Adnexal Mass, Ovarian and Tubal Neoplasms, Breast Disorders
1/111
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
112 Terms
What is the normal size of a premenopausal ovary?
4-6 cm (about the size of a kiwi).

What is the normal size of a postmenopausal ovary?
Around 2 cm (about the size of a kidney bean).
Why is any palpable adnexal mass in a postmenopausal woman considered high risk?
The risk of malignancy increases significantly in postmenopausal women; such masses are considered 'guilty until proven innocent'.
What are the 2 pillars of evaluation of adnexal masses?
Age and menopausal status, and mass characteristics.
What is the gold standard for initial imaging of an adnexal mass?
Transvaginal Ultrasound (TVUS).
What are the ultrasound characteristics of a benign adnexal mass?
Simple cysts (unilocular), thin walls, no solid components, and 'ground glass' echoes (endometriomas).
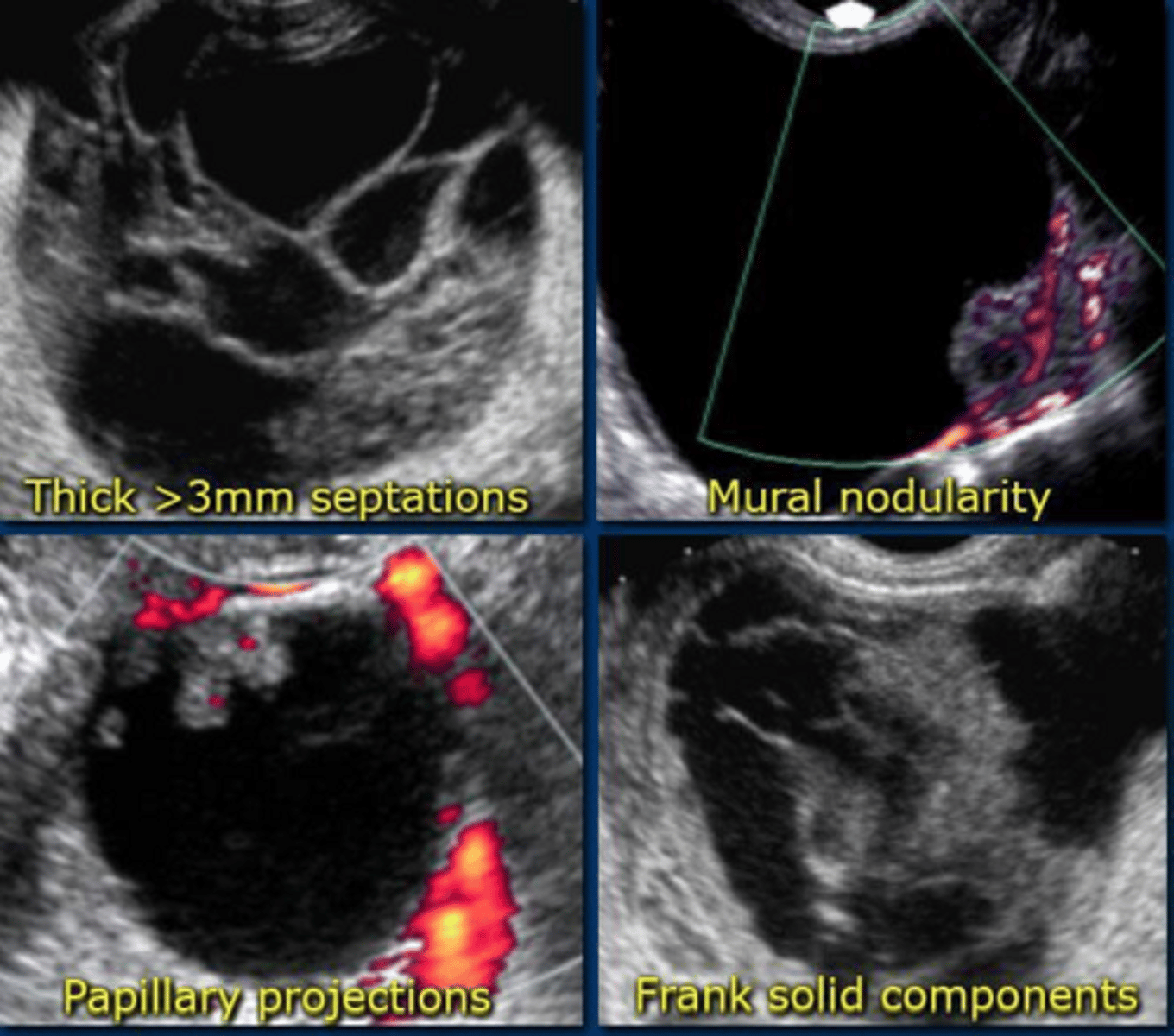
What are the ultrasound characteristics of a malignant adnexal mass?
Solid components, thick septations, irregular borders, and internal vascularity on Doppler.
