RESPIRATORY SYSTEM
1/98
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
99 Terms
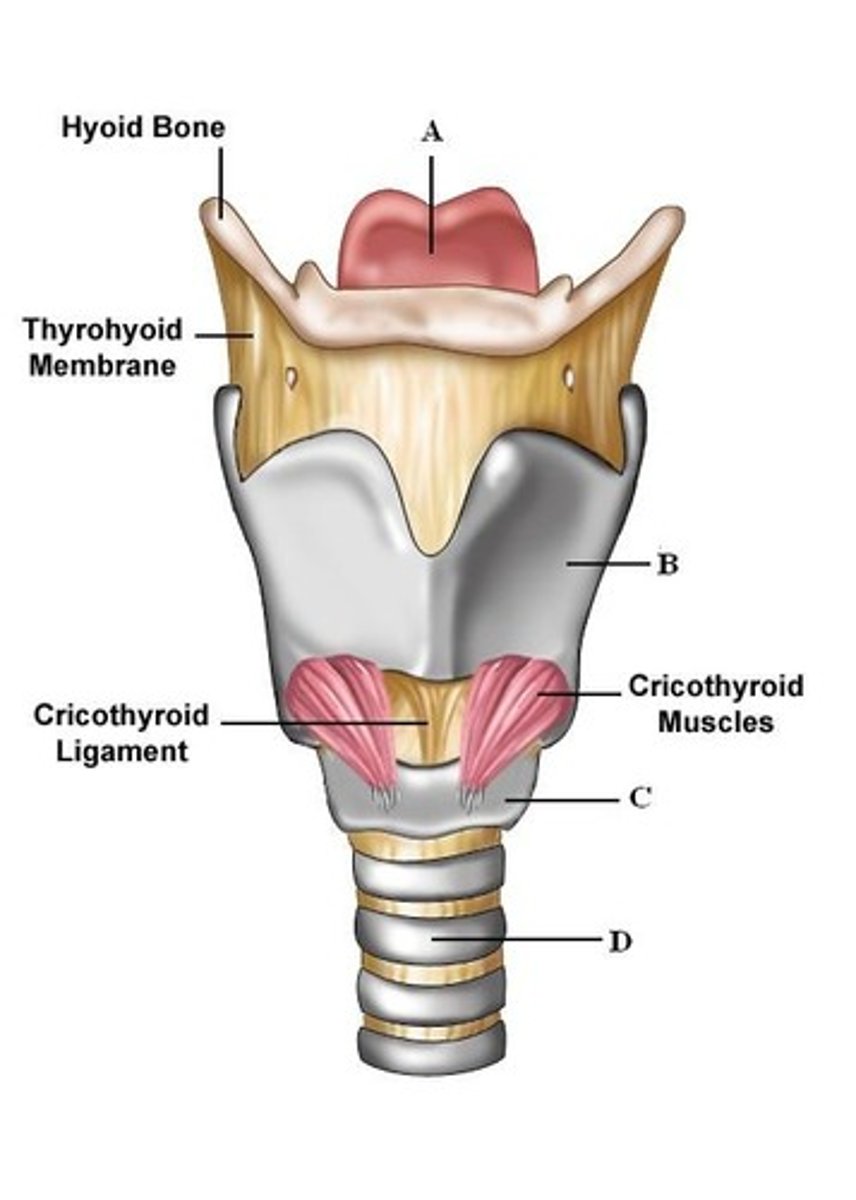
- pseudostratified ciliated columnar epithelium
- glottis
- epiglottis (elastic cartilage)
- cartilages (hyaline, thyroid, cricoid)
- vocal cords (vesitbular-inelastic ; vocal folds-very elastic)
describe the larynx
- pseudostratified ciliated columnar epithelium
- submucosal glands
- tracheal cartilages ( c-shaped)
- trachealis smooth muscle (ANS control diameter)
describe the trachea
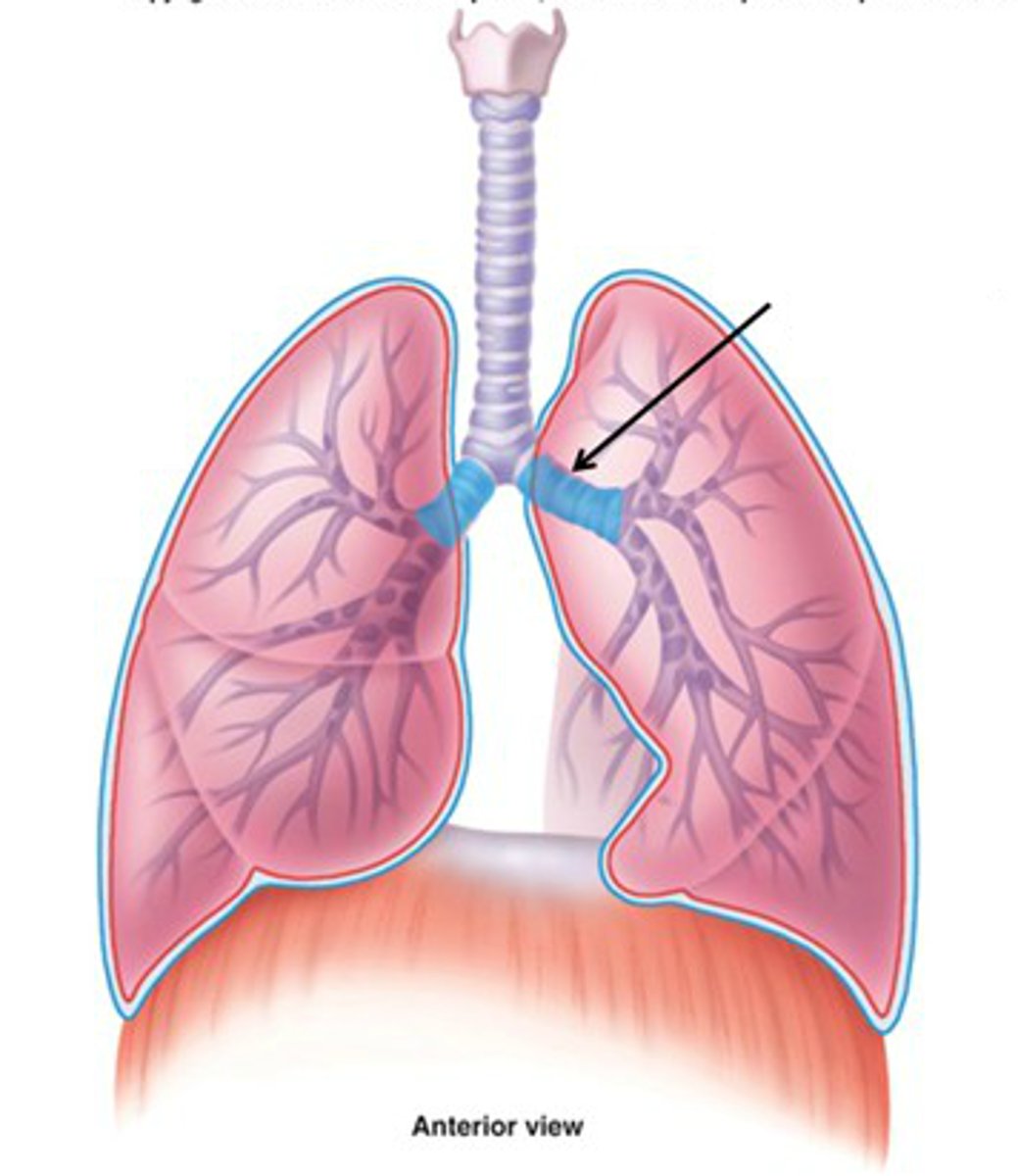
- c shaped cartilage rings
- R is larger in diameter and more vertical than L
- enter lungs at hilum
- branching of airways - bronchial tree
describe the R/L primary bronchi
- secondary (lobar)
- tertiary (segmental): gives rise to bronchopulmonary segments
- decrease cartilage (rings to plates)
- increase smooth muscle
describe the bronchial tree
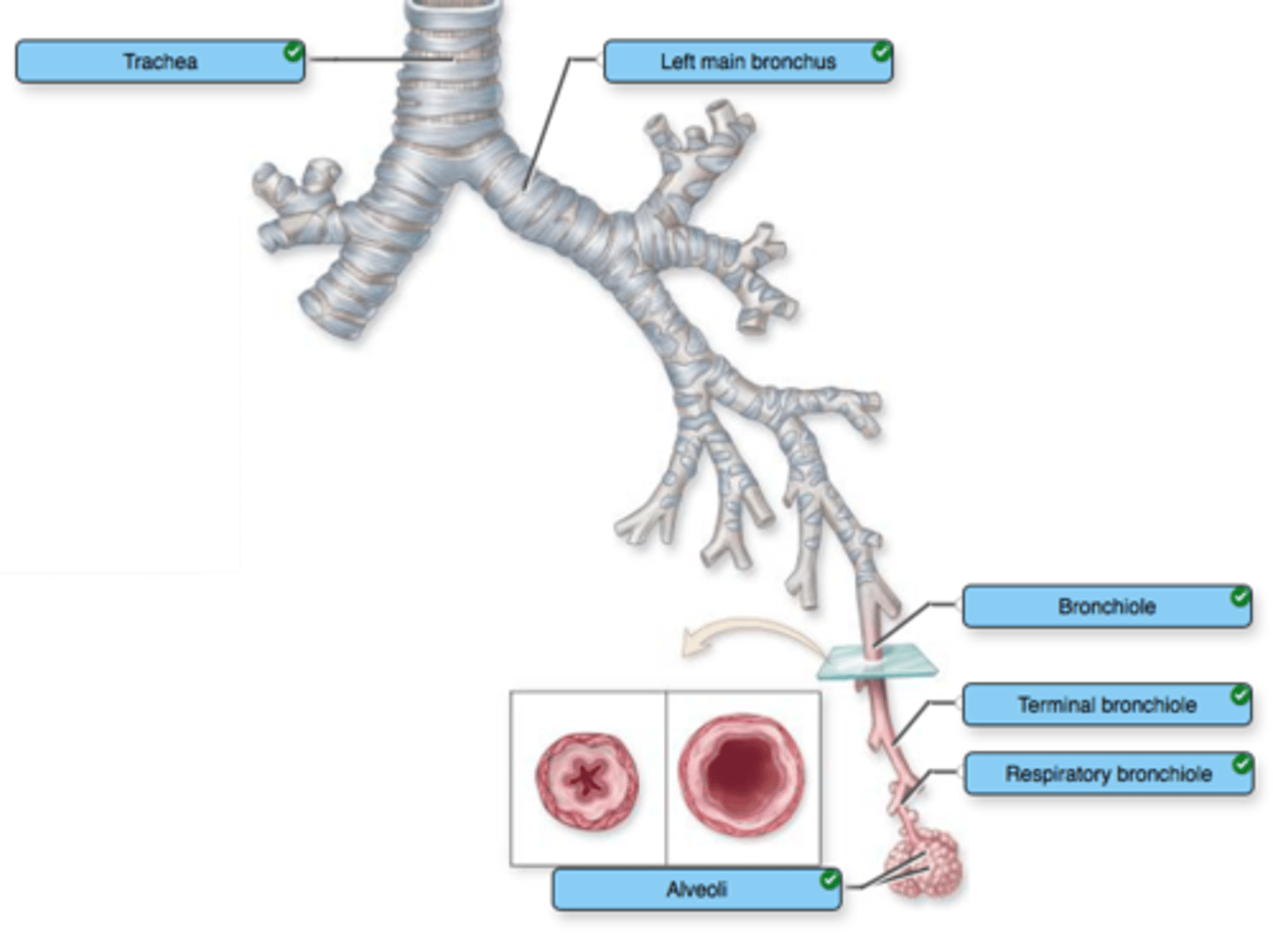
- less than 1 mm
- terminal (last conducting zone); respiratory (first resp zone)
- simple cuboidal epithelium
- lose cartilage; sparse to no cilia
- smooth muscle (ANS control; bronchodilation/constriction)
describe bronchioles
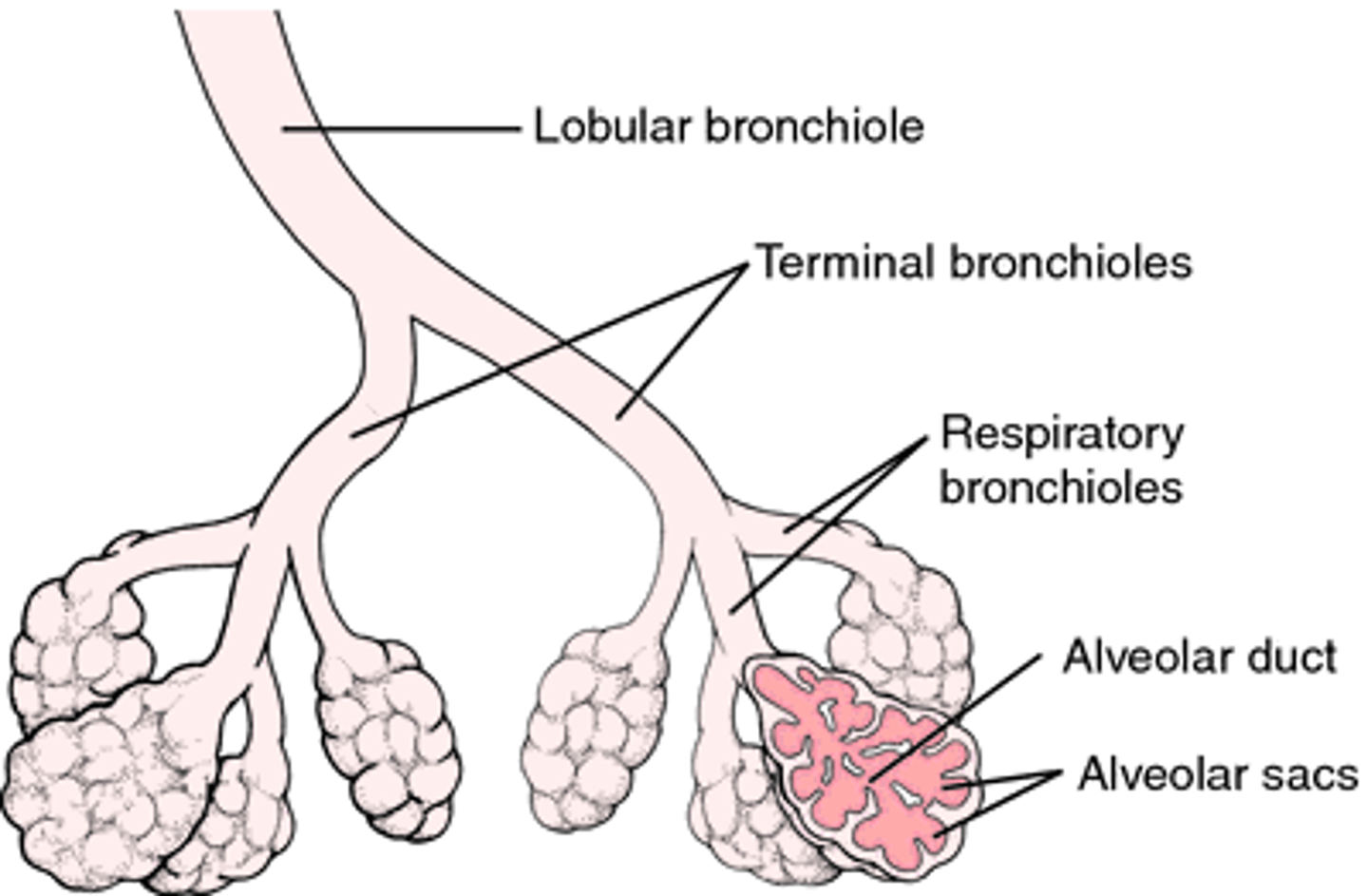
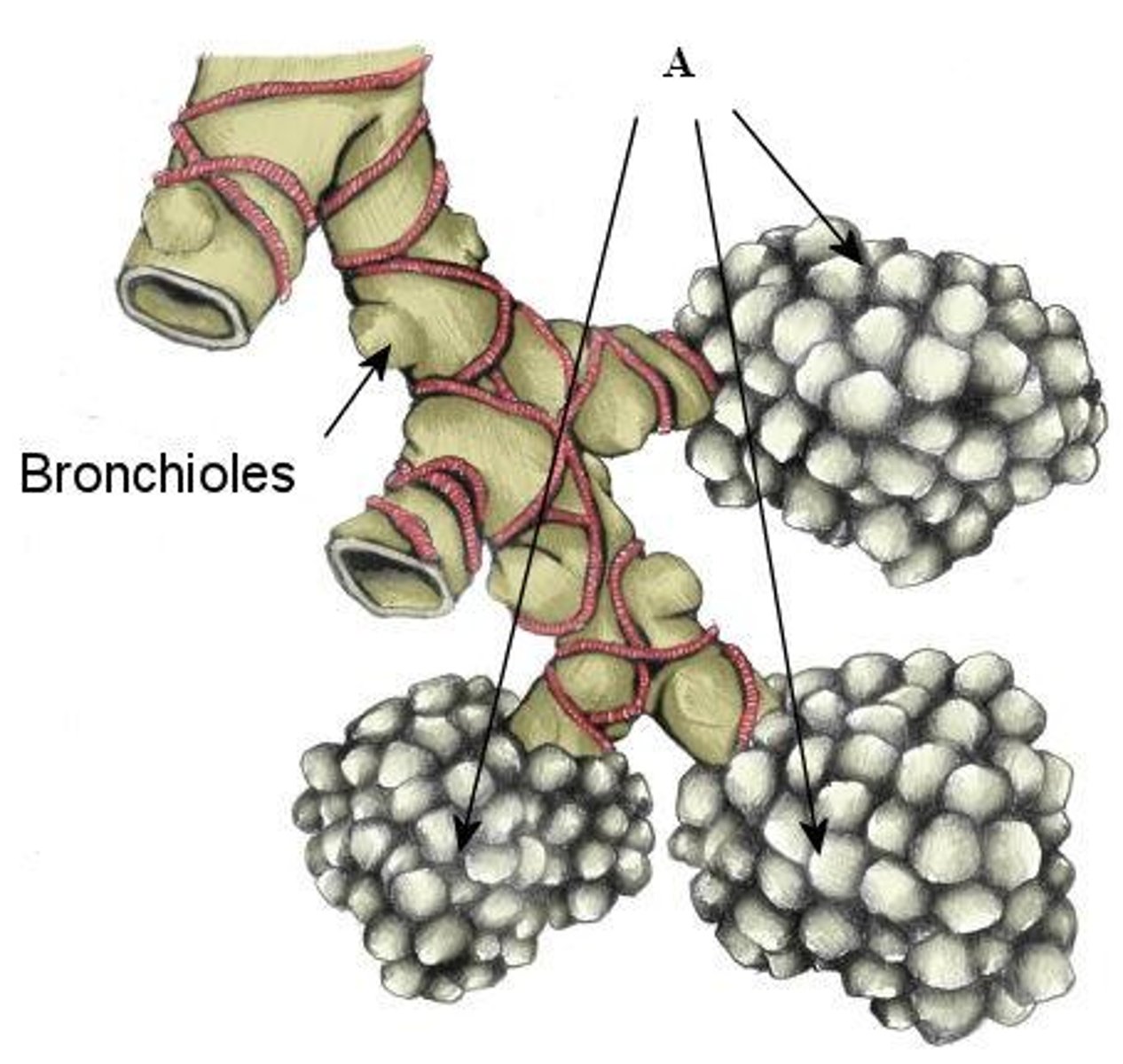
- alveolar pores
- elastic fibers
- pulmonary capillaries
- exchange ( huge surface area)
describe alveoli
- pulmonary ventilation (move air in/out)
- external respiration (gas exch bwn lungs + blood)
- gas transport (move O2 + CO2)
- internal respiration (gas exch btwn blood + tissues)
functions of the respiratory system
