Ther Ex Exam 1
1/111
Earn XP
Description and Tags
Shoulder
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
112 Terms
Exercise Prescription
1. Safety
2. Targets appropriate tissue
3. Fits desired results
4. Functionality
5. Economy/added benefits
Best 5 Glute Med Exercises
Side plank abd, DL down
Side plank abd, DL up
Single limb squat
Clamshell (Hip Clam) 4
Front Plank with hip ext
Best 5 exercises for Glute Max
Front plank with hip ext
Gluteal squeeze
Side plank abd, DL up
Side plank abd, DL down
Single limb squat
Skater squat
The Three R’s
Reset: PT led changes such as joint mobs, soft tissue mobs dry needling, etc..
Reinforce: Things such as banded joint flexions
Reload: Such as squads, lunges etc..
Mobility problems with tissue
Neural tension
Fascial tension
Muscle shortening
Hypertrophy
Trigger point activity
Scarring and fibrosis
Mobility problems with joint
Osteoarthritic
Osteoarthrosis
Fusion
Subluxation
Adhesion capsulitis
Dislocation
Motor control/ stability problems
• Motor control dysfunction (ex: muscle late to activate)
• Mechanical breathing dysfunction (Using accessory muscles instead of diaphragm)
• High threshold strategy (overactive global) - Ex hamstring overactivity
• Local muscle dysfunction
• Poor static stability
• Poor dynamic stability
Pec Major Function
Shoulder adduction
Shoulder IR
Horizontal Adduction
Protracted shoulder position is associated with
Narrow subacromial space
Causes impingement and inhibits rotator cuff
Causes decreased force production in elevation and inhibits lower trap
Possible causes of increased kyphosis and rounded shoulder
Pec minor tightness
Motor control problem
How can increased thoracic kyphosis contribute toShoulder impingement syndrome?
It restricts thoracic extension, which can alter scapular movement and reduce shoulder elevation.
What is scapular dyskinesis?
Abnormal movement or positioning of the scapula during shoulder motion.
How does scapular dyskinesis contribute to SIS?
It can decrease the subacromial space and increase impingement of shoulder structures.
Why is thoracic extension important for shoulder elevation?
Adequate thoracic extension allows normal scapular upward rotation and optimal overhead motion.
What should clinicians assess in patients with SIS besides the shoulder?
Thoracic posture, thoracic extension ROM, and scapular mechanics
Increased thoracic kyphosis → Decreased thoracic extension → Scapular dyskinesis → SIS
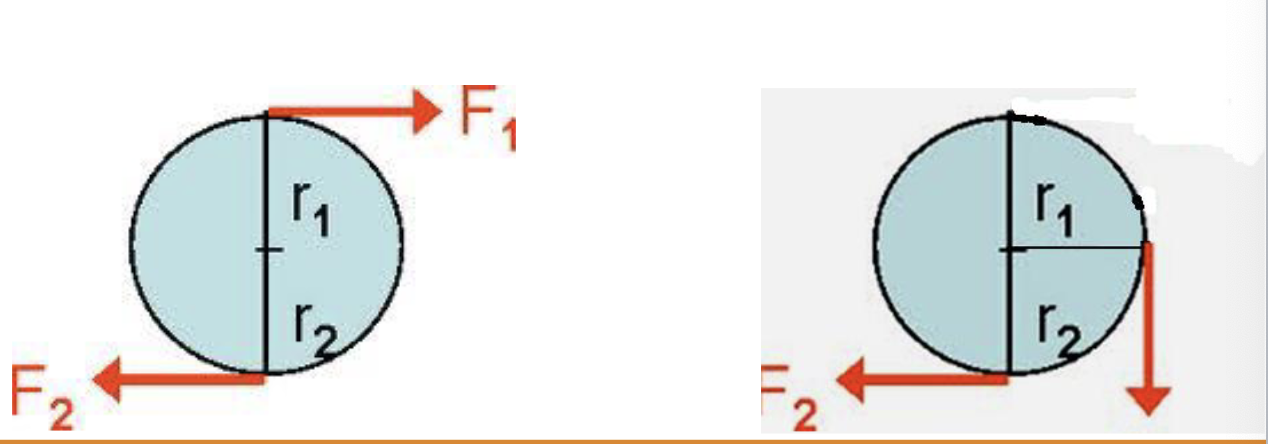
Force Couple
Two forces of equal magnitude but opposite direction with parallel line of application. The force couple causes the body to rotate around an axis perpendicular to the plane of the forces.
Deltoid functions to
Elevate the arm and produces superior translation of humeral head
Inferior and medial forces of rotator cuff (RC) offset _____
superior translation of deltoid (specifically the Infraspinatus, Teres minor, subscap).
The posterior cuff and subscap appears to have a greater role in the force couple than the supraspinatus
Describe the force couple of the shoulder
During shoulder abduction, the deltoid elevates the arm but also causes superior translation of the humeral head toward the acromion, which can decrease the subacromial space and increase the risk of impingement. To counteract this, the rotator cuff muscles—particularly the infraspinatus, teres minor, and subscapularis—create an opposing inferior and medial force, while the supraspinatus compresses the humeral head into the glenoid. Together, these muscles form a force couple that centers and stabilizes the humeral head in the glenoid fossa, preventing excessive superior migration during arm elevation.
Scapular force couple- Upward and Downward rotaiton
The scapular force couple for upward rotation is formed by the upper trapezius, lower trapezius, and serratus anterior. These muscles work together to rotate the scapula upward during arm elevation, allowing full overhead motion and keeping the shoulder mechanics normal.
Downward Rotation of scapula is provided by Rhomboid major, Pec Minor and Levator Scapulae
What happens if we inhibit lower and middle trap in Abduction?
