disorders of the musculoskeletal system - lecture 31
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
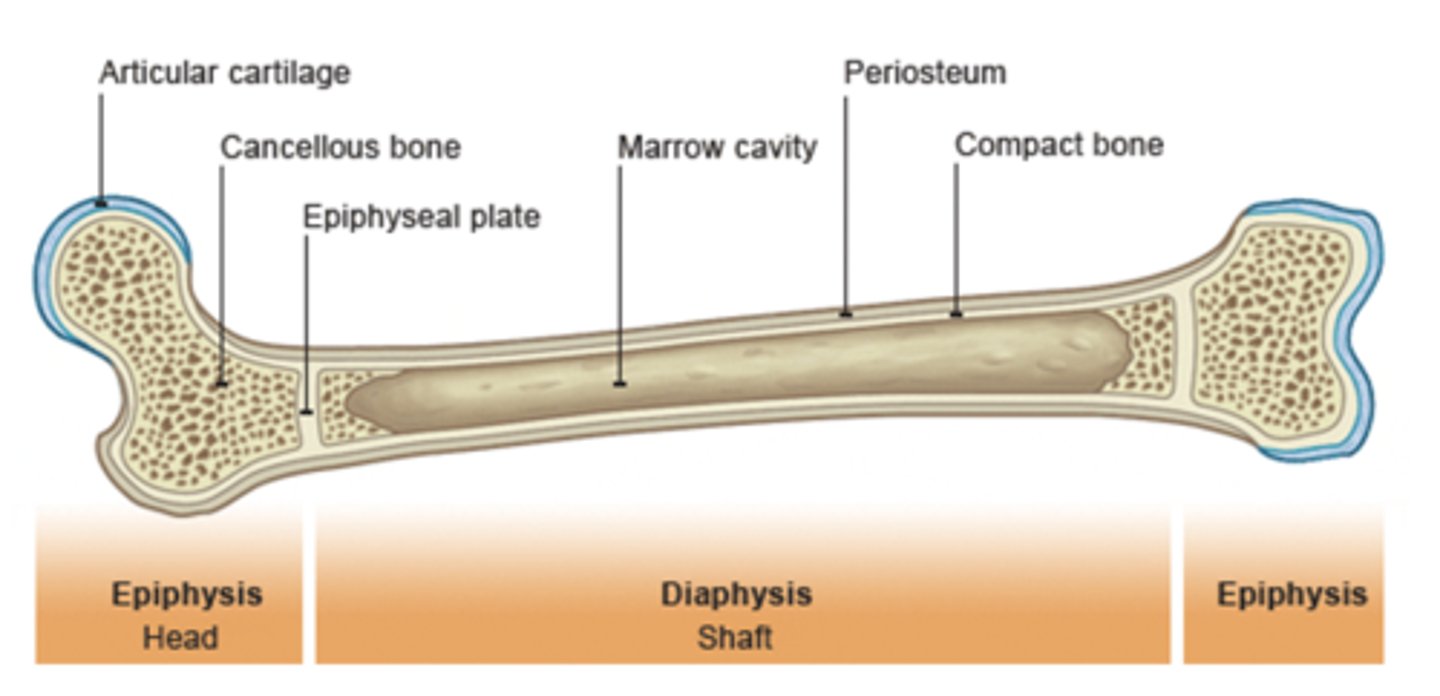
Structural Support
Bones give the body its shape and framework. They allow us to stand, sit, and move in complex ways by maintaining structural integrity.

Bone (Osseous) Tissue
Connective tissue that provides:
- Support/protection
- Levers for muscle
- Mineral storage
Bone is well ______________ (Implication for healing?)
- blood/oxygen/nutrients: this is why we need the bone to be vascularized
vascularized
organic - extracellular matrix
Collagen fibers (~90%)- tensile strength
Ground substance (proteins and polysaccharides)- support and adhesion
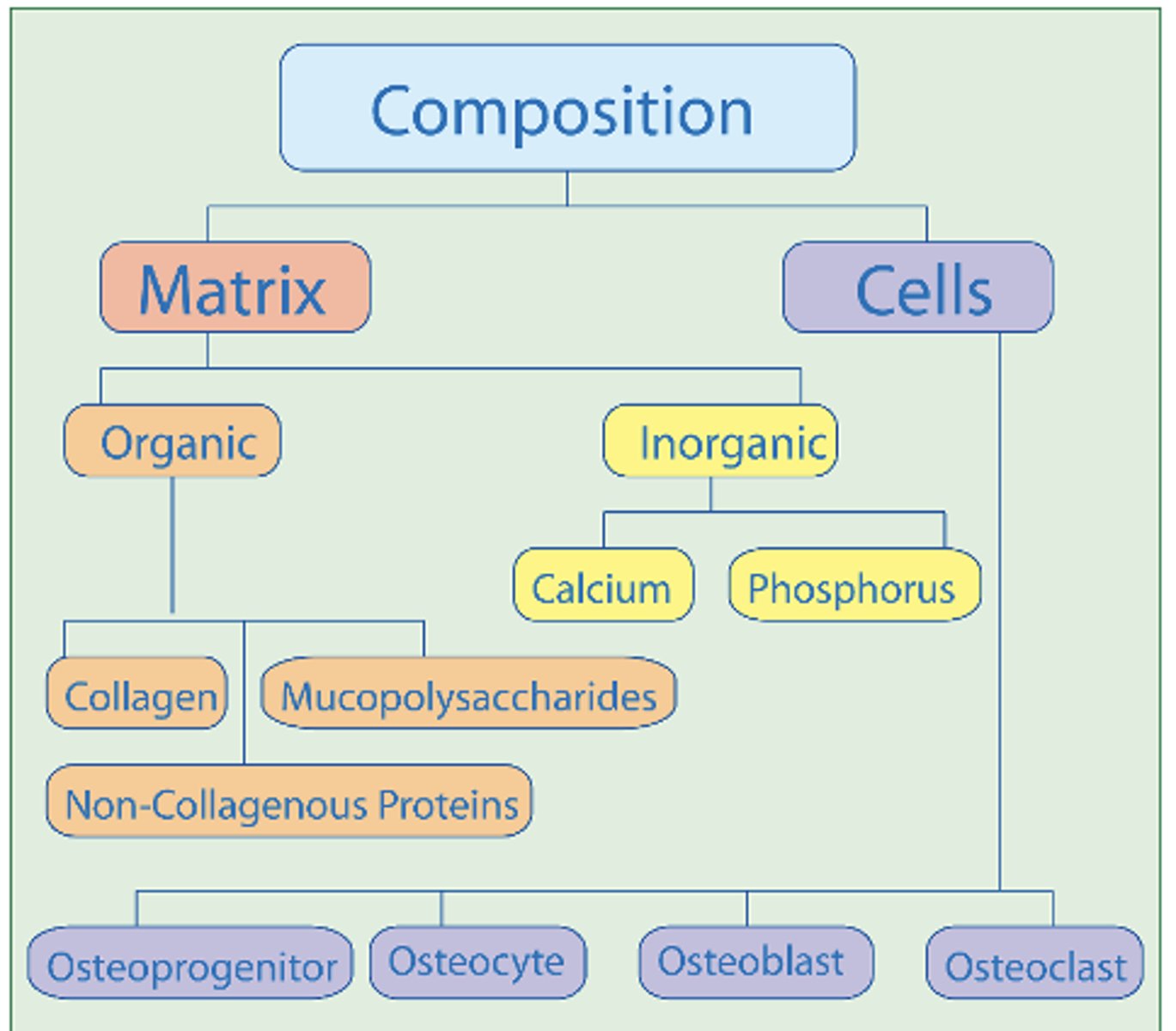
inorganic salts - extracellular matrix
Calcium and phosphate
25% of bone’s volume, but half of its weight
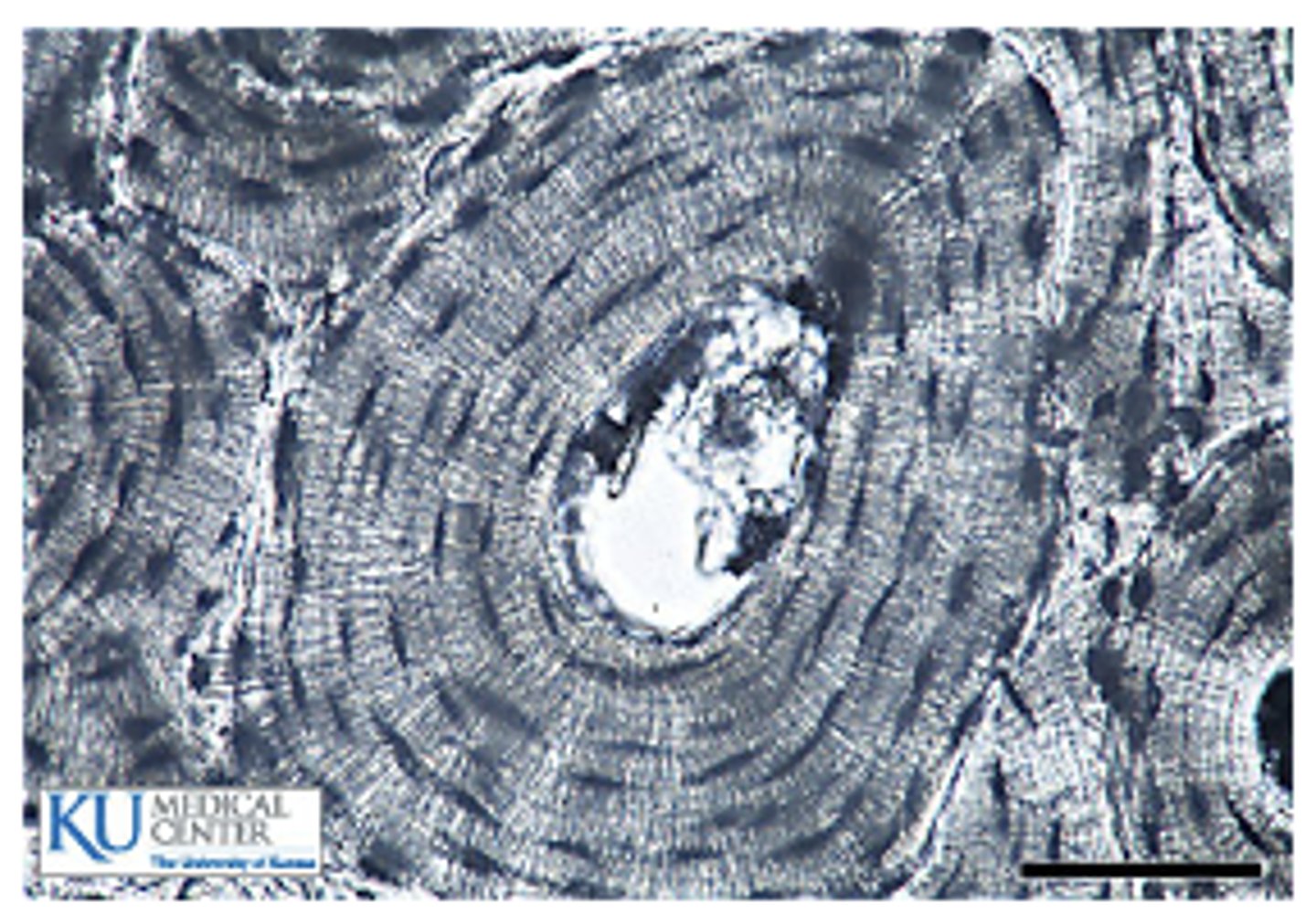
compact bone
Outer shell
Densely packed, calcified extracellular matrix (more rigid)
Functional Unit: Osteon
Bones contain ______ compact and spongy bone in different proportions
both
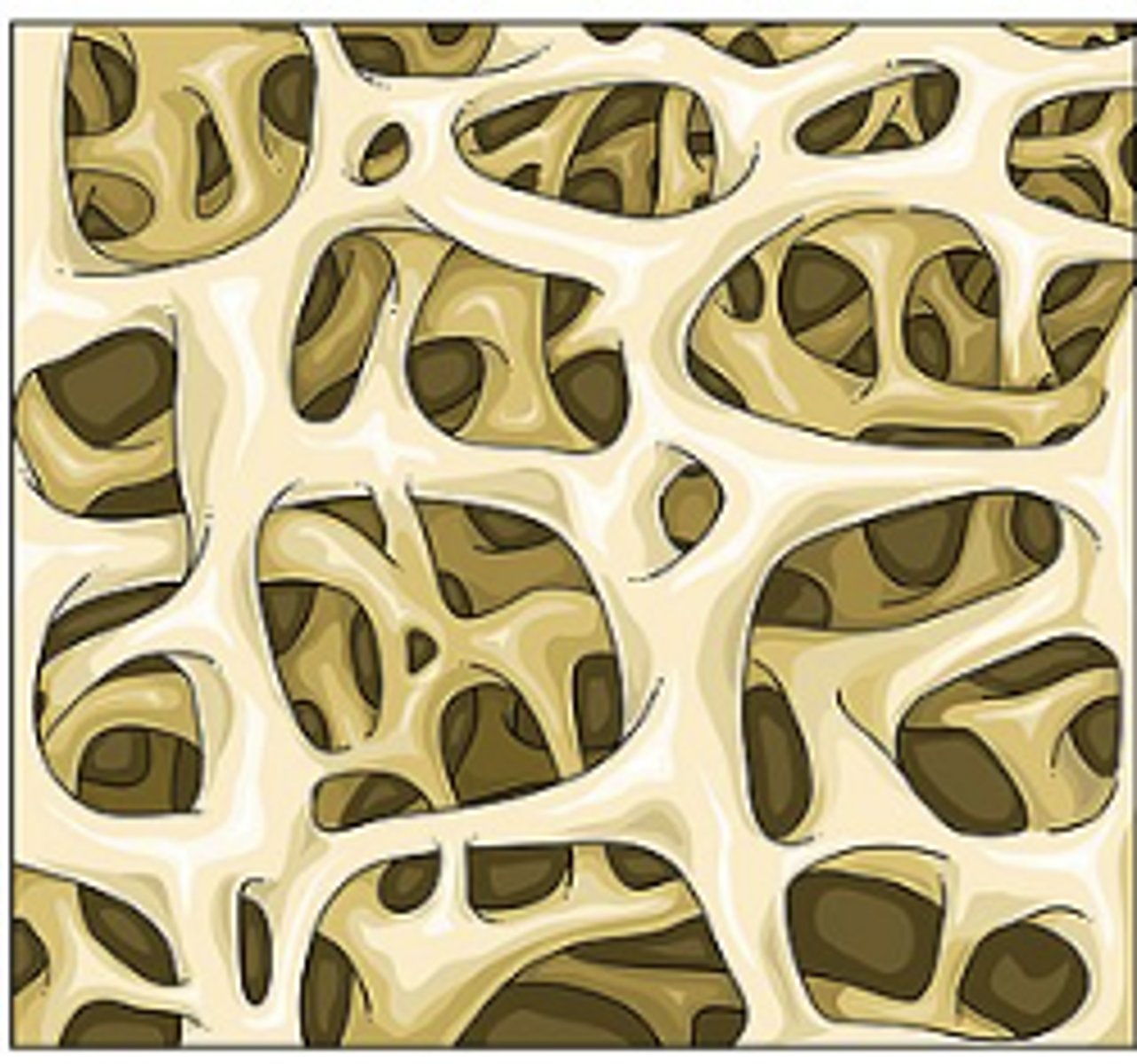
Spongy Bone (trabecular, cancellous)
Inner bone
Light weight, lattice like pattern
Compressive (force absorption)
Functional Unit: Trabeculae
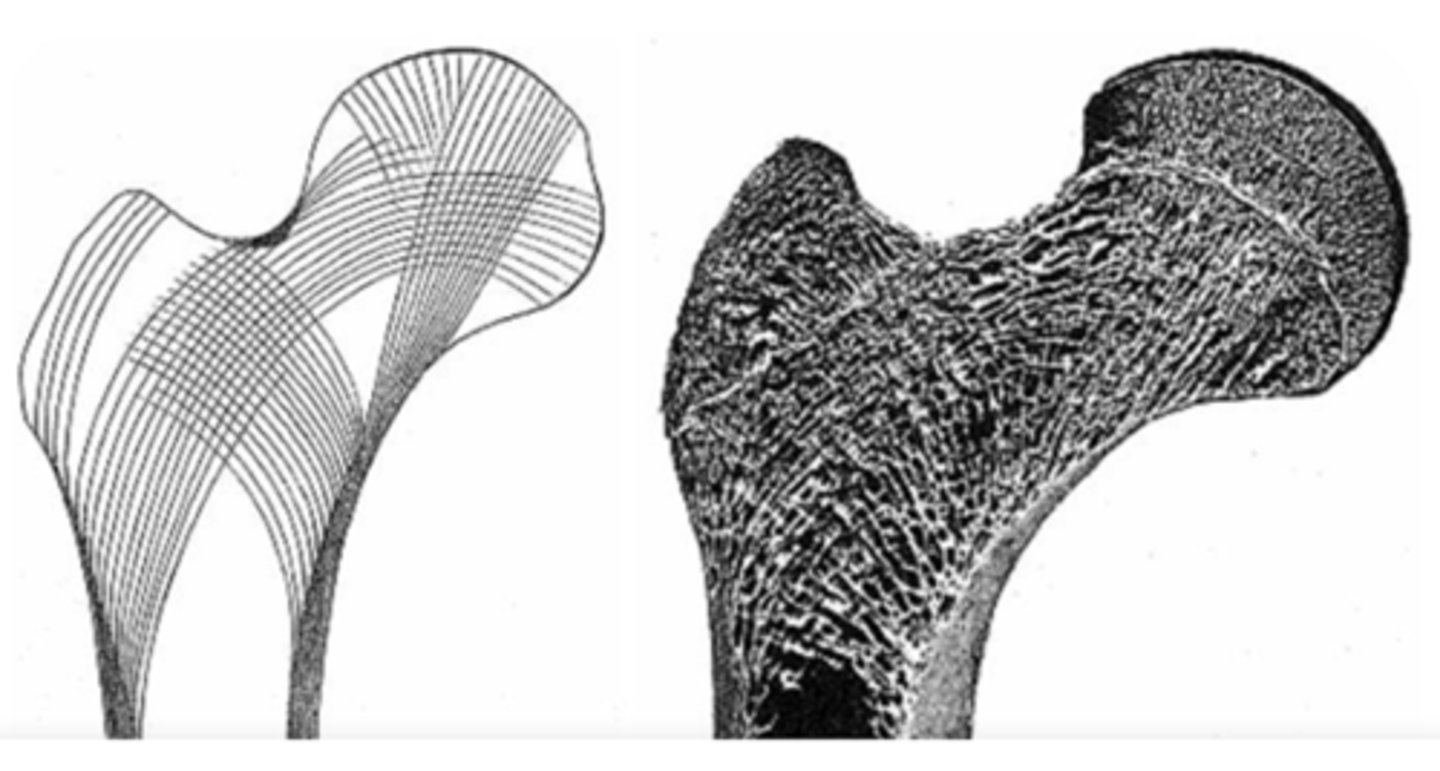
Trabeculae remodeled to align with ....
