EKG quiz 2
1/74
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
75 Terms
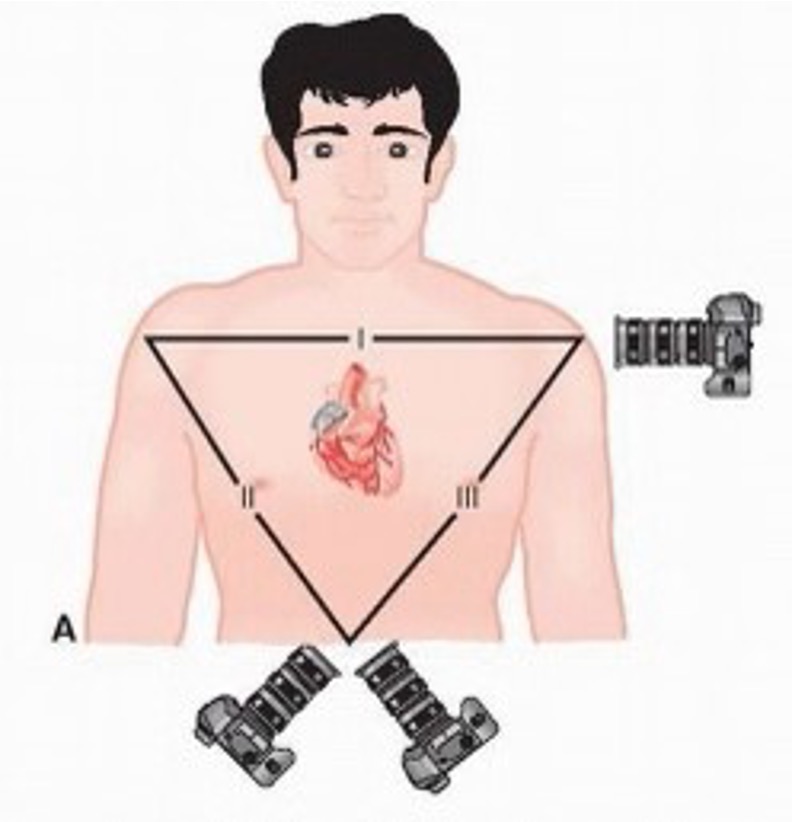
What are the limb / bipolar leads?
I- pos electrode on L shoulder, neg electrode on R shoulder
II- pos electrode on L foot, neg electrode on R shoulder
III- pos electrode on L foot, neg electrode on L shoulder
what are augmented leads?
one physical lead on pt, one theoretical neg pole in center of heart (Wilsons terminal)
aVL, aVR, aVF
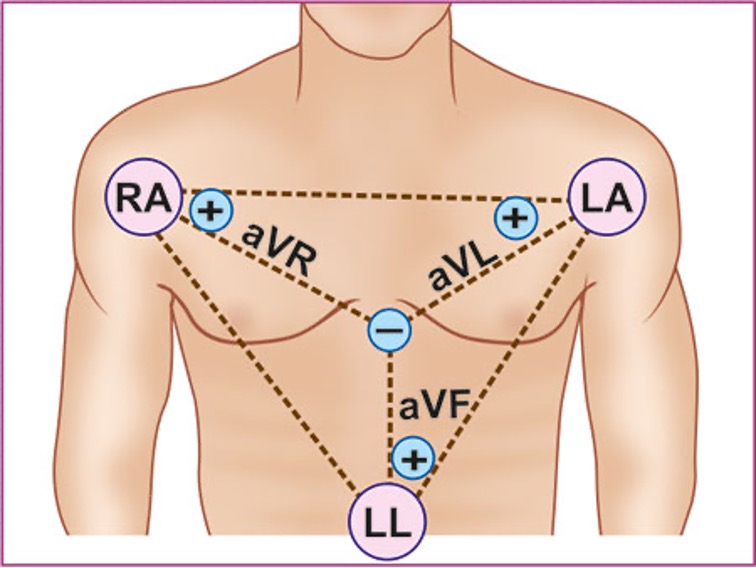
Where is aVL placed?
pos lead on L shoulder, looking at central terminal
where is aVR placed?
pos lead on R shoulder and looking at central terminal
where is aVF placed?
pos lead on L foot and looking up at terminal central
What are the hexaxial leads?
first 6 leads of 12 lead
I, II, III, aVR, aVL, aVF
What does the hexaxial reference system determine?
normal axis of heart
what are precordial / chest leads?
unipolar leads which use central terminal as neg pole
V1-V6
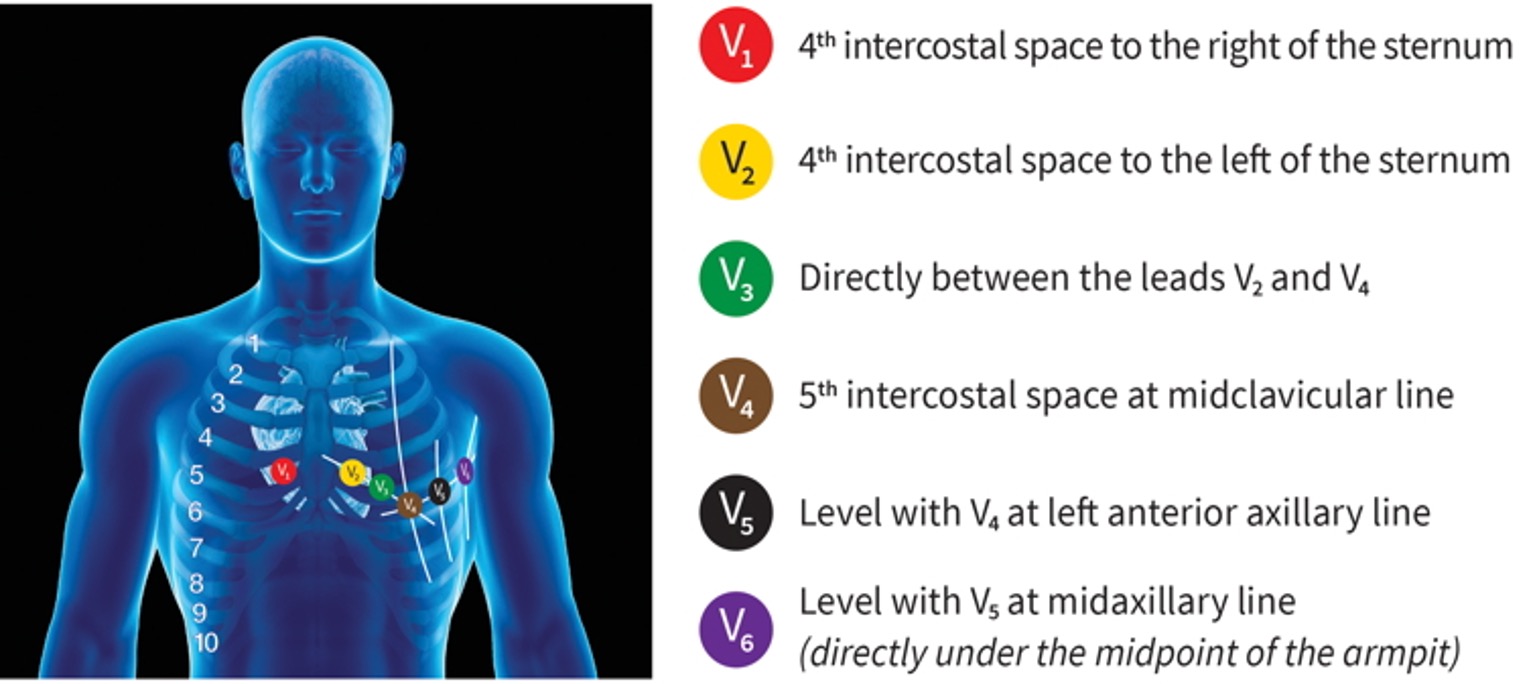
where is V1 placed?
4th ICS R of sternum
where is V2 placed?
4th ICS L of sternum
where is V3 placed?
directly bt V2 and V4
where is V4 placed?
5th ICS at midclavicular line
where is V5 placed?
level w/ V4 at left anterior axillary line
where is V6 placed?
level w/ V5 at midaxillary line (directly under armpit)
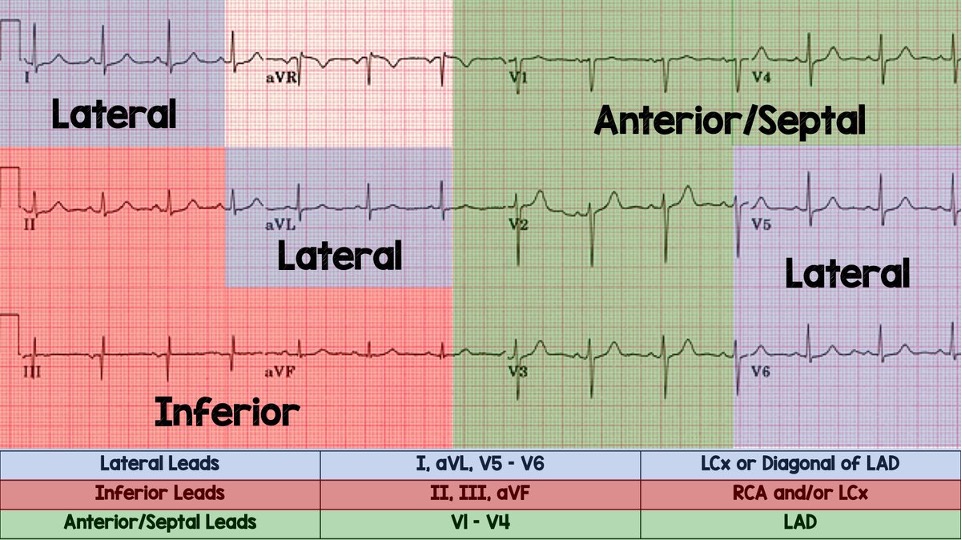
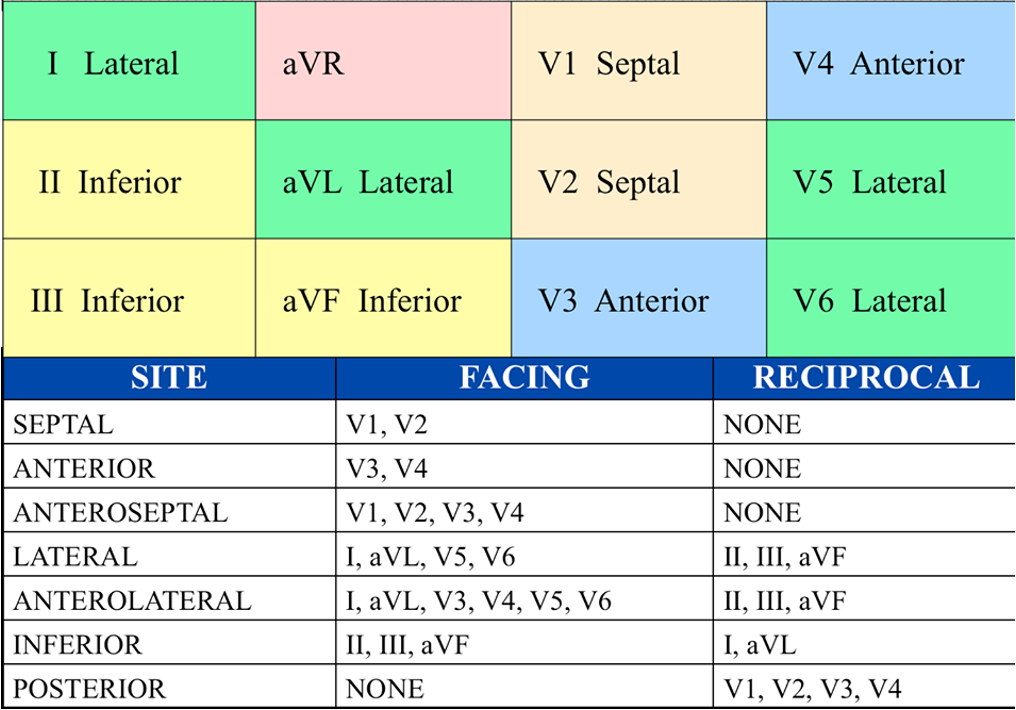
what leads look at septal wall?
V1 and V2
what leads look at anterior wall of LV?
V3 anda V4
what leads look at lateral wall of LV?
I, aVL, V5, V6
what leads look at inferior wall?
II, III, aVF
what are contiguous leads?
2 or more leads which look at same area of heart
-V1-V4
-II, III, aVF
-I, aVL, V5, V6
what leads are used to determine cardiac axis?
I and aVF
What would a normal axis look like on ECG?
both I and aVF mostly positively deflected
what would an ECG w/ LAD show?
I mostly pos. aVF mostly neg
What does RAD look like on ECG?
I mostly neg, aVF mostly pos
How does extreme RAD show on ECG?
both I and aVF mostly neg deflected
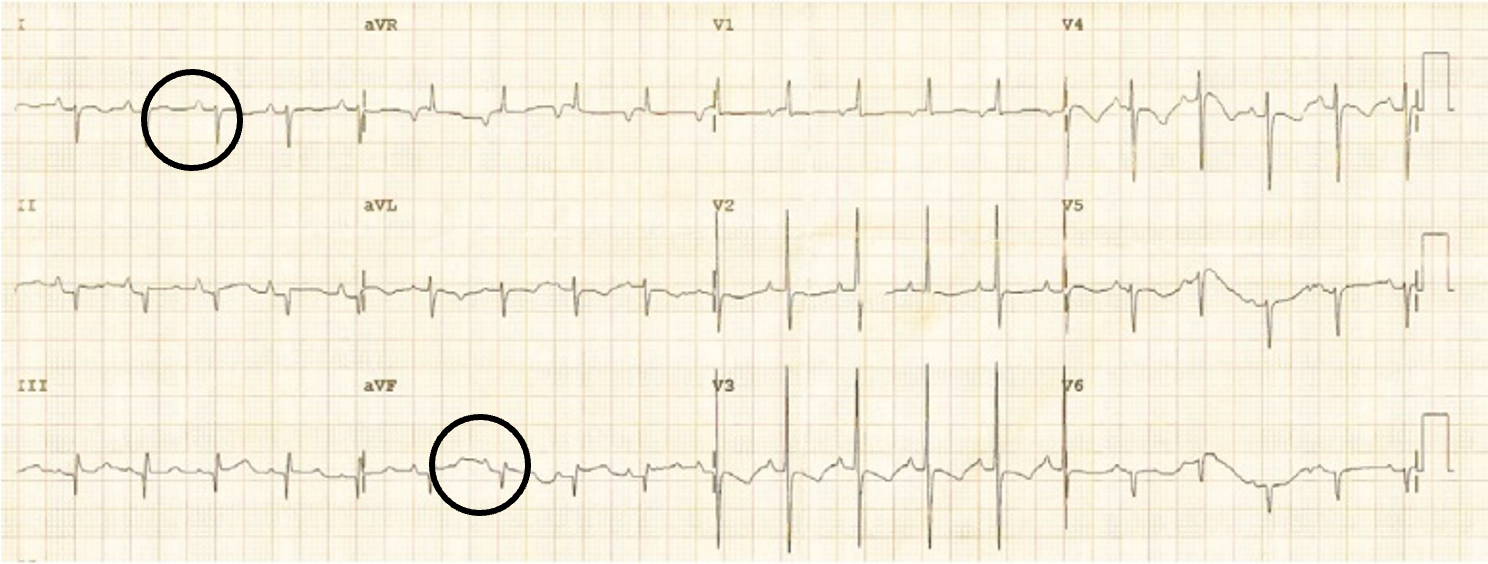
what is often very first sign of cardiac ischemia?