the scapula cannot upwardly rotate, posteriorly tilt, and externally rotate effectively possibly narrowing the subacromial space and increasing risk for impingement
Which scapular muscles are emphasized during resisted shoulder extension and adduction?
If you resist shoulder extension and adduction, you will often see increased activity in:
Rhomboids (retraction + downward rotation)
Levator Scapulae (elevation + downward rotation)
Primary impingement:
Compression of the RC between the humeral head and the acromion, corocoacromial ligament, coracoid, or AC jt
Secondary Impingement
impingement due to the underlying instability of the GHJ. (instability could be due to increased capsuloligamentous length or poor RC function or both)
Internal Impingement:
The undersurface of the SS and IS rub on the posterior-superior glenoid rim or are compressed between the humeral head and the posterior glenoid in the 90/90 position
Pts. with SIS demonstrate decreased SA activation from
30 -120°
Overhead athletes have greater risk of impingement
Which muscles showed the greatest decrease of activity with impingement
all 4 cuff muscles and mid deltoid
Roles of the Scapula
1. Be a stable part of the GH articulation
2. Retraction/protraction along the thoracic wall (helps dissipate forces to GHJ during overhead activity)
3. Elevation of the acromion and glenoid fossa in throwing or overhead activity
4. Base for muscle attachment
5. Links the proximal to distal force transmission
Scapular Translations
◦ Protraction (decreases IR&ER strength ≈ 20%)
Retraction (increases subacromial space)
◦ Elevation – depression
Normal shoulder complex elevation
upward rotation(45- 55°)
posterior tilting (20-40°)
ER of scap (15-35°) (post tilt and ER usually don’t occur until after 90°)
Which scapular muscles activate before the posterior deltoid during prone extension and prone horizontal abduction with ER?
The middle trapezius (MT) and lower trapezius (LT) activate first.
They stabilize the scapula before arm movement, providing a stable base for the posterior deltoid and rotator cuff.
Which exercises have been shown to activate the middle and lower trapezius before the upper trapezius?
Prone extension
Side-lying external rotation
Prone horizontal abduction with ER
Which muscles show significantly increased activity once shoulder elevation exceeds 120°?
Serratus Anterior (SA) and Lower Trapezius (LT).
The following have been shown to elicit mid-trap and serratus anterior contractions while minimizing upper-trap
◦ Prone extension
◦ Forward flexion in side lying
◦ ER in side lying
◦ Prone horizontal abd with ER
◦ Push-up plus
Scapular Inhibition affects
ability to produce torque for stability and impaired coordination of the firing patterns of the scapular muscles
Scapular Dyskinesis
◦ Dysrhythmia: The scapula demonstrates premature or excessive elevation or protraction, non-smooth or stuttering motion during arm elevation or lowering, or rapid downward rotation during arm lowering.
◦ Winging: The medial border and/or inferior angle of the scapula are posteriorly displaced away from the posterior thorax.
is generally characterized by a lack of upward rotation, a lack of posterior tilting and increased medial rotation of the scapula
Normal scapulohumeral rhythm:
The scapula is stable with minimal motion during the initial 30° to 60° of humerothoracic elevation, then smoothly and continuously rotates upward during elevation and smoothly and continuously rotates downward during humeral lowering. No evidence of winging is present.
Tests to Assess Scapular Dyskinesis
Scapular Reposition Test
Scapular Assistance Test (modified)
Scapular Dyskinesis Test
Scapular Retraction Test
Scapula Reposition Test
1. Perform Hawkins-Kennedy and Neer tests
2. Grasp the scapula with the fingers contacting the AC joint anteriorly and the palm and thenar eminence contacting the spine of the scapula posteriorly, with the forearm obliquely angled toward the inferior angle of the scapula for additional support on the medial border.
3. Apply a moderate force to the scapula to encourage scapular posterior tilting and external rotation, and to approximate the scapula to a mid position on the thorax.
4. Any pain-provoking test can be repeated with the scapula manually repositioned using the SRT.