compressive forces
osteoprogentior cells
undifferentiated cells that differentiate into osteoblasts. found in the periosteum, endosteum, and epiphyseal growth plate of growing bones

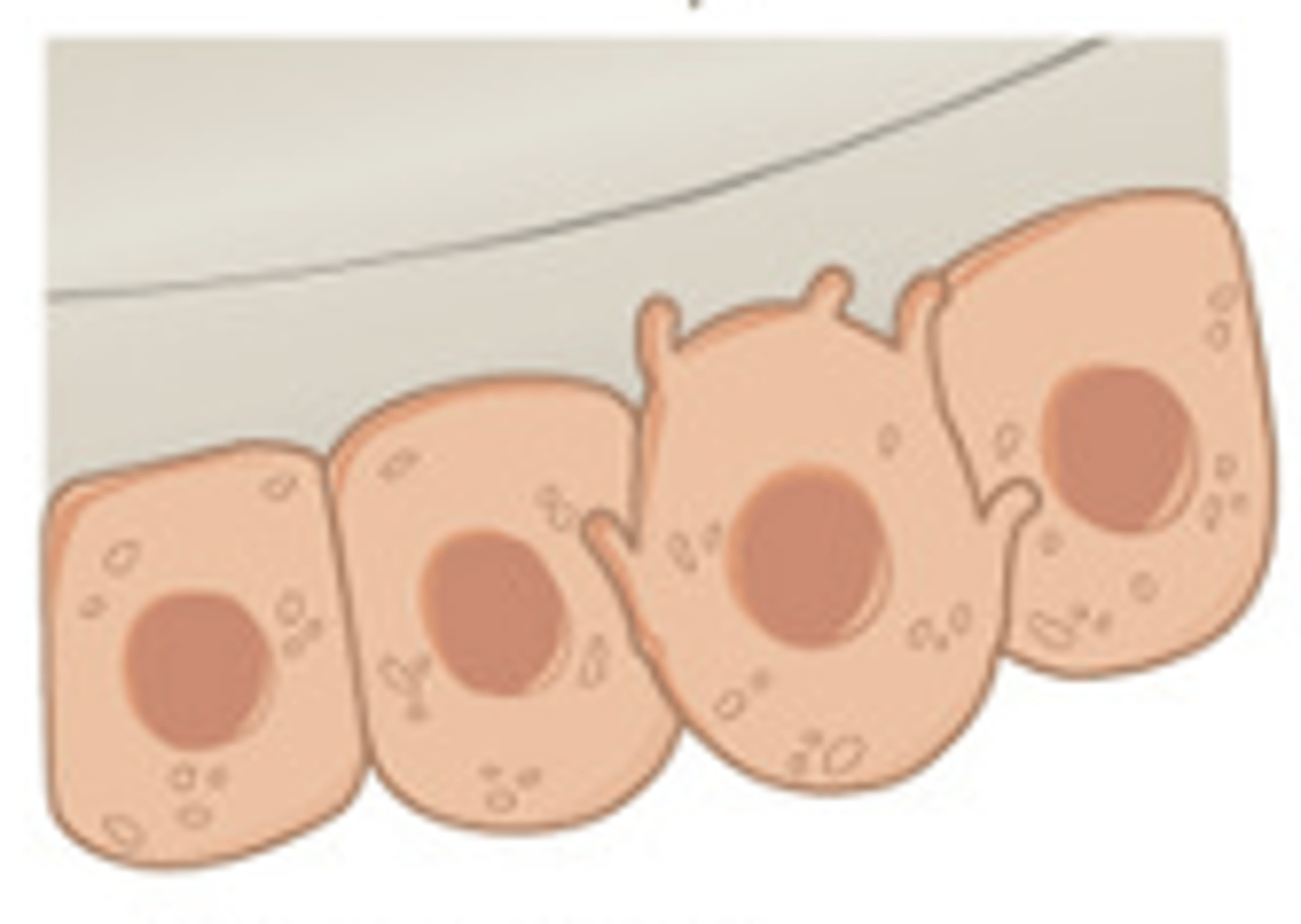
osteoblasts
bone building cells that synthesize and secrete the organic matrix of bone. participate in calcification of the organic matrix
osteocytes
mature bone cells, for maintenance of bone matrix. play an active role in releasing calcium into blood

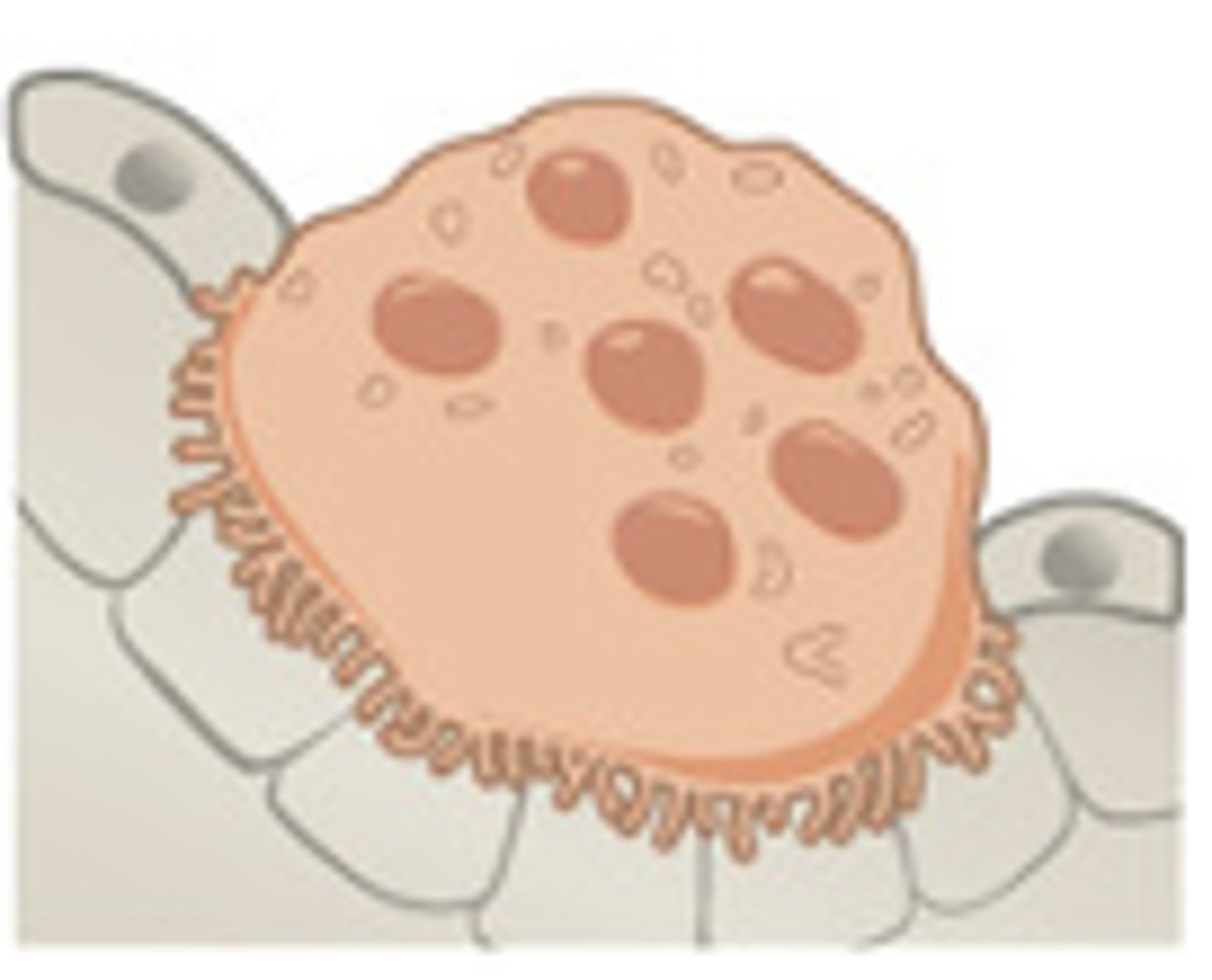
osteoclasts
bone chewing cells responsible for resorption (removal of bone mineral and organic matrix)
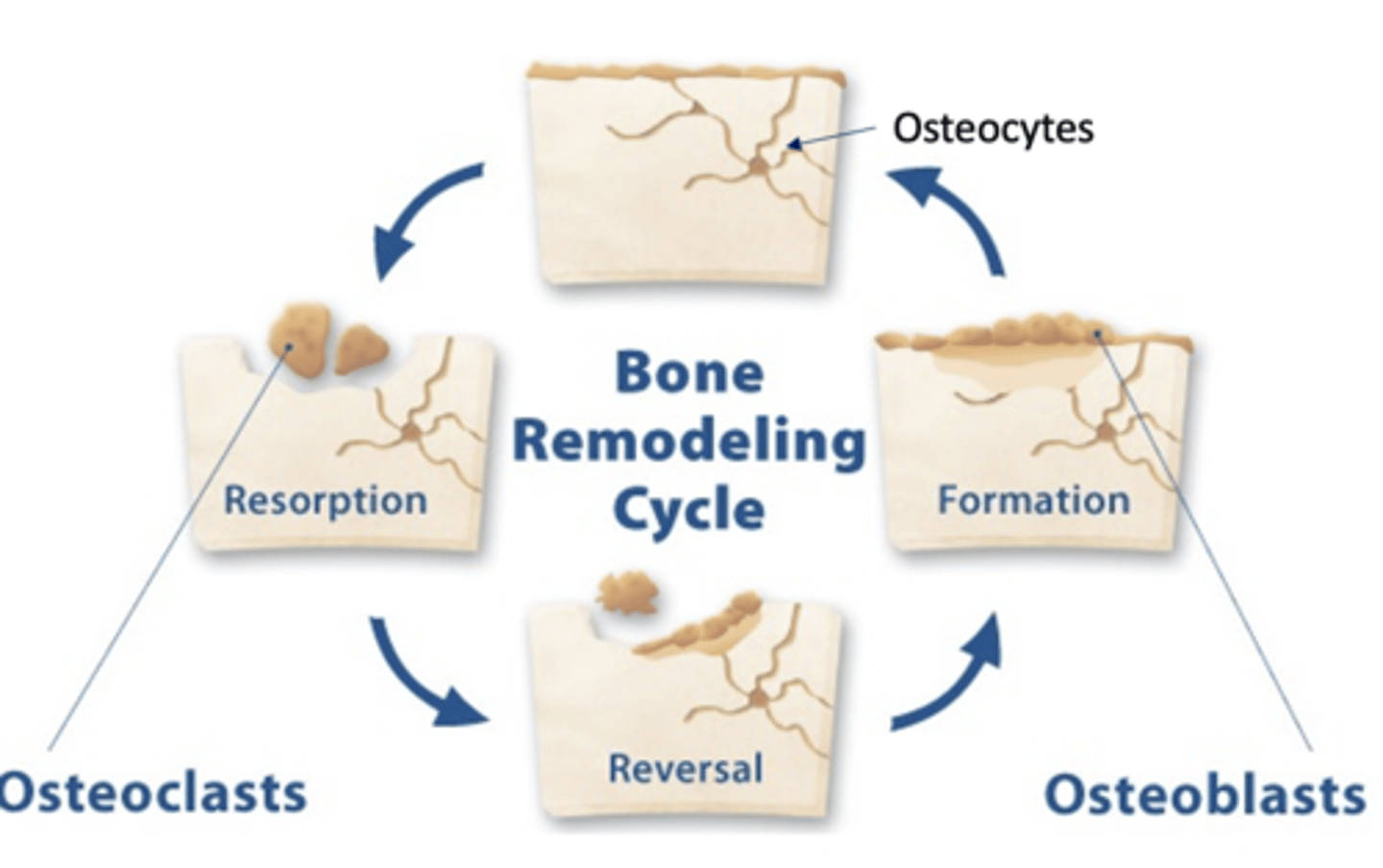
In normal bone, the remodeling cycle of resorption and formation is at __________
equilibrium
which of the following is an organic component of the bone matrix?
a. calcium
b. phosphate
c. collagen
d. magnesium
c. collagen
which statement correctly describes spongy (trabecular) bone?
