Immunology Exam 3
1/201
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
202 Terms
What characteristics define mucosal tissue?
Mucus-secreting epithelium
Tight junctions
Directly exposed to external environment
Major site of pathogen entry
Produces secretory IgA (SIgA)
What are some examples of mucosal tissue?
GI tract
Respiratory tract
Urogenital tract
Mammary glands
Conjunctiva (eye)
What are mucins?
Large glycoproteins (rich in serine/threonine)
Form gel-like structure
What is mucus? What role does mucus play in immunity?
Secretion composed of mucins + enzymes + peptides
Produced by goblet cells
What are commensal microorganisms?
Normal microbiota living in symbiosis with host
Usually beneficial but can become pathogenic if barrier breaks
What role does mucus play in immunity?
Physical barrier trapping pathogens
Prevents microbial entry
Contains antimicrobial substances
What are gnotobiotic mice? How do they differ from mice that contain a regular microbiome?
Mice with known or no microbiota (often germ-free)
What are the anatomical effects? What are the immunological effects? (I don’t expect you to memorize these, but rather understand them and be able to recognize what impact the lack of microbiome might have)
Anatomical effects:
Underdeveloped gut structures (e.g., smaller Peyer’s patches)
Thinner mucosal layers
Immunological effects:
Poor immune system development
Reduced lymphoid tissue
Reduced IgA production
Impaired immune regulation
💡 Takeaway: microbiome is essential for immune development
What are five of the symbiotic benefits of the microbiome?
Prevent pathogen colonization (competition)
Aid digestion
Produce vitamins (e.g., vitamin K)
Stimulate immune system development
Maintain epithelial barrier integrity
What are examples of secondary lymphoid tissues at mucosal sites (GALT)?
Peyer’s patches
Appendix
Isolated lymphoid follicles
Tonsils/adenoids (related)
What is the inductive compartment?
Site of antigen sampling & lymphocyte activation
Located under epithelium
Involves:
Dendritic cells
M cells
What is the effector compartment?
Located in lamina propria
Contains:
Plasma cells
Effector T cells
Macrophages
What are the differences between systemic immunity and mucosal immunity?
Feature | Systemic | Mucosal |
|---|---|---|
Exposure to microbes | Rare | Constant |
Inflammation | Strong | Limited |
Strategy | Reactive | Proactive |
Key regulators | Less Treg | High Treg + IL-10 |
Mucosal immunity avoids inflammation to prevent damage
How does the innate immune response in the gut work? What role do intestinal epithelial cells play?
First line defense
Detect pathogens via PRRs
What is are the types of PRRs on intestinal epithelial cells?
TLRs (surface)
NLRs (cytoplasmic)
What are the three responses to PRR activation?
NLRP3 inflammasome → NFκB activation
Antimicrobial peptides (defensins)
Cytokines (IL-1, IL-6)
What is the role of NFκB?
Master transcription factor
Drives inflammatory gene expression
Why are innate immune response short-lived?
Epithelial cells replaced every ~2 days
What role/function do intestinal macrophages play?
Phagocytosis
Pathogen elimination
How are intestinal macrophages structurally and functionally different than conventional macrophages/blood monocytes?
❌ No cytokine secretion
❌ No respiratory burst
❌ No co-stimulation (not APCs)
“Inflammation-anergic”
What is the role of NFκB?
Inactivated → prevents inflammation
What is the role of TGFβ
Suppresses NFκB
Maintains anti-inflammatory state
What are the cell types of the intestinal epithelium? What are their functions?
Cell | Function |
|---|---|
Enterocytes | Absorption |
Goblet cells | Mucus |
Paneth cells | Antimicrobial peptides |
M cells | Antigen transport |
What is follicle-associated epithelium and how is it different than other areas of the intestinal epithelium?
Covers lymphoid follicles
Lacks goblet + Paneth cells
More vulnerable → allows antigen entry
What is the role of the microfold (m) cell? What are microfold (m) cells?
