Diagnostics- Radiology
1/93
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
94 Terms
AP positioning
A->P
taken from the front
ex: bedside
PA positioning
P->A
taken from the back
best for chest x-rays
Lateral positioning
From the pt side
Left -> Right
Decubitus position
x-ray taken while pt is laying on the side
best for looking at fluid layering
Oblique positioning
x-ray taken at a 45 degree angle
x-ray
white: opaque
(bone, metal, fluid)
CT
white: increased attenuation (hyperdense)
MRI
white: increased signal intensity
(fat, bone marrow)
nuclear medicine
white: increased tracer uptake
(tumor, bleeding)
barium studies
white: radioplaque
ultrasound
white: hyperechoic
(bone, gas)
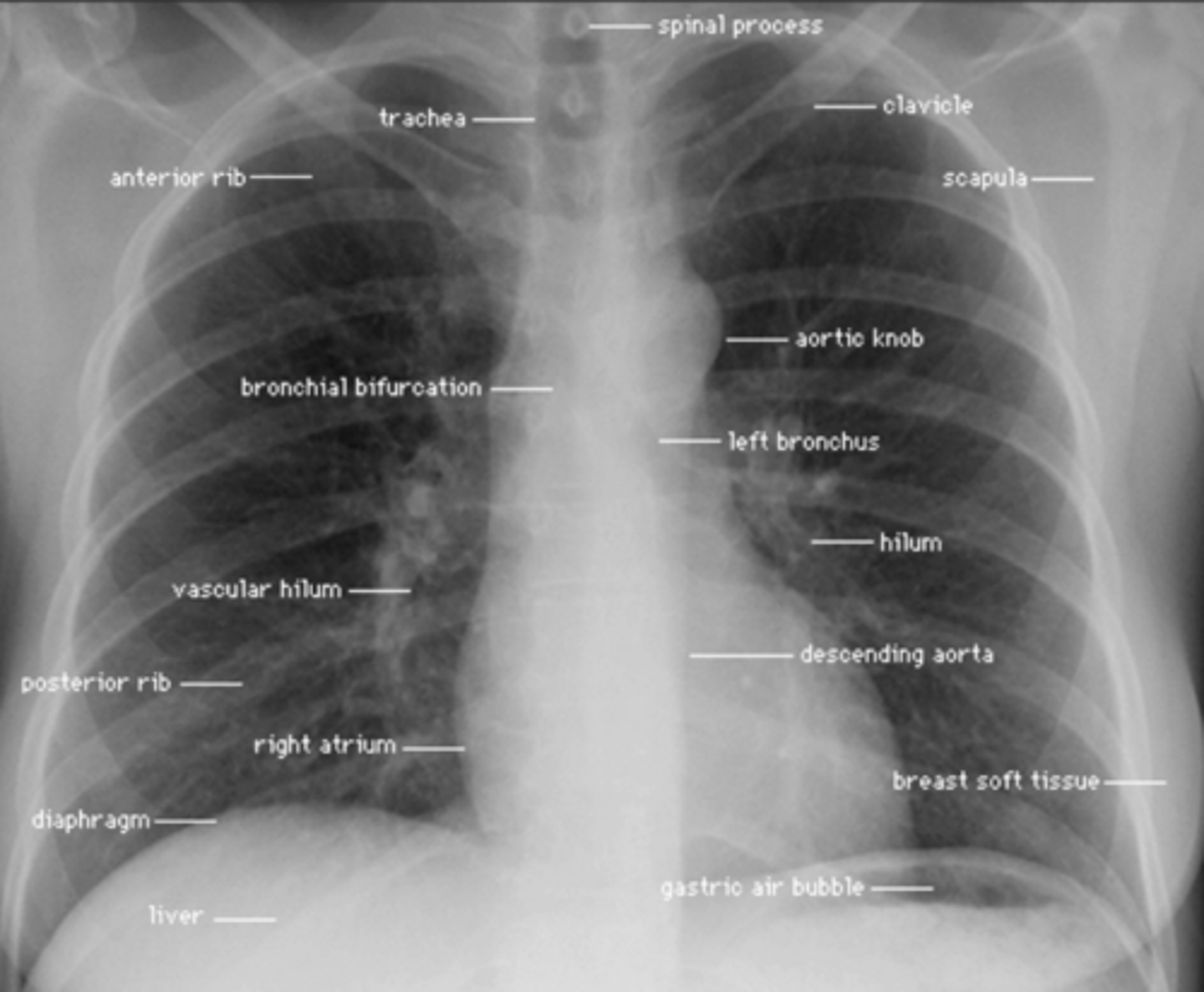
frontal x-ray
A: airways (trachea, bronchi)
B: bones (clavicle, ribs)
C: cardiac (position and structures)
D: diaphragm (angle, elevation, effusion)
E: extras
lateral x-ray
retrosternal angle: the space behind the sternum (dark)
hilar region: triangular depression of the bronchus
fissures
-R/L major fissure only in lateral view
-R minor fissure in both lateral and anterior view
thoracic spine: should get darker more inferiorly
diaphragm
normal abdominal x-ray
air/fluid level:
no more than 2-3 in the small bowel
none in large bowel
distension is <2.5 cm small bowel and <6.0 large bowel
DISTENSION IS NORMAL
stool (appears cloudy)
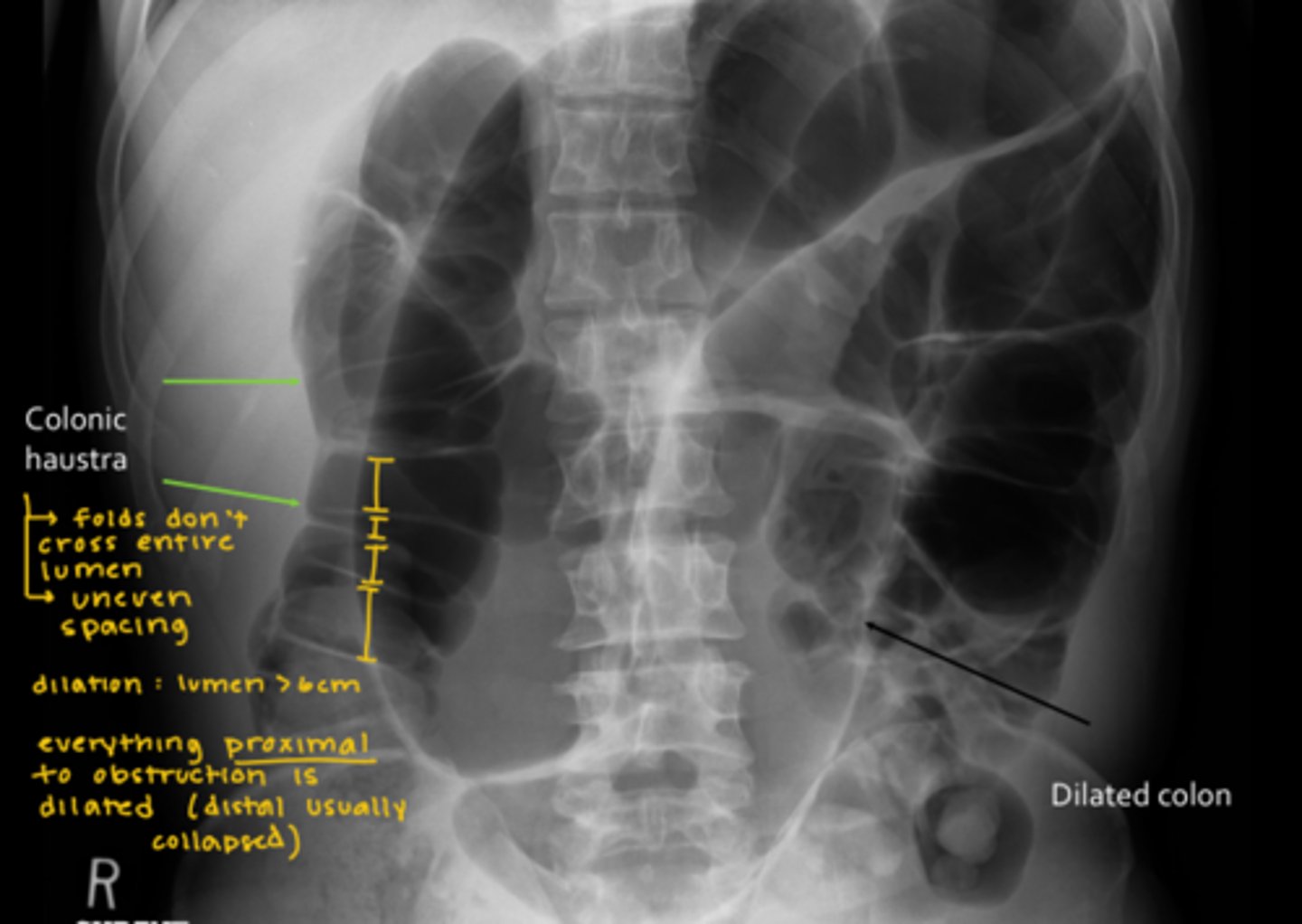
abnormal abdominal x-ray
DILATION IS ABNORMAL
>2.5 small bowel and >6.0 large bowl
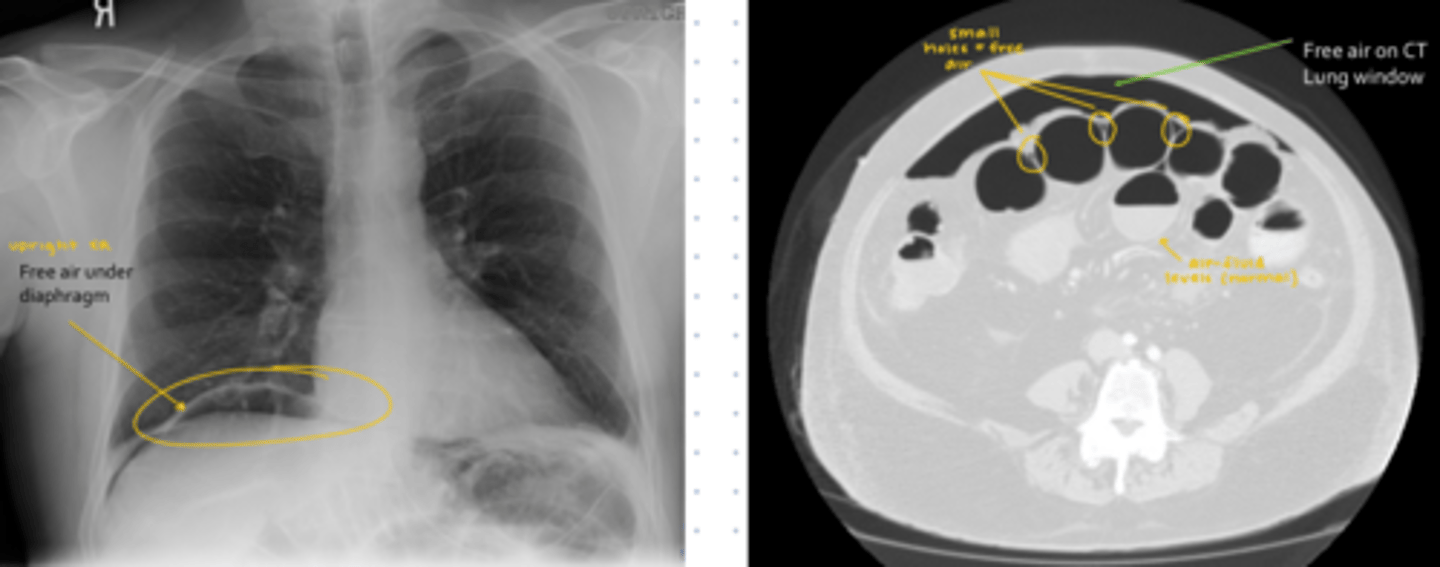
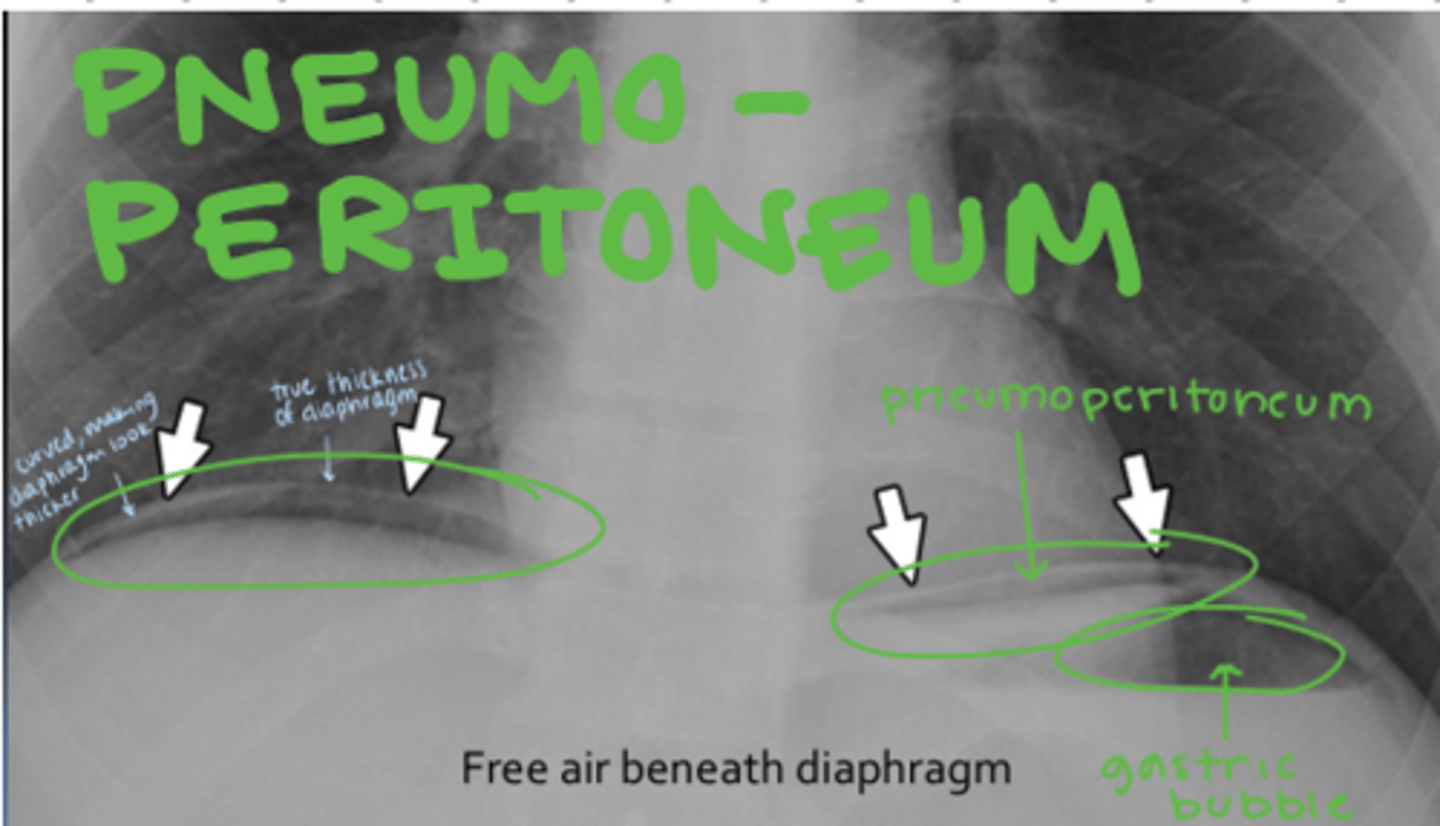
free air under the diaphragm (pneumoperitoneum)
calcification
ideal minimum # of view for plain films
chest: 2 (PA most ideal)
extremities: 2
spine: 3 (lateral most ideal)
X-ray
best uses: QUICK chest, abdominal, orthopedic pathology, foreign body, GI screening
benefits: portable and common
contraindications: none
limitations: less detailed
ultrasound (US)
best uses: superficial structures (ex: female pelvis), blood flow, "small structures"
benefits: cheap, low-risk
contraindications: none
limitations: deep structures are harder to view
CT
best uses: acute head pathology, abdominal/pelvic pathology, trauma, chest pathology, ortho workup
benefits: detailed
contraindications: radiation (impacts pregnant women) and possible allergy to IV contrast (CKD)
limitations: not portable
MRI
giant magnet, not portable
organ specific: brain, spinal cord, joints
white on MRI: fat, fluid
nuclear medicine
radioisotopes tagged to agents
NOT for pregnant
assesses function of organs, detect malignancy, evaluates for transplant rejection
black: increased radioactive uptake
interventional radiology
minimally invasive procedures using pictures
dilated large bowel
-uneven spacing, >6.0 cm
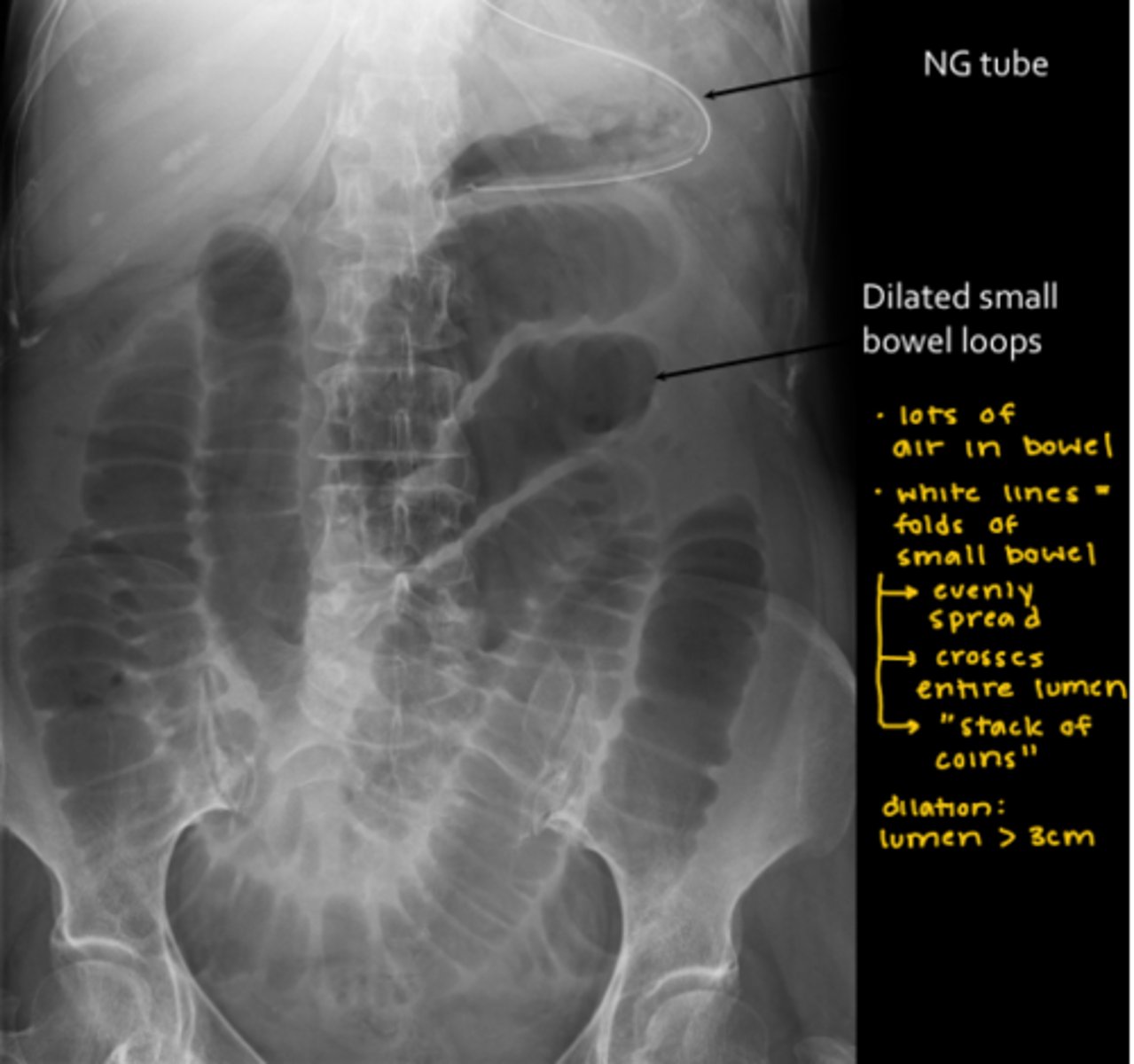
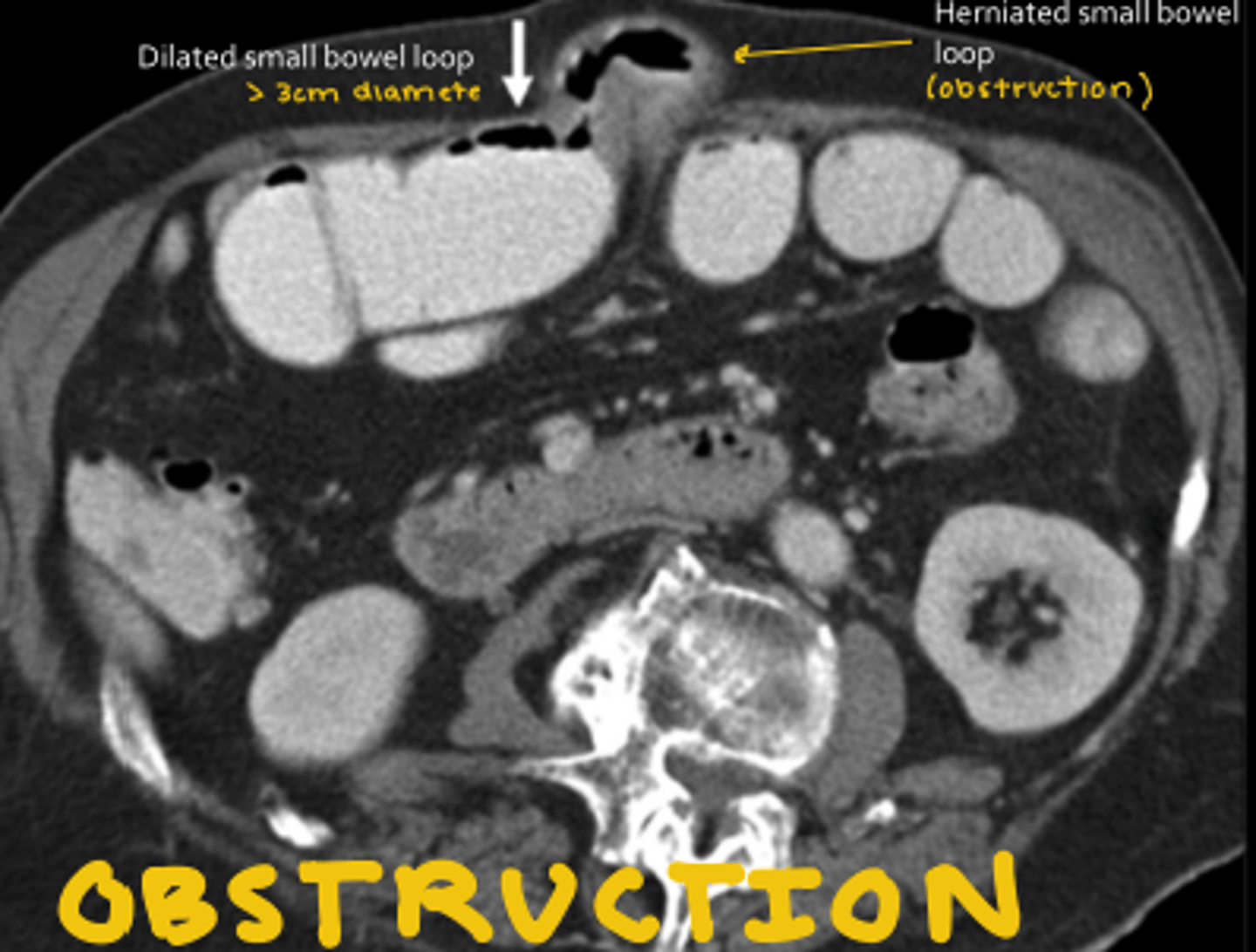
dilated small bowel
-"stack of pennies", >2.5 cm
Best modality for free air?