hyperacute T waves
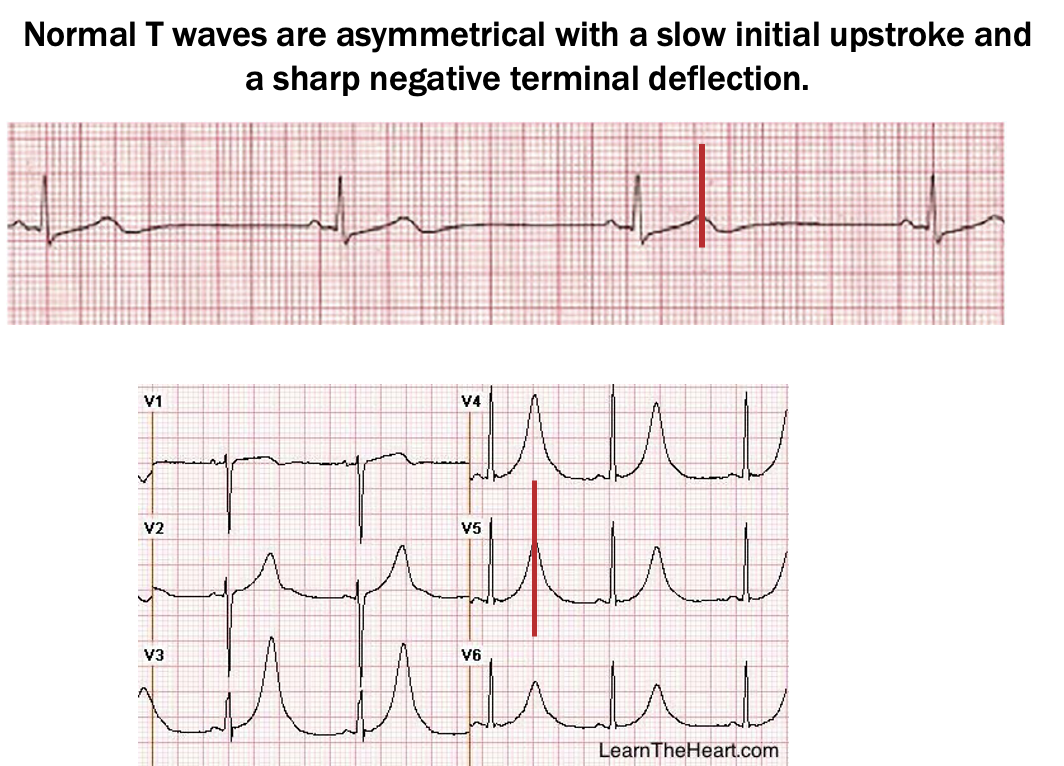
what are hyper acute T waves?
broad, inc in amplitudes and symmetrical
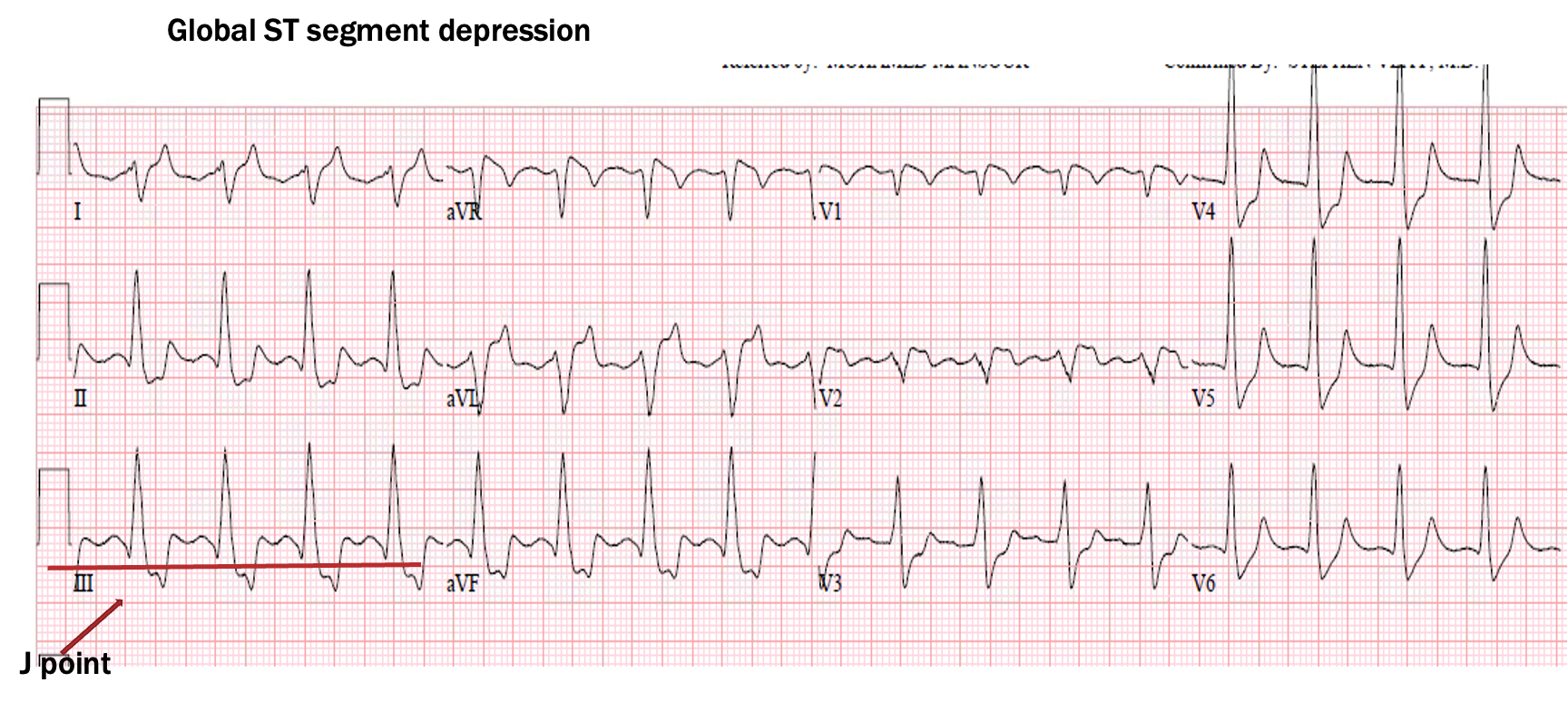
what represents subendocardial ischemia?
ST seg depression
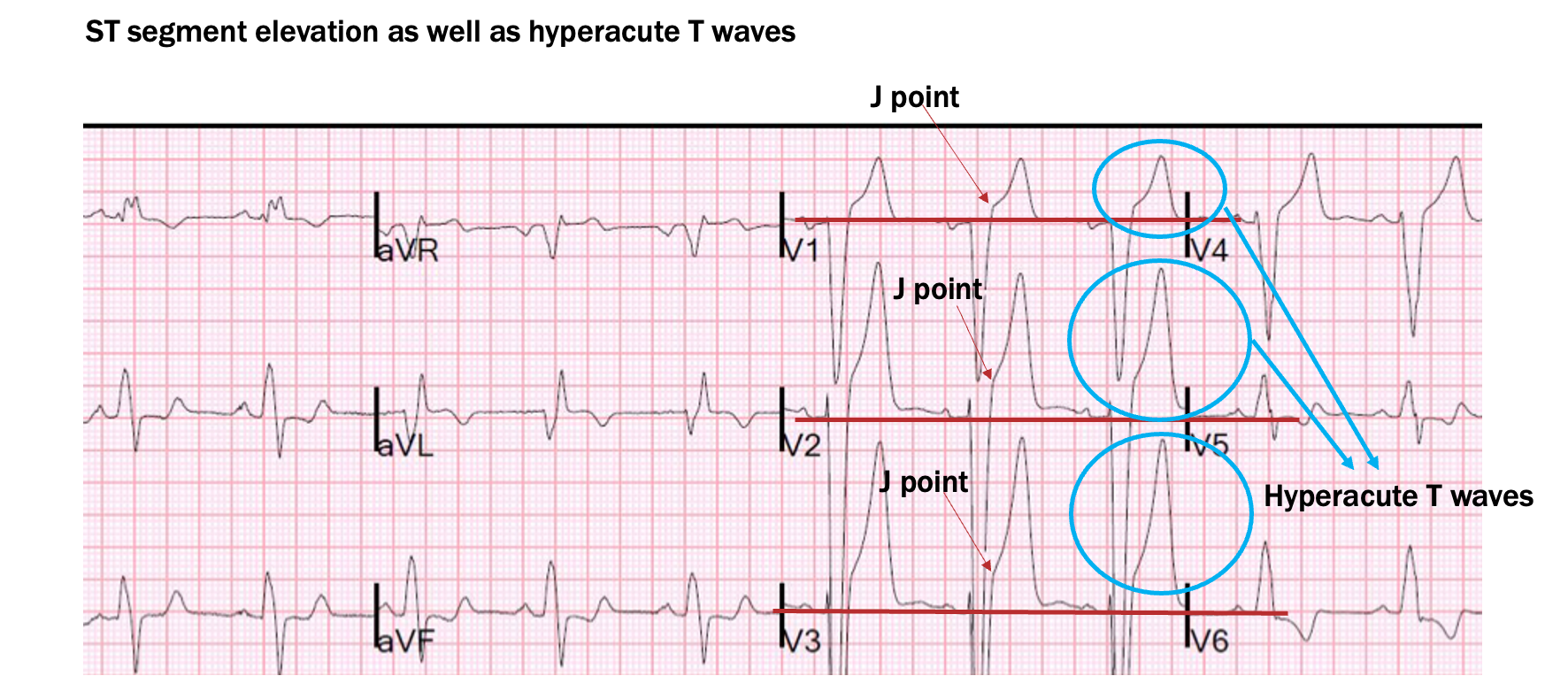
what represents transmural ischemia / injury?
ST seg elevation
What do pathological Q waves represent?
infarction and actual death of cardiac tissue, either from previous or acute cardiac event
What is criteria for pathological Q waves?
longer than 0.04 s in duration (1 small box)
deeper than 2 mm or 2 small boxes
or deeper than 25% of height of R wave if present
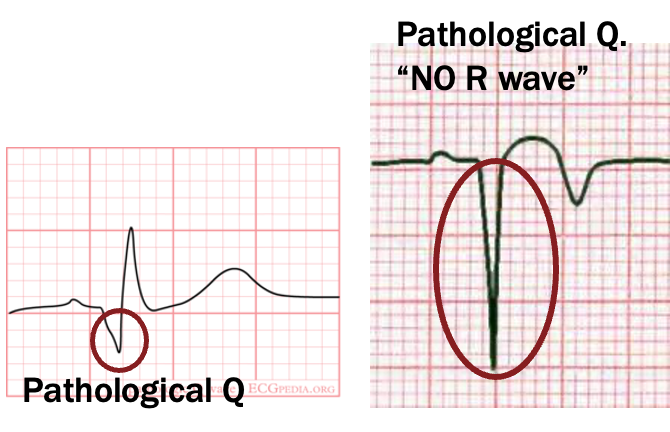
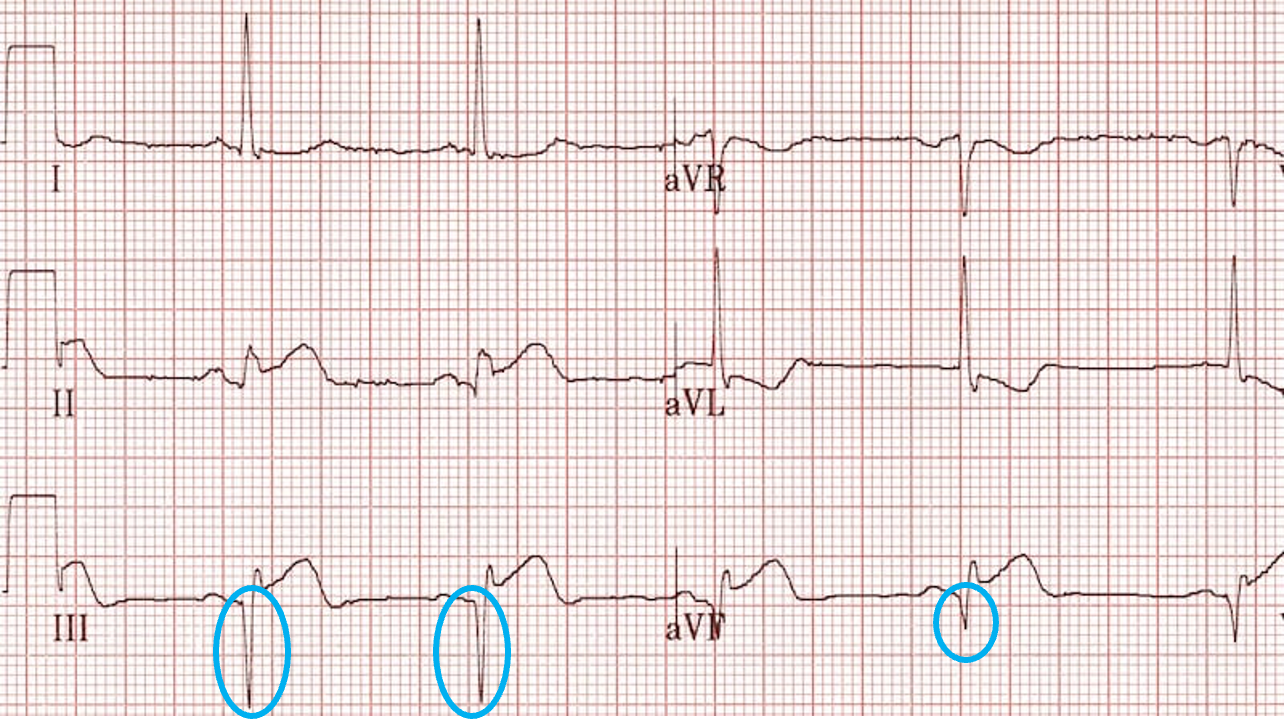
what is this
pathological Q waves
what are reciprocal changes?
mirror image of cardiac event on opposite leads which look at same area of heart
confirmatory sign of cardiac ischemia
list the reciprocal leads
septal: V1, V2 and none
anterior: V3, V4, and none
anteroseptal: V1-V4 and none
lateral: I, aVL, V5, V6 and II, III, aVF
anterolateral: I, aVL, V3-V6, and II, III, aVF
inferior: II, III, aVF and I, aVL
posterior: none and V1-V4
what is a STEMI?