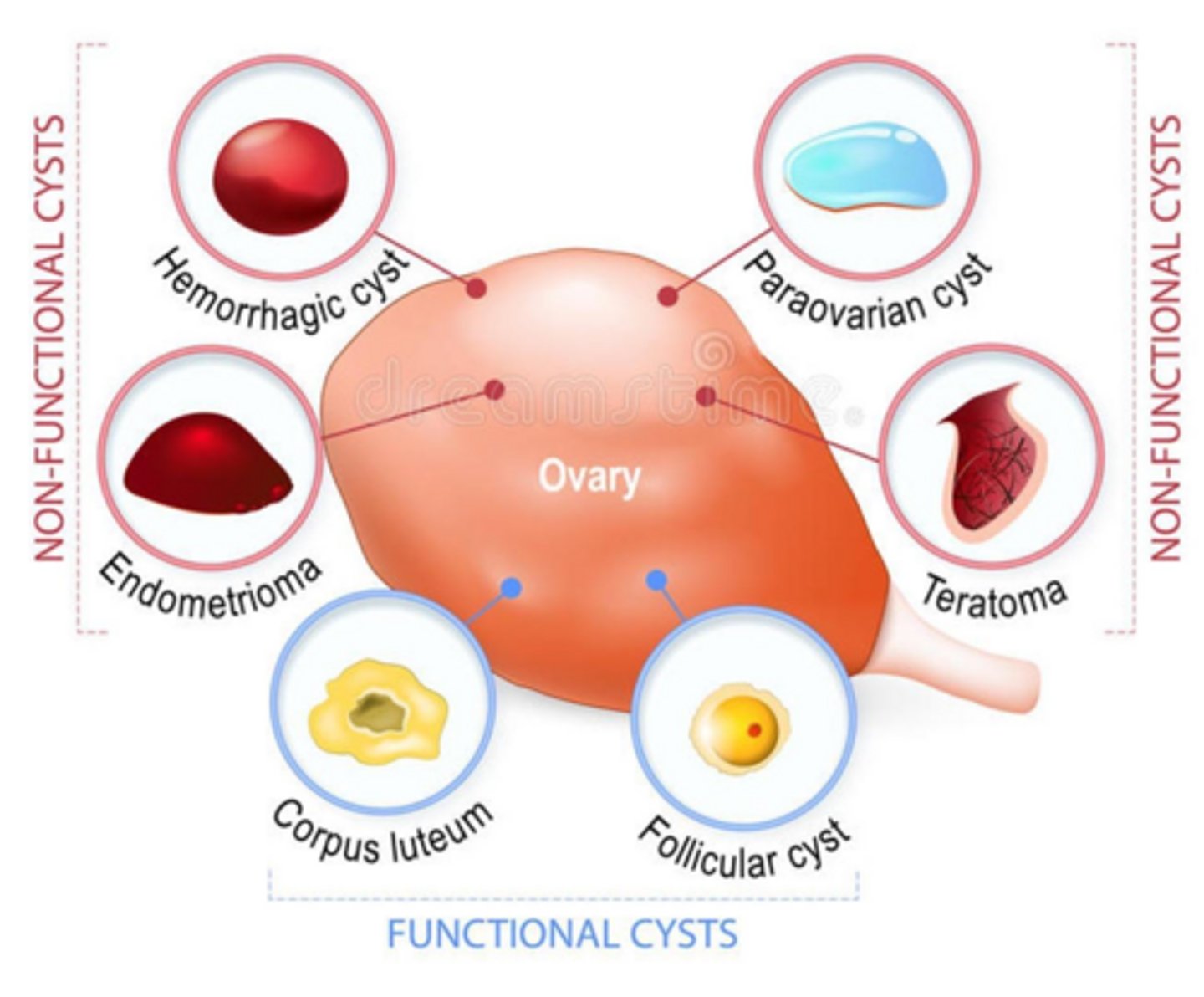
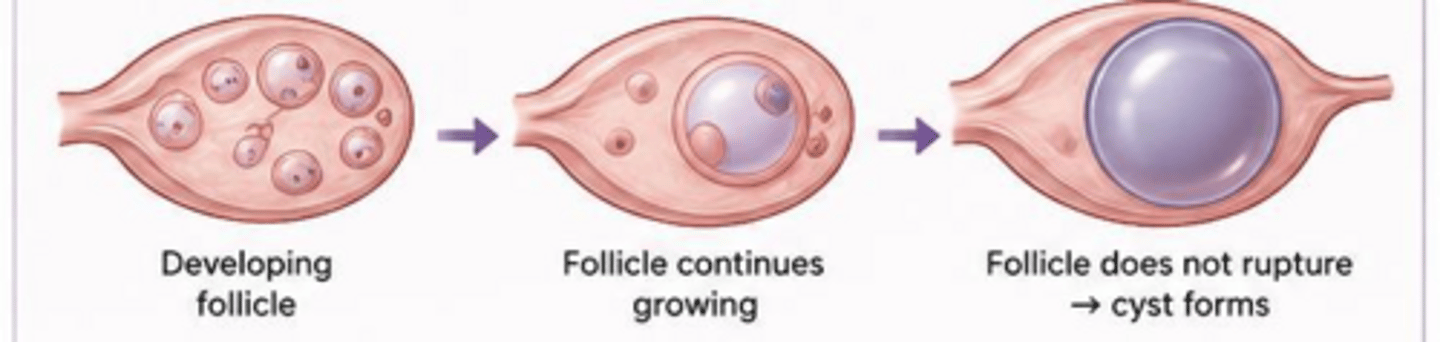
What is the pathogenesis of a follicular cyst?
Occurs when the dominant follicle fails to rupture or an immature follicle fails to undergo atresia.
