Case 4: Ann Green
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
Osteoarthritis (OA): Description
Joint degeneration (articular cartilage, subchondral bone (under cartilage), synovium)
Affects knee > hip > hand
OA: Epidemiology
Risk factors…
Increasing age
Obesity
Joint stress
Female
OA: Etiology
Primary: Idiopathic
Secondary:
Hemochromatosis: Excess Fe deposition
Wilson disease: Excess CU deposition
Ehlers-Danlos syndrome: Defective collagen synthesis
DM
Osteonecrosis (avascular necrosis): Decreased blood supply = Bone necrosis
Alkaptonuria: Defective tyrosine metabolism
Congenital joint disorders
Joint trauma
OA Etiology: Osteonecrosis
Clinical Presentation:
Early: Asymptomatic
Advanced: Limited movement, joint pain + swelling
Local tenderness
Investigations: US
Jagged non-rounded bone head
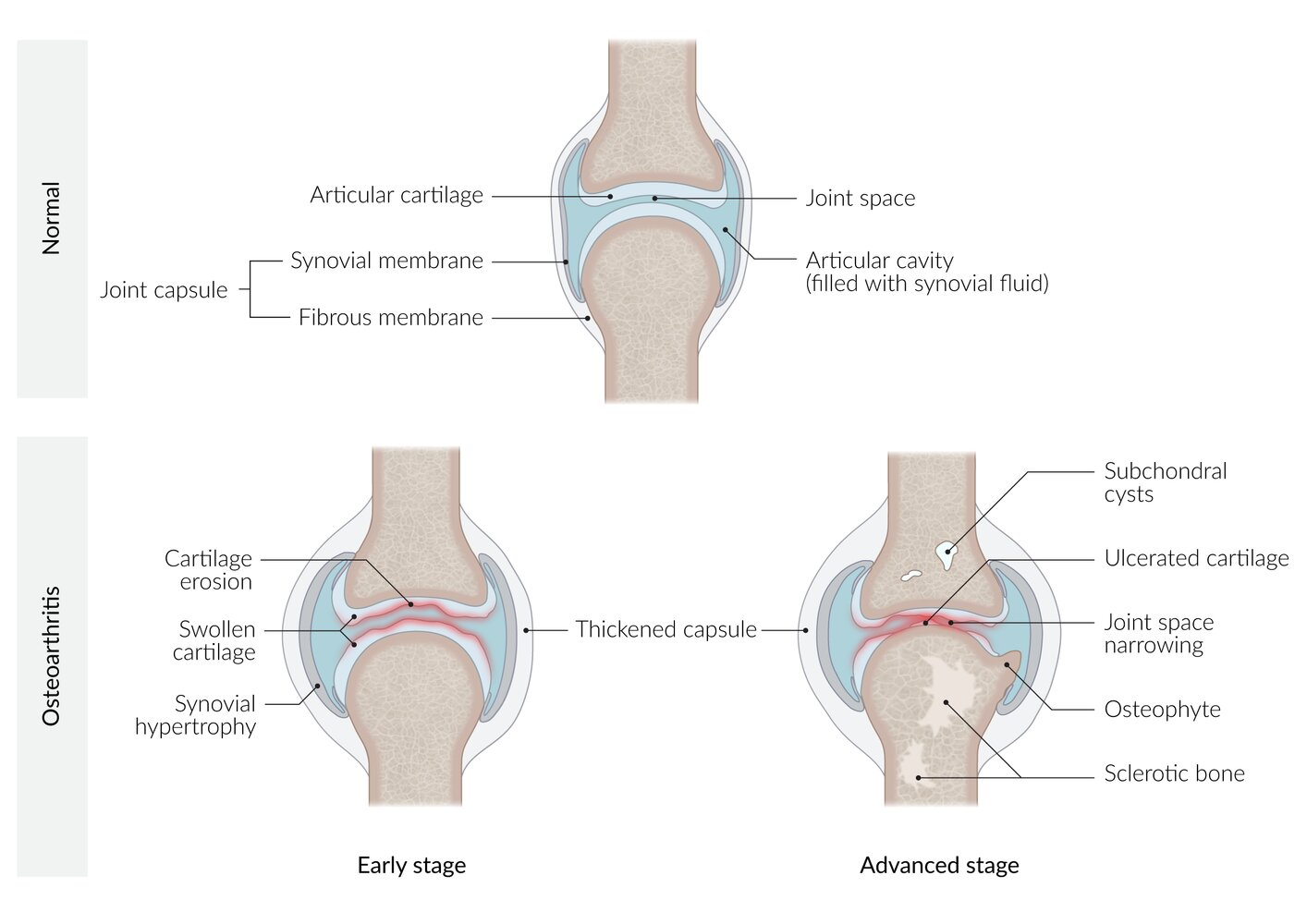
OA: Pathophysiology
Chronic mechanical stress on joints + decreased proteoglycans (age-related) = Decreased articular cartilage elasticity
Increased friability
Cartilage degeneration + inflammation + swelling = Joint space narrow and thicken + subchondral bone sclerosis
Chondrocyte hypertrophy = Fibroblast-like collagen production = Decreased elasticity + thicken joint articular cartilage