Scapular Assistance Test
Have the patient perform elevation under normal conditions and assess the pain experienced
Manually assist scapular upward rotation and posterior scapular tilting (not part of the original test) during shoulder elevation and determining this effect on pain
A positive test is when pain with elevation is either decreased or abolished during the assisted maneuver.

Scapular Dyskinesis Test
The patient should perform 5 repetitions of bilateral, active, weighted shoulder flexion and bilateral, active, weighted shoulder abduction (frontal plane)
Testing begins with arms at the side of the body, elbows straight, and shoulders in neutral rotation
The patient simultaneously elevates their arms overhead as far as possible to a 3-second count using the ‘‘thumbs up’’ position and then lower to a 3-second count.
The patient should hold dumbbells according to body weight, 3 lb. for those weighing less than 150 lb. and 5 lb. for those weighing 150 lb. or more.
Scapular Dyskinesis Test Rating Scale
◦ Normal motion: no evidence of abnormality
◦ Subtle abnormality: mild or questionable evidence of abnormality, not consistently present
◦ Obvious abnormality: striking, clearly apparent abnormality, evident on at least 3/5 trials (dysrhythmias or winging of 1 inch or greater displacement of scapula from thorax)
Final rating is based on combined flexion and abduction test movements.
◦ Normal: Both test motions are rated as normal or 1 motion is rated as normal and the other as having subtle abnormality.
◦ Subtle abnormality: Both flexion and abduction are rated as having subtle abnormalities.
◦ Obvious abnormality: Either flexion or abduction is rated as having obvious abnormality
Scapular Retraction Test
• The examiner first grades the strength in forward flexion following standard manual muscle testing procedures.
• The examiner then places and manually stabilizes the scapula in a retracted position
• A positive test occurs when the demonstrated strength is increased in the retracted position.

Push-up Plus
Perform normal push up and add maximal scapular protraction once the elbows are extended.
Push-up plus exercises have been advocated for use in shoulder rehabilitation, because it has been shown to elicit high serratus anterior muscle activity.
Note: The exercise can be modified for stability by having the pt perform the exercise on the wooble board or unstable surface. You can also scale uo by having the pt perform the exercise with one leg extended or with one arm to increase the demands on the stabilizers.
Knee Push-up plus(KPP)
KPP with ipsilateral leg extension, and one handed KPP provided the low UT/SA ratio and high SA activity
One handed KPP also produces a synergist activity of the posterior deltoid and the IS
hip extension promotes increased activity of the serratus anterior on the ipsilateral side and increased lower trap activity on the contralateral side
Note: Ext of the ipsilateral hip targets serratus and contralateral targets lower trap. Elevation in the scapular plane tends to increase the activity of the upper trap. Elevation with ER tends to increase the activity of the lower trap and decreases the ratio of the UT/LT
Scapular Exercises - Inferior Glide
Each subject was placed in an upright sitting position with the test arm abducted to 90° with fist clenched on a firm supportive surface. Each subject was instructed to apply pressure with his or her fist in the direction of arm adduction and instructed to inferiorly depress their scapula and hold this position for 5 seconds
Note: Isometric nd closed chaine. Good for SA contraction with less lower trap. Adduction force causes increased SA Space

Scapular Exercises - Low Row:
Subjects placed their hand on the anterior edge of the surface with palm facing posteriorly. Subjects were instructed to extend their trunk and push their hand maximally against the surface in the direction of shoulder extension and instructed to retract and depress the scapula; the isometric contraction was performed for 5 seconds.
Note: Greatest posterior delt activation, greater SA than UT contraction. Early SA activation in neutral postion

