fluid, electrolyte, and acid-base balance
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
Water percentage of body
60% of body
Compartments of fluid
separated by selectively permeable membranes, moving from one side to the other
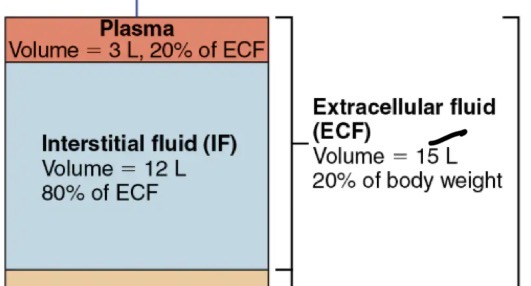
Extracellular fluid: plasma + interstitial fluid
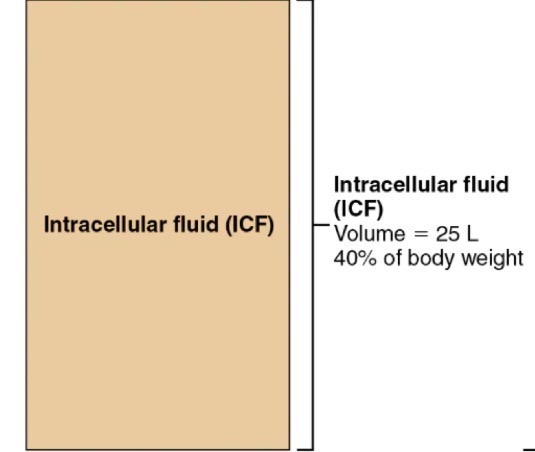
Intracellular fluid
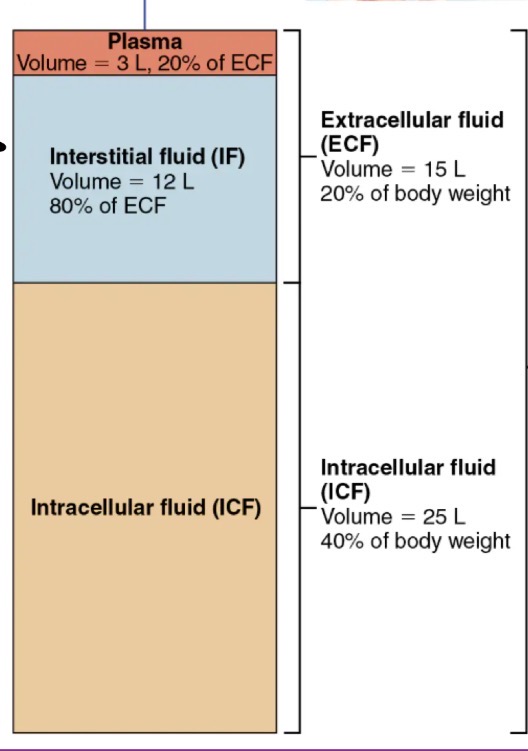
Extracellular fluid
plasma (in blood vessels)
Interstitial fluid (on cell side)
Intracellular fluid
in cells
Composition of body fluids
solutes
Electrolytes
Nonelectrolytes
Solutes in body fluids
What is dissolved in water
Electrolytes in body fluids
Compounds that dissociate into ions in water
has a greater osmotic power than nonelectrolytes
Has a greater ability to cause fluid shifts
Nonelectrolytes in body fluids
Do not dissociate in water
eg. glucose, lipids, creatine, and urea
Do not really conduct electricity
Universal solvent
Can dissolve a lot of solutes (WATER!)