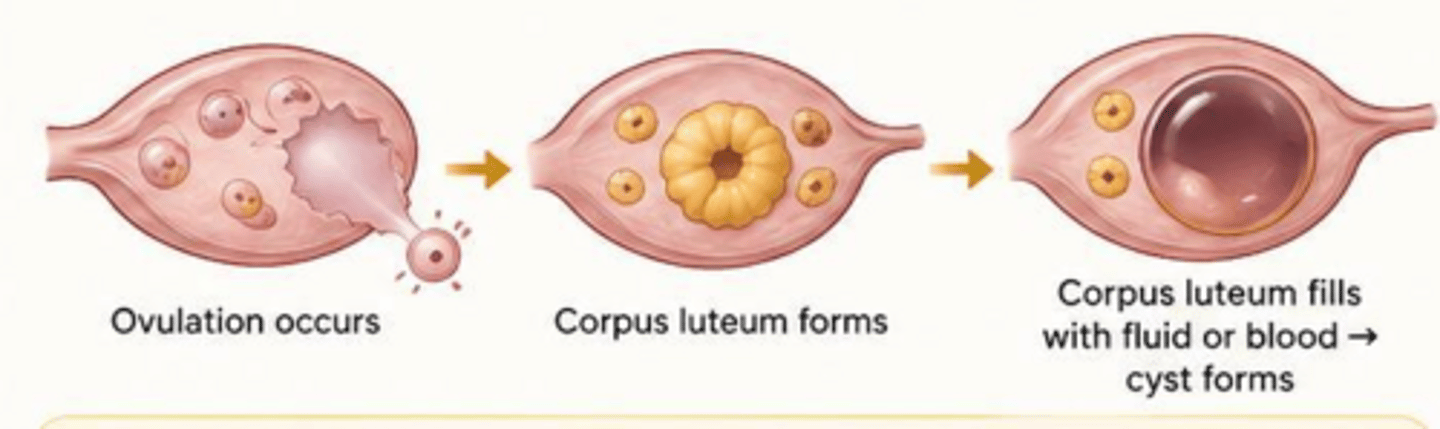
What is the pathogenesis of a corpus luteum cyst?
Occurs when the corpus luteum fails to regress after ovulation and instead seals off, filling with blood or fluid.
What is the standard management for a simple functional ovarian cyst?
Expectant management ('watchful waiting'), as most resolve in 1-2 menstrual cycles.
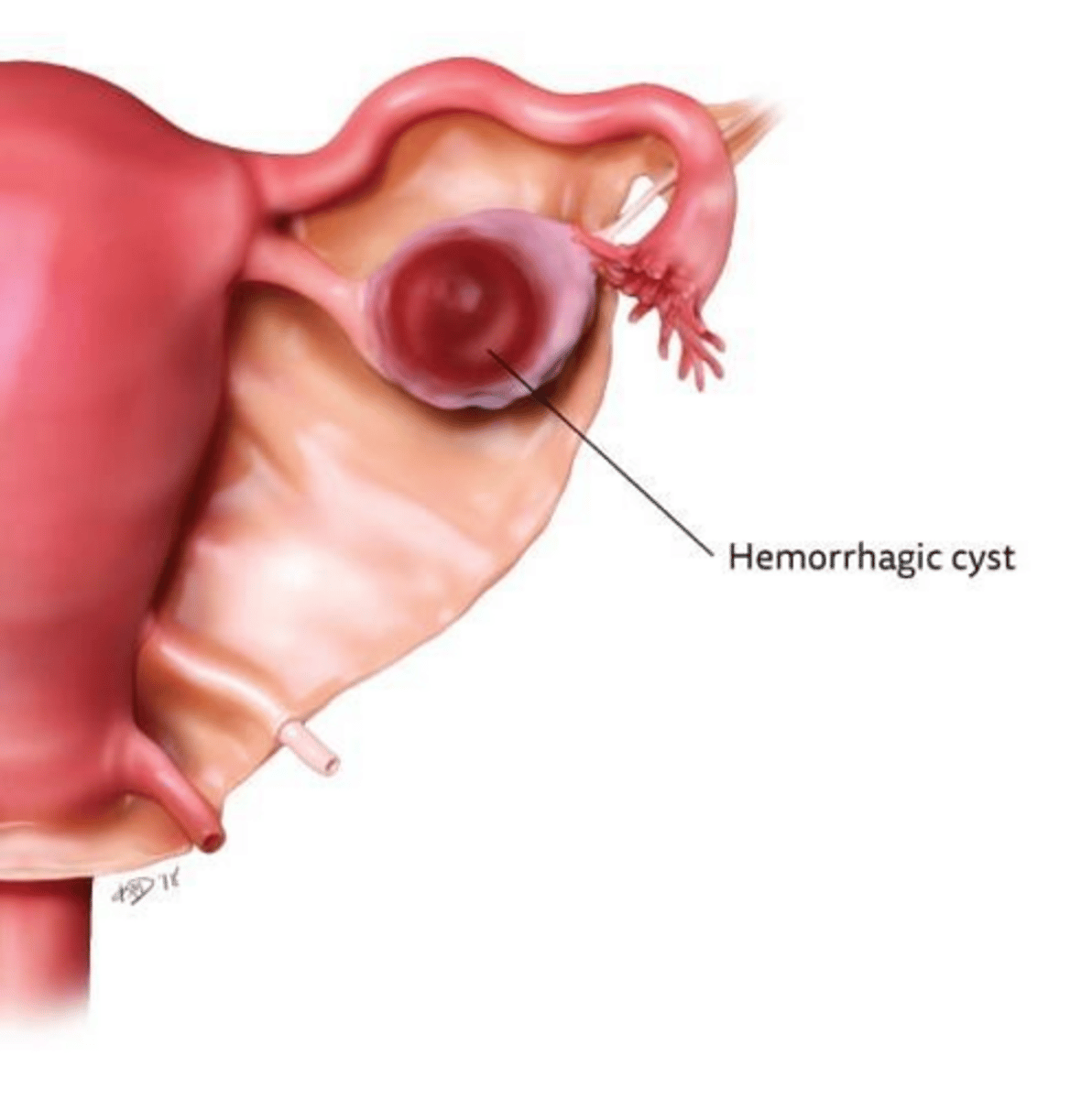
What is the pathogenesis of a hemorrhagic cyst?