CT
How free air appears on plain film and CT
Best uses for US and CT in abdomen/ pelvis
US: "small parts" female reproduction, gall bladder, ectopic pregnancy, scrotom for torsion
CT: major organs, free fluid, bowel, cancer, trauma
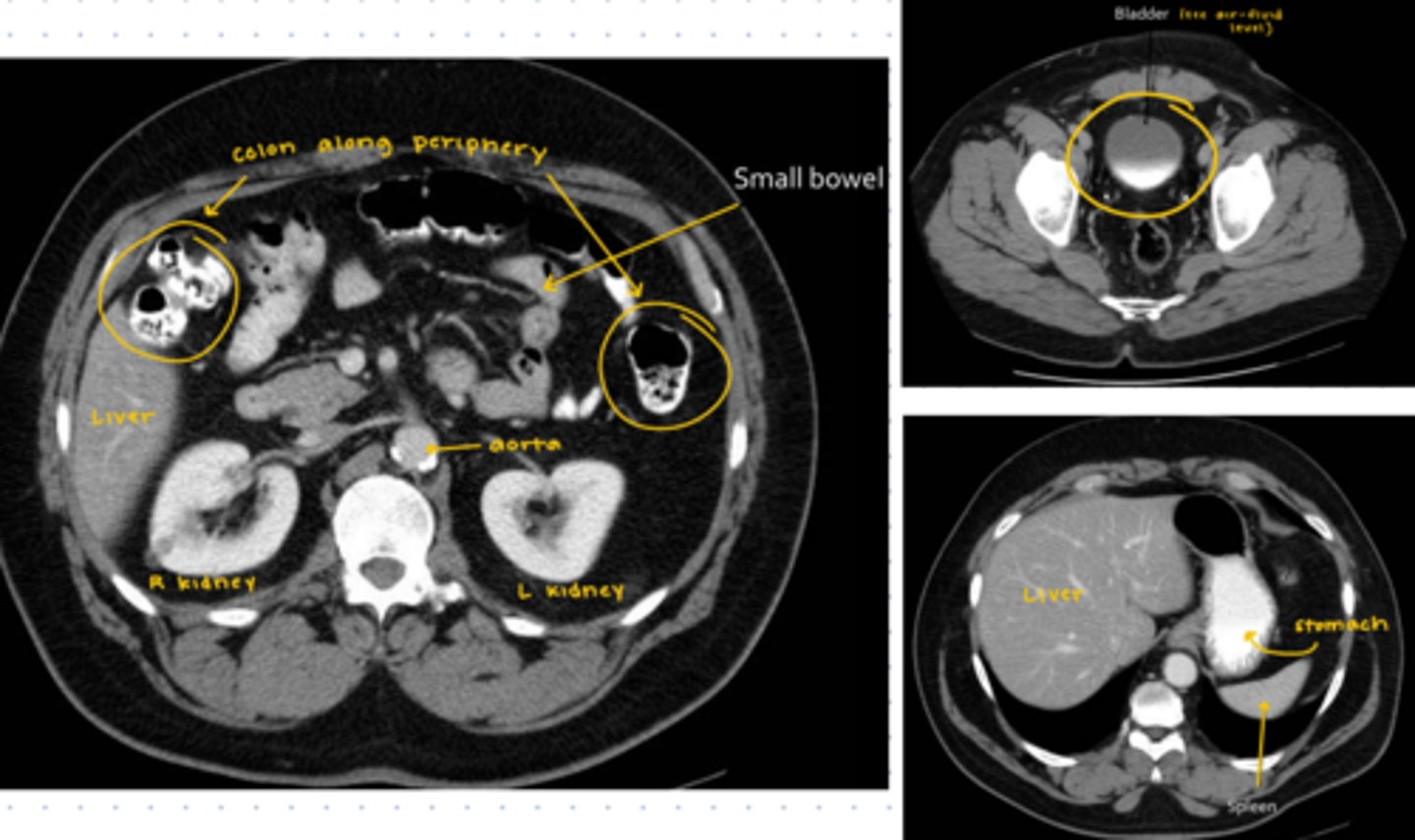
Recognize the abdomen CT scan
-liver, spleen, colon, small bowel, aorta, kidneys, bladder
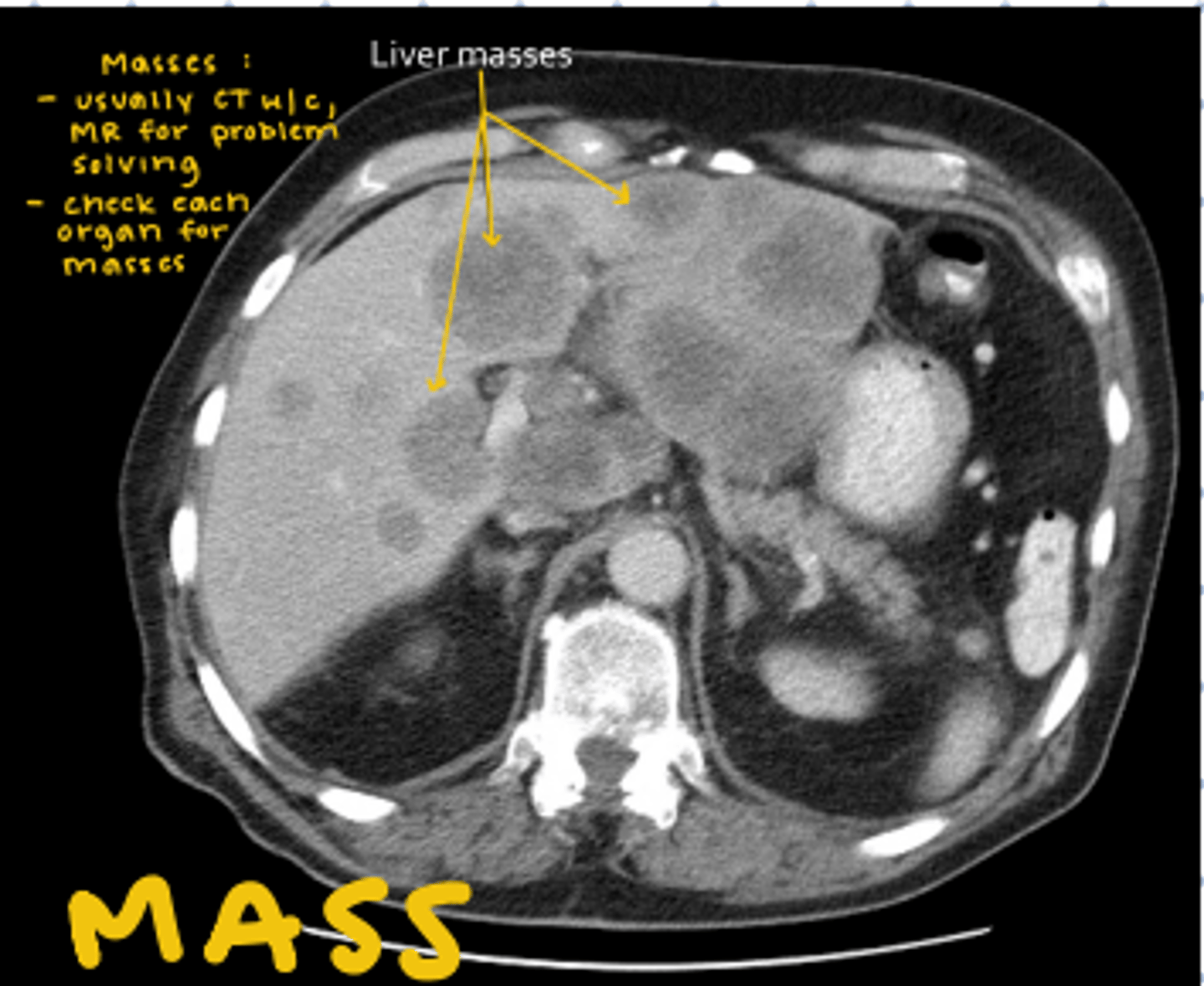
Mass in abdomen
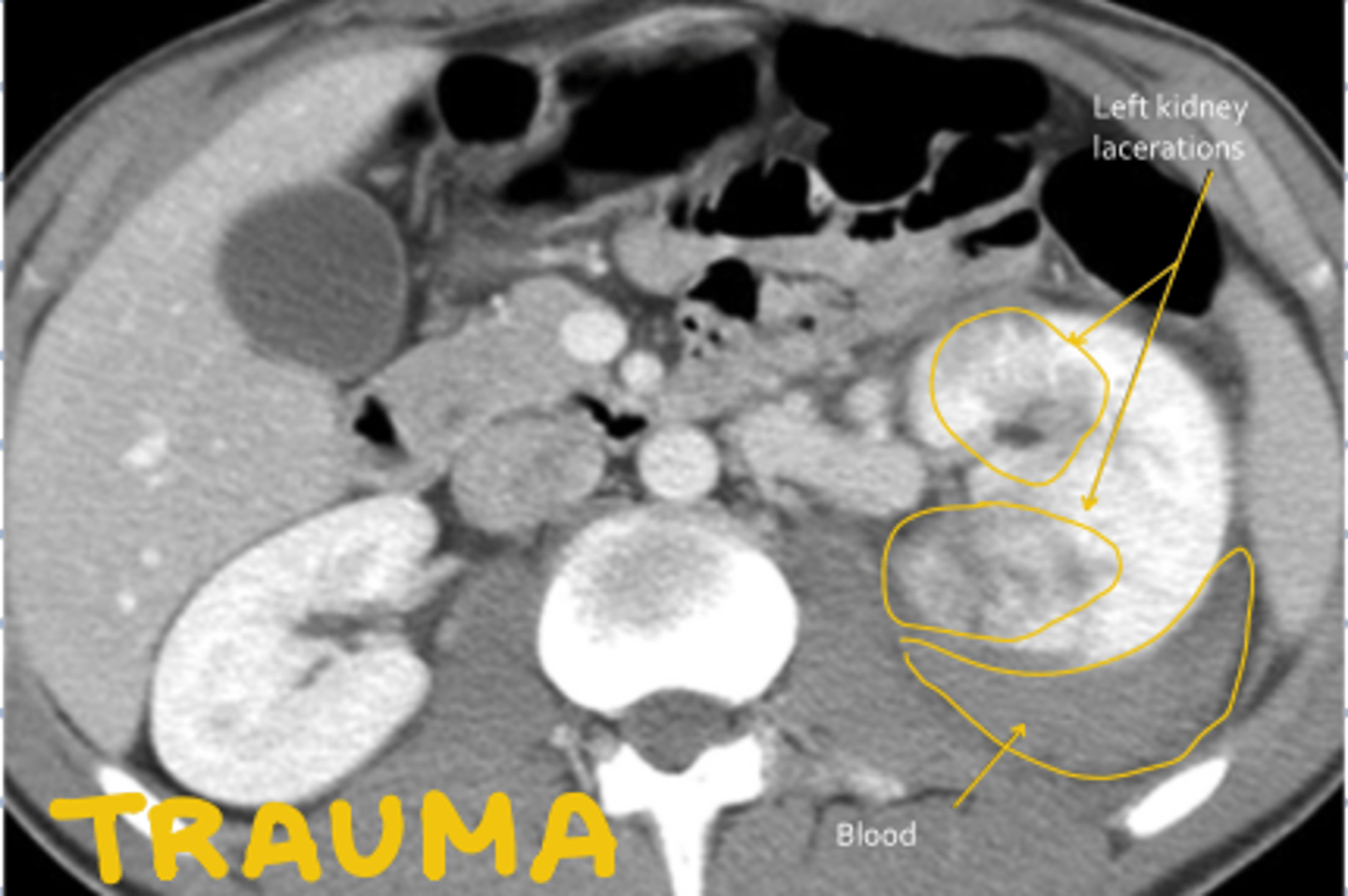
Trauma in abdomen
obstruction in abdomen
-aka hernia
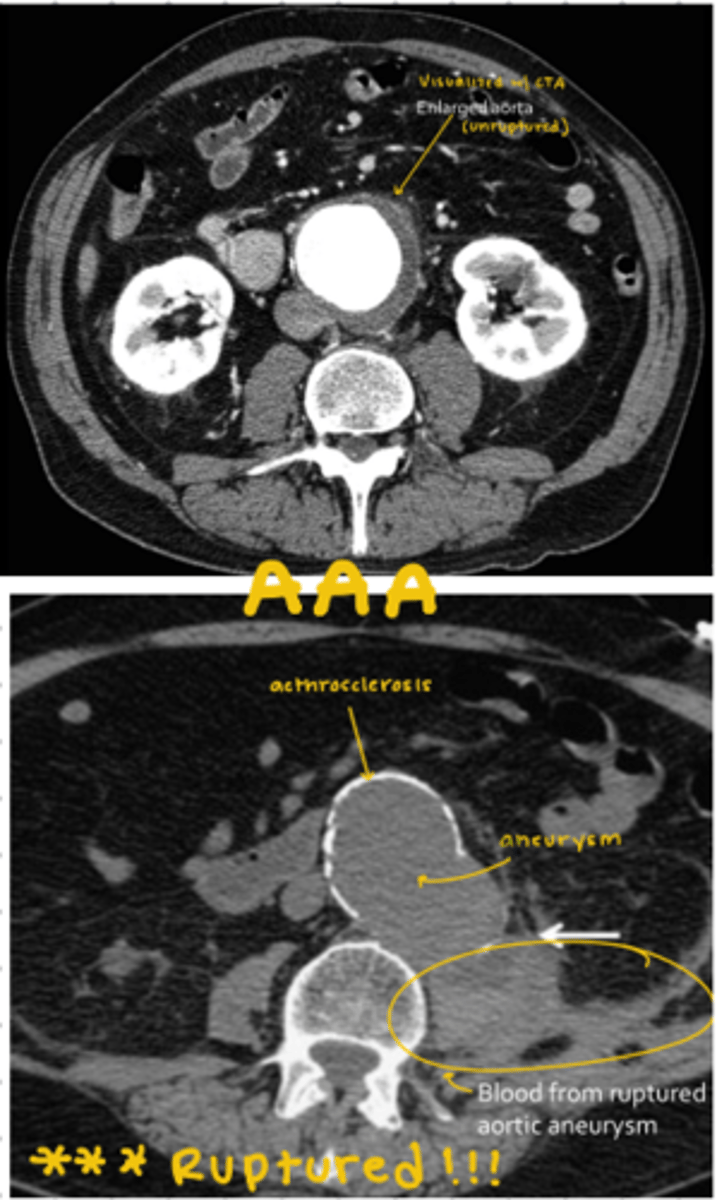
AAA
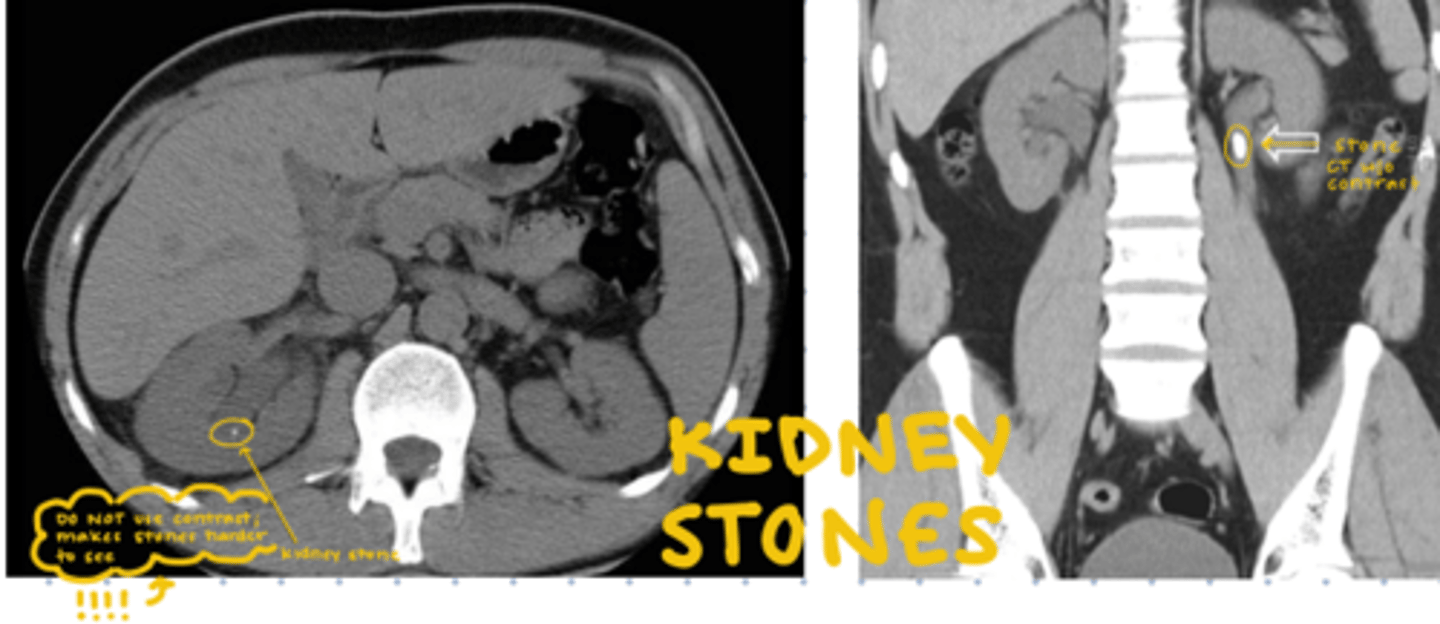
kidney stones
-don't use contrast
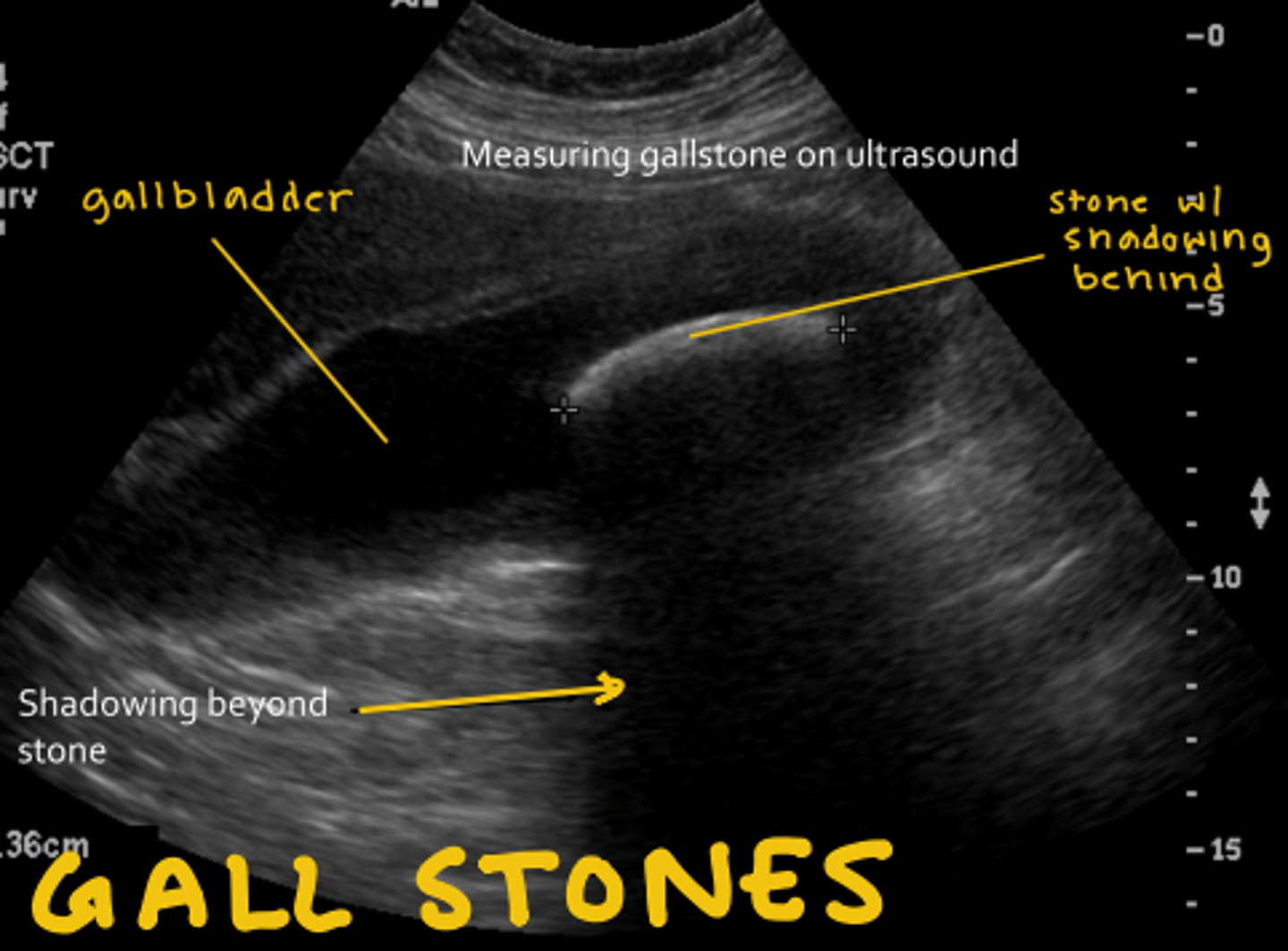
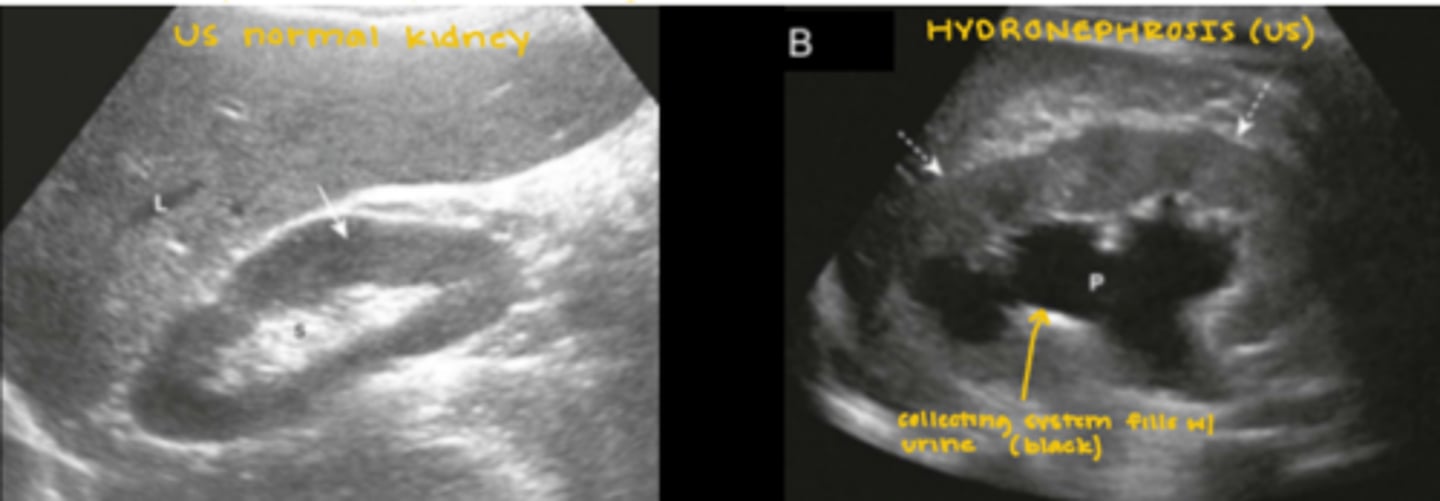
gallstone on US
-has shadowing behind
hydronephrosis on US
simple pancreatitis
needs no imaging (also UTI and hepatitis)
conditions that require imaging
-cholecystitis (US, NM)
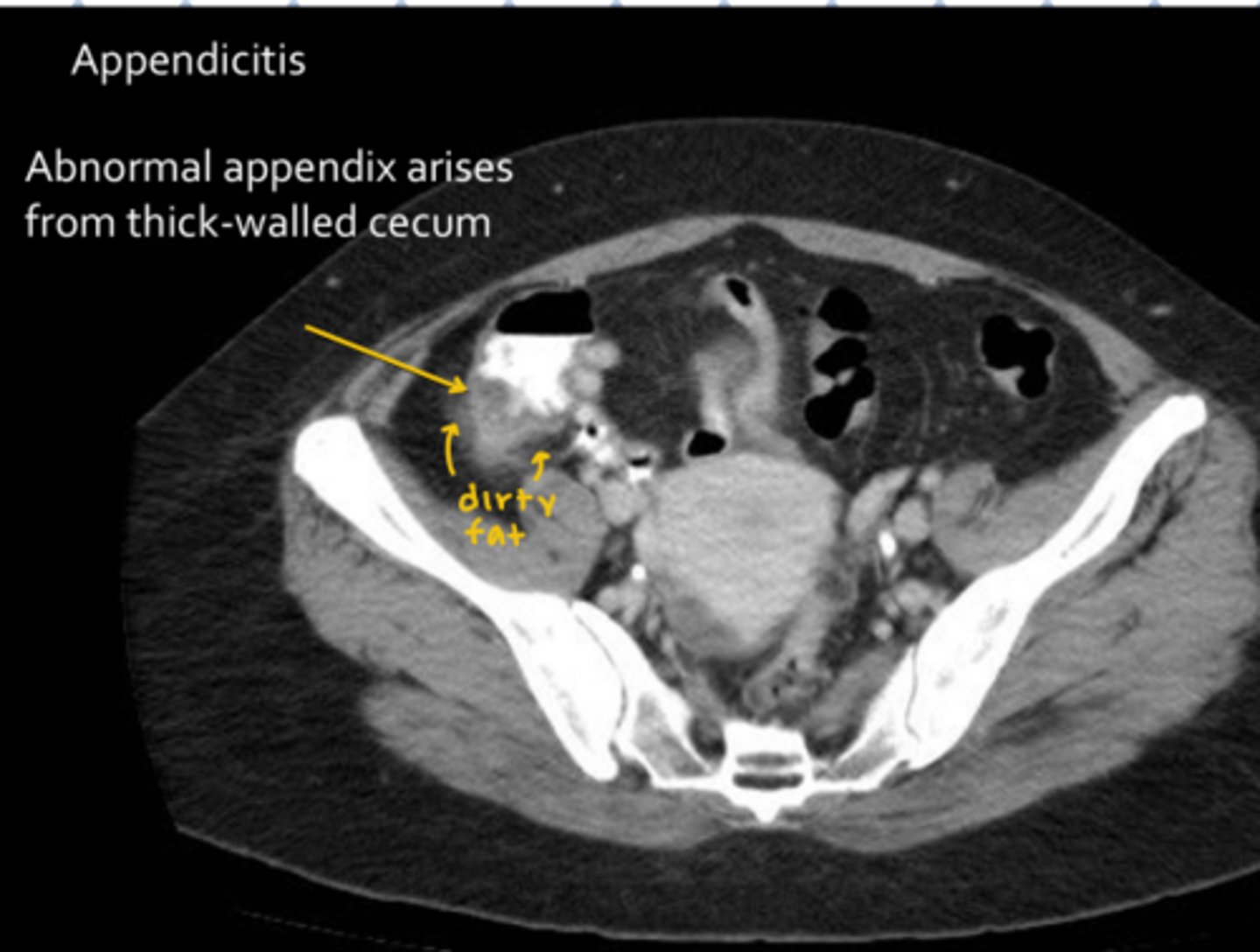
-appendicitis (CT)
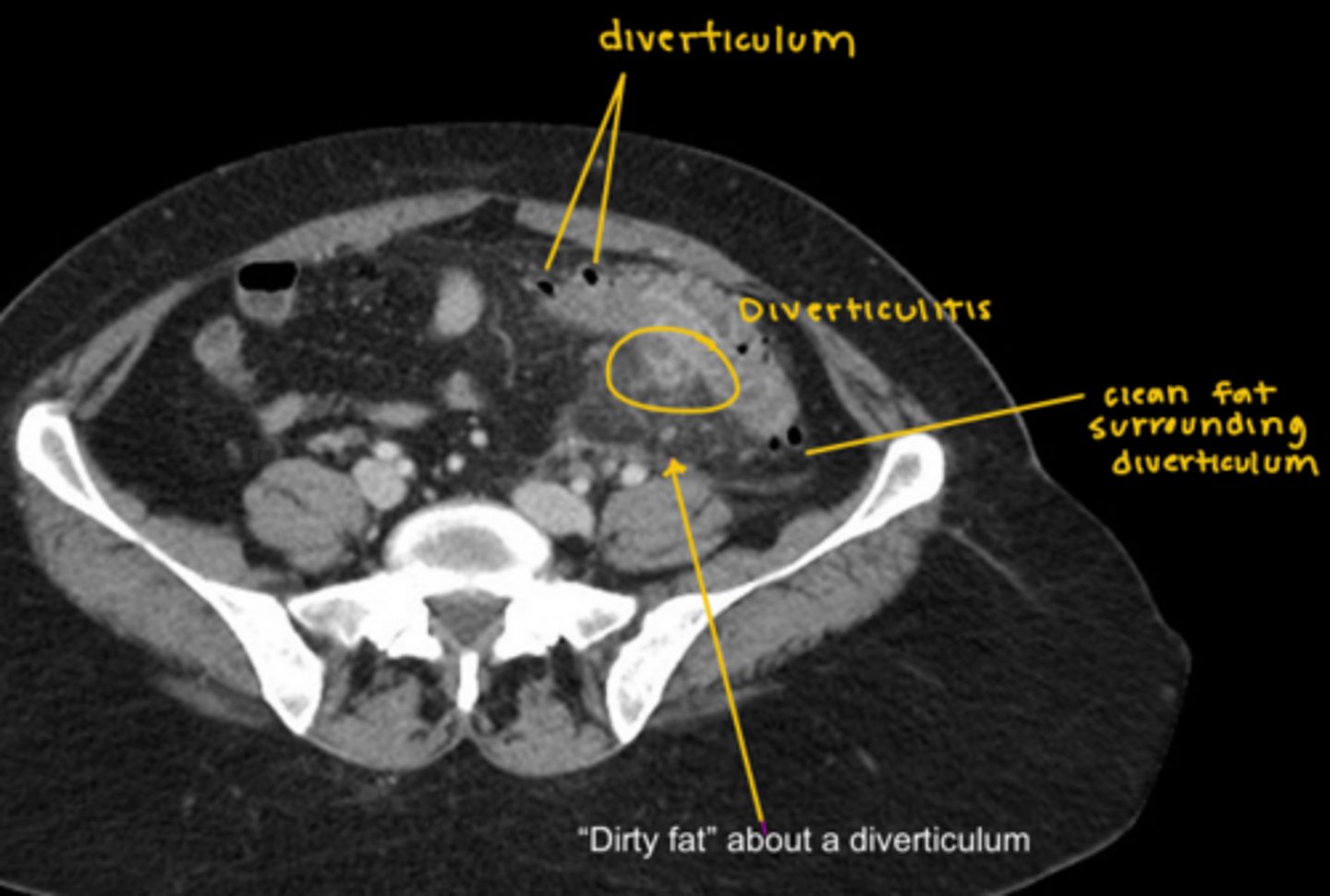
-diverticulitis (CT)
Appendicitis CT
Diverticulitis CT