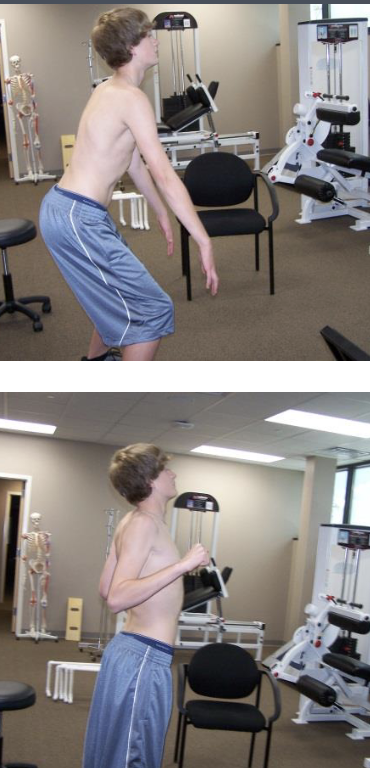
Lawn Mower:
Subjects began the exercise with their trunk flexed and rotated to the contralateral side from the instrumented arm with their hand at the level of their contralateral patella. Subjects were instructed to rotate the trunk toward the instrumented arm and extend the hip and trunk to a vertical orientation while simultaneously placing their instrumented arm at waist level and retracting their scapula so that they try to place an “elbow into their back pocket” position. Body movement was smooth, but the retraction position was to be completed with a strong contraction of the muscles.
Note: Good coordination of 3 upward rotators, UT, MT, SA (Watch for inpigement)
Robbery
The patient begins in a standing position with the trunk flexed to approximately 40° to 50° with arms forward flexed and palms facing the thighs. While keeping the elbows close to the body, each subject moved into trunk and arm extension and flexed the elbows so palms were facing up and away from the body while simultaneously pinching both scapulae toward his or her back pockets with a strong 5- second contraction.
Note: Good coordination of 3 upward rotators
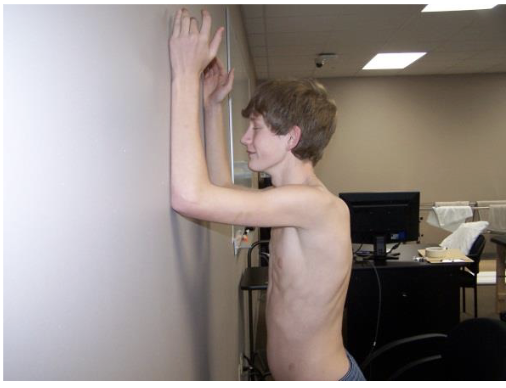
Wall Slide
The patient places the forearms on a wall in neutral with elbows flexed and arm in the plane of the scapula. The patient is then instructed to slide the forearms up the wall and lower with control.
Note: SA activation during wall slide is not much different than a push up plus exercise. However, this exercise allows for this activation overhead, where pts with shoulder impingement have been shown to have altered scapular mechanics and decreased SA activity.
Lateral Wall Slide
The patient places the forearm on a wall in neutral with elbows flexed and arm in the plane of the scapula or in the sagittal plane. The patient elevates and arm while isometrically externally rotating and horizontally abducting into the wall.

Posterior Wall slide
The patient places the forearms on a wall in neutral with elbows flexed and the shoulder horizontally abducted and externally rotated. The patient is then instructed to slide the forearms up and down the wall and lower with control. The patient should stop elevation if the forearms start to lose contact with the wall
Note: Shoulder mobility can be a problem. To make it harder perform in prone to have scapular retraction against gravity.