Bone tissue attempt to repair damage = Osteophyte formation (bone outgrowth)
OA: Clinical Presentation
Pain with movement
Relief at rest
Joint stiffness + decreased ROM
Early: In morning
Advanced: Throughout the day
Asymmetric joint involvement
Crepitus
Knee:
Locking/crepitus
Bowed legs
Joint swelling with activity
Hip: Pain in groin
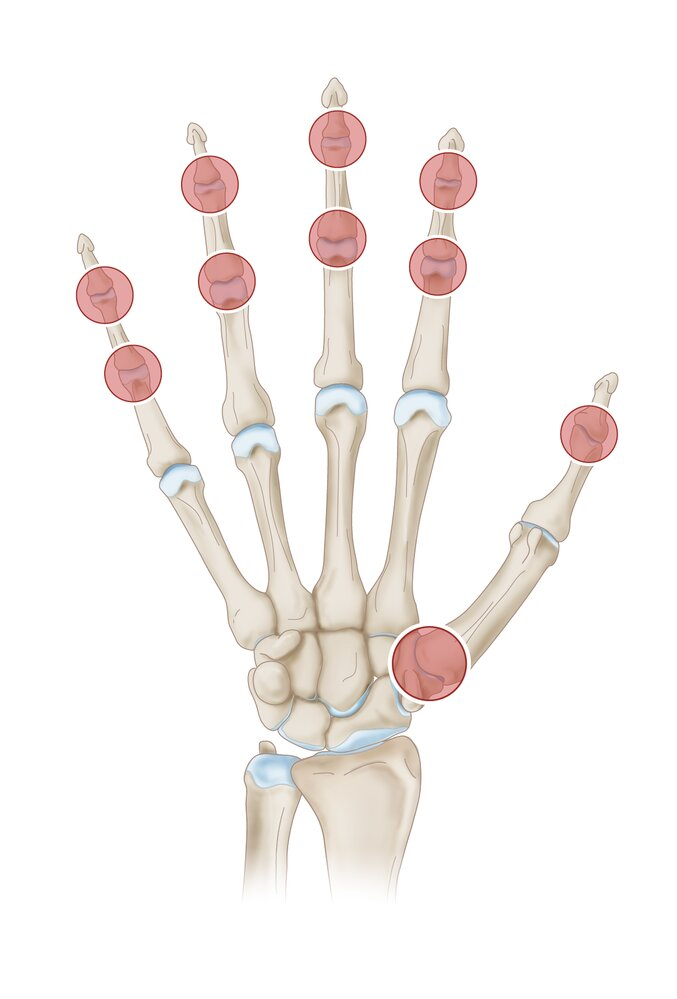
Hands:
Heberden’s Nodes: Pain + nodes on dorsal DIP
Bouchard Nodes: Pain + nodes on dorsal PIP
Rhizarthrosis: 1st CMC joint
OA: Investigations
Suspect in ≥ 45 years + clinical presentation
Imaging
Labs
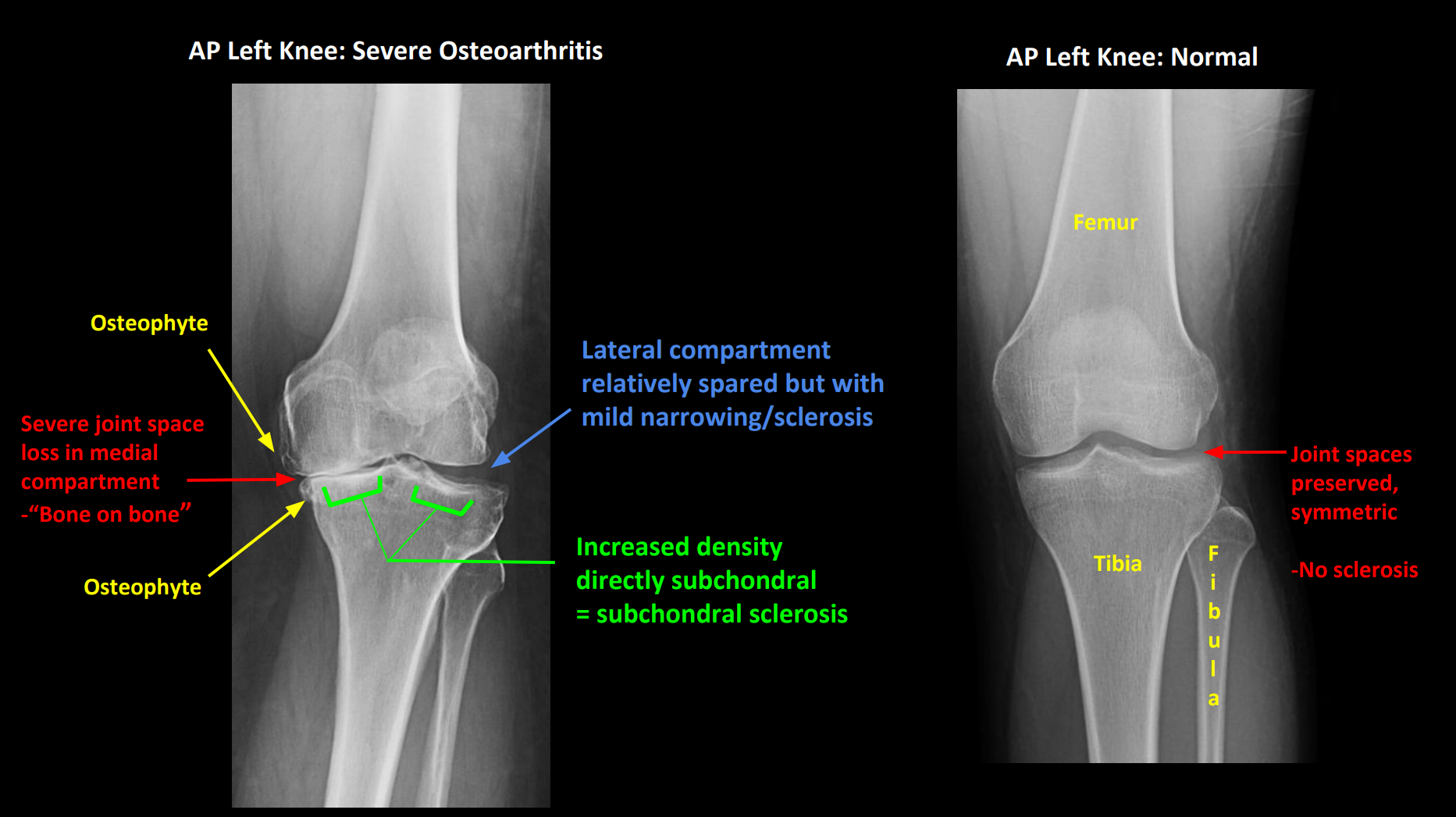
OA Investigations: Imaging
XR: First-line
4 cardinal signs (LOSS)
Loss of joint space
Irregular
Osteophytes
Spurs/densification on joint edge
Subchondral cysts
Fluid-filled cyst on joint surface (from joint stress)
Subchondral sclerosis
Increased bone density below joint cartilage
OA Investigations: Lab Tests
Blood test: Normal inflammatory markers
Erythrocyte sedimentation rate (ESR)
C-reactive protein (CRP)
Athrocentesis: Synovial fluid analysis
WBC < 2000/mm³ (no inflammation)
OA: Treatments
Non-pharmacological
Pharmacological
Surgery
OA Treatment: Non-Pharmacological
Exercise + physical therapy
