LESSON 3: DILATED CARDIOMYOPATHY ECHO PARAMETERS
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
Name 8 2D FINDINGS IN DCM
LV size
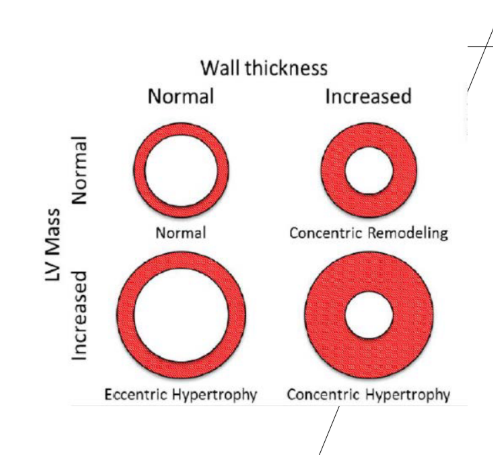
What happens to the mass in the LV
What shape configuration of the LV?
what happens to the global LV systolic function ?
what 3 things can you use to see that^?
what may be present?
Left ventricular enlargement
• Increased Left Ventricular Mass
(reflects a heart attempting to compensate for damage by stretching and growing to maintain its ability to pump blood, eccentric hypertrophy.)
• Spherical configuration of the LV
• Decreased global LV systolic function indices
(indicate that the heart's main pumping chamber (the left ventricle) is weak and cannot effectively squeeze oxygen-rich blood to the body.)
• EF
• Global Longitudinal Strain
(a sensitive echocardiographic measurement that quantifies the percentage of shortening (deformation) of the heart's left ventricle muscle fibers from base to apex during systole.)
• Fractional Shortening
• RWMAs may be present (most of the time aren’t affected by CAD)
name 5 2D SECONDARY FEATURES OF THE LEFT SIDE
there will be possible what especially at the LV apex?
evidence of ventricular what? (what movement - hint)
abnormal what motion due to what delay?
what happens to the MV annulus and coaptation of the MV leaflets
what is seen of the MV leaflets due to what?
what is another important measurement in PLAX???????????
Possible mural thrombus, especially at the LV apex
• Evidence of ventricular dyssynchrony
• Abnormal septal motion due to conduction delay
• Dilated MV annulus and incomplete coaptation of the MV leaflets
• Tethering or tenting of MV leaflets due to LV remodeling
(secoundary & functional)
(LVID?)
Name 2D SECONDARY FEATURES OF THE RIGHT SIDE
size of the atria
size of the RV
may exhibit _____ RV function
list 5 measurements made for the RV function
what happened to the IVC with _____inspiratory collapse
Enlarged atria
• Right ventricular enlargement
• May exhibit decreased RV function (measured by the following)
• FAC %
• S’
• TAPSE
• RV strain
• RV 3D EF
• Dilated IVC with reduced inspiratory collapse
What happens with the Mass in DCM, explain:
Even though we have ______ to _____ walls the heart must accommadte to the volume _____ flow in order to do this it increases its _____
increased ___ comes from combination of ventricular ________ and _______ muscle ______
Even though we have normal to thin walls the heart must accommadate the volume over flow in order to do this it increase its mass,
increased mass comes from combination of ventricular didilatation and enlarge muscle cell
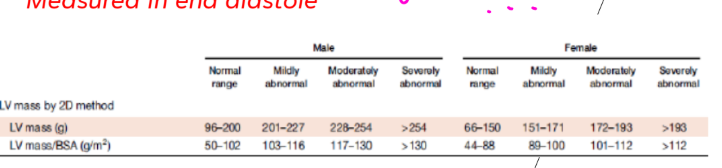
LV mass is increased in DCM
Increased LV mass = more total LV muscle/tissue than normal. In DCM, this often happens with LV enlargement/dilation, but LV mass is not the same as LV size; size is the chamber dimension, mass is the amount of myocardium.
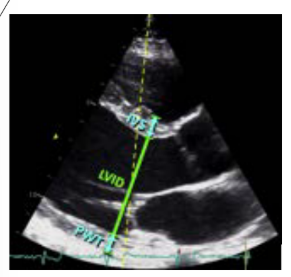
LV MASS: LINEAR METHOD
what are the three things we use here and when do we measure?
IVS- Interventricular septum
LVID- LV inner diameter
PWT- posterior wall thickness
Measured in end diastole
what happens to the LVID- LV inner diameter in DCM pt
LVID increase above normal limits in DCM
what is the linear method formula ?
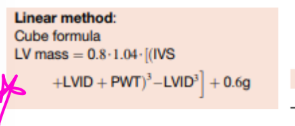
what type of hypertrophy does DCM have?