For chest radiology, plain films are usually first
When to move onto CT:
-abnormal x-ray
-persistent infiltrate
-trauma
-pulmonary embolus
-aorta
-cancer work-up
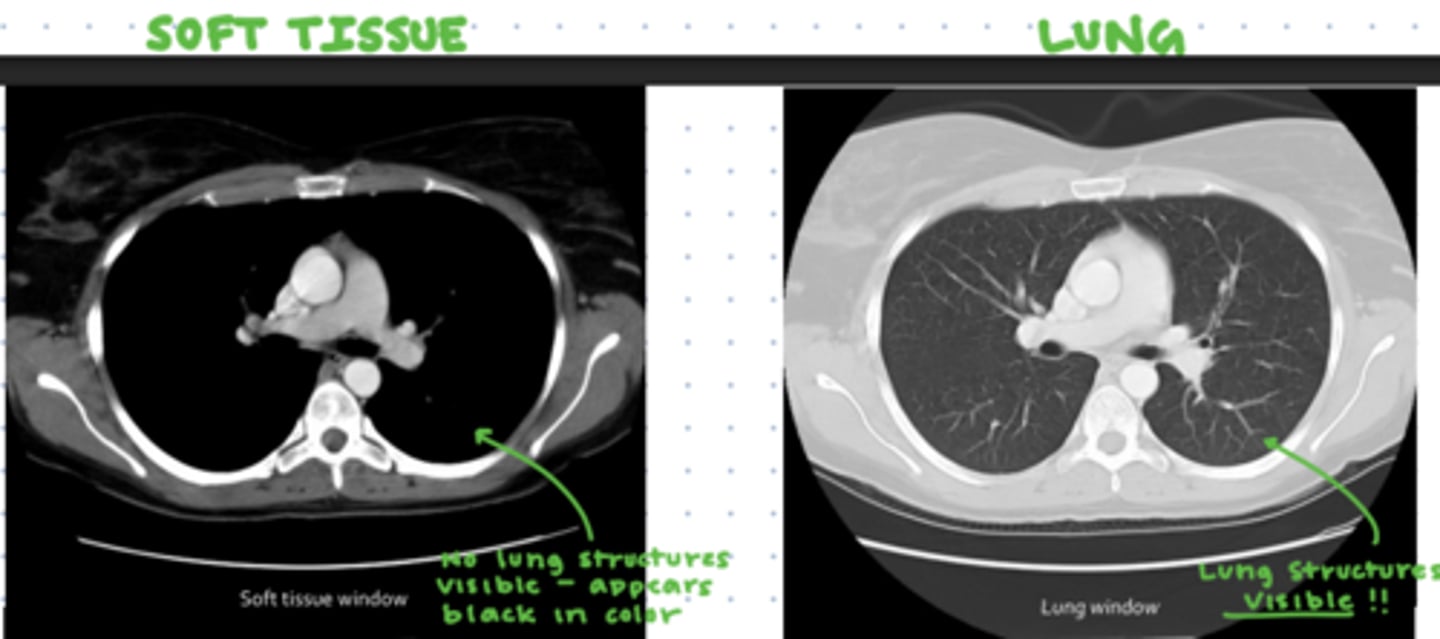
Soft tissue v. Lung windows on CT
Identify chest CT anatomy
-lungs
-esophagus
-trachea
-major and minor fissures
-heart
-aortic arch
-ascending and descending aorta
-aorto-pulmonary (AP) window
-R and L main bronchi
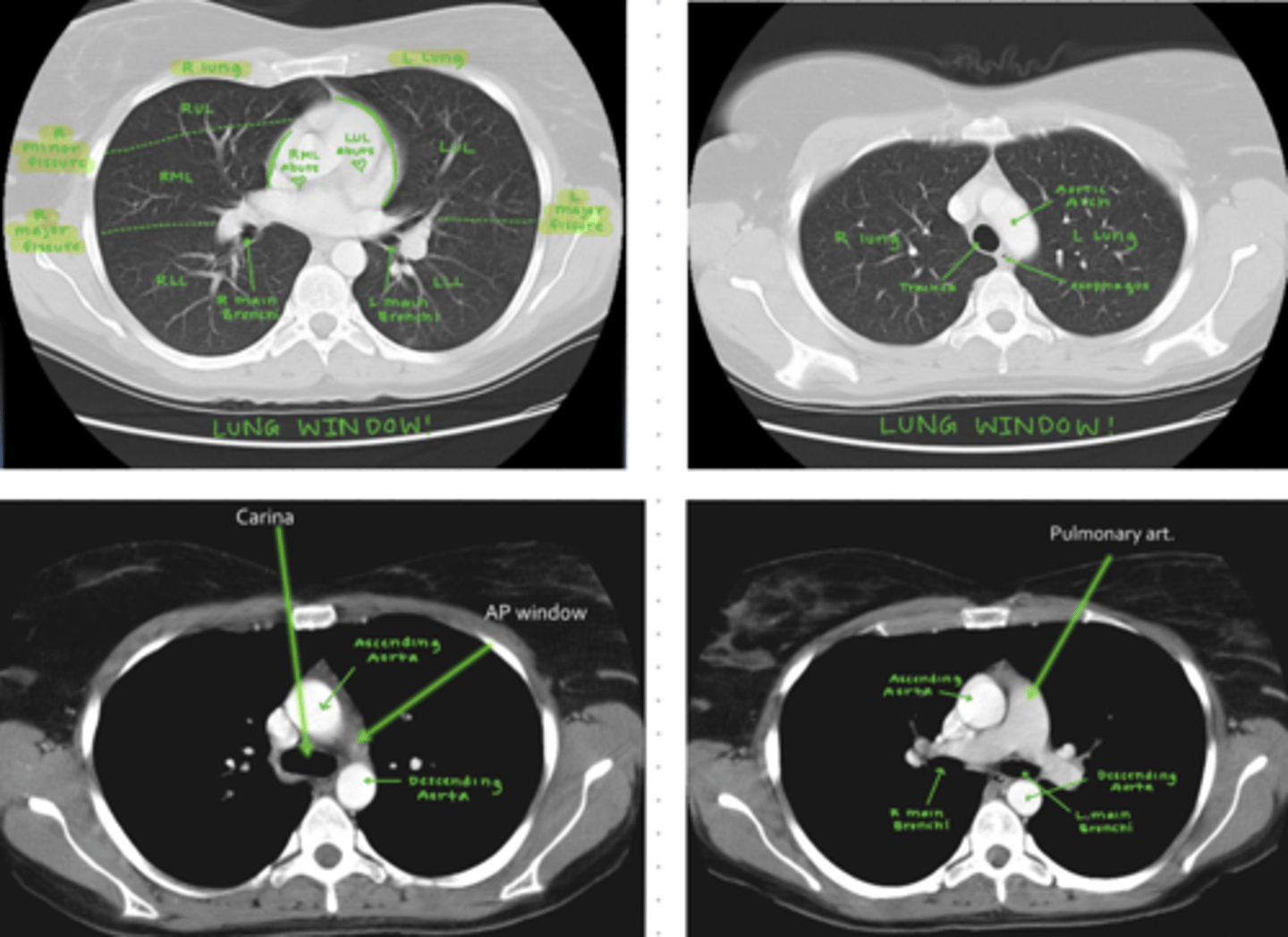
lung structures as they pertain to heart borders
RML abuts R heart border
LUL (lingula!) abuts L heart border
Importance of spine appearance in evaluating lung pathology on a lateral chest x-ray
spine should get darker moving inferiorly and spacing between vertebrae should be even
doesn't get darker: opacity in LLL
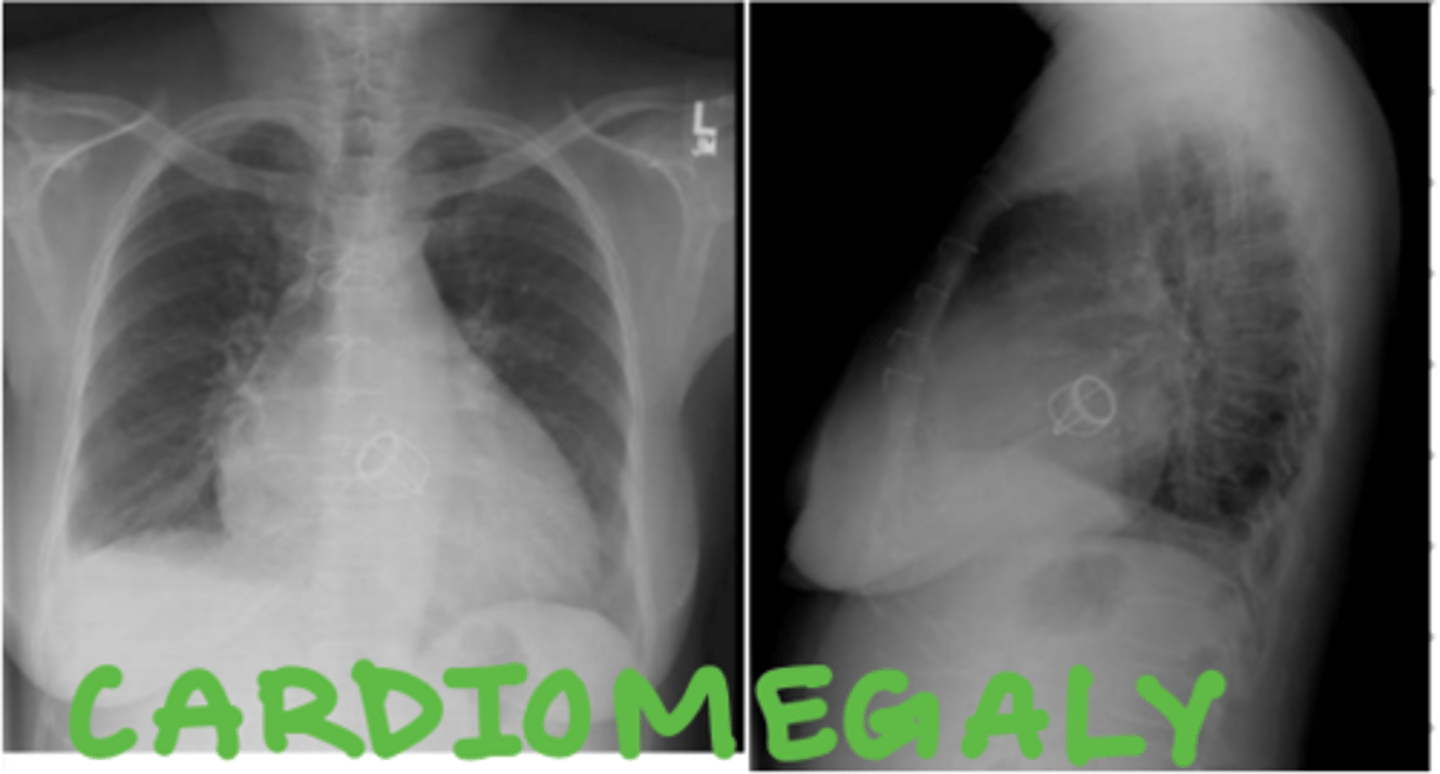
cardiomegaly
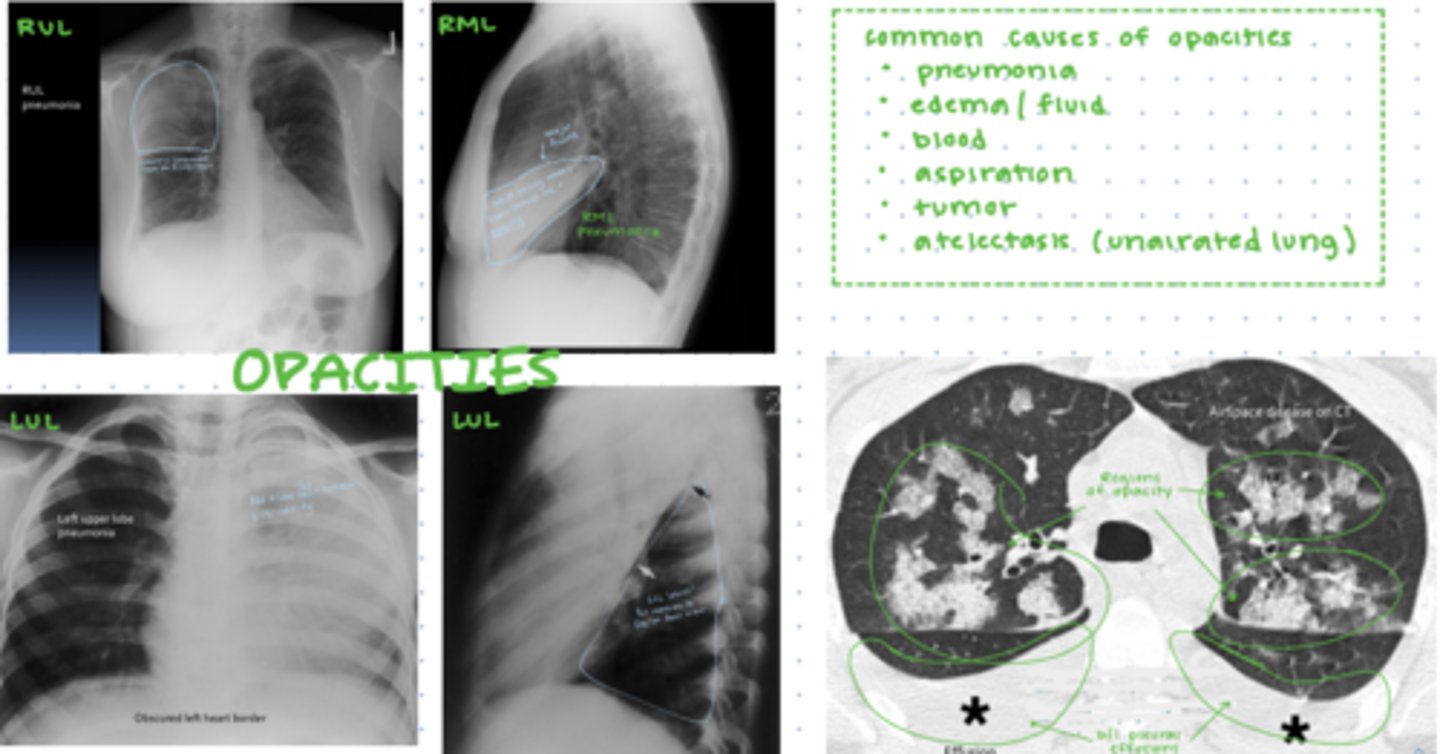
opacities
could be due to: pneumonia, edema, blood, aspiration, tumor, atelectasis
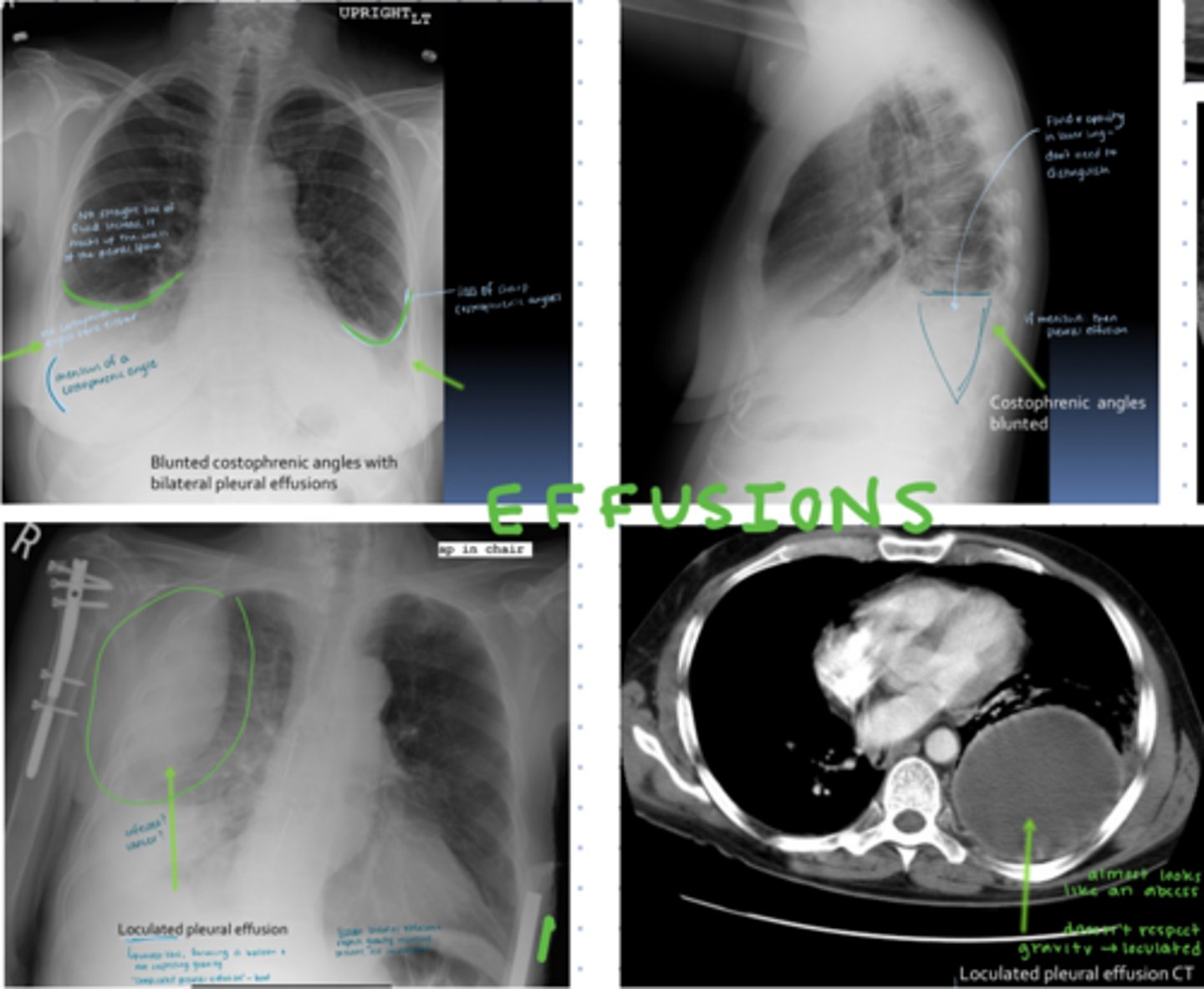
effusions
-costophrenic angles blunted
-opacity with menisci
simple: respect gravity