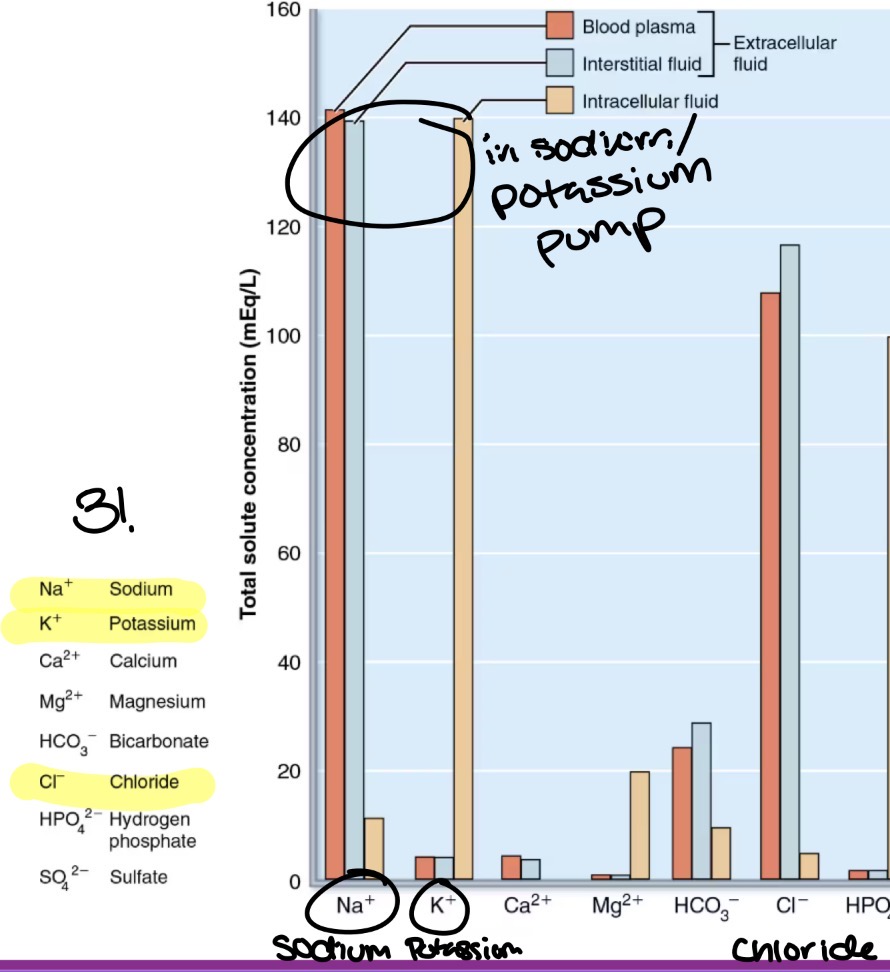
Comparison of Extracellular and Intracellular fluids
Opposite of each other due to cellular ATP dependent Na+/K+ pumps
Extracellular: more sodium (Na+) and very little potassium (K+)
Intracellular: more potassium (K+) and very little sodium (Na+)
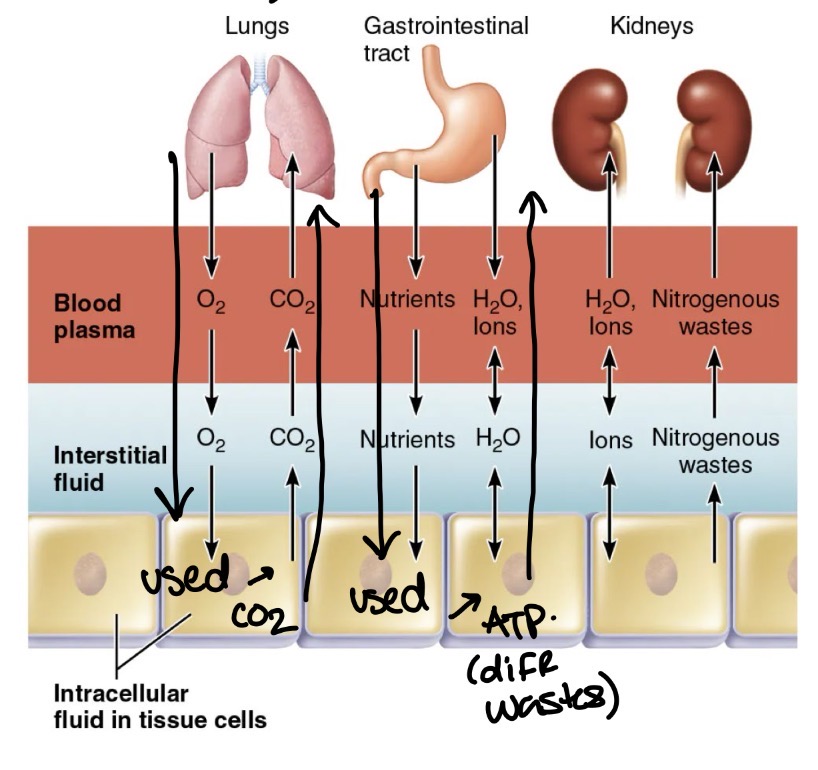
Fluid movement in compartments
between plasma and IF across capillary walls
Between IF and ICF across cell membrane
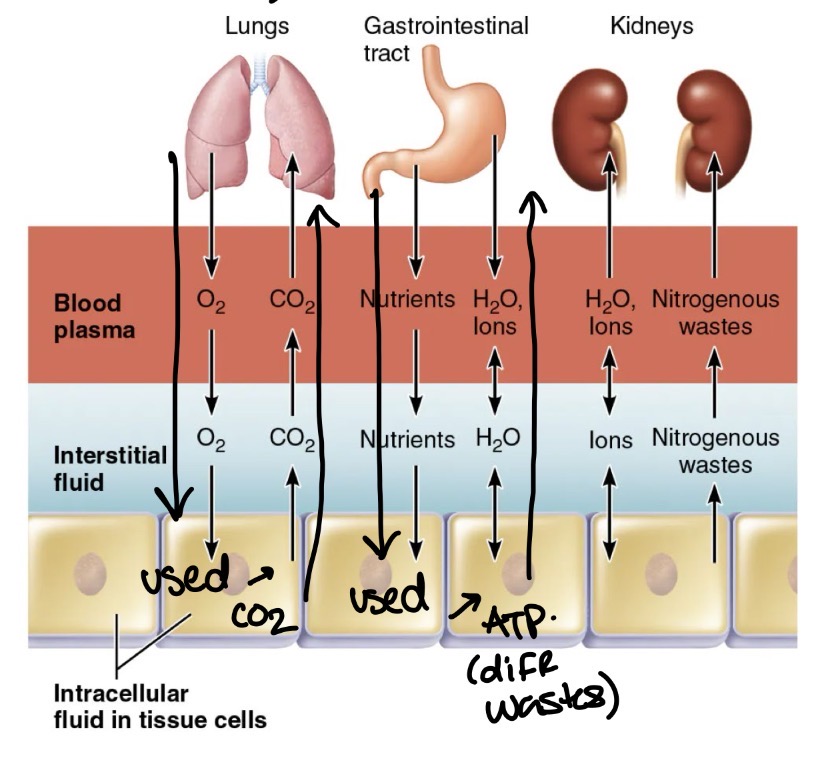
Fluid movement between plasma and IF
Across capillary walls
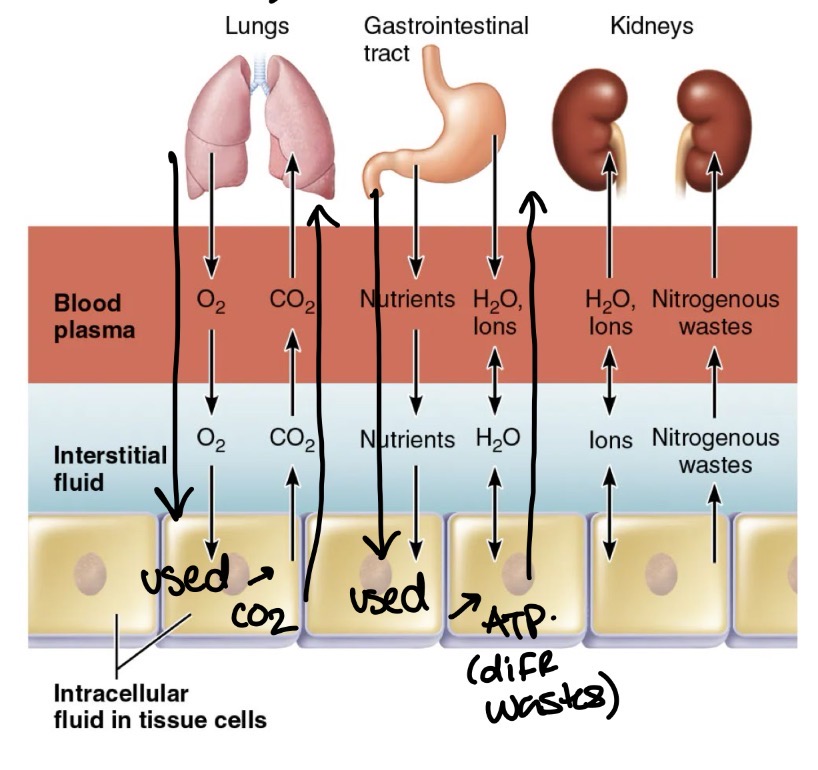
Fluid movement between IF and ICF
Across cell membrane
water: 2 way osmotic flow
Nutrients, wastes, gases: unidirectional
Ions: move selectively
Changes in solute concentration in any compartment…
Leads to net water flows
Major sources of water intake & output
Regulated by:
sensory receptors (eg. baroreceptors): osmolarity, blood volume, blood pressure
Hypothalamus: thirst center
Hormones
Kidneys
Cardiovascular System: ANP hormone detect if water needs to one in
Regulations of water intake by hypothalamic thirst center
hypothalamic osmoreceptors detect ECF osmolality; activated by
Increases plasma osmolality of 1-2%
Dry mouth
Decreased blood volume or pressure
Angiotensin II or baroreceptor input
Maintenance of Body Fluid Osmolality
maintained at 300 mOsm
