NURS 444 Heart Rhythms & EKG interpretation
1/114
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
115 Terms
what is the sequence in which electrical conduction travels through the heart?
SA node, AV node, bundle of his, bundle branches, purkinje fibers
P wave on the EKG represents what?
atrial depolarization/contraction
PR segment on the EKG represents what?
AV node delay in conduction
QRS complex on the EKG represents what?
conduction from the bundle of his/branches/purkinje fibers, causing ventricular depolarization/contraction
T wave on the EKG represents what?
ventricular repolarization
cardiac output is determined by?
heart rate x stroke volume
each small box on the EKG represents _____ seconds. Each large box on the EKG represents _____ seconds. 5 large boxes on the EKG represents _____ seconds
0.04, 0.20, 1
what is the expected range of time for the PR interval
0.12-0.20s or 3-5 small boxes
what is the expected range of time for the QT interval
0.33-0.43s or 8-11 small boxes
what is the expected range of time for the P wave
0.12s or <3 small boxes
what is the expected range of time for the QRS complex
0.06-0.11s or <3 small boxes
what is the expected range of time for the R-R interval
0.60-1.00s or 3-5 large boxes
amplitude (height/voltage): 1 small box equals _____ mV and 1 large box equals _____ mV
0.1, 0.5
what is the expected amplitude/height/voltage of the R wave
>0.5 or >1 large box
what is the expected amplitude/height/voltage of the T wave
>0.05, upright
what is the 5 step EKG analysis in order?
HR, regularity, P waves, PR interval, QRS width
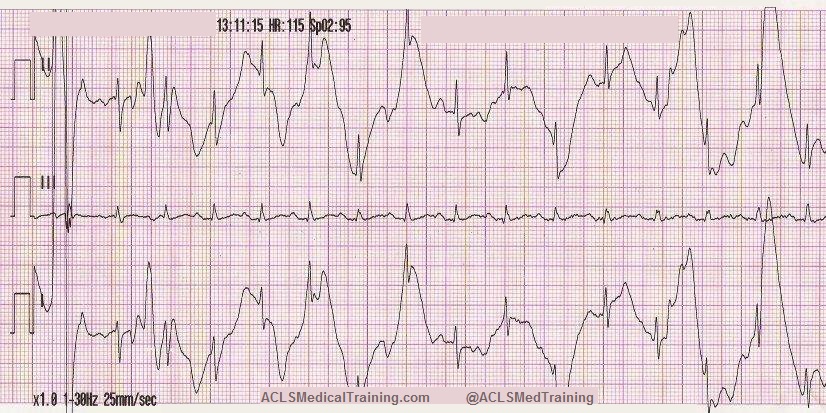
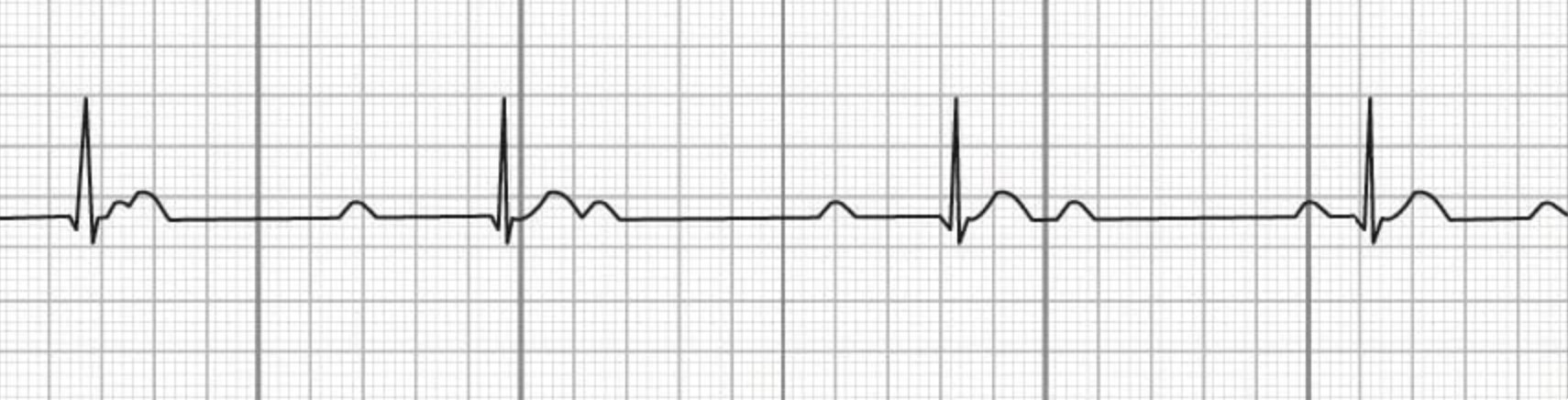
this EKG strip is showing what rhythm?
