5 Phases of Rehab
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
What are the five phases of rehab?
1) max protection
2) moderate protection
3) minimum protection
4) no protection
5) return to sport
How can you determine what phase someone is in?
-tissue status
-patient perception
-movement tolerance
What should a tissue status assessment include?
clinical signs
-alignment
-end feel
-swelling
healing timeline
diagnostic imaging
-radiographs
-MRI
-diagnostic ultrasound
What is the shortcoming of tissue status?
-does not always correlate with symptoms (pain is multifactorial)
-doesn't inform the rehabilitation specialist on the best course of treatment
What are the self-reported outcome measures?
-functional: higher score desirable
-disability: lower score desirable (disability index)
-kinesiophobia: lower score desirable (TSK)
-confidence scale: higher score desirable
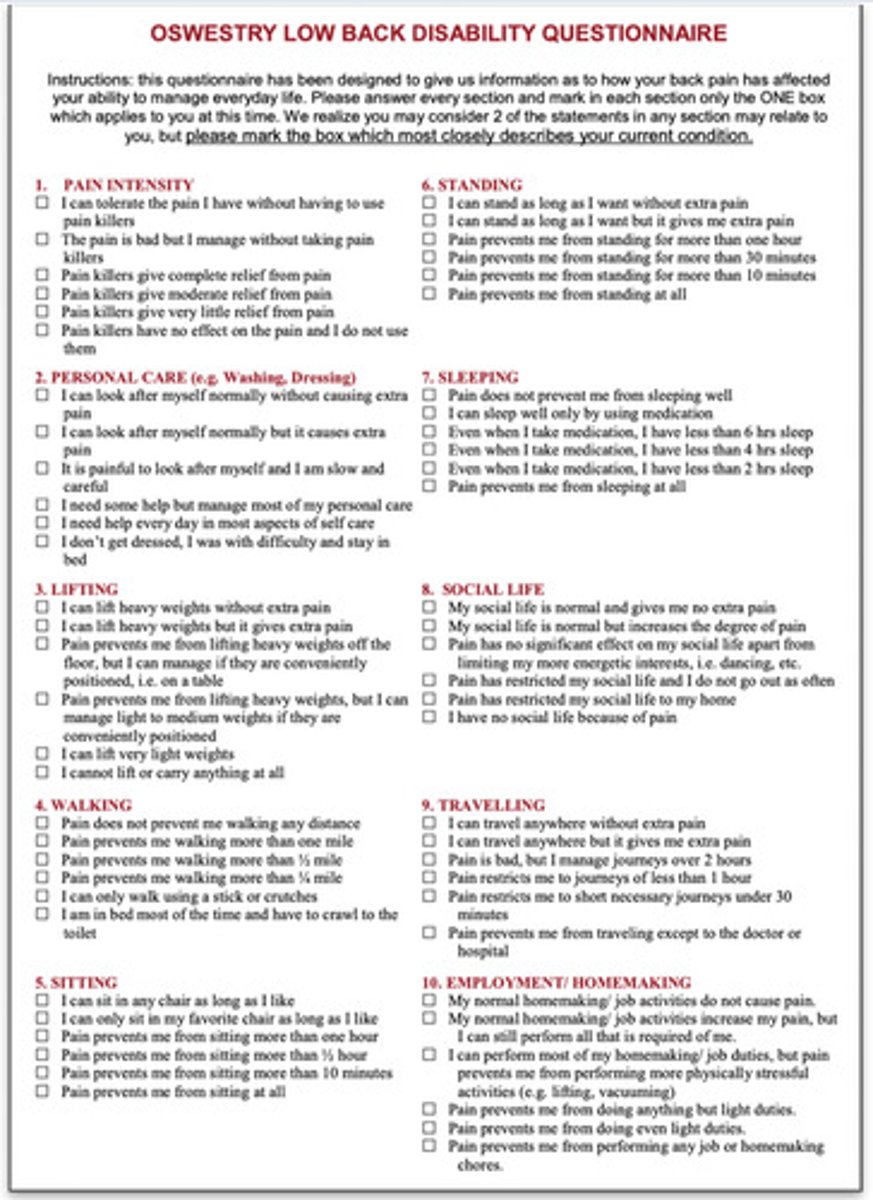
How can you determine staging using the Oswestry Disability Index?
