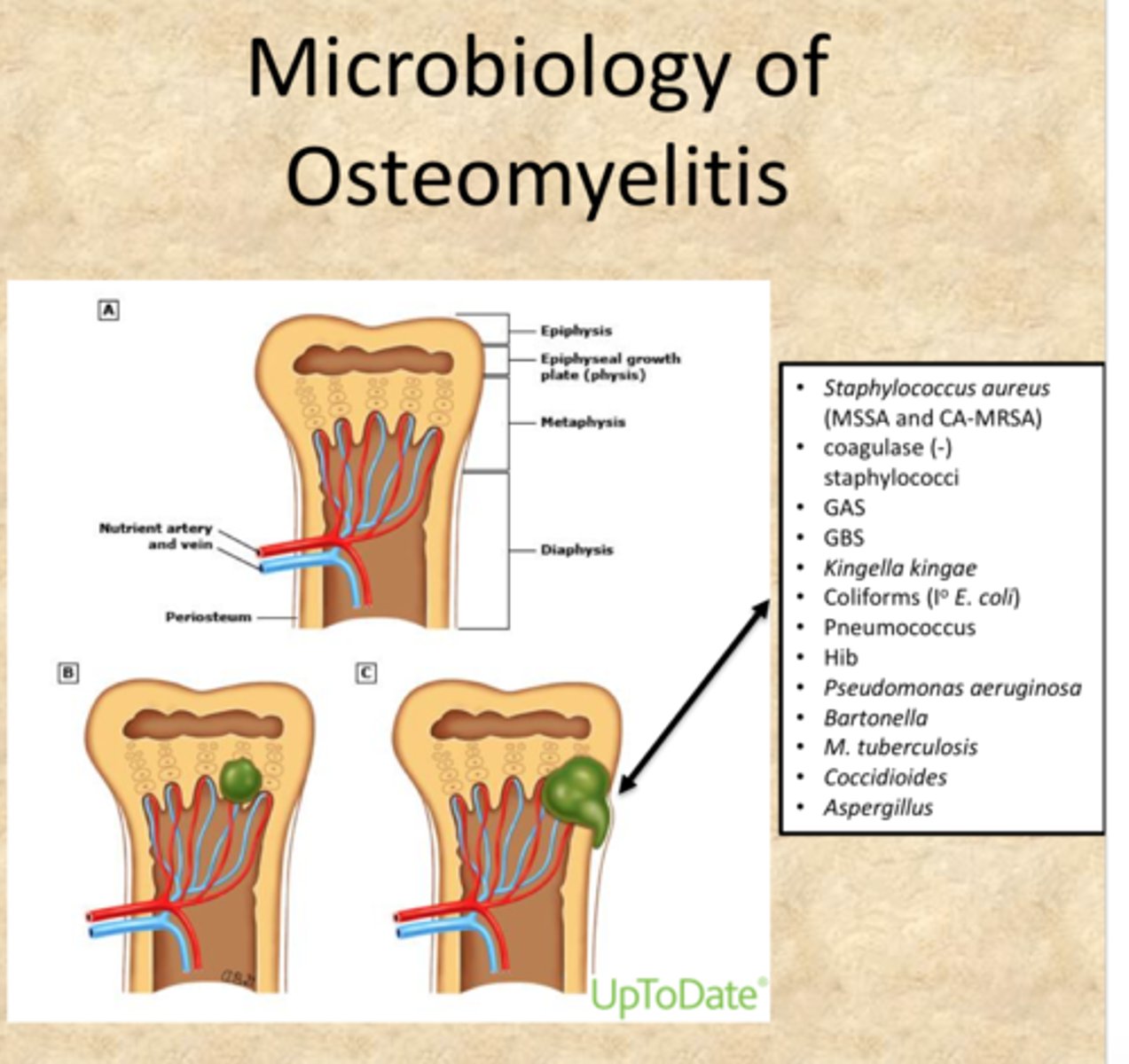
Most common cause of infection
Staphylococcus aureus.
• Microorganisms grow and pressure increases d/t non-expanding nature of bone
• Increased pressure leads to ischemia and vascular compromise of periosteum
• Infection spreads obstructing blood flow & causing necrosis
• Bone death occurs
Sequestrum
Area of dead bone separates from living bone.