a. forms the outer shell of bone
b. composed of densely packed osteons
c. also known as cortical bone
d. has a lightweight, lattice pattern
d. has a lightweight, lattice pattern
which bone cell type is responsible for bone resorption (bone chewing)
a. osteoclasts
b. osteoblasts
c. osteocytes
d. osteoprogenitor cells
a. osteoclasts
in norma;, healthy adult bone, the remodeling cycle is characterized by:
a. a constant increase in bone mass
b. an equilibrium between bone reabsorption and bone formation
c. a constant decrease in bone mass
d. no remodeling once the bone has matured
b. an equilibrium between bone reabsorption and bone formation
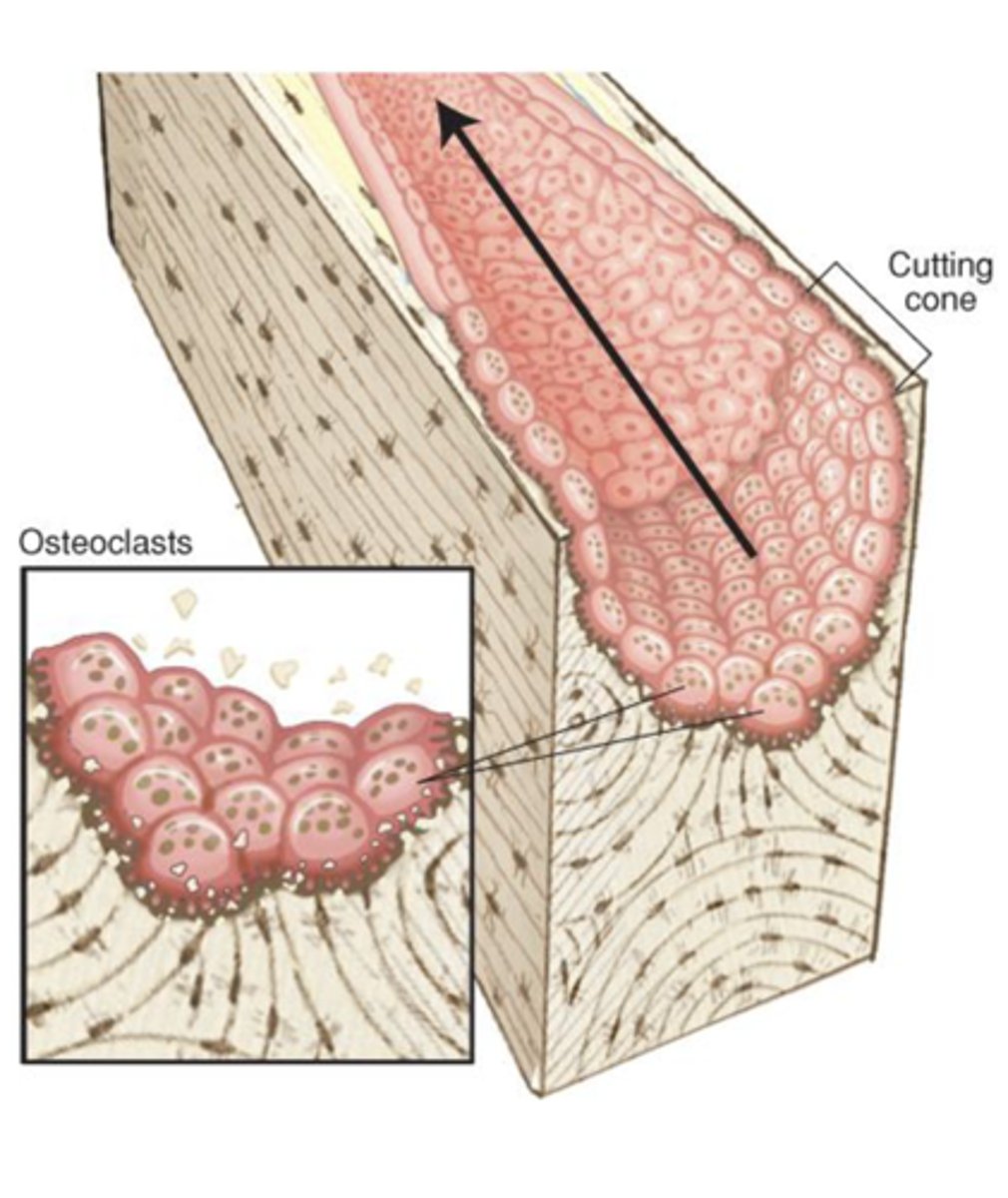
1. ___________ resorption of existing bone
Organic and inorganic components are removed, creating a _______-______ space in the osteon
Soluble factors (e.g. OPG) released during resorption aid in the recruitment of osteoblasts to the site
("__________")
1. Osteoclastic
2. tunnel like
3. reversal
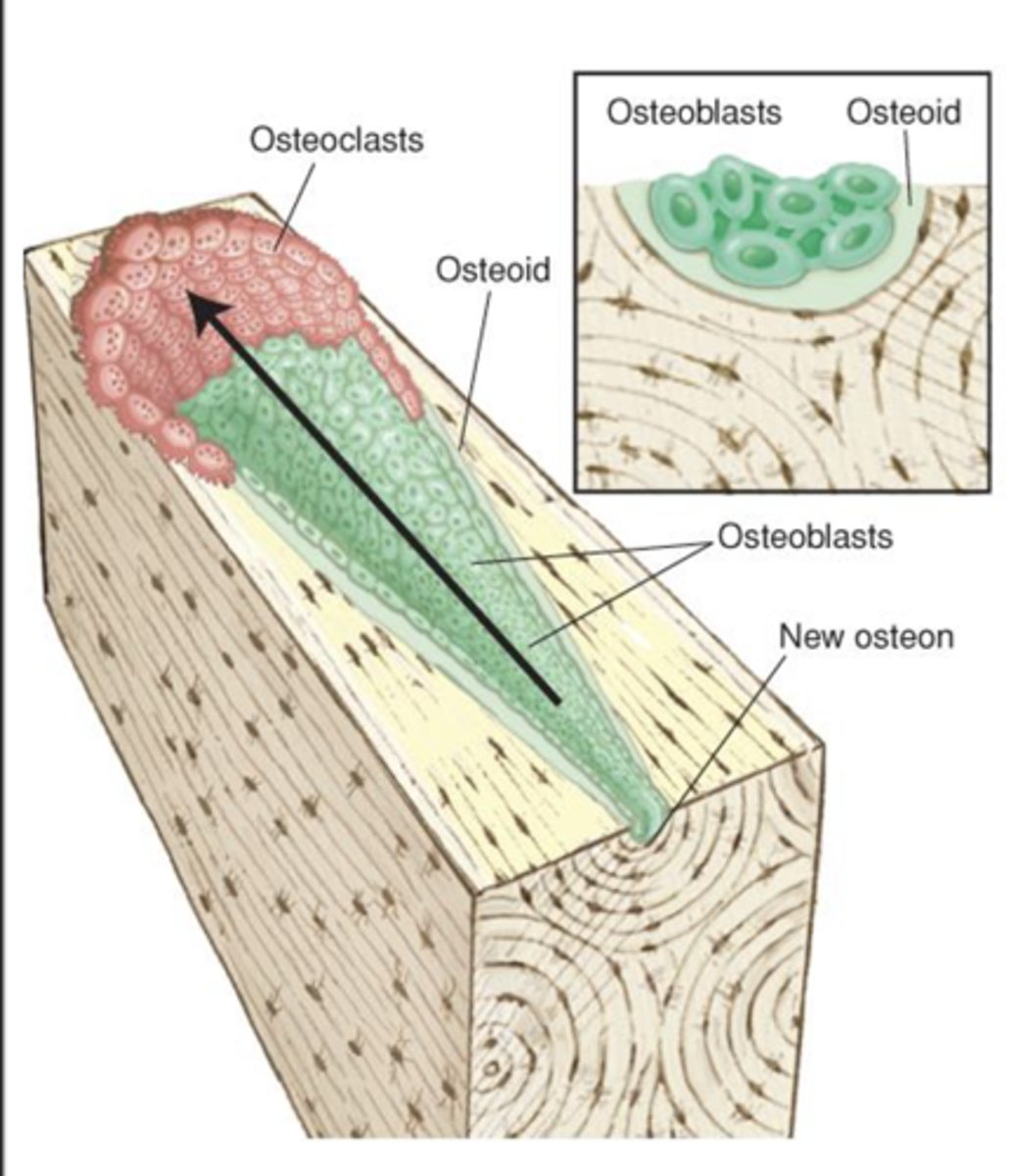
___________ begin to deposit organic matrix (osteoid) on the wall of the osteon canal
Successive lamellae are deposited, and the canal attains relative proportions of original osteon
When they receive a signal, osteoblasts release RANKL (induces osteoclast activity)
Osteoblasts
RANKL
Receptor activator of nuclear factor kappa-Β ligand
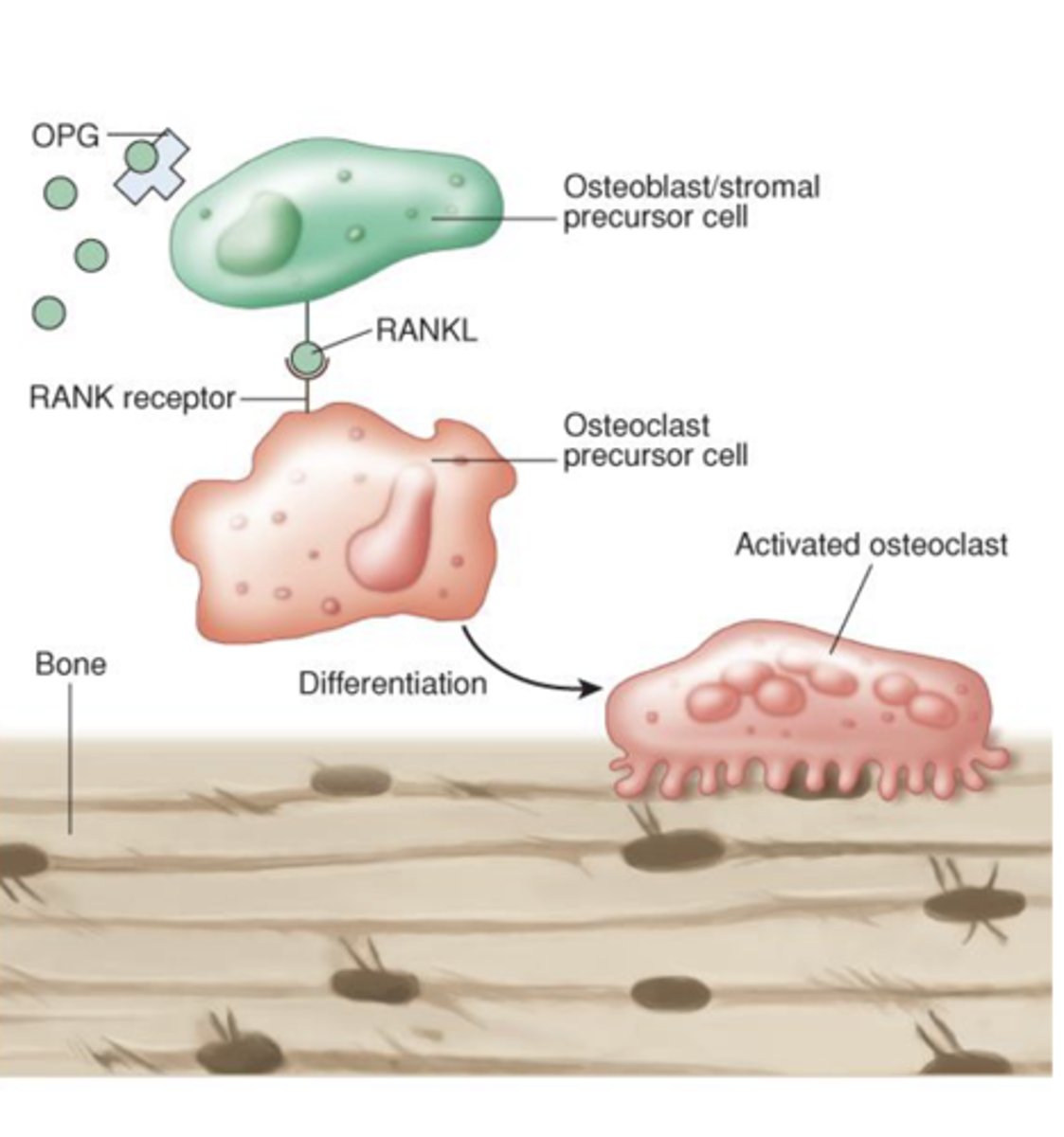
Paracrine system that balances resorption and formation
1. _______
-- Produced by osteoblasts
-- Binds to RANK receptor and promotes activation of osteoclasts
2. ______________________
-- “Decoy” receptor to block RANKL activity to ensure balance
1. RANKL
2. Osteoprotegerin (OPG)
Dysregulation of the RANKL/OPG system plays a role in ...
pathogenesis of bone diseases
which statement best describes the role of RANKL in bone remodeling?
