Rapid sequence intubation: pharmacology and therapeutics
1/22
Earn XP
Description and Tags
Dr. Ko Phar 644
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
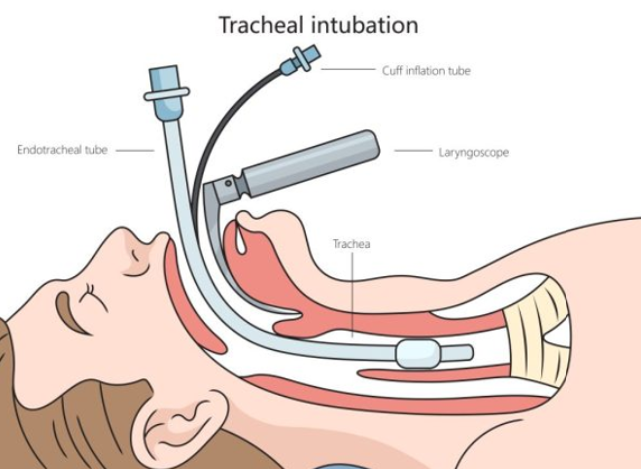
Intubation
Endotracheal tube (ETT) is placed into the trachea to maintain an open airway
RSI
Rapid sequence intubation is used in emergent situations
Indications for RSI:
•Airway protection (e.g., from coma, trauma, overdose)
•Respiratory failure (e.g., severe COPD/asthma exacerbation)
•Anticipated clinical deterioration (i.e., sepsis progressing to shock)
Laryngoscope moves mouth down to place ETT down airway
do not want to intubate esophagus - will not help pt breathe
the ETT is attached to something for ventilations such as a mechanical ventilator
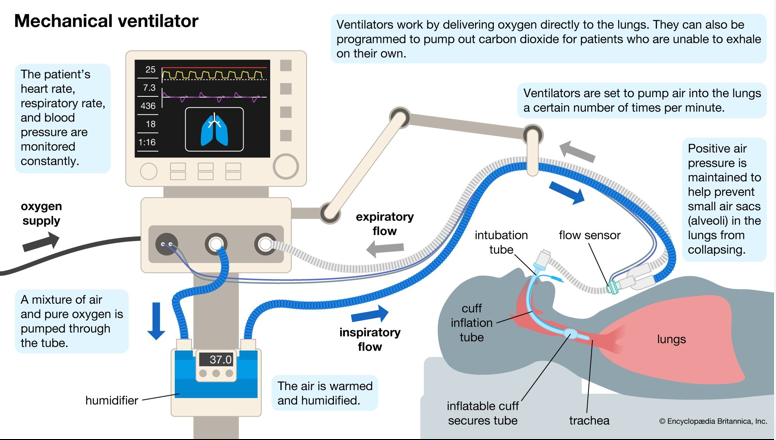
Mechanical ventilation
ET tube is connected to a ventilator machine; ventilator settings are adjusted to deliver oxygen and induce lung expansion/contraction to maintain O2 levels
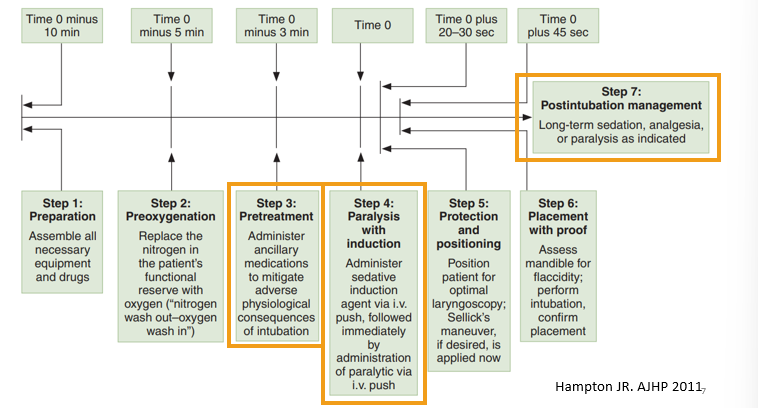
The seven “P’s” of RSI
focus on steps that have to do with meds - pharmacist role
Don’t get confused by step 4 - do not want to paralyze the pt… something?