Specialized antigen-sampling cells
Perform transcytosis (transport antigen across epithelium)
What is transcytosis?
transport antigen across epithelium
What is the intraepithelial pocket?
Contains:
DCs
T cells
B cells
What is oral tolerance?
No immune response to food antigens
How does the experiment with ovalbumin demonstrate the role of oral tolerance?
Oral exposure → suppressed immune response
Injection → strong immune response
💡 Shows gut promotes tolerance, not immunity, to food
What is the role of CD103+ DCs? What types of T cells do they present to?
activate Tregs
Present to:
Tregs
TFH cells
When those T cells activate B cells, what antibody isotypes do they produce?
B cell activation → produces:
IgM → IgA
How do they function in the presence of infection? In the absence?
No infection: promote tolerance (via IL-10)
Infection: activate adaptive immunity
Where are mucosal lymphocytes activated?
Peyer’s patches
Mesenteric lymph nodes
Once they circulate, where do they go?
Return to mucosal tissues: homing
What are the molecules that allow them to home to the mucosal tissue? (specifically MAdCAM-1)
Key molecules:
CCR9
α4β7
MAdCAM-1
What is the distribution and nature of lymphocytes in the gut?
Always present (even without infection)
Types:
CD4⁺ (lamina propria)
CD8⁺ (epithelium)
αβ and γδ T cells
What are intraepithelial lymphocytes?
Specialized CD8⁺ T cells
Functions:
Kill infected cells
Promote repair
Maintain barrier
How do B cells in the gut work? What is the ‘first wave’? What is the ‘second wave’?
First wave:
IgM secretion
Second wave:
Class switch → IgA
What is the poly Ig receptor (pIgR)?
Transports IgA/IgM across epithelium
What is the secretory component?
Remains attached to IgA
Protects from degradation
Anchors to mucus
What is the role of IgA in maintaining tolerance?
Neutralizes pathogens
Prevents microbial entry
Does NOT activate complement → anti-inflammatory
💡 Maintains tolerance while providing protection
What are the differences between IgA1 and IgA2?
Feature | IgA1 | IgA2 |
|---|---|---|
Hinge | Long | Short |
Flexibility | High | Lower |
Protease resistance | Low | High |
IgA2 dominant in colon (more bacteria)
What are the potential causes of and problems caused by selective IgA deficiency?
Causes:
Failure to class switch from IgM
Effects:
Often mild (compensation by other antibodies)
Problems:
Chronic lung infections
Giardia infections
Additional:
Maternal IgA (breastfeeding) provides protection
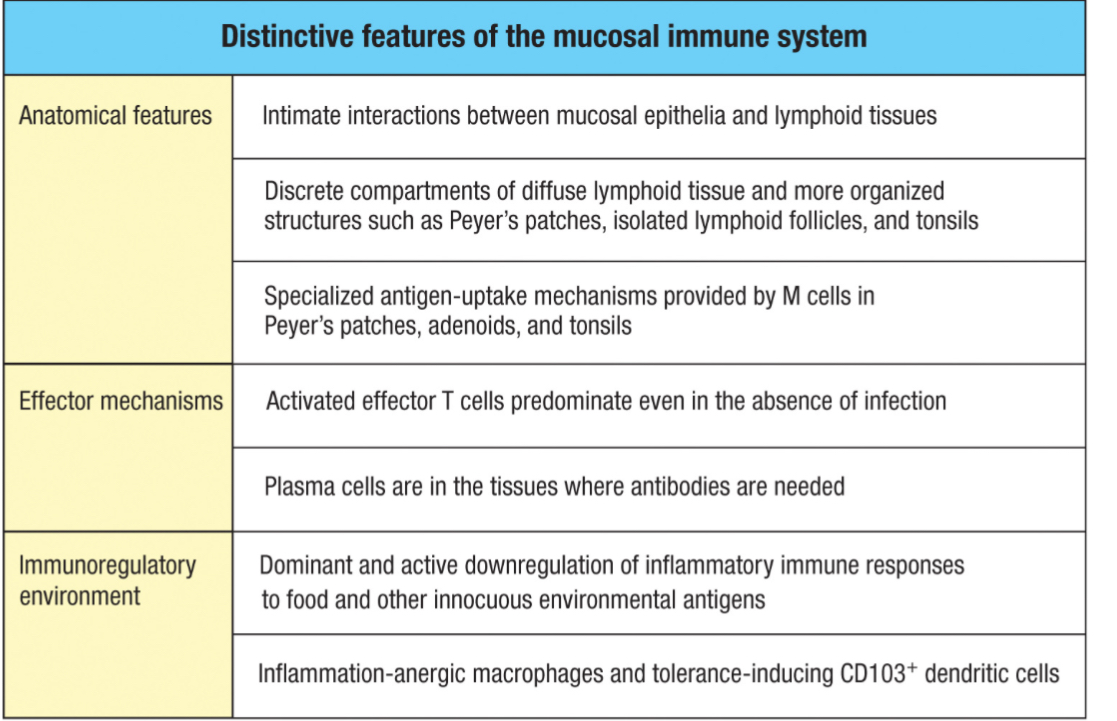
Know the table titled ‘Distinctive features of the mucosal immune system