-higher scores= max protection phase
-moderate score= moderate protection phase
-low score= min protection phase
-zero/very low score= no protection phase or RTS
What is the difference between load tolerance and load capacity?
load tolerance: point at which a given load results in symptoms
load capacity: maximal amount of force a tissue may generate prior to failure
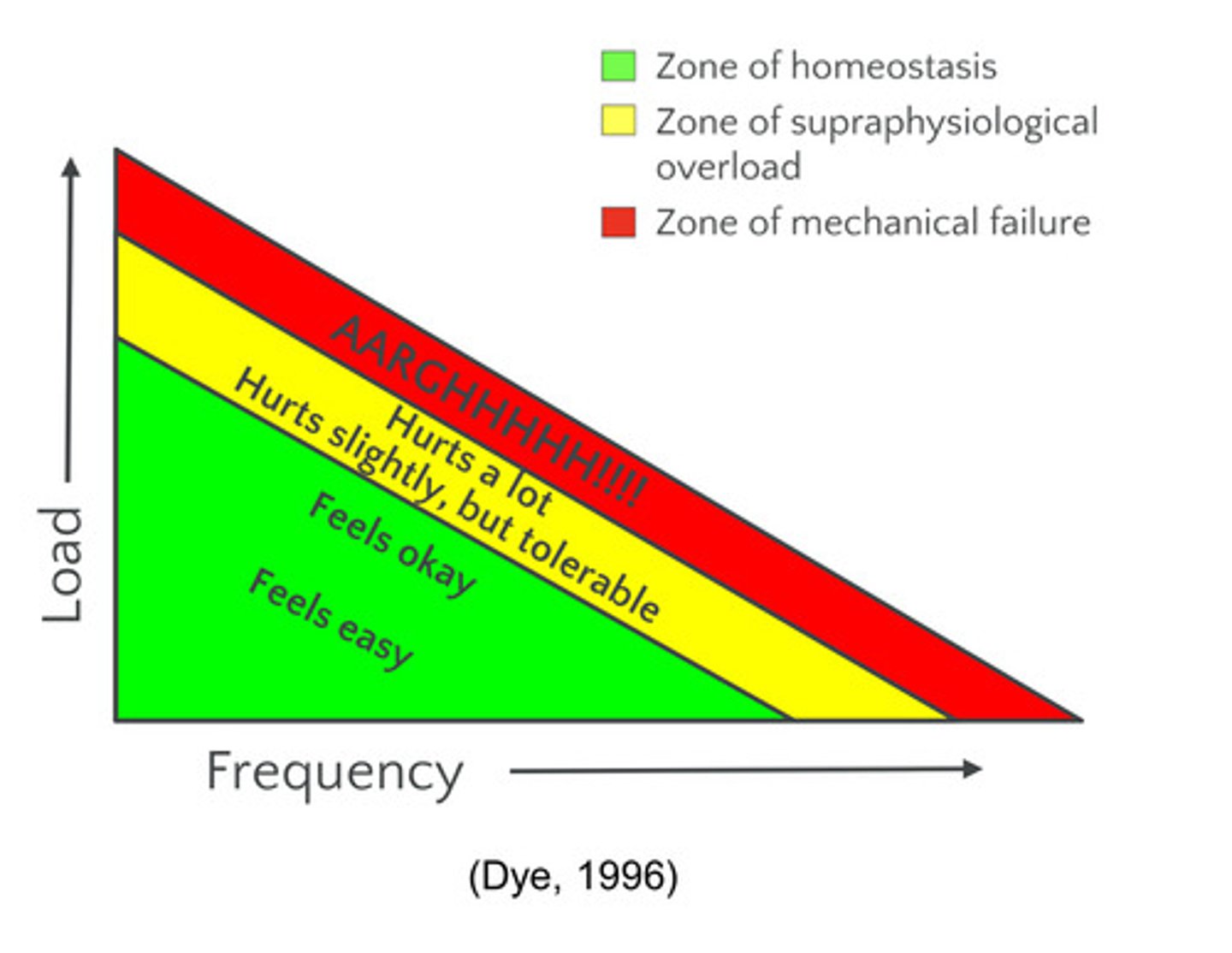
What is the relationship between load and frequency?