- smell
- speech
- innate (nonspecific) defenses
what are some smaller additional functions of respiratory system
- nose , nasal cavity
- pharynx (naso-, oro-, laryngo-)
what structures make up the upper respiratory
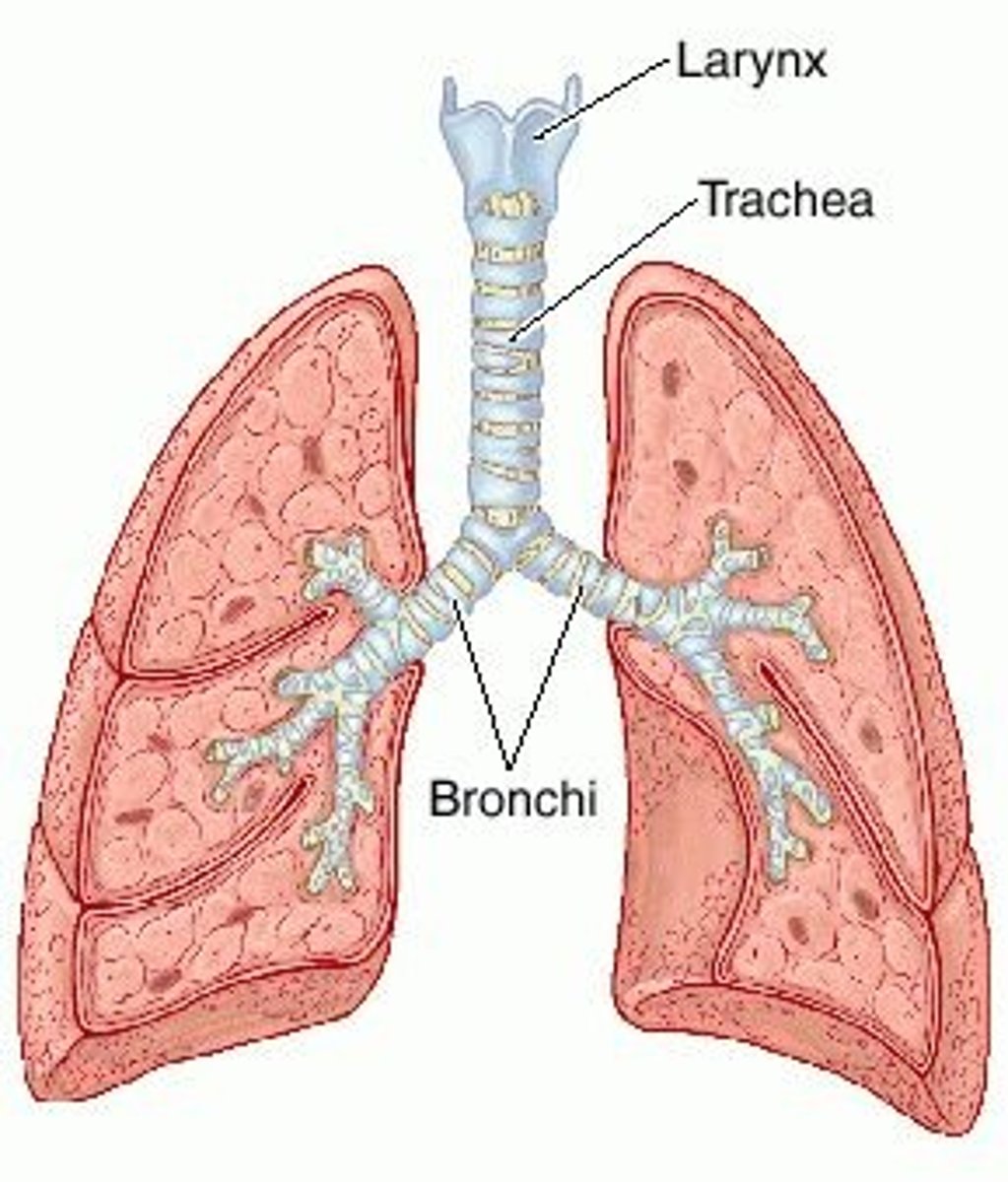
- larynx
- trachea
- bronchi
- bronchioles
- alveoli
what structures make up the lower respiratory
mucous membrane
-> tissue: epithelium + lamina propia
-> mucus secreted by goblet cells & glands in CT
-> may have cilia
describe the respiratory mucosa
- filters air (nasal hairs)
- warms air (mucosa is vv vascular)
- humidifies air (water from lining evaporates into incoming air)
- cleans air (cilia, antibodies in mucus, macrophages)
- olfaction (olfactory epithelieum)
- pseudostratfied ciliated columnae (move dirty mucus to pharynx)
- nasolacrimal ducts (drainage)
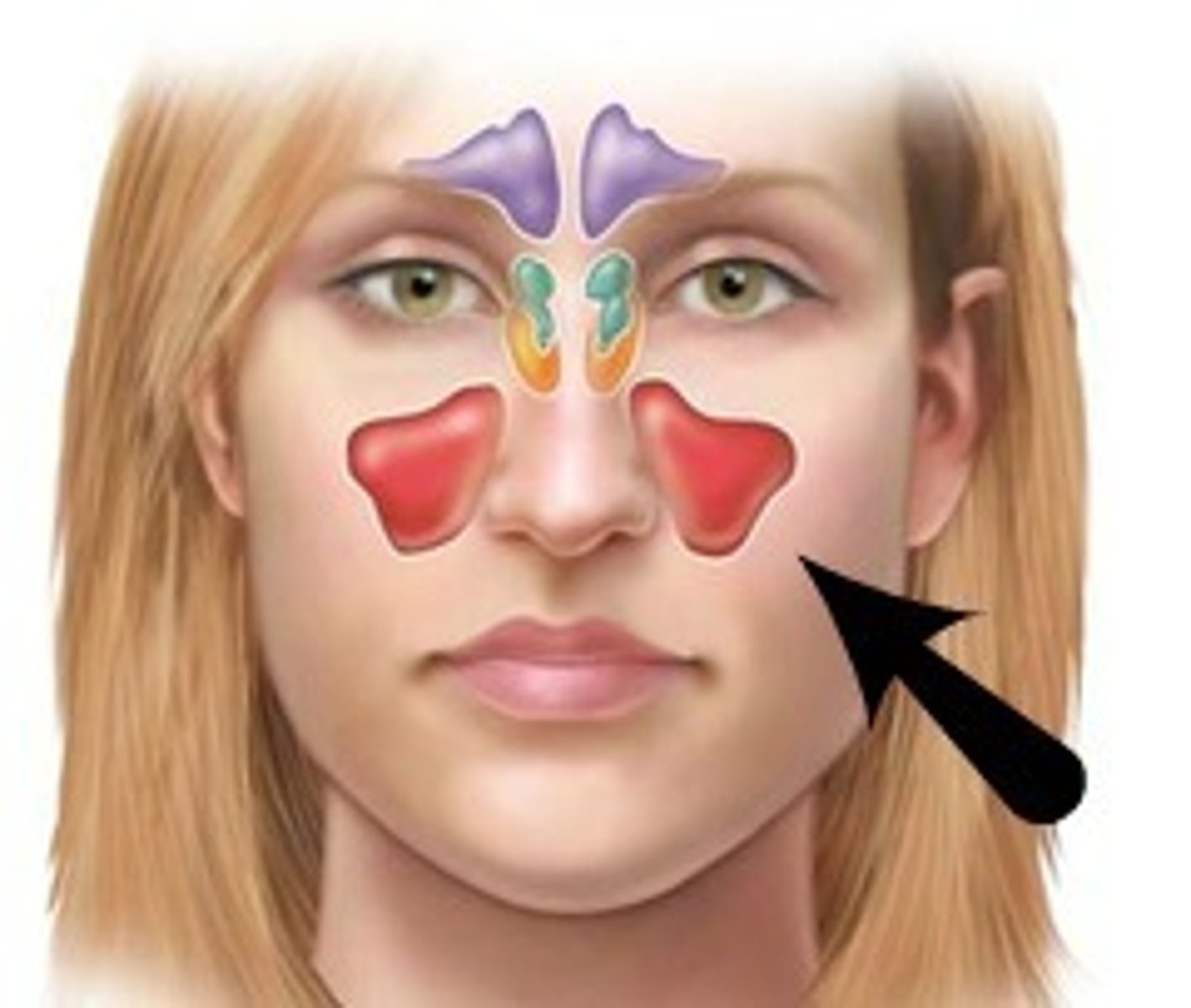
- paranasal sinuses
describe the functions of the nasal cavity
- frontal
- ethmoidal
- sphenoidal
- maxillary
what are paranasal sinuses
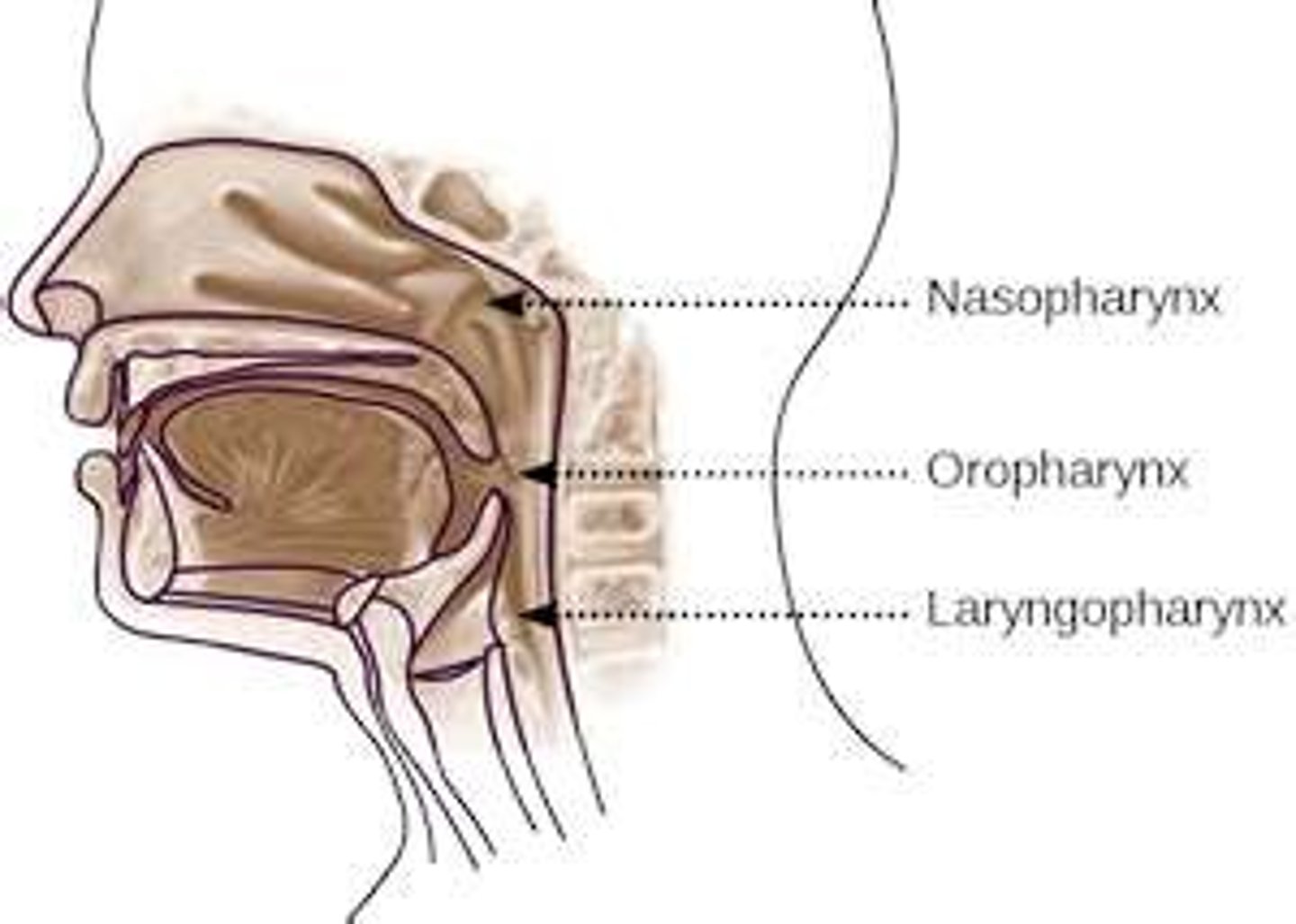
- pseduostratified ciliated columnar
- auditory tubes (eustachian, pharyngotympanic)
- pharyngeal tonsil
describe the nasopharynx
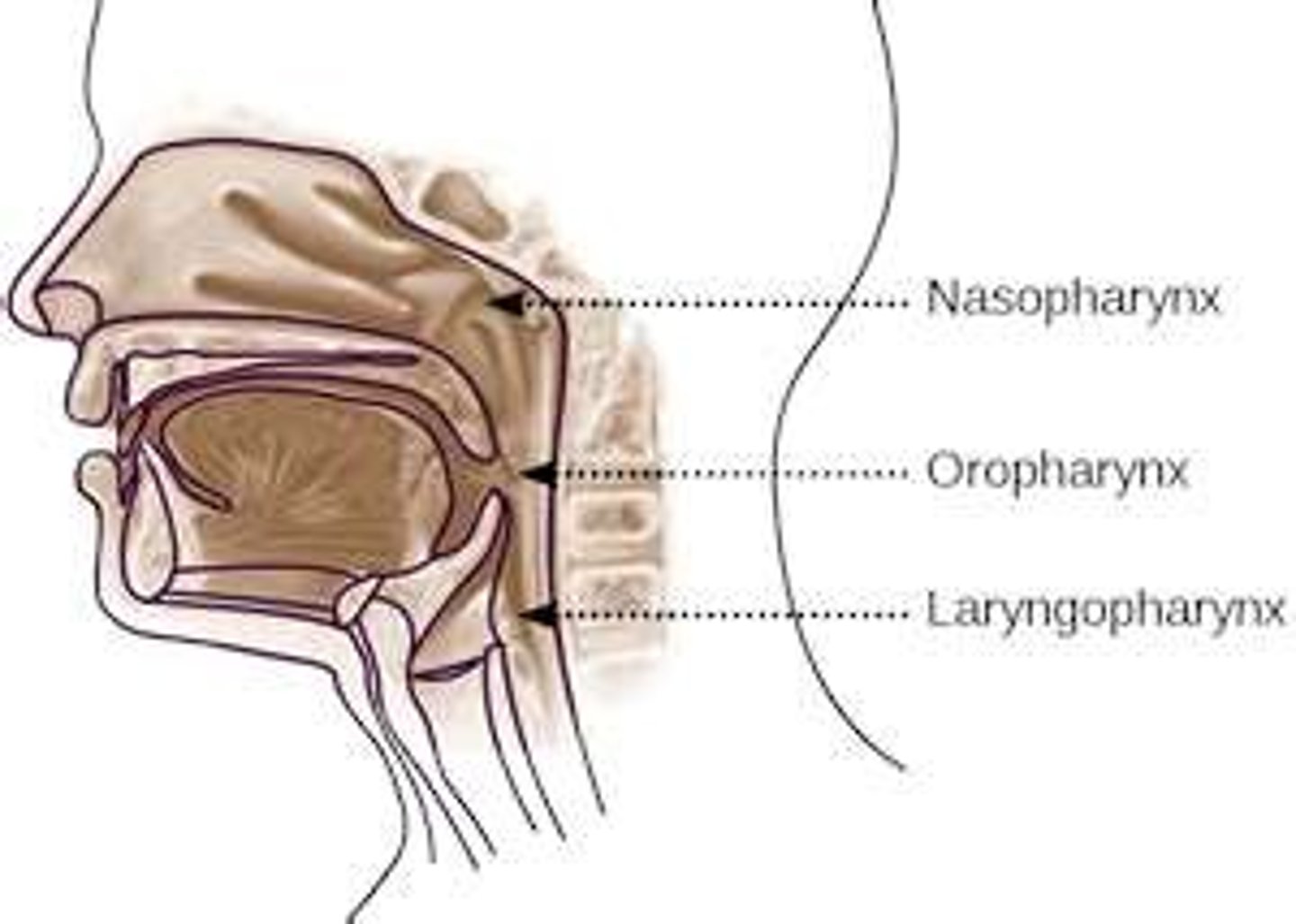
- stratified squamous epithelium
- palatine and lingual tonsils
describe the oropharynx
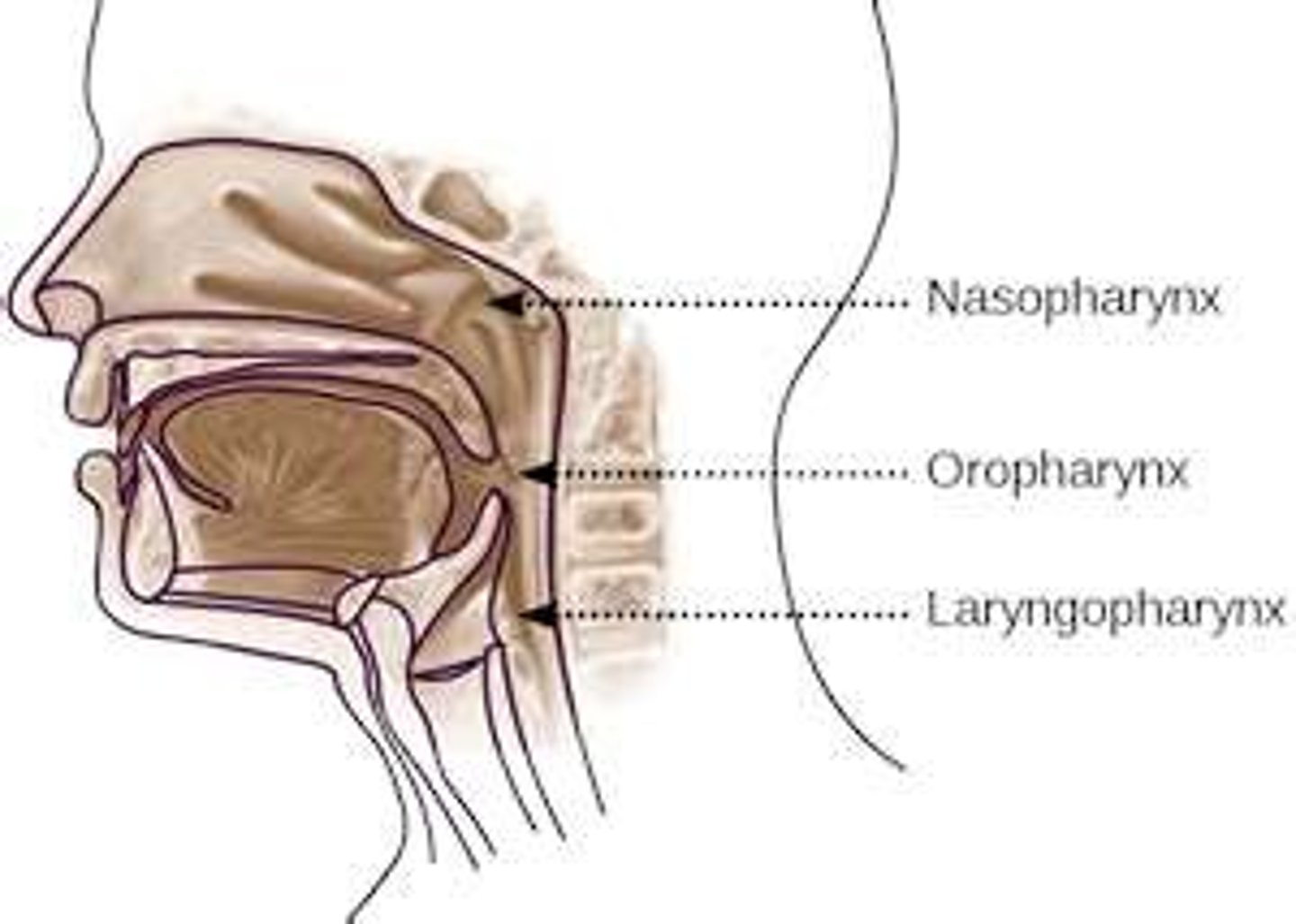
- stratified squamous epithelium
describe the laryngopharynx
skeletal muscle (aids in swallowing)
what muscle is the pharynx
- respiratory bronchioles
- alveolar ducts
- alveolar sac of multiple alveoli
what are the respiratory zone structures in order