a. RANKL is produced by osteoclasts to inhibit osteoblasts
b. RANKL binds to the OPG receptor to stimulate bone formation
c. RANKL is produced by osteoblasts and promotes osteoclasts activation
d. RANKL acts as a decoy receptor for OPG, blocking osteoclasts
c. RANKL is produced by osteoblasts and promotes osteoclasts activation
osteoprotegrin (OPG) functions as a decoy receptor by:
a. binding to RANKL, thereby preventing osteoclast activation
b. binding to calcium to enhance bone calcification
c. stimulating osteoblasts to resorb bone
d. inhibiting collagen production in bone matrix
a. binding to RANKL, thereby preventing osteoclast activation
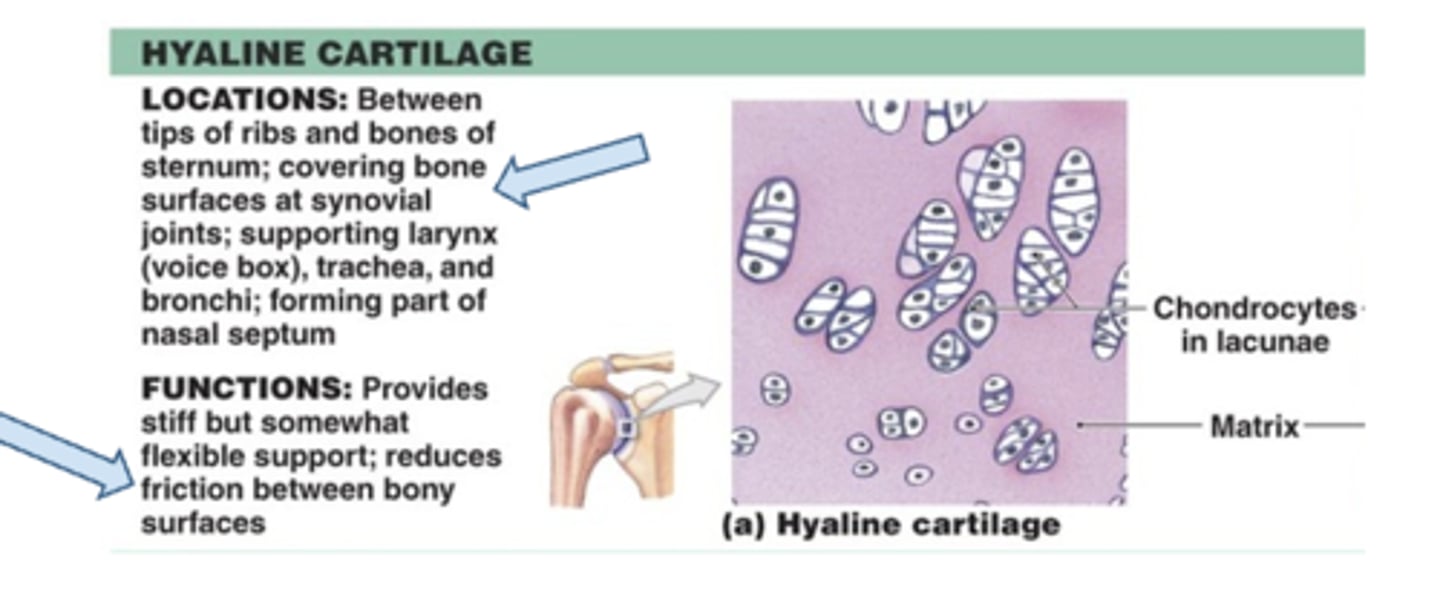
Cartilage
Chondrocytes & matrix
avascular - if its gone its gone
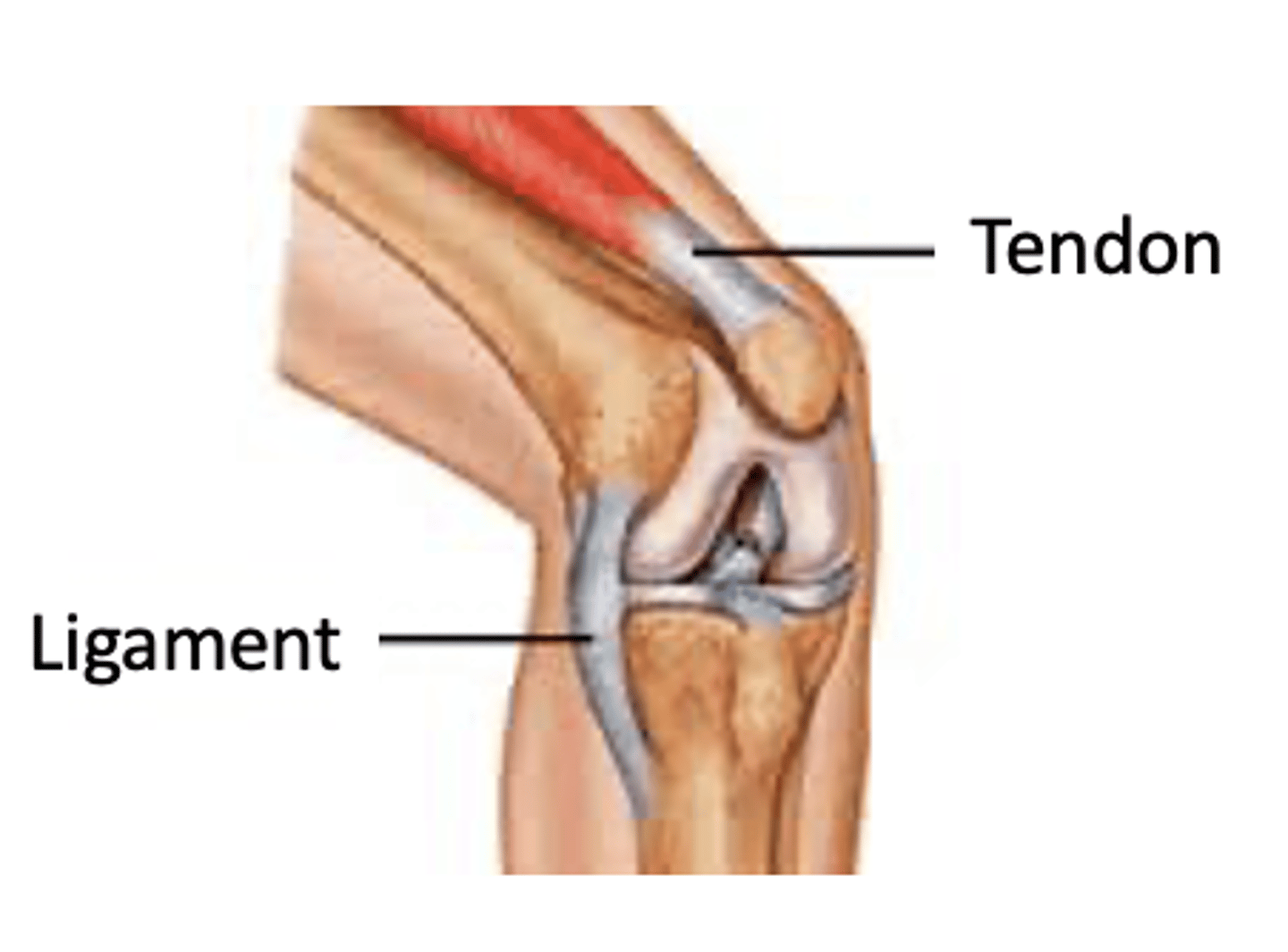
Ligaments and tendons
have a limited blood supply
(Implication for healing?)
Dense regular connective tissue
-- Inelastic collagen fibers
-- High tensile strength
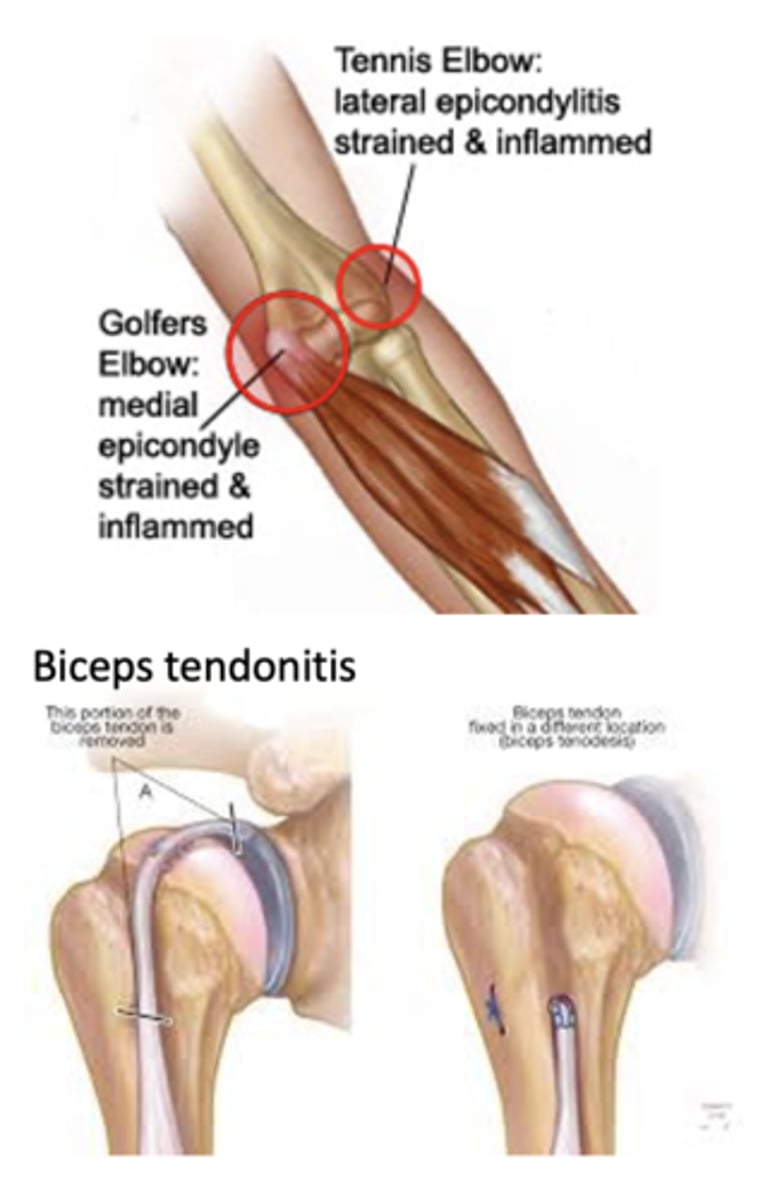
tendonitis
Inflammation of a tendon where it attaches to or contacts a bone
Causes: Repetitive motion/overuse
Symptoms:
- Pain
- Tenderness
- Weakness
Treatments:
- Rest
- Occupational therapy &/or PT
Bracing and exercise
- Anti-inflammatory medications
- Surgery in severe cases (tears)
Strain
Stretching or partial tear in a muscle or muscle–tendon unit
Inflammatory response and fibrous tissue replacement at the site
Symptoms: Pain, stiffness, swelling, and local tenderness
Common sites: Lower back, neck, hamstring
Sprain
Involves ligaments or joint capsule
Due to abnormal or excessive movement of a joint
Symptoms: Pain, rapid swelling, discoloration, and limited function
Common sites: Ankle, knee (ACL), elbow
treatment for strain and sprain
Rest, Ice, Compression, and Elevation (RICE) --> Movement, Exercise, Analgesia, Treatment (MEAT)
The affected area may be immobilized until pain/swelling is reduced (24-48 hours)
Early diagnosis, treatment, and rehabilitation are essential in preventing weakening of injured area due to immobilization
compression: only at rest
Disruption in the continuity of a bone:
Causes: High compression, tension, shearing, bending, or torsion forces
which are bones best at resisting?
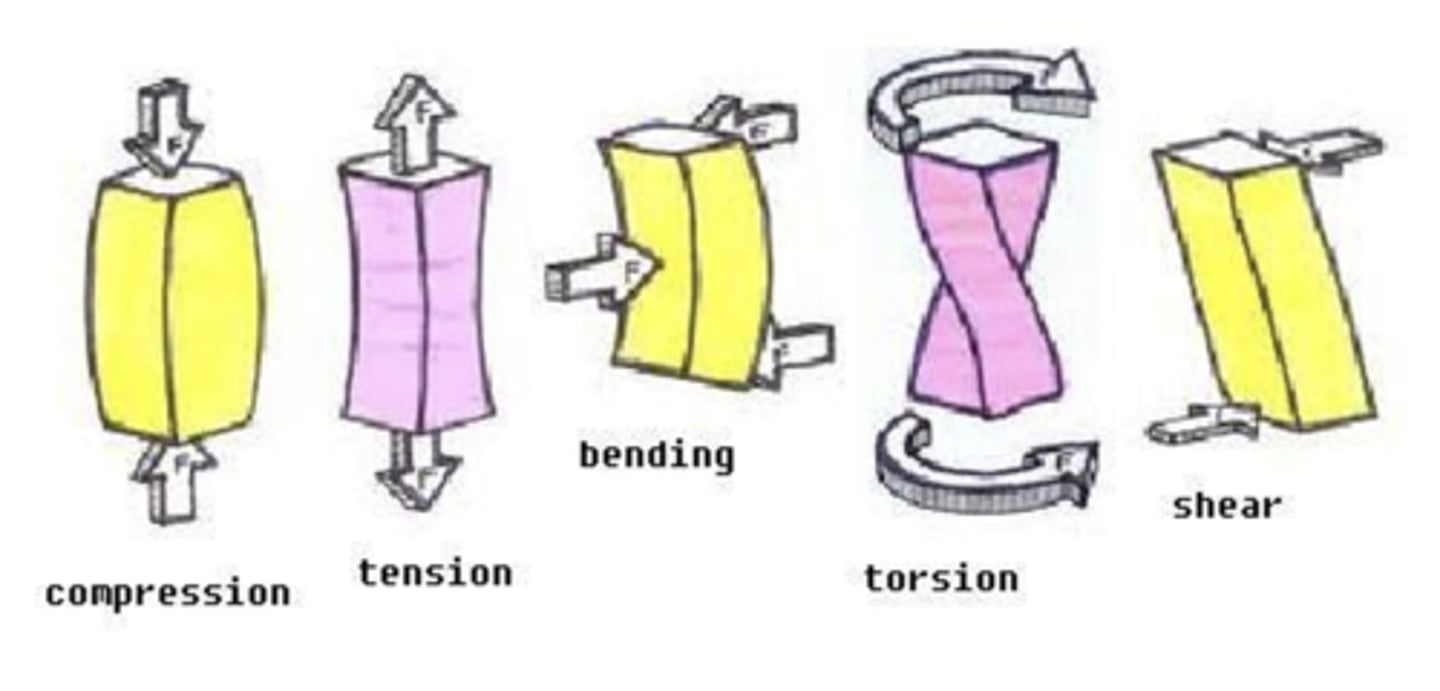
fractures
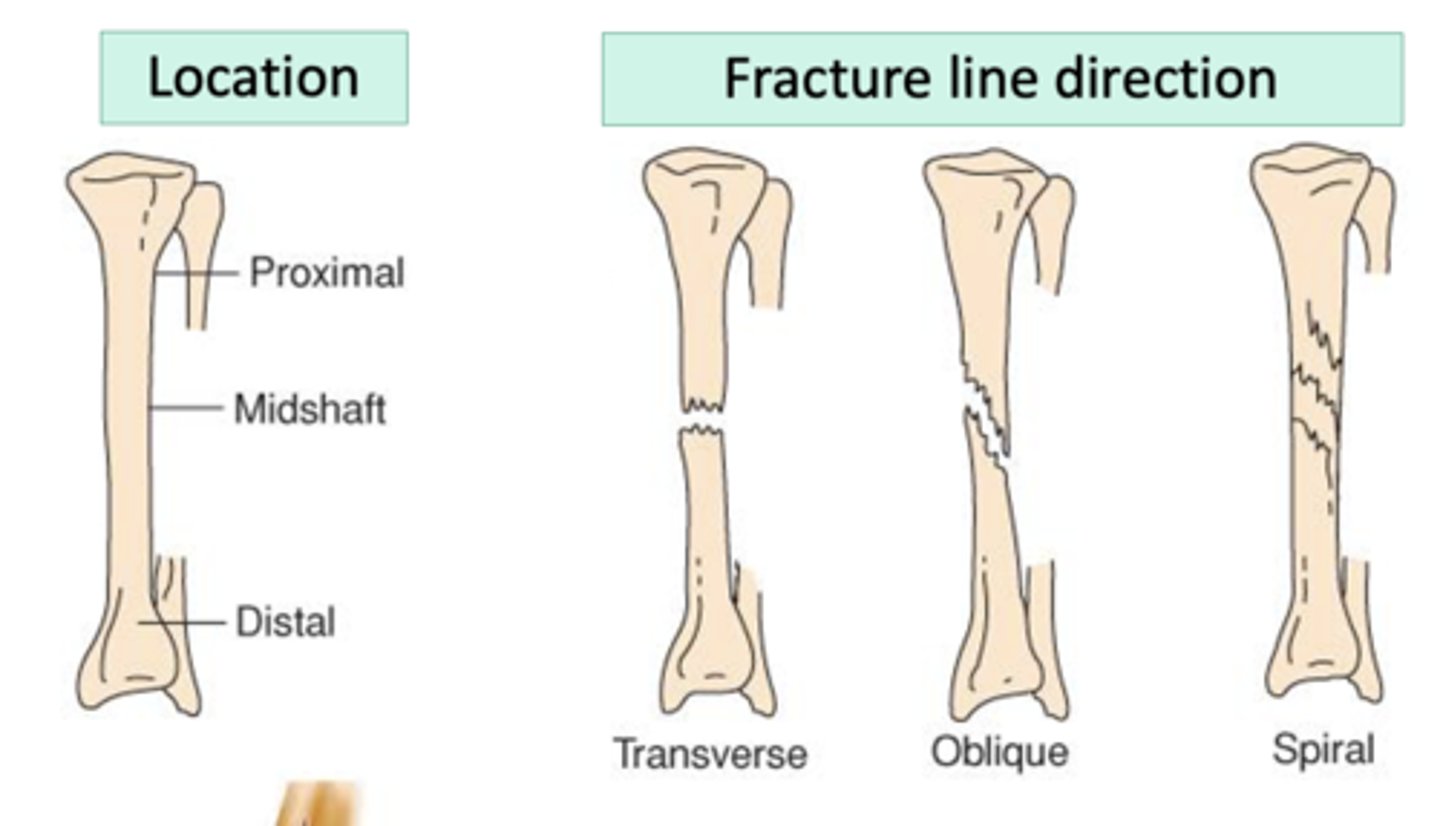
Further classified by:
- Open or closed
- Location
- Type or pattern of fracture line
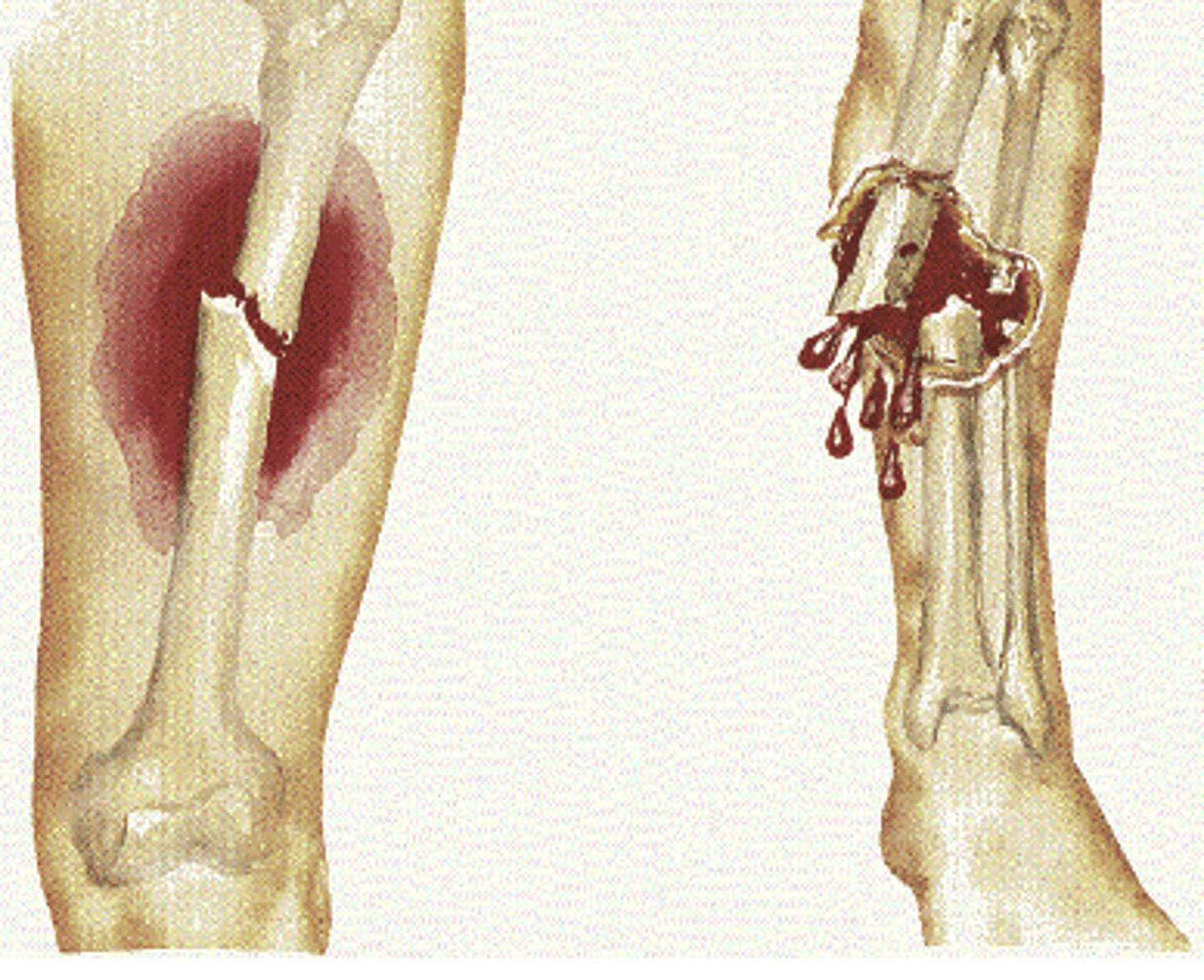
what is an immediate concern with an open fracture?
