Hereditary endocrine tumor syndromes
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
Components of the endocrine system
Pituitary gland
Thyroid
Parathyroid glands
Adrenal glands
Pancreas
Kidneys
Pituitary gland
- size of a pea and sits behind the nose and below the base of the brain
- secretes several hormones (**TSH, ACTH, prolactin)
Thyroid
- size of a quarter on the neck with left and right lobes
- secretes thyroid hormone and calcitonin (regulates calcium levels and decrease blood calcium levels)
Parathyroid glands
- 4 embedded in the back of the thyroid
- regulate blood calcium levels and increase blood calcium levels
Adrenal glands
- located above the kidneys
- secrete cortisol, aldosterone, androgens, and cateholamines
Common tumors of the adrenal glands
- Adrenal cortical carcinoma
- Adrenal cortical adenoma
- Tumor of the adrenal medulla
Pancrease
- regulates blood sugar levels (endocrine) and aids in digestion (exocrine)
- secretes insulin, glucagon, gastrin, VIP
Pancreatic neuroendocrine tumors (PNET)
- benign or malignant
- arise in hormone-producing cells of the pancreas
Syndromes associated with increased endocrine tumor risk
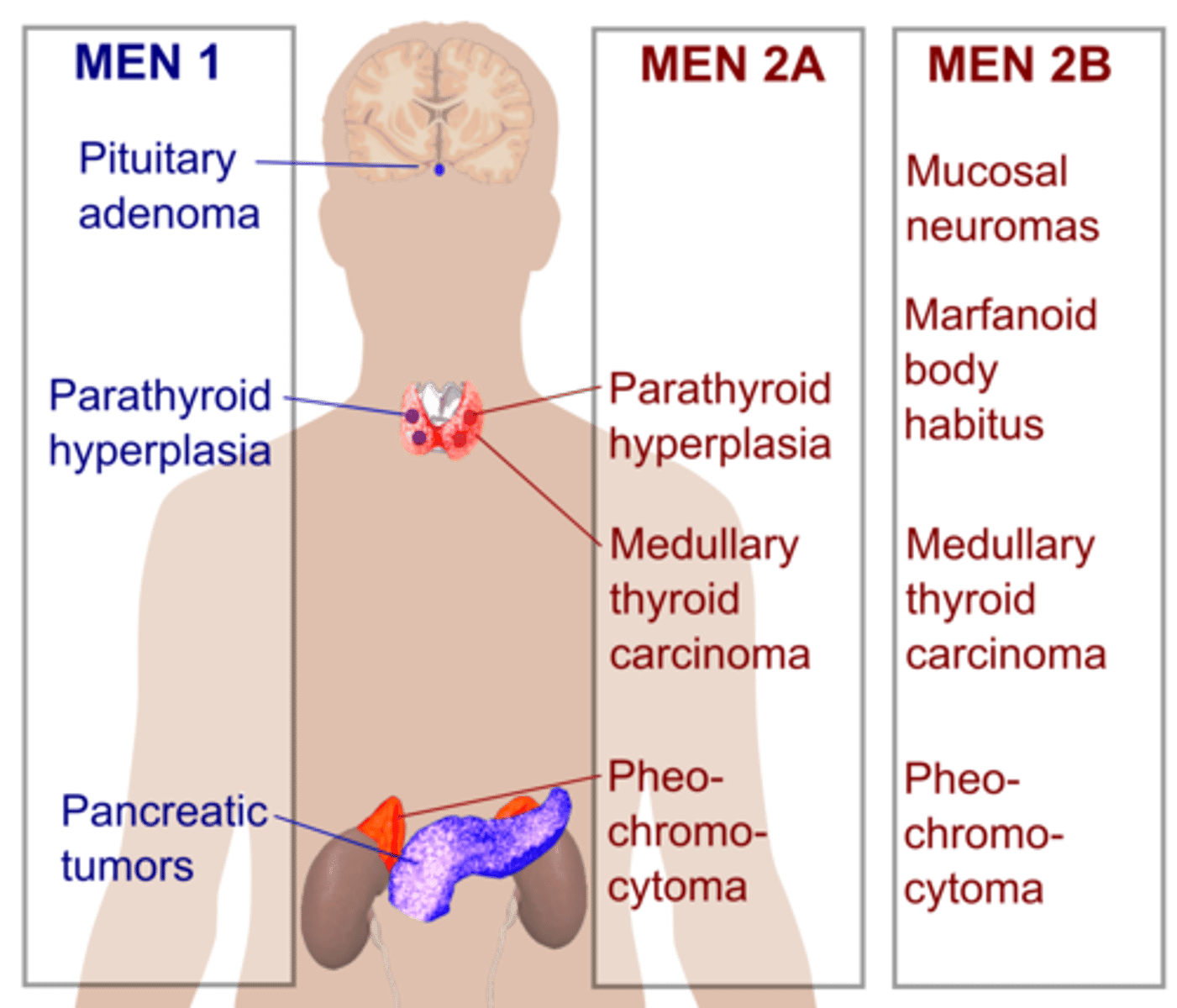
MEN1
MEN2
Multiple endocrine neuplasia type 1 (MEN1)
- MEN1 gene
- tumor suppressor gene producing menin
- clinical diagnostic criteria
**if you meet clinical diagnostic criteria, you will probably meet insurance guidelines for coverage for germline genetic testing
Clinical diagnostic criteria for MEN1
Presence of TWO endocrine tumors from the following THREE sites:
1) parathyroid glands
2) pituitary glands
3) GEP (gastro-entero-pancreatic tract)
**clinical diagnoses are made prior to genetics
MEN1 parathyroid involvement
- hyper-parathyroidism
- elevated blood calcium level (PTH level often elevated as well)
MEN1 pituitary involvement
- anterior pituitary tumors (30-40%)
**most common is prolactinoma (can cause oligomenorrhea/amenorrhea, sexual dysfunction, gynecomastia)
MEN1 GEP tract involvement
- gastrinomas/ZES (40%) in the duodenum or sometimes pancreas
- causing upper-abdominal pain, diarrhea, esophageal, reflux, ulcers
**80% patients with MEN1 have GEP tract involvement
MEN1 features
- parathyroid, anterior pituitary, or well-differentiated endocrine TUMORS
- benign skin tumors, adrenal cortical tumors, carcinoid tumors, phenochromocytomas (adrenal medulla)
MEN1 clinical management
- yearly biochemical investigations (5)
- head MRI every 3-5 years (5)
- abdominal CT or MRI every 3-5 years (20)
- annual chest CT, SRS, octreotide scan
- discuss prophylactic thymectomy, parathyroidectomy surgery, medication for other organs based on family history
Multiple endocrine neoplasia type 4 (MEN4)
- CDKN1B gene
- clinically indistinguishable from MEN1
**full phenotypic spectrum not currently known
**if you are worried about MEN1, you BETTER test BOTH MEN1 gene and CDKN1B gene
Multiple endocrine neoplasia type 2 (MEN2)
- RET gene (proto-oncogene with GAIN OF FUNCTION)
- 3 clinical subtypes: MEN2A, MEN2B, FMTC
RET GOF Mutation
Constitutive activation and dimerization of RET causes tumorigenesis via unregulated activation of the MAPK, P13K/AKT, JAK2/STAT3, and PLCy pathways
**activation of proto-oncogenes can result in the production of proteins that drive cell division, inhibit apoptosis (programmed cell death), or promote angiogenesis (the formation of new blood vessels)
MEN2 clinical features
- medullary thyroid cancer
- pheochromocytoma (nerve sheath tumors on the adrenal glands)