lobulated: does not respect gravity
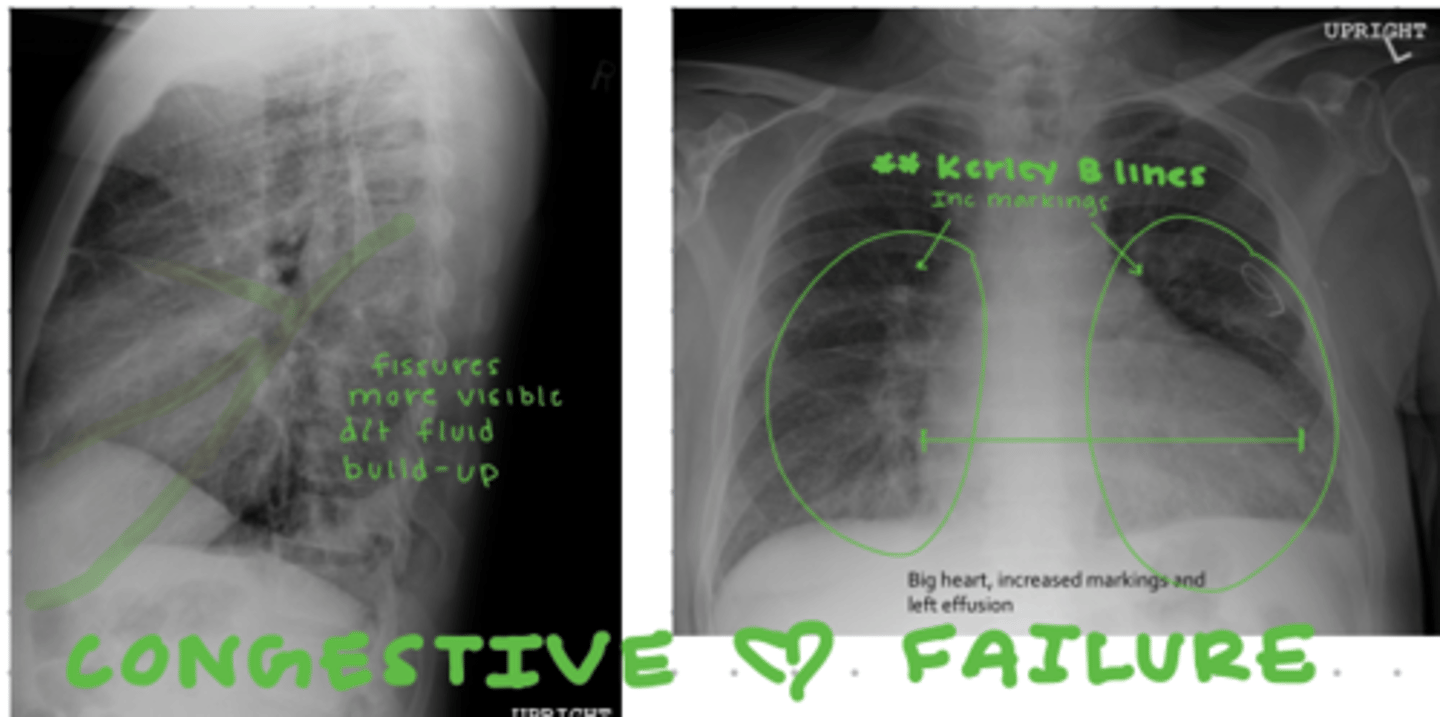
heart failure
-enlarged heart
-thickened fissures
-Kerley B lines
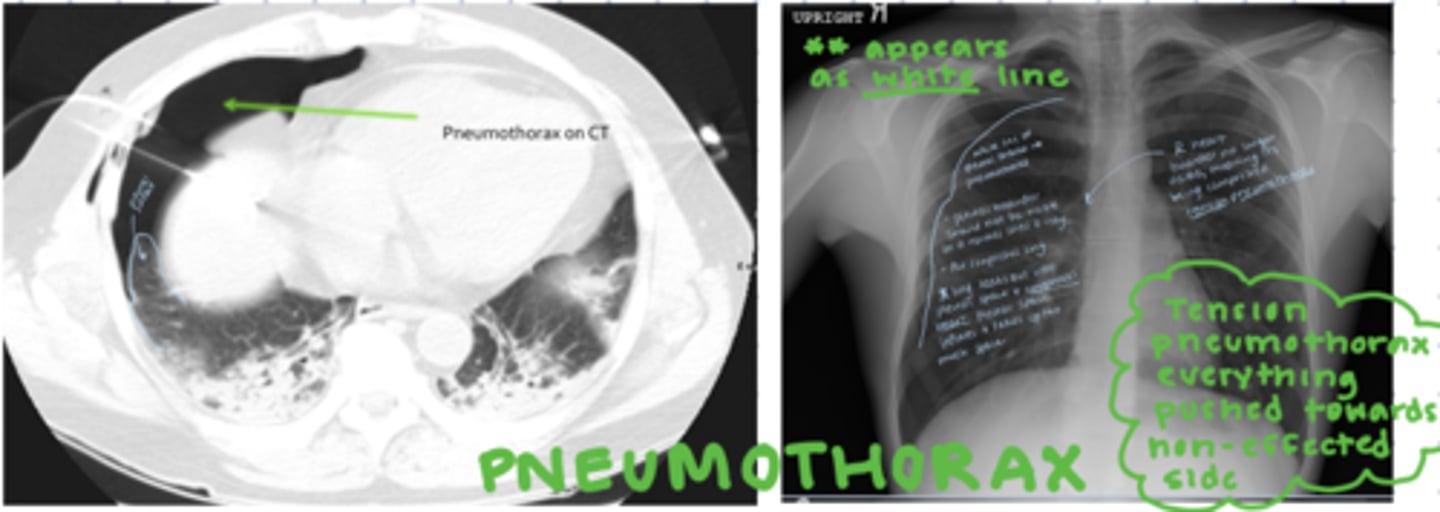
lung collapse/pneumothorax
-pleural border appears as white line
-AIR COMPRESSES
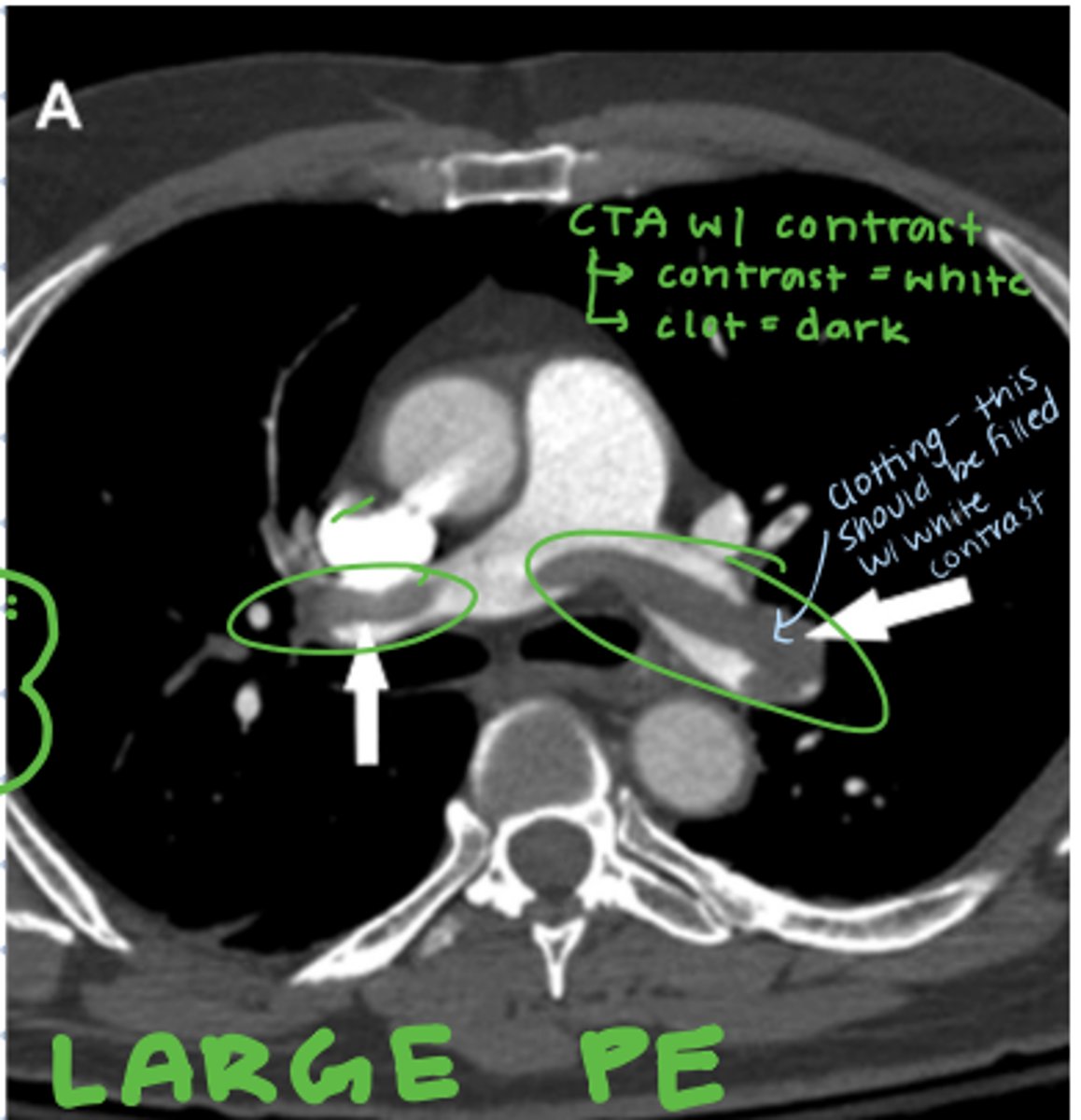
large PE
-clotting near heart
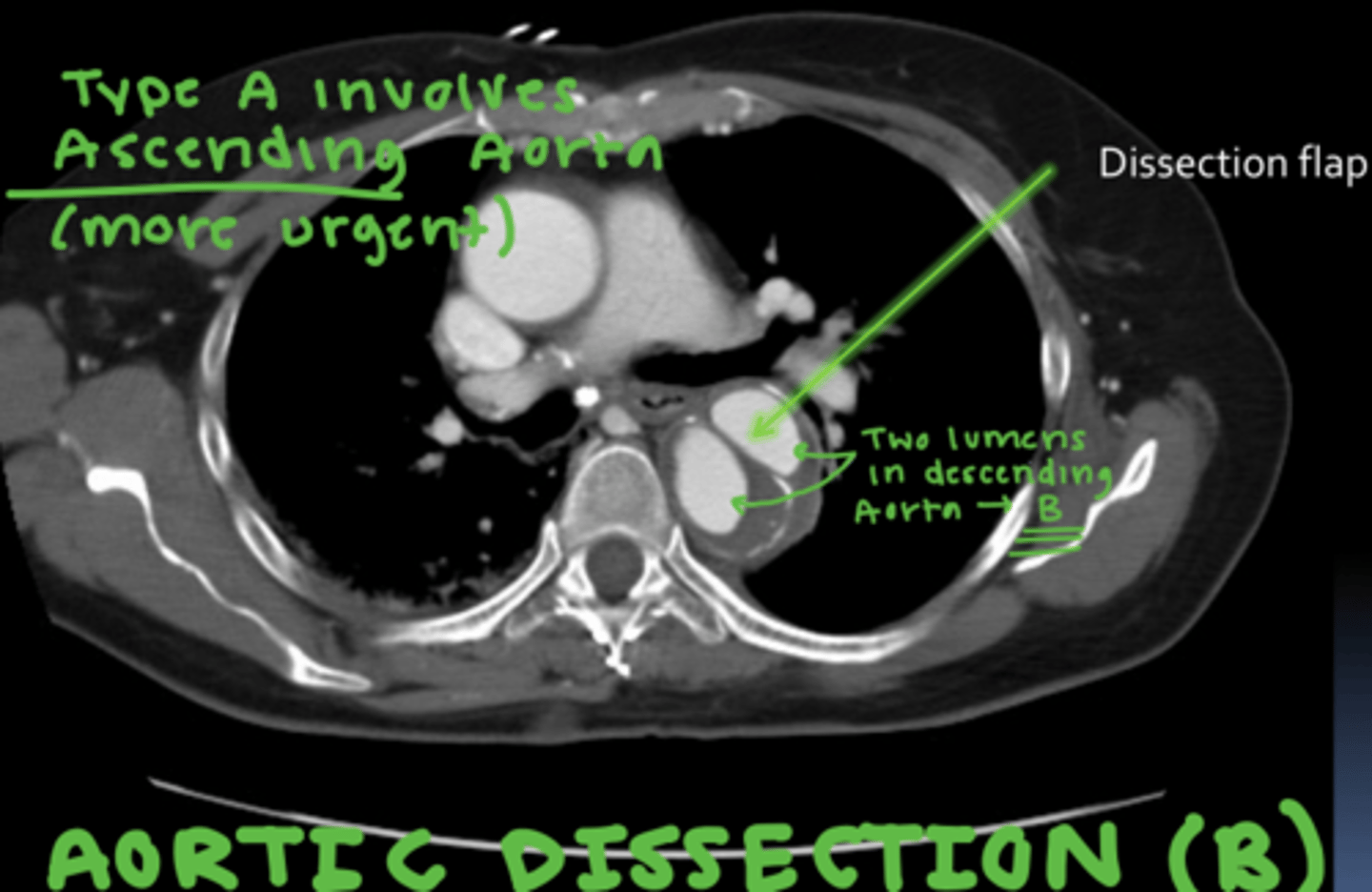
aortic dissection
-splitting into 2 lumens of aorta
A: ascending aorta
B: descending aorta
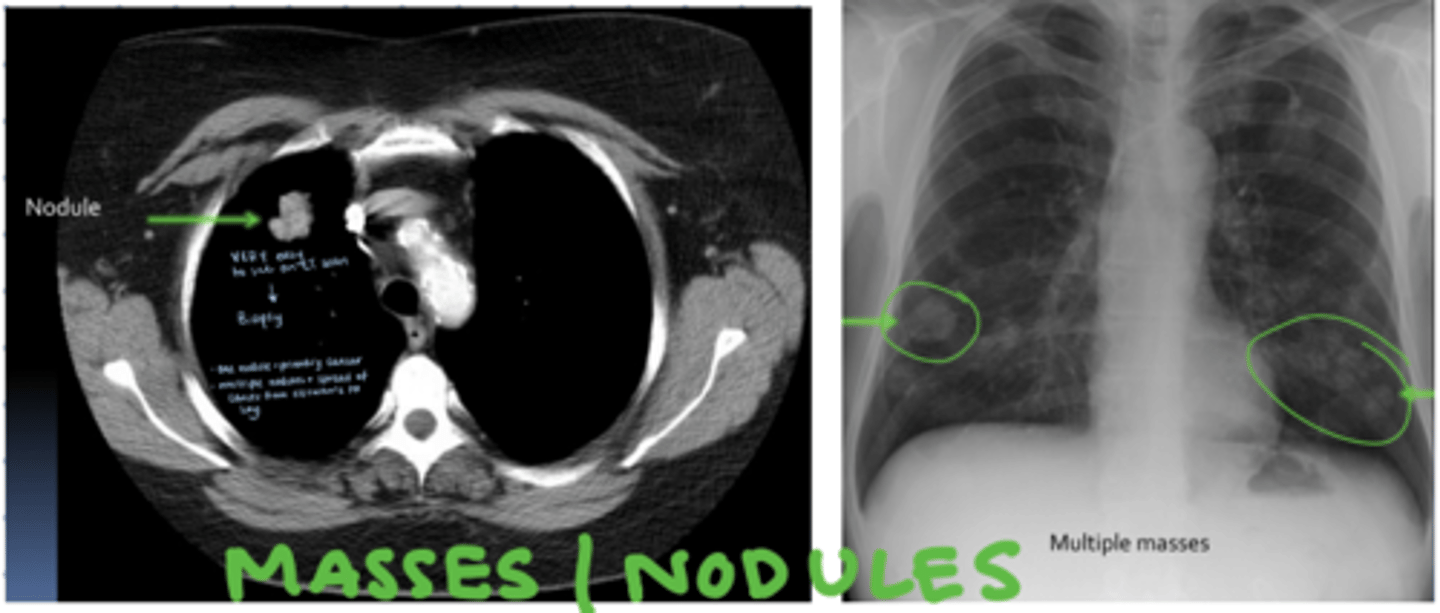
lung nodules/masses
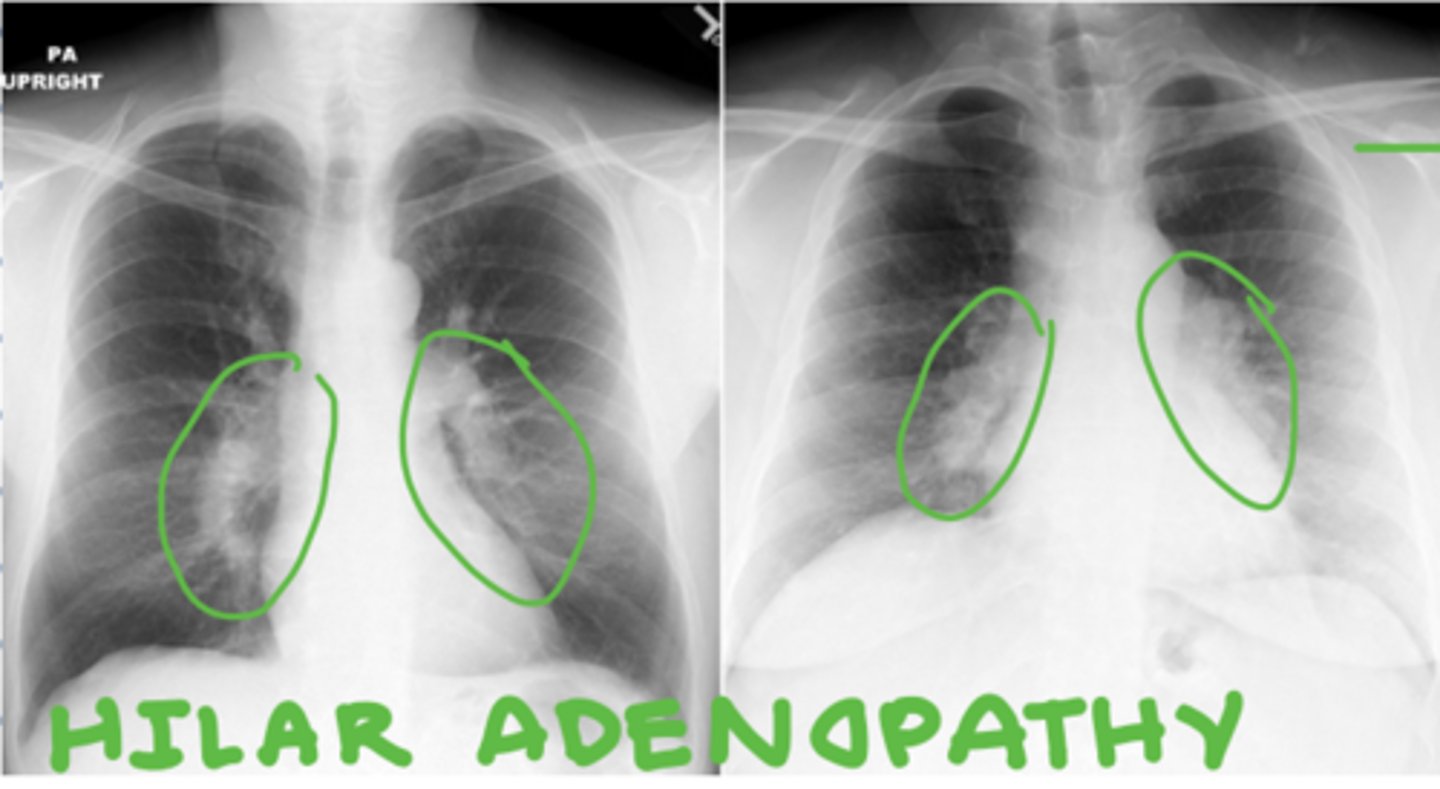
hilar adenopathy
-swelling of lymph nodes in hilar region
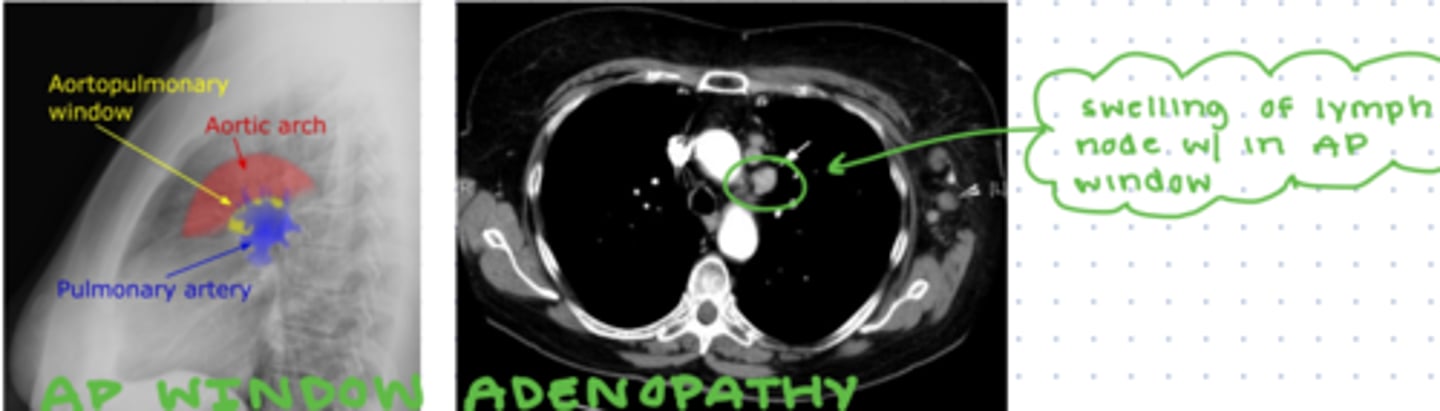
AP window adenopathy
-swelling of lymph node in AP window
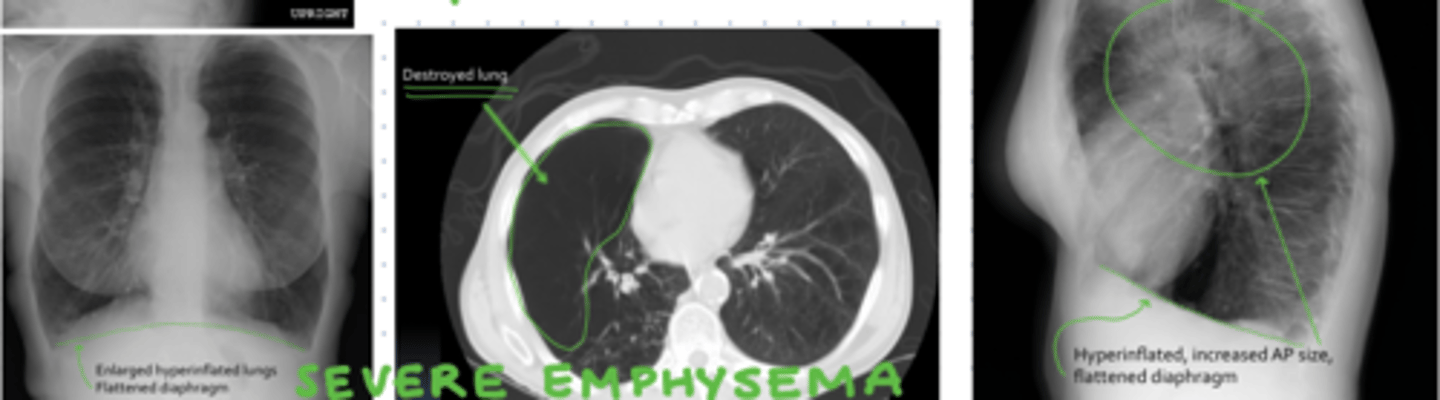
severe emphysema
-hyperinflated lungs
-flattened diaphragm
pneumoperitoneum
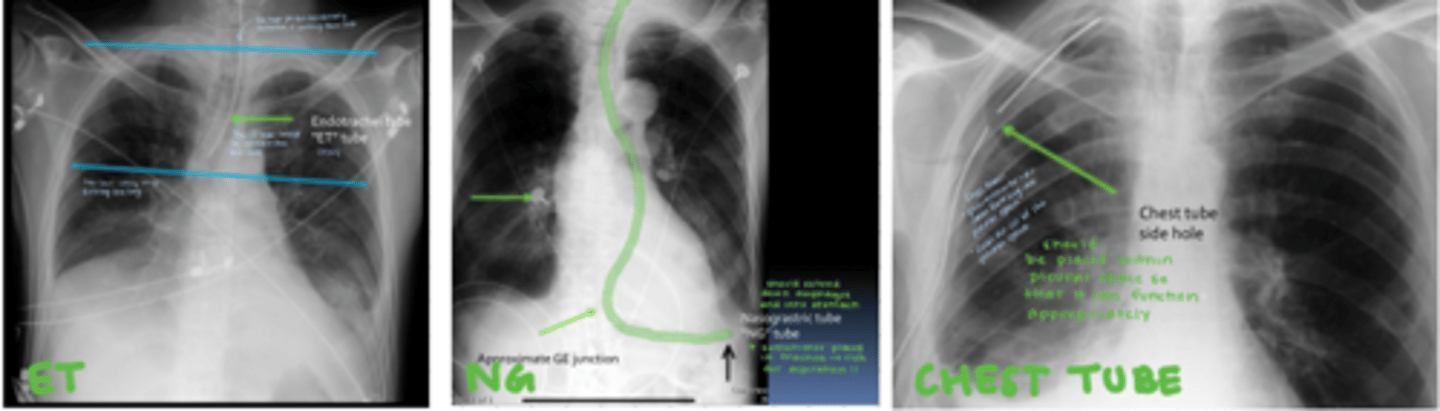
correct placement of ET tube, NG tube, and chest tube
common cause of pneumothorax
lung biopsy
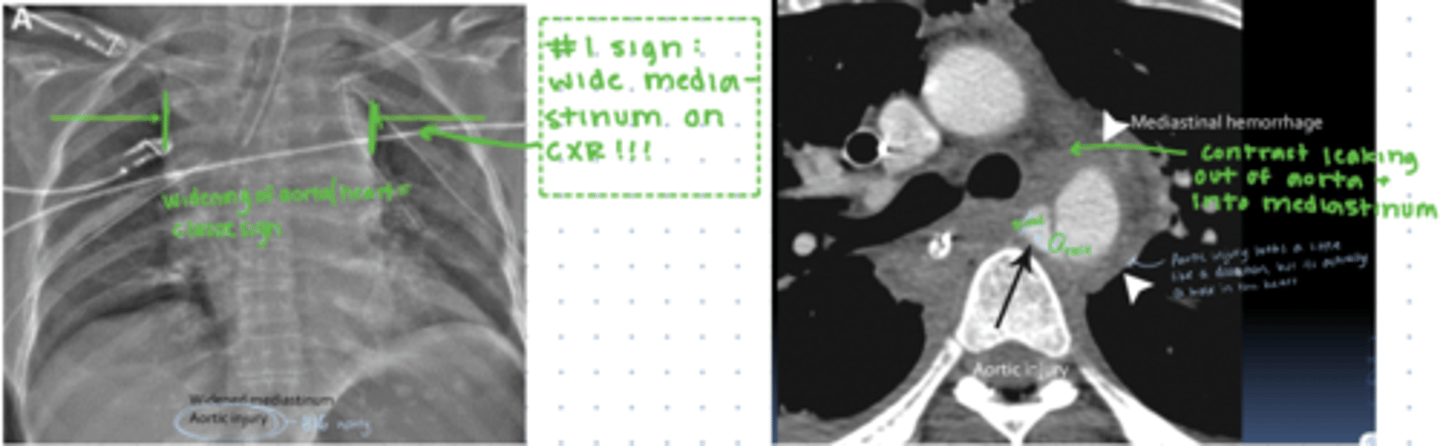
Signs of traumatic aortic injury on x-ray and CT