infection
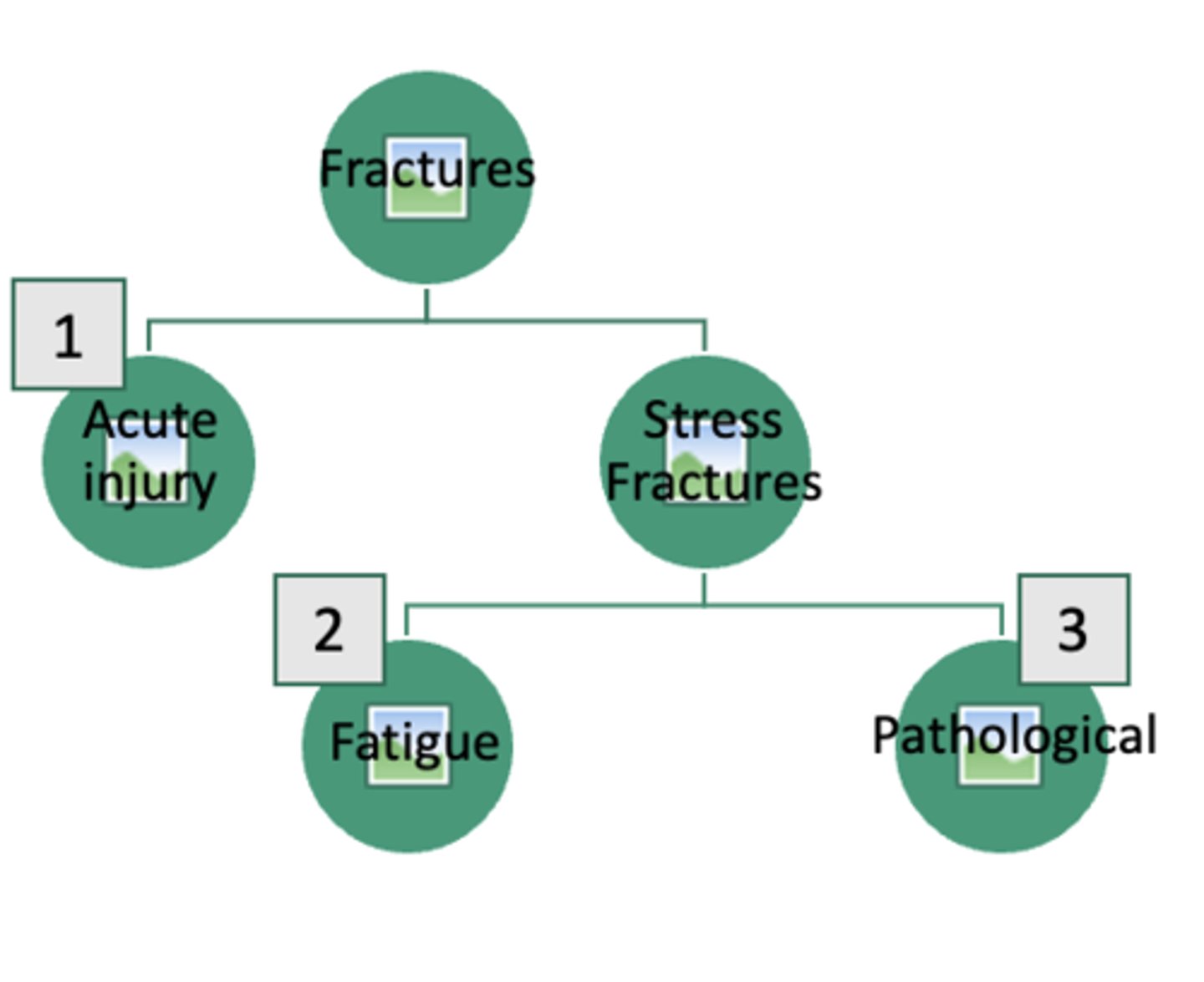
Greenstick
seen in children, partial break in bone continuity

types of fractures
fractures (2)
Pain, tenderness, swelling, loss of function, deformity of the affected part, abnormal mobility
Types of deformities (long bones)
- Angulation
- Shortening
- Rotation
X-ray confirms diagnosis, directs treatment
Treatment:
1. reduction
2. immobilization
3. preserve/restore function

which of the following best describes tendonitis?
a. inflammation of a tendon where it attaches to or contacts a bone
b. a complete rupture of a tendon
c. degeneration of joint cartilage
d. a chronic condition only seen in elderly patients
a. inflammation of a tendon where it attaches to or contacts a bone
which of the following is the best description of a sprain?
a. always leads to bone fractures
b. involves ligaments or joint capsule with pain and swelling
c. only involves muscle fibers
d. results exclusively from direct compact
b. involves ligaments or joint capsule with pain and swelling
a fracture that partially breaks the bone and is commonly seen in children is called:
a. spiral
b. oblique
c. greenstick
d. comminuted
c. greenstick
what is the immediate concern with an open (compound) fracture?
a. difficulty diagnosing the fracture on x ray
b. increased bone density
c. inability to reduce the fracture
d. possible infection due to bone exposure
d. possible infection due to bone exposure
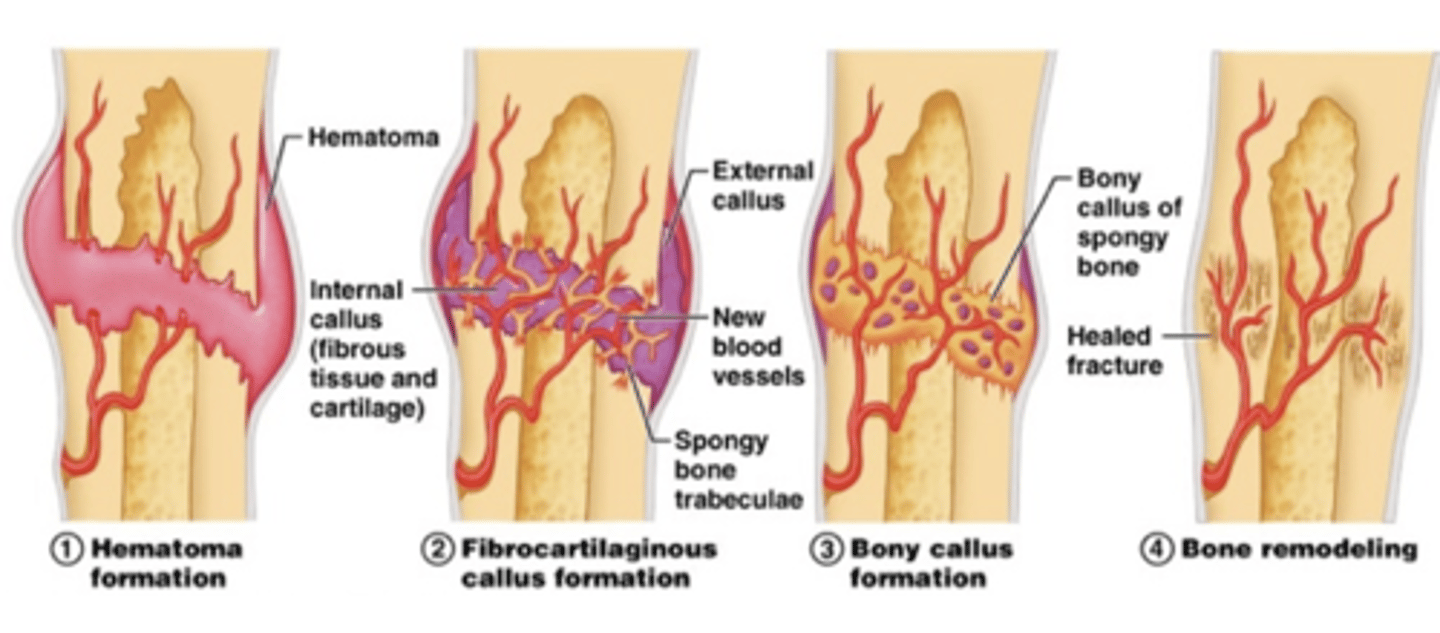
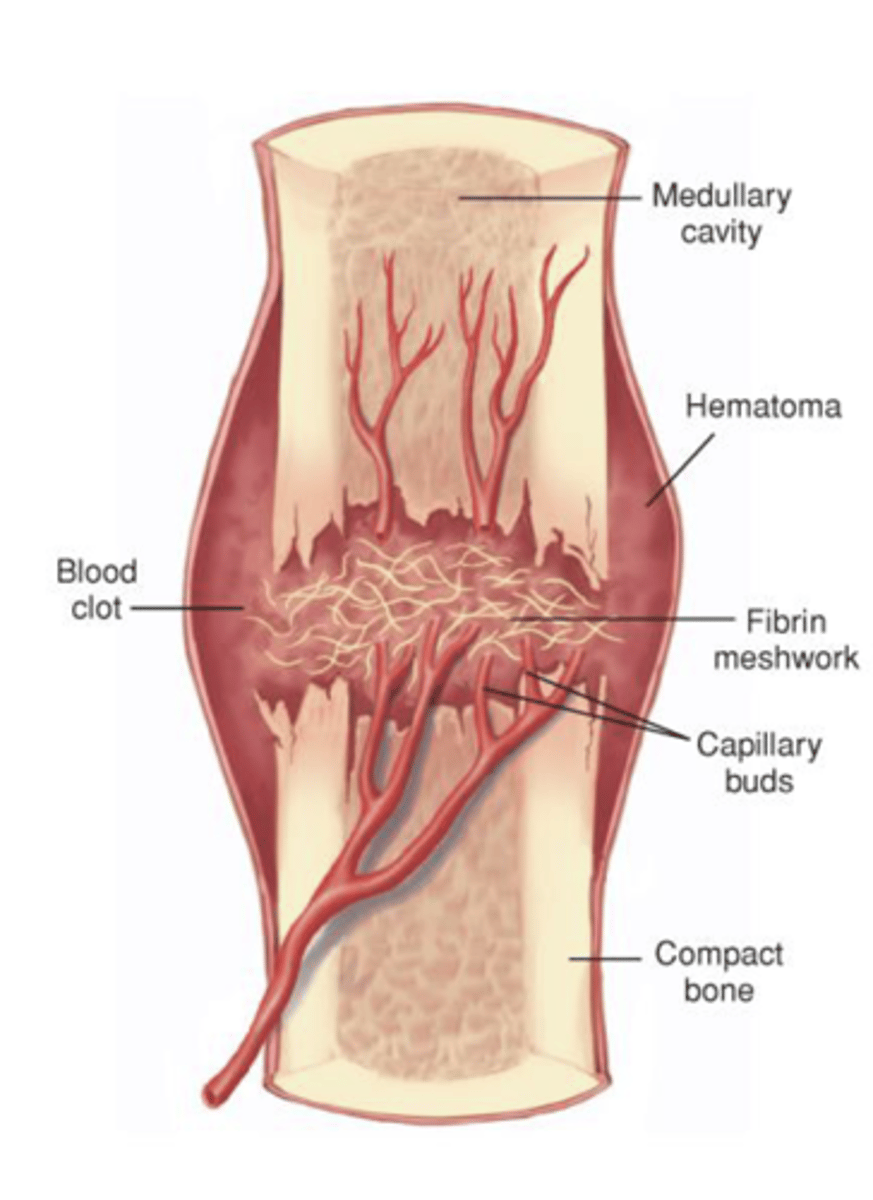
stages of fracture healing
hematoma formation