artifact
how do you use the 6-second strip method to determine HR? (when HR is regular)
the number of QRS complexes x 10
how do you use the large box method to determine HR? (when HR is regular)
300 divided by the number of large boxes between an R-R interval
how do you use the small box method to determine HR? (when HR is regular)
1500 divided by the number of small boxes between an R-R interval
HR regularity patterns: a regular HR is characterized by:
consistently equal R-R intervals
HR regularity patterns: a regularly irregular HR is characterized by:
irregular R-R intervals that follow a pattern of irregularity
HR regularity patterns: an irregularly irregular HR is characterized by:
irregular R-R intervals that do not follow a pattern of irregularity
what is the determining factor for when a heart rhythm becomes dangerous?
when it affects cardiac output and becomes symptomatic
what EKG abnormalities are consistent with HYPOkalemia? (K+ < 3.5)
flat/inverted T waves, prominent U waves, ST depression
what dysrhythmias is a patient at risk for developing with HYPOkalemia? (K+ < 3.5)
PVCs, PACs, torsades, Vfib
when a patient is experiencing a dysrhythmia consistent with HYPOkalemia (K+ < 3.5), what are the appropriate nursing actions/tx?
replace K+, continuous monitoring, hold digoxin
what EKG abnormalities are consistent with HYPERkalemia? (K+ > 5.5)
peaked t waves, wide qrs, sine wave, asystole
what dysrhythmias is a patient at risk for developing with HYPERkalemia? (K+ > 5.5)
bradycardia, heart block, Vfib, asystole
when a patient is experiencing a dysrhythmia consistent with HYPERkalemia (K+ > 5.5), what are the appropriate nursing actions/tx?
calcium gluconate, bicarb, insulin + dextrose, kayexalate, dialysis
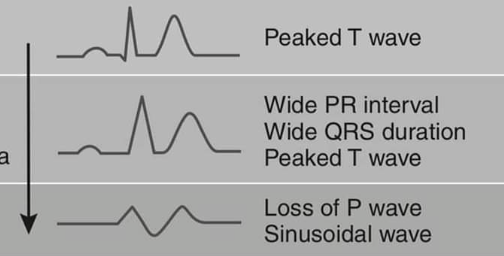
the image shown depicts progressive EKG abnormalities that are consistent with what condition?
hyperkalemia
what EKG abnormalities are consistent with HYPOmagnesemia? (Mg2+ < 1.7)
prolonged QT, wide QRS, flat T waves
what dysrhythmias is a patient at risk for developing with HYPOmagnesemia? (Mg2+ < 1.7)
torsades, PVCs, Vfib
when a patient is experiencing a dysrhythmia consistent with HYPOmagnesemia (Mg2+ < 1.7), what are the appropriate nursing actions/tx?
IV mag sulfate
what is the order of nursing actions/tx to respond to a patient in torsades de pointes?
give IV mag sulfate, check mag and K+ levels, identify and stop QT prolonging drug
what is the tx in order for symptomatic/unstable bradycardia requiring intervention?