Eccentric Hypertrophy
SPHERICITY INDEX
what is it used to evaluate?
how do you calculate ?
what is it a predictor of in DCM patients?
To evaluate the shape of the LV
• Calculation of the ratio between ED length and width
• Predictor of survival in DCM patients
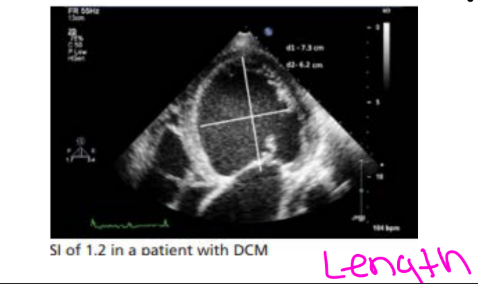
SPHERICITY INDEX
what number tell’s us it is poor prognosis?
A perfect sphere will be what number ?
<1.5 is poor prognosis
• A perfect sphere will equal 1
Tell me 3 ways we can determine LV SYSTOLIC FUNCTION?
EF measured by 2D Biplane method (4 & 2 chamber)
GLS
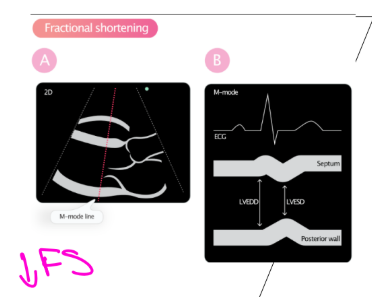
FRACTIONAL SHORTENING (FS%)
what is the EF formula, and how is the EF usally in DCM pt?
EF= (EDV-ESV)/EDV
EF is low in DCM pt (40-30 % severly abnormal)
Slove EF%
Example
4C EDV = 130 mL
4C ESV = 60 mL
2C EDV = 110 mL
2C ESV = 50 mL
EDV = 130 + 110 / 2 = 120 mL
averaged ESV = 60 + 50 / 2 = 55mL
120 - 55 / 120 = 65 / 120 × 100 = 54%
what is the normal value for GLS?
Normal value ≤ -18%
what is the formula for FRACTIONAL SHORTENING?
FS% = (LVEDD-LVESD/LVEDD) x 100
What is the normal % for FRACTIONAL SHORTENING
Normal 25-35%
Practice Problem: Fractional Shortening
A patient has:
LVEDD = 6.0 cm
LVESD = 4.8 cm
Calculate the FS%.
FS% = [(LVEDD − LVESD) / LVEDD] × 100
Work:
FS% = [(6.0 − 4.8) / 6.0] × 100
FS% = (1.2 / 6.0) × 100
FS% = 0.20 × 100
FS% = 20%
Answer: FS = 20%
Interpretation:
Normal FS is about 25–35%, so 20% is reduced, suggesting decreased LV systolic function in DCM.
What suggests LV systolic function seen in dilated CM?
A reduced FS suggests LV systolic function seen in dilated CM
A reduced FS suggests LV systolic dysfunction.”
FRACTIONAL SHORTENING is less accurate in what two things?
RWMAs
• LV dilation/ remodeling
whats more accurate way of finding EF is it using the FS% or Biplane method?
Biplane method
LV DIASTOLIC FUNCTION
What do we need? (things we need to assess / obtain while scanning?) name 5
Pulmonary veins
• MV inflow PW
• MV annulus TDIs
• LAVi
• TR
LV DIASTOLIC FUNCTION
what are two things that are associated with this (patho and hemodyanmics)
name 2, what is typically the grade? what happens to the ventricle and LVEDP?
• Typically grade II or greater
• Stiff noncompliant ventricle increases the LVEDP
what RWMA’S do we see with DCM?
“Global hypokinesis with severely reduced LV systolic function”
what does “Global hypokinesis mean (meaning as in the segments of the heart whats going on with them?)
All segments of the heart are reduced uniformly
RWMA’S:
typical cause..? DCM is the most common form of what?
non ischemic cardiomyopathy (due too myocardial disease not cause by CAD, but not all non ischemic cardiomyopathy is DCM other things that can cause it)
“Typical cause: non-ischemic cardiomyopathy” means:
When the LV is weak everywhere equally — called global hypokinesis — it is more typical of non-ischemic cardiomyopathy.
Non-ischemic means the weakness is not mainly from blocked coronary arteries or a heart attack.
When RWMAs can be seen in a DCM looking heart
what are the other factors we can see, name 4
^if the heart looks like DCM but you see regional wall motion abnormalities, think about an underlying cause.
RWMA suspect a primary or secoundary causes?