-wide mediastinum
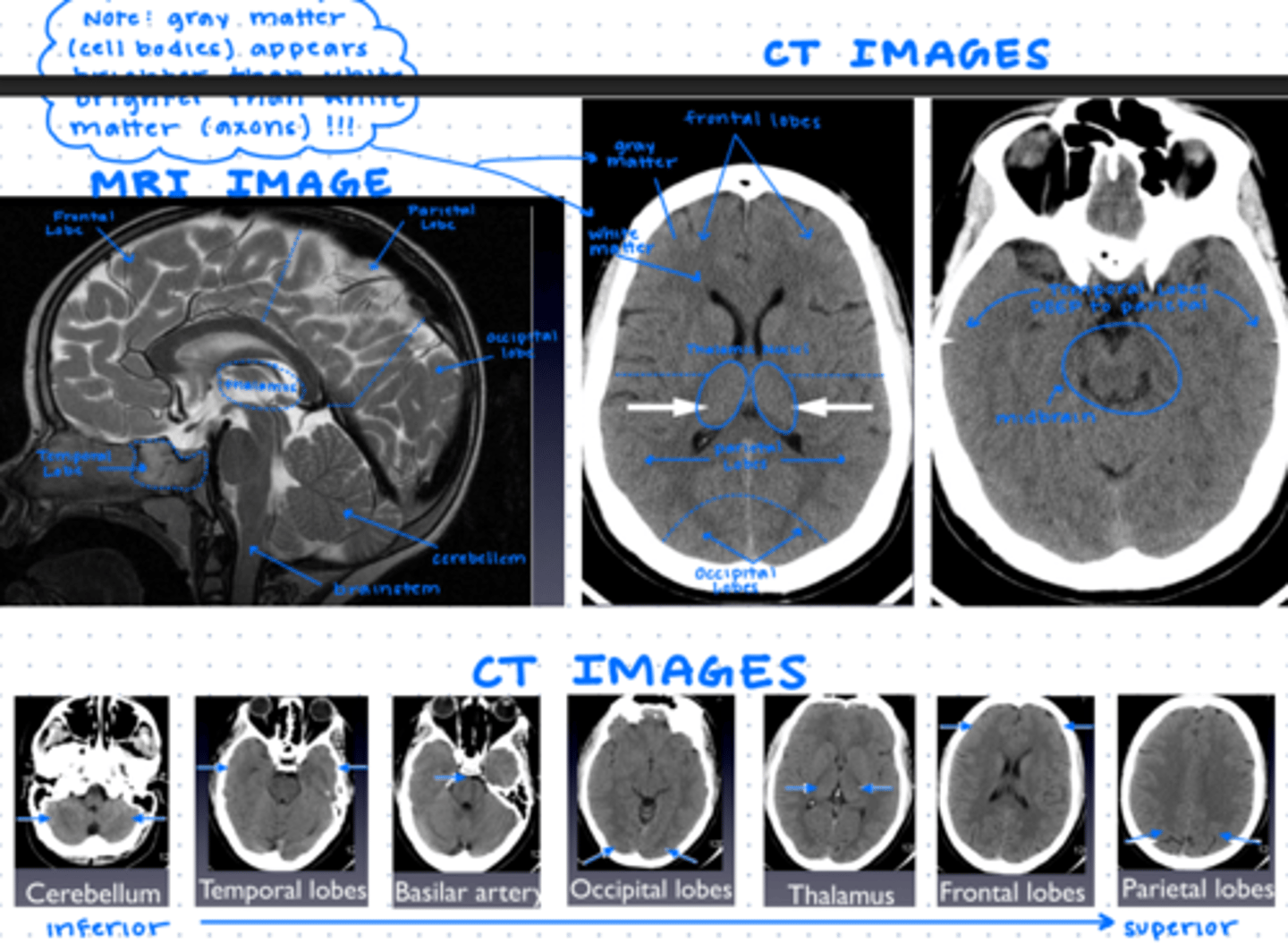
brain anatomy
-Frontal, parietal, temporal, occipital lobes
-Thalamus
-Cerebellum and brain stem
-Basilar, vertebrals, internal carotids, anterior, posterior, and middle cerebral arteries
-Normal appearance of gray and white matter
(gray is gray, white is darker than gray)
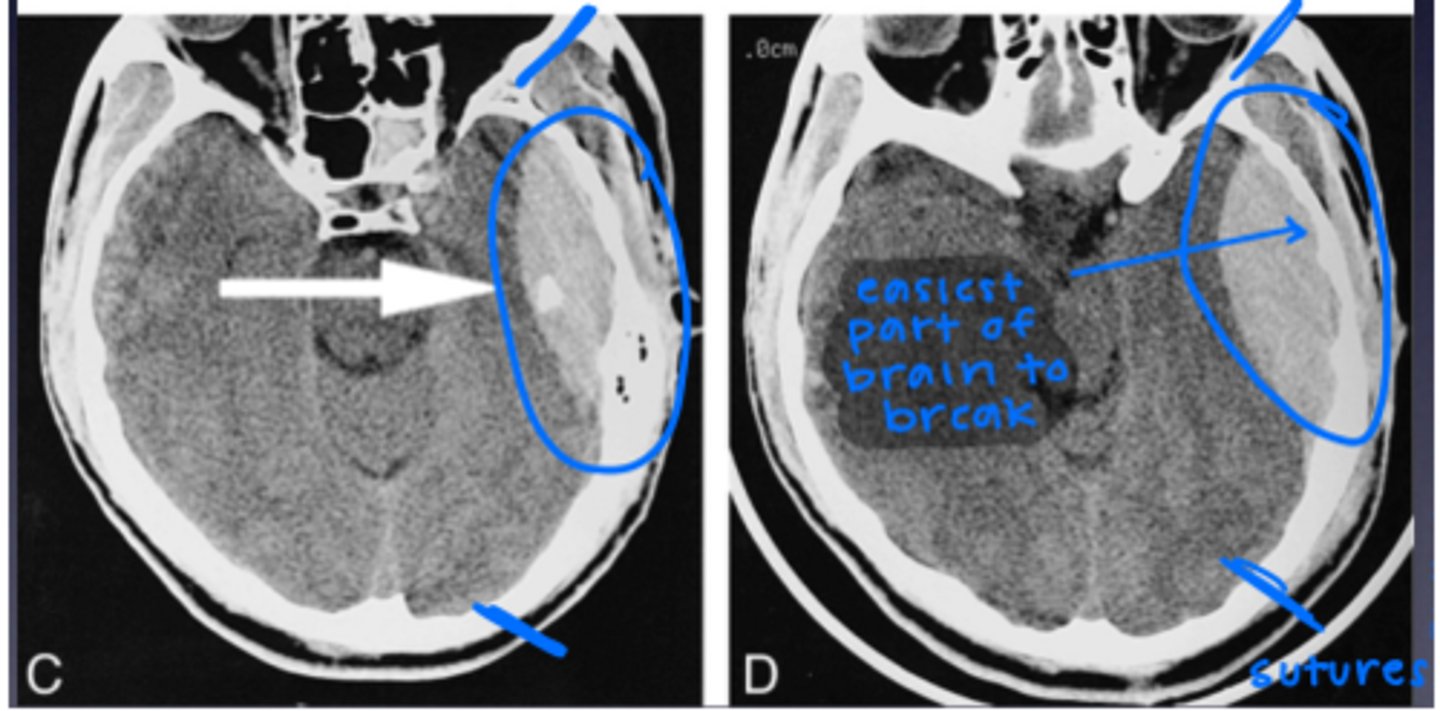
Epidural hemorrhage
-skull and dura mater
-confined by sutures
-can cross midline
-skull fracture
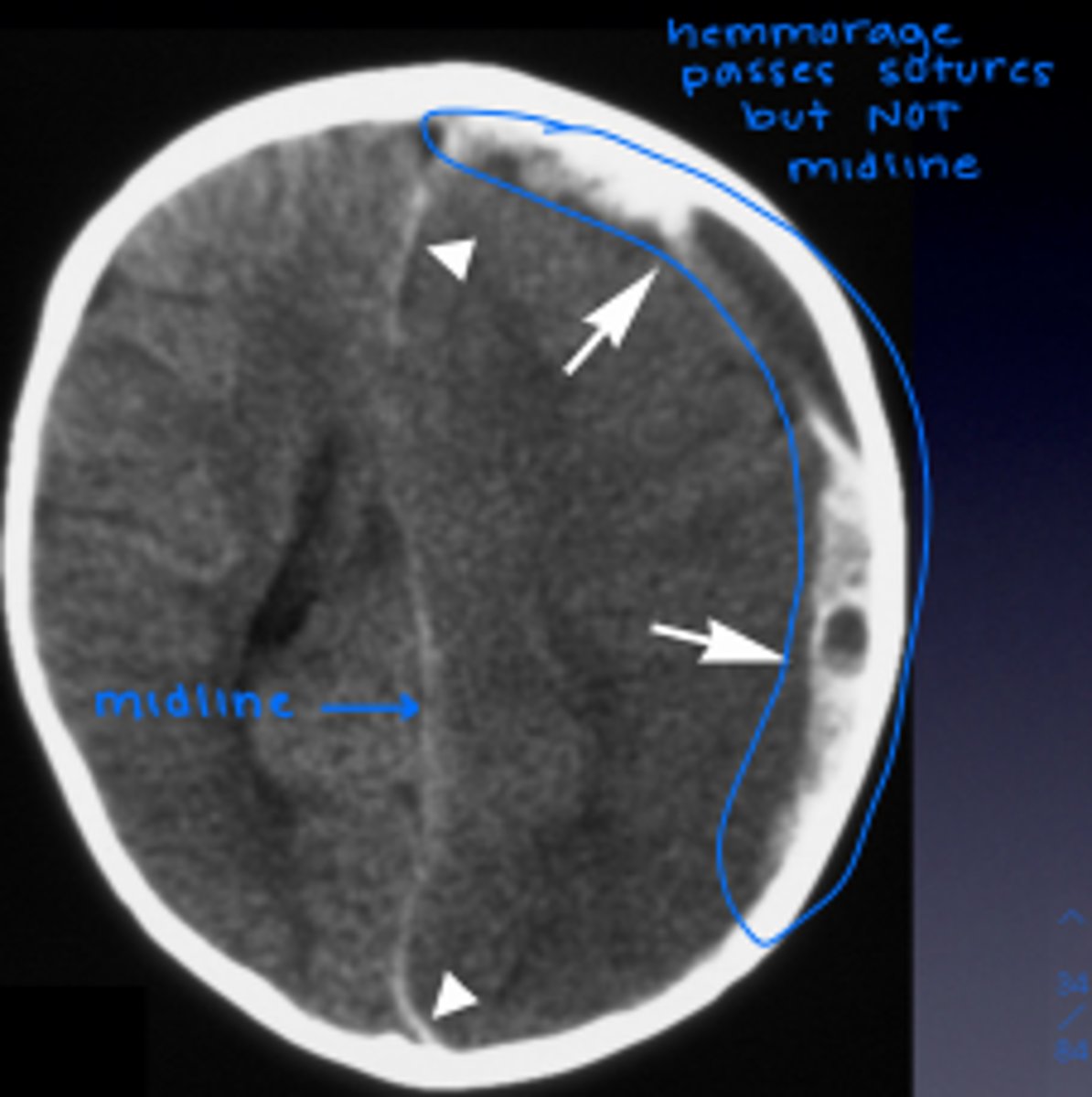
Subdural hemorrhage
-dura mater and arachnoid
-can cross sutures
-cannot cross midline
-trauma, elderly, child abuse(shaking)
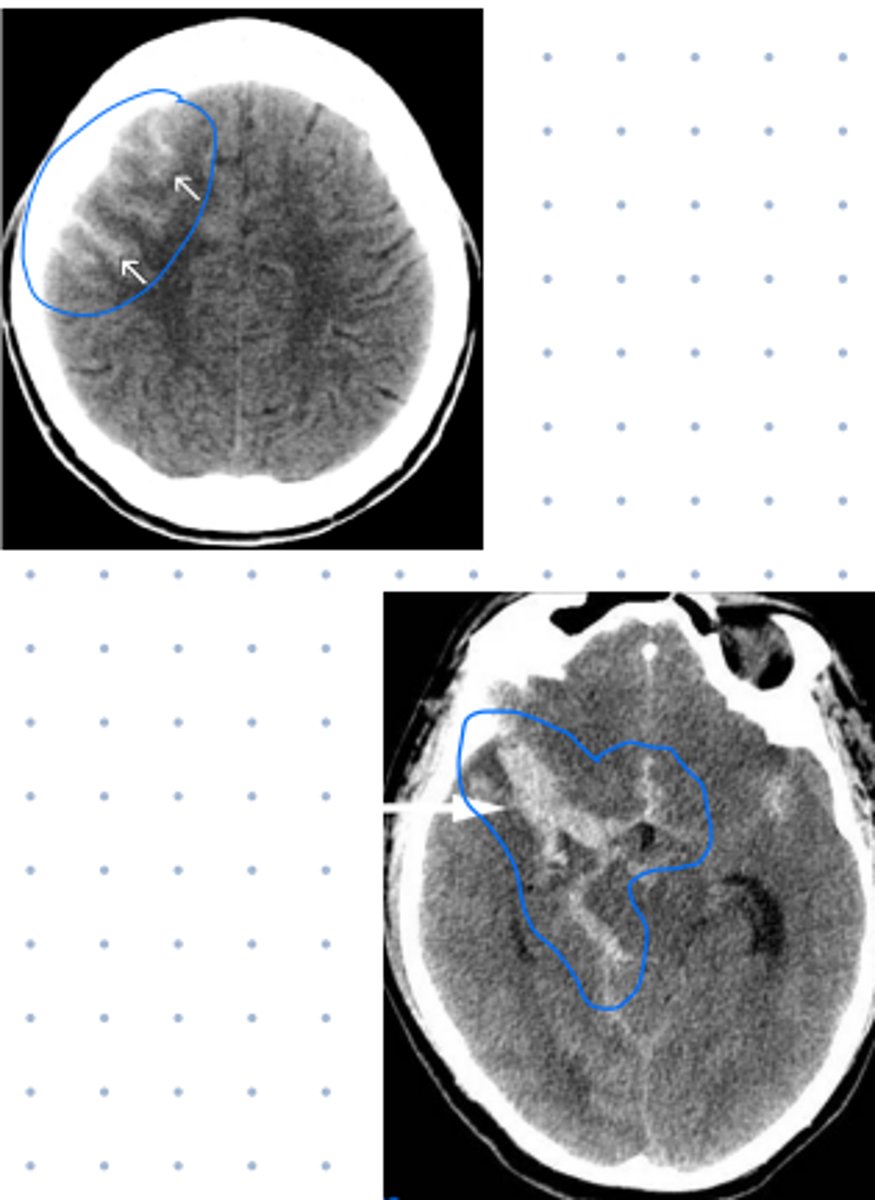
Subarachnoid hemorrhage
-arachnoid and pia mater
-looks like it spreads out
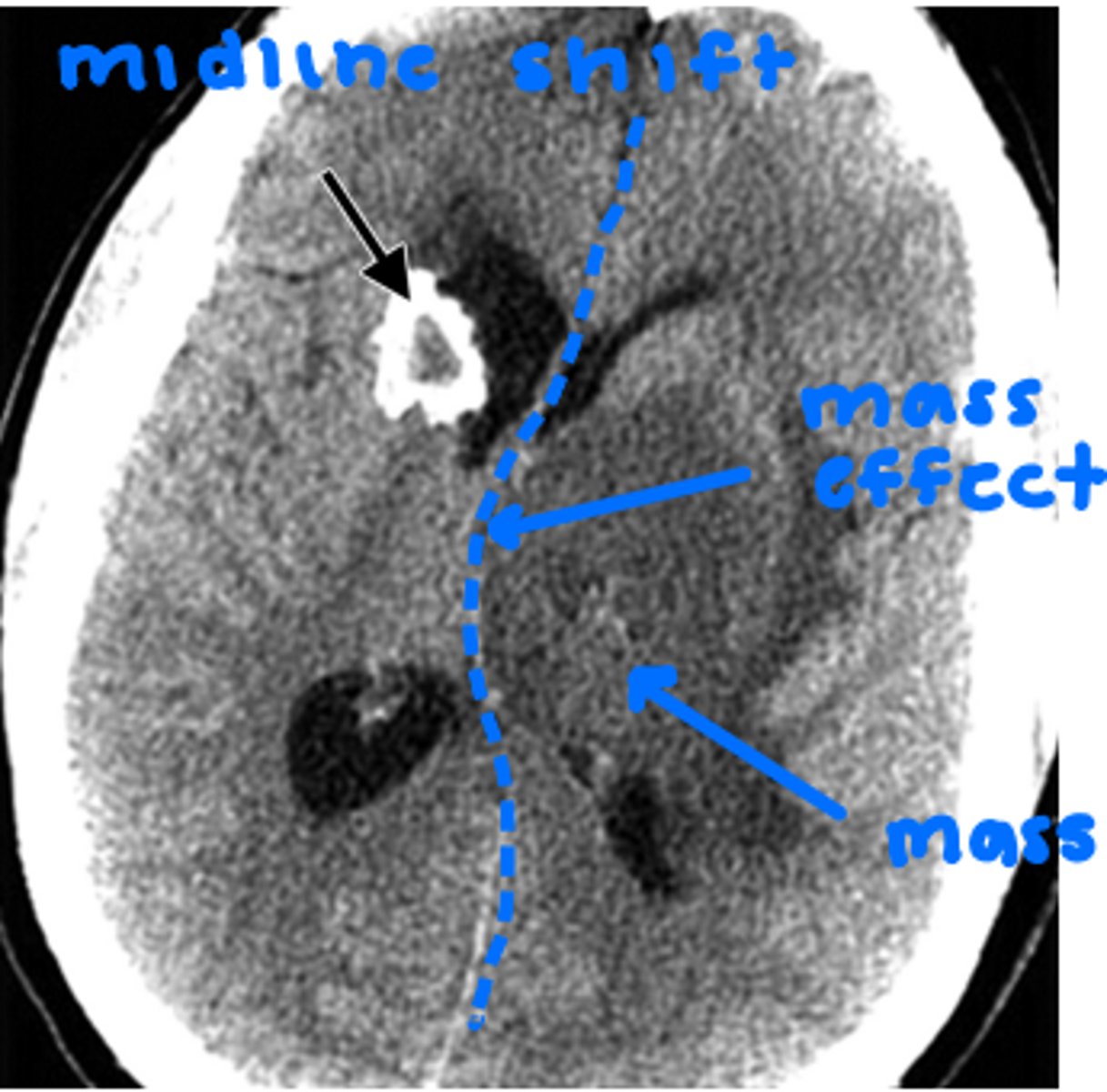
intracranial mass: brain tumor
mass effect: lesion compresses surrounding brain tissue
midline shift: midline shifted to R or L
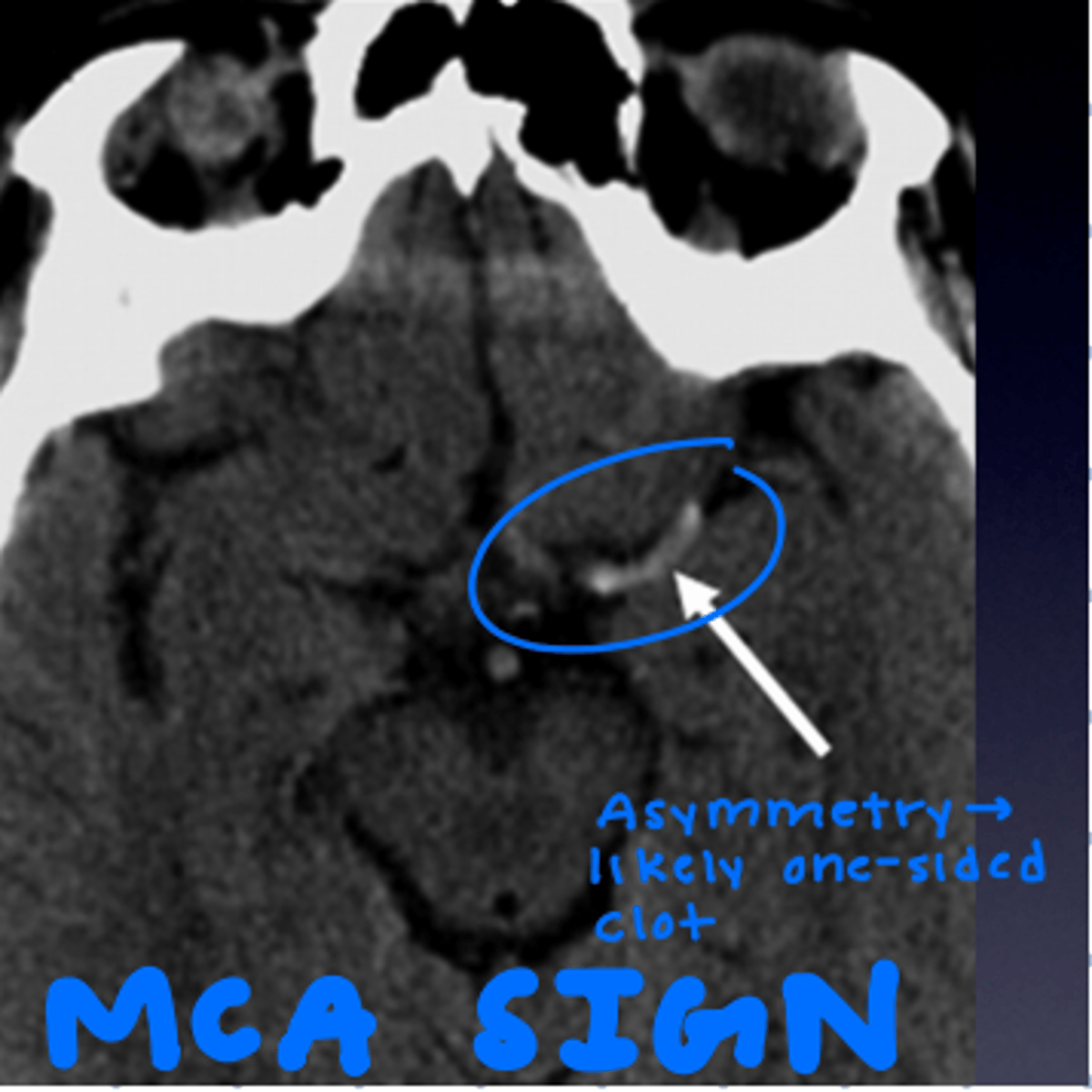
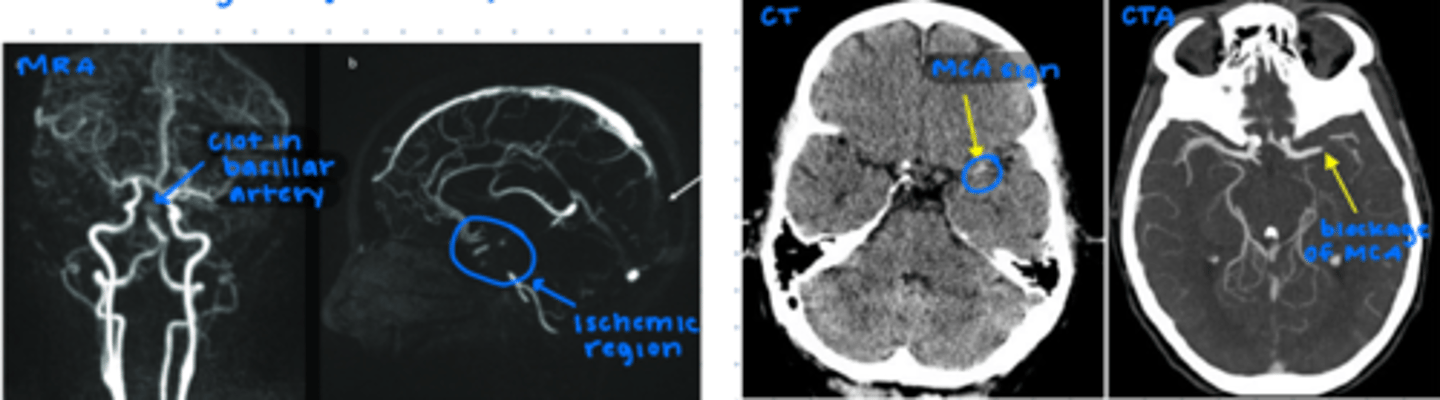
dense MCA sign
SUGGEST STROKE