Bleeding occurs into a functional cyst (most commonly a corpus luteum)
When should a simple ovarian cyst be re-evaluated via ultrasound?
If it is greater than 5 cm, repeat ultrasound in 6-8 weeks.
What ultrasound finding is classic for a hemorrhagic cyst?
A 'fishnet' or 'cobweb' reticular pattern (fibrin strands) or a variable solid appearance.
Which patient population is at high risk for massive hemorrhage from ovarian cysts?
Anticoagulated patients.
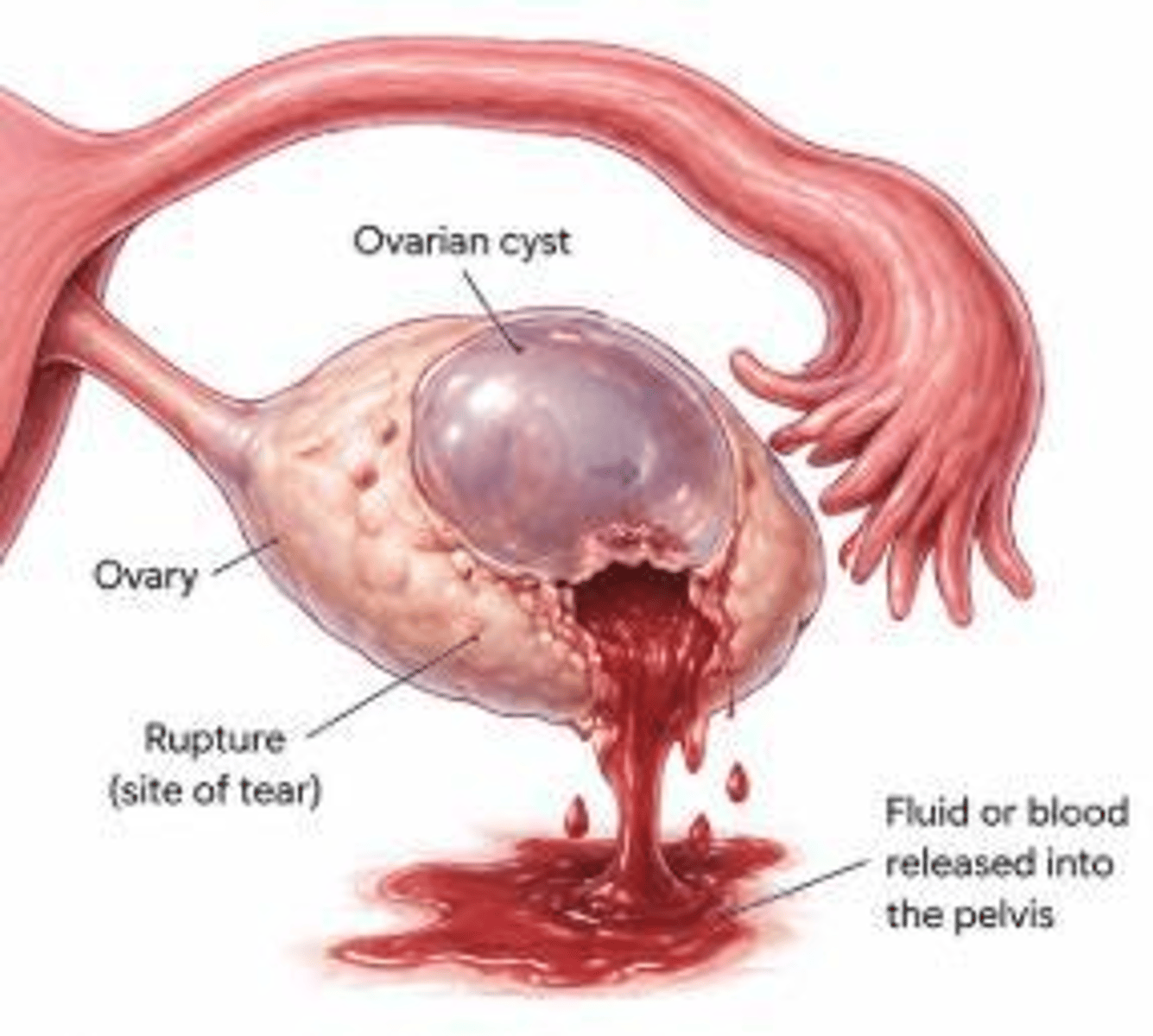
What is Kehr's sign in the context of a ruptured ovarian cyst?
Referred shoulder pain caused by hemoperitoneum irritating the diaphragm.
What is the mandatory lab test for a patient presenting with a suspected ruptured ovarian cyst?
Beta-hCG, to rule out ectopic pregnancy.