load: force imparted onto body (ie. LB, KG, or N)
frequency: cycles and/or duration (ie. sets, reps, seconds, or hours)
symptoms result from the interplay of load and frequency
What is Thomee's pain monitoring guide?
>5/10 pain= red
3 to 5/10 pain= yellow
<3/10 pain= green
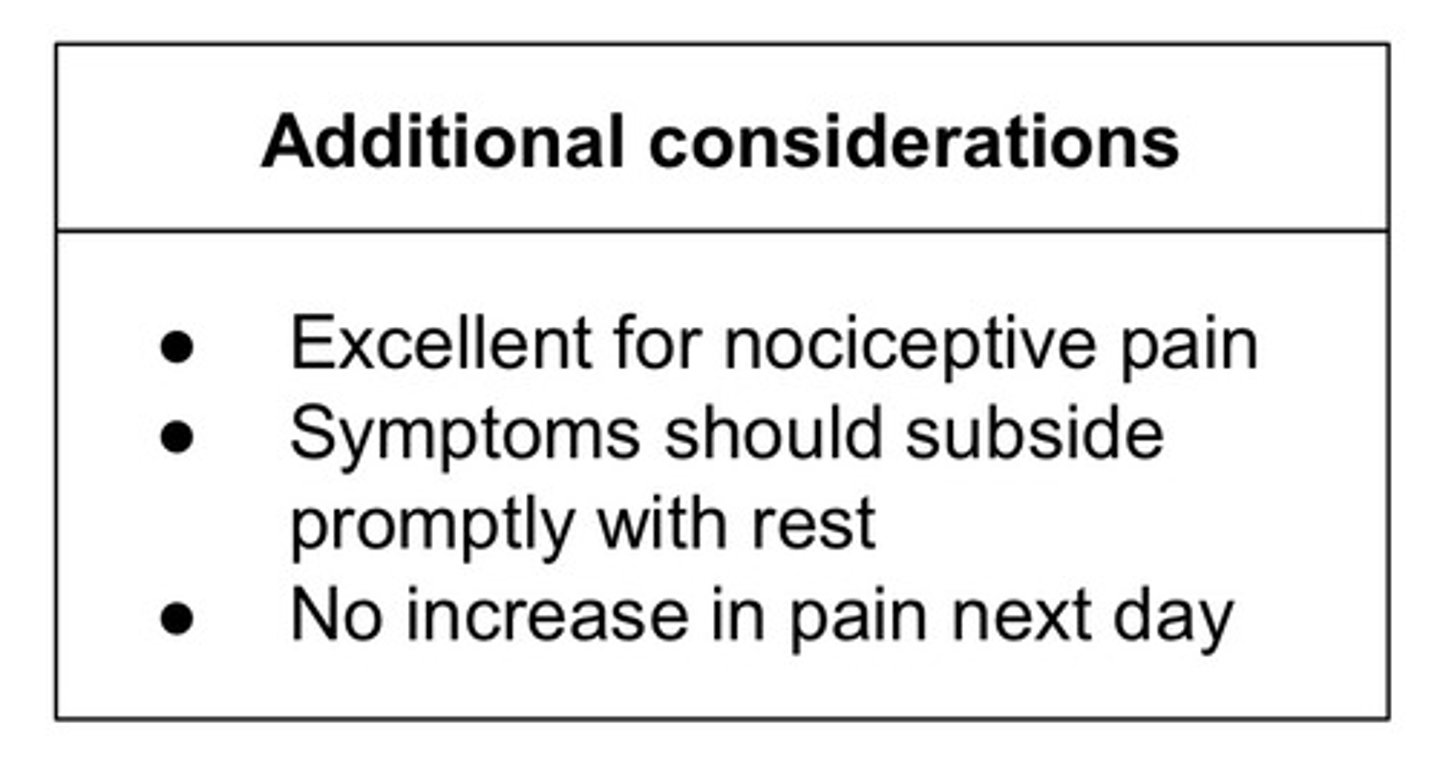
What is Cormack's rule of 10?