Blood vessels in the bone and surrounding tissues bleed into and around the fragments forming a hematoma
Fibrin meshwork forms and seals the fracture site
-- Initiates healing process
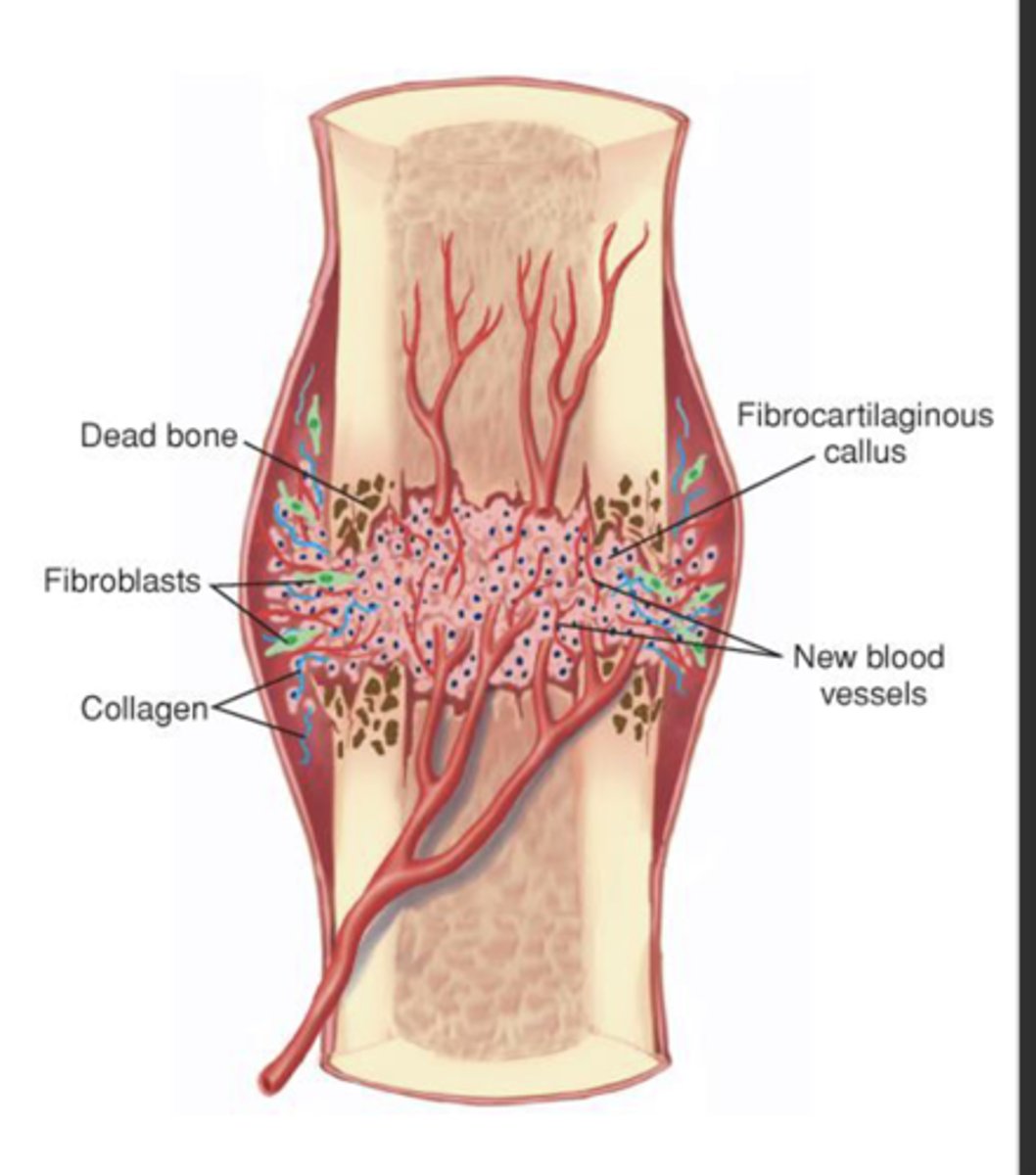
fibrocartilaginous callus formation
Granulation tissue called procallus is formed
Fibroblasts invade the procallus
Fibroblasts produce soft callus bridge that connects bone fragments
Callus formed by end of 2nd or 3rd week, not strong enough for weight bearing
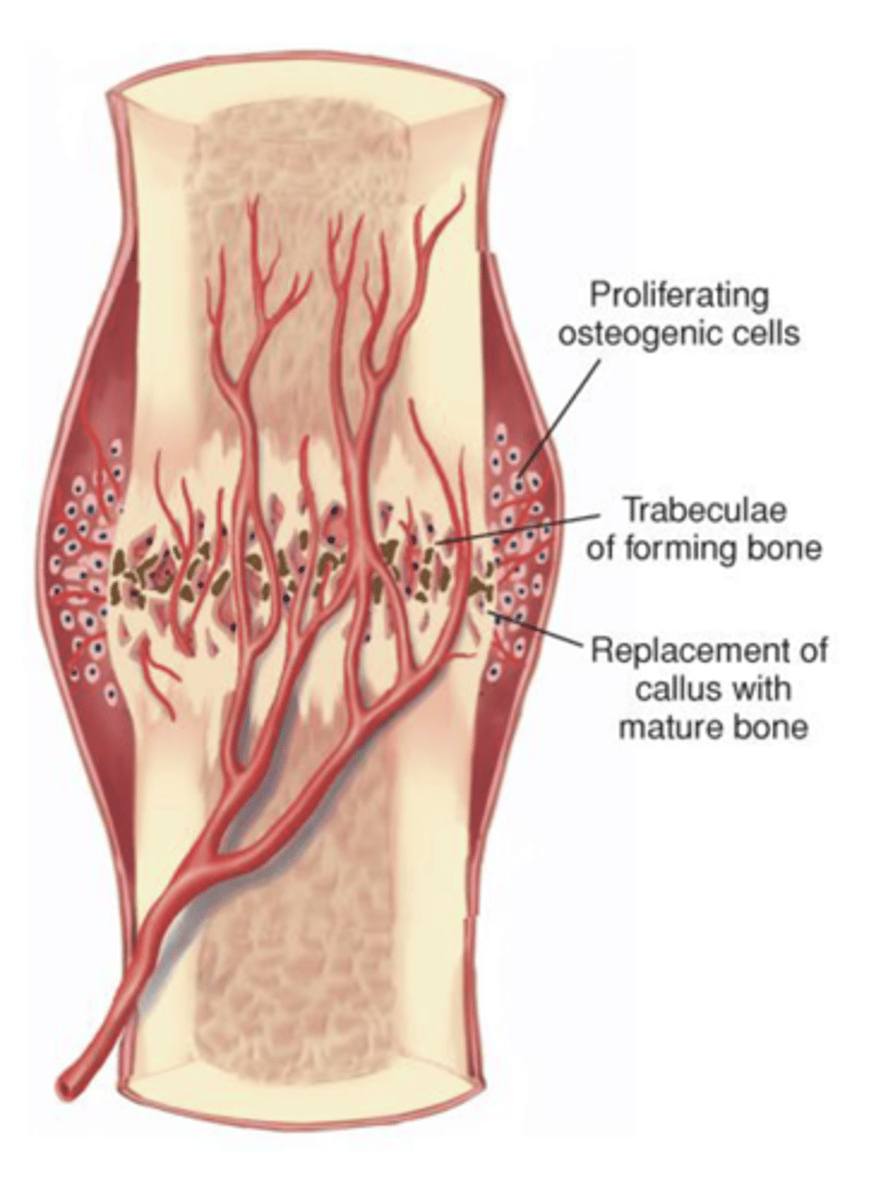
bony callus formation
Cartilage is ossified to form a bony callus
Formation of bone progresses toward the fracture site until a new bony sheath covers the callus
Fibrocartilage is converted to woven bone and gradually calcifies into mature bone
Begins 3 to 4 weeks after injury and continues for months later
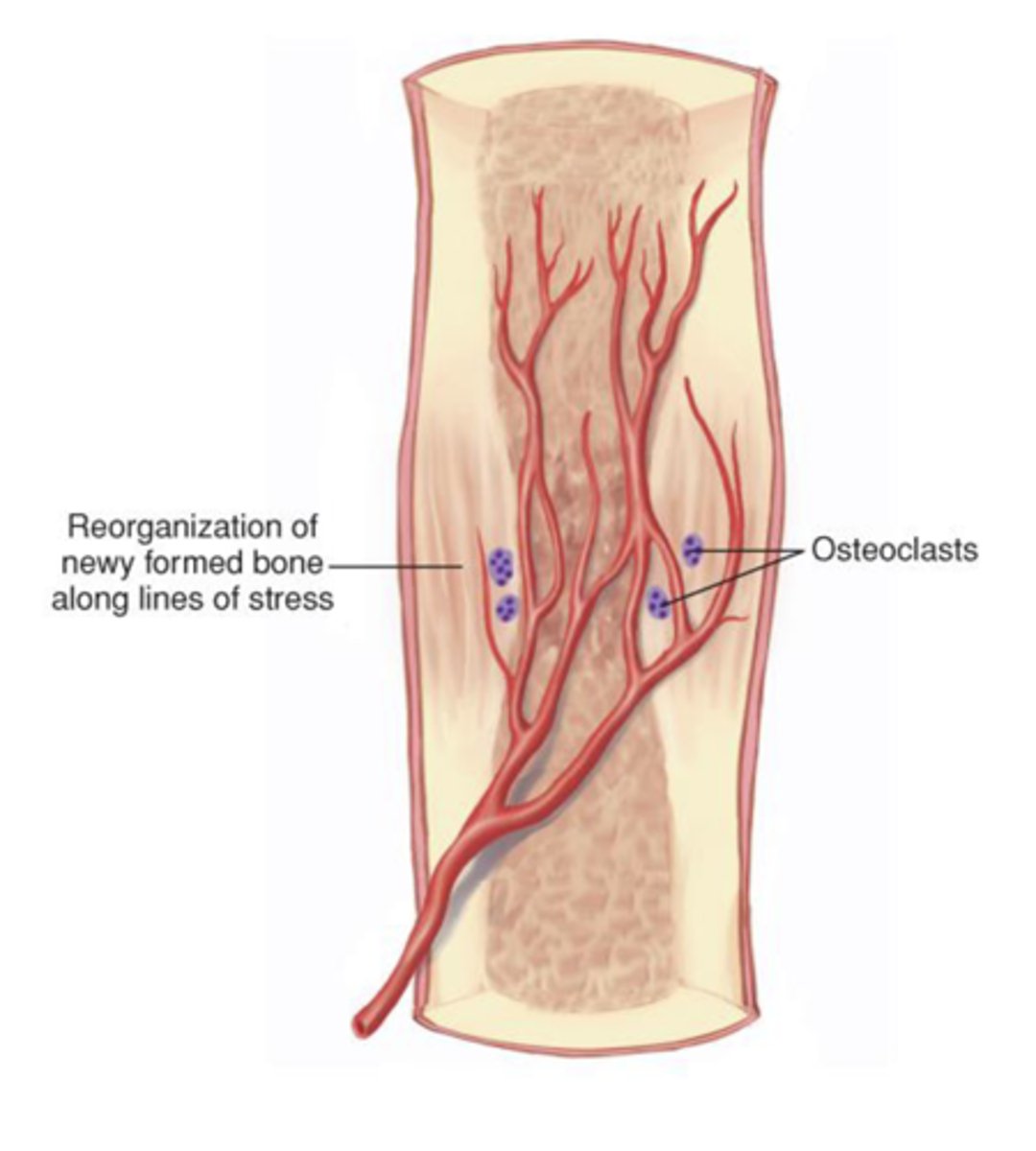
remodeling
Dead bone is removed by osteoclasts
Compact bone replaces spongy bone
Excess material is removed and compact bone is laid to reconstruct the shaft
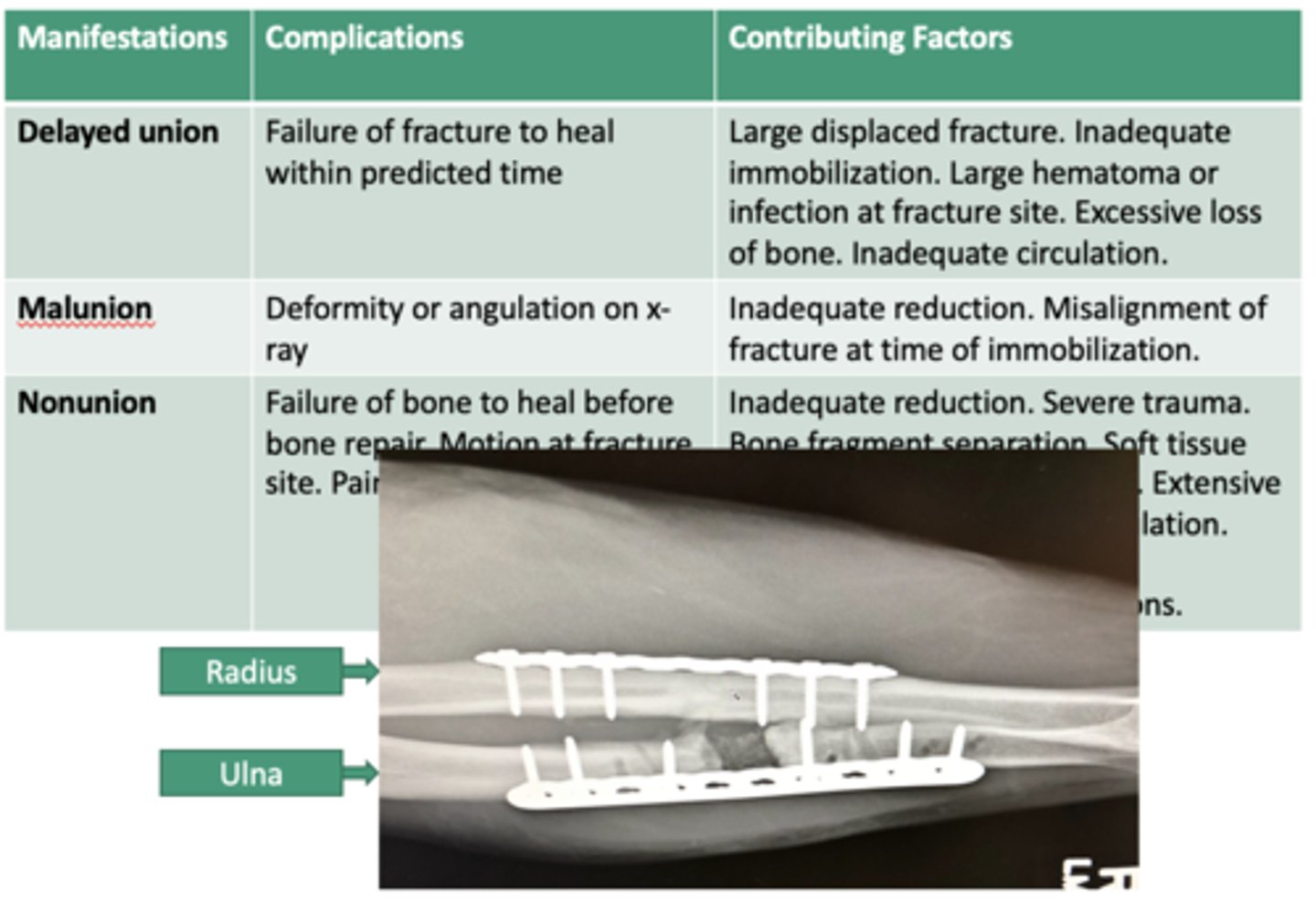
complication of fractures
Compartment Syndrome - complication of fracture
Increased pressure within limited space
Compromises circulation and function
-- Screen for signs
Nerve and muscle death in 8 hrs
Treatment: Relieve pressure (fasciotomy)

Wolff’s Law
a tissue adapts to the level of stress imposed upon it
-- Strengthening and weakening- depending on level of stress
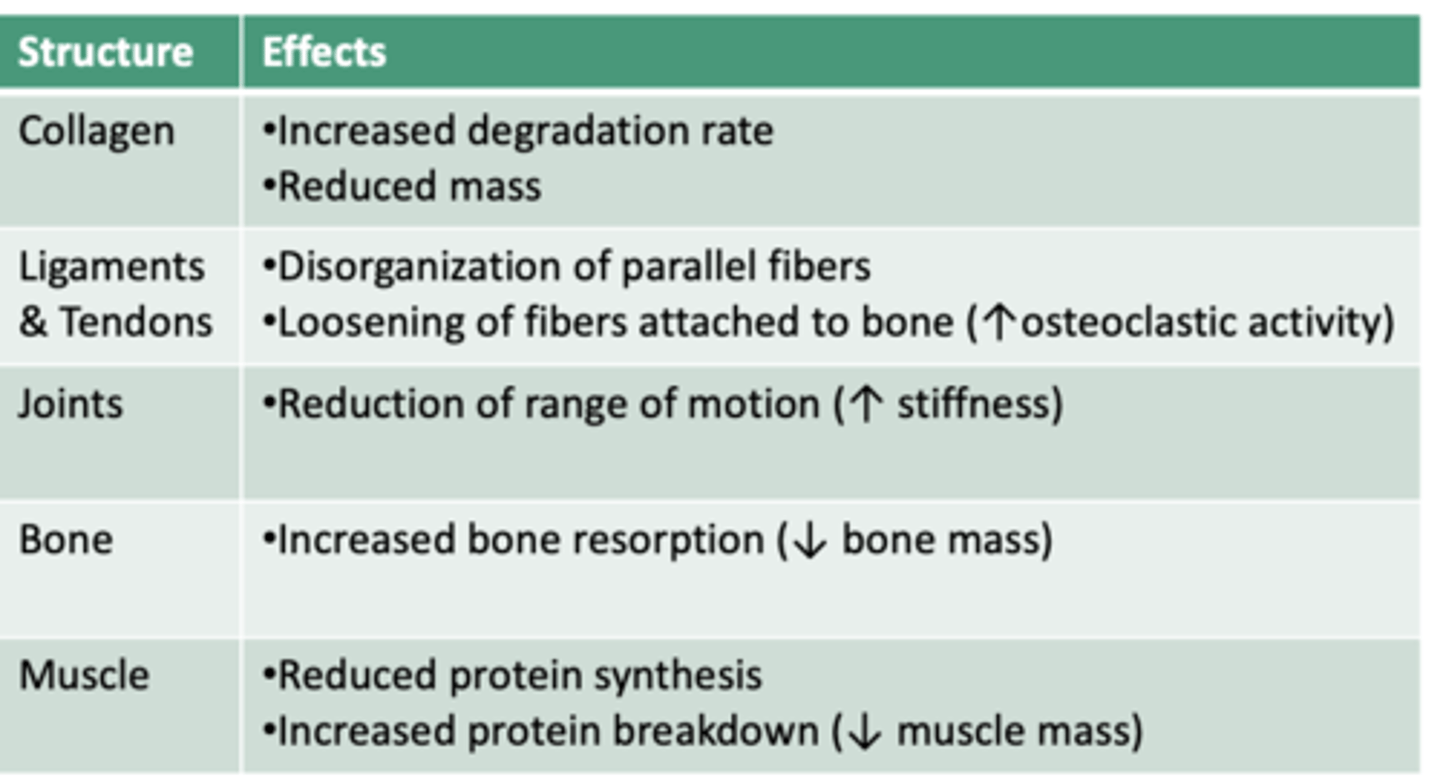
What can a patient do to regain mass & function after immobilization (disuse atrophy)?