1 mm or more of ST seg elevation in 2 or more contiguous leads w/ or w/o reciprocal changes
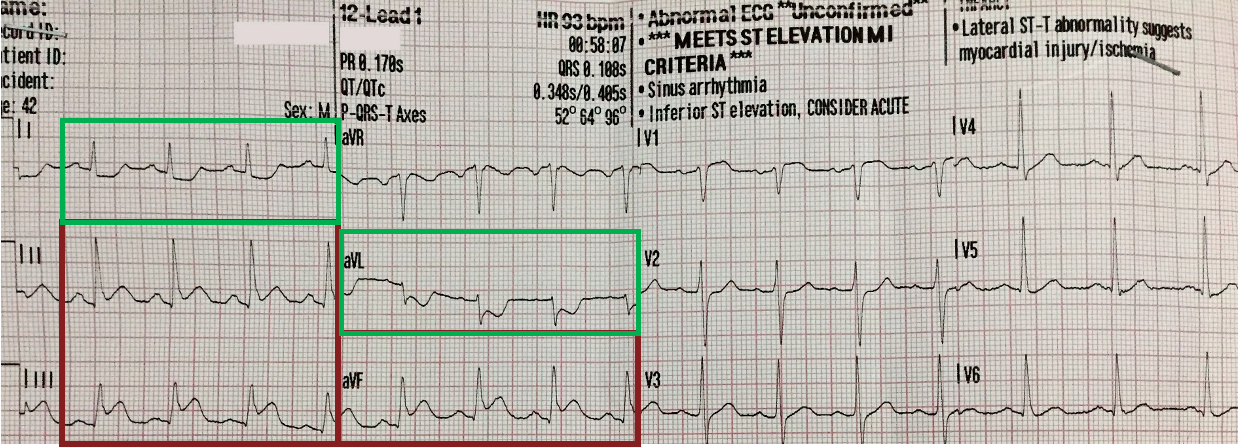
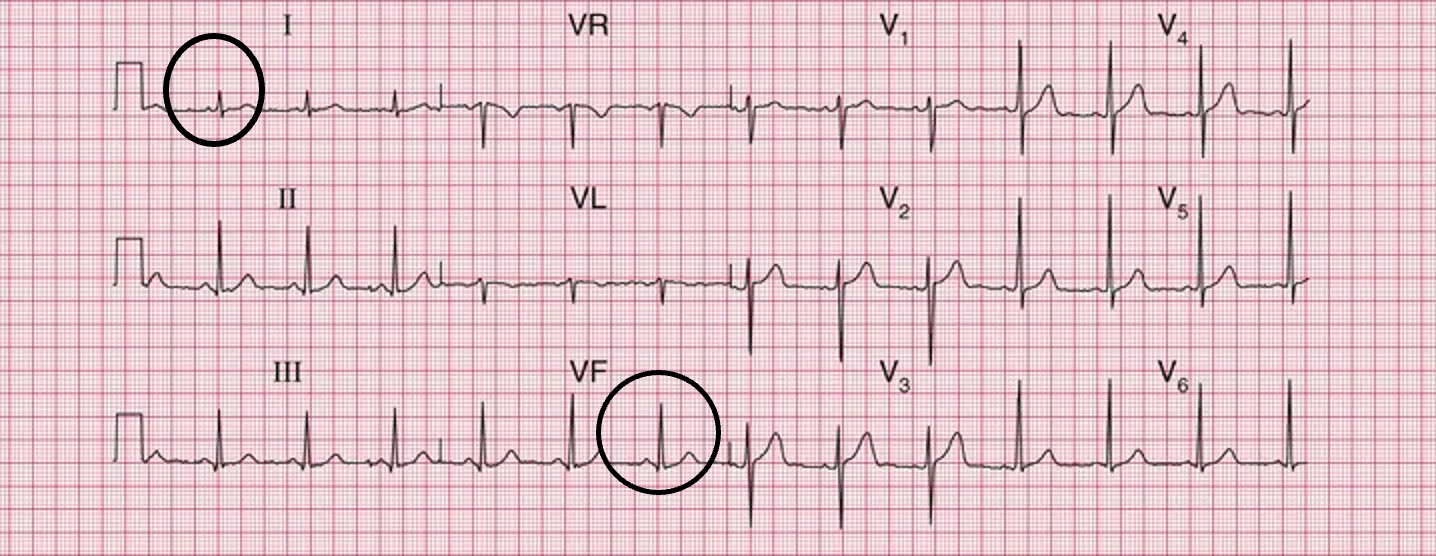
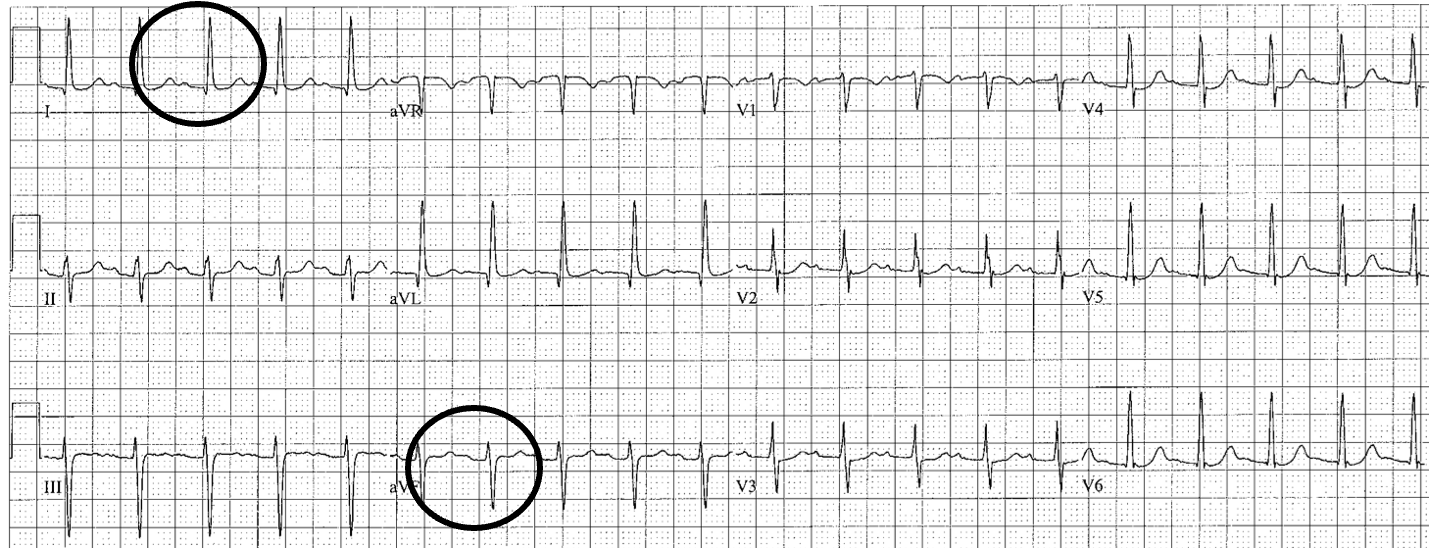
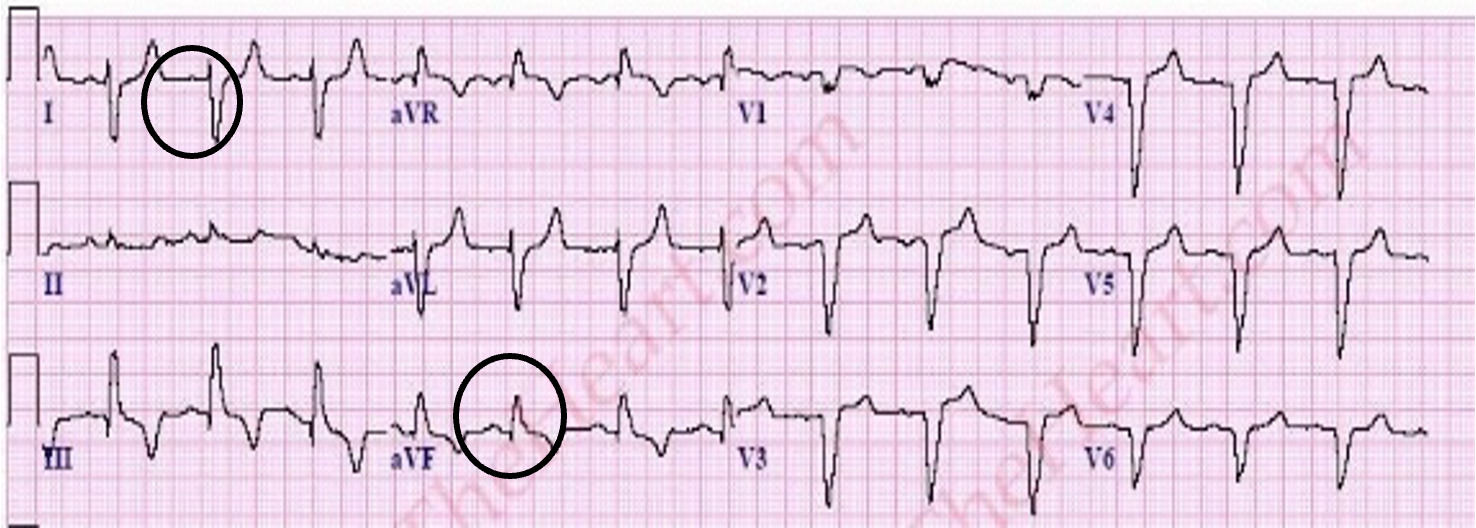
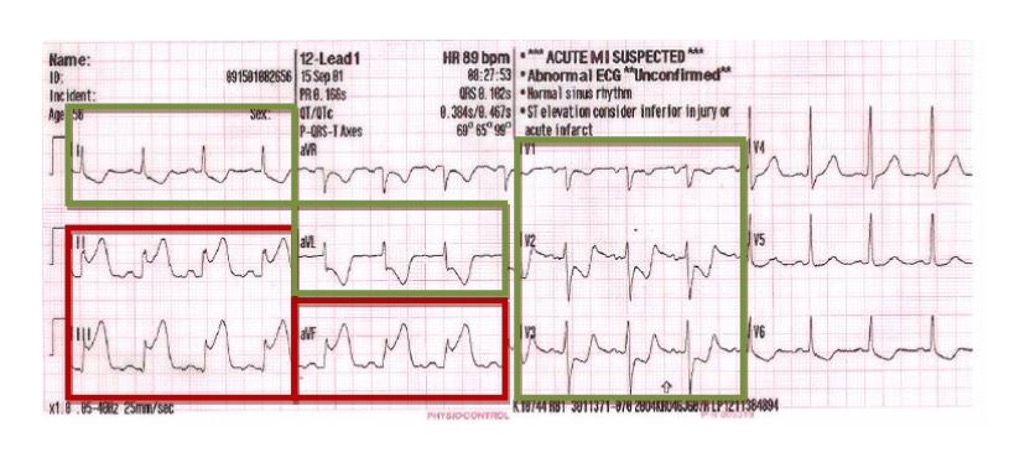
what is this?
lateral wall STEMI (elevation in lateral leads I and aVL, reciprocal depression in inferior leads III and aVF)
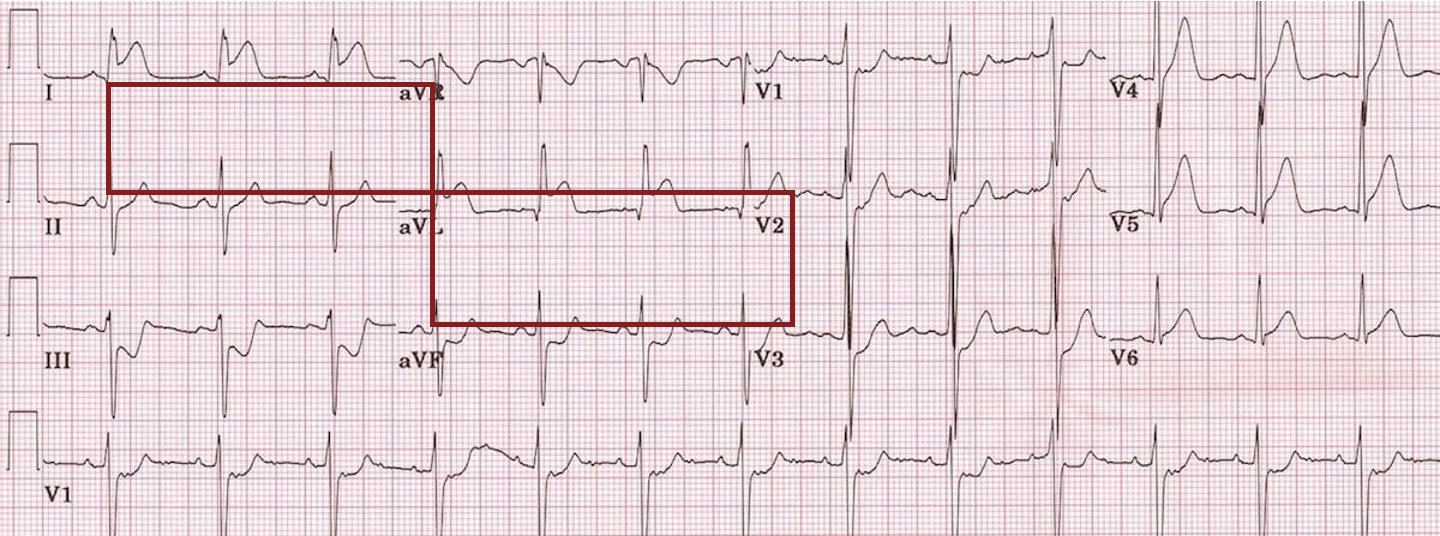
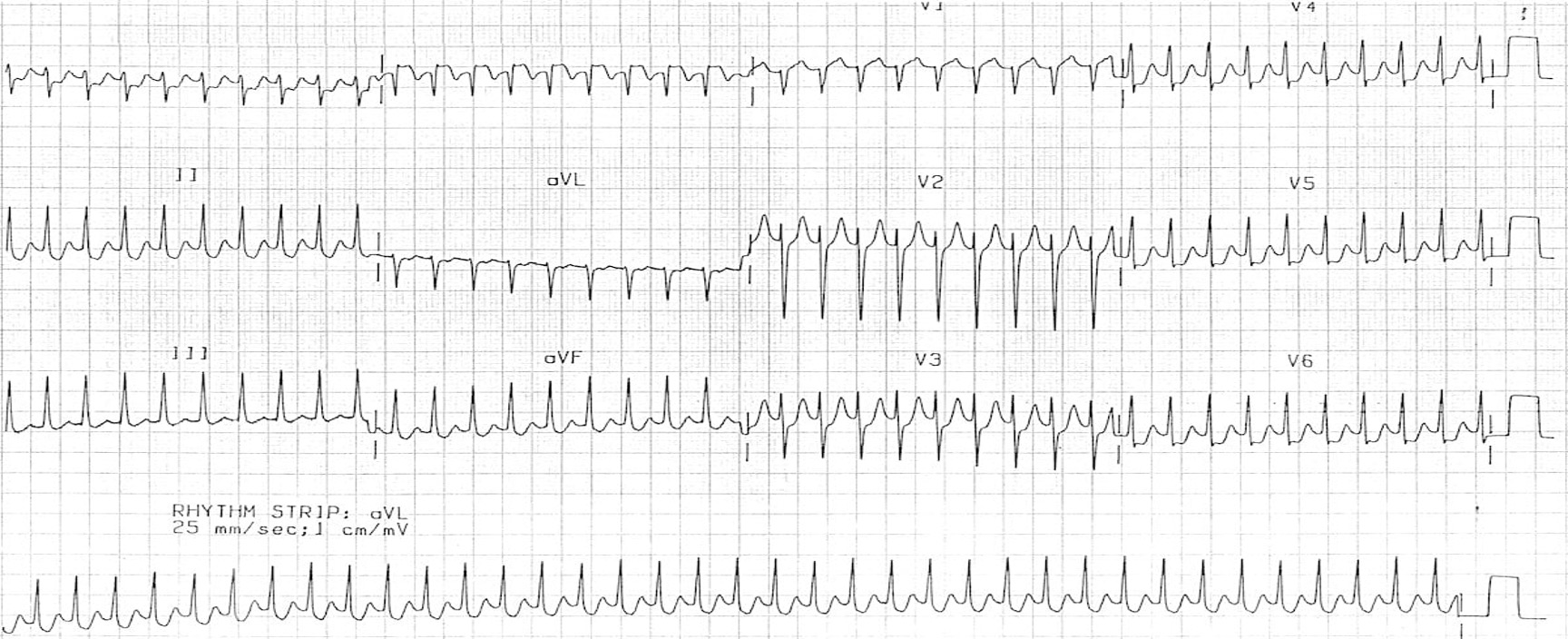
what is this?