- macrophages
- alveolar type 1
- alveolar type 2
what are the 3 alveolar cells
- simple squamous epithelium cells
- alveolar pores (equalize pressure between alveoli)
what is alveolar type 1
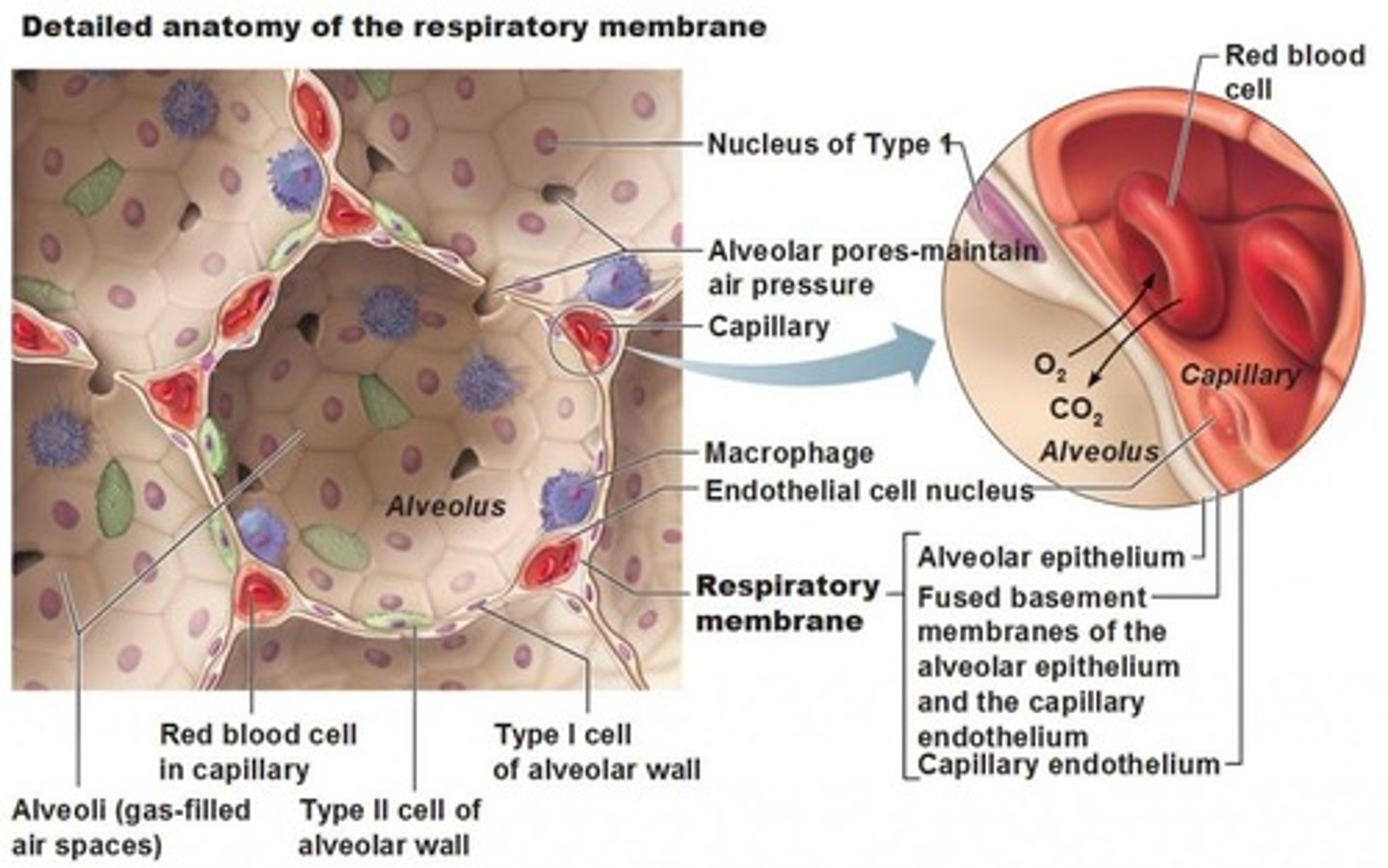
- epithelial cells that secrete surfactant
- decreases surface tension to keep alveoli from collapsing (easier to inflate)
what is alveolar type 2
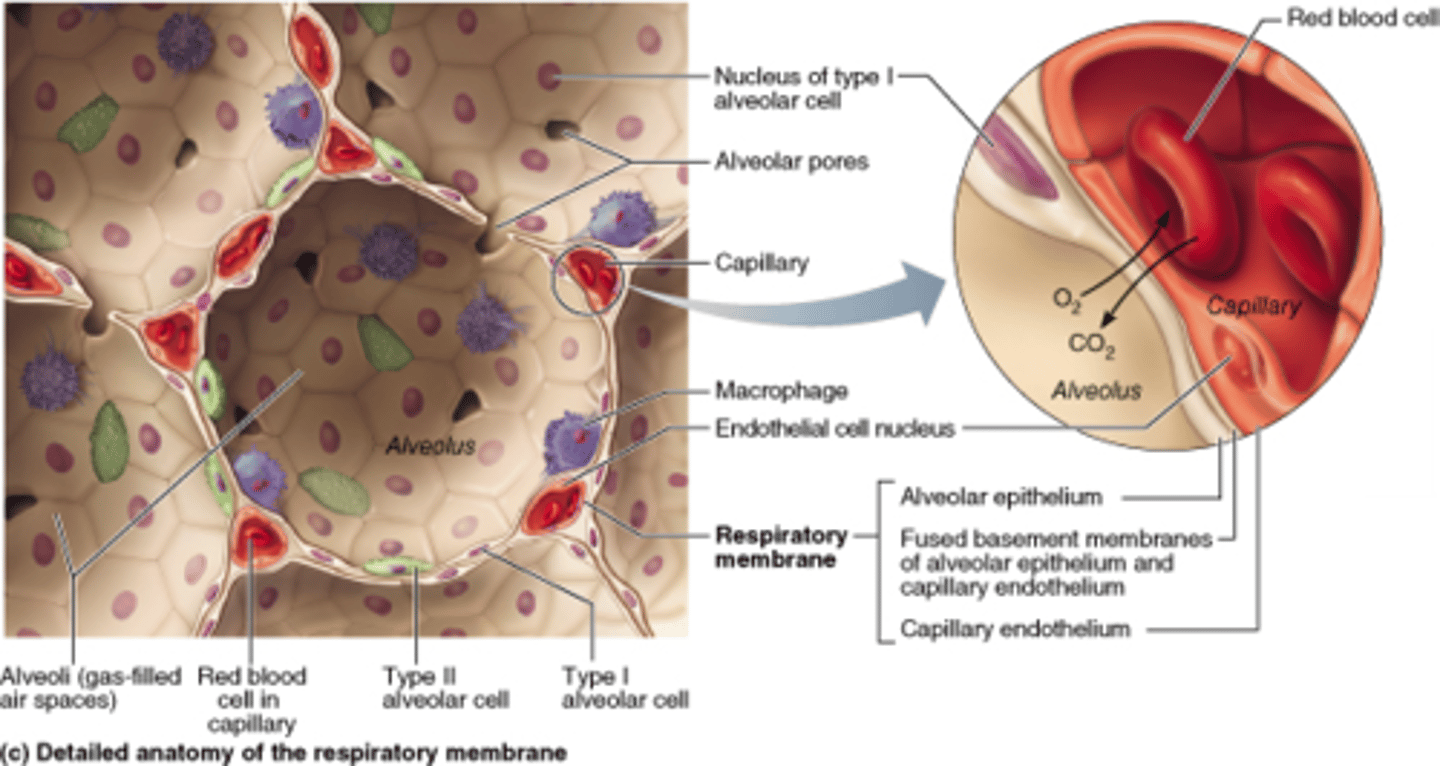
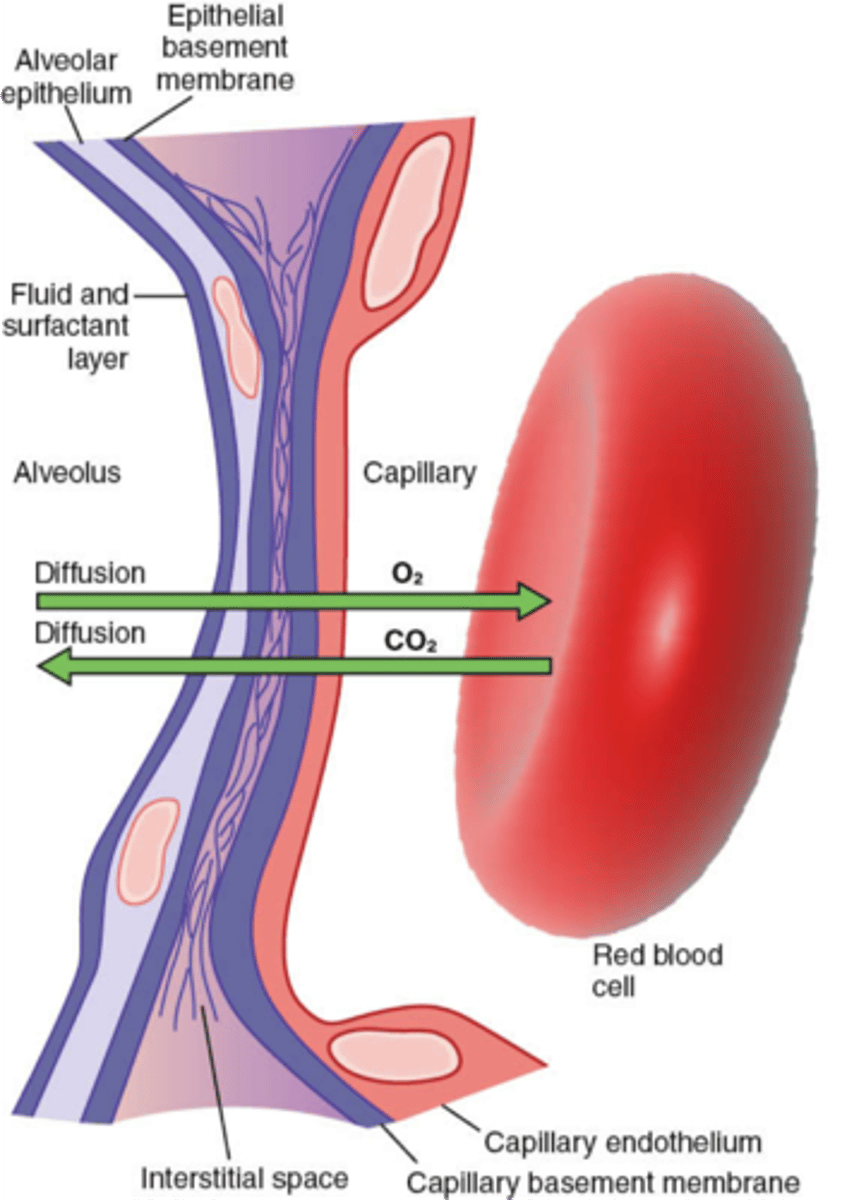
- both THIN for easy exchange (gas diffusion)
- alveolar wall: simple squamous w/ thin basement membrane
- capillary wall: endothelial cells (simple squamous) w/ thin BM
describe the respiratory membrane
- R has 3 lobes ; L has 2 (divided by fissures)
- hilum (entrance/exit into and out of lung; houses BV, LV, nerves)
- air filled spaces surrounded by elastic tissue
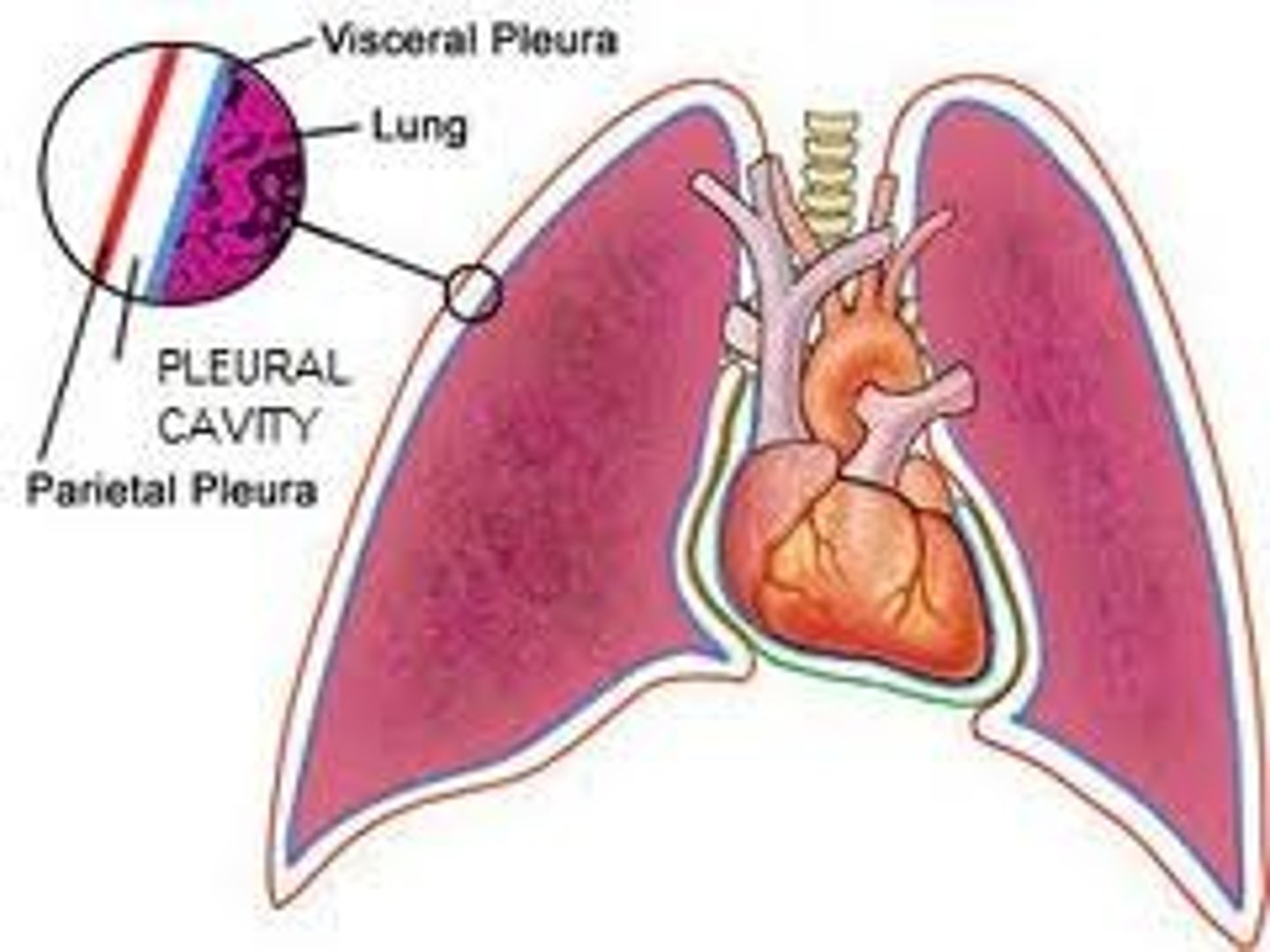
- enclosed in pleural cavity filled w/ small amount of fluid (dec friction)
describe the lungs
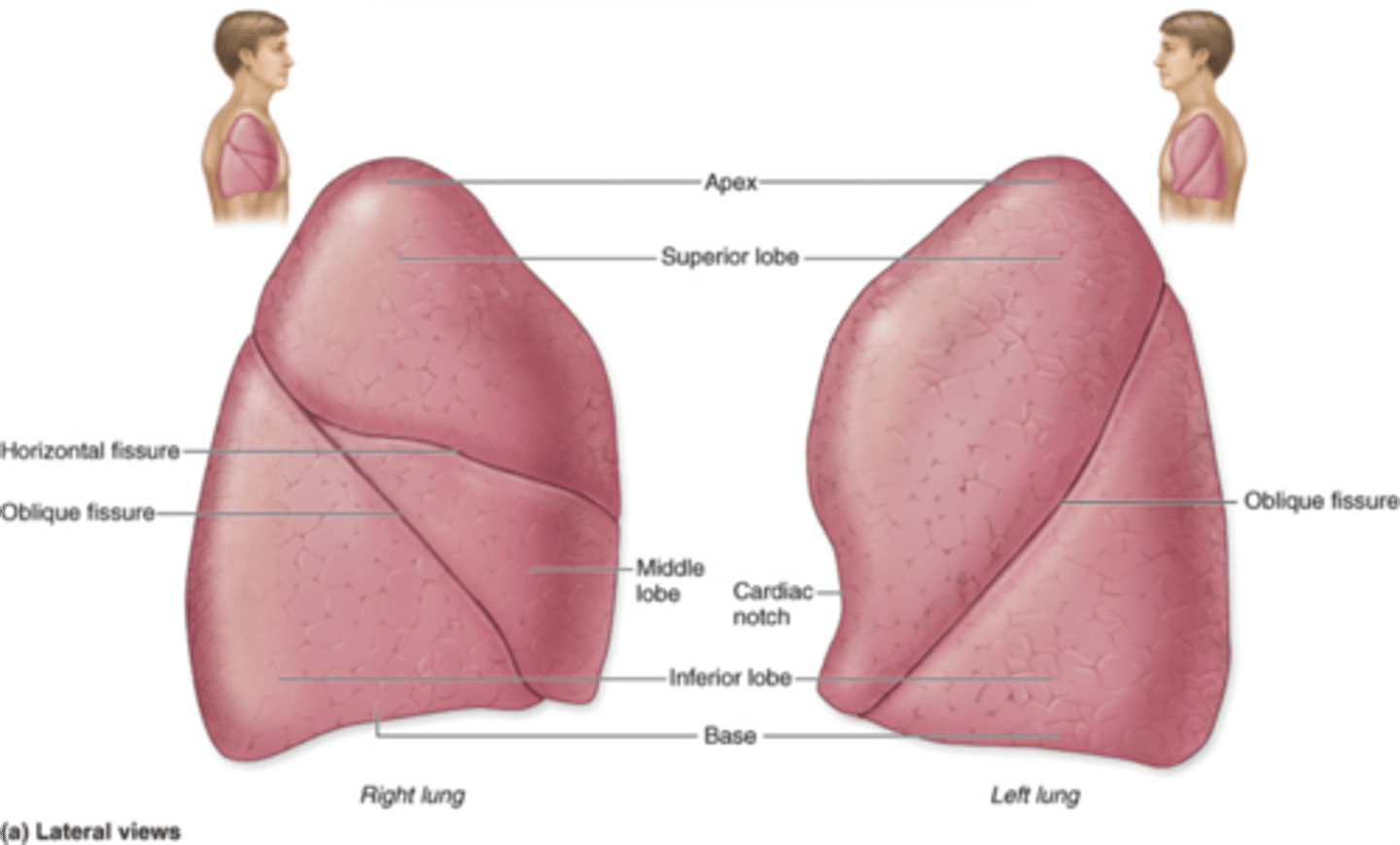
left - has 2 lobes and cardiac notch (room for heart)
which lung is smaller
visceral - membrane on outside of lung
parietal - lines walls of thoracic cavity, diaphragm, mediastinum
---> both produce serous fluid
pleural cavity - space between (decrease friction during expan+recoil)
describe the pleura surrounding the lungs
- keeps membranes from separating
--> pulls lungs outward toward thoracic wall
--> opposes lung collapse
what is the purpose of high surface tension in pleural fluid
pressure in alveoli
- increases and decrease during breathing