IV atropine, transcutaneous pacing, transvenous pacing, treat underlying cause
what is the tx in order for symptomatic/unstable tachycardia requiring intervention?
identify and treat the cause
the image shown depicts what cardiac arrhythmia?
atrial fibrillation
complications of Afib include:
blood clot, stroke, HF from loss atrial kick (decrease in CO)
pharmacological management of rate control in afib includes:
metoprolol, diltiazem, digoxin
long term pharmacological management of afib includes:
rate control: BBs, non-dhp CCBs. rhythm control: amiodarone, flecainide, ablation. anticoag: apixaban, warfarin
what interventions are appropriate for unstable afib?
anticoagulants if >48hrs then synchronized cardioversion 120-200 J biphastic
if a patient has ubstable NEW onset afib, cardioversion can be initiated without anticoagulant therapy. if the patients afib has lasted >_____, you must ______ prior to cardioversion, unless hemodynamically unstable, due to risk of stroke.
48hrs, initiate anticoagulant therapy first
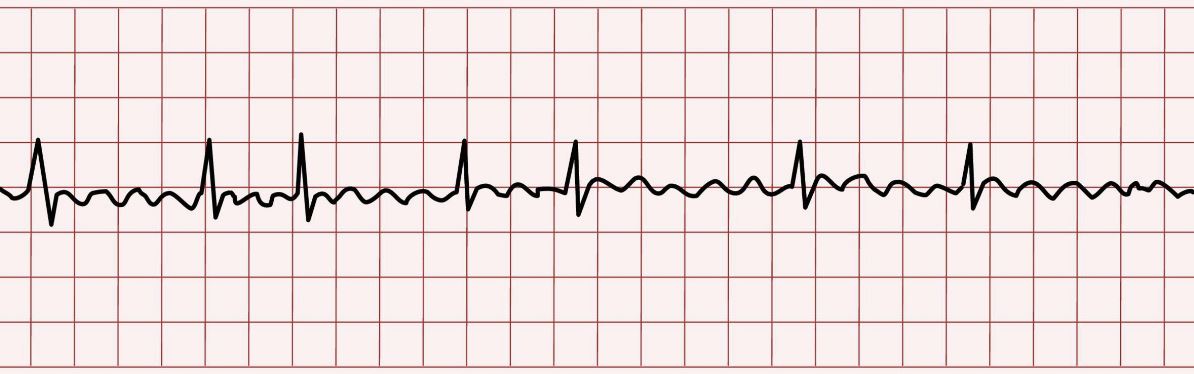
the image shown depicts what cardiac arrhythmia?
atrial flutter
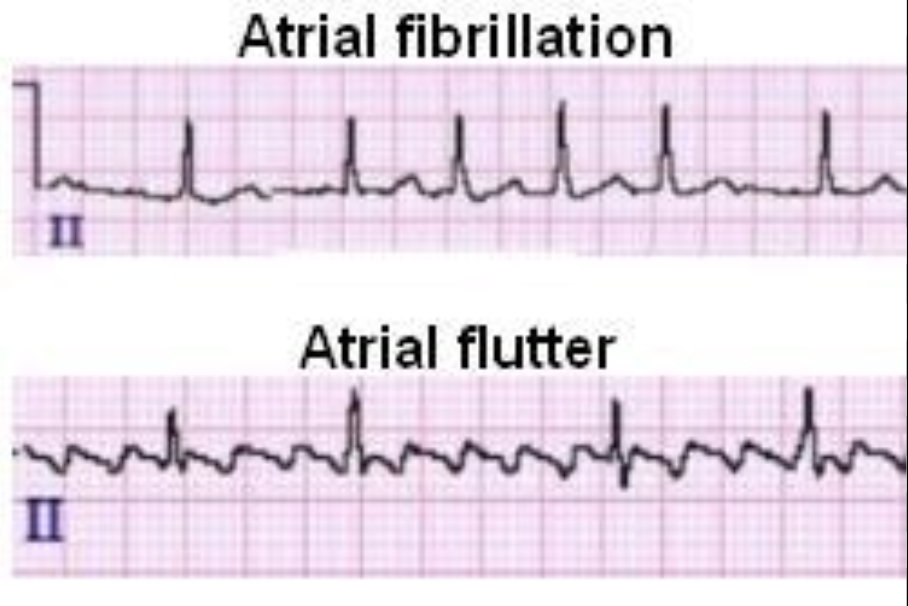
what distinguishing factors set atrial fibrillation apart from atrial flutter on an EKG?