antero-septal STEMI (elevation in anterior and septal leads V1-V3)
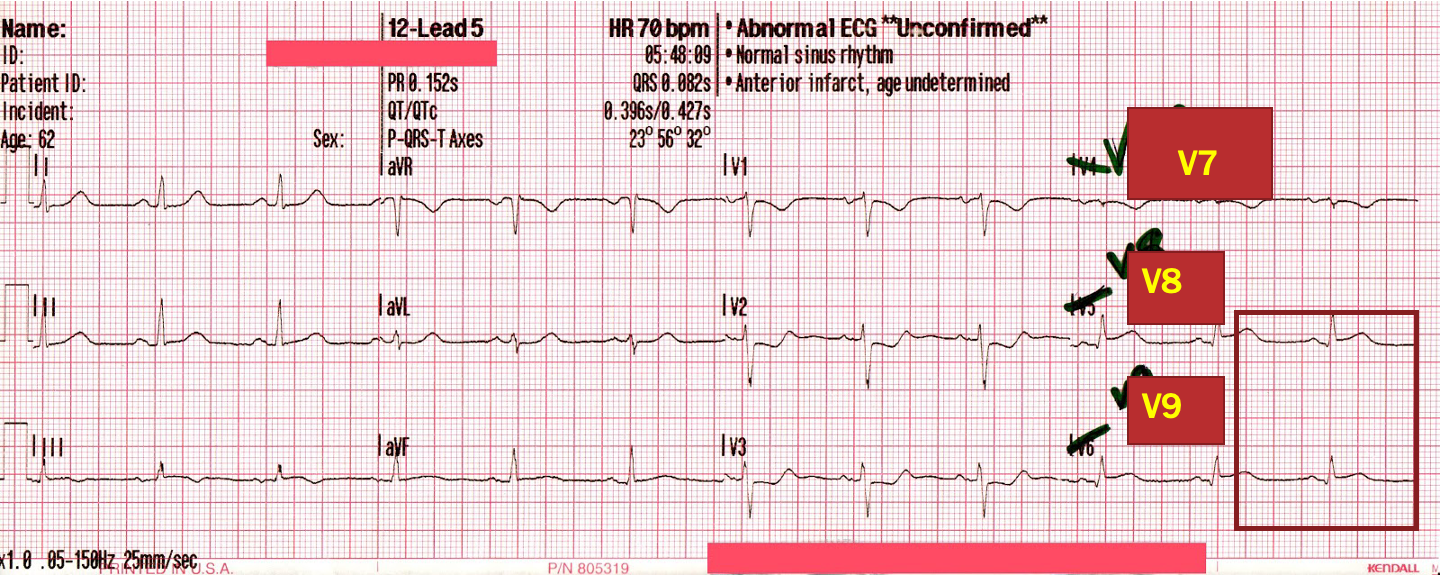
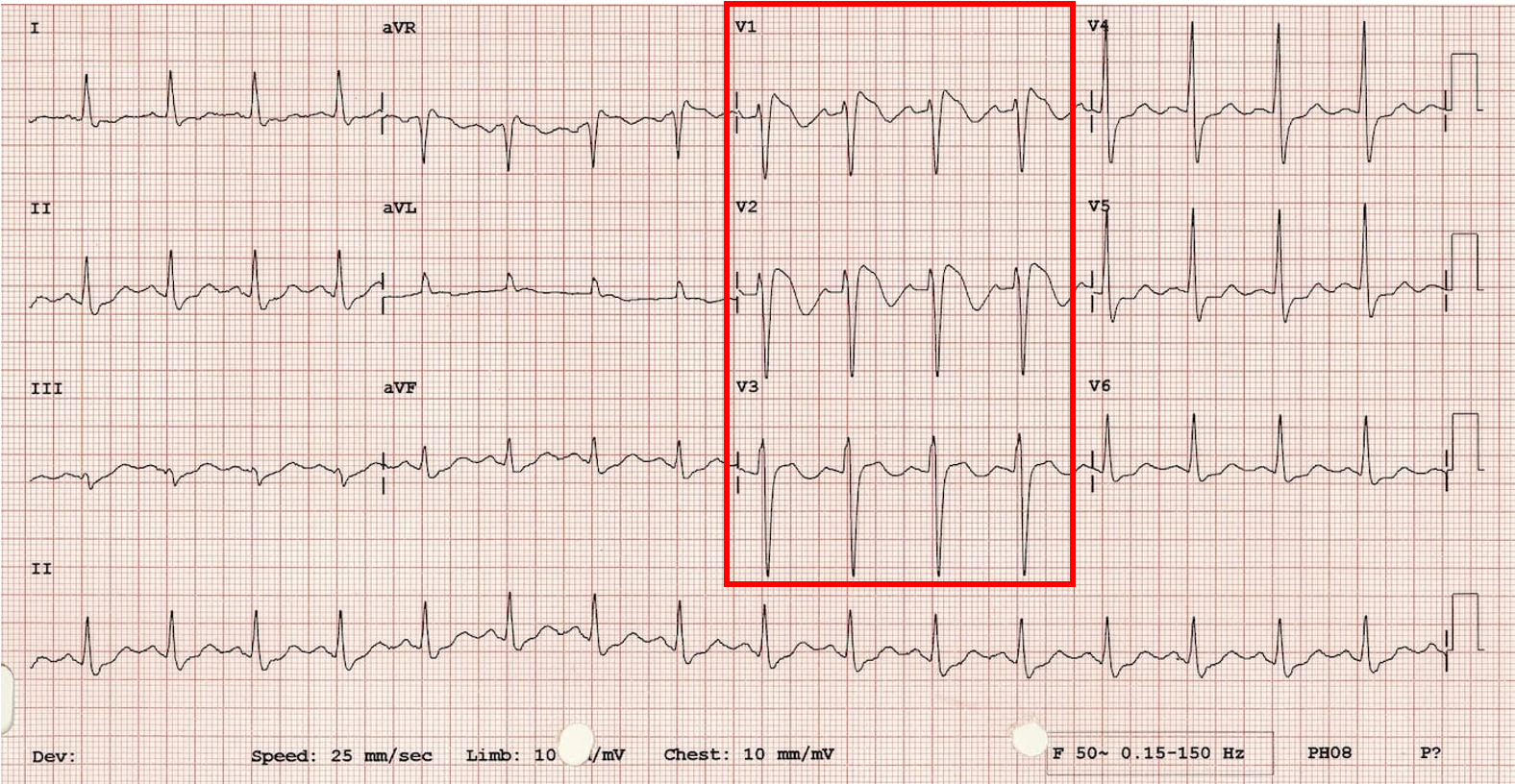
what is posterior STEMI?
isolated ST depression in V1-V4 w/ no ST elevation anywhere
typically result of occlusion/stenosis of Lcx; must obtain posterior EKG
how do you obtain posterior EKG?
V4-V6 moved to back of pt and labeled V7-V9; also referred to as 15 lead
st elevation in these confirms posterior wall STEMI
how do you r/o RV involvement in inferior STEMI?
V4 moved to R of sternum 5th ICS midclavicular line; marked as V4R
elevation confirms RV involvement
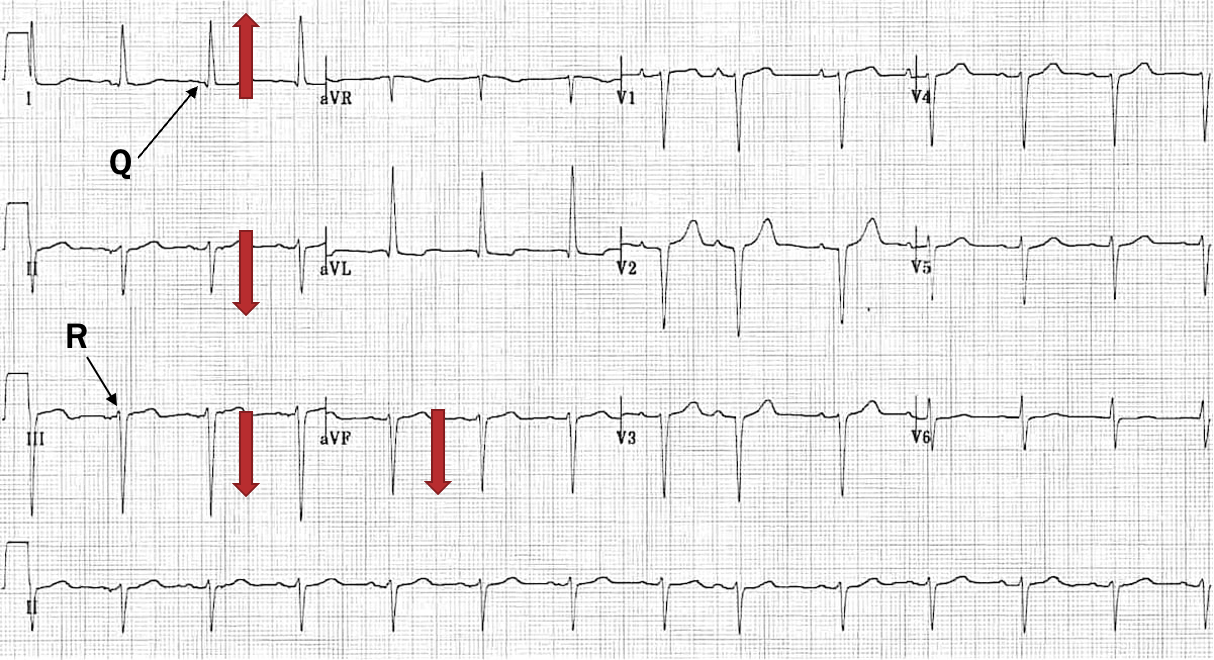
what is MC intraventricular conduction abnormality during acute MI?
LAFB
what is LAFB criteria?
LAD- pos I and neg aVF
Q wave in I and R wave in III- q1r3
mostly neg II
mostly neg III
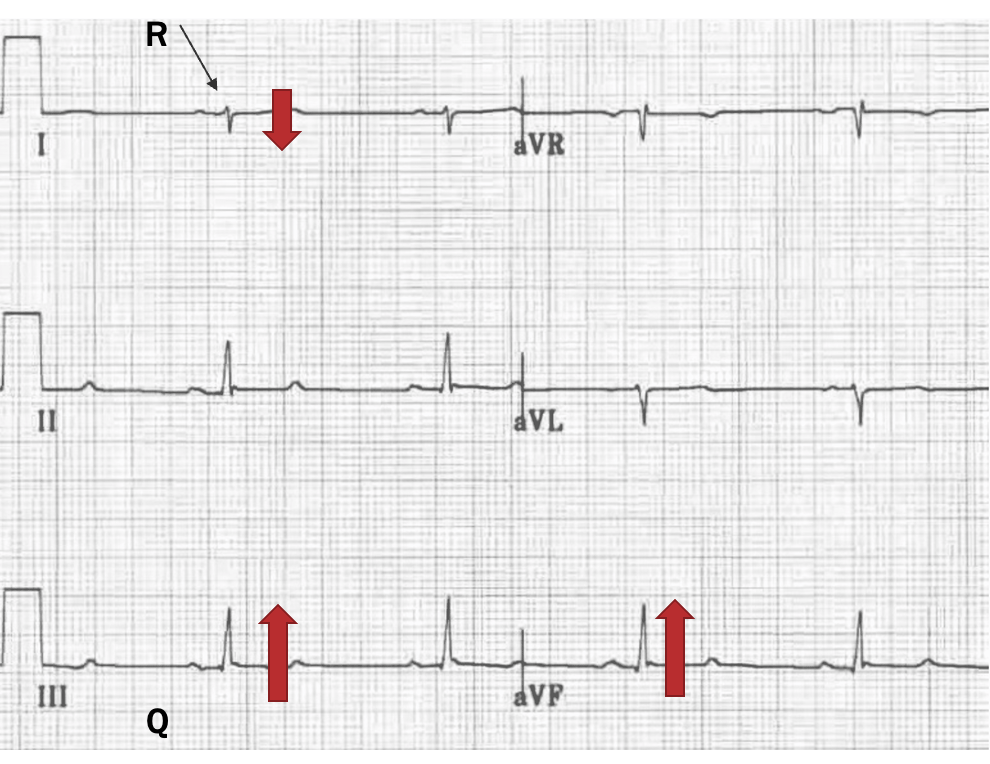
what is LPFB criteria?
RAD- neg I and pos aVF
R wave in I and Q wave in III- r1q3
mostly pos III
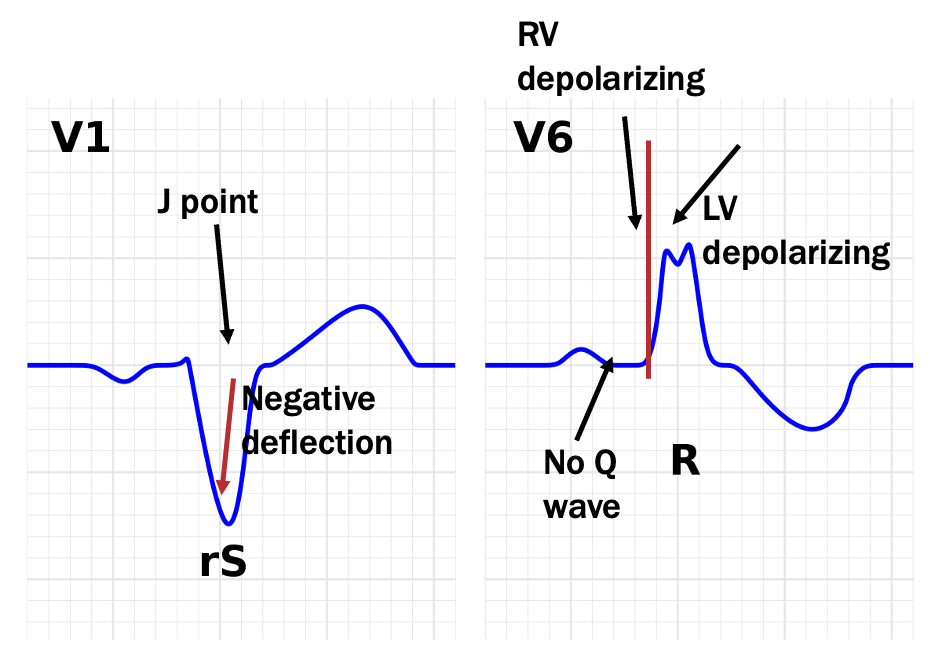
LBBB criteria
QRS complex longer then 0.12 s in duration (3 small boxes)- best measured in V1
RS pattern in V1- find J, travel backwards, first deflection is negative
double QRS- notching of QRS in lateral leads (I, aVL, V5, V6) best seen in V6
lack of Q waves in lateral leads
what is this?
LBBB- no Q in lat leads, notching of QRS, QRS wider than 0.12 s in V1, RS pattern in V1
RBBB criteria
QRS longer 0.12 s / 3 small boxes in V1
rSR pattern in V1- pos deflection behind J point
double QRs- slurred S waves in lateral leads (I, aVL, V5, V6) best seen in V6
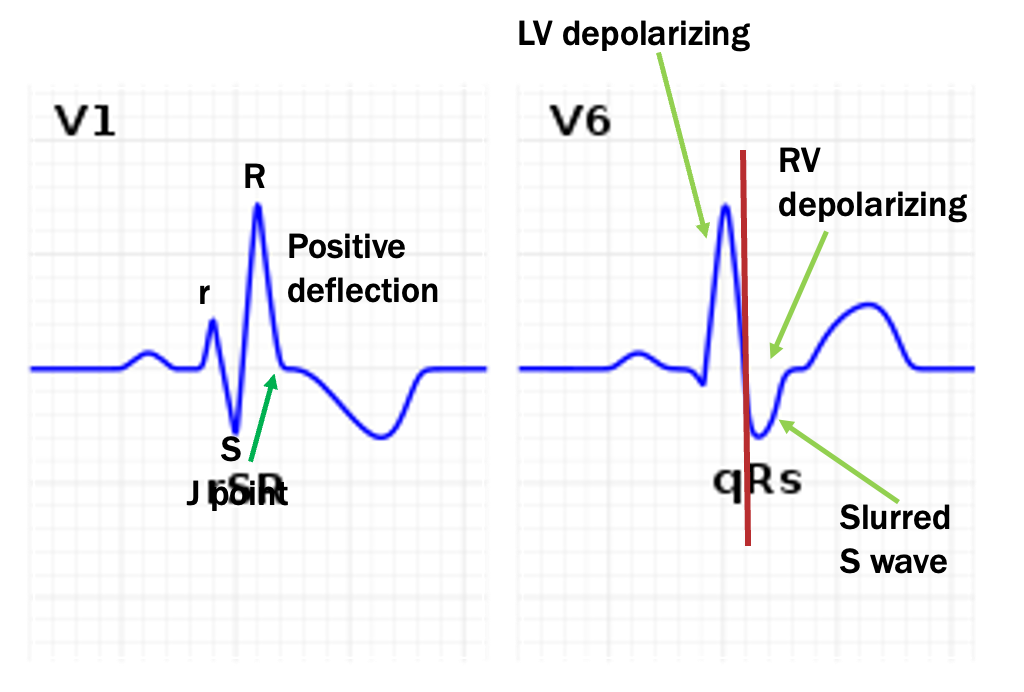
what is this?