What is the management for a hemodynamically unstable patient with a ruptured ovarian cyst?
Surgical intervention for hemostasis.
What type of cyst is non-functional?
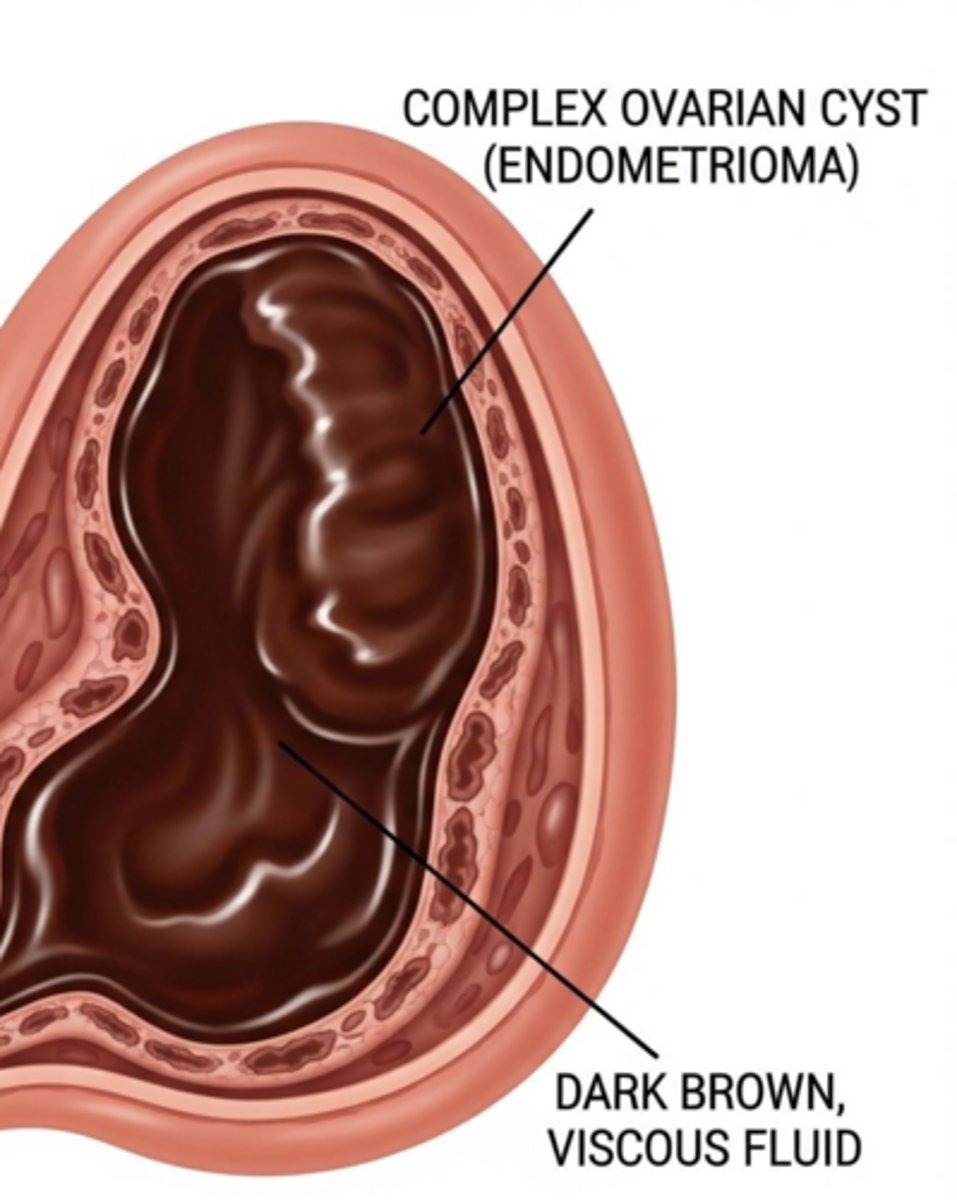
Endometriomas
What are the clinical features of an endometrioma ('chocolate cyst')?
Chronic pelvic pain, dysmenorrhea, and dyspareunia.
What is the characteristic ultrasound appearance of an endometrioma?
Homogeneous internal 'ground-glass' echoes.
When is a surgical cystectomy considered for endometriomas?
If cyst is large >3cm or if infertility is a concern.
What are the symptoms of a ruptured endometrioma?
Acute, excruciating pelvic pain.
Why is a ruptured endometrioma considered a surgical emergency?
The 'chocolate' fluid is highly caustic to the peritoneum, causing an intense chemical inflammatory response (chemical peritonitis).
How do you diagnose a ruptured endometrioma?
Elevated WBC count and inflammatory markers due to chemical peritonitis.
What is the classic clinical triad for a tubo-ovarian abscess (TOA)?
Fever, chills, and acute pelvic pain, often with vaginal discharge.
What is the first-line management for a tubo-ovarian abscess?
Inpatient IV antibiotics (Ceftriaxone, Doxycycline, and Metronidazole).
When is surgical drainage indicated for a tubo-ovarian abscess?
If there is no response to medical therapy within 48-72 hours.
What is a hydrosalpinx?
Distension of the fallopian tube with fluid, usually due to distal blockage from prior PID, ectopic pregnancy, or surgery.
