Human Herpes Viruses (HHVs)
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
What does the HHV family Herpesviridae consist of?
8 groups:
• HHV 1 ( Herpes simplex Type 1; HSV-1)
• HHV 2 (Herpes simplex Type 2; HSV-2)
• HHV 3 (Varicella Zoster Virus; VZV)
• HHV 4 (Epstein Barr Virus; EBV)
• HHV 5 (Cytomegalovirus; CMV)
• HHV 6
• HHV 7
• HHV 8 → related to Kaposi’s sarcoma
Which groups of Herpes viruses are in the Alphaherpes group and what are their characteristics?
Alphaherpes viruses consist of HHV1 (HSV-1), HHV2 (HSV-2), HHV3 (VZV)
• Tropism: Infects epithelial cells on skin and mucous membranes
• Site of latency: neurons (sensory ganglia), short reproductive cycles
Which groups of Herpes viruses are in the Betaherpes group and what are their characteristics?
Betaherpes viruses consist of: HHV5 (CMV), HHV6, HHV 7
• Tropism: Infect monocytes, lymphocytes and epithelial cells
• Site of latency: Lymphocytes/monocytes
Which groups of Herpes viruses are in the Gammaherpes group and what are their characteristics?
Gammaherpes viruses consist of: HHV4 (EBV), HHV 8
• Tropism: Infect lymphocytes, B cells and epithelial cells
• Site of latency : B cells, endothelial cells
Common features of herpesviruses:
• Have a lipid bilayer envelope and are linear dsDNA viruses (Baltimore group I)
• Latent infection resulting in lifelong infection:
- Primary infection
- Reactivation of latent (recurrent)
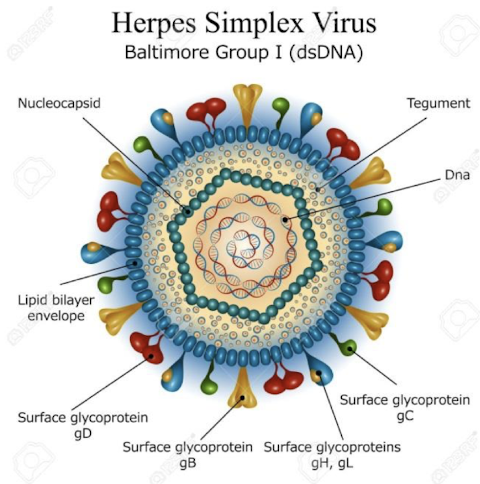
What is involved in the Herpesvirus lifecycle?
Virus binds specific receptors via glycoproteins, fuses with cell membrane; capsid delivers DNA to the nucleus
Transcription / translation: 3 phases
Immediate early- DNA binding proteins that regulate the transcription of early genes
Early – DNA polymerase & thymidine kinase (unique in HSV-1/HSV-2, VZV) to facilitate DNA replication
Late- structural proteins
Assembly in nucleus
Release of virions from cell via exocytosis with host cell death
What is the epidemiology of Herpes Simplex Viruses Type 1 and 2
(HHV 1 and HHV 2)?
- Worldwide distribution; no animal reservoir
- Direct contact with infected oral, genital or skin lesions secretions in a HSV carrier onto damaged mucous membranes or skin
- Both asymptomatic and symptomatic shedders
- HSV-1: acquired young via saliva or secretions from oral/skin lesions
- HSV-2: acquired via sexual contact / genital lesions or by childbirth
Pathogenesis of HHV 1 + 2:
• Entry via epithelial cells in the skin or mucous membranes at inoculation site
• Incubation period 4 – 6 days before clinical lesion appears; local inflammatory response before lesions rupture
• Enters the sensory nerves innervating site of replication and becomes latent in sensory ganglia; minimal gene expression; excellent immune and treatment evasion
• Viremia & dissemination may occur in immunocompromised people
• Reactivation due to stress, UV, immunosuppression; infectious virus travels down nerve and replicates in epithelial cells at nerve ending
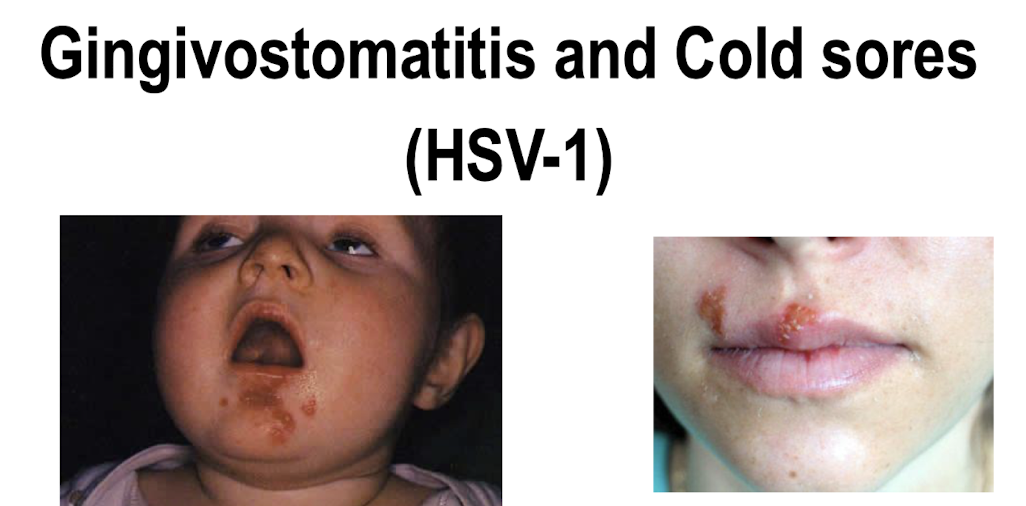
What HHV causes gingivostomatitis & cold sores & what are they?