RBBB- slurred S in lat leads, rSR pattern and QRS wider than 0.12 s in VI
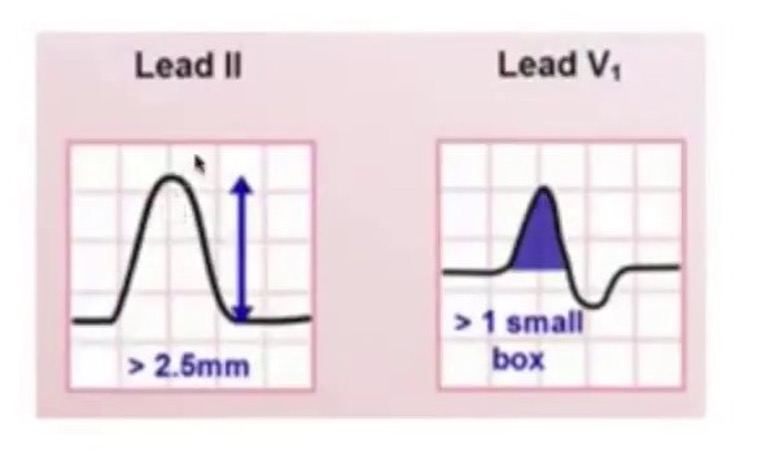
what is RAE also known as?
P-pulmonale
what is criteria for RAE?
upright P wave taller than 2.5 mm in limb leads
biphasic P wave w/ lager pos initial deflection and neg smaller terminal deflection in V1
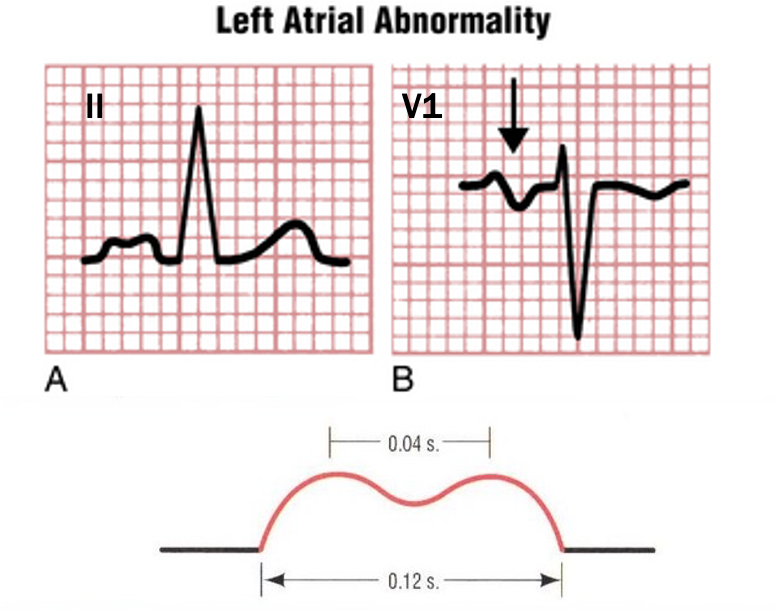
what is LAE also known as?
P-mitrale
What is criteria for LAE?
upright humped P wave at least 0.12 s in duration and 0.4 s distance bt humps
biphasic P wave w/ small initial pos deflection and large neg terminal deflection in V1
RHV criteria
R:S ratio 1mm or more in V1-V2 (more R than S)
supportive:
RAE
RAD
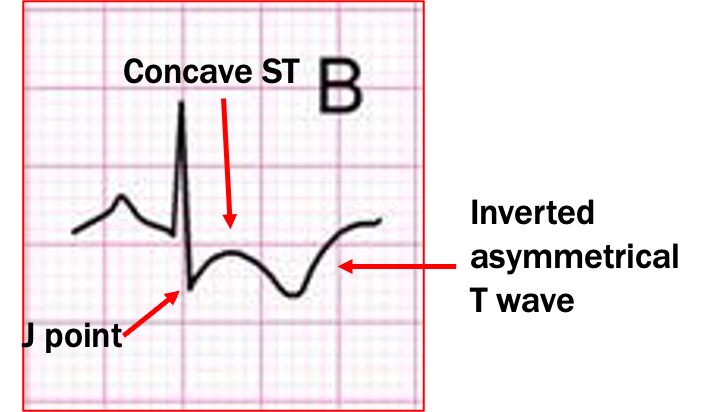
strain pattern- concave ST set turning into inverted asymmetrical T wave in V1-V2
exclusionary: RBBB, posterior wall MI, children < 8
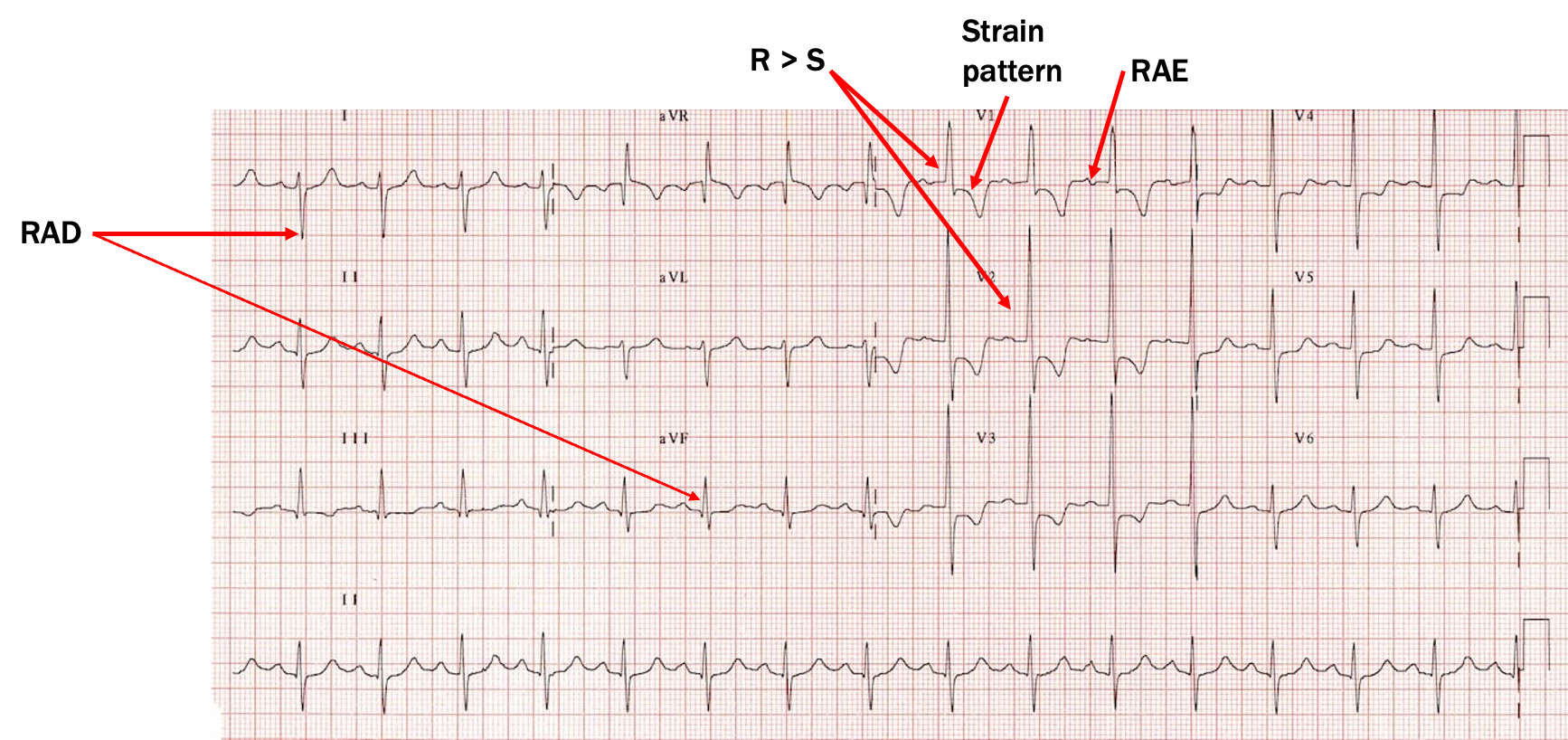
what is this?
RVH
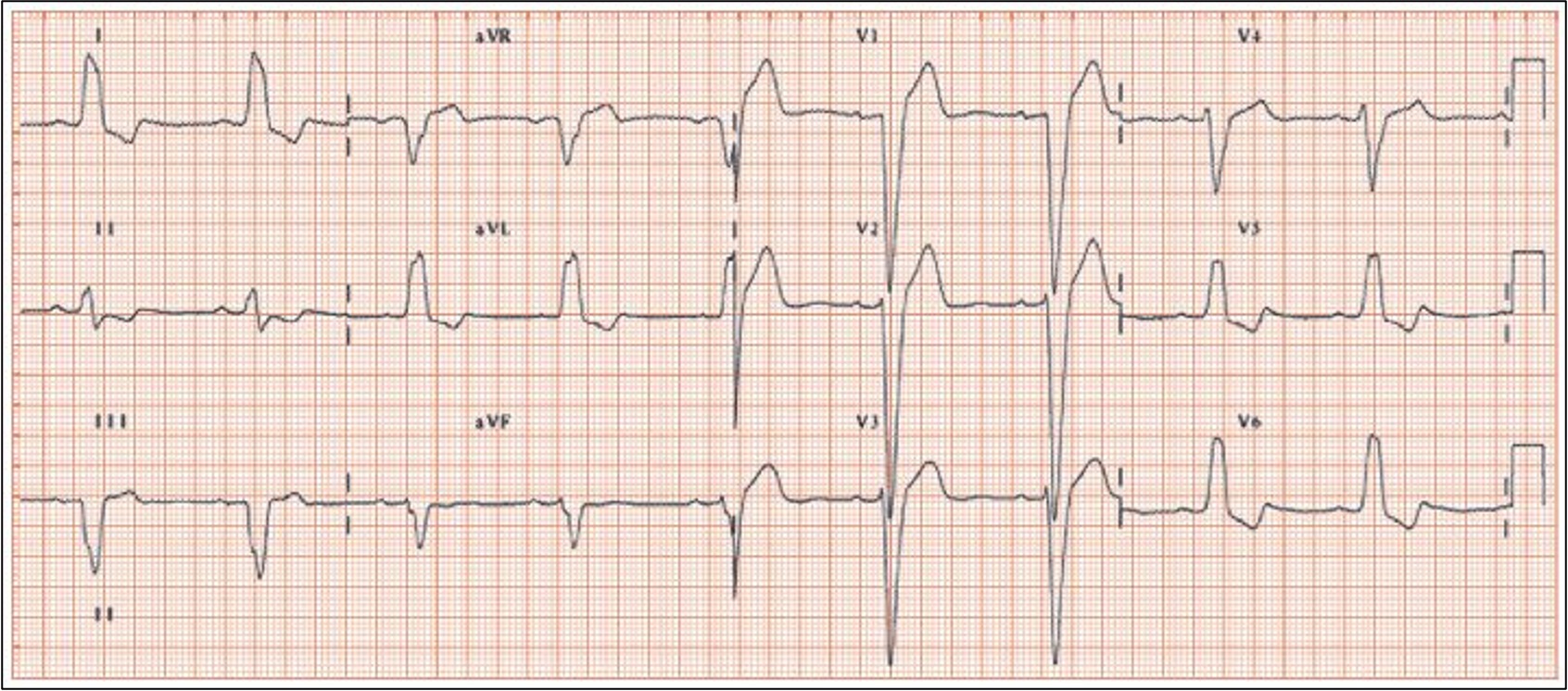
LVH criteria
causes LAD w/ deep S waves in V1-V2 and tall R in lat leads
add deep S to taller R = equal to or greater than 35 mm
R wave in aVL greater than 12mm
any chest leads greater than 45 mm
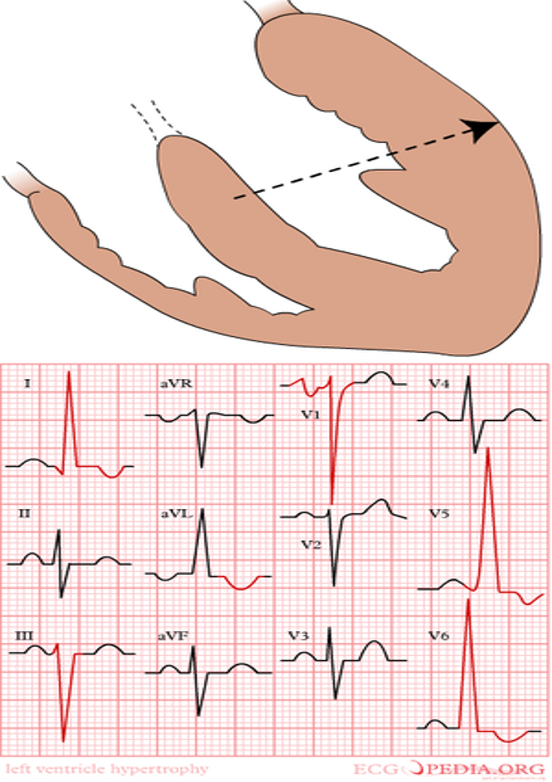
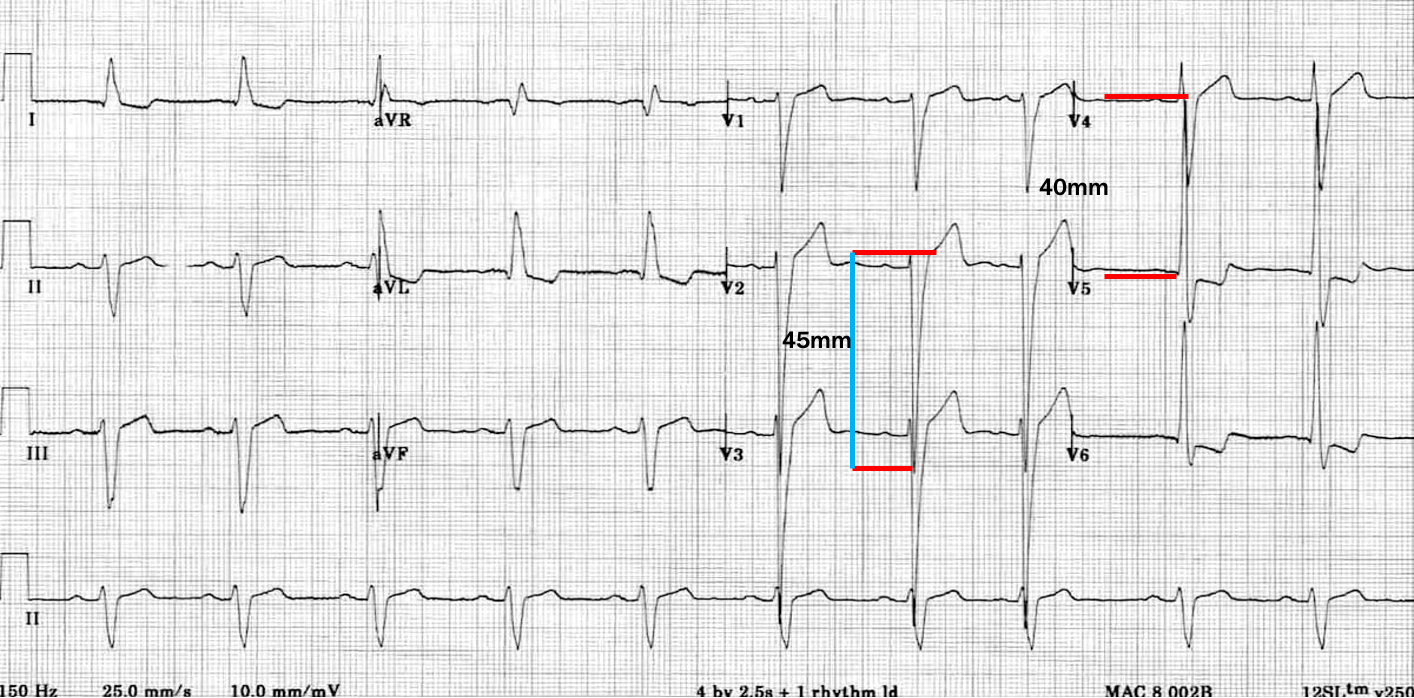
what is this?