Rise in osmolality (dehydration)
Blood becomes salty
stimulates this mechanism, ADH (antidiuretic hormone) release to kidneys
Decreased BP → Renin-angiotensin-aldosterone mechanism from kidneys activated
Increased thirst, decreased urine (to not waste water), restore Blood Pressure
Decrease in osmolality (hyperhydration)
thirst inhibition
ADH (antidiuretic hormone) inhibition (NOT released)
Increased Blood volume/BP → Atrial Natriuretic peptide: stretch receptors in right atrium dilate blood vessels to decrease BP + increase urine output to decrease blood volume
Hypotonic Hydration
ECF is diluted (too much water)
Hyponatremia
ECF is low in solute concentration (low sodium)
Edema
Accumulation of fluid in interstitial space (pitting edema)
causes Hyponatremia

Electrolyte balance
Includes salts, acids, and bases
Salts provide
neuromuscular excitability
Secretory activity
Membrane permeability
Sodium imbalances
Hypernatremia; Sodium excess
Hyponatremia: Sodium deficit
Hypernatremia
Excess sodium
caused by dehydration
Consequences: thirsty, confused, lethargic, possible coma, twitching, convulsions
Hyponatremia
Sodium deficit
caused by excess water retention, excess water intake, vomiting, diarrhea, burned skin, gastric suction, diuretics, less aldosterone, renal diseases, excess ASH release