• Antibiotics have difficult time reaching sequestrum
• Sequestrum needs surgical debridement or sinus tract develops and purulent drainage leaks out

S/s of acute osteomyelitis (less than 1 month)
• Bone pain that worsens with activity, unrelieved by rest, swelling, tenderness and warmth at infections site
• Systemic findings: fever, night sweats, chills, nausea, malaise
S/s chronic osteomyelitis (greater than 1 month)
• Infection did not respond to antibiotics
• Chronic pain
• Scar tissue may form and become further site for microorganisms
• Monitor for sepsis
Dx studies for osteomyelitis
• Bone or soft tissue biopsy
• Blood and wound cultures
• Usually don't appear on x-ray for 2 -4 weeks after initial symptoms
• Bone marrow edema can be found on MRI = early sign
Interprofessional care for osteomyelitis
• Aggressive, prolonged antibiotic therapy
• Surgical debridement for abscess or ulceration
• Possible acrylic bead chains containing antibiotics implanted
• Removal of orthopedic implant device if causative agent (hip/knee repair)
Nursing diagnoses/patient problems for osteomyelitis
• Acute Pain
• Impaired physical mobility
• Lack of knowledge
Planning for osteomyelitis
• Pain & fever management
• Complications associated are rare, but can be serious.
• Encourage adherence to the treatment plan.
• Facilitate a positive outlook on the outcome of the infection.
Health promotion for osteomyelitis
•Control of other infections (UTI, Pressure injuries)
•At risk patients = diabetes, orthopedic prosthetic implants, vascular insufficiency
•Contact PCP if patient experiences bone pain, fever, swelling, restricted limb movement
Acute care of osteomyelitis
• Immobilization of affected limb helps decrease pain & reduce further injury
• Dressings are used for drainage
• Teach patient about long term antibiotic use and side-effects: Diarrhea, blood in stools, mouth sores, hives, c-diff, thrush
Ambulatory care of osteomyelitis
• Long term antibiotic infusions
• Dressing changes
• Physical & psychological support
Benign bone tumors
Osteochondroma = overgrowth of cartilage & bone near end of bone at the growth plate
•Painless, hard, immobile mass
•One leg or arm longer than the other
•No treatment needed
Malignant bone tumors
• Sarcoma = malignant tumor that develops in bone, muscle, fat, nerve, or cartilage
• Osteosarcoma: Extremely aggressive primary bone cancer that spreads to distal sites. Gradual onset of pain and swelling in affected bone. Pain may be worse at night & increased activity
Metastatic bone cancer
• Occurs from metastasis from other sites (breast, colon, prostate, lungs, kidney, thyroid)
• Metastatic cells travel from primary tumor to bone via lymph & blood supply
• Pathological fractures common due to weakened bone
• High serum calcium occurs as damaged bones release calcium
Nursing management of bone cancer
• Monitor tumor site for swelling, changes in circulation, decreased movement/sensation or join function
• Prevent fractures
• Treatment for hypercalcemia if decalcification occurs
• Manage pain
• Radiation therapy for palliative care to help shrink tumor & decrease pain
• Assist with acceptance of prognosis
Muscular dystrophy
• Group of genetic disease characterized by progressive symmetric wasting of skeletal muscles without evidence of neurologic involvement
•Corticosteroid therapy = part of standard of care
Main treatment goals with muscular dystrophy
• Preserve mortality and independence through exercise, physical therapy, and use of assistive devices
• Prolonged bedrest should be avoided as immobility causes muscle wasting
• Teach ROM, nutrition, signs of disease progression
• Eventually leads to cardiac & respiratory cessation as muscles waste
Duchenne's Muscular Dystrophy
Progressive weakness & wasting of muscles.
Onset: 3-5 years old
Genetic: primarily males
-H/o motor development delay, clumsiness, frequent falls, difficulty climbing stares, running, & riding tricycle
-Waddling gait, ambulation frequently impossible by age 12
-Breathing muscles affected, life-threatening infections are common. Usually leads to death by age 15-18 years
Nursing considerations for Duchenne's muscular dystrophy
-Fatigue
-Mobility
-Frequent infections
-Psychological effects
-Maintain function
Localized low back pain
Pt feels soreness or discomfort when specific area of lower back palpated
Diffuse low back pain
Comes from deep tissue and larger area
Why is low back pain common?