- hyperparthyroidism
Most common type of thyroid cancer
Papillary
Rarest type of thyroid cancer
Medullary thyroid cancer (aggressive, deadly)
**IMMEDIATELY think MEN2
Most common form of MEN2
MEN2A
Clinical diagnostic criteria for MEN2A
2+ specific endocrine tumors:
1) medullary thyroid cancer (95%)
2) pheochromocytoma
3) parathyroid adenoma/hyperplasia
MEN2B is characterized by ____
- early and very aggressive medullary thyroid cancer (100%)
- risk for pheochromocytomas
- smaller risk for parathyroid hyperplasia and adenomas
- characteristic facial features (mucosal neuromas on the tongue/palate, progressive thickening of the lips, neuromas on the eye lids, marfanoid habitus, ganglioneuromatosis of the GI tract)
**way less common than MEN2B
**50% de novo
MEN2 management
- genetic testing of proband and all at-risk family members (by age 5)
- prophylactic thyroidectomy with autotransplant of the parathyroid glands (5)
- annual screening for pheo through blood work, imaging (8-20)
- annual screening for parathyroid disease through biochemical testing (8-20)
Familial medullary thyroid cancer (FMTC)
- considered a sub-type of MEN2A
- no pheo/parathyroid hyperplasia
- medullary thyroid cancer (later onset, decreased penetrance)
**strict clinical criteria so pheochromocytoma risk is not erroneously missed
RET mutations in apparently sporadic MTC
Germline mutation in RET gene found in ~7% of medullary thyroid cancers with no family history or MEN2 features
**RET gene testing should be offered to any patient with medullary thyroid cancer
MEN1 vs MEN2
PGL
Paraganglioma
PCC
Pheochromocytoma
Hereditary PGL-PCC
- SDHx, MAX, TMEM127 genes
- tumors of neuroendocrine tissue in central core from base of skull to pelvis and tumors of the adrenal medulla
**suspected in any individual with PGL or PCC
Paragangliomas (PGL)
Tumors in neuroendocrine tissue in central core from base of skull to pelvis which may secrete catecholamines and metanephrines
Pheochromocytomas (PCC)
Paragangliomas in the adrenal medulla that, typically, are secretory
Clinical diagnostic criteria for PGL-PCC
Multiple PGL/PCC (especially if bilateral!)
- multifocal, with multiple synchronous or metachronous tumors
- recurrent
- early onset (<45y)
- extra-adrenal
- metastatic
**may also include pulmonary chondromas, RCC, oncocytic neoplastic kidney tumors, papillary thyroid cancer, pituitary adenomas, GISTs
Most common genes associated with PGL-PCC
SDHB
SDHD
**panel testing is key unless a familial variant is known
**there is variable penetrance
PGL-PCC mnemonic
SDHB = Bad (more likely to become malignant)
SDHD = Dad (POI - paternal)
SDHC = Cyst (rhymes with GIST)
SDHA = All of the above ^^^
POI Inheritance
This is an imprinting thing (think about inheriting vs expressing)
PGL-PCC medical management
- annual blood analysis for biochemical markers
- whole body MRI every 2 years
- endoscopic eval for GIST
- avoid cigarette smoking, high altitude, extreme physical exertion
**begin surveillance between ages 6-10 years
Pre-appointment endocrine genetic counseling considerations
- was any IHC tumor testing done?
- referral/specialist notes...what are patients symptoms?
- any known familial variant?
During appointment endocrine genetic counseling considerations
- medical history and family history should be tailored (pheos/paras/MEN1/2)
- appropriate test (panel vs targeted)
- psychosocial considerations (impact for family members, complexity of inheritance patterns, MEN2 subtybes, age of onset)