HSV-1
Gingivostomatitis: Primary infection; incubation period 2-12 days; associated with fever, pharyngitis followed by vesicles around and inside the mouth; difficulty feeding; clears 1-2 weeks
Cold sores: Indicative of a reactivation of latent HSV-1 virus; may be
asymptomatic or symptomatic; 1 or 2 episodes on lips per year
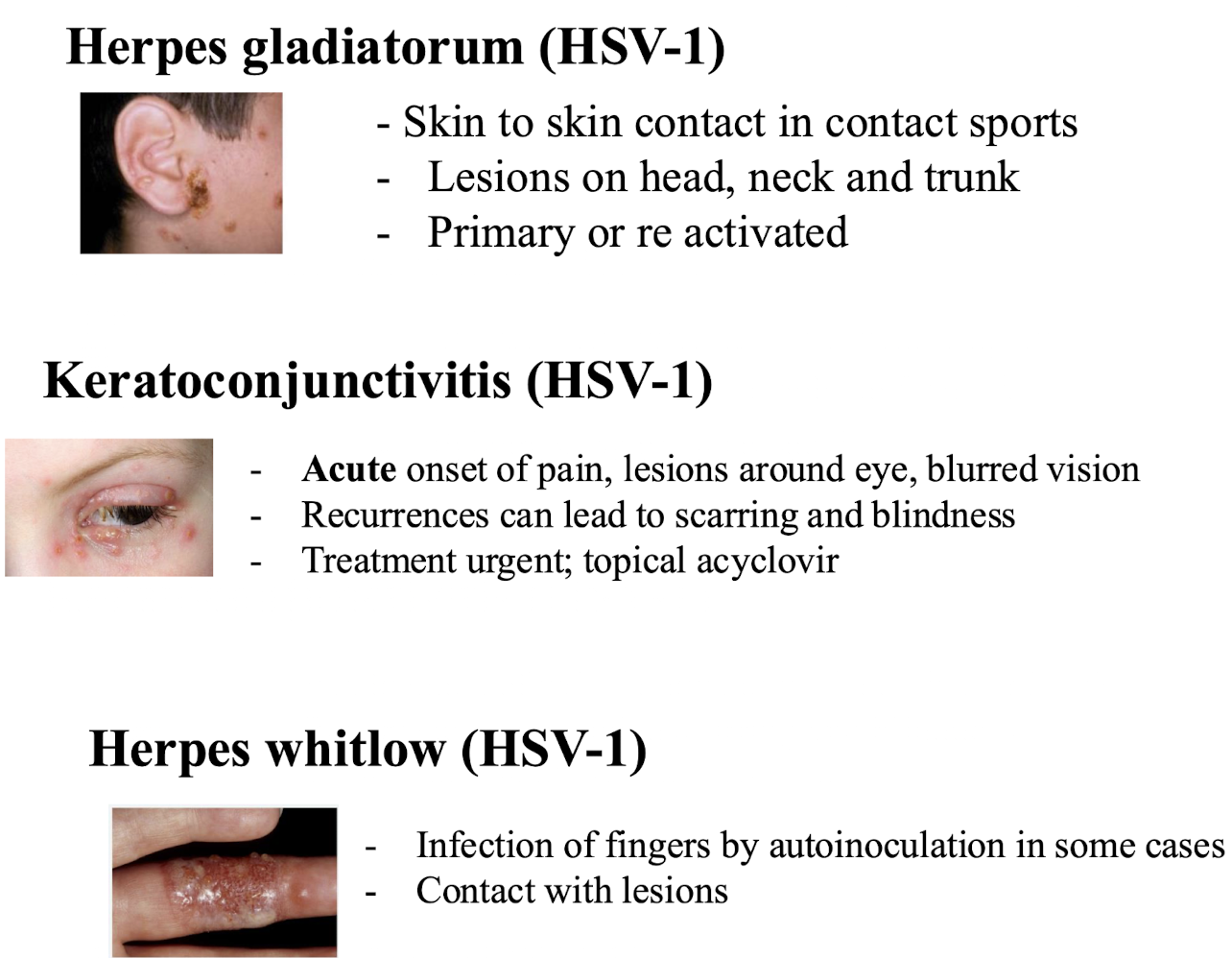
What other symptoms are caused by HSV-1?