LVH
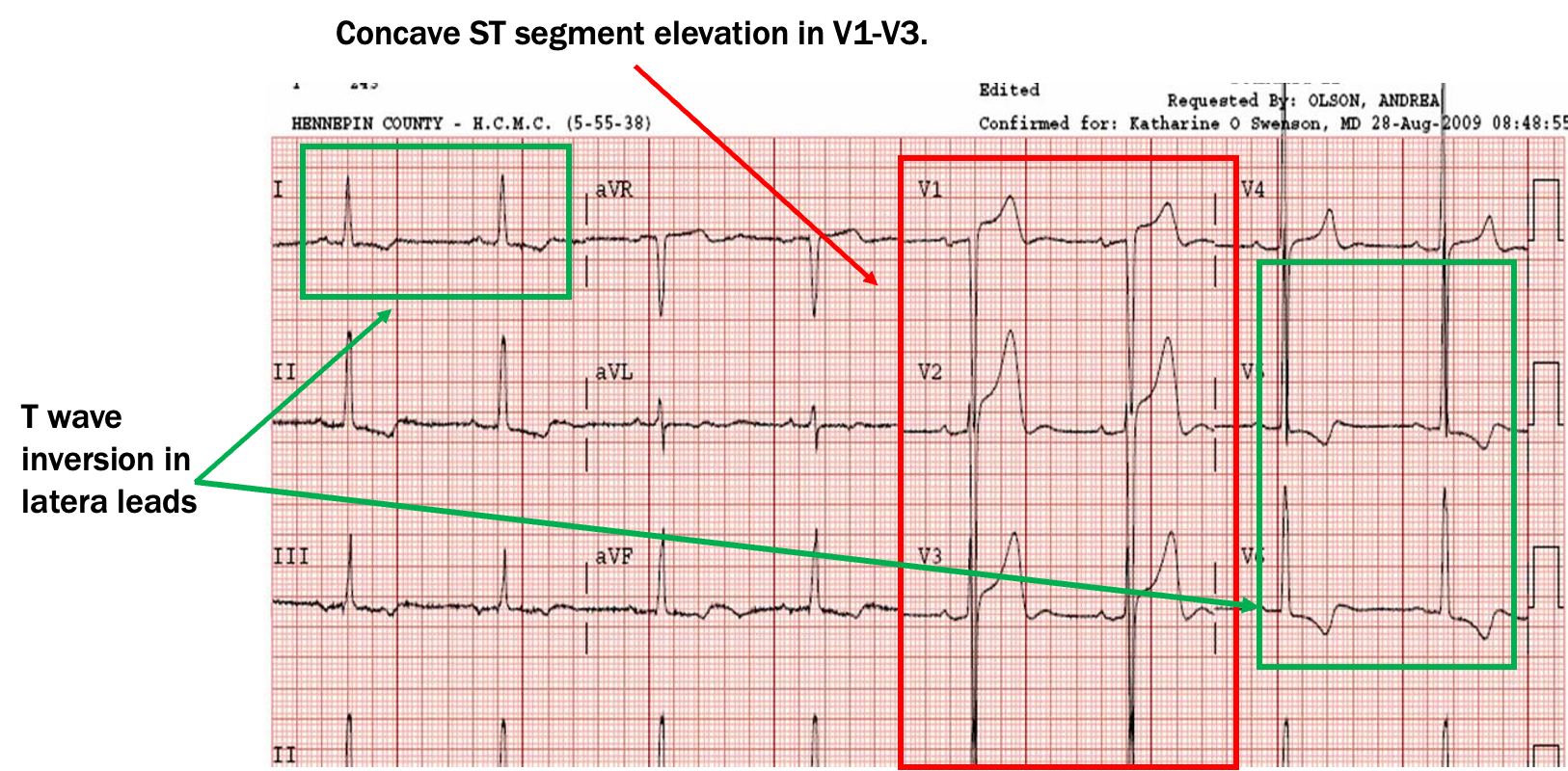
what are examples of STEMI mimics?
LVH, pericarditis, BER, brugada syndrome, LBBB, vent paced rhythm, hypothermia
what is MC STEMI mimic?
LVH (concave upward contour ST seg elevation in V1-V3, T wave inversion on lateral leads)
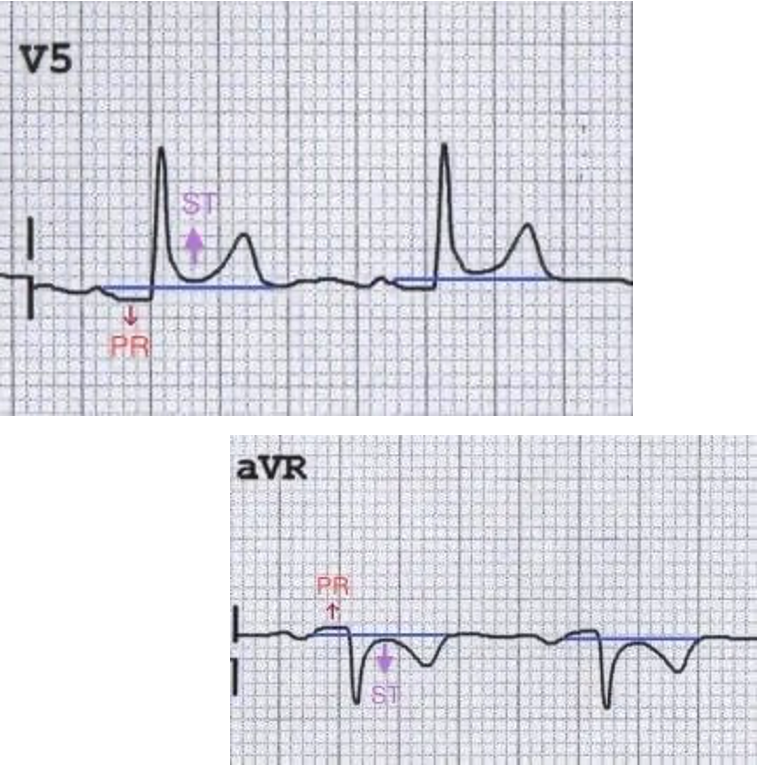
What are pericarditis ECG findings?
PR seg depression
global concave ST seg elevation
w/ no reciprocal ST depression anywhere (except aVR and V1)
PR seg elevation in aVR
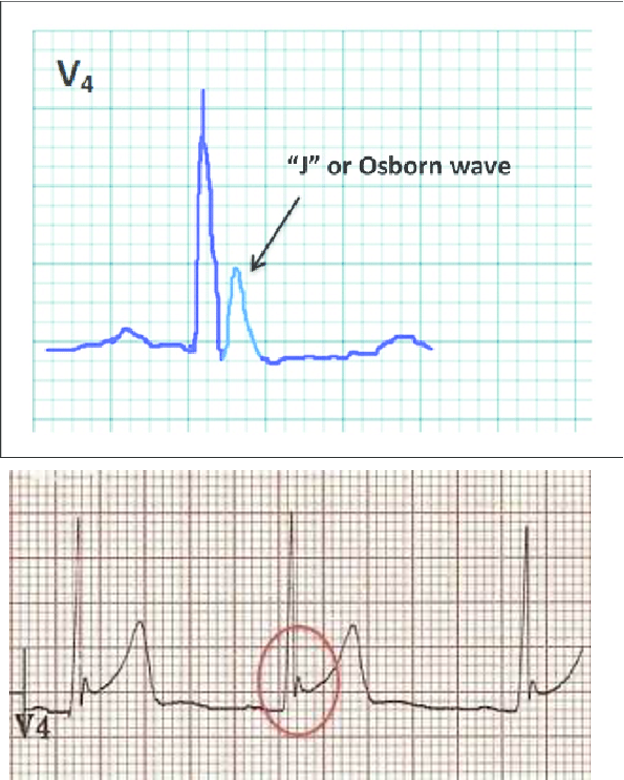
what is early depolarization (BER)?
normal variant ST segment elevation; mostly in young men
-global concave shaped ST seg elevation
-terminal QRS notching (J wave fishhook sign or Osborn wave)
-large T waves (sometimes symetrical)
-no reciprocal ST seg depression on ECG anywhere outside of aVR and V1
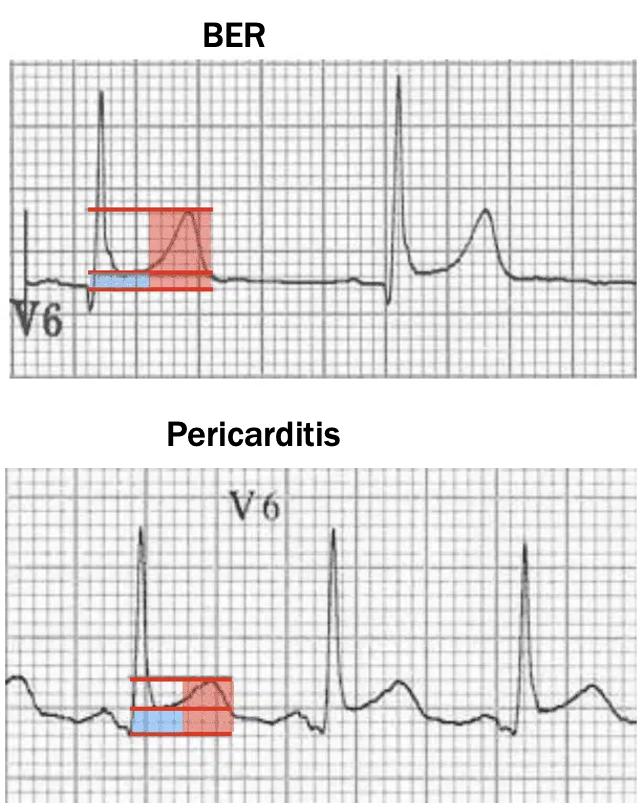
how do you differentiate b/t pericarditis and BER?
w/ lead V6
BER- more T wave than ST elevation;
pericarditis- more ST elevation than T wave
what is brugada syndrome?
inherited arrhythmogenic dz which affects sodium channels of RVOT
MC in young males o Southeast asian decent
what are the two main findings of brugada syndrome?
type 1- Coved shape: convex shaped ST elevation in V1-V3
type 2- carousel horses sign: saddle shape type ST elevation in V1-V3
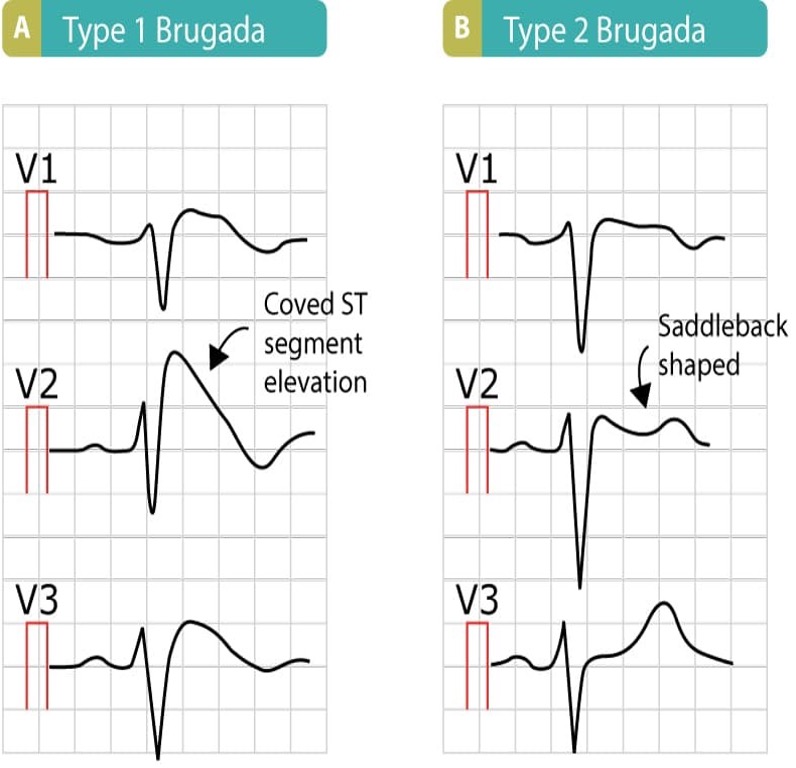
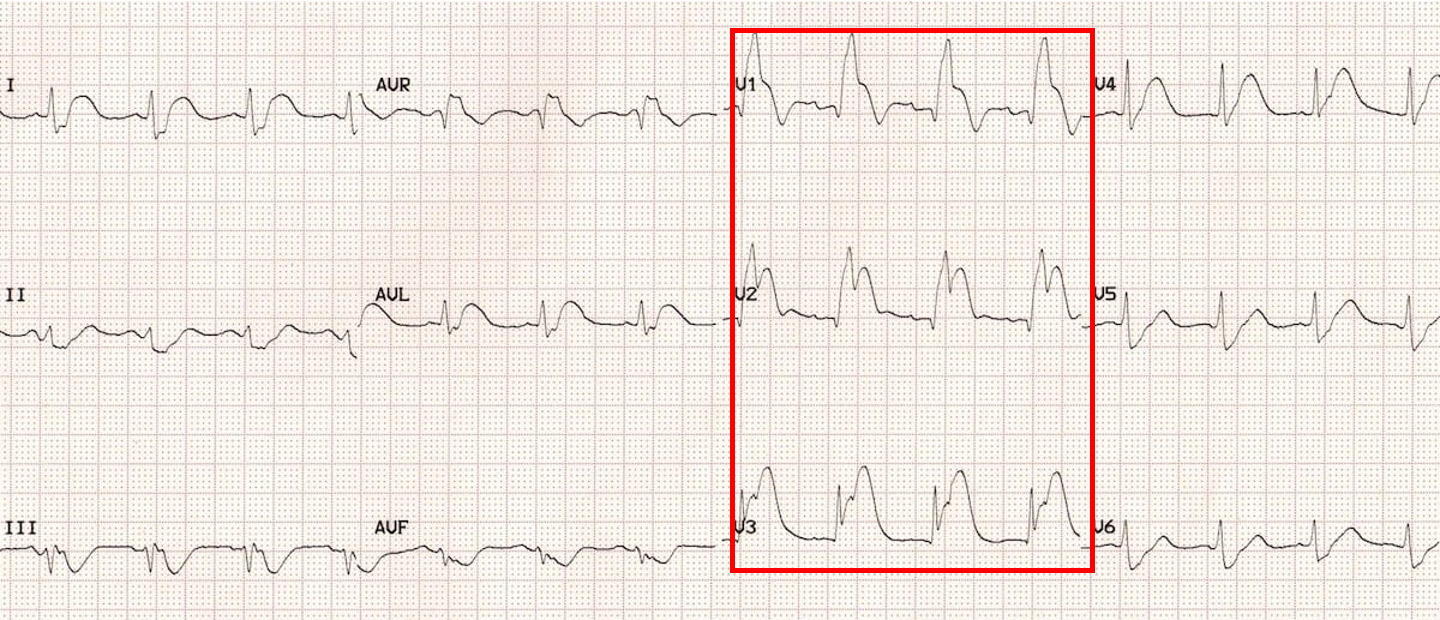
what is this?
