RW Type 2 Diabetes
1/162
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
163 Terms
What is the incretin effect?
When food is ingested incretin hormones are released
Inc. insulin secretion
Dec. glucagon secretion
What is the Sodium-Dependent Glucose Transporter-2 (SGLT2)?
Reabsorbs glucose from the in kidney
What are the main differences in presentation of T2DM (vs. T1)?
Older age
Gradual onset
Positive family history
Obese or history of obesity
Metabolic syndrome common
Often asymptomatic
No ketones at diagnosis
Microvascular & macrovascular complications common
No autoantibodies
What are non-drug therapies for T2DM?
Diet - portion control, limit sugar and carbs
Weight loss
Physical activity
When is bariatric surgery recommended?
Any patient with BMI > 40 kg/m2
BMI between 35-40 kg/m2 with poor glucose control
When is weight management drug therapy indicated?
Drug therapy if BMI >30 kg/m2
OR< BMI >27 kg/m2 with one or more obesity related complication
What are drugs used for weight management?
Orlistat
Lorcaserin
Phentermine/topiramate
Naltrexone/bupropion
Liraglutide/Semaglutide/Tirzepatide
What is a normal fasting plasma glucose?
<100 mg/dL
What is a impaired (prediabetes) fasting plasma glucose?
100-125 mg/dL
What is a fasting plasma glucose in diabetes?
≥126 mg/dL
What is a normal 2hr postload plasma glucose?
<140 mg/dL
What is an impaired (prediabetes) 2hr postload plasma glucose?
140-199 mg/dL
What is a 2hr postload plasma glucose in diabetes?
≥200 mg/dL
What are diagnostic criteria for diabetes?
A1c ≥6.5%
FPG ≥126
2hr PPG ≥200
Random ≥200 w/symptoms of hyperglycemia
(Same for all types)
What is the A1c goal for diabetes?
≤7%
How often should A1c be monitored in diabetes patients?
Every 3 months if not at goal
Every 6 months if at goal
What is the FPG goal for diabetes?
80-130 mg/dl
What is the PPG goal for diabetes?
<180 mg/dl
How often should a diabetes patient test their BG?
Once per day if on oral agents or basal insulin
3-4 x/day if multiple daily insulin injections
What is the oral first drug of choice, in T2DM patients without CVD/HF/CKD?
Metformin
Why is metformin the 1st line agent in diabetes?
Effective (high A1c dec.)
Safe (no hypoglycemia)
Inexpensive
Widely available
What is the agent of choice in a patient whose goal is weight loss?
GLP-1s
What is the agent of choice in a patient with ASCVD or indicators of high CVD risk?
SGLT-2
In a patient with ASCVD/high risk, who is already on an SGLT-2, what can be added if additional therapy is needed?
GLP-1
Or pioglitazone (not as good as GLP-1)
What is the agent of choice in a patient with HF?
SGLT-2
What is the agent of choice in a patient with CKD?
SGLT-2
In a patient with CKD, who is already on an SGLT-2, what can be added if additional therapy is needed?
GLP-1
If a patient, who is newly diagnosed with T2DM, has an A1c of <8.5% what therapy is indicated?
Metformin
If a patient, who is newly diagnosed with T2DM, has an A1c of ≥8.5% what therapy is indicated?
Dual therapy
In pt.'s who's A1c is >1.5% above goal
In patients with A1c's >1.5% above goal (7%), what is indicated?
Dual therapy
If a patient, who is newly diagnosed with T2DM, has an A1c of >10% what therapy is indicated?
Early introduction of insulin
If a patient, who is newly diagnosed with T2DM, has BG levels >300 mg/dL what therapy is indicated?
Early introduction of insulin
When should insulin be introduced early (in newly diagnosed patients)?
Early introduction of insulin should be considered if there is evidence of:
ongoing catabolism (weight loss),
if symptoms of hyperglycemia are present,
When A1C levels (>10%) or blood glucose levels (>300 mg/dL) are very high
When injectable therapy is indicated, what is the best initial therapy for MOST patients?