afib: irregularly irregular, fibrillary pattern. aflutter: regular or regularly irregular, sawtooth pattern
atrial _____ is more responsive to cardioversion than atrial _____
flutter, fibrillation
atrial flutter: what is the key finding of atrial and ventricular rate?
atrial 250-350, ventricular often 150 (2:1)
treatment of aflutter is largely similar to the treatment of _____
atrial fibrillation
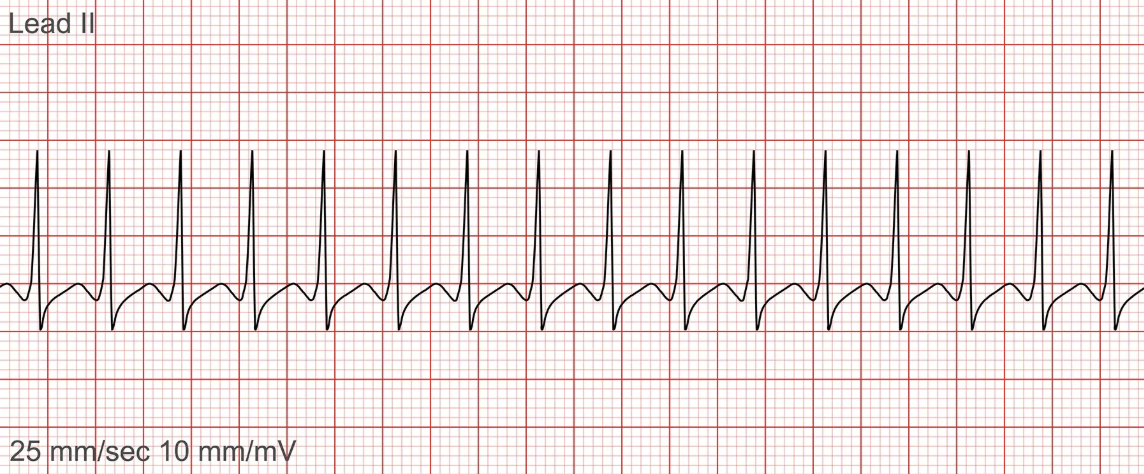
the image shown depicts what cardiac arrhythmia?
paroxysmal supraventricular tachycardia (PSVT)
what is the key finding for ecg abnormalities that identifies PSVT?
sudden onset of regular narrow complex tachycardia, abrupt start and stop, P waves not visible before QRS, rate often 150-250
what is the stepwise treatment for stable PSVT?
vagal maneuver, adenosine, diltiazem or metoprolol IV, catheter ablation for long term
what is the treatment for unstable PSVT?
synchronized cardioversion
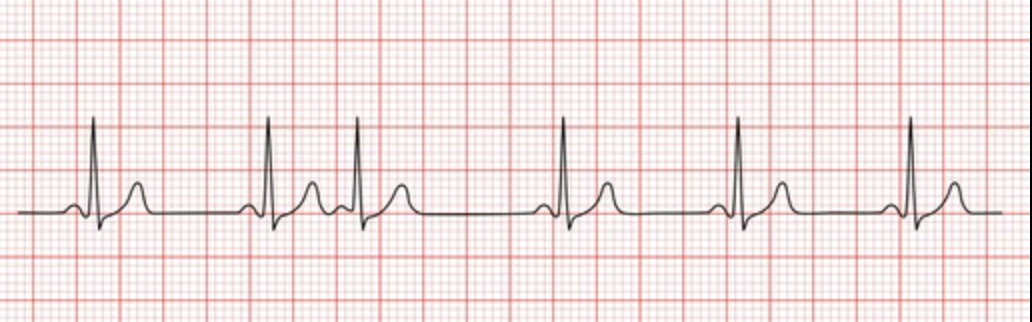
the image shown depicts what cardiac arrhythmia?
premature atrial contraction (PAC)
what is the key finding in ecg abnormalities that identifies PACs?