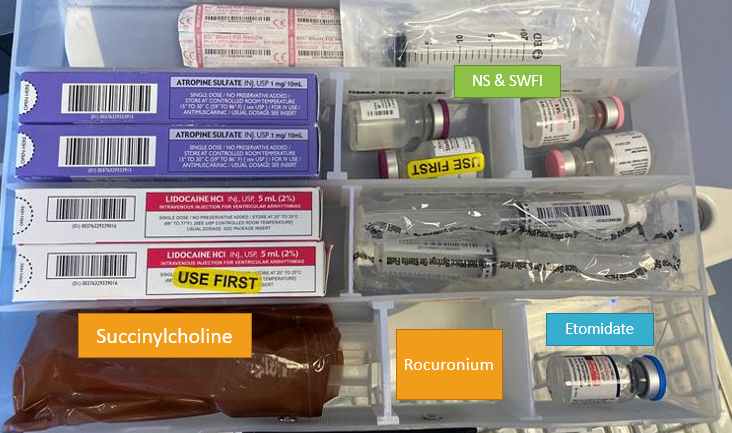
RSI Kit
Pretreatment (T = -3 minutes)
•Goals: optimize hemodynamics and mitigate the physiologic effects of intubation
•Blunt sympathetic surge or bronchospasm due to endotracheal tube insertion, or
•Prevent hypotension from induction agents
•Limited/weak data to support the benefit of pretreatment agents in RSI, so infrequently used in clinical practice
Pretreatment agents
Agent & Dose | Rationale & Potential Clinical Uses | Side Effects |
Fentanyl 1-2 mcg/kg (max 200 mcg) | Blunt sympathetic response to ETT insertion May consider in: -Elevated ICP (TBI, intracranial hemorrhage) -Aortic dissection -Myocardial infarction | Hypotension and respiratory depression (high doses) (No strong evidence of benefit in studies, not commonly used) |
Lidocaine 1-1.5 mg/kg (usually syringe size of 100 mg for adults) | Blunt cough reflex or bronchospasm in response to ETT insertion May consider in: -Elevated ICP (TBI, stroke) -Asthma | Bradycardia, heart block Hypotension (No strong evidence of benefit in studies, not commonly used) |
Atropine 0.01 mg/kg (adults) 0.02 mg/kg (peds) (max 0.5 mg) | Prevent (or treat) bradycardia May consider in: -Pediatric patients (<1 yr most susceptible) who are receiving succinylcholine | Tachycardia, flushing, urinary retention, constipation |
Phenylephrine 100-200 mcg (adults) | Prevent (or treat) hypotension associated with ETT insertion and induction meds
| Risk of reflex bradycardia |
Inductions
Purpose: sedate the patient so they are asleep for the intubations
ideally, also provide amnesia and pain control
Given as a single IV push dose, based on pts weight
may have to guestimate weight, so not have a ton of time
RSI Induction Agents
Etomidate
IV Dose: 0.3 mg/kg
O: Immediate
D: 5-15 min
Hemodynamically neutral, Short-acting
Warnings and AEs: Myoclonus, adrenal suppression, nausea & vomiting
Ketamine
IV Dose: 1-2 mg/kg
O: : 30-90 sec
D: 10-30 min
Clinical Pearls: Provides pain control + sedation
Bronchodilation helpful in severe asthma requiring intubation
Warnings and AEs: Hypertension, tachycardia, myocardial ischemia, nystagmus,
increased secretions, emergence phenomenon, elevated intraocular pressure (IOP)
Propofol
Midazolam
Etomidate (Amidate)
•Binds to GABA-A receptors and positively modulates their activity to increase GABA-ergic transmission à sedative and hypnotic effects
•Also inhibits 11-beta-hydroxylase which is necessary for cortisol synthesis à adrenal suppression
•Concern over whether this effect impacts patients with sepsis who have relative adrenal insufficiency (more on this later in the course), but large meta-analyses have failed to find a difference in outcomes with 1 dose = insufficient evidence to avoid in RSI for septic patients
•AE: Myoclonus not usually seen in RSI due to NMBA use
there have been seizure risk w use, may use something else if pt is having seizure
•Used all the time b/c - Has several properties (fast onset/short duration, hemodynamically neutral, not a controlled substance) that make it a “go-to” first line for RSI
short duration significance?