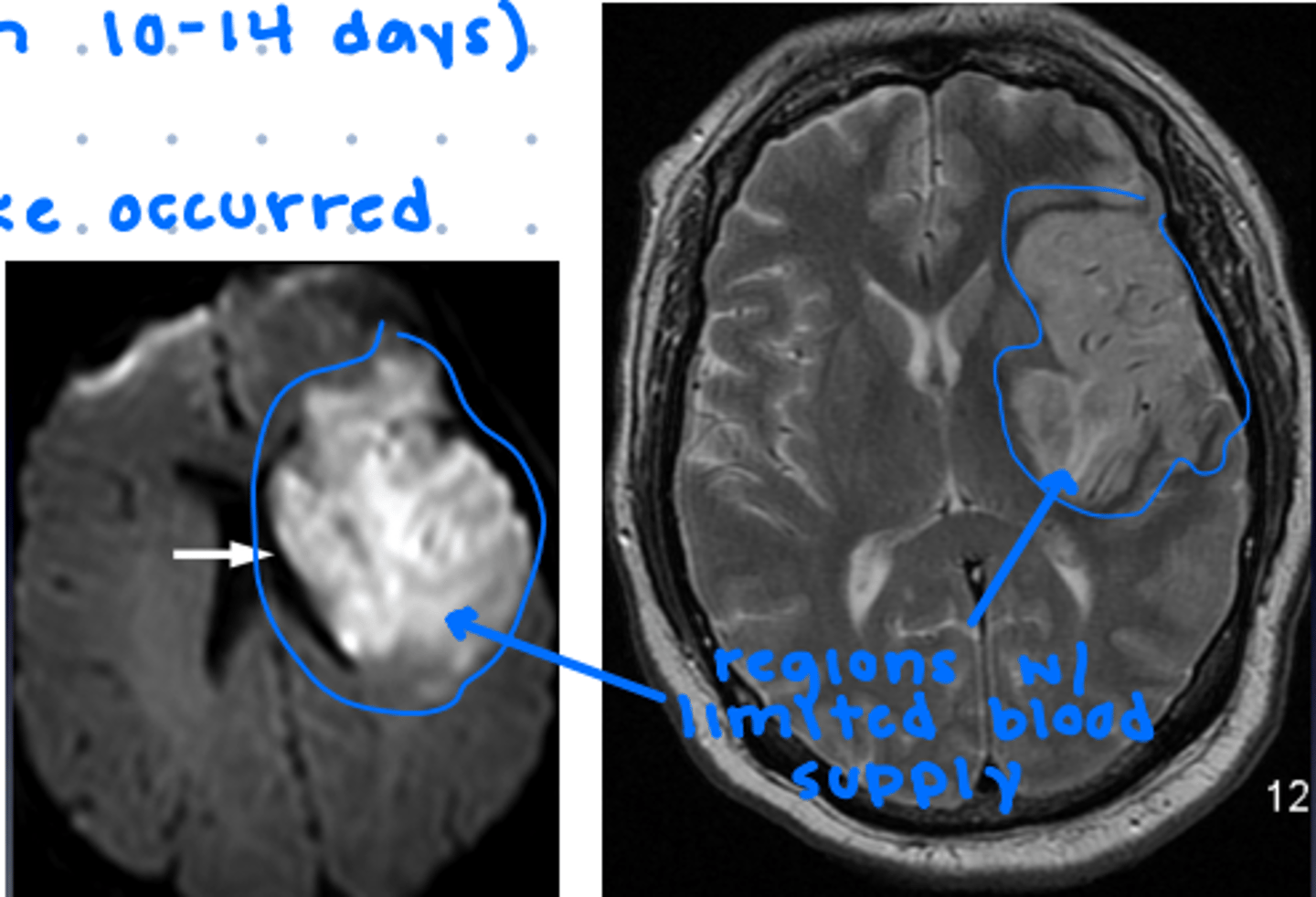
Diffusion weighted imaging (DWI)
BEST FOR STROKE IDENTIFICATION
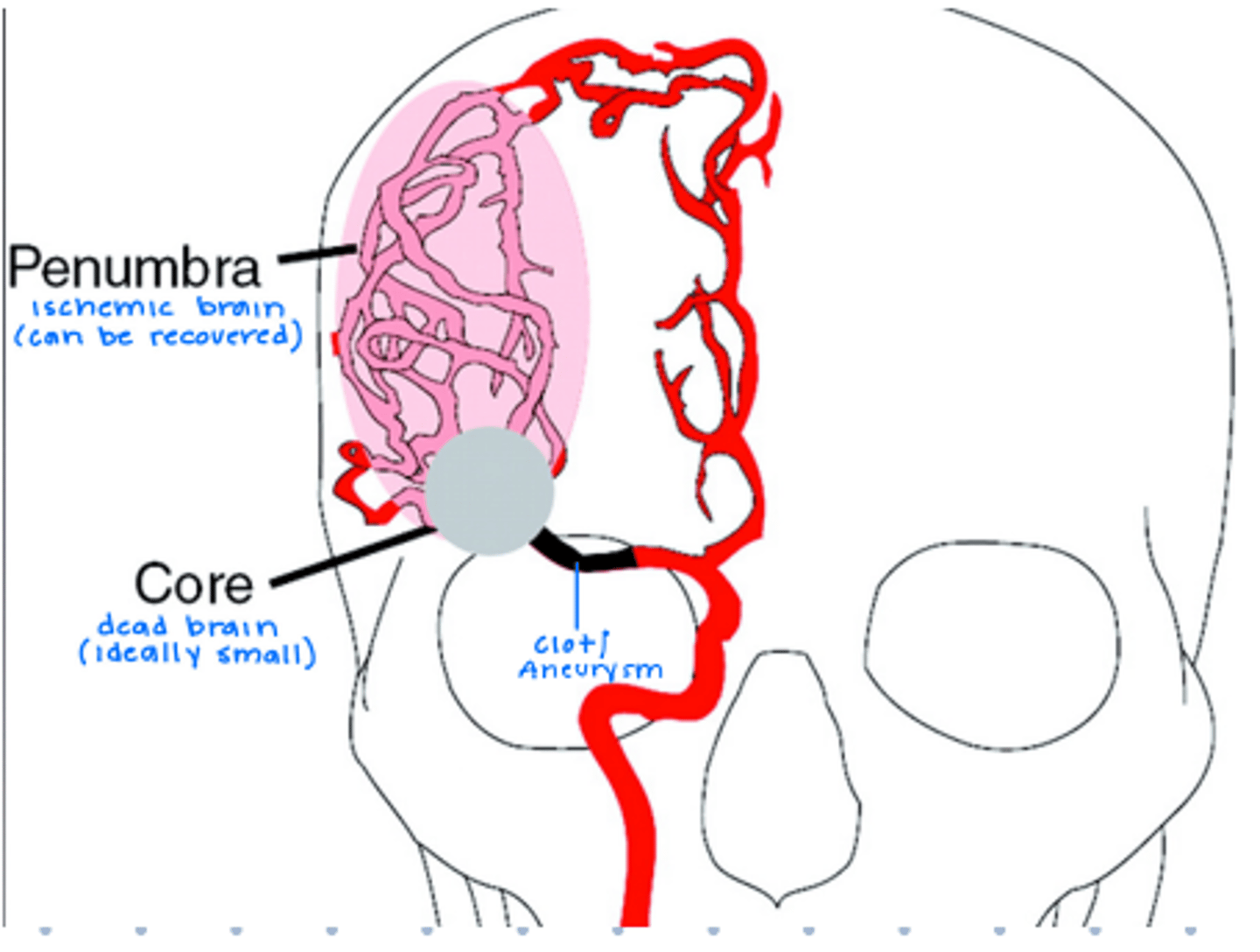
----CVA-----
core: infarcted brain tissue supplied immediately upstream of clot/aneurysm (DEAD)
penumbra: ischemic tissue upstream (CAN BE RECOVERED)
identify large clots on angiogram/ MRA/ CTA
aneurysm on MRI and angiogram
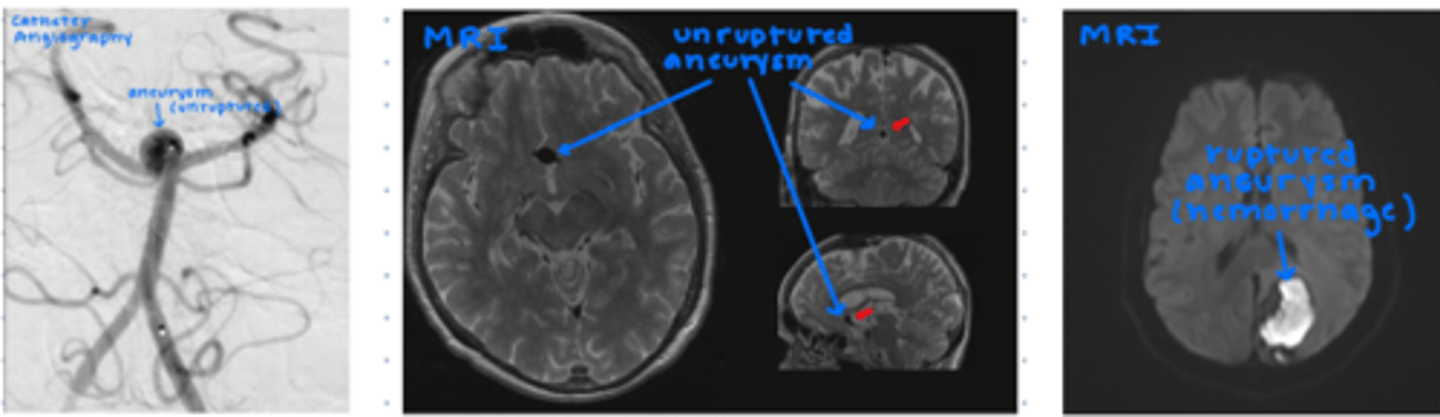
Relationship of aneurysms and subarachnoid hemorrhage
ruptured intracranial aneurysm can cause subarachnoid hemorrhage
Best test for evaluated bleeding in the brain
CT
spinal trauma imaging criteria
-age over 65
-history of malignancy
-pain lasting 6+ weeks
-significant trauma
-neurological deficit
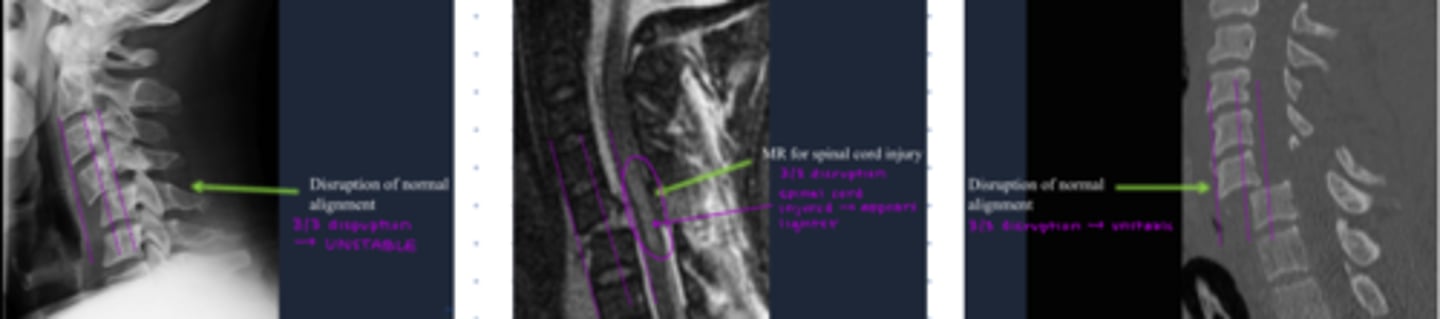
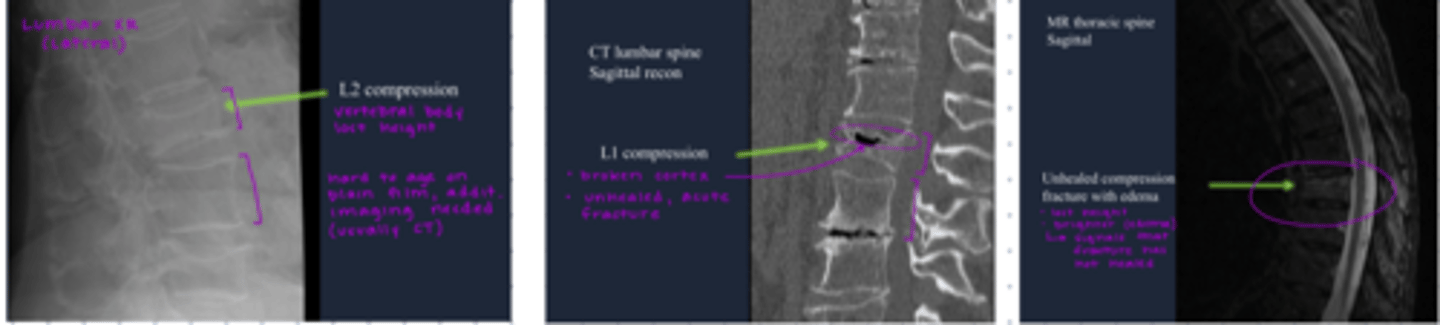
x-ray: compression fractures, instability
CT: acute trauma, osseous injuries
MRI: the best- evaluates bone, soft tissues, discs, spinal cord, nerve roots
unstable fractures involves 2 columns
anterior column: anterior longitudinal ligament, anterior 2/3 columns