GLP-1 or GIP/GLP-1
Used prior to insulin in most pt.'s
When should insulin be used as the first injectable therapy?
Symptoms of hyperglycemia are present
When A1c or blood glucose levels are very high (A1c >10% or BG ≥300 mg/dL)
When a diagnosis of Type 1 diabetes is a possibility
What type of insulin should be initiated first?
Basal insulin
Any basal insulin is appropriate for initial therapy
What is the initial dose of basal insulin?
10 units per day
OR 0.1-0.2 mg/kg per day
How should basal insulin be titrated?
2-4 units every 3-4 days
Until fasting blood sugars at goal
What is basal insulin titrated to?
Fasting blood glucose goal
How should a patient self-titrate if their blood sugar is >180 mg/dL?
Increase by 4 units
How should a patient self-titrate if their blood sugar is 130-180 mg/dL?
Increase by 2 units
How should a patient self-titrate if their blood sugar is 70-130 mg/dL?
Continue same dose
How should a patient self-titrate if their blood sugar is <70 mg/dL or they are experiencing hypoglycemia symptoms?
Decrease by 2 units
If a patient on basal insulin needs additional therapy, what is preffered?
GLP-1 or Tirzepatide (GLP-1/GIP)
Preferred over adding mealtime bolus insulin or switching to pre-mixed formulation
What combination injectable therapy is generally recommended?
Add GLP-1
OR, GLP-1/GIP
Why are GLP-1s and GLP-1/GIPs recommended for combination injectable therapy?
CV benefit
Weight loss
How should bolus insulin be added?
Add bolus at largest meal
Equivalent to using 3x/day
What is the difference between bolus dosing at largest meal and 3x/day dosing?
Equivalent effect on A1c
Multiple dialy injections improve A1c more rapidly
What are advantages of bolus insulin?
Easy to titrate (increase by 1-2 units every 3-4 days)
Well-tolerated
What are disadvantages of bolus insulin?
Hypoglycemia
Weight gain
Increased cost
Increased injections
Less convenient - timing with meals
What are advantages of GLP-1 Agonists?
Low risk of hypoglycemia
Weight loss or neutral
CV benefit
More convenient - once weekly or combination products
Can be administered regardless of meals
What are disadvantages of GLP-1 Agonists?
Increased cost
Tolerability
What are advantages of Basal insulin/GLP-1 combinations?
Decreased injection burden - one shot daily
Decreased cost - one copay
What are disadvantages of Basal insulin/GLP-1 combinations?
Need to titrate dose
Maximum dose of basal insulin due to GLP-1
What are pre-mixed combination insulins?
Fixed combinations of basal and bolus insulin
What is the initial dose of pre-mixed combination insulins based on?
Initial dose based on insulin dose
Divide 1/2 am and PM
OR, 2/3 am and 1/3 pm
What are advantages of pre-mixed combination insulin?
Less expensive - one copay or available OTC
Both basal and bolus insulin in one injection (2 injections vs. 4 for basal/bolus)
Less chance for dosing errors
What are disadvantages of pre-mixed combination insulin?
Has to be given with meals due to bolus insulin
Unable to titrate one insulin without adjusting the other
What is the initial dose of bolus insulin?
4 units per day
OR, 10% of basal dose
How should bolus insulin be titrated?
Increase by 1-2 units every 3-4 days
How should bolus insulin be adjusted if pre-lunch sugar is elevated?
Increase breakfast bolus insulin
How should bolus insulin be adjusted if pre-dinner sugar is elevated?
Increase lunch bolus insulin
How should bolus insulin be adjusted if pre-bedtime sugar is elevated?
Increase dinner bolus insulin
When looking at a patient's BG data, what issues should be addressed first?
Address hypoglycemia (by lowering most recent dose) first
Then can begin addressing highs
What are the relative potencies of diabetes drugs as monotherapies?