Plank saws
While protracting scapula in plank position, rock caudal and cranial
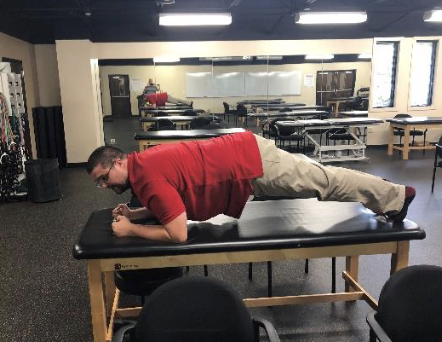
Shoudler taps
While in a plank position, maintain solid position and tap the opposite shoulder with the non-affected hand
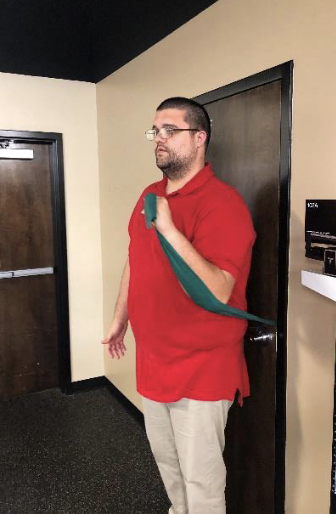
Serratus Upper-cut:
grasp theraband in hand and have the band in contact forearm and wrapping around the elbow. Punch upward and protract the shoulder at 120⁰
Types of scapular Mobs
Superior/ inferior
Upward/ Downward
Distraction
Why is core stability important for shoulder function?
Core stability allows efficient transfer of force from the legs and trunk to the arm. Poor core control can contribute to shoulder dysfunction and decreased performance.
Which muscles are most responsible for decelerating the arm after a throw?
The posterior rotator cuff (infraspinatus and teres minor), posterior deltoid, and middle/lower trapezius contract eccentrically to slow the arm and stabilize the shoulder.
Which muscles are most responsible for acceleration phase in a throw?
Pec major
Latissimus dorsi
Subscapularis
How can hip weakness or tightness affect the shoulder?
It can disrupt force transfer through the kinetic chain, increasing stress on the shoulder.
Note: The breakage of the kinetic chain at this level means that shoulder rotation velocity must increase by 15% to 40% to maintain the same hand kinetic energy. The alterations in biomechanics and loads may place translatory (i.e., increased external rotation) or rotary (i.e., increased angular velocity) stresses on the labrum, causing or accentuating labral injury.” (Burkhart, 2000)
Corkscrew Test
The corkscrew test can be clinically useful and quick to assess problems in lower-limb and trunk stability, which may then warrant further detailed evaluation (The patient perform a single leg squat, if the patient ‘corkscrews,’ that is, twisting at the knee and hip the test is positive, it is useful to test both sides, dysfunction is more commonly seen on the contralateral leg to the throwing shoulder. Can also be used for knee collapse)
What would happen if the supraspinatus becomes weak/ paralyzed?
The deltoid will require 101% more force. And there is a higher risk of superior translation of the humerus. The supraspiantus pulls the head of the humerus in to the glenohumeral space.
Role of the RC
Mid-range stability is provided by the rotator cuff in a function termed ‘concavity compression’ where the stabilizing force of the rotator cuff contraction compresses the convex humeral head into the concavity of the glenoid.
Shoulder rotator imbalance has been shown to be
predictor of shoulder injuries
Note: IR strength increases with overhead activities (throwing, hitting, serving) without a comparable increase in the eccentric strength of the ER
ER with Towel
Assists in isolation of ERs
Controls unwanted motion
Elevates IS muscle activity by 10%
Prevents decreased blood flow to SS
Increases SA space