Constant exposure to microbes
Strong tolerance mechanisms (Tregs, IL-10)
Minimal inflammation
Dominance of IgA
Continuous presence of effector cells
Specialized antigen sampling (M cells, DCs)
Shared immunity across mucosal sites
primary immune response
Driven by naïve B and T cells
Requires:
Antigen presentation
Co-stimulation
Chromatin = closed
Few transcription factors present
Higher activation threshold
What are the important cells of immunological memory?
Long-lived plasma cells (LLPCs) → maintain antibodies
Memory B cells → rapid antibody production
Memory T cells → rapid cellular response
What are the important distinctions between long-lived plasma cells and memory B cells?
Feature | LLPCs | Memory B Cells |
|---|---|---|
Location | Bone marrow | Circulate |
Division | Do NOT divide | Can proliferate |
BCR | ❌ None | ✅ Present |
Function | Constant antibody secretion | Rapid response upon re-exposure |
Antibody | Already secreting | Activated upon re-exposure |
What role does FcγR2B(1) in the regulation of B cells and B cell memory?
Expressed on naïve B cells
Binds IgG → inhibits activation
Key idea:
Prevents unnecessary activation of naïve B cells
Memory B cells & plasma cells DO NOT express it
→ allows rapid secondary response
What is hemolytic disease of newborn? (Erythroblastosis Fetalis)
Destruction of fetal RBCs by maternal antibodies
Secondary immune response
Driven by memory B and T cells
Faster activation
No co-stimulation required
Chromatin = open (epigenetically primed)
Transcription factors already present
Lower activation threshold
difference between primary vs secondary immune responses
Primary Response:
Long lag time (slow activation)
Lower magnitude
Shorter duration
Antibodies: IgM → IgG
Occurs upon first exposure
Secondary Response:
Short lag time (rapid response)
Much greater magnitude
Longer-lasting
Dominated by high-affinity IgG (or IgA/IgE)
Occurs upon repeat exposure
How does hemolytic disease happen?
Rh⁻ mother exposed to Rh⁺ fetus (first pregnancy)
Primary response → IgM (does NOT cross placenta)
Second pregnancy:
Memory response → IgG produced
IgG crosses placenta → destroys fetal RBCs
What is Rhogam? How does it prevent Erytrhoblastosis Fetalis?
Injection of anti-RhD IgG antibodies
Mechanism:
Binds fetal Rh⁺ RBCs in mother
Prevents maternal immune system from recognizing antigen
Prevents memory formation
What is the role of CD45 (including CD45RA and CD45RO) in distinguishing between naïve and memory T cells? In this case, how does structure help determine function?