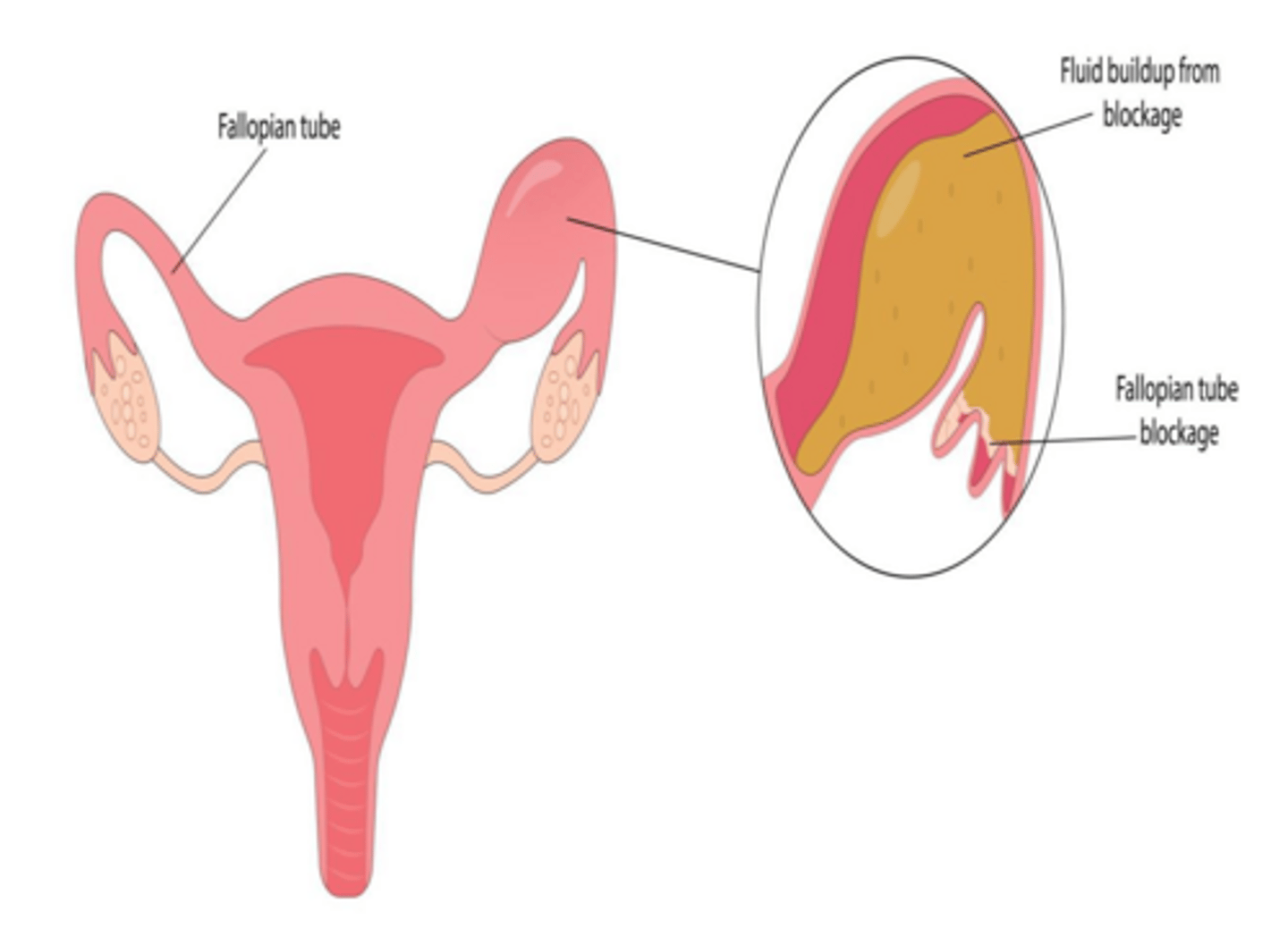
What is the characteristic ultrasound appearance of a hydrosalpinx?
A sausage-shaped, cystic structure separate from the ovary.