• Lumbar region bears most of weight of body
• Most flexible region of spinal column
• Has nerve roots that are at risk for injury or disease
• Has a naturally poor biomechanical structure
Risk factors for low back pain
• Obesity, stress, lack of muscle tone, fracture of spine, family hx, jobs that require heavy lifting/vibration (jack hammer), and extended periods of sitting
Acute low back pain
• 4 weeks or less
• Often caused by trauma or hyper flexion on lower back (heavy lifting, sports injury, excessive yard work, MVC)
• Symptoms often develop 24 hours after injury occurred
Nursing implementation for low back pain
• Proper body mechanics
• Healthy body weight
• Stop smoking: tobacco impairs circulation to intervertebral discs causing low back pain
Acute care of low back pain
• NSAIDS and/or muscle relaxants (cyclobenzaprine)
• Avoid prolonged bedrest
• Hot/cold compresses
• Muscle stretching and strengthening
Ambulatory care of low back pain
• Make episode an isolated event
• Strengthening supporting muscles
Chronic low back pain
Last > 3 months or involves repeated incapacitating episode
Causes of low back pain
• Degenerative conditions (arthritis, disk disease)
• Osteoporosis
• Weakness from the scar tissue of prior injury
• Chronic strain on lower back muscles from obesity, pregnancy, or postures
• Congenital spine problems
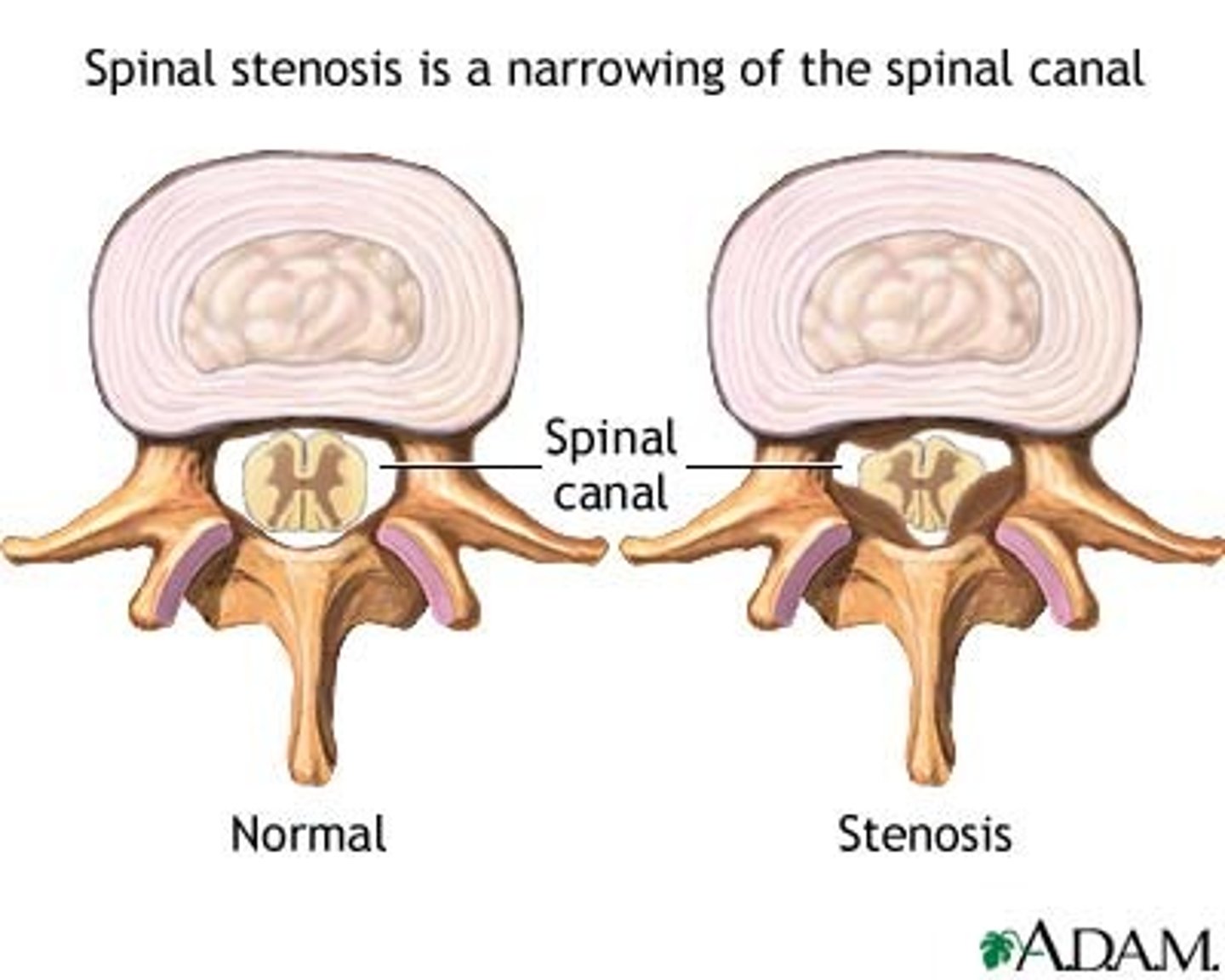
Spinal stenosis
• Narrowing of spinal canal
• Osteo or rheumatoid arthritis, spinal tumors, Paget's disease, traumatic damage to vertebral column, scoliosis
• Pain starts in lower back and radiates to buttock and leg & worsens with walking/sitting
• Decreased pain when pt bends is sign of stenosis
Degenerative disc disease (DDD)
• Loss of fluid in intervertebral discs with aging
• Discs lose elasticity, flexibility, shock-absorbing abilities, and thin
Herniated disc
Spinal disc bulges outward between vertebrae.