CD45:
Required for T cell activation
CD45RA (Naïve T cells):
Larger molecule
Harder interaction with TCR
Higher activation threshold
CD45RO (Memory T cells):
Smaller (alternative splicing)
Easier TCR interaction
Lower activation threshold
Structure → Function:
Smaller CD45RO → closer TCR interaction → faster activation
What are the three types of memory T cells? How do their migration patterns differ from one another?
1. Central Memory (TCM)
Circulate in:
Blood
Lymph nodes
Function: long-term surveillance
2. Effector Memory (TEM)
Circulate in:
Blood + peripheral tissues
Function: rapid response
3. Resident Memory (TRM)
Stay in tissues
Function: immediate local protection
What are the various models of memory cell differentiation (generally, not specifically)? Which is most likely to be correct?
General models:
Linear differentiation (naïve → effector → memory)
Parallel differentiation
Asymmetric division (MOST accepted)
Asymmetric division:
Unequal distribution of mTORC1
Results:
Proximal → effector cell
Distal → memory cell
What is antigenic original sin? Why does it occur? How does it impact the primary immune response to various pathogens?
Immune system prefers existing memory response over new response
Why it occurs:
Memory cells activate faster than naïve cells
Impact:
Can lead to less effective response to new pathogens/variants
Why is the flu a good example of original antigenic sin? (high mutation rate)
High mutation rate
Old antibodies may not match new strains
What is the importance of cross-reactivity and cross-protection?
Cross-reactivity:
One immune response recognizes similar antigens
Cross-protection:
Immunity to one pathogen protects against another
Importance:
Basis of vaccines
Provides broader immunity
Can be beneficial OR sometimes misleading (wrong target)
What is the key difference between active and passive immunization?
Active immunity = your body makes the response → memory formed
Passive immunity = receive pre-made antibodies → no memory
active vs. passive; natural vs. acquired?
Type | Natural | Artificial |
|---|---|---|
Active | Infection | Vaccine |
Passive | Maternal antibodies | Antibody transfer (e.g., antiserum) |
Why might it be advantageous to use passive immunization?
Immediate protection
Useful for:
Venom/toxins
Immunodeficient patients
Why might it be disadvantageous to use passive immunization?
Temporary
No memory
Possible immune reactions
What is the nomenclature used in vaccine (e.g. horse α-snake, etc.)
Example: horse α-snake antibodies
Source (horse) + target (snake toxin)
What are vaccines?
Preparations containing:
Weakened/killed pathogen OR
Pathogen components
Stimulate immune system → memory without disease
Immunization vs vaccination
Immunization = protection achieved
Vaccination = exposure event
What is the difference between vaccination and variolation?
Variolation:
Use of live smallpox → risky
Vaccination:
Use of cowpox → safer (cross-protection)
What are the reasons that smallpox is the only disease to be eradicated?
Low mutation rate
Strong, effective vaccine
Human-only reservoir
What are the three major goals of vaccination?
Safety
Efficacy (immunogenicity)
Sustainability (cost, accessibility)
In general, what are correlates of immune protection?
High IgG levels (systemic)
High IgA levels (mucosal)
What is meant by rational vaccine design?
Use pathogen structure/genetics to design vaccines
What is meant by reverse vaccinology?
Use knowledge of pathogen biology to identify targets
What characteristics give a vaccine the strongest response?