- always equalizes w/ atm p
describe intrapulmonary pressure
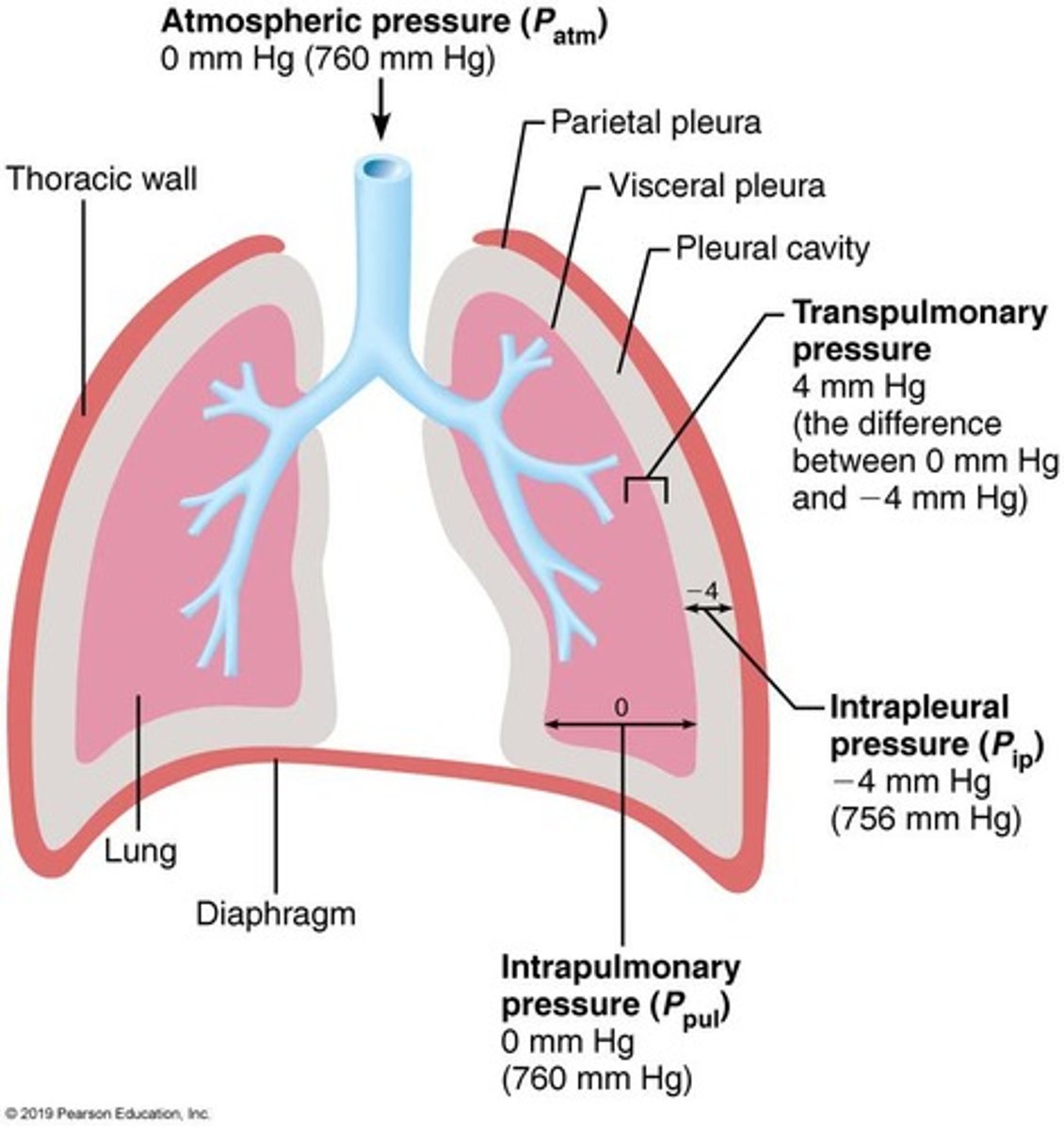
pressure in the pleural cavity
- increases/decreases during breathing
- always is 4 mm Hg LESS THAN intrapulmonary
- negative pressure
describe intrapleural pressure
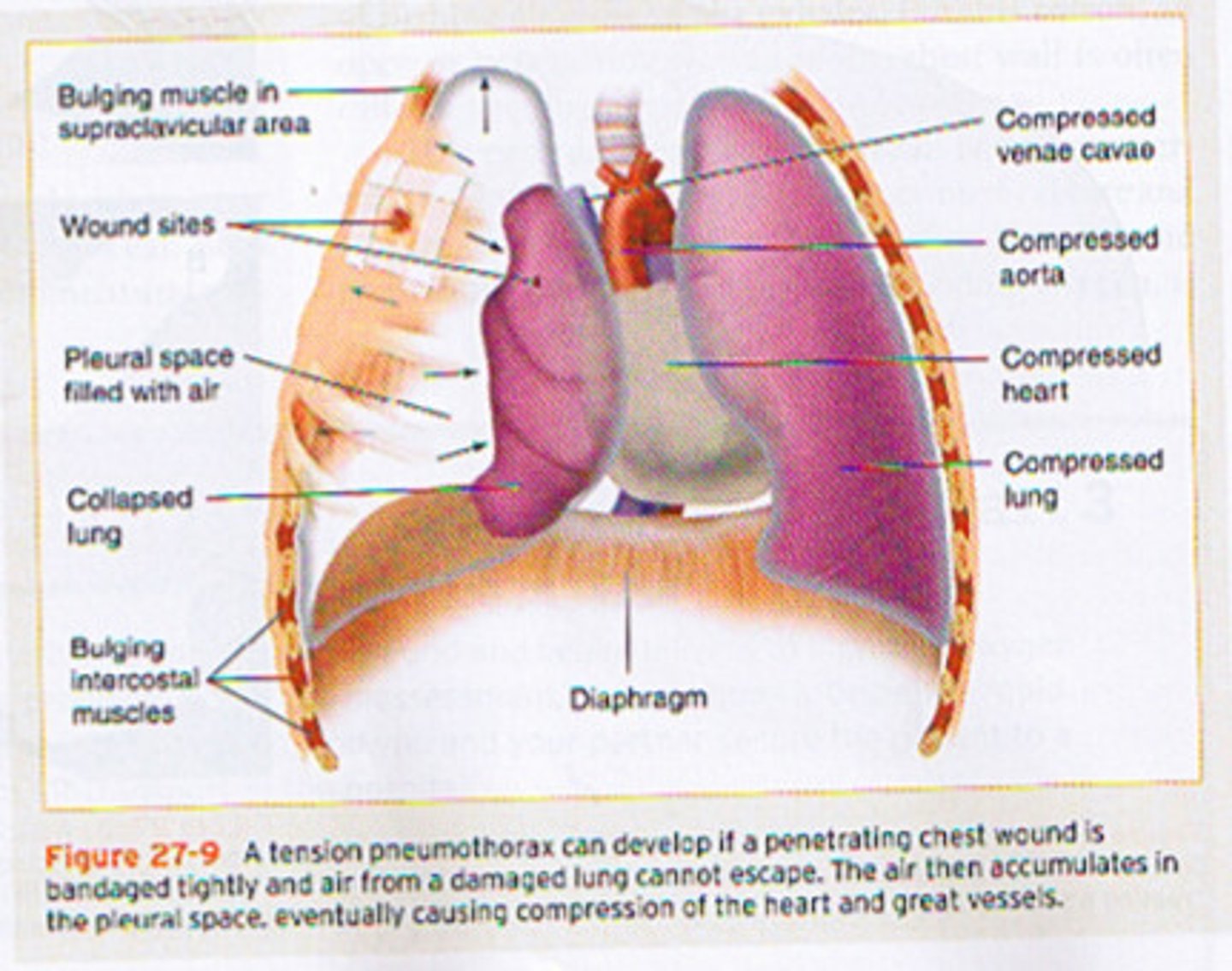
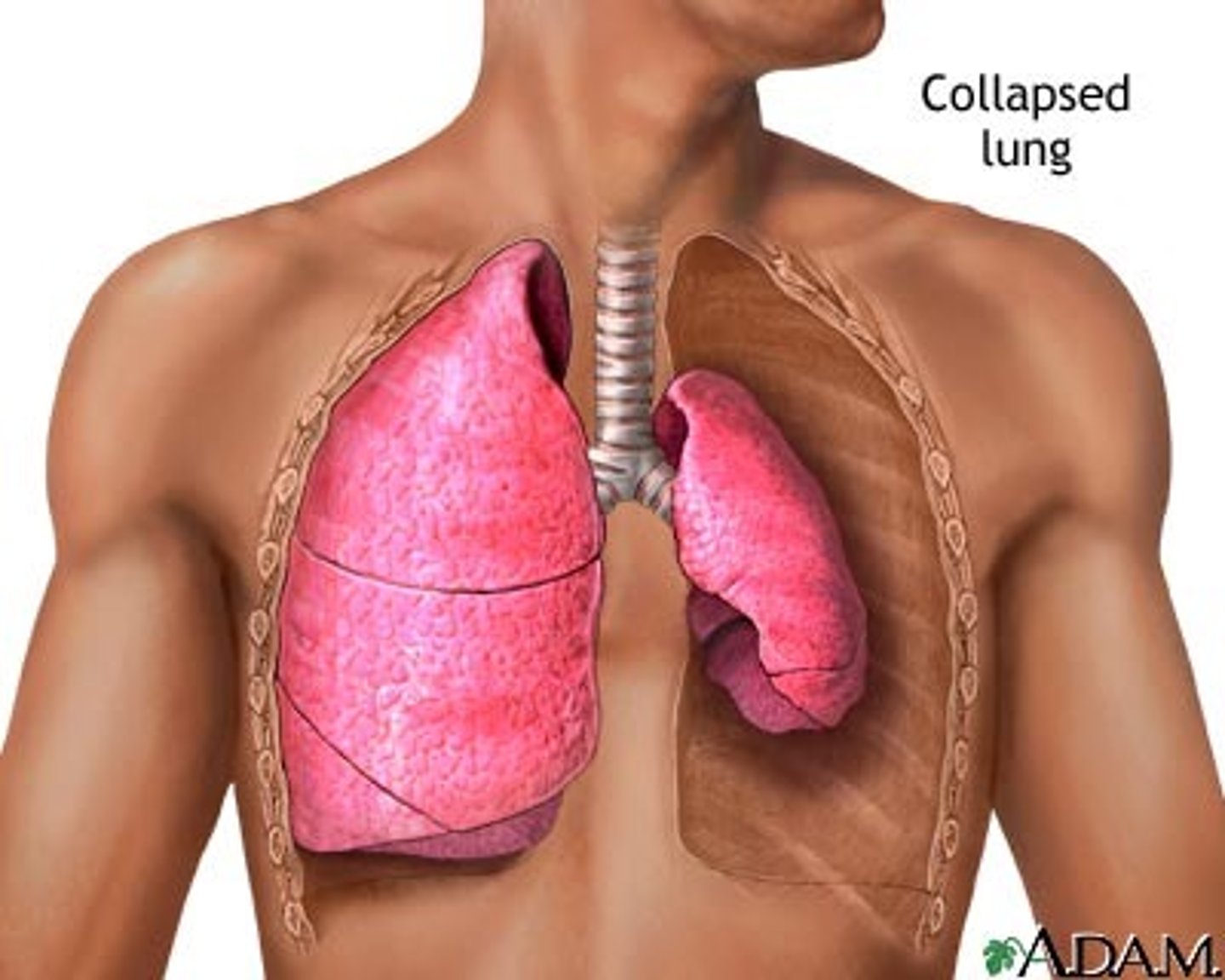
occurs when air enters the pleural cavity, causing loss of negative pressure and surface tension, which results in lung collapse
what is a pneumothorax
fancy word for collapsed lung
what is atelectasis
O2 poor blood leaves the heart through pulmonary arteries, goes to capillaries around alveoli where gas exchange occurs, and then returns oxygenated to the heart through pulmonary veins
blood supply to lungs: pulmonary circulation
aorta -> bronchial arteries: provide systemic blood to lung tissue (except alveoli)
bronchial veins -> azygous -> SVC -> RA
OR
bronchial veins -> pulmonary veins -> LA
Bronchial circulation delivers oxygenated blood from the aorta to nourish lung tissues, and the blood returns either to the right atrium through the azygos system or mixes with pulmonary venous blood going to the left atrium
blood supply to lungs: bronchial circulation
- mvmnt of air btwn the atm and alveoli
- gases move into/out of lungs based on pressure gradients that occur w/ changes in volume of thoracic cavity
- FLOW = P / R
describe ventilation (breathing)
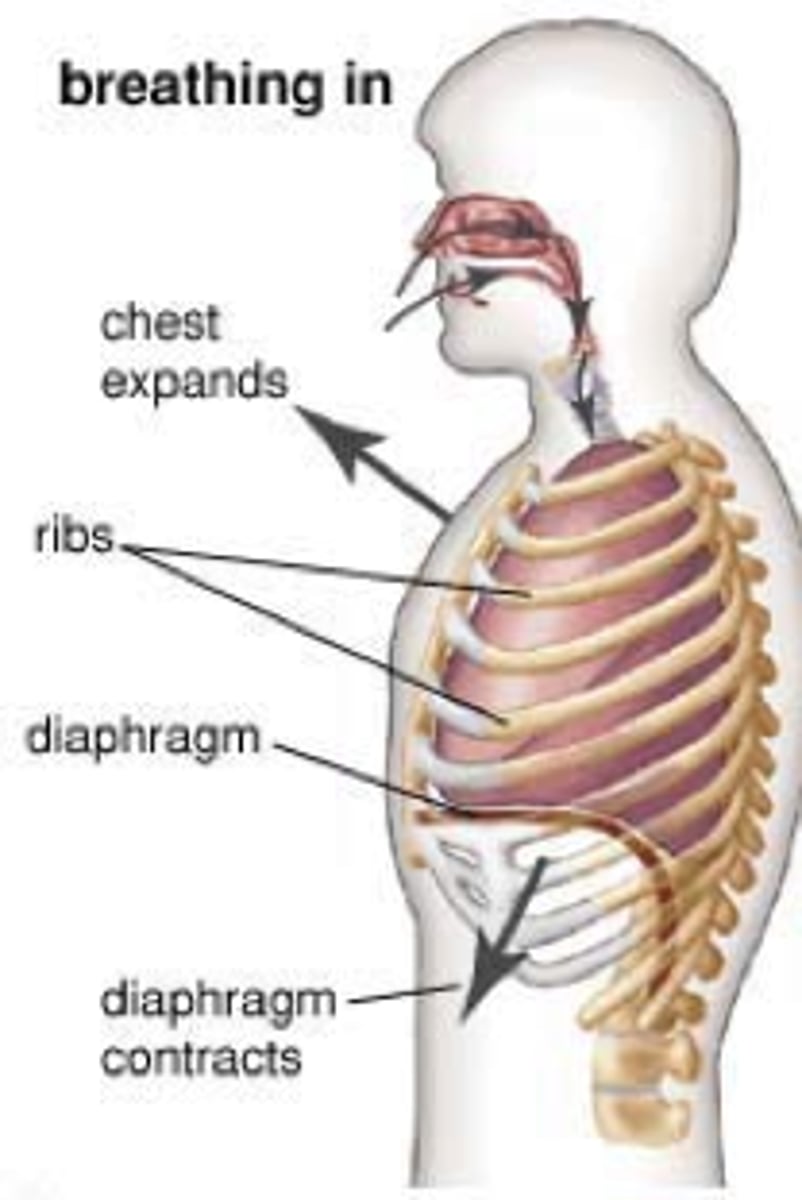
- P inside lungs must be less than atm P for air to flow IN
- thoracic volume increases
--> diaphragm : contracts and lowers floor (75%)