-used to determine the maximum rate of perceived exertion (RPE) for a patient with pain
-calculated by subtracting the patient's pain level from 10; difference is the max RPE to be utilized
-great for patients with high levels of pain in which exercise is not contraindicated (ie. nociplastic pain)
-should monitor next day response and adjust accordingly
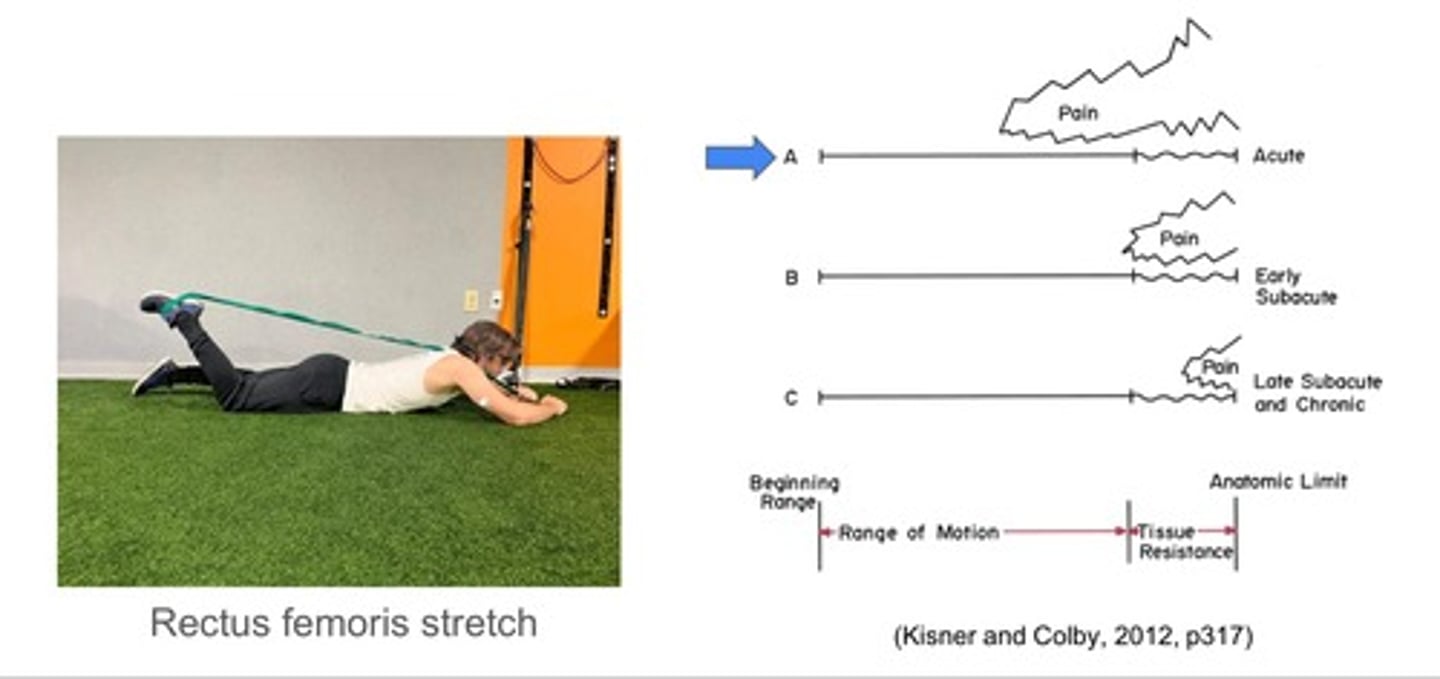
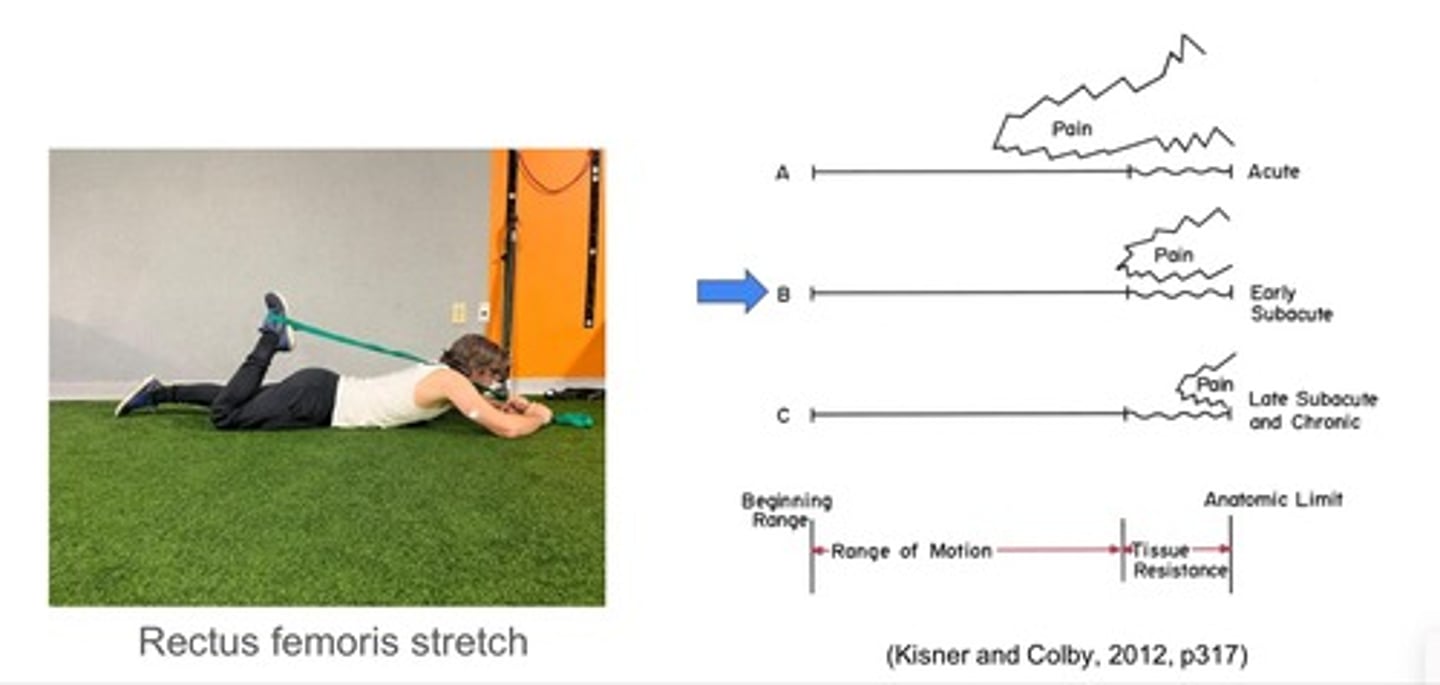
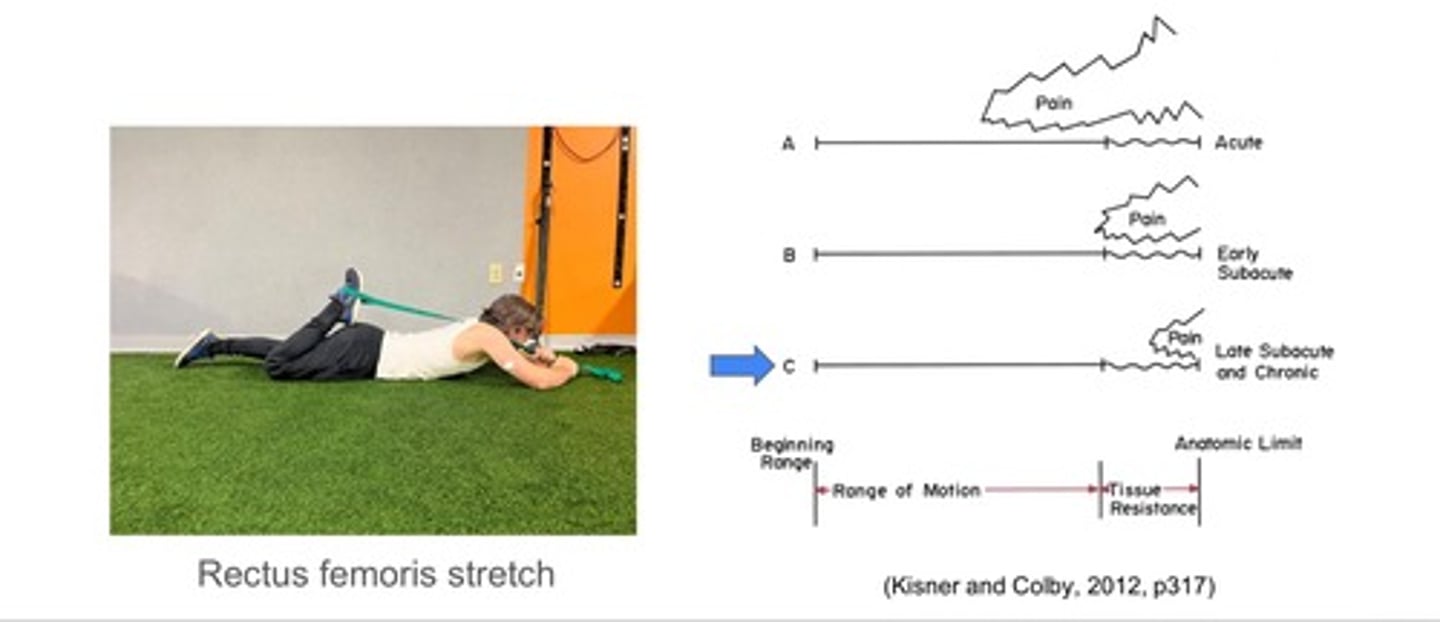
What is stretch tolerance?