What load is often recommended for early rotator cuff strengthening?
lighter loads (~40% effort) may be better than heavy loads because heavier loads can increase unwanted muscle substitution and joint stress. Closed-chain exercises (where the hand is fixed on a surface) help "preset" the rotator cuff, meaning they promote co-contraction of the shoulder muscles and improve joint stability. Early in rehabilitation, RC exercises should often be performed with a fixed base of support to enhance scapular stability and coordinated muscle activation before progressing to more demanding open-chain exercises.
What exercise can be used to facilitate subscapularis contraction?
The belly press exercise.
Note: it is difficult to isolate because larger muscles such as the pectoralis major and latissimus dorsi also produce internal rotation. The belly press exercise can be used to facilitate and assess subscapularis activation. Additionally, prone exercises are beneficial for rotator cuff training because the position tends to reduce the contribution of the pec major and latissimus dorsi, allowing the rotator cuff muscles to work more effectively.
Why are prone exercises useful for rotator cuff training?
They decrease the contribution of the pec major and latissimus dorsi, allowing better rotator cuff activation
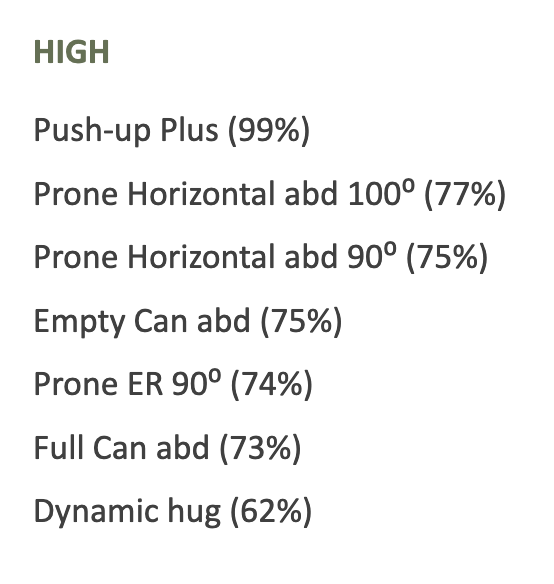
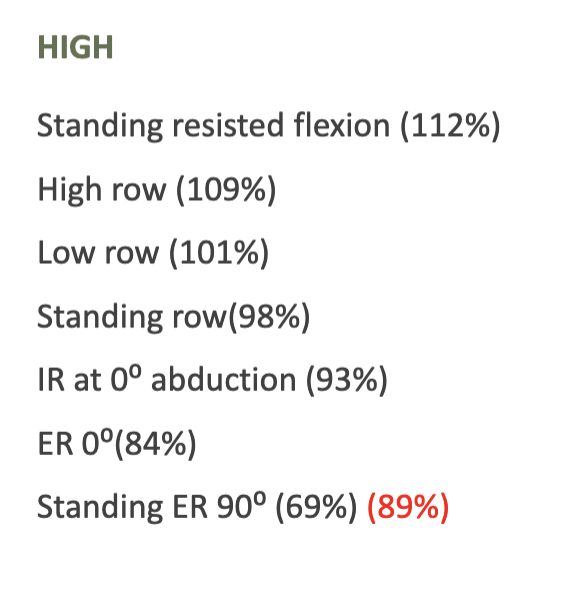
Exercises that promote high Supraspinatus activity
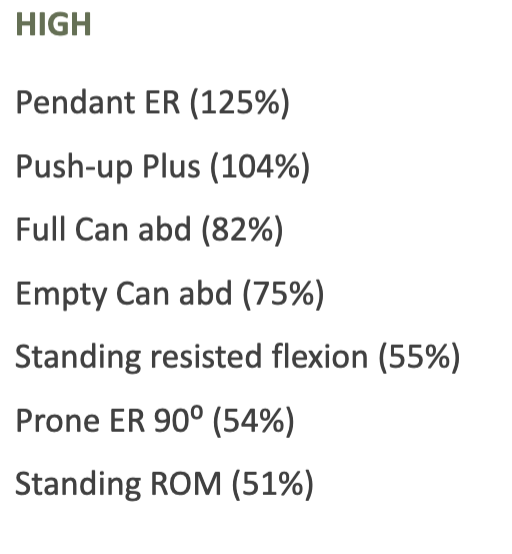
Exercises that promote high Infraspinatus activity
Exercises that promote high Subscapualris activity
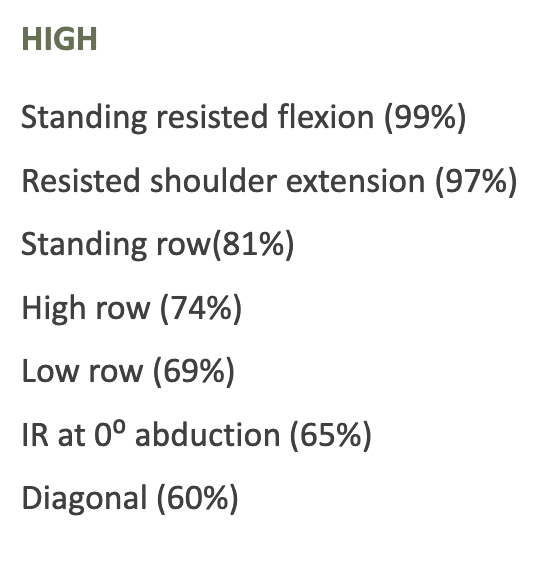
Exercises that promote high Supraspinatus activity
Note: The teres minor (along with the infraspinatus) contracts to compress the humeral head into the glenoid and resist excessive anterior/superior translation.
What does AMBRI stand for?
A = Atraumatic
M = Multidirectional
B = Bilateral
R = Rehabilitation is the best treatment
I = Inferior capsular shift if surgery is needed
What type of patient typically has AMBRI instability?
A patient with generalized laxity/hypermobility and instability in multiple directions without a traumatic event.
What is the primary treatment for AMBRI?
Rehabilitation focused on rotator cuff and scapular stabilizer strengthening.
Note: Inferior capsular shift is the preferred surgery if needed
What does TUBS stand for?