Herpes gladiatorum (HSV-1)
- Skin to skin contact in contact sports, present as head, neck or trunk lesions, can be linked with primary or re-activated infection
Keratoconjunctivitis (HSV-1)
→ Acute onset of pain, lesions around eye, blurred vision, recurrences can lead to scarring and blindness; treatment urgent; topical acyclovir
Herpes whitlow
→ Infection of fingers by autoinoculation in some cases, or via lesion contact
What is a serious complication of a HSV-1 infection?
Acute sporadic encephalitis in immunocompetent hosts:
linked with Primary infection or reactivation; 2-3 cases/million people /year
• Higher rates in 5-30yo and >50yo
• Sx; Acute onset of fever, confusion, vomiting, altered level of consciousness (LOC), seizures progress to decreased LOC, coma, and death (severe cases)
• Range in severity from mild to severe severe disease
– High mortality (70-90%) and morbidity (<10% normal) in pre-antiviral era
– Urgent IV acyclovir has led to decreased mortalitiy (<20% and 40%) & return to normal neurological function
• High incidence of permanent neurological damage - short-term memory loss, seizures
What are common clinical symptoms associated with genital herpes caused by HSV-2?
Primary infection is sexually transmitted; fever, headache, myalgias
In women: local pain and itching, vaginal discharge, lymphadenopathy, vesicles and ulcers on vulva, perineum, vagina, cervix
In men: vesicles on shaft or glans of penis; may be associated urethritis
Over 1/2 of primary HSV-2 infections are asymptomatic ie HSV-2 antibody positive no history of disease
Recurrent genital herpes is frequent in 1st year after primary infection reduces after that
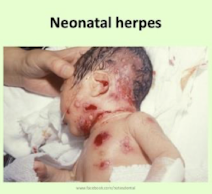
What are common clinical symptoms associated with neonatal herpes caused by HSV-2?
> 85% cases by infection with HSV-2 acquired from maternal genital secretions during delivery; severe risk to child if primary infection occurs during 3rd trimester
• C section for women with active lesions and/or positive cultures
3 major patterns of disease (likely a spectrum)
Lesions of skin, eyes, and mouth (SEM)
CNS disease – encephalitis with/without SEM
Disseminated disease – liver, lungs, CNS (most severe)
What is the treatment for neonatal HSV-2 infection & what occurs if it is untreated?
IV acyclovir is administered for neonates with serious disease:
• Untreated mortality exceeds 80% in disseminated disease, and 50% in CNS disease
May present with hepatitis, fulminant liver failure, multiorgan failure, seizures, encephalitis, rash
Incidence varies with prevalence of HSV
What is a complication associated with a primary HSV-2 genital infection?
Aseptic meningitis; incidence of 7% in women & 2% in men
Sx. Fever, headache, vomiting, photophobia about 3-12 days after the appearance of the genital lesion
Benign, no long term effects if treated
How does recurring HSV present in immunocompetent individuals?
Immunocompetent
– Asymptomatic shedder
– Herpes labialis (“cold sore”)
– Genital HSV (3-9 episodes per year)
– Keratoconjunctivitis
– Encephalitis
How does recurring HSV present in immunocompromised individuals?
Immunocompromised
– Extensive mucocutaneous disease
– Oesophagitis
– Pneumonitis
– Hepatitis
– Encephalitis
How are HSV diagnosed?
Clinical manifestations observed & undergo laboratory confirmation:
E.g. Virus isolation; Swabs from vesicle fluid (skin for cold sores, whitlow)
• Human fibroblasts or other cell types - CPE 24hrs.
• Confirm by IFA
Antigen detection from vesicular fluid
Molecular PCR (genital swabs, CSF for meningitis or encephalitis)
Direct visualisation from vesicle fluid or swab of base of lesion; EM or Tzanck smear
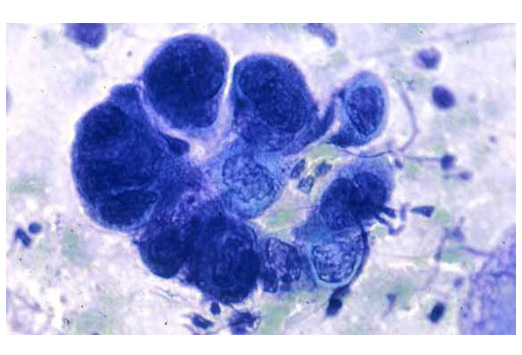
What is a Tzanck smear?
A diagnostic test used to identify HSV infections by examining fluid from vesicles.
It involves scraping the base of a lesion and staining the sample to visualise multinucleated giant cells under a microscope.
How are HSV treated?