middle column: posterior longitudinal ligament, posterior 1/3 of vertebral body
posterior column: pedicles, articular facets, facet capsule, lamina, spinous processes, ligamentum flavum, interspinous ligament
recognize spinal column fractures
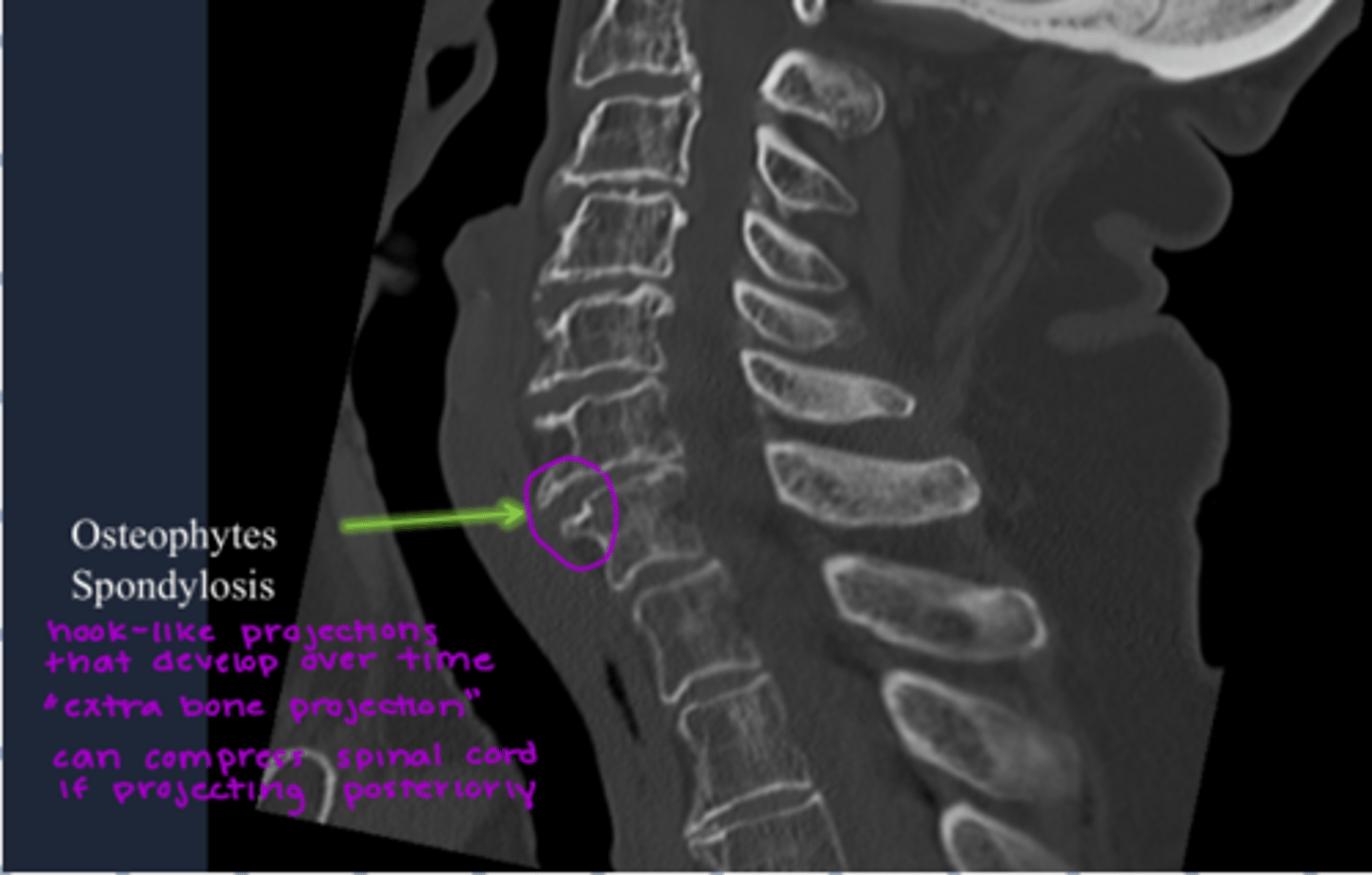
spondylosis
-osteophytes
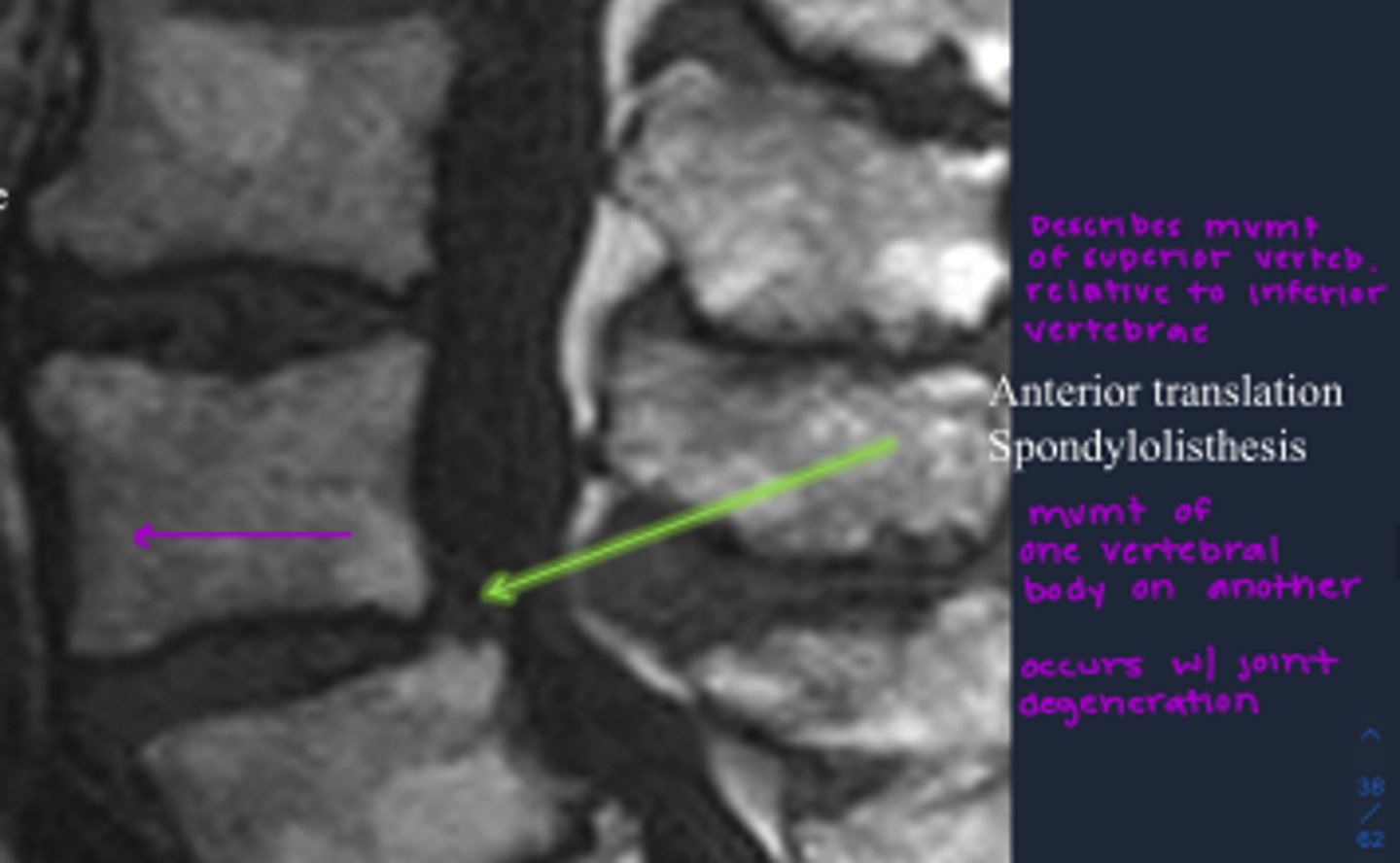
spondylolisthesis
-translation
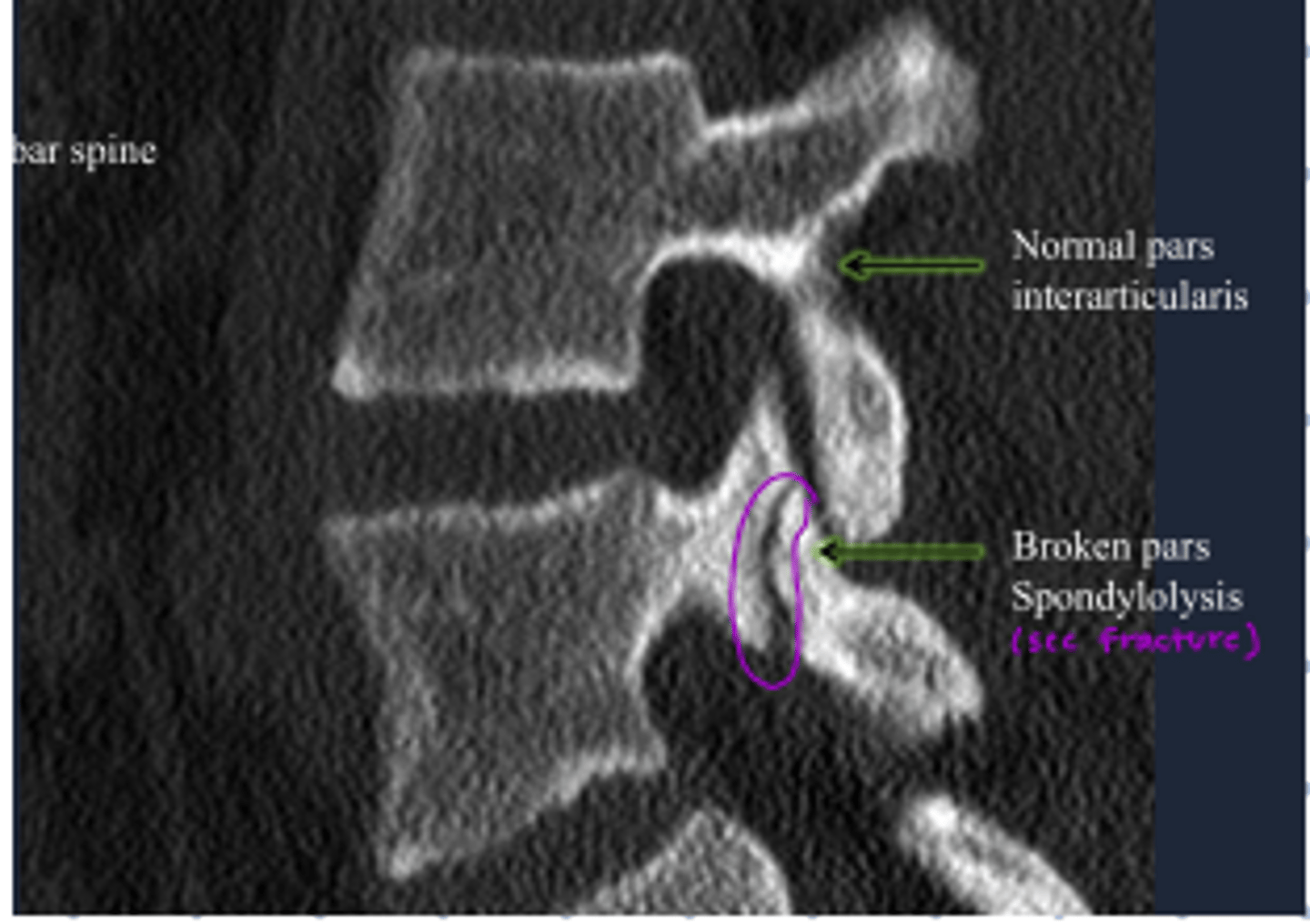
spondylolysis
-defect thru facet joint
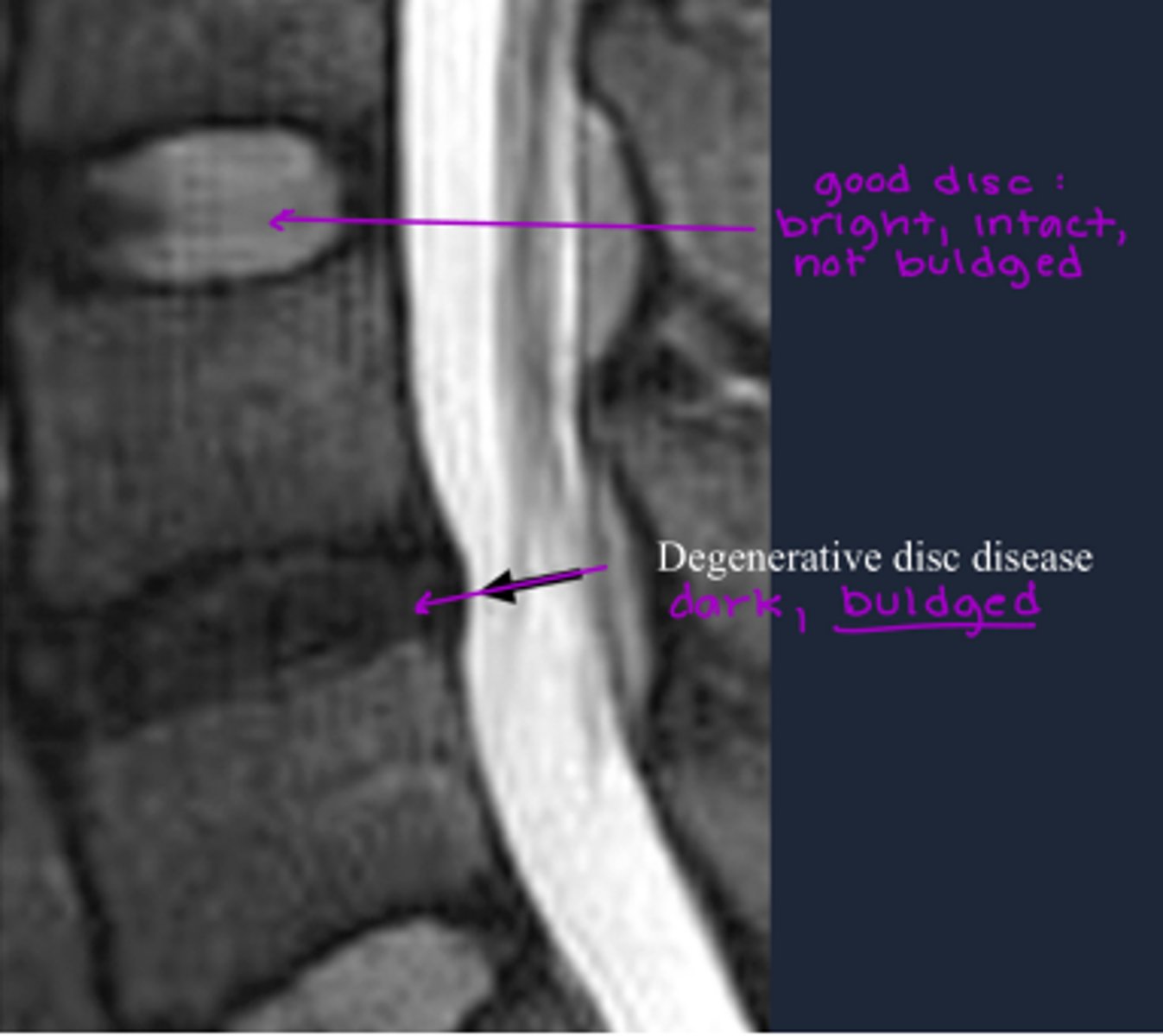
DARK DISCS= DEGENERATIVE
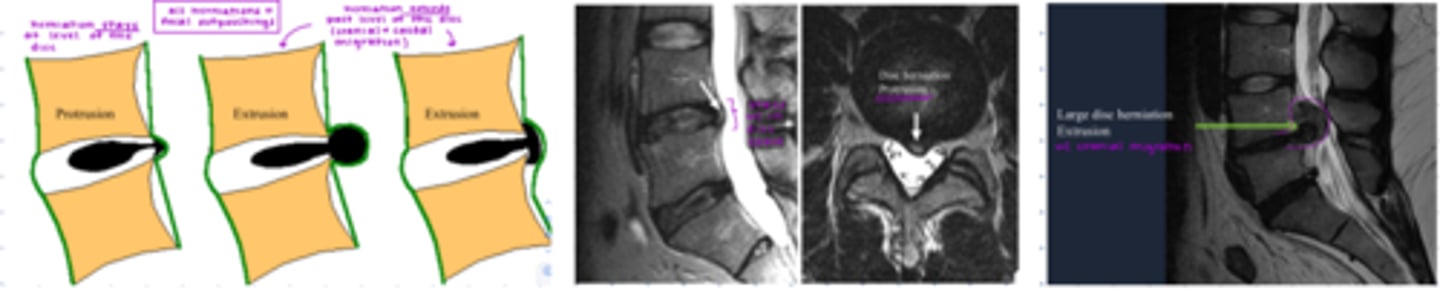
Herniated disc
Protrusion: stays at level of the disc
Extrusion: extends past levels of disc
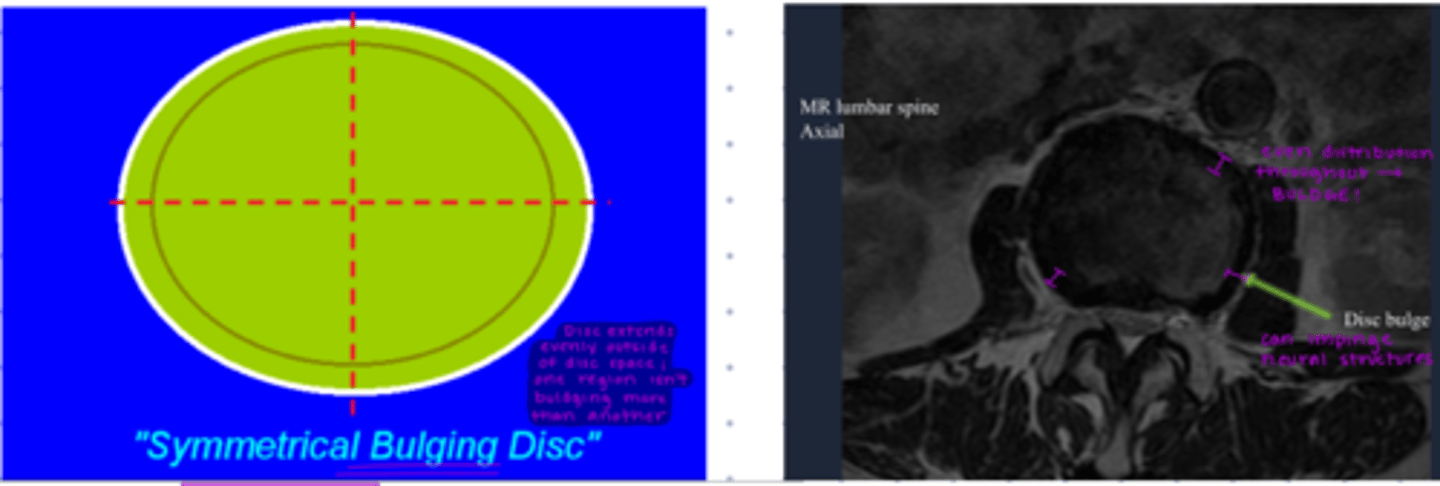
Bulging Disc
-extends evenly out of disc space
Compression fractures of the spinal column
Imaging modality of choice in MSK(musculoskeletal) trauma
x-ray
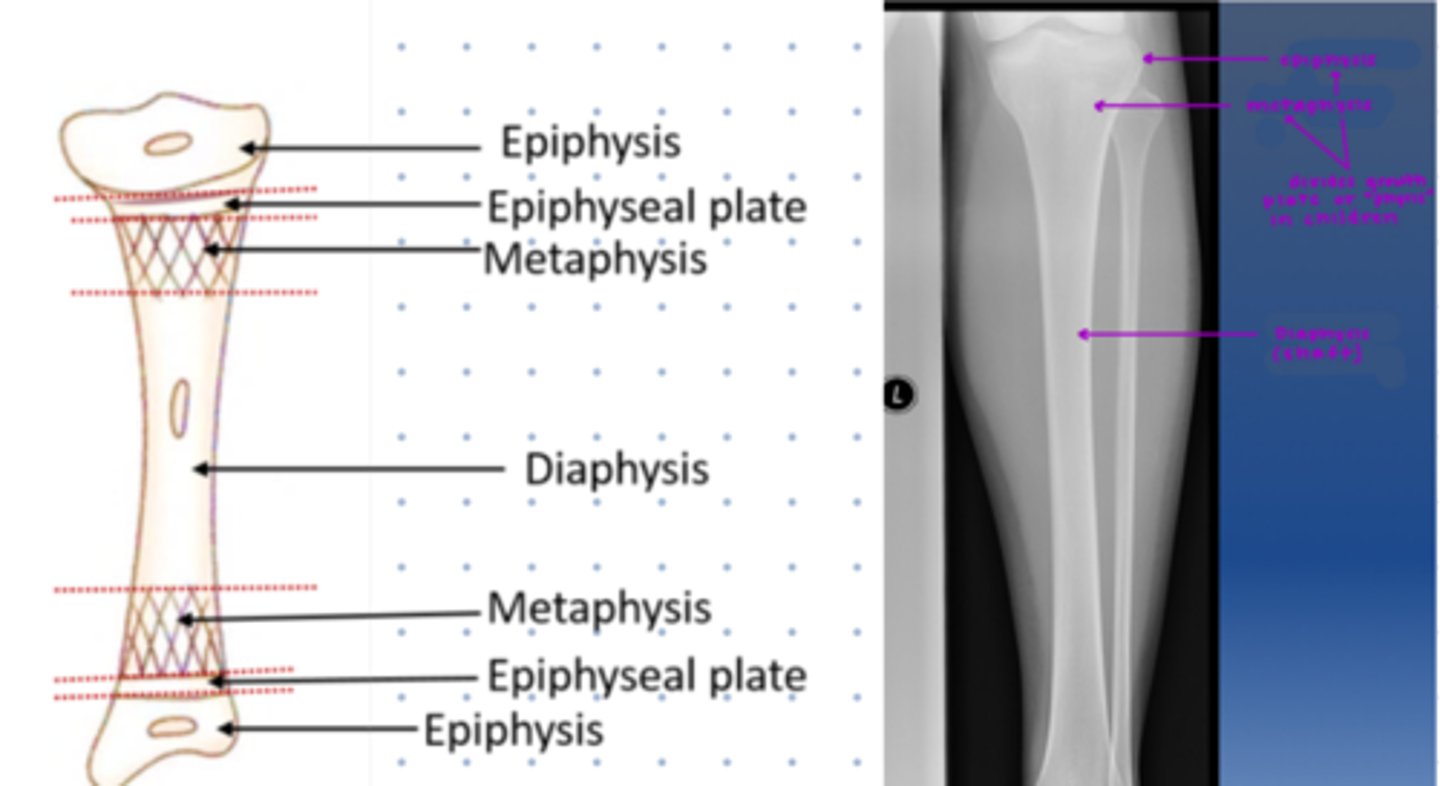
Identify epiphysis, metaphysis, and diaphysis
Location of scaphoid bone of the hand
damage can sever artery leading to it becoming osteonecrotic