• May result from undistributed pressure with DDD
• Pain down buttock, below knee & along sciatic nerve
• May have saddle anesthesia
• Reflexes may or may not be present, numbness/tingling reported
Treatment for degenerative disc
• Limit spinal movement, NSAIDS, muscle relaxants, heat/ice application, transcutaneous electrical nerve stimulator (TENS), corticosteroid injections
• Teach good body mechanics, back-strengthening exercises
Surgical interventions for degenerative disc
• Intradiscal Electrothermoplasty
• Laminectomy
• Discectomy
• Spinal Fusion
• Disc replacement = Charite disc
Nursing management of disc surgery
• Maintain proper spinal alignment
• Logroll lumbar fusion patients, pillows for alignment and support
• Do NOT use bed trapeze for spinal pt
• Pain control
• Monitor for cerebrospinal fluid (CSF)leak: Headaches, notable leak (clear or slightly yellow), High glucose concentration
Nursing management of disc surgery (2)
• Monitor neuro status, especially peripheral sensation/movement
• Monitor for respiratory distress from spinal cord edema
• Report new muscle weakness or paresthesia immediately
• Monitor for incontinence or bowel problems as sphincter nerve impairment can occur
• Implement back braces as ordered/needed
• Assess surgical site and bone donor site
• Iliac crest = most common donor site
• Usually causes greater pain that incision site
Foot disorders
• Promote properly fitted shoes that conform to foot rather than current trends
• Trim toenails straight across
• Education for diabetics and foot care
Osteoporosis
• Chronic, progressive marked by low bone mass & deterioration of bone tissue, leading to increased bone fragility
• "silent thief" = robs skeleton of its banked resources
Why is osteoporosis more common in women?
• Lower calcium intake than men
• Less bone mass b/c smaller frames
• Bone resorption begins at earlier age & increases at menopause (decline in estrogen)
• Pregnancy & breastfeeding deplete skeletal reserve
• Longevity increases risk - women tend to live longer
S/s of osteoporosis
-Joint pain
-Low back pain
-Neck pain
-Backache
-A gradual loss of height and an accompanying stooped posture
-Fractures of the spine, wrist, or hip
Osteoporosis pathophysiology
• Peak bone mass (maximum bone tissue) achieved by age 20
• Determined by: heredity, nutrition, exercise & hormone function
• Bone remodeling = bone is continuously being deposited of osteoblasts & reabsorbed by osteoclasts
• Osteoblast = cell responsible for new bone formation