• Oral/topical Acyclovir, Valacyclovir
• Oral/topical Penciclovir for primary oral and genital infection
• IV Acyclovir for neonates & encephalitis
• Side effects; nausea, diarrhea, headache, tremors
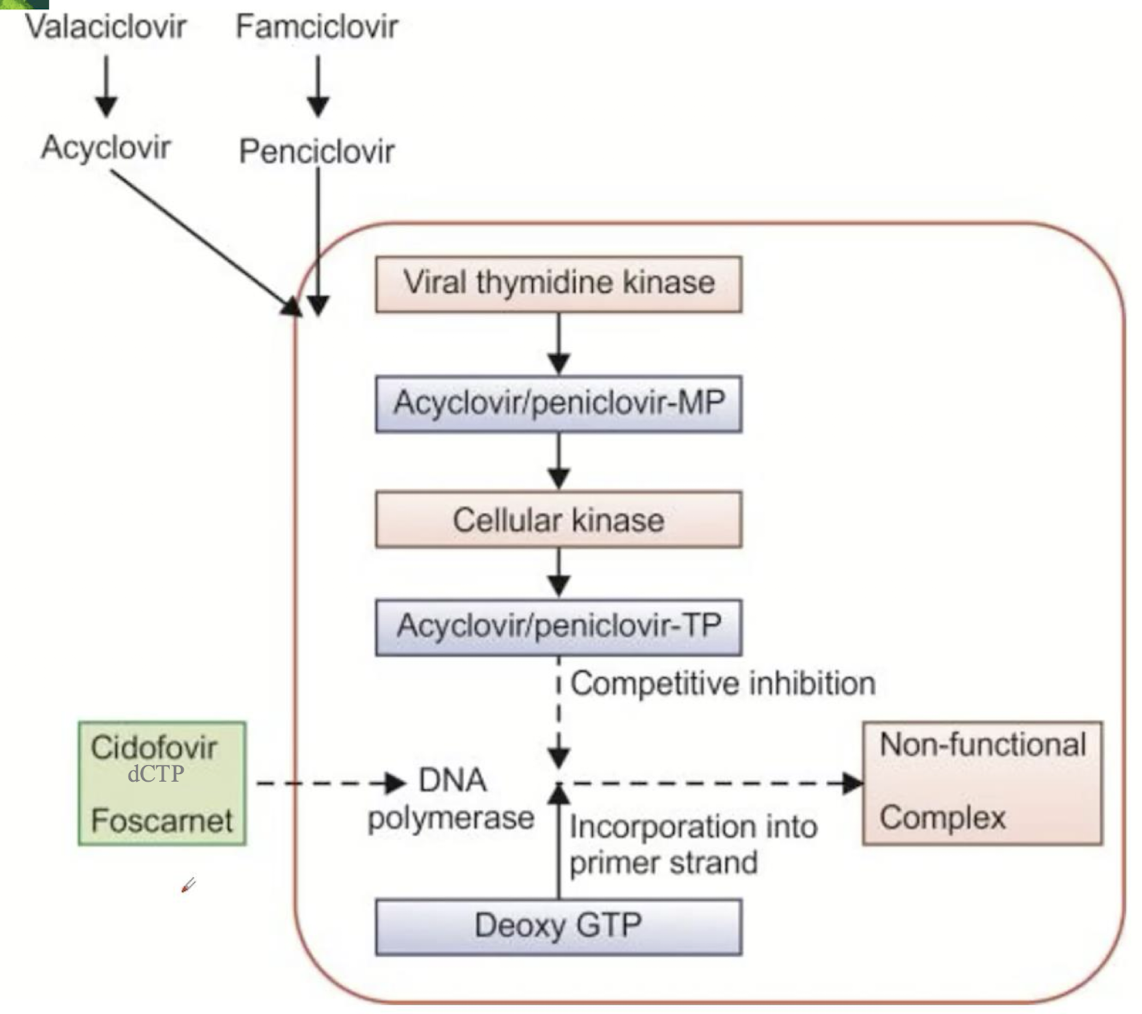
Acyclovir and derivatives: mechanism of action
• It is a guanosine nucleoside analogue that inhibits the replication of HSV-1, HSV-2, VZV
• Phosphorylated by viral thymidine kinase → to acyclovir monophosphate followed by phosphorylation to acyclovir triphosphate by cellular kinases
• Incorporated into viral DNA causing chain termination
What are the 2 distinct clinical syndromes associated with VSV
infections? (alphavirus)
1. Varicella (chickenpox): is the primary disease
Can have serious consequences in adults and in immunosuppressed
Included in childhood immunisation programmes in Ireland since October 2025
2. Zoster (Shingles) is the reactivation of latent virus
Rarely life-threatening
Causes significant morbidity in the form of post-herpetic neuralgia
(debilitating and difficult to treat)
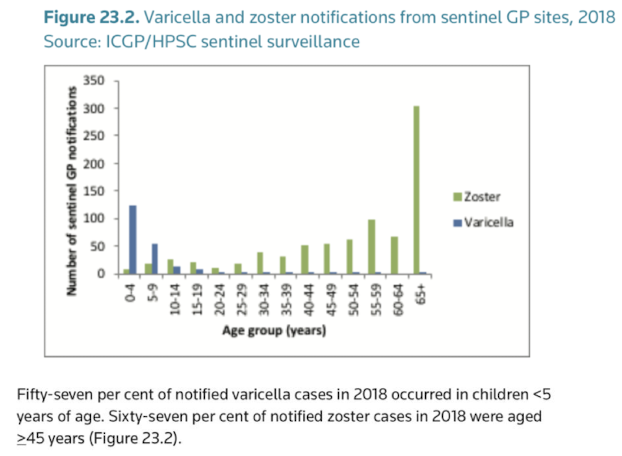
Epidemiology of VSV:
• VZV is highly infectious (R0 10-12)
• Spread via espiratory droplets or direct contact with vesicular fluids or contact with infected objects
• Peak age of infection in western world is children <5yo
• <10% of adults remain susceptible to infection