-->external intercostals: pull ribs up and out (25%)
- active process (req somatic motor neurons to stimulate skeletal contraction)
describe inspiration
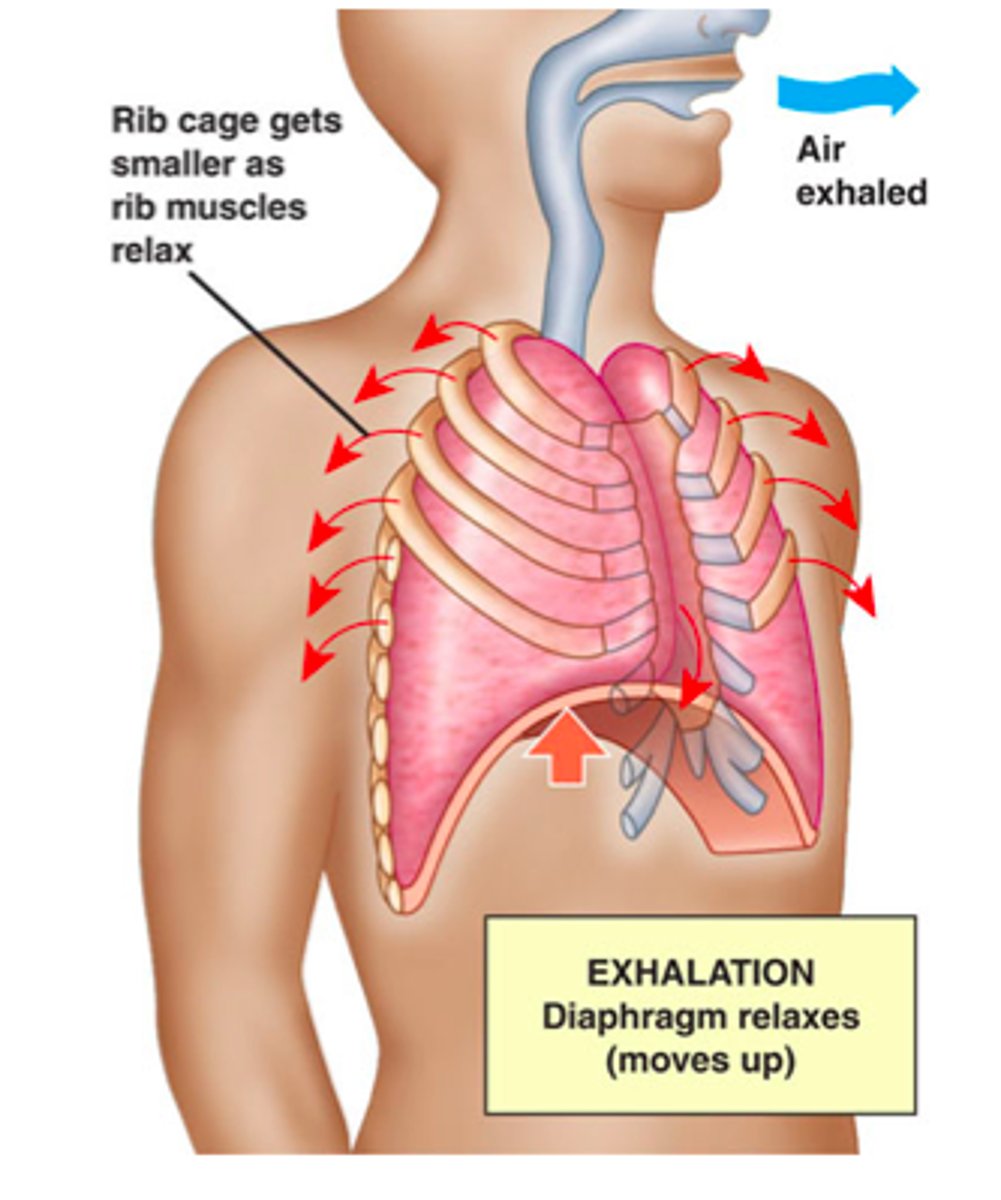
- P inside lungs must be greater than atm P for air to flow OUT
- thoracic volume decreases
--> inspiratory muscles relax
--> elastic recoil of lungs
- passive process
describe expiration
forced inspiration/expiration
- uses addtl muscles to increase/decrease thoracic volume and create larger pressure gradients
what is hyperpnea
- internal intercostals (pulls ribs down + inward)
- abdominal muscles (lowers ribs pulled down, abdominal organs pushed up)
what addtional muscles used for forced expirartion
- scalenes, pectoralis minor (pull ribs up)
- sternocleidomastoid (pull up on sternum)
- erector spinae (extension if vertebral column)
what addtional muscles used for forced inspiration
spirometer
what is used to measure air volume during breathing
compliance ( V/P)
how easily lungs can expand; depends on elasticity of lung tissue and thoracic cage & surface tension of alveoli
radius of airway
poiselle law (R = Lη/r4)
physical obstruction
bronchoconstriction/dilation
describe airway/ air flow resistance factors
RR = breaths per minute (avg is 12/min)
MV = RR x TV (12/min x 500mL = 6L/min)
what is respiratory rate and minute ventilation
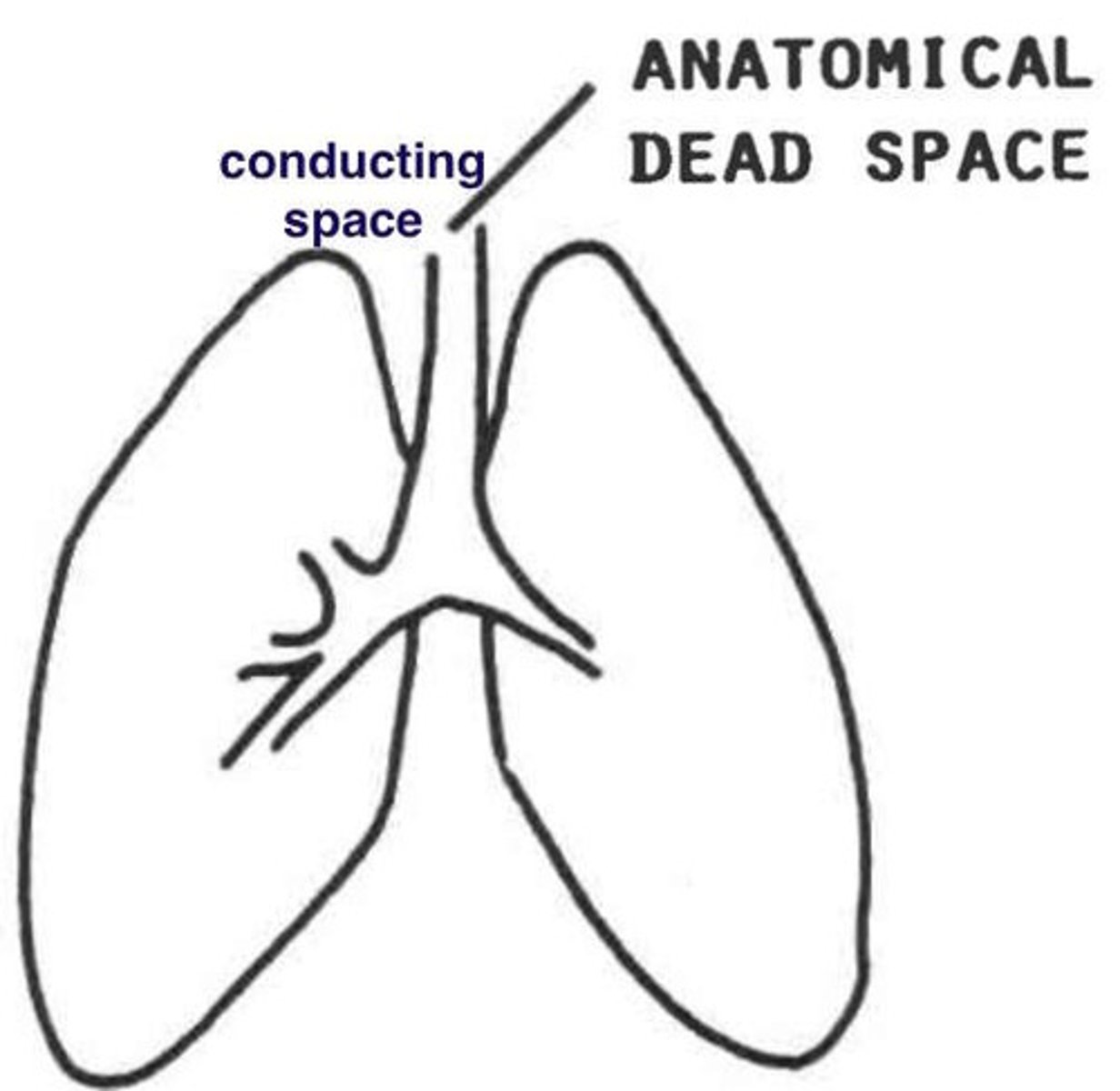
- conducting airways : no gas exchange is occurring
- approx 150mL
- not all inspired air reaches alveoli and involved in gas exchange
what is anatomic dead space
PV = how much air moves in/out of lungs