• Osteoclast = cell responsible for aged bone resorption
• Normally equal
• Osteoporosis: bone resorption exceeds bone deposition
Medications can interfere with bone metabolism
• Corticosteroids, anti-seizure drugs, heparin
• Educate patient on potential side effects of corticosteroids (major contributor)
Interventions for osteoporosis
• Care focused on proper nutrition, calcium & vitamin D supplements, exercise, prevention of falls/fractures, and medications
• Calcium intake 1000 mg/day for women and 1200 mg/day men
• Milk, yogurt, cottage cheese, ice cream, spinach, sardines
• Educate about importance of absorption so pt needs to take calcium pills in doses
• Hard for body to absorb doses greater than 500 mg in 1 setting
• Remain active to avoid bone loss: walking 30 min a day 3x/week
Paget's Disease
• Chronic skeletal bone disorder where excessive bone resorption is followed by replacement of normal marrow by vascular, fibrous connective tissue
• New bone is larger, disorganized, and weaker
• Causes may be viral or genetic
• Uncommon in people under age 40
• More common in men
S/s of paget's disease
• May present with waddling gait, bone pain, fatigue
• Patients report becoming shorter
• Pathologic fracture is most common complication & first sign of Paget's
What drugs are used to slow bone resorption
Bisphosphonate drugs
Nursing management of Paget's disease
• Educate about risk for falls: Poor lighting, area rugs, pets in home, clutter
• Keep patient as active as possible to slow demineralization of bone from disuse or extended immobilization
Rheumatoid arthritis (RA)
• Chronic, systemic autoimmune disorder characterized by inflammation of connective tissue in synovial joints
• Increased pain with repetitive movements
• Patients need rest and to rest affected areas
• Heat helps relieve joint stiffness and warm up tissues
• Corticosteroids reduce inflammation
• Monitor blood glucose levels
• Monitor effectiveness via labs
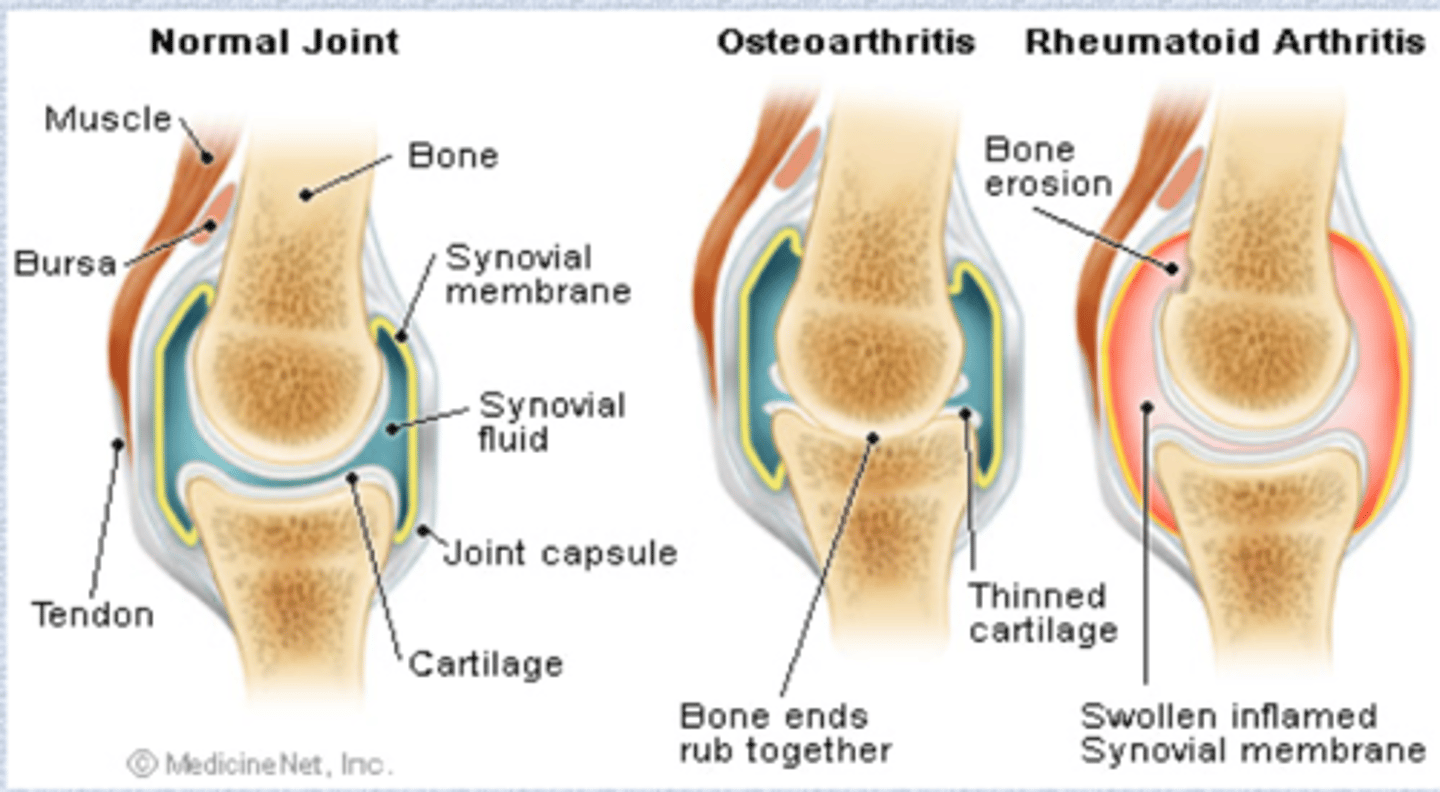
Osteoarthritis (OA)
• Slowly progressive non-inflammatory disorder of synovial joints
• More common in women
• Exacerbated with repetitive movements
• Joint pain is major symptom & reason patients seek help
• Occurs after periods of rest
• Difference from RA
Osteoarthritis vs. rheumatoid arthritis in the joint
Fibromyalgia syndrome (FMS)
• Chronic pain marked by musculoskeletal pain & fatigue with tender points
• Clinical manifestations: Tender areas, painful muscles, sleep disturbances, IBS
• Often take NSAIDs/pain medications