• Epidemiology will change due to vaccine
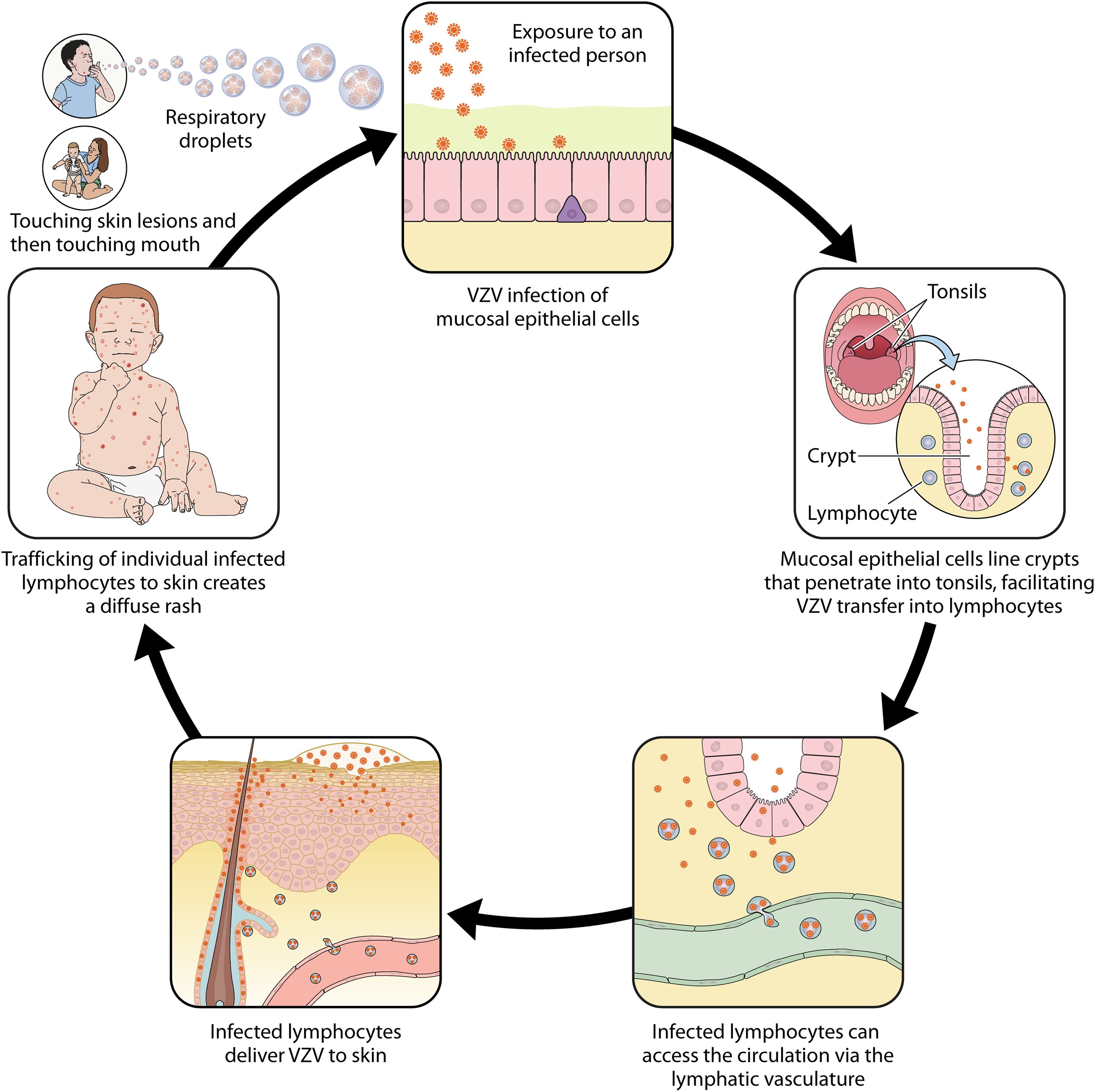
Pathogenesis of primary VZV Infection:
• Spread by respiratory droplets; typical childhood infection
• Incubation period ~ 2 weeks
• Targets epithelial cells in URT before being spread by blood to skin where it infects capillary endothelial cells and adjacent fibroblasts/epithelial cells
• Lesions progress from macules→papules→vesicles then break down with crust formation; mild in children more severe in adults
• Patients considered infectious from 2 days before rash and 4-5 days afterwards until existing vesicles have crusted
Complications of Varicella (chickenpox) - most common → rare
• Secondary bacterial infection of skin lesions
→ Most common complication, especially in children, typically involving streptococci and staphylococci
• Pneumonitis → incidence increased in pregnant women, 10% of smokers, 32% of children with leukaemia (25% mortality)
• Haemorrhagic chickenpox: commonly seen in immunocompromised (uncommon otherwise)
–> Haemorrhage into skin and GIT; hepatitis; thrombocytopenia; ACV and ICU
• Encephalitis
–> 3-4 cases per 10000 children (more common in adults); appears within a week of rash; resolves 2-4 weeks
0.1-0.2% more serious- Headache, vomiting, confusion; high mortality (5-20%) and neurological sequelae
Why is Varicella in Pregnancy so serious?