T = Traumatic
U = Unidirectional
B = Bankart lesion
S = Surgery often needed
Note: Surgery usually needed; results are good
What is a Bankart lesion?
Detachment of the anterior-inferior labrum from the glenoid, commonly occurring after an anterior shoulder dislocation.
Mostly associated with TUBS
Anterior shoulder instability commonly involves ___
Bankart lesion - Avulsion of the anterior labrum
Caused by falling on outstretched arm
ER/ABD/ Ext
Can be loose anterior capsule without labral damage
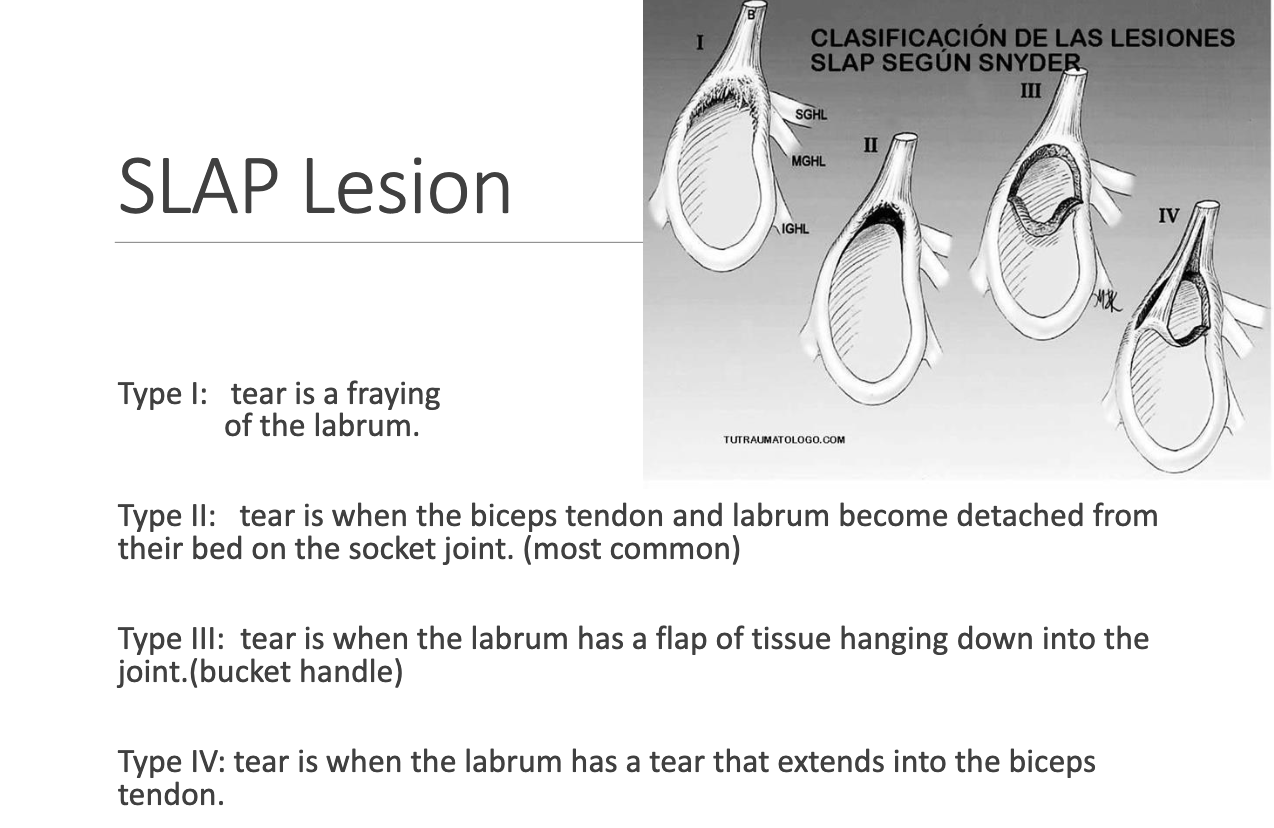
What does SLAP lesion stands for
Superior
Labrum
Anterior to
Posterior
May be due to chronic traction injury of the biceps on the superior labrum, or fall on outstretched arm
Slap lesion types
What is the main rehab goal for shoulder hypermobility?
Improve muscle performance and motor control of the dynamic stabilizers. Treatment must focus on the cause of hypermobility by improving mobility of relatively less mobile segments and concurrently reducing mobility at more mobile segments.
Treatment for GH Instability/ Hypermobility
Specific joint mobilization (posterior capsule)?
Immobilization (max. 3 weeks) IF subluxation is diagnosed.
AROM against gravity as patient regains strength and motor control.
Main target muscle tends to be subscapularis as well as gradually resisted exercises for pectoralis major, latissimus, teres major. Infraspinatus and teres minor are also often targeted.
Note: Must have stable scapula for rotator cuff function to be effective!
Hypomobility often coexists with
Hypermobility
Treatment?
Manual stretching with concurrent strengthening of weakened antagonist.
What is GIRD (Glenohumeral internal rotation deficit)?
Loss of ≥20° of internal rotation in the throwing shoulder compared to the non-throwing shoulder
What is Total Rotational Motion (TRM)?
IR + ER measured with the shoulder abducted to 90
When is TRM considered normal?
When it is within 5° of the non-throwing shoulder.
What are two common causes of GIRD?
Osseous adaptations (humeral retroversion) and soft tissue tightness (posterior capsule/musculature)
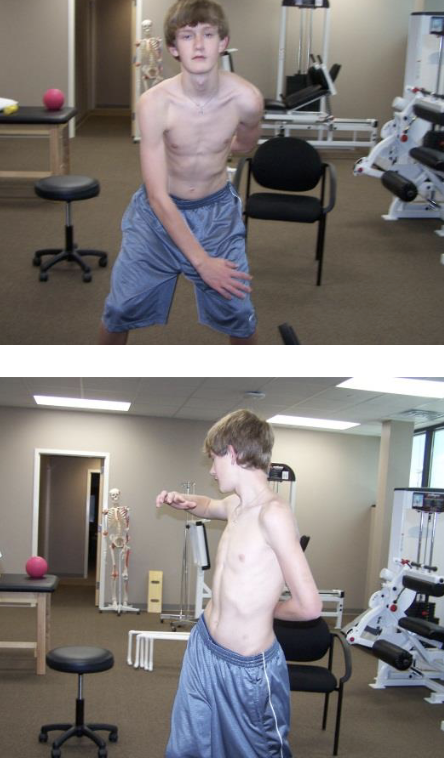
Rotator Cuff Exercise - Prone ext
The subject is prone, with the shoulders resting in 90° forward flexion. From this position the subject performs bilateral extension to neutral position, with the shoulder in neutral rotation.
Note: MT and LT active prior to PD