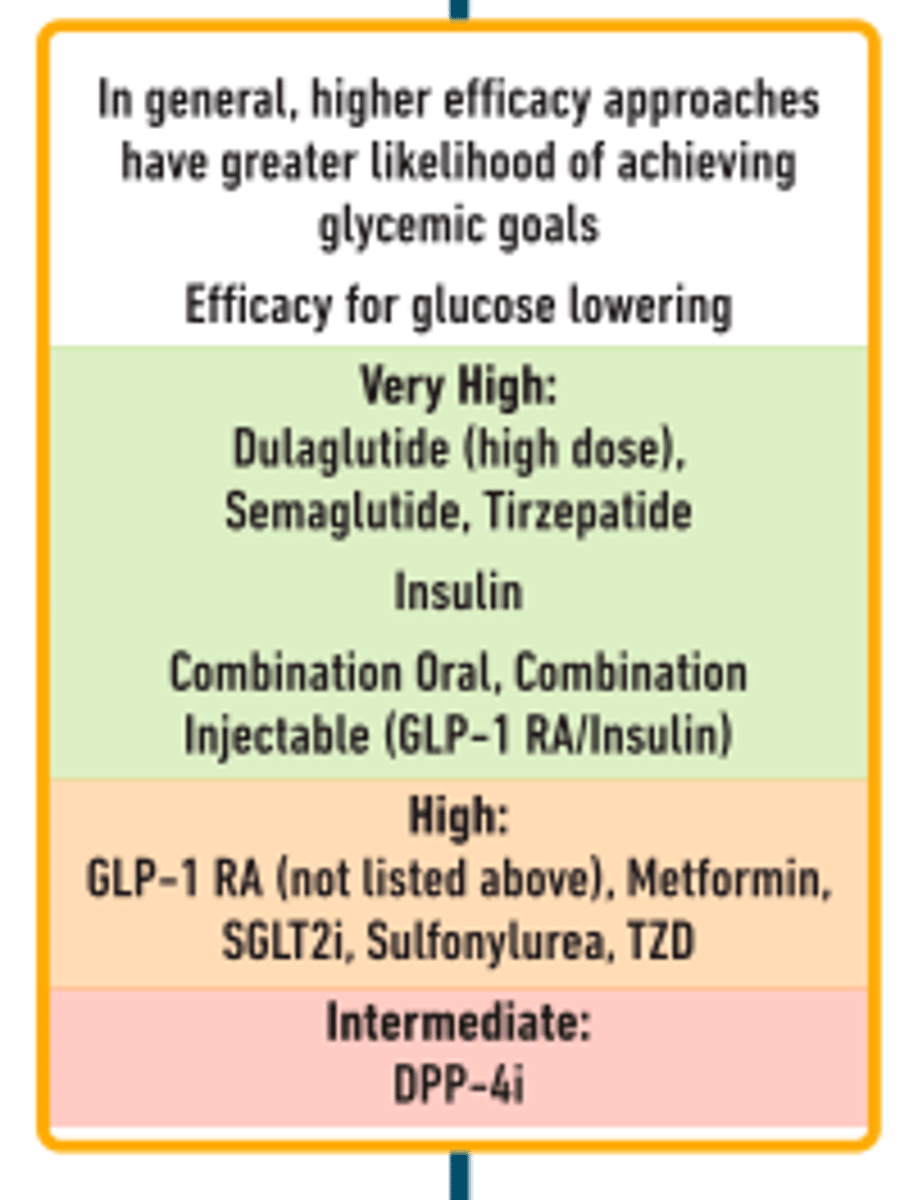
Which drugs have very high potency?
GLP-1s (dulaglutide, semaglutide)
Tirzepatide
Combination oral
Combination injectable
What is the approximate A1c decrease from very high potency drugs?
≥2%
Which drugs have high potency?
GLP-1s (other than dula/semaglutide)
Metformin
SGLT-2i's (-gliflozin)
Sulfonylurea (glipizide, glimepiride, glyburide)
TZD (pioglitazone)
What is the approximate A1c decrease from high potency drugs?