Can lead to severe varicella pneumonia in mother (late 2nd /early 3rd trimester) linked with 2 major problems based on timing of infection:
Congenital varicella syndrome (1st trimester)
Rare:1-2% risk in mothers infected in 1st 20 weeks
Sx. of skin scarring, limb hypoplasia, rudimentary digits, and CNS defects in newborns
–Mortality rates of 30% in the first few months of life
Neonatal varicella infection (Just before or after delivery)
Highest risk of infection if mother develops varicella one week before to one week after delivery as neonate will have insufficient transferred immunity
Varicella in pregnant women treated with acyclovir and VZIG
(varicella immunoglobulin); babies exposed to VZV in the first 28 days of life should also receive VZIG
What is VZV Reactivation (Zoster)?
Lifetime risk of developing Zoster is 24-30% following 1º infection, single reactivation can occur decades after initial infection
Virus reactivates in ganglion, travels down sensory nerve, and forms vesicular rash classically restricted to dermatome supplied by that nerve
Associated with intense destructive inflammatory changes in ganglion (manifests as severe pain)
What is a complication of VZV Reactivation (Zoster)?
Post herpetic neuralgia; persistent severe pain in the affected dermatome for about a month or more AFTER the zoster has resolved; incidence increases with age
• Immunosuppressed individuals are more likely to experience more than one episode of reactivation
Disseminated disease (through viraemia from original dermatome) also more common
How is VSV treated?
Using Acyclovir , Valacyclovir, Famciclovir for Herpes Zoster (Shingles)
Acyclovir +/- VZIg for:
– Varicella or zoster in immunocompromised individuals
– Varicella in pregnancy
– Neonatal varicella
– Varicella pneumonia in normal host
How is VSV prevented?
Passive immunisation:
Human immunoglobulin with high titres of antibody to VZV (VZIG)
Recommended for susceptible “at-risk” individuals with “significant” exposure
Administered ASAP, preferably within 96 hours, but beneficial up to 10 days
May not prevent infection, but intended to prevent serious forms of disease.
What are examples of active immunisation for VSV?
Varivax/Varilex; live attenuated vaccine that reduces the severity of varicella with 2 doses at 12months & in junior infants
Zostavax; live attenuated vaccine that prevents zoster and post herpetic neuralgia; ≥ 50 years
Shingrix; Subunit vaccine (envelope glycoproteins) that prevents zoster and post herpetic neuralgia; ≥ 50 years; 2 doses 2-6 months apart
75% of recipients seroconvert following vaccination
What is the epidemiology of EBV? (HHV 4)
• Infection usually occurs at early age; transmitted in saliva and almost always clinically silent; lifelong carrier
• Latent in a small number of memory B cells in circulation; intermittent virus shedding from mouth and pharynx leading to transmission
• Infection in adolescence can cause Infectious Mononucleosis (Glandular fever) but most have no symptoms when infected
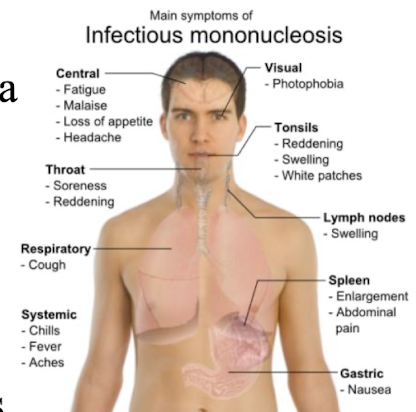
What is Infectious Mononucleosis which is caused by EBV?
Primary infection in adolescents – saliva i.e. kissing a virus shedding carrier
Sx: Sore throat, fever, headache, fatigue, rash uncommon
Generalised lymphadenopathy is almost always present; marked in cervical region (neck)
Splenomegaly in about 60% cases; enlarged liver in 10%
Mild cases resolve in days but 1-4 weeks more common; convalescence
What are the 5 main EBV related cancers?