Physical and/or occupational therapy
Return to daily activities
Structured exercise
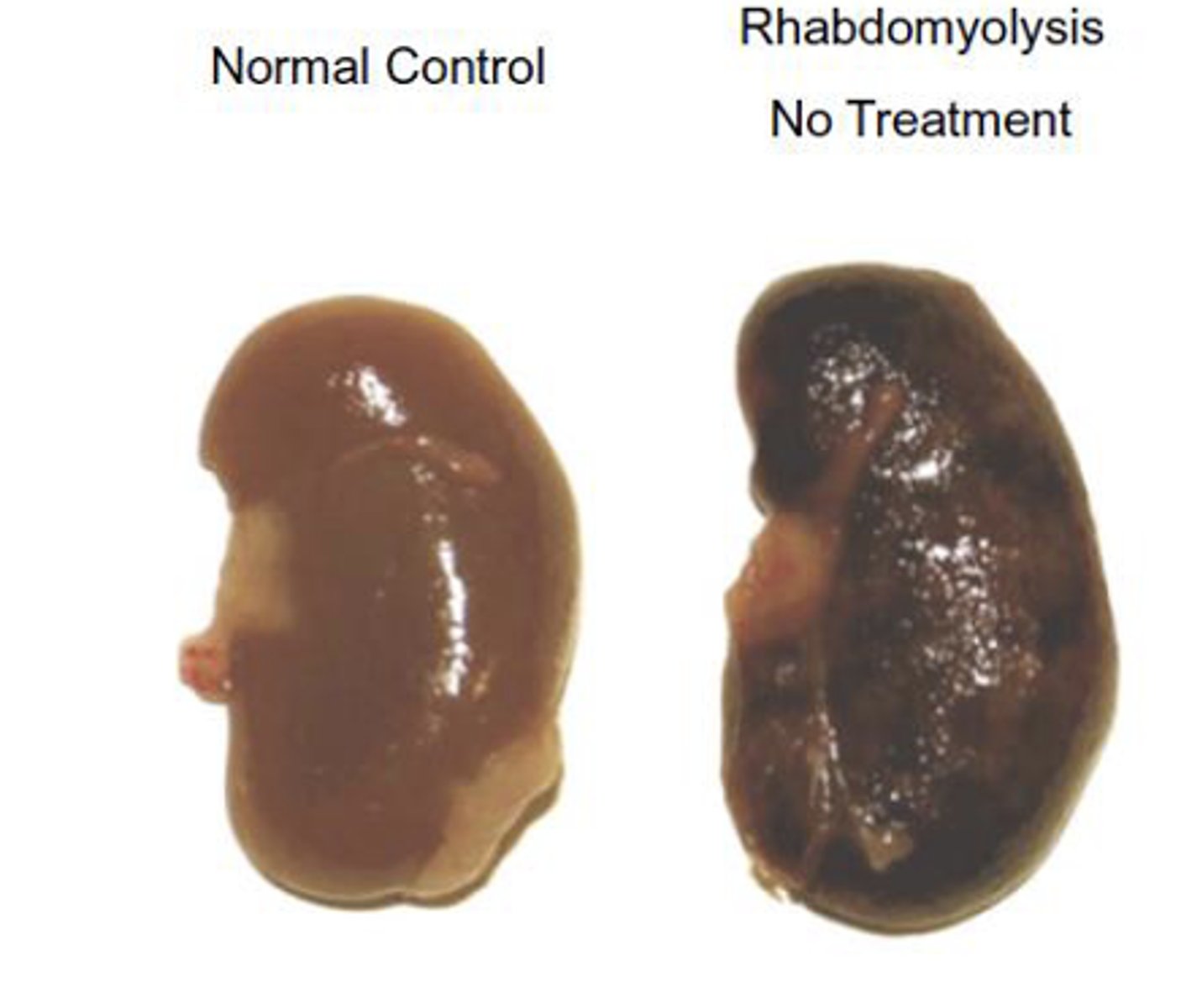
rhabdomyolysis
Direct or indirect severe muscle injury (e.g., trauma, statins, excessive alcohol) and release of myoglobin into the blood
Symptoms:
- Excessive muscle pain, muscle weakness
- Dark red or brown urine
- Serum creatine kinase and myoglobin are elevated
Complications: Acute renal failure, fatal heart rhythm disturbances, hypovolemic shock, disturbances of electrolyte balance, metabolic acidosis, hyperthermia, compartment syndrome
Overall mortality rate is ~5%
Treatments:
IV fluids
Fasciotomy
Stop drug use (if applicable)
osteomyelitis
Acute or chronic infection of the bone and marrow
Pyogenic - Staphylococcus aureus is most common cause
-- Hematogenous- Originates with infectious organisms that reach the bone through the bloodstream.
-- After open fracture, bacteria from patient’s skin run high risk of establishing colonies inside the bone
Symptoms:
- Bacteremia (chills, fever, malaise)
- Bone lesion (pain, reduced motion)
Treatment:
- Identify causative organism
- Treat organism (e.g., antibiotic)
- Rest & pain management
Possible drainage

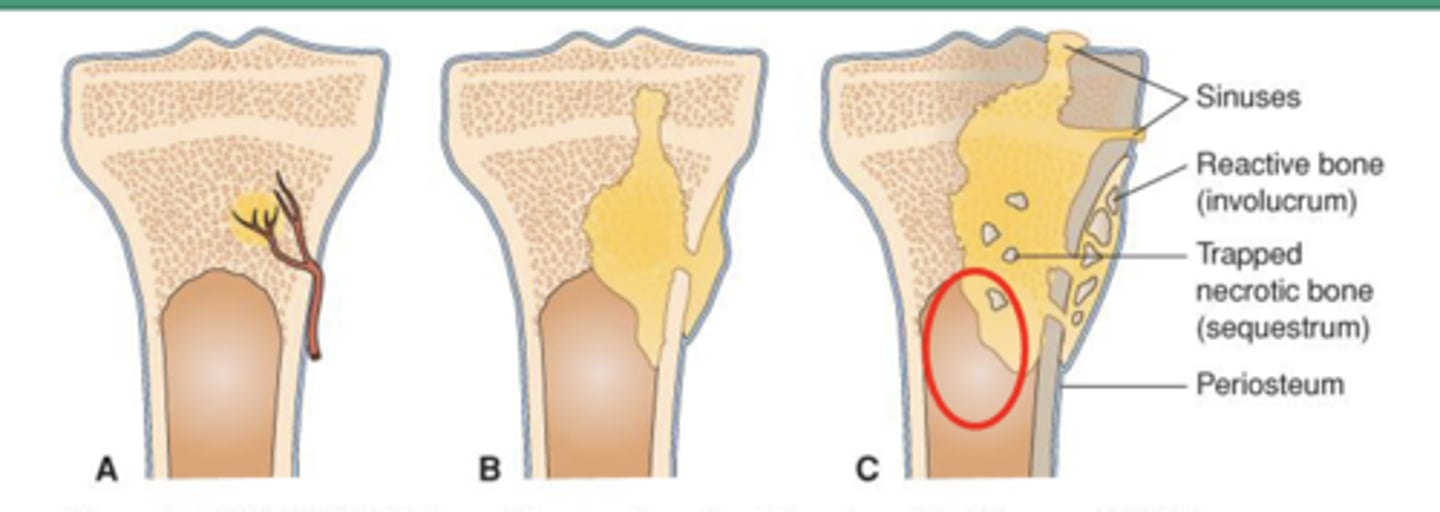
hematogenous osteomyelitis
A: Systemic infection spreads to bone
B: Purulent exudate collects as infection spreads, shearing off perforating arteries
C: Bone necrosis; necrotic bone separates from live bone to form devascularized fragments, called sequestra
D: Catch it early, long term consequences are relatively rare (less than 1-10%) – but include increase in fracture, development of chronic or reoccurring infection
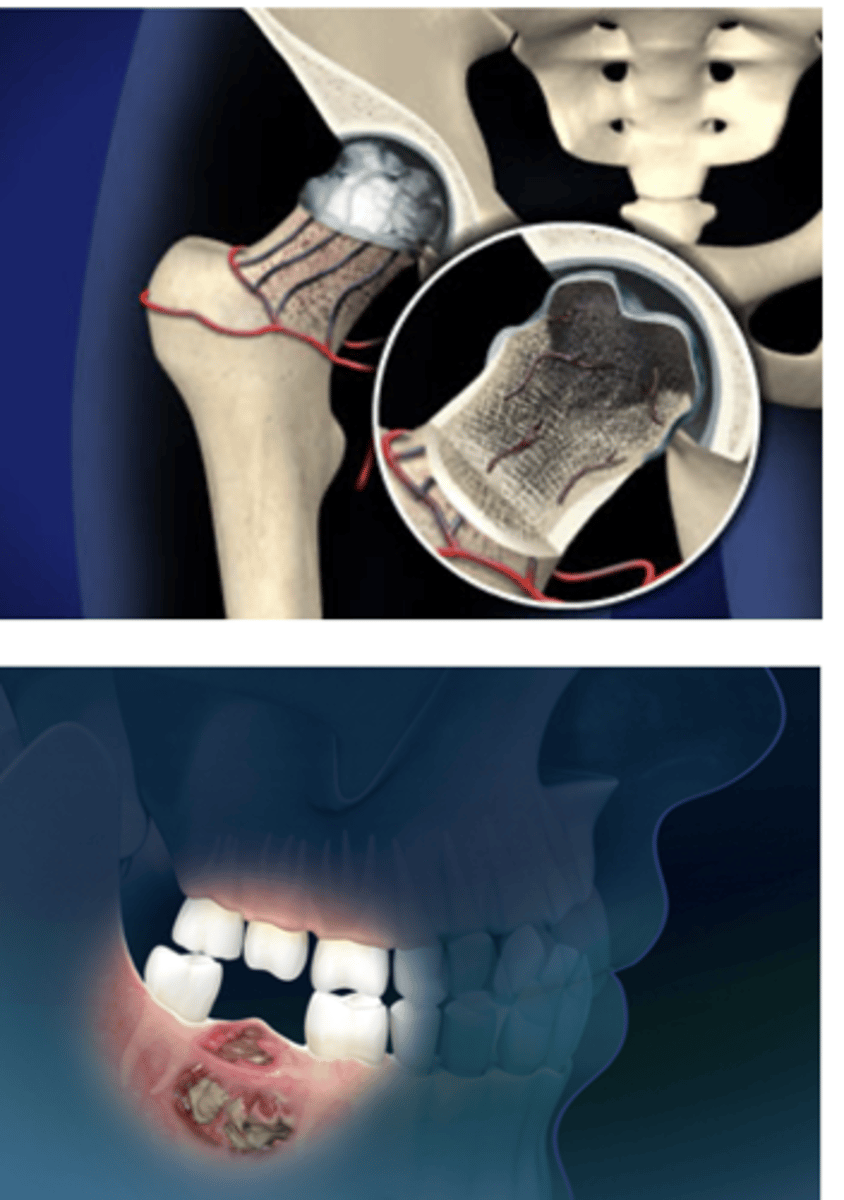
osteonecrosis
Aseptic destruction of a segment of bone due to an interruption in blood flow
Sites with poor collateral circulation (e.g., femoral head) are most commonly affected
Symptoms:
- Depend on location & severity
- Pain with activity (can progress to pain at rest)
Treatment:
- Short-term immobilization or limited weight-bearing
- Exercises
- NSAIDs
- Advanced: total joint replacement
Jaw osteonecrosis risk increases with bisphosphonate therapy
Genu Varum (bowlegs)
outward bowing of knees (>1 in.) when medial malleoli are touching.