Consequences: decreased blood volume and blood pressure (excess water: confusion, coma, twitching, convulsions)
Potassium imbalances
Hyperkalemia: potassium excess
Hypokalemia: potassium deficit
Hyperkalemia
Potassium excess
caused by renal failure, aldosterone deficit, burns or severe tissue injuries that cause K+ to leave cells
Consequences: nausea, vomiting, diarrhea, bradycardia, cardiac arrest, skeletal muscle weakness, flaccid paralysis
Hypokalemia
Potassium deficit
caused by GI tract disturbances (vomiting/diarhea), gastric suction, starvation, excess aldosterone, diuretic therapy
Consequences: cardiac arrhythmias, flattened T wave on ECG, muscular weakness, confusion, nausea/vomiting
Calcium imbalances
hypercalcemia: calcium excess
Hypocalcemia: calcium deficit
Hypercalcemia
Calcium excess
caused by hyperparthyroidism, excess vitamin D, prolonged immobilization, renal disease (decreased excretion)
Consequences: decreased neuromuscular excitability leading to cardiac arrest, skeletal muscle weakness, confusion, coma, kidney atones, nausea/vomiting
Hypocalcemia
Calcium deficit
Caused by burns in damaged tissues, hypoparathyroidism, Vit D deficiency, renal tubular diseases, renal failure, diarrhea
consequences: increases neuromuscular excitability leading to tingling fingers, tremors, skeletal muscle cramps, convulsions,
Sodium balance
Most significant
cotransport
RMP
Depolarization