Ischemic cardiomyopathy = poor blood flow/CAD caused damage (artery clog)
Prior MI with remodeling = old heart attack damaged one region, then LV remodeled/dilated
Myocarditis = inflammation damaged parts of the myocardium
Pacing induced/LBBB DCM = electrical delay causes abnormal contraction pattern
These are considered secondary causes because something else damaged that region of myocardium.
Simple flashcard:
RWMAs suspect a secondary cause
DCM usually causes global hypokinesis
That means the whole LV is weak everywhere, kind of evenly.
But RWMA = regional wall motion abnormality
That means only certain walls/segments are moving poorly, while other areas may move better.
So your teacher is saying:
If the LV looks dilated like DCM but only certain regions are abnormal, that may suggest the DCM appearance is from a secondary cause, such as:
Ischemic cardiomyopathy = poor blood flow/CAD caused damage
Prior MI with remodeling = old heart attack damaged one region, then LV remodeled/dilated
Myocarditis = inflammation damaged parts of the myocardium
Pacing induced/LBBB DCM = electrical delay causes abnormal contraction pattern
The key line is: “RWMAs suspect a secondary cause.” That means RWMAs make you think, “Why is only part of the ventricle abnormal?” instead of simple non-ischemic DCM where the weakness is usually more global.
what does Spontaneous echo contrast tell you
LV smoke
describe what LV smoke is?
Temporary RBC ______occurring in fresh blood in a ____flow state
____flow sate causes concern for what?
what does it cause’s a concern for? name 3
Temporary RBC clumping occurring in fresh blood in a low flow state
• Low flow sate causes concern for thrombus formation
• LV thrombus & Mural or Apical thrombus
when we see LV smoke what should we used and espically when what?
Always use Definity contrast with poor endocardial definition and/or EF<30%.
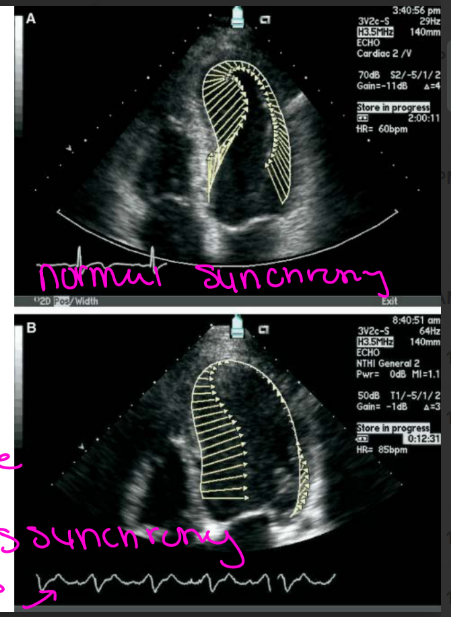
what does DYSSYNCHRONY mean?
The heart muscle does ____ contract in a ____ matter in DCM
The heart muscle does not contract in a uniform matter in DCM
(the septal and lateral wall are not firing at the same rate)
in DYSSYNCHRONY
what does the LV do to affect the conduction pathways, and how is it affected ?
Name two things that are altered?
LV enlargement-longer conduction pathways
• Altered myocyte alignment and calcium handling
( due to the myocardium stretches and remodles in DCM thats why get those longer condution pathways and fire at different rates - thats what dyssynchront is)
Myocytes = heart muscle cells
They are supposed to be organized in a way that helps the LV squeeze efficiently.
Altered myocyte alignment means the muscle cells/fibers are stretched, remodeled, and not lined up as well because the LV is enlarged/dilated.
Calcium handling means how heart cells use calcium to contract and relax. Calcium is like the “signal” that tells the muscle cell to squeeze. If calcium handling is abnormal, the contraction becomes weaker or delayed.
in DYSSYNCHRONY what are the electrical components in the pt name two and what is it associated with?
what happens with the QRS
what arrthimya is there
associated with what function and outcomes
Wide QRS
LBBB (electrical and mechanical dyssynchrony, 30 -40 % common to see in DCM - very common to see
Associated with worse LV function and outcomes
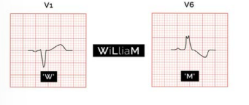
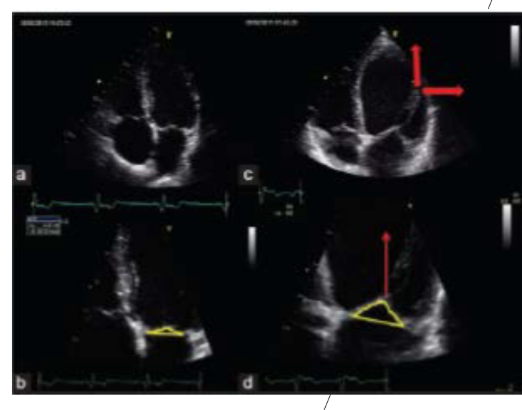
what is this showing?