Targets immunodominant epitopes
Activates both B and T cells
Live attenuated
Weakened live pathogen
Advantages:
Strong immune response
Few boosters
Disadvantages:
Risk of reversion
Not safe for immunocompromised
Requires refrigeration
Inactivated or killed
Dead pathogen
Advantages:
Safe
Stable
Disadvantages:
Weaker response
Requires boosters
Poor T cell response
Toxoid
Inactivated toxin
Example:
Tetanus
Advantage:
Neutralizes toxin
Disadvantage:
Only works for toxin-mediated disease
Purified Protein/Peptide Subunit; Purified Carbohydrate Subunit
Protein:
Purified proteins
Carbohydrate:
Polysaccharides
Advantages:
Safe
Targeted
Disadvantages:
Weak immune response
Carbs → no T cell help (need conjugation)
Recombinant Vectors
Virus delivers antigen genes
Advantages:
Strong response
Mimics infection
Disadvantages:
Immune response to vector
Stability issues
mRNA
mRNA → host makes antigen
Advantages:
Fast to produce
Strong immune response
What is the polio virus? What is the disease it causes?
Causes poliomyelitis (paralysis)
What are the two types of polio vaccines? What are the similarities between the two? What are the differences?
Feature | Salk | Sabin |
|---|---|---|
Type | Killed | Live attenuated |
Route | Injection | Oral |
Risk | Safer | Risk of reversion |
What are the types of vaccine excipients? What are their purposes?
Preservatives → prevent contamination
Adjuvants → boost immune response
Stabilizers → storage stability
Antibiotics → prevent bacterial growth
Inactivating agents → kill pathogens
What is an adjuvant?
Enhance immune response
Functions:
Increase inflammation
Improve antigen presentation
Stabilize antigen
What are liposomes? What are ISCOMs?
Delivery systems
Help antigens enter cells → activate CTL response
What is a vaccine schedule? What is a booster?
Schedule = timing of doses
Booster = additional dose to strengthen immunity
What is the NVICP? Why was it established? How does it work?
Compensation system for vaccine injury
Why:
Created after vaccine safety concerns
How:
No-fault system
Requires “preponderance of evidence”
Panel includes medical, legal, and lay experts
What is VAERS? How does it work?
Reporting system for adverse events
Monitors vaccine safety
What are the consequences of non-vaccination?
Disease outbreaks
Loss of herd immunity
Increased mortality
What are therapeutic vaccines? What are some examples?
Treat disease (not prevent)
Examples:
Cancer vaccines
Can you distinguish between the terms coronavirus, SARS-CoV-2, and COVID19?
Coronavirus = virus family
SARS-CoV-2 = specific virus
COVID-19 = disease
What is the spike (S) protein
Viral surface protein
Binds to ACE2 receptor
How does coronavirus infect us?
Inhalation of droplets
Spike protein binds ACE2
Virus enters cell
Replicates
Spreads → inflammation
What is the ACE2?
Host receptor on respiratory cells
Entry point for virus
What is herd immunity? How is it defined? How is it determined?
When enough people are immune → spread decreases
Determined by:
R₀ (infectivity)
Regarding infectious disease, what is the relationship between infectivity and mortality (in general)? What is the relationship between infectivity and mode of transmission (in general)?
Higher infectivity → usually lower mortality
Higher mortality → usually lower spread
Mode of transmission:
Airborne → higher spread
Contact → lower spread
How do mRNA vaccines work?
mRNA enters host cells
Cells produce antigen (spike protein)
Immune system responds
Memory formed
what is hypersensitivity?
An exaggerated or inappropriate immune response
Causes more damage than the antigen/pathogen itself
Typically occurs during secondary immune responses
Which characteristics make parasites different than other parasites?
Multicellular
Too large for phagocytosis
Biologically similar to host → harder to target
In general, what is the body’s strategy to eliminate a parasite?
Physical expulsion:
Coughing, sneezing, vomiting, diarrhea
Barrier defenses:
Increased mucus
“Explosive” immune responses to dislodge parasites
What are the characteristics of ‘type 2’ immunity?
Driven by TH2 cells
Cytokines:
IL-4 → IgE production
IL-5 → eosinophils
IL-13 → mucus production
Key cells:
Mast cells
Basophils
Eosinophils
Dominant antibody: IgE