Prone Horizontal Abduction with External Rotation
The subject is prone, with the shoulders resting in 90° forward flexion. From this position the subject performs bilateral horizontal abduction to horizontal position, with an additional external rotation of the shoulders at the end of the movement.
Note: High infraspinatus activity, low UT/ LT ratio. MT and LT active prior to PD and UT. Would not start day 1

External rotation in side lying
The subject is side lying with the shoulder in neutral position and the elbow flexed 90°. From this position the subject performs maximum external rotation of the shoulder, with a towel between the elbow and trunk to avoid compensatory movements.
Note: MT and LT active prior to UT

Prone Elevation
Shoulder elevation with the subject in prone, the shoulder abducted approximately 100°, the arm externally rotated, and resistance applied at the wrist.

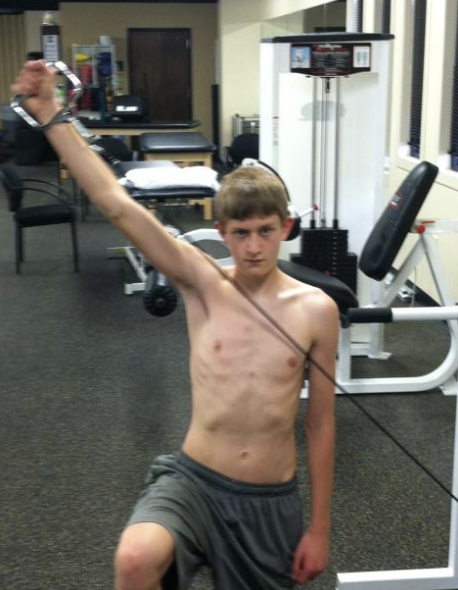
Diagonal Pattern D2 Flexion
Gripping tubing handle in hand of involved arm, begin with arm out from side 45° and palm facing backward. After turning palm forward, proceed to flex elbow and bring arm up and over involved shoulder. Turn palm down and reverse to take arm to starting position.
Note: High supraspinatus activity. Needs good trunk control. Big ROM and has multiple planes.
Diagonal Pattern D2 Extension
Involved hand will grip tubing handle overhead and out to the side. Pull tubing down and across your body to the opposite side of leg. During the motion, lead with your thumb

Empty Can
Shoulder abduction in the scapular plane (30° anterior to the frontal plane) with internal rotation and resistance applied at the wrist

Full Can
Shoulder abduction in the scapular plane (30° anterior to the frontal plane) with external rotation and resistance applied at the wrist. Also better for lower trap activation with elevation over 90° than wall slides and push-up plus.
Note: Infraspinatus and subscapularis activity higher in full can. Better than push up plus and wall slide for LT hardwick. Shrugging is a compensation (mirror) and impingement may be a problem.

Banded Full Can
Same as full can but adds horizontal moment

Pendant External Rotation
Shoulder external rotation in 0° abduction with the elbow at the side and flexed 90° and resistance applied at the wrist. ER has similar activity at 0°, 45°, and 90°, but 0° is the best position to isolate and may offer less chance of impingement.

Prone External Rotation
With the subject in prone, the shoulder abducted to 90° and the elbow flexed to 90° and resistance applied at the wrist to end range external rotation.