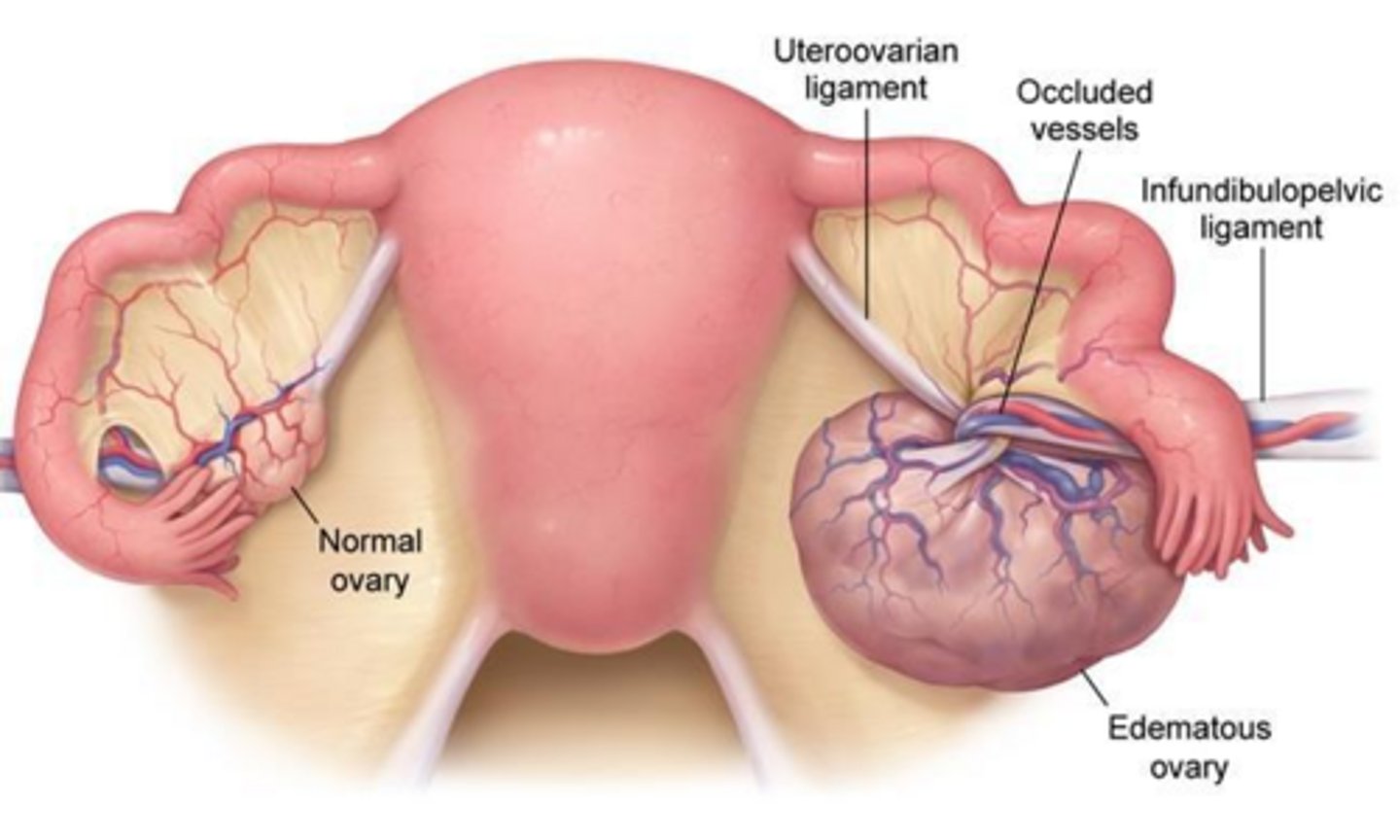
What is the pathogenesis of ovarian torsion?
Partial or complete rotation of the ovary on its vascular pedicle, leading to ischemia and necrosis.
What is the most common clinical presentation of ovarian torsion?
Sudden-onset, severe, sharp, unilateral pelvic pain, often accompanied by nausea and vomiting.
Does normal blood flow on Doppler ultrasound rule out ovarian torsion?
No, normal flow does not rule out torsion. For testing purposes, IT DOES.
What is the management for ovarian torsion?
Laparoscopic detorsion and assessment of viability.
What is the classic clinical triad for an ectopic pregnancy?
Amenorrhea, vaginal bleeding, and pelvic pain.
What are the diagnostic criteria for an ectopic pregnancy using TVUS?
An empty uterus combined with a tubal ring sign (gestational sac outside the uterus).

When is Methotrexate indicated for the management of an ectopic pregnancy?
When the patient is hemodynamically stable, hCG is <5000, there are no fetal heart tones, and no absolute contraindications exist.
Why is ovarian cancer often referred to as the 'silent killer'?
Symptoms are often vague and non-specific until the disease reaches an advanced stage (Stage III+).
What is an 'omental cake' in the context of ovarian cancer?
A firm mass in the upper abdomen, often palpable on physical exam.
What is a Sister Mary Joseph nodule?
A palpable, often painful, and sometimes discolored nodule in the umbilicus, indicating potential malignancy.
Name three protective factors against ovarian cancer related to ovulation.
Combined hormonal contraceptives, DEPO use pregnancy/breastfeeding, and tubal ligation/salpingectomy.
What is the initial study method of choice for ovarian masses?
TVUS
Why is it contraindicated to biopsy a suspected ovarian mass?
Biopsy can cause the tumor to 'seed' the peritoneum.
What is the primary role of CA-125 in ovarian cancer management?
Monitoring treatment response; it is unreliable for screening in pre-menopausal women.
What type of imaging is crucial for staging of ovarian cancer?
CT abdomen/pelvis.
What are the 3 kinds of histologic classifications of ovarian cancer?
Epithelial (90%), germ cell, and sex-cord stromal
Which histologic subtype of ovarian cancer is most common?
Epithelial tumors (specifically Serous Cystadenocarcinoma).
What are Psammoma bodies and which ovarian tumor are they associated with?
Concentric calcifications associated with Serous Cystadenocarcinoma.
What marker is used for epithelial tumors?
CA-125. Used for treatment monitoring, not screening.
Which germ cell tumor is the most common malignant germ cell tumor of the ovary?
Dysgerminoma.
What marker is used for dysgerminoma?
LDH (Lactate dehydrogenase)
Which tumor marker is associated with Yolk Sac Tumors?
Alpha-fetoprotein (AFP).
What is the most common benign ovarian neoplasm and why is it prone to torsion?
Mature Cystic Teratoma (Dermoid Cyst); it is prone to torsion due to its weight and buoyancy.
What is Meigs syndrome?
A triad of ovarian fibroma, ascites, and right-sided pleural effusion.
What do thecomas secrete?
Estrogen. This can increase the risk of endometrial cancer.
What is the standard surgical management for ovarian cancer?
TAH-BSO (Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy), omentectomy, and lymph node sampling.