can cause temporary adrenal suppression
Ketamine (Ketalar)
•Works at multiple receptors which produce intended effect and side effects:
•NMDA antagonist, monoaminergic (MAO) antagonist, glutamate antagonist (nyastygmas) à dissociative anesthestic and anxiolytic properties
•NMDA + opioid receptor partial agonist effects à analgesia
•Stimulates catecholamine release à increase HR, BP, bronchodilation through adrenergic receptors, increases intraocular pressure
•Negative inotropic effects à myocardial depression in patients without adequate catecholamine stores (e.g., in shock or sepsis)
•Emergence phenomenon = hallucinations, vivid dreams, altered mood
hallucination can be managed by giving an BZD (Lorazepam)
in RSI pts, will be giving other meds in addn to this one, so may not be too worried ab the drugs’ side effects
•Unique beneficial properties: maintains respiratory drive, provides pain control
•Unique concerns: elevated IOP, catecholamine release, controlled substance
Propofol (Diprivan)
•GABA-A agonist, increases the duration of open GABA channels and NMDA (very little) antagonist properties à sedative effects
•Lipophilic and rapidly crosses BBB for fast onset (milky white appearance)
•AEs: Causes significant myocardial depression, decreased contractility, reduced MAP and cardiac index à hypotension, bradycardia limit its use in RSI
definitely will see hypotension and bradycardia given this drug 100% of the time
•Milky white appearance; may sting during IV administration
Midazolam (Versed)
•Short-acting benzodiazepine, direct agonist of GABA-A receptors à sedation
•Dose-dependent hypotension due to decreased vascular tone (decreased SVR) even at low doses of 2-4 mg
•Doses required for RSI are huge and so not commonly used in practice
Controlled substance
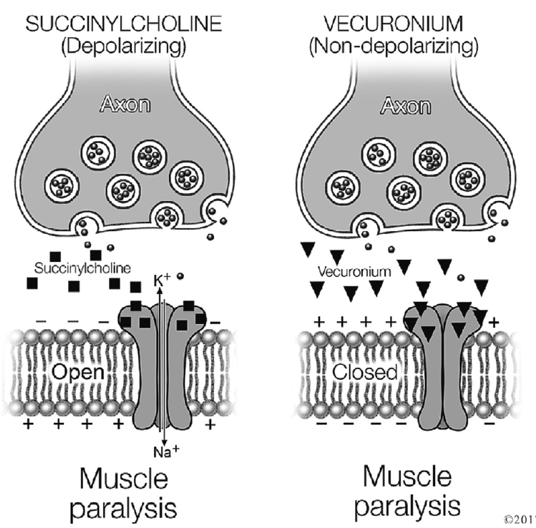
Paralytics
•Neuromuscular Blocking Agents (NMBAs) = “paralytics”
•Use in RSI: airway muscle paralysis to allow for ETT placement
•However, affects all skeletal muscles, leading to full body paralysis for duration of paralytic agent
•Depolarizing NMBA binds AChR and triggers immediate action potential vs. nondepolarizing is competitive inhibitor of AChR
Examples:
Succinylcholine
Vecuronium or Rocuronium
RSI Paralytic agents
Drug | IV Dose | Onset & Duration | Uses & Clinical Pearls | Warnings |
Succinylcholine (“Succs”) | ***1.5 mg/kg (but round up/ overestimate the dose) | O: 30-45 sec D: 5-15 min | Optimal onset/ duration of action Only paralytic that can be given IM | Malignant hyperthermia Risk of cardiac arrest due to hyperkalemia in patients w/ elevated K+ or risk: undiagnosed skeletal muscle disorders, ESRD, or baseline hyperkalemia, diseases with upregulation of ACh receptors (burn or crush injury >24 hrs ago, muscular dystrophy, spinal cord injury, demyelinating neuromuscular disease, severe immobility), |
Rocuronium (“Roc”) | ***1 - 1.2 mg/kg (use IBW if possible) | O: 45-60 sec D: 45-120 min | Preferred agent if succinylcholine is not appropriate | Long duration of action – requires empiric post-intubation sedation! In ED, 1.2 mg/kg dose preferred |
Vecuronium | 0.1 - 0.2 mg/kg | O: 2-4 min D: 40-60 min | Longer onset of action; reserve for drug shortages | |
Succinulcholine
•Ideal PK properties for RSI: fast onset & short duration. Use if you can!
great bc do not want to paralyze pt for longer than they need to be
•Depolarizing NMBA causes efflux of K+ (exchanged for Na+) and transient hyperkalemia (not an issue in normal K pts, caution in high risk hyperkalemic pts)
•Patients at risk of arrhythmia/cardiac arrest from hyperkalemia should NOT receive succinylcholine! Avoid for:
•ESRD on dialysis
•Baseline hyperK+
•Patients with diseases with an upregulation of AChR should also not receive succinylcholine (excessive K+ efflux could lead to much more severe hyperkalemia)
•Muscular dystrophy, demyelinating neuromuscular diseases like Multiple Sclerosis, severe immobility or spinal cord injury, sepsis >7 days
•Burn or crush injury >24h (some sources say 72h)
•Contraindicated in malignant hyperthermia (MH) or history of MH
•Can also cause bradycardia (do not give repeated doses)