brugada syndrome type 1
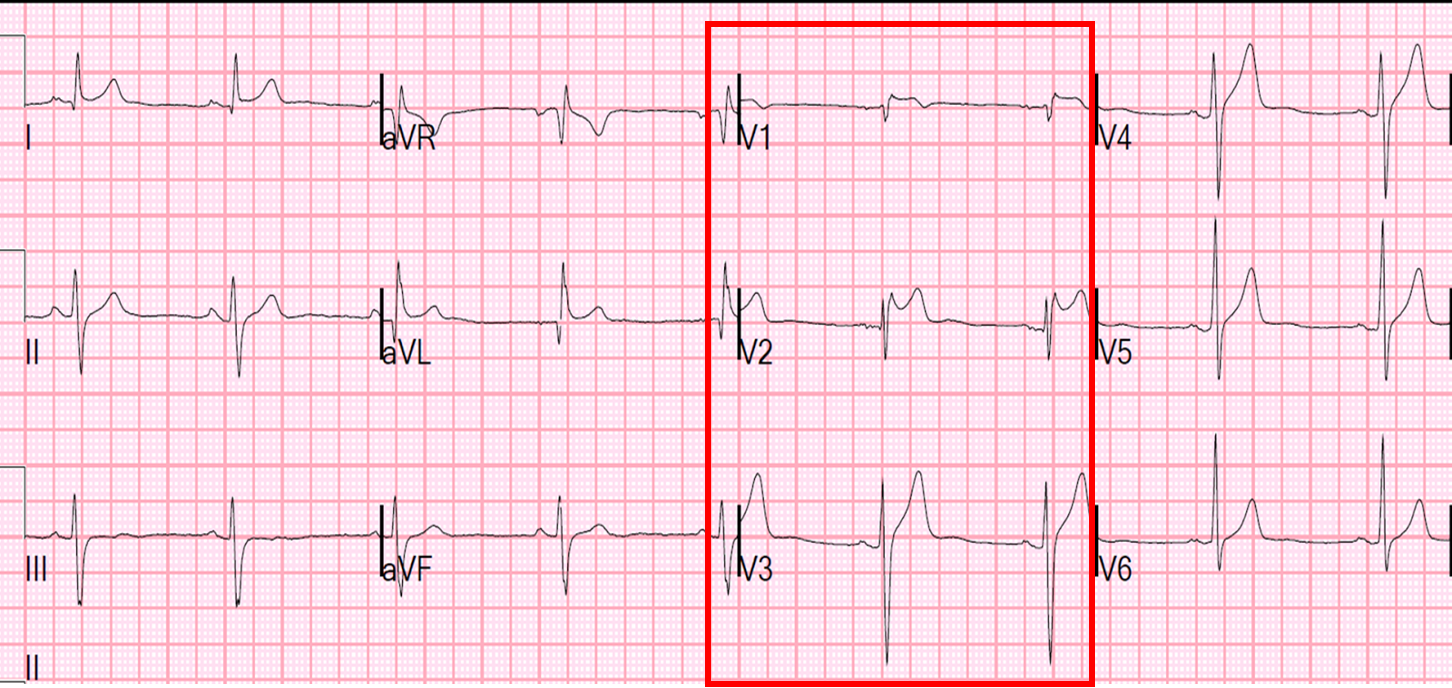
what is this?
brugada syndrome type 2
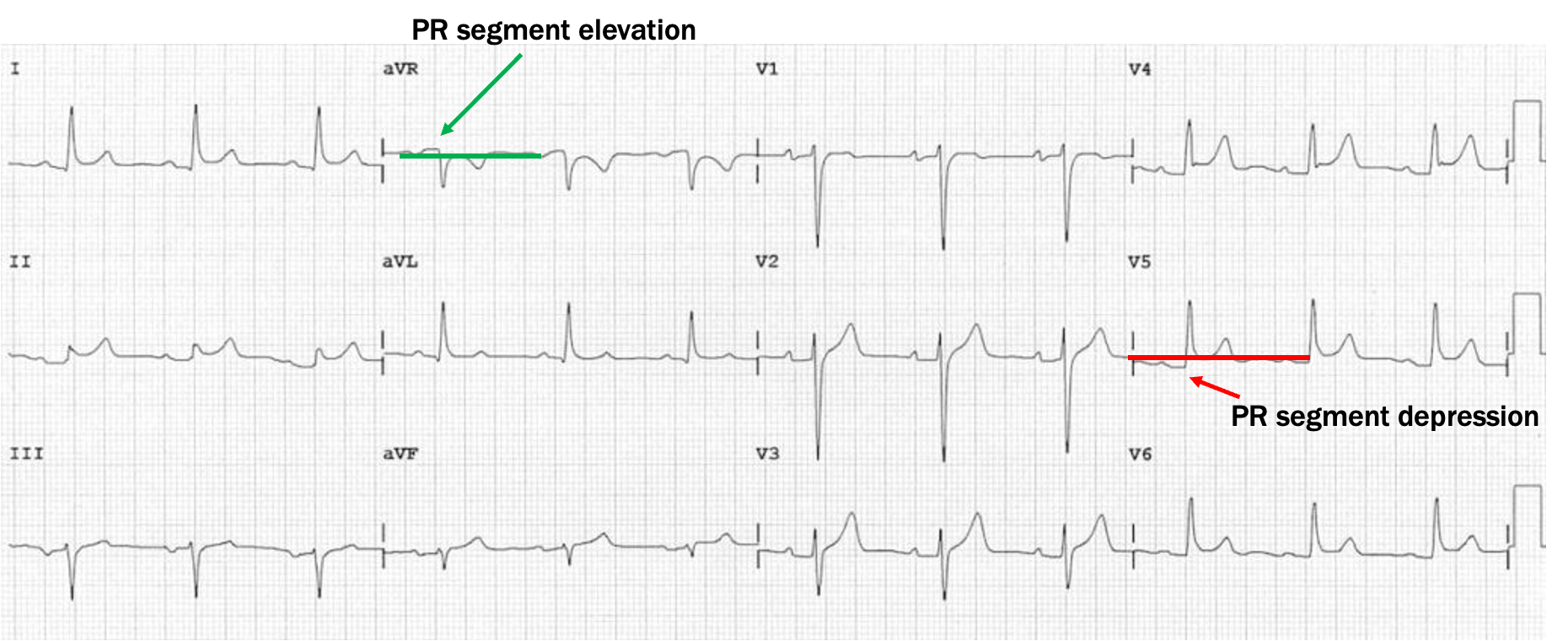
what is this?
pericarditis
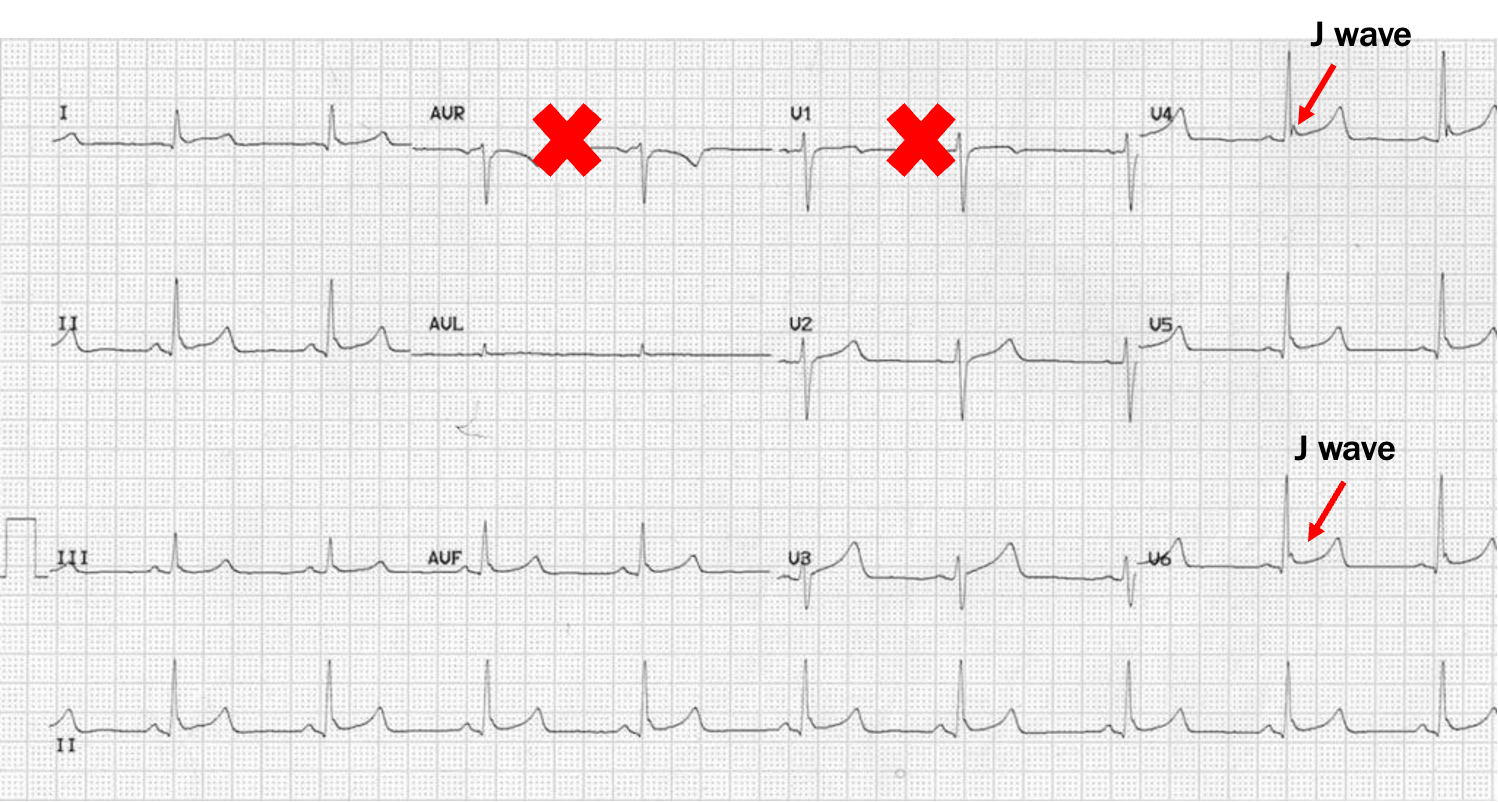
what is this?
BER
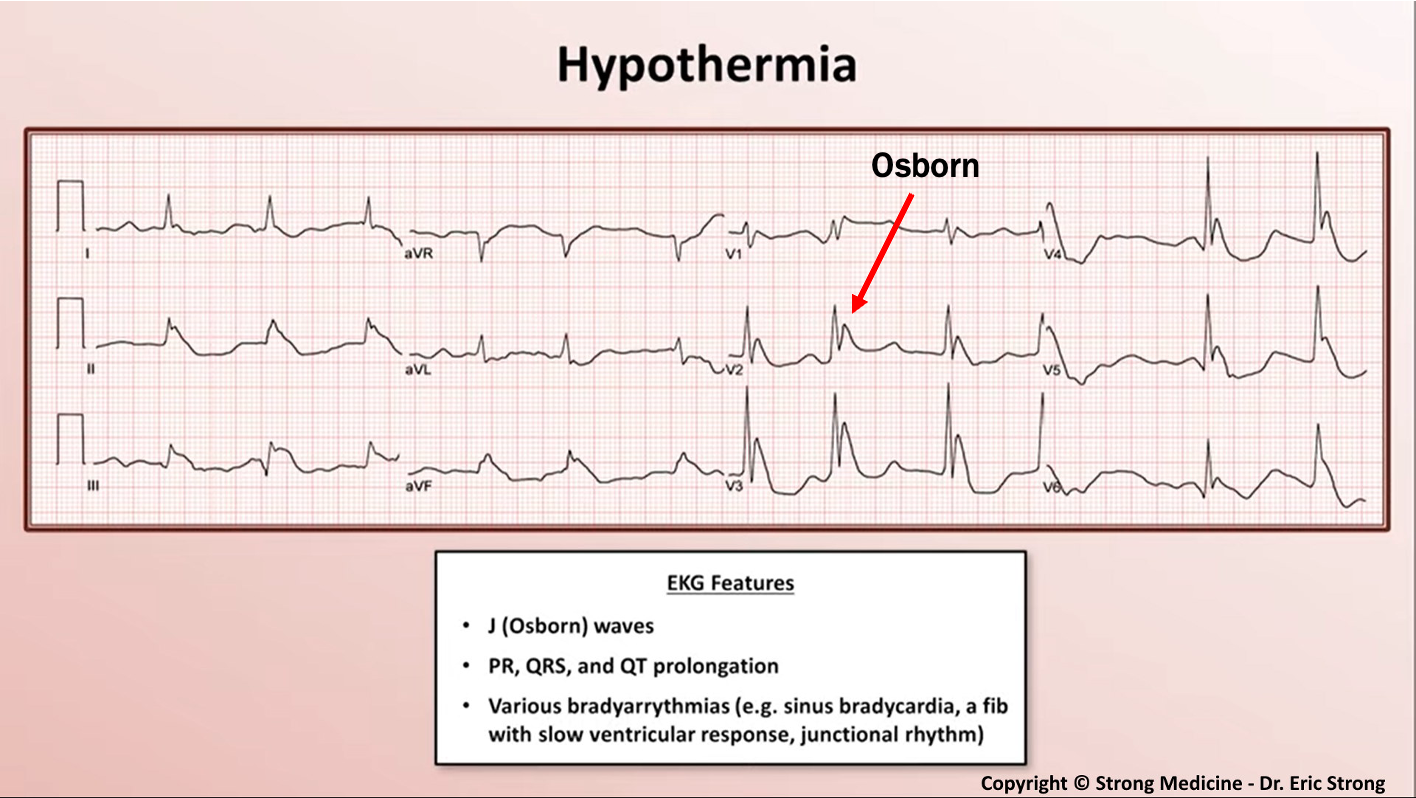
hypothermia ECG findings
35C- sinus bradycardia followed by prolongation of intervals; below 32C- Osborn waves commonly mistaken for STEMIs
(changes in ECG due to acidosis not temperature)
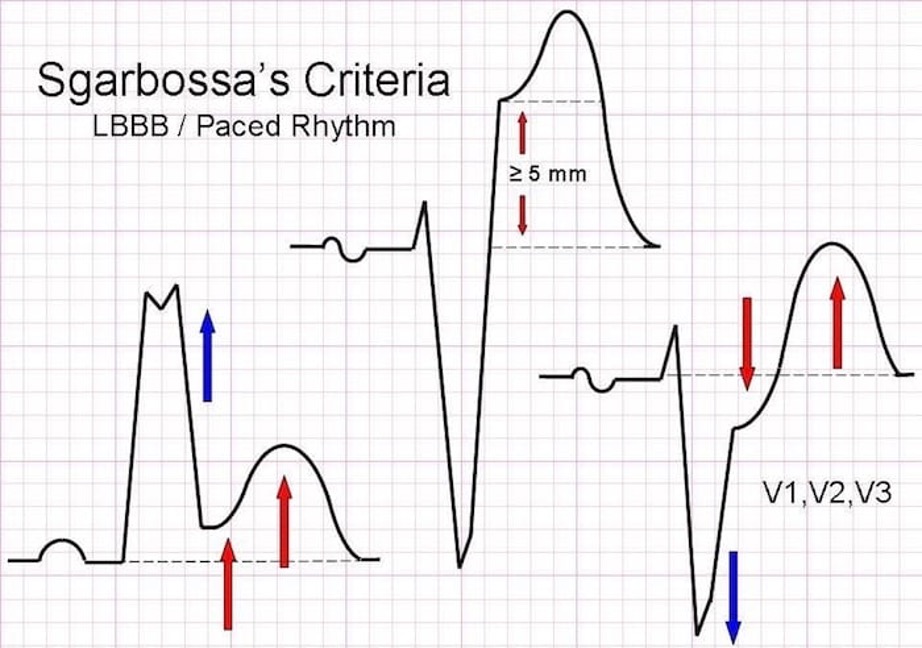
how do you dx acute MI in presence of LBBB or vent paced rhythm?
sgarbossa’s criteria
what is sgarbossa’s criteria?