Weight loss
Supportive devices (cane, knee brace)
OA Treatment: Pharmacological
NSAIDs
Acetaminophen
Opioids
Intraarticular glucocorticoid injections
OA Pharmacological: NSAIDs
First-line
Topical: Knee
Oral: Inadequate with topical or hip OA
OA Pharmacological: Acetaminophen
Second-line
Less effective than NSAIDs
OA Pharmacological: Opioids
Short-term use
Not recommended
OA Pharmacological: Intraarticular Glucocorticoid Injections
Local short-term relief in hip + knee
OA Pharmacologic: Adverse Effects
From long-term use
NSAIDs:
Increase GI bleeds
Increase MI risk
Worsen HTN + edema
Renal toxicity
Acetaminophen: Liver injury
Opioids:
Constipation
CNS effects
Intraarticular Glucocorticoid Injections:
Pain + swelling
Hyperglycemia
HTN
OA Treatment: Surgery
Arthroplasty: Partial/complete joint replacement with endoprosthesis (artificial joint)
Arthrodesis: Fuse bones in joint position
OA: Complications
Limiting function (walking, sleeping)
Pain
Osteonecrosis (less common)
OA: Prognosis
Highly variable
Remain stable with treatment
Slow evolution → Joint replacement
OA vs Inflammatory Arthritis (IA): Pathophysiology
OA: Mechanical + age-related joint degradation
IA: Autoimmune disorder = Immune cells (T cells) attack/damage synovial joints