Burkitts lymphoma
Hodgkins lymphoma
Post transplant lymphomas
B cell lymphomas in AIDs patients
Nasopharyngeal carcinoma (Chinese)
Burkitts lymphoma
Endemic (African) BL
Childhood cancer common in equatorial Africa; Jaw tumors
EBV found in 100% of cases
Incidence higher in regions in which malaria is hyperendemic
C- myc translocation leading to high expression of c-myc and high cell proliferation
Chemotherapy gives excellent results

Hodgkin’s Lymphoma
• Infectious mononucleosis risk factor
• In developed countries 40% of tumour cells contain virus
• Usually involves lymph nodes/abdomen

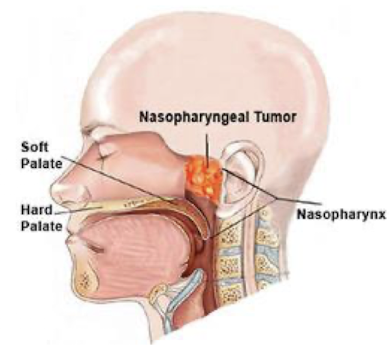
Nasopharyngeal carcinoma & its prevalence
• Mostly found in the nasopharynx & linked to the EBV virus.
• High prevalence in Southern China and Africa, due to both genetic
and environmental factors
• Chinese diet of a high amount of smoked fish, which contain nitrosamines, well known carcinogens (environmental).
• Nasal obstruction, discharge, bleeding, deafness
• Responds well to radiotherapy; 5 year survival rates of about 50%
EBV Diagnosis
Laboratory diagnosis involves molecular and serological methods:
(Serology)
Heterophile agglutinins; monospot test to diagnose IM
ELISA; Detection of IgM and IgG antibodies against EBV antigens.
PCR can be used for viral DNA detection.
Epidemiology of Cytomegalovirus (HHV 5)
• Latent infection; periodic asymptomatic shedding in saliva, breast milk, urine, semen/cervical secretions; infection spread by contact with these fluids
Babies: transmits across placenta, within birth canal, breast milk
Young children: transmission via saliva or urine
Older people: sexually; present in semen/cervical secretions
Blood/ solid organ and bone marrow from seropositive donors CMV can transmit the virus
CMV Clinical Symptoms
– Presents as asymptomatic infection in most children and adults
Complications associated with those who are:
Immunocompromised - Transplant or AIDS patients
Pneumonitis following bone marrow transplant
Have AIDS: disseminated disease (retinitis, colitis)
Pregnant women: primary infection can occur during pregnancy or reactivation of infection
What are the 3 different types of CMV infection in babies?
Congenital (most serious) - primary infection in early pregnancy of the mother or reactivation, the virus can spread via the placenta to the foetus
Primary infection can cause microcephaly, deafness, brain calcification and hepatosplenomegaly; can result in hearing loss or developmental delay
Perinatal- during birth
Postnatal- breast milk
*Postnatal or perinatal rarely symptomatic or associated with long term problems
What are the 3 main diagnostic approaches of CMV?
Culture and DEAFF (Detection of Early Antigen Fluorescent Foci pp65) testing
Serological diagnosis:
Useful for detecting primary infection; CMV specific IgM in the absence of IgG
In immunocompromised measurement of antibody levels may not be helpful
Molecular: PCR to detect and quantify – viral load
How is Valganciclovir used as a treatment for congenital CMV in immunocompromised individuals?
• Nucleoside analogue phosphorylated by VIRAL UL97 protein;
incorporated into viral DNA → chain terminator
• Accumulates in CMV infected cells
• Excreted by kidneys – however toxicity includes neutropenia and renal impairment
• Crosses Blood Brain Barrier
What is a 2nd line therapy of CMV?
Foscarnet second line therapy – competitive inhibitor of the viral polymerase enzyme; used to treat resistant strains of CMV.
What are characteristics of HHV6 and HHV7?
Human herpesvirus 6 (roseola) has two variants, 6A and 6B.
• Found worldwide and in the saliva of >90% of adults; most children infected by 2years.