concordant ST elevation of 1mm or more in any lead w/ pos QRS
concordant ST depression of 1mm or more in V1-V3
discordant ST elevation of 5mm or more in any lead w/ neg QRS
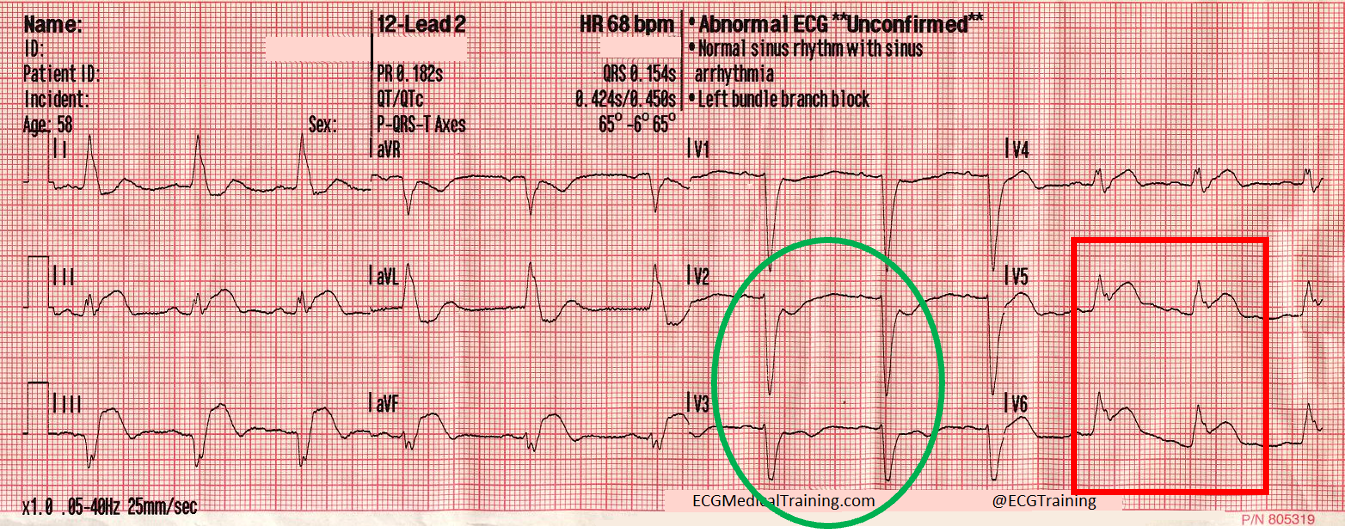
what does this ECG show?
sgarbossa’s criteria
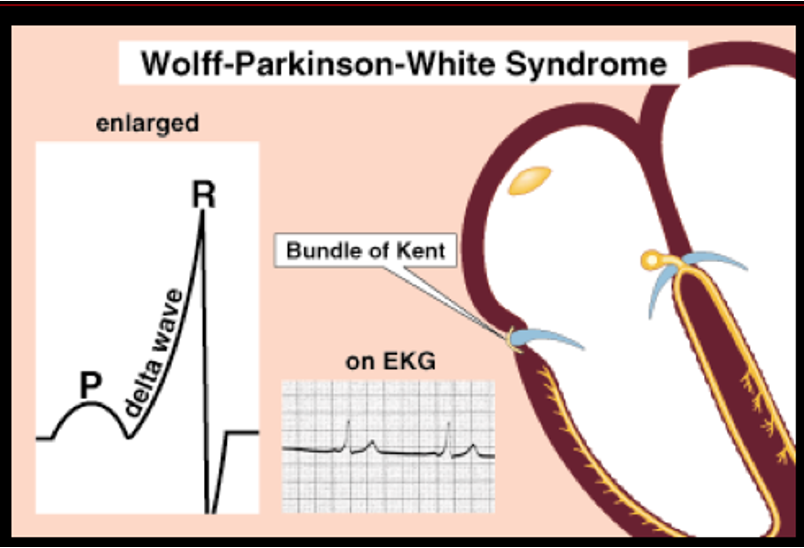
what is the WPW diagnostic triad?
short PR interval
wide QRS
delta wave
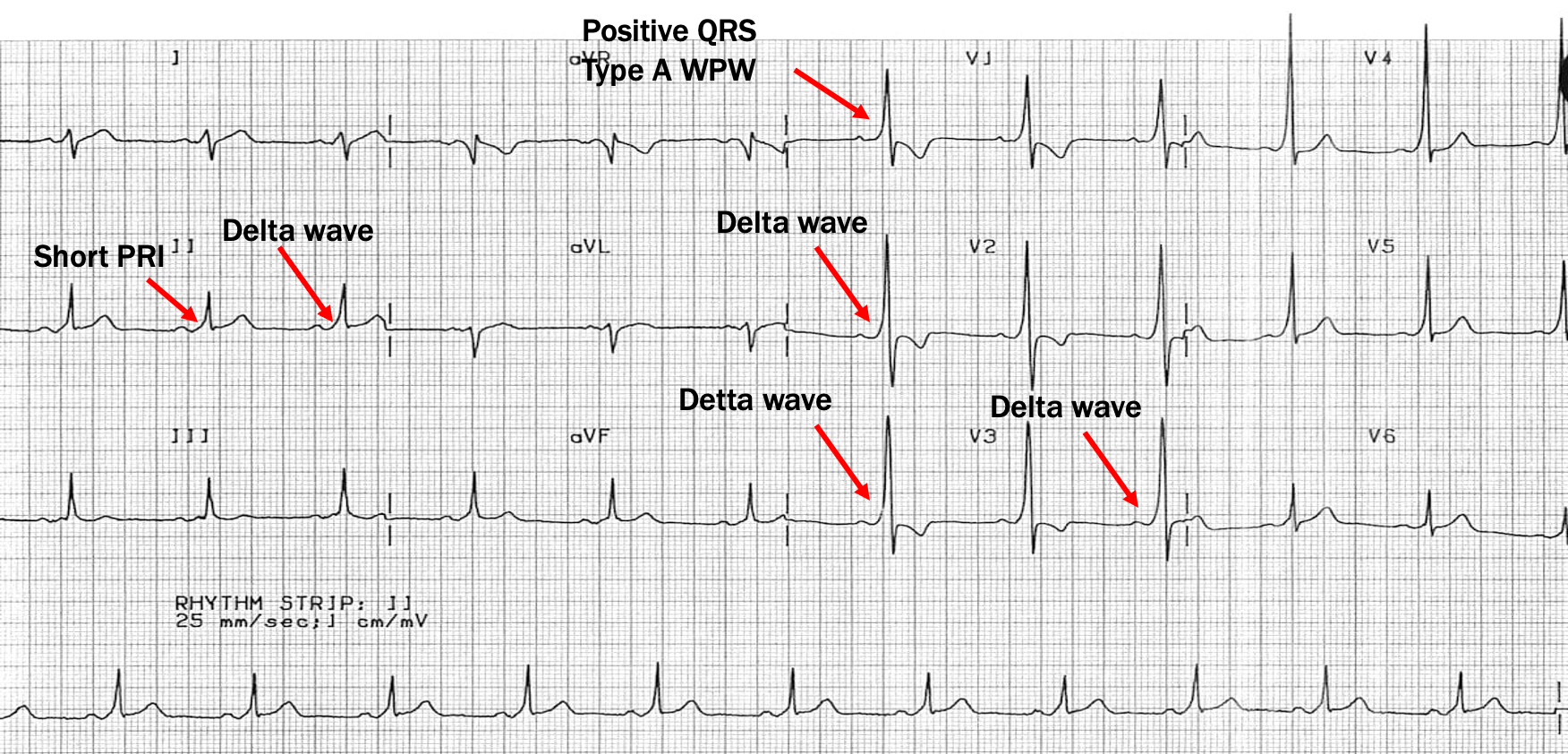
what is type A WPW?
left sided Kent bundle produces QRS complex that is mostly positive in V1
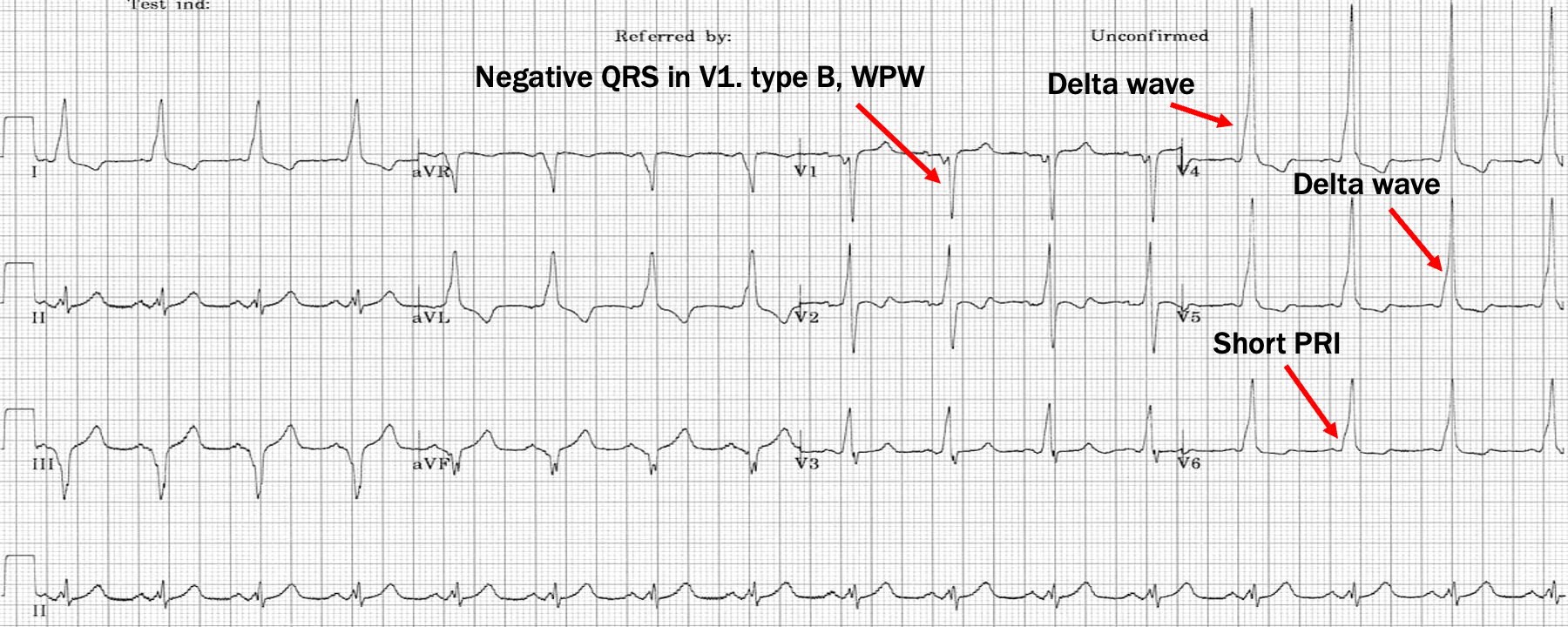
what is type B WPW?
Right sided Kent bundle produces QRS complex that is mostly neg in V1
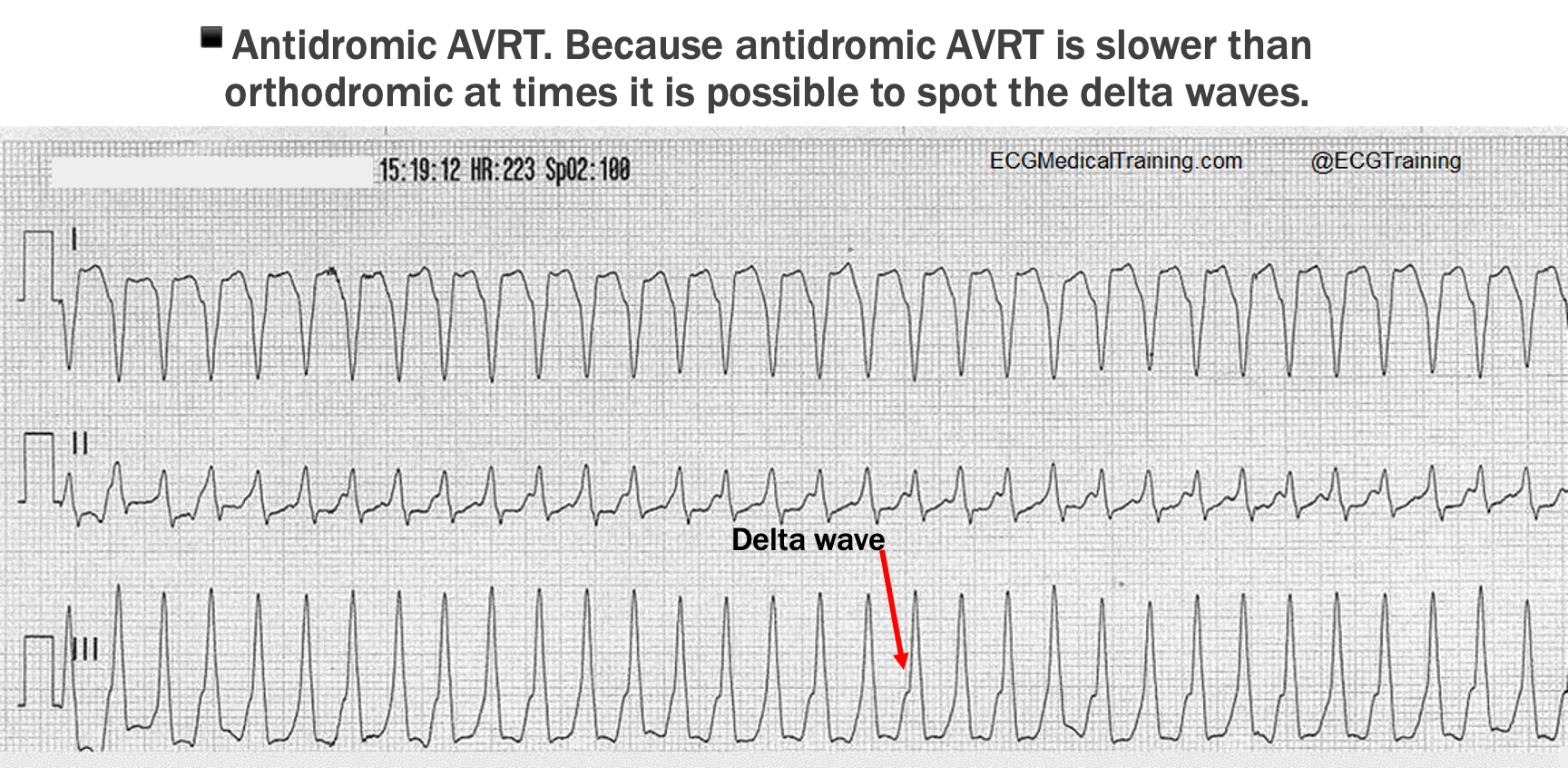
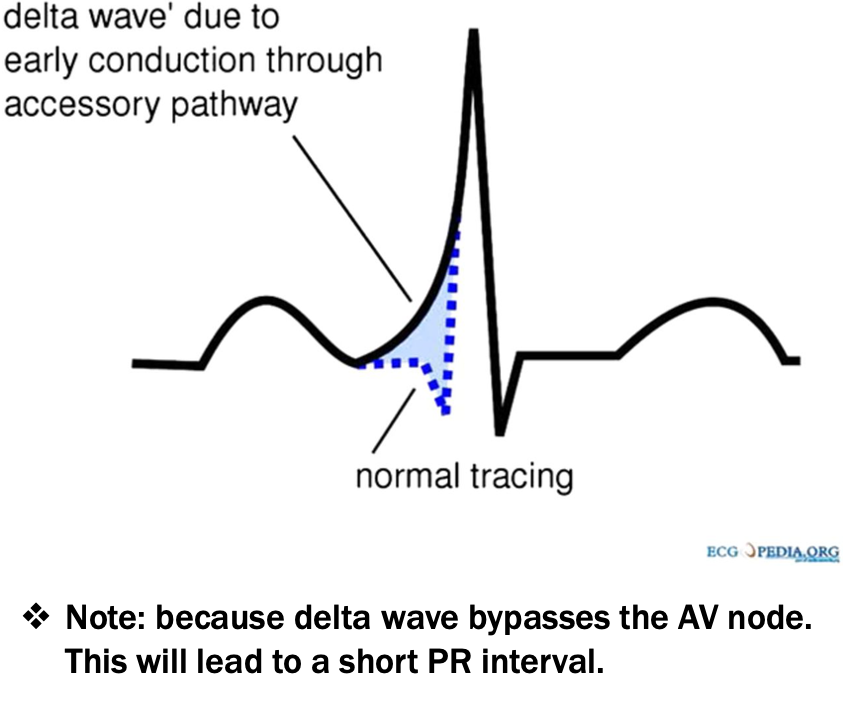
what is a delta wave?
slurring upstroke of QRS, diagnostic of WPW
what is orthodromic AVRT?
anterograde conduction (towards vents) occurs through normal pathway and up accessory pathway
produces regular narrow complex tachycardia
what is antidromic AVRT?
conduction occurs down accessory pathway and up normal pathway, retrograde (towards atria)
produces regular, monomorphic and wide tachycardia