refers to a tissue's tolerance to lengthened positions; depending on acuity of injury, a tissue may exhibit differences in stretch tolerance
-earlier onset of pain= more severe
-later onset of pain= less severe
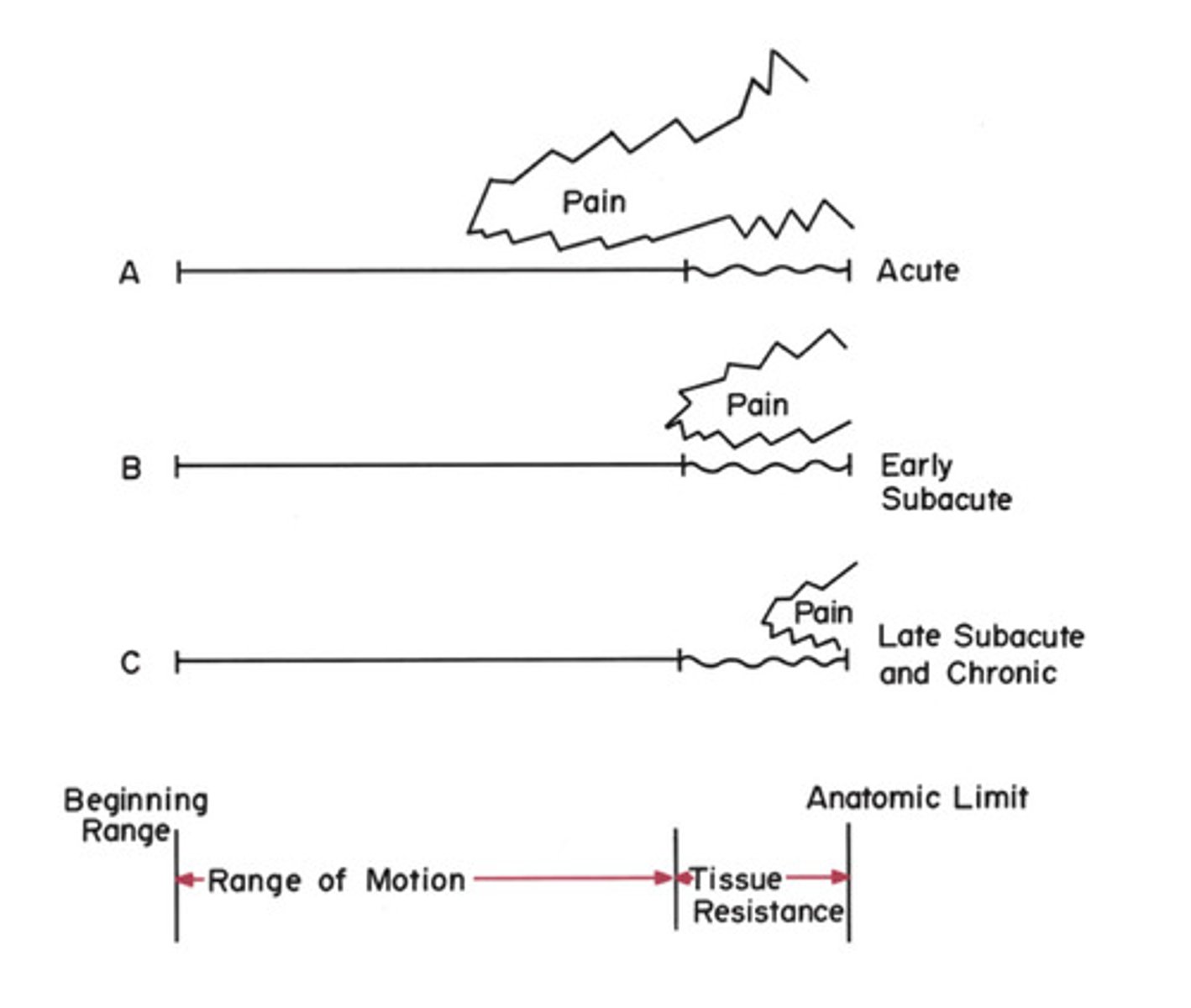
Stretch Tolerance of Rectus Femoris (Acute)
Stretch Tolerance of Rectus Femoris (Subacute)
Stretch Tolerance of Rectus Femoris (Chronic)
What are the goals of the maximum protection phase?
-temporary off-loading of symptomatic structures
-reduce arthrogenic muscle inhibition (AMI)
-in presence of soft-issue injury, promote tissue healing and inflammation reduction
What is the treatment in the maximum protection phase?
education, activity modification, external support, pain/swelling modulation, gentle muscle activation (guided by pain)
How can you avoid introducing nocebo?
don't use pathoanatomic explanations when possible, except for acute injuries with obvious pathoanatomic source
-consider describing symptoms in the context of tissue sensitivity
-analogies may be helpful to explain difficult concepts
ex. your body's alarm system is going off; don't say "your disc is bulging"
What are offloading strategies?