When to do follow up imaging in trauma patients
important to ensure there are no persistent complaints
f/u when it isn't resolving
x-ray--> CT(some fractures)--> MRI(soft tissue/bone marrow)
comminuted
more than 2 fracture fragments
interarticular
if fracture reaches articular surface (joint)
if so, CT/MRI needed
displacement
movement of distal fragment relative to proximal
open
whether the fracture extends thru skin
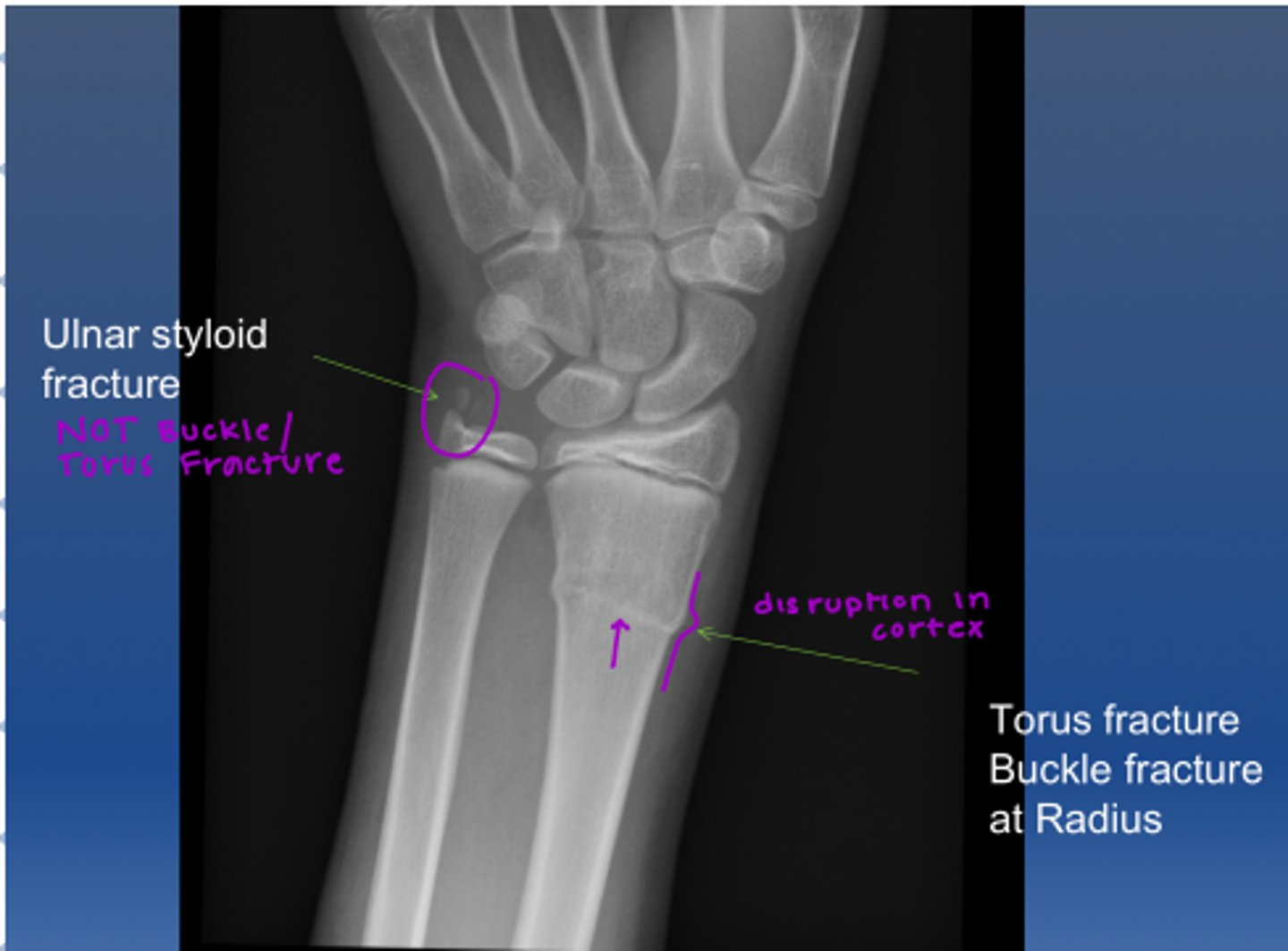
long bone fractures- buckle/torus
-fracture without a cortical break
-common in kids
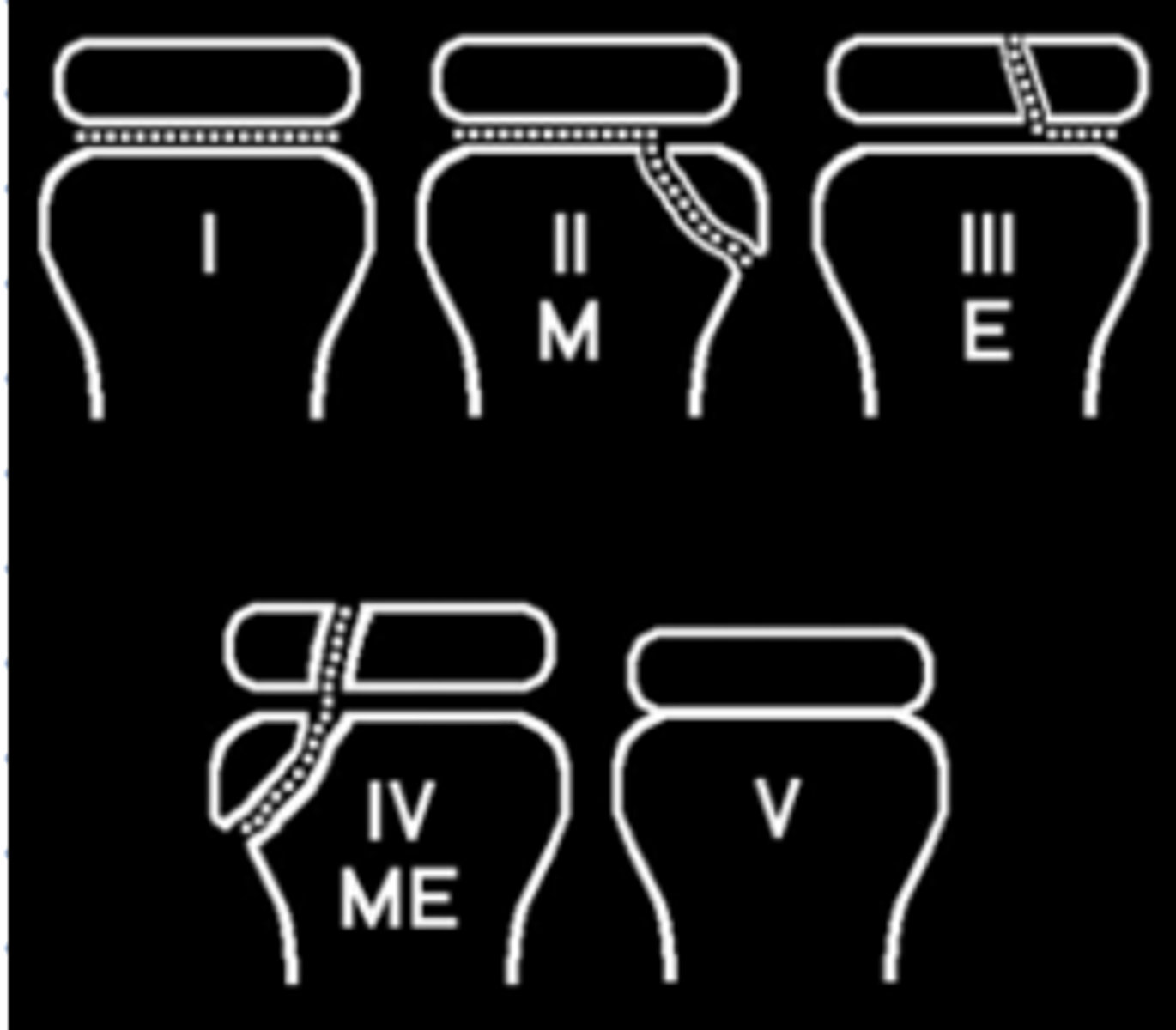
Salter Harris classification (Pediatric)
type 1: fracture thru physeal plate
type 2: fracture thru metaphyseal
type 3: fracture thru epiphyseal
type 4: fracture thru meta&episeal
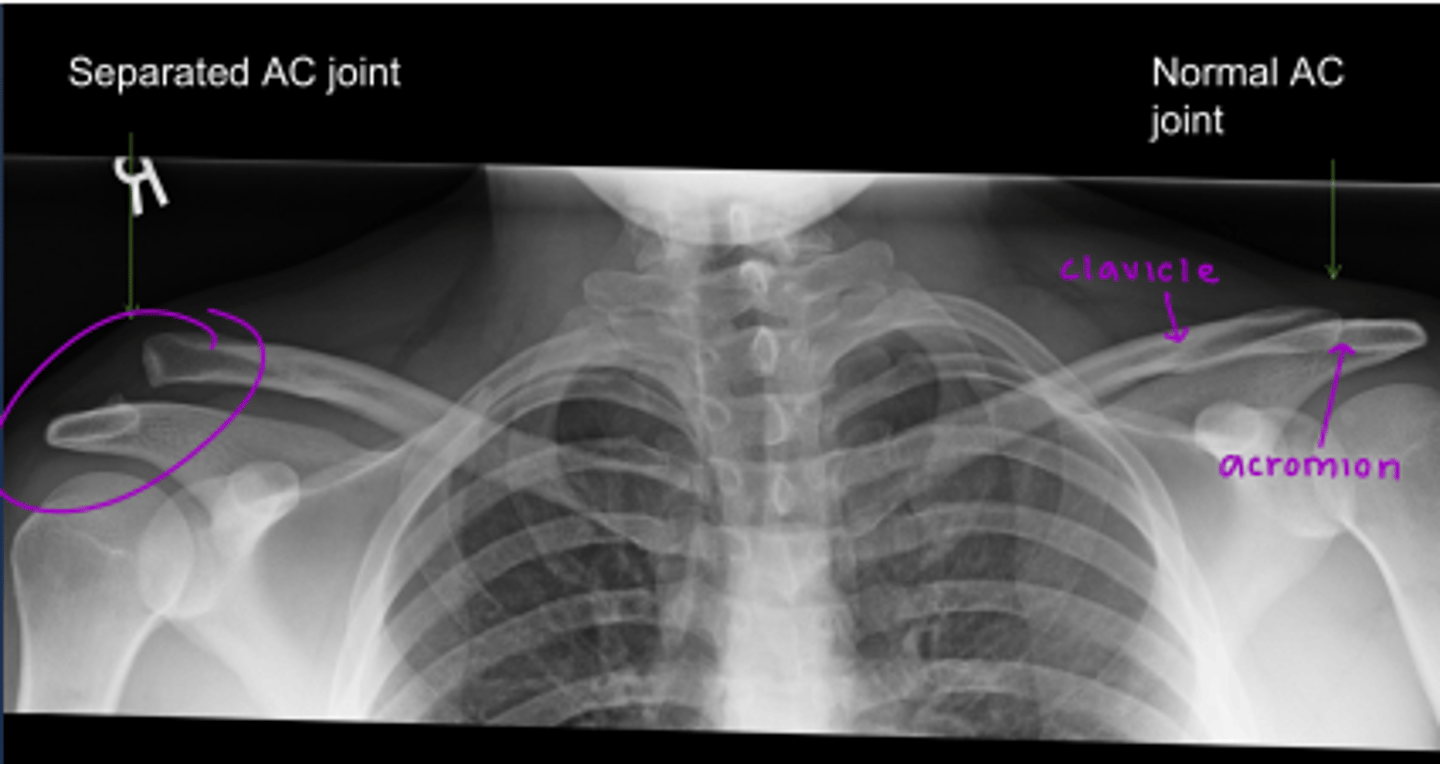
Separation : acromioclavicular joint
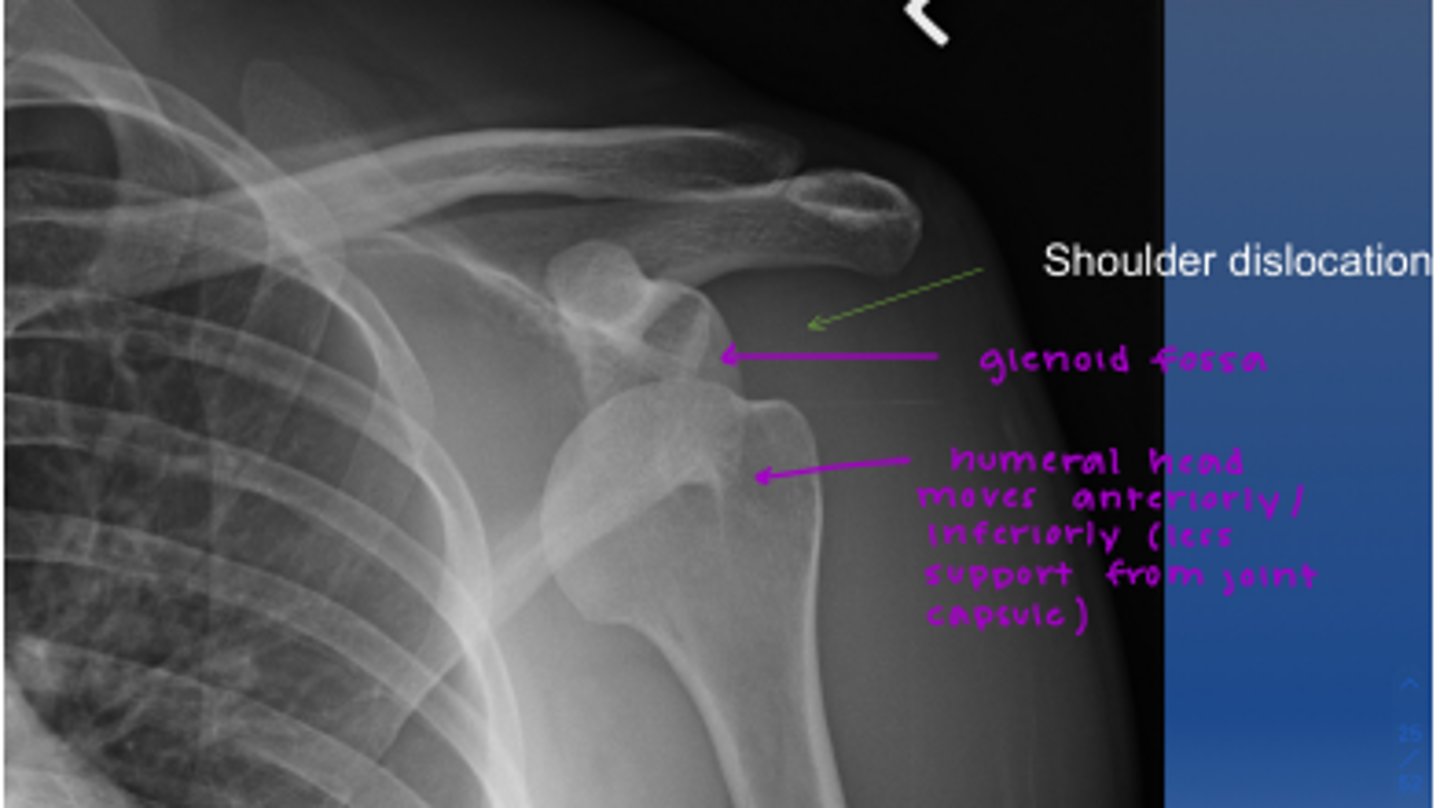
Dislocation: glenohumeral joint
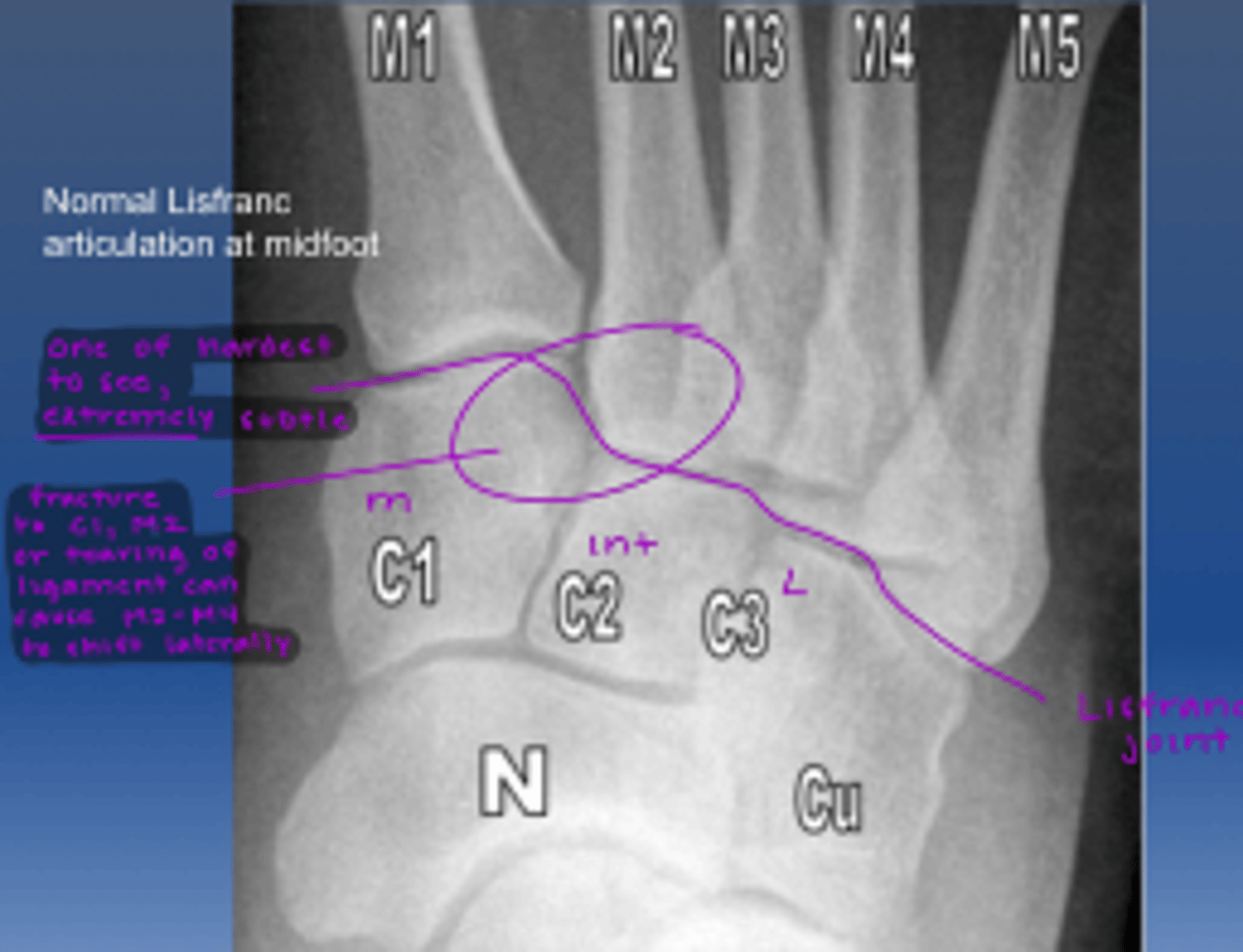
lisfranc fractures of the foot
-on medial cuneiform of 2nd metatarsal
-important to catch! can cause M2-M4 shift laterally