OA vs IA: Clinical Presentation
Morning stiffness
OA: < 30 mins
IA: > 1 hour
Joint swelling
OA: Cool + hard
IA: Warm + soft
Joint pain
OA: Relieved by rest
Tender + deep → From bones
IA: Persistant
Soft + boggy
OA vs IA: Investigations
Blood test
OA: No inflammatory markers
IA: Increased…
ESR
Normal Men: 0-15 mm/hr
Normal Women: 0-20 mm/hr
CRP
Normal: < 10 mg/L
Synovial fluid analysis
OA: < 2000/mm³
More fluid, less viscous
IA: > 2000/mm³
Analgesics: Tylenol
Acetaminophen
Tylenol: Indications
Fever
Pain
Preferred in pregnancy
Tylenol: MOA
Reversible COX inhibition
Mainly in CNS
Tylenol: Efficacy
Preferred for mild symptoms
Antipyretic + analgesic
Tylenol: Toxicity
Gastric symptoms (minimal)
Liver toxicity + failure
Analgesics: NSAIDs
Ibuprofen
Diclofenac
Naproxen
Aspirin
NSAIDs: Indications
Acute + chronic pain
RA
IA
Acute gout attack
Headache/migraine
Fever
Indomethacin: Close patent ductus arteriosus
NSAIDs: MOA
Reversible COX inhibition = Decrease prostaglandin synthesis
Aspirin: Irreversible COX inhibition
NSAIDs: Efficacy
Preferred for moderate/severe symptoms
Antipyretic + analgesic + anti-inflammatory
NSAIDs: Toxicity
Gastric ulcers
Heart attack
Stroke
Renal impairment