R-R is irregular, p waves are present before every QRS but irregular in rate and morphology followed by partial compensatory pause
when are PACs dangerous?
>6/min, couplets/runs >3, post-MI, symptomatic, frequent PACs are precursor to afib
what is the stepwise treatment for PACs?
treat the underlying cause and reduce triggers, beta blockers for symptomatic frequent PACs, monitor for progression to afib

the image shown depicts what cardiac arrhythmia?
premature ventricular contraction (PVC)
what is the key finding in ecg abnormalities when identifying PVCs?
wide/bizarre shaped QRS occurring early without preceding p wave followed by full compensatory pause
when do PVCs become dangerous?
>6/min, bigeminy (ever other beat), trigeminy (after every third beat), couplets (2 in a row), runs of 3 or more precursor to Vtach, r on t phenomenon may trigger vtach.
what is the stepwise plan of care for managing PVCs?
correct mag and/or K+, stop offending agents, beta blockers for frequent symptomatic PVCs, amiodarone only for structural heart disease, ablation for refractory symptomatic PVCs
what is the appropriate action for PVCs in acute MI?
notify provider immediately
what is the most dangerous PVC pattern and why?
r on t phenomenon may trigger vtach
what are the shockable rhythms?
vtach with pulse, vfib
the image shown depicts what cardiac arrhythmia?
ventricular tachycardia
cardioversion vs defibrillation: _____ is an electrical shock given to a patient who DOES have a pulse for the purpose of correcting an arrhythmia (back to sinus rhythm), and is given during the R wave
cardioversion
cardioversion vs defibrillation: _____ is an electrical shock given to a patient who DOES NOT have a pulse for the purpose of resetting the heart, used in Vfib or pulseless Vtach, and is not given at a specific time (should be done immediately)
(note: this info is tue in NCLEX world. in the real world, and for the purpose of NURS 444 exams, no pulse = no shock. start CPR!)
defibrillation
when does vtach become dangerous? (note: its always dangerous until proven otherwise)
SBP<90, altered LOC, chest pain, poor perfusion, no pulse
what is the treatment for stable ventricular tachycardia with a pulse?
IV amiodarone OR synchronized cardioversion
what is the treatment for UNstable ventricular tachycardia with a pulse?
synchronized cardioversion immediately
what is the treatment for pulseless ventricular tachycardia?
NCLEX = defibrillate, real world = start cpr, epi, amiodarone

the image shown depicts what cardiac arrhythmia?
torsades de pointes
torsades de pointes is most commonly caused by _____
hypomagnesemia
what is the treatment for unstable and/or pulseless torsades de pointes?
defibrillate, cpr
what is the treatment for stable torsades de pointes with pulse?
IV mag sulfate first, ID and stop trigger meds

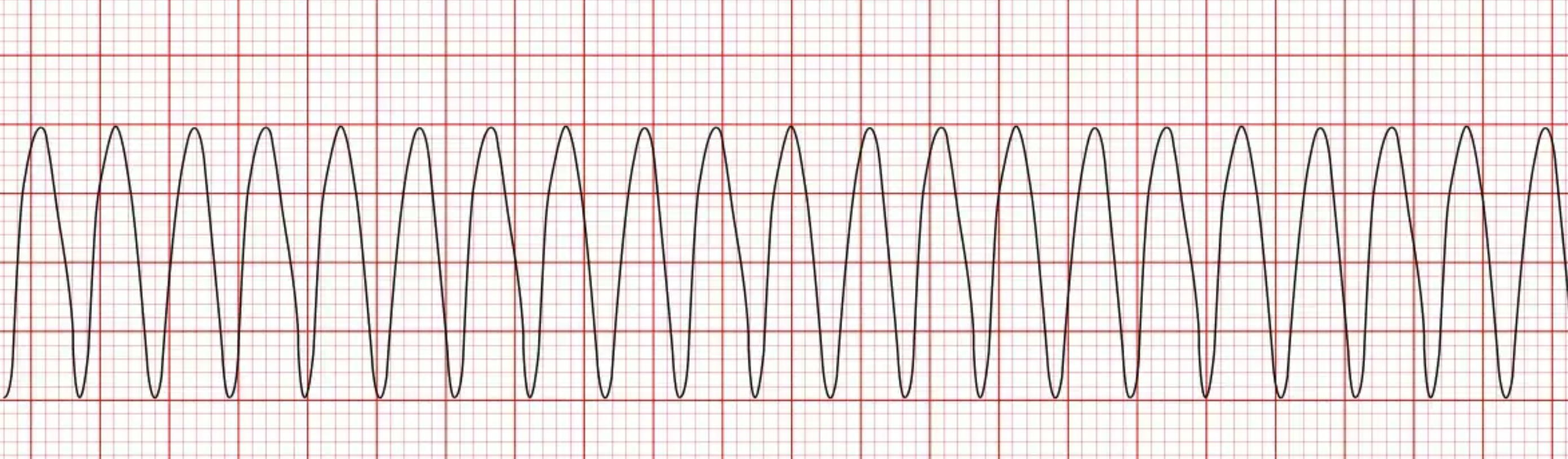
the image shown depicts what cardiac arrhythmia?