LBBB
For DYSSYNCHRONY what are the mechanical things we see on echo
talk about te LV segments contraction***
septal motion
apex moves how
Different LV segments contract at different times****
Early inward septal motion
Apex moves side to side
in DCM pt what will be the size of the LA
Will have LA enlargement
In DCM pt what happens to the MV annulus and coaptation of the MV leaflets what does this lead to?
Dilated MV annulus and incomplete coaptation of the MV leaflets leads to MR (secondary/functional MR)
In DCM pt tethering or tenting of MV leaflets due to what?
Tethering or tenting of MV leaflets due to LV remodeling (this secoundary / functional)
what is the MR CONTINUITY EQUATION / Regur volume
SV of MV = MV CSA x MV VTI
SV LVOT = LVOT CSA x LVOT VTI
Regurgitant Volume = SV MV – SV LVOT
MR CONTINUITY EQUATION, what is the regur fraction

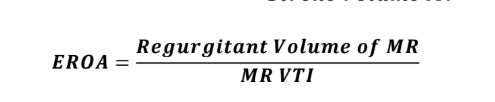
MR CONTINUITY EQUATION, what is the EROA?
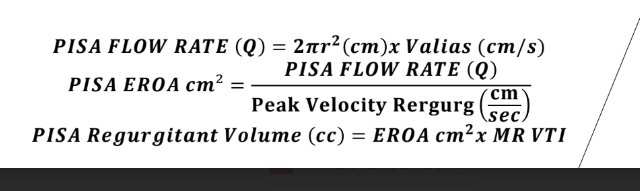
MR PISA EQUATION & EROA & Regurgitant volume
for the RIGHT HEART , what are findings that you can associated with DCM pt name name 5, and name 5 ways which allow you determine the RV function that can tell us the EF / how well the RV is functioning?
there is what due to the backflow of blood
what is the size of the atria
what is the size of the RV
May exhibit _____ RV function
What happens with the IVC with ______inspiratory collapse
list 5 measurement
PHTN (due to the backflow)
• Enlarged atria
• Right ventricular enlargement
• May exhibit decreased RV function
• FAC %
• S’
• TAPSE
• RV strain
• RV 3D EF
• Dilated IVC with reduced inspiratory collapse
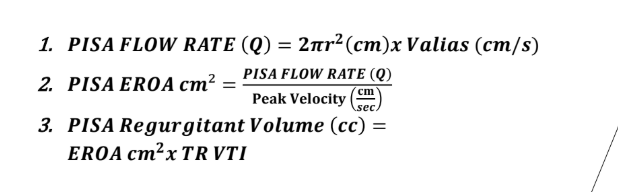
TRICUPSID REGURGITAITON
PISA fllow rate formula
EROA
Reg vol
PHTN
What images do we need for assessment? name two and give me the formula that we would use
TR signal
• IVC assessment
• RVSP = 4(TR Velocity)2 + RAP
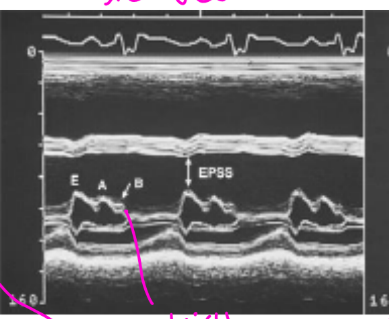
M-MODE CHARACTERISTICS IN DCM tell me 3
EPSS >6 MM
• B-BUMP
• DECREASED AORTIC ROOT MOTION AND EARLY AVC (b/c of decreased CO)
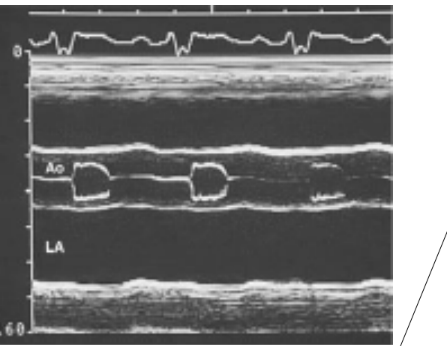
what does EPSS > 6 MM tell us? and what does it indicate
Large space between the mitral anterior leafleat and septal wall, indicates a decreased EF
what does the B-Bump tell us?
High LVEDP and LAP
(MV leafleats remain semi open in diastole it occurs b/c the LAP exceeds the LV pressure which prolongs the a wave for a little and thats why you see the b - bump)
Pracrice MATH
MR PISA Radius is 1.0 cm
Aliasing Velocity is 34 cm/s
MR Peak Velocity 480 cm/s
MR VTI 132.2 cm
answer 58 ml