-- May require bracing after 2 years old
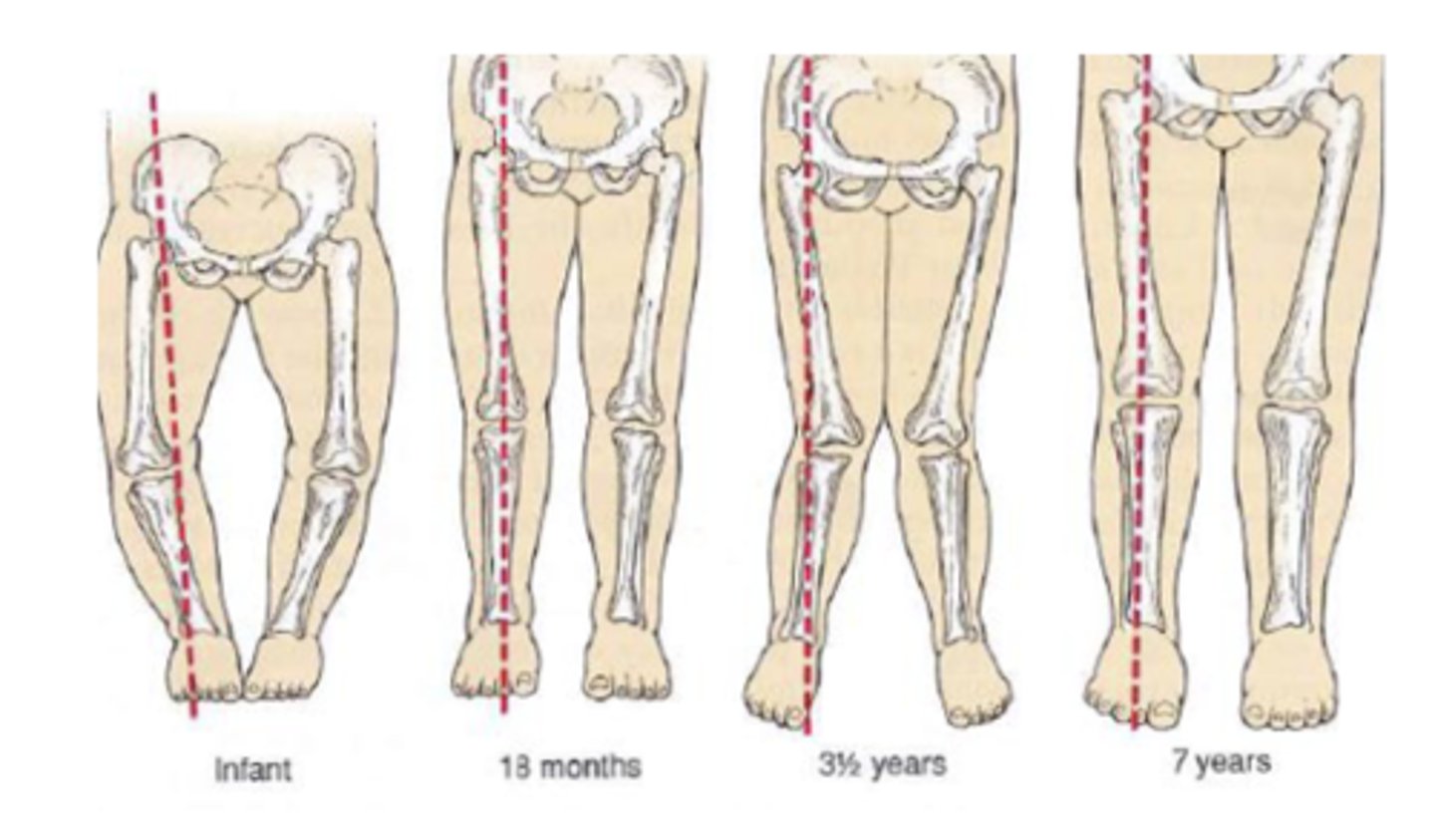
Genu Valgum (knock-knees)
medial malleoli do not touch when knees touch.
- Common at age 3-4
- May require exercise, surgery as treatments if not resolved by 7 years old
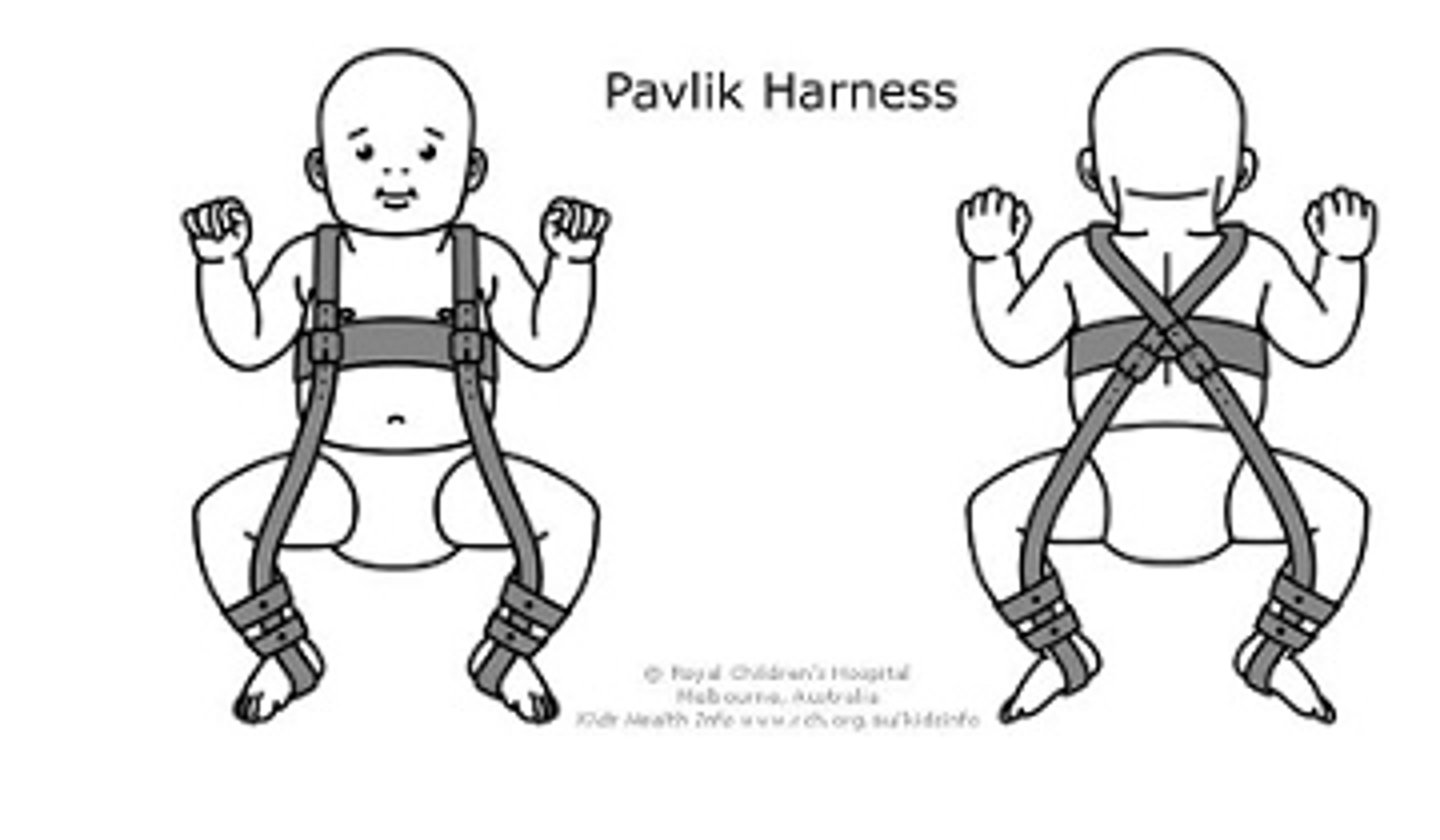
Developmental Hip Dysplasia
Screening: Ortolani test
Flex/abduct hips
Should be equal, produce no click
Treatment: Pavlik harness
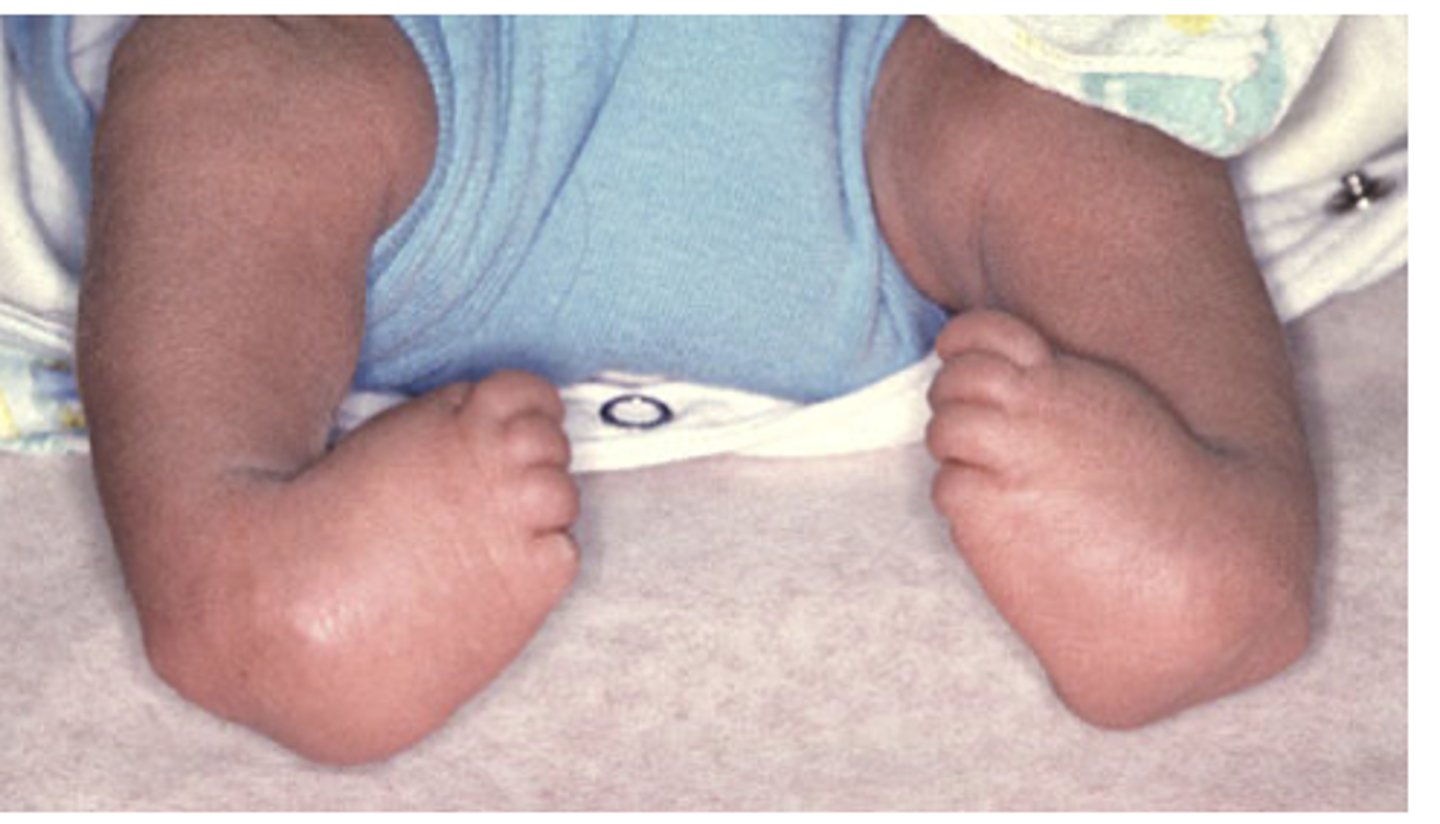
Congenital Clubfoot
One of the most common pediatric orthopedic conditions
•Treated by manipulation, casting, surgery
Postural scoliosis
Small curve that corrects with bending. Corrected with passive and active exercises.
Complications
•Breathing problems (in severe scoliosis)
•Low back pain.
•Lower self-esteem.
•Persistent pain if there is wear and tear of the spine bones.
•Spine or nerve damage from an uncorrected curve or spinal surgery.
•Leakage of spinal fluid.
Structural scoliosis
Fixed deformity
Congenital (vertebral development)
Neuromuscular (cerebral palsy, DMD)
Idiopathic- majority
Complications
•Breathing problems (in severe scoliosis)
•Low back pain.
•Lower self-esteem.
•Persistent pain if there is wear and tear of the spine bones.
•Spine or nerve damage from an uncorrected curve or spinal surgery.
•Leakage of spinal fluid.

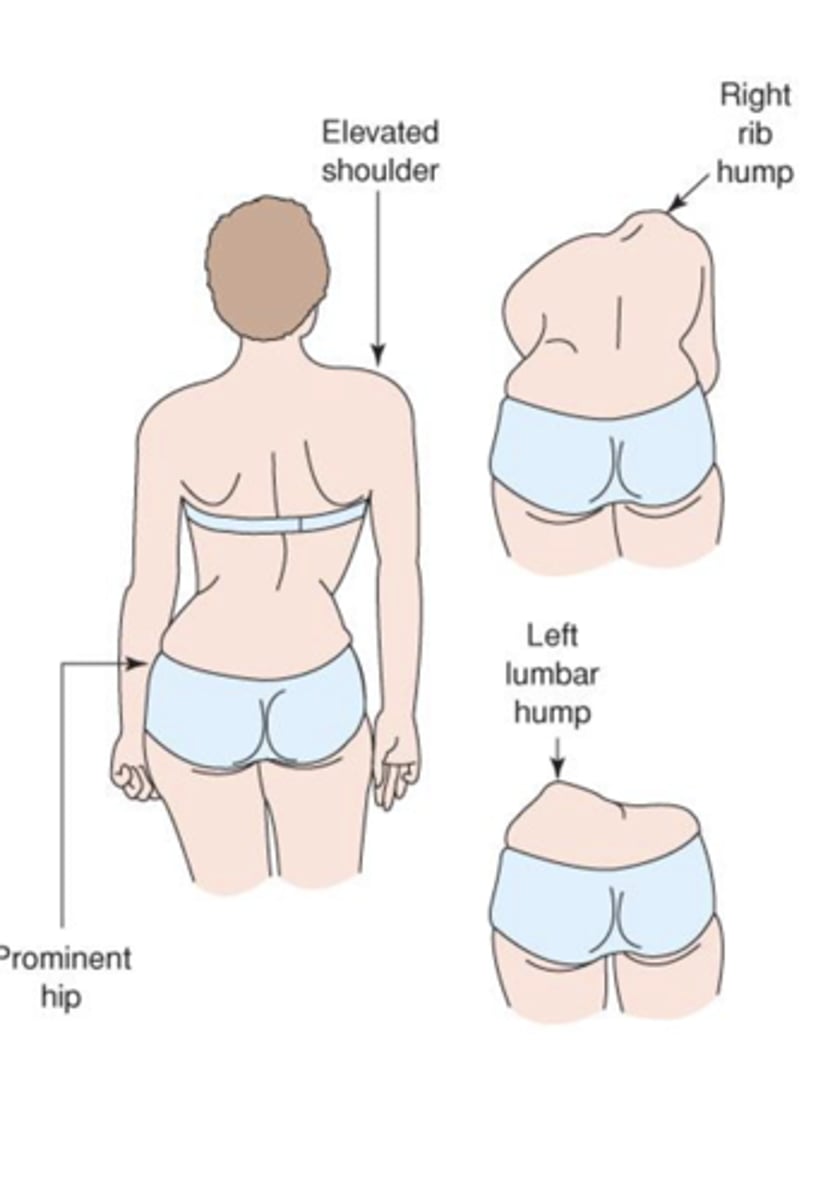
thoracic vs lumbar scoliosis
Cardinal signs of scoliosis
Uneven shoulders or iliac crest
Prominent scapula on convex side of curve
Asymmetry of thoracic cage
Treatments:
- Depend on severity and likelihood to progress
- Curves 20-30°: Considered
- Curves 30-40°: Bracing
- Curves 40-45°+: Surgery
which of the following best describes hematogenous osteomyelitis?
a. infection that enters through a penetrating wound
b. infection spreading from nearby soft tissue
c. infection that originates from organisms in the bloodstream
d. infection introduced during surgery
c. infection that originates from organisms in the bloodstream
which of the following is the most common form of scoliosis?
a. congenital
b. neuromuscular
c. idiopathic
d. postural
c. idiopathic