ventricular fibrillation
what is the key finding in ecg abnormalities that identifies vfib?
chaotic unidetifiable waveforms
which cardiac arrhythmia is ALWAYS pulseless, ALWAYS cardiac arrest?
ventricular fibrillation
what is the stepwise treatment for ventricular fibrillation?
check patient/leads, confirm unresponsiveness, check for pulse, defibrillate (NCLEX only or if pt has pulse), start cpr, epi, amiodarone

the image shown depicts what cardiac arrhythmia?
1st degree AV block
what is the key finding in ecg abnormalities that identifies a 1st degree AV block?
prolonged P-R interval >0.20s, regular or brady HR
when is a 1st degree heart block benign/requiring no treatment?
when asymptomatic in athletes, aging, increased vagal tone
when does 1st degree heart block become dangerous?
symptomatic, PR interval continues to lengthen, new onset post MI, syncope and severe bradycardia
what is the treatment for asymptomatic 1st degree heart block?
monitor for progression, ID and stop triggers
what is the treatment for symptomatic 1st degree heart block?
ID and stop triggers, atropine for brady, pacing if all else fails

the image shown depicts what cardiac arrhythmia?
2nd degree heart block type 1
what is the key finding in ECG abnormalities that identifies a 2nd degree heart block type 1?
normal or brady HR, PR interval progressively lengthens with each beat until a QRS is dropped, then resets
what is the treatment for asymptomatic 2nd degree heart block type 1?
monitor for progression, ID and stop triggers
what is the treatment for symptomatic 2nd degree heart block type 1?
ID and stop triggers, atropine for brady, pacing if all else fails

the image shown depicts what cardiac arrhythmia?
2nd degree heart block type 2
what are the key findings in ECG abnormalities that identify a 2nd degree heart block type 2?
normal PR interval, HR irregular, random QRS drops without a pattern
when does a 2nd degree heart block type 2 become dangerous?
always dangerous due to hemodynamic instability and will lead to asystole if untreated
what is the stepwise treatment for a 2nd degree heart block type 2?
immediate transcutaneous pacing, transvenous pacing, permanent pacemaker
the image shown depicts what cardiac arrhythmia?
3rd degree heart block
what is the key findings in ECG abnormalities that identifies a 3rd degree heart block?
atria and ventricles contracting independently of each other, atrial rate 60-100, ventricular rate 20-40 (escape), P waves have no relation to QRS
what is the most dangerous type of heart block?
3rd degree is a medical emergency
when does a 3rd degree heart block become dangerous?
always dangerous due to hemodynamic instability and will lead to asystole if untreated
what is the stepwise treatment for a 3rd degree heart block?
immediate transcutaneous pacing, transvenous pacing, permanent pacemaker
what is the stepwise treatment for asystole?
confirm unresponsiveness, check pulse, immediate cpr, epi
ECG shows organized electrical activity on the monitor, but the patient is unresponsive and has no pulse. what is this called?
pulseless electrical activity (PEA)
when does PEA become dangerous?
always dangerous, the heart is not beating