1.5-2%
Which drugs have intermediate potency?
DDP-4i
What is the approximate A1c decrease from intermediate potency drugs?
0.5-1%
What class is metformin?
Biguanide
What is the MOA of metformin?
Decreases insulin resistance
Decreases hepatic glucose output
Enhances peripheral glucose uptake
What A1c decrease does metformin cause?
High (1.5-2%)
Does metformin have a risk of hypoglycemia?
No
What is the effect of metformin on weight?
Neutral
What are the CV effects of metformin?
Neutral
Possible benefit on MACE
What is the main side effect of metformin?
GI
Manage by titrating up slowly or using ER form
What are side effects of metformin?
GI
May dec. Vit B12 levels
Concern for lactic acidosis in renal disease
C/I in hospitalized unstable congestive HF
How should the dec. in Vit B12 caused by metformin be managed?
Should be monitored at least yearly
How should metformin be used in renal disease?
Do not start if CrCl<45 ml/min
If patient already on therapy: can continue if CrCl 30-45 ml/min
Discontinue if CrCl<30 ml/min
If a patient has intravenous radiocontrast media, what should be done with their metformin?
Wait 48 hours for restart of metformin
What condition is metformin contraindicated in?
Contraindicated in unstable congestive heart failure requiring hospitalization
What are the names of the SGLT-2 inhibitors?
-gliflozin
Canagliflozin
Dapagliflozin
Empagliflozin
Ertugliflozin
How much do SGLT-2 inhibitors decrease A1c?
Intermediate to high
Less effective as GFR decreases (still used in CKD)
What makes SGLT-2 inhibitors less effective for decreasing A1c?
Decreased GFR
Less effective in CKD, but still used due to renal protective effects
Do SGLT-2 inhibitors have a risk of hypoglycemia?
No
What effect do SGLT-2 inhibitors have on weight?
Intermediate loss (2-3 kg)
Mainly water loss due to diuretic effect
(beneficial in HF)
What is the effect of SGLT-2 inhibitors on major cardiac adverse events (MACE)?
Beneficial
What is the effect of SGLT-2 inhibitors in heart failure?
Beneficial
What is the effect of SGLT-2 inhibitors in renal dysfunction?
Beneficial
Benefit when CrCl <60 ml/min or albuminuria
What are side effects of SGLT-2 inhibitors?
Euglycemic diabetic ketoacidosis
Dehydration/hypotension
Mycotic and genitourinary infections
(most common SE)
Fournier's gangrene
What is Euglycemic diabetic ketoacidosis, as a side effect of SGLT-2 inhibitors?
Presents like DKA (acidosis, N/V, fluid deficit)
But BG may be normal/not as high
How can Euglycemic diabetic ketoacidosis, a side effect of SGLT-2 inhibitors, be prevented?
Discontinue 3-4 days prior to planned surgeries, critical illness, prolonged fasting
What is Fournier's gangrene, as a side effect of SGLT-2 inhibitors?
Necrotizing fasciitis of the perineum
What classes of drugs are considered incretins?
GLP-1 receptor agonists (-tide's)
DDP4 Inhibitors (-gliptan)
GLP-1/GIP agonist (Tirzepatide)
Should two incretins be used together?
Generally, do not use the two classes of incretins together
Avoid combining GLP-1s, DDP4i's, and GLP-1/GIP
What are the names of the GLP-1 receptor agonists?
-tide's
Exenatide (Byetta, Bydureon)
Liraglutide (Victoza)
Dulaglutide (Trulicity)
Semaglutide (Injectable: Ozempic; Oral: Rybelsus)
Which GLP-1s are formulated as weekly injections?
Exenatide ER
Semaglutide
Dulaglutide
Tirzepatide (GLP-1/GIP)
Which GLP-1s are formulated as a daily oral tablet?
Semaglutide (Rybelsus)