interventions used to decrease demand on symptomatic structures
-alternate movement
-assistive device
-use of orthotics and/or bracing
-shoe wear modification
-tape
o elastic: may have more of a neurological input [ie. kinesiology tape])
o rigid (more structural input [ie. athletic tape, Mulligan tape, McConnell tape])
![<p>interventions used to decrease demand on symptomatic structures</p><p>-alternate movement</p><p>-assistive device</p><p>-use of orthotics and/or bracing</p><p>-shoe wear modification</p><p>-tape</p><p>o elastic: may have more of a neurological input [ie. kinesiology tape])</p><p>o rigid (more structural input [ie. athletic tape, Mulligan tape, McConnell tape])</p>](https://knowt-user-attachments.s3.amazonaws.com/98d73ac0-c5df-4bab-a01f-f934a2a89a51.jpg)
WHat are some pain/swelling modulation techniques?
-massage
-joint mobilizations/manipulations
-limb elevation
-compression (ie. sleeves, bandages, pneumatic game ready, water submersion*)
-e-stim
-medications
-cryotherapy
*if pool is heated, could increase inflammation
What are the goals of the moderate protection phase?
-continue to improve muscle activation
-increase muscular endurance (more endurance prescription)
-restore muscle cross-sectional area (low load/high frequency can cause some hypertrophy)
-increase motion in hypomobile segments
-in presence of soft-tissue injury, promote tissue maturation
What is the treatment in the moderate protection phase?
low load/high volume muscle activation (guided by pain), ROM, continued external support
What are the goals of the minimal protection phase?
-increase endurance
-continue to improve muscle cross-sectional area
-initiate strength training
-in presence of soft-tissue injury, promote tissue reorientation
What is the treatment in the minimum protection phase?
light tissue stress/tension (guided by pain), incorporation of functional movements, low impact cardiovascular activity
ex. squatting, deadlift, jogging, etc.
What are the goals of the no protection phase?
-increase level of activity
-continue to increase muscle strength
-improve power
What is the goal of the no protection phase?
address remaining strength deficits, incorporate exercises to improve rate of force development (power), and progress to higher impact cardiovascular activity
ex. sprinting
WHat are the goals of the return to sport phase?
-allow adequate time to adapt to rigors of sport
-increase patient's confidence
-avoid re-injury secondary to training loads
What is the treatment for the return to sport phase?
sport-specific exercises, consultation on gradual return to practice/play
What are the three return to sport phases?
1) performance training (sport specific)
2) practice participation (reintegration, gradual ramping)
3) play (return to competition)
[5 phases of rehab]
True or False: The greater the pain, the greater the degree of tissue involvement.
FALSE
The goal of this phase is to increase level of physical activity, muscle strength, and power.
a) maximum protection
b) moderate protection
c) minimum protection
d) no protection
d) no protection
The goal of this phase is to facilitate tissue maturation, muscle activation, and restoration of joint mobility.
a) maximum protection
b) moderate protection
c) minimum protection
d) no protection
b) moderate protection
The goal of this phase is to facilitate tissue reorientation, muscle strength, and endurance.
a) maximum protection
b) moderate protection
c) minimum protection
d) no protection
c) minimum protection
Pain at the very end of ROM (beyond the point of tissue resistance) would be expected with which phase?
a) maximum protection
b) moderate protection
c) minimum protection
d) no protection
c) minimum protection
d) no protection
True or False: In Scott Dye's Envelope of Function Model, the zones where symptoms arise remain the same, regardless of the individual.
FALSE
Pain at the beginning of a ROM would be associated with what phase?
a) maximum protection
b) moderate protection
c) minimum protection
d) no protection
a) maximum protection
True or False: The patient denies pain during ROM but has deficits in RFD. This is consistent with the no protection phase.
TRUE
Which of the following is not an example of an off-loading strategy?
a) alternate movement
b) use of orthotics or bracing
c) assistive device
d) pulsed ultrasound
d) pulsed ultrasound
True or False: When educating patients, you should always use pathoanatomic explanations.
FALSE