(breathing rate x Tidal volume)
AV = how much fresh air reaches alveoli
(breathing rate x (TV - dead space))
* rate and depth have large effects of AV
pulmonary vs alveolar ventilation
- pontine respiratory centers
- ventral respiratory group (VRG)
- dorsal respiratory group (DRG)
- phrenic nerve
name the respiratory centers in the brain stem
- control the rate and depth of breathing
--> basic and forced breathing patterns
function of respiratory centers in medulla oblongata
- inspiratory + expiratory neurons
- somatic motor neurons to inspiratory muscles
--> inhibited by expiratory neurons (from pontine resp group)
- somatic motor neurons to accessory muscles (for forced insp/exp)
describe the ventral respiratory group (VRG)
- receives peripheral sensory input & communicates w/ VRG
--> chemoreceptors
--> irritant receptors
--> stretch receptors
describe the dorsal respiratory group (DRG)
- located in the pons
- modifies rate and depth of breathing
- communication w/ VRG to help w/ transition btwn inhalation & exhalation
--> inspiration = 2 sec
--> expiration = 3 sec
--> resting breathing rate = 12-15 breaths/min
describe the pontine respiratory group
- responsive to changes in gases and pH in arterial blood
- carotid bodies
--> stimulated by inc pCO2, dec pH or dec pO2 (<60mmHg)
--> glossopharyngeal nerve (IX)
- aortic bodies
--> vagus nerve
describe peripheral chemoreceptors
- responsive to pH changes in CSF
--> stimulated by inc pCO2 which causes a dec in pH (increase H+)
describe central (medulla) chemoreceptors
negative feedback mechanisms:
1. increased arterial pCO2
2. decreases pH in brain ECF
3. central chemoreceptors respond to H+ in brain ECF
4. med resp centers -> resp muscles -> increase ventilation (more CO2 out)
5. arterial pCO2 and pH go back to normal
how does pCO2 regulate ventilation
central : mediates 70%
peripheral: mediates 30%
what is the percentage each chemoreceptor mediates the CO2 response
HYPER: increased arterial p CO2
HYPO: decreased arterial p CO2
hypercapnia vs hypocapnia
decreased oxygen availability to the tissues
5 types: anemic, ischemic, hypoxemic, histotoxic, CO poisoning
what is hypoxia
decreased RBCs; abnormal or decreased Hb
what is anemic hypoxia
impaired/blocked circulation
what is ischemic hypoxia
abnormal ventilation; pulmonary disease; low ambient air pO2 (high altitude)
what is hypoxemic hypoxia
cells unable to use O2, as in metabolic poisons (cyanide)
what is histotoxic hypoxia
200x greater affinity for Hb than O2
what is CO poisoning
hyperventilation is the increased depth and rate of breathing that exceeds body's need to remove CO2
--> increases RR in response to acidosis (ketoacidosis, lactic acidosis)
describe hyperventilation vs increased RR
hypoventilation is the decreased depth and rate that is inadequate to meet the body's need to remove CO2
--> decreases RR in response to metabolic alkalosis (vomiting, ingestion of excess antacids)
describe hypoventilation vs decreased RR
hyperventilation (increased pH levels and low CO2 levels)
respiratory alkalosis is caused by?
hypoventilation (decreased pH levels and high CO2 levels)
respiratory acidosis is caused by?