What is the current recommended approach to breast screening for average-risk women?
Breast self-awareness; formal monthly Breast Self-Exams (BSE) are not routinely recommended due to high false-positive rates.
What are the most common breast complaint and what is the most important step in evaluation?
Pain and mass; History
What is the best time during the menstrual cycle to perform a breast exam?
Days 7-10 (late follicular phase), when breasts are least tender and nodular.
Why does breast exam accuracy decrease during the luteal phase?
Progesterone-driven epithelial cell proliferation makes breasts more tender and nodular.
What is the recommended patient position for breast palpation?
Supine with the ipsilateral arm raised overhead to flatten breast tissue against the chest wall.
Which finger pads should be used during breast palpation?
The pads of the 2nd, 3rd, and 4th fingers.
What is the most effective pattern for total breast coverage during palpation?
The vertical strip pattern.
How many levels of pressure should be applied at each palpation location?
Three levels: light, medium, and deep.
What details must be included when documenting a palpable breast mass?
Location (laterality, clock position/quadrant, distance from nipple), size (cm), consistency, mobility, borders, and tenderness.
What is the primary advantage of 3D Tomosynthesis Mammography?
It takes multiple slices of the breast to see through dense tissue and reduces call-back rates.
According to USPSTF 2024 guidelines, at what age should average-risk breast cancer screening begin?
Age 40.
What is the recommended frequency for screening mammography according to the USPSTF?
Biennial (every 2 years).
At what age is routine mammography screening typically discontinued?
Age 74 or 75, depending on the organization and shared decision-making.
What is the recommended screening protocol for BRCA 1/2 carriers?
Annual MRI starting at age 25, with the addition of an annual mammogram at age 30.
What is the '10-year rule' for family history in breast cancer screening?
Annual mammogram and MRI beginning no later than age 40 or 10 years before the youngest affected family member's diagnosis.
What is the preferred initial imaging modality for a palpable breast mass in a pregnant patient?
Ultrasound.
Which imaging modality is the first-line study for a breast mass in patients aged 40 and older?
Diagnostic mammography.
What is the first-line imaging modality for a breast mass in patients under age 30?
Ultrasound, to avoid unnecessary radiation due to high breast density.
What are the clinical characteristics of a fibroadenoma?
Solid, mobile, painless, and well-circumscribed; typically seen in ages 15-35.
How can a breast cyst be differentiated from a solid mass on ultrasound?
A cyst is fluid-filled, whereas a solid mass will appear as a solid structure.
What are the classic clinical characteristics of breast carcinoma?
Hard, fixed, irregular borders, and painless; typically seen in patients aged 50 and older.
What are four mammogram findings of concern?
Microcalcifications, spiculated mass, distortion of normal architecture, and any discrete nonpalpable lesion.
What does the BI-RADS system communicate to physicians?
It categorizes the likelihood of breast cancer and provides standardized recommendations for follow-up.
At what BI-RADS score is a biopsy typically warranted?
BI-RADS 4 and greater.
Why is ultrasound preferred over mammography for younger patients?
Younger patients often have denser breast tissue, which ultrasound can evaluate more effectively than mammography.
What is the recommended screening for patients with extremely dense breasts (BI-RADS D)?
Supplemental breast MRI (Category 1 for ages 50-75).
What is the clinical presentation of fat necrosis in the breast?
Firm, irregular mass, usually following trauma or surgery.
What is the recommended screening frequency for average-risk women according to NCCN?
Annual mammography starting at age 40.
What are the indications for breast MRI screening in high-risk women?
BRCA 1 and 2 mutations, residual lifetime risk ≥20%, and prior chest radiation.
Why is Gadolinium-based contrast contraindicated in pregnancy?
It is contraindicated because it crosses the placenta and may pose risks to the fetus.
What is the goal of an excisional biopsy?
To remove the entire abnormality.
What is the primary utility of Fine-Needle Aspiration (FNA) in a palpable breast lump?
To determine if the lump is a simple cyst.
What findings in a breast cyst aspirate require further diagnostic evaluation?
Bloody aspirate, no fluid obtained (solid mass), residual mass after fluid withdrawal, or rapid recurrence.
What is the preferred initial biopsy approach for a solid breast mass?
Core-needle biopsy (14-16 gauge).
What are the clinical characteristics of physiologic nipple discharge?
Bilateral, multi-ductal, and non-spontaneous (occurs only with expression).
What are the clinical characteristics of pathologic nipple discharge?
Unilateral, single-duct, and spontaneous.
What is the most common cause of bloody nipple discharge?
Intraductal papilloma.
What is the first-line diagnostic imaging for pathologic nipple discharge?
Diagnostic mammogram.
What is the definition of galactorrhea?
Non-lactational milk production due to excess prolactin (disruption of the tuberoinfundibular pathway).
What is the initial step in the workup of galactorrhea?
Pregnancy test (hCG) to rule out physiologic lactation.
What is the first-line medication for hyperprolactinemia-induced galactorrhea?
Cabergoline or bromocriptine.
When does cyclic mastalgia typically occur?
During the luteal phase of the menstrual cycle.
What is the most effective first-line treatment for mastalgia?
Reassurance after a negative physical exam (and imaging if indicated).
What is the most common pathogen in mastitis?
Staphylococcus aureus.
What is the recommended management for mastitis in a breastfeeding mother?
Antibiotics (Dicloxacillin or Cephalexin) and continuing to breastfeed.