• Replicates in T and B cells
• HHV 7 predominantly infects CD4+ T cells and can be reactivated by T cell activation; widespread infection of children
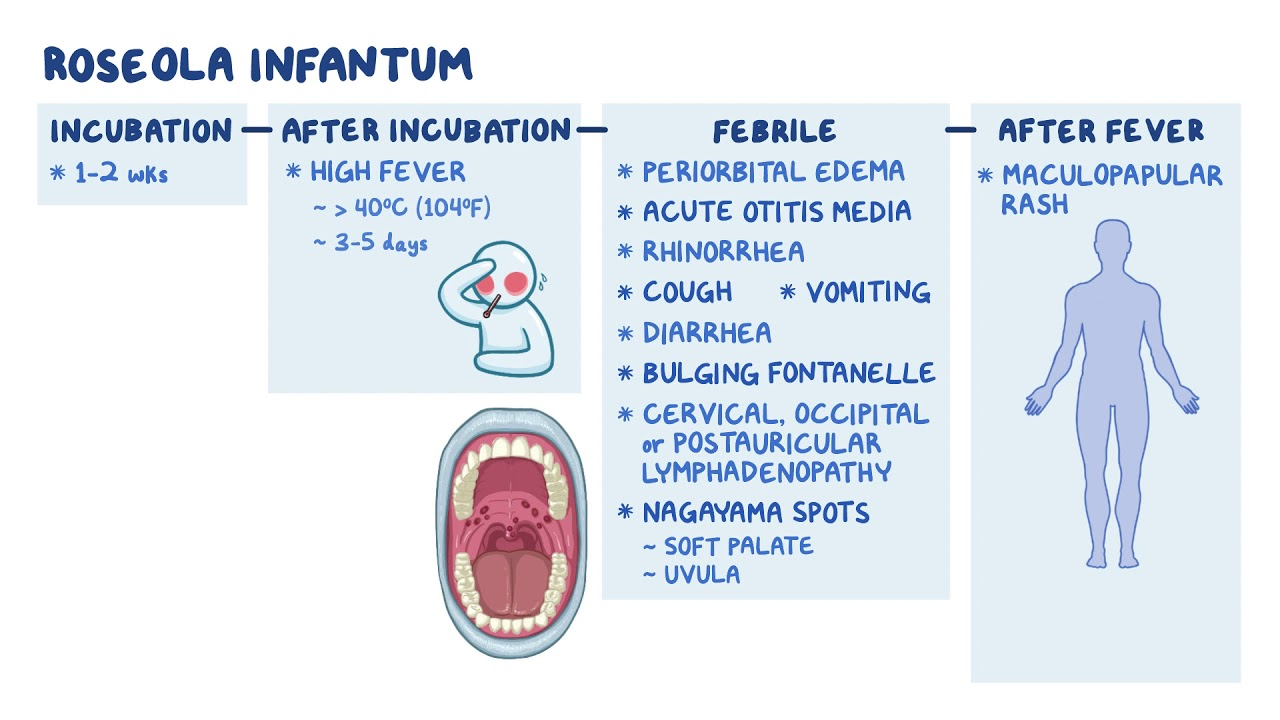
What does a primary HHV-6B infection cause in infants and young children?
Roseola infantum or sixth disease;
3-5 days of high fever
Sometimes upper RT symptoms and lymphadenopathy; after fever subsides, a macropapular rash appears on trunk and neck that lasts a few days
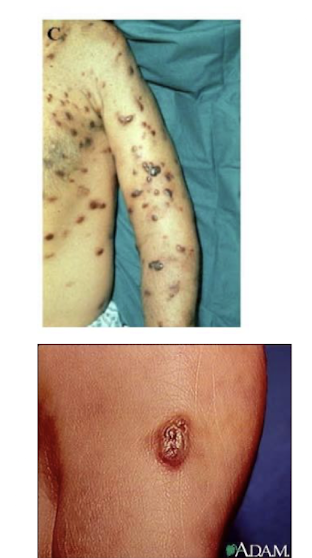
What condition is HHV 8 associated with?
Kaposi's sarcoma, primary effusion lymphoma:
Form of skin cancer that can involve internal organs
Primarily affects immunocompromised individuals such as those with HIV/AIDS.
Seroprevalence 1-2.5% in US blood donors
HHV1 targets ____________with latency in the _____ which causes diseases such as ___________
Targets → Mucoepithelia
Latency → In neurons
Disease → Causes oral, ocular lesions, encephalitis etc
HHV2 targets ____________with latency in the _____ which causes diseases such as ___________
Targets → Mucoepithelia
Latency → In neurons
Disease → Genital, ocular, disseminated disease
VZV (HHV3) targets ____________with latency in the _____ which causes diseases such as ___________
Targets → Mucoepithelia
Latency → In neurons
Disease → Chicken pox, shingles
EBV (HHV4) targets ____________with latency in the _____ which causes diseases such as ___________
Targets → B lymphocytes, epithelia
Latency → B lymphocytes
Disease → Infectious mononucleosis, tumours
CMV (HHV5) targets ____________with latency in the _____ which causes diseases such as ___________
Targets → Epithelia, monocytes lymphocytes,
Latency → Monocytes lymphocytes, DC
Disease → Numerous infections incl. congenital disease, pneumonia, retinitis
HHV6 targets ____________with latency in the _____ which causes diseases such as ___________
Targets → T lymphocytes & others (lymphotrophic)
Latency → T lymphocytes
Disease → Roseola in infants
HHV7 targets ____________with latency in the _____ which causes diseases such as ___________
Targets → T lymphocytes (esp CD4+ T cells) & others
Latency → T lymphocytes
Disease → Roseola
HHV8 targets ____________with latency in the _____ which causes diseases such as ___________
Targets → Endothelial cells & B cells
Latency → B lymphocytes
Disease → Kaposi's sarcoma, primary effusion lymphoma