- stretch receptors in bronchi and bronchioles
- inhibition of inspiration
- prevents over-inflation of lungs w/ forced inspirations
describe the inflation hering-breuer reflex
- receptors in alveolar wall
- as lung vol decreases w/ forced expirations, expiratory centers inhibited, inspiratory centers stimulated
describe the deflation hering-breuer reflex
- primary motor cortex
- stimulates somatic motor neurons
- limited conscious control (cant override chemorecptor influences)
describe cerebral dominance role in controlling respiration
emotions may affect breathing rate & depth via ANS
- sympathetic: bronchodilation ; increase RR
- parasympathetic: bronchoconstiction; decrease RR
describe limbic system role in control of respiration
- hypothalamus: body temp effects (thermoregulation)
- irritant receptors in airways: bronchoconstriction, parasym mediated
- sneezing: irritant in nasal cavity
- coughing: irritant in larynx, trachea, bronchi
describe other controls of respiration
- decreased in lung compliance
- increase in resistance to air flow
- decreased respiratory function
effects of age on the respiratory system
- cilia is paralyzed/destroyed
- bronchial irritation and inflammation
- breakdown of elastin in CT of lungs
effects of smoking
- bronchial edema
- chronic productive cough
- bronchospasm
effects of chronic bronchitis
- destruction of alveolar walls
- loss of lung elasticity
- air trapping
effects of emphysema
- nasal hairs
- tears drainage
- mucous secretion (trap debris, lysozyme, defensins, IgA)
- turbulent flow in nasal cavity (nasal conchae)
- cilia
- macrophages
list the defenses of respiratory system
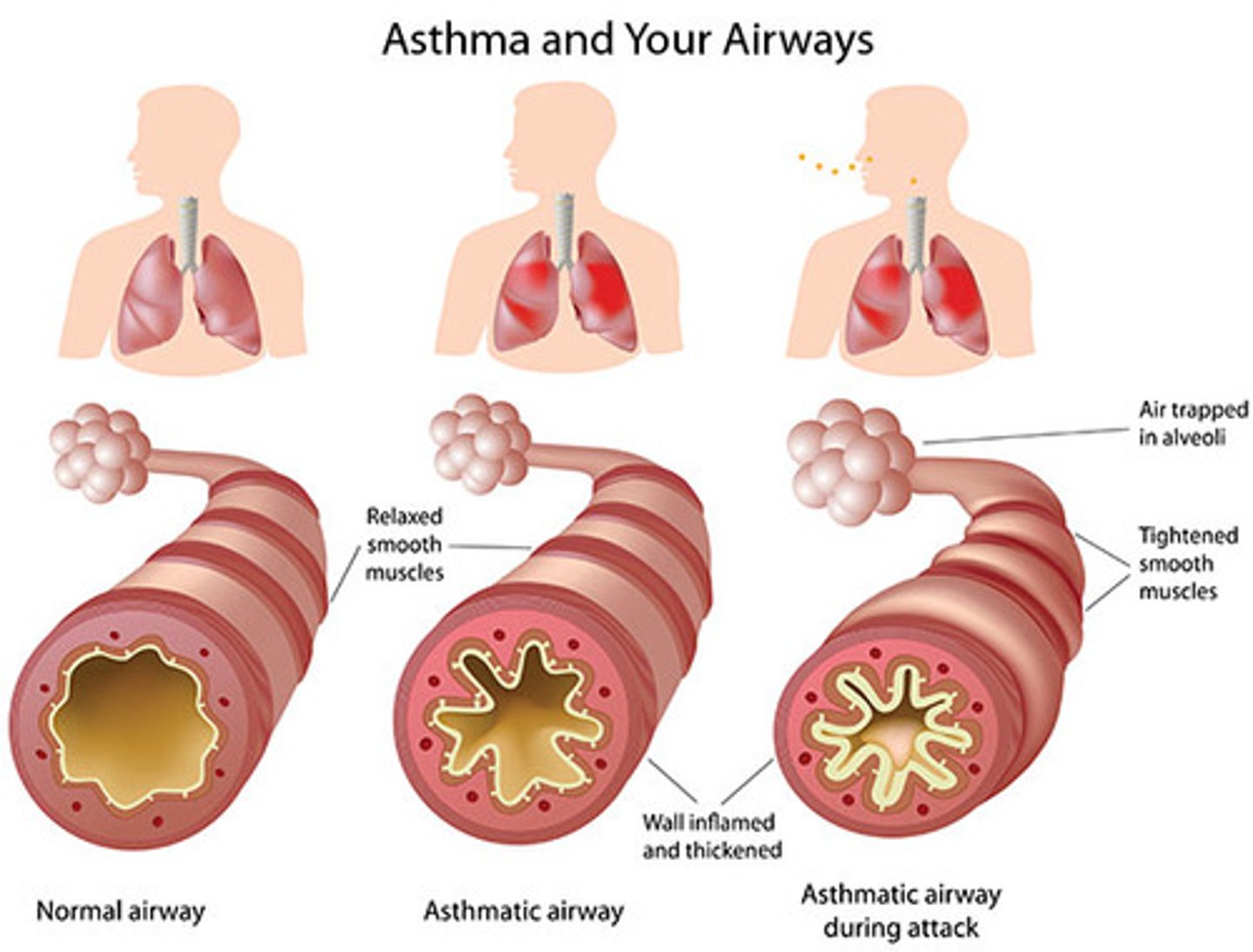
- chronic airway inflammation due to hypersensitivity to a variety of stimuli
--> allergens, emotional, exercise, cold air, cigarette smoke, etc
- airway obstruction: increased mucous secretion and bronchospams
descirbe asthma
- narrowing due to atherosclerotic plaque
- increase resistance and decrease blood flow
- increases arterial pressure
- increase in net filtration pressure
--> higher pressure increases capillary hydrostatic pressure, which is the primary driver of net filtration in the lungs
describe atherosclerosis of pulmonary artery
- bacterial infection (mycobacterium tuberculosis)
- macrophages, lymphocytes, and fibroblasts aggregate to form granulomas
--> latent: doesn't grow, cant spread, no symptoms
--> active: causes symptoms, can spread and lead to death
* can become active due to stress & weak immune system
describe tuberculosis
- uncontrolled cell growth of abnormal epithelial and/or glandular cells
- various types: most often caused by smoking (carcinogens)
describe lung cancer
80-90% of lung cancers
- inhaled air is drier and contaminated
- nicotine : constricts terminal bronchioles (dec airflow)
- CO: binds to Hb (dec o2 carrying capacity)
- irritants: inc mucus, swelling of mucosal lining, destroy cilia
- chronic use: destruction of elastic fibers (emphysema-trapped air)
describe the effects of smoking
- premature newborns (before 28 week gestation)
- alveolar collapse due to lack of surfactant
- symptoms: labored & irregular breathing
--> flaring of nostrils during inhalation
--> grunting during exhalation
--> bluish skin color (decreased O2)
describe respiratory distress syndrome
between alveoli and blood (alveolar gas exchange)
location of diffusion of gases during external respiration
between cells and blood (systemic gas exchange)
location of diffusion of gases during internal respiration
- concentration gradient (partial pressure gradient)
--> daltons law
- distance, size, solubility, temp, surface area
- solubility in plasma
--> henry's law : the higher the pressure, the greater amount of gas into solution (vice versa)
what are some diffusion factors
pp = % of gas x 760 mmHg
atmospheric pressure is 760 mmHg and each gas contributes a % of that
(daltons law)
how to calculate partial pressure
arterial
- pO2 = 95 mmHg
- pCO2 = 40 mmHg
- pH = 7.4
venous
- pO2 = 40 mmHg
- pCO2 = 46 mmHg
- pH = 7.37
normal blood values
in alveoli pO2 is high (about 104 mmHg)
in deoxygenated blood entering the lungs pO₂ is low (about 40 mmHg)
- O2 diffuses from alveoli into blood (high to low)
in the blood arriving at the lungs pCO₂ is high (about 45 mmHg)
in the alveoli pCO₂ is lower (about 40 mmHg).
- CO2 diffuses from the blood into the alveoli
explain external (alveolar) gas exchange using partial pressure gradients for CO2 and O2.
in the blood (coming from the lungs): high pO₂ (95 mmHg)
in the tissues (cells): low PO₂ (~40 mmHg or less)
- O2 diffuses from the blood into the cells
in the tissues (cells): high pCO₂ (45 mmHg)
in the blood: lower pCO₂ (40 mmHg)
- CO₂ diffuses from the cells into the blood
Explain internal (systemic) gas exchange using partial pressure gradients for CO2 and O2.
0.25 seconds ( total is 0.75 seconds)
- oxygen reserve time
- ensure efficient gas exchange under stress or impairment
functional significance of the time it takes for oxygenation of blood in the pulmonary capillaries at rest
- dissolved in plasma (2%)
- bound to hemoglobin (98%)
--> HbO2
--> % saturation of Hb - amount of O2 bound (dependent on pO2, pH, temp, metabolic activity)
how is oxygen transported in the blood
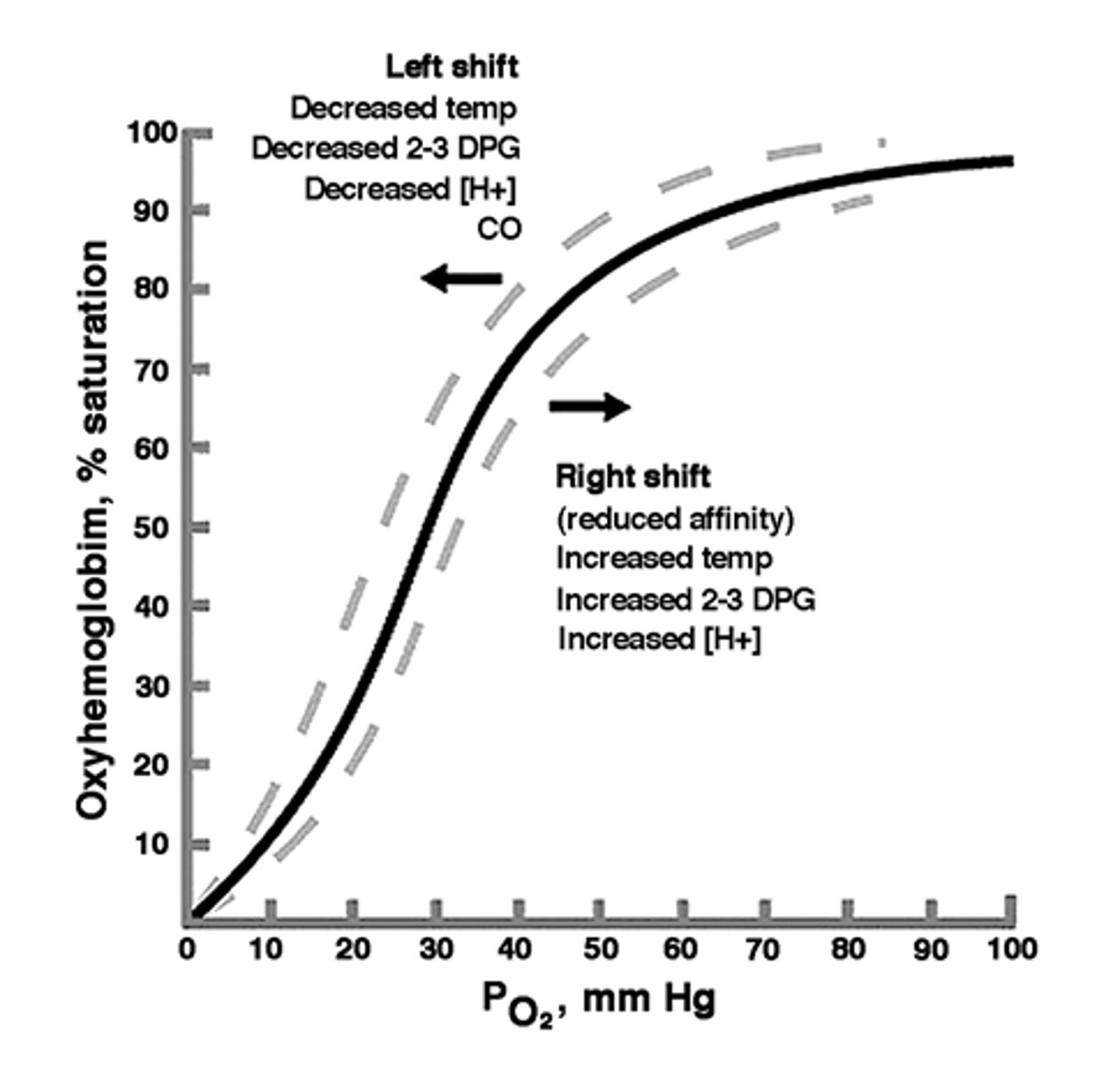
- not linear: refleccts affinity differences w/ changing pO2
- greater than/equal 60 mmHg : near max saturation
- at 40 mmHg (resting) : 75% saturation
- less than 40 mmHg: increased unloading from Hb
describe the oxygen-hemoglobin dissociation curve
increase of pO2 increases %Hb saturation
decrease of pO2 decreases %Hb saturation
how does increase/decrease in pO2 affect % O2 sat of Hb
increase of pCO2 decreases % saturation (rightward shift)
decrease of pCO2 increases % saturation (leftward shift)
how does increase/decrease in pCO2 affect % O2 sat of Hb
increase of pH increases % saturation (leftward shift)
decrease of pH decreases % saturation (rightward shift)
how does increase/decrease in pH affect % O2 sat of Hb
increase of temp decreases % saturation (rightward shift)
decrease of temp increases % saturation (leftward shift)
how does increase/decrease in temp affect % O2 sat of Hb
increase of 2,3-DPG decreases % saturation (rightward shift)
decrease of 2,3-DPG increases % saturation (leftward shift)
how does increase/decrease in 2,3-DPG affect % O2 sat of Hb
- formed by RBCs during glycolysis (anaerobic metabolism)
- increased in hypoxic conditions (high altitude, anemia)
- decreases binding of O2 to Hb and increases unloading of O2
what is 2,3-DPG
- dissolved in plasma (7%)
- bound to hemoglobin (23%)
- HCO3- (70% as bicarbonate ion)
how is CO2 transported in the blood
- the lower the pO2, the more CO2 carried in the blood in the form of HbCO2
- high pO2 results in more CO2 dissolved in plasma
what is haldane effect
- fetal has higher affinity for O2
--> important for moving O2 from placenta to fetal tissues
fetal vs adult Hb
Still learning (28)
